
Heart Rate, Stress, and Occupational Noise Exposure among Electronic Waste Recycling Workers



Abstract
:1. Introduction
2. Experimental Section
2.1. Overview
2.2. Site Description and Recruitment

2.3. Questionnaire and Activity Log
2.4. Noise Exposure and Heart Rate Measurements
2.5. Data Cleaning and Statistical Analysis
3. Results
3.1. Demographics

{kind=link}
{kind=link}
| Variable | N | Mean | SD |
|---|---|---|---|
| Age (years) | 57 | 25.8 | 7.9 |
| Daily work duration (hours) | 53 | 10.5 | 2.2 |
| Work experience (years) | 53 | 5.8 | 3.9 |
| Daily income (GHS) | 57 | 2.3 | 1.4 |
| Duration lived at Agbogbloshie (years) | 57 | 6 | 4.2 |
| PSS score | 53 | 25 | 5.2 |
| Category | N | % | |
| Sleep near Agbogbloshie | 56 | 98.2 | |
| Marital status | Single | 22 | 38.6 |
| Married | 32 | 56.1 | |
| Divorced/Separated | 3 | 5.3 | |
| Education | None | 31 | 54.4 |
| Primary | 11 | 19.3 | |
| Middle/JSS | 12 | 21.1 | |
| Secondary/SSS | 3 | 5.3 | |
| Experience tinnitus | Never | 13 | 22.8 |
| Almost never | 5 | 8.8 | |
| Sometimes | 21 | 36.8 | |
| Fairly often | 4 | 7.0 | |
| Very often | 14 | 24.6 | |
| Experience exhaustion after work | Sometimes | 4 | 7.0 |
| Almost always | 21 | 36.8 | |
| Always | 31 | 54.4 | |
| Experienced shortness of breath or difficulty in breathing in last two weeks | Never | 21 | 36.8 |
| Almost never | 6 | 10.5 | |
| Sometimes | 21 | 36.8 | |
| Almost always | 5 | 8.8 | |
| Always | 4 | 7.0 | |
| Experienced dizziness over the last two weeks? | Never | 15 | 26.3 |
| Almost never | 6 | 10.5 | |
| Sometimes | 25 | 43.9 | |
| Almost always | 7 | 12.3 | |
| Always | 4 | 7.0 | |
| Experienced heart beating abnormally over the last two weeks? | Never | 10 | 17.5 |
| Almost never | 4 | 7.0 | |
| Sometimes | 26 | 45.6 | |
| Almost always | 9 | 15.8 | |
| Always | 8 | 14.0 | |
| Diagnosed with high blood pressure | 7 | 12.3 | |
| On medication | 1 | 1.8 | |
| Experience difficulties hearing | 15 | 26.3 | |
| Diagnosed with hearing loss? | 2 | 3.5 |
3.2. Self-Reported Exposures
| Variable | Category | N | % |
|---|---|---|---|
| Exposed to noise at work | 55 | 95.9 | |
| Bothered/annoyed by loud noise at work | Not at all | 13 | 22.8 |
| A little | 24 | 42.1 | |
| A great deal | 20 | 35.1 | |
| Exposed to noise away from work | 45 | 78.9 | |
| Bothered/annoyed by noise at night | Not at all | 16 | 28.1 |
| A little | 21 | 36.8 | |
| A great deal | 20 | 35.1 | |
| Sleep affected by noise at night | Never | 14 | 24.6 |
| Almost never | 7 | 12.3 | |
| Sometimes | 19 | 33.3 | |
| Fairly often | 7 | 12.3 | |
| Very often | 10 | 17.5 | |
| Exposed to unfavorable physical conditions at work | Never | 2 | 3.5 |
| Sometimes | 20 | 35.1 | |
| Almost always | 9 | 15.8 | |
| Always | 26 | 45.6 | |
| Experience violence or harassment at work | Never | 1 | 1.8 |
| Almost never | 6 | 10.5 | |
| Sometimes | 34 | 59.6 | |
| Almost always | 10 | 17.5 | |
| Always | 5 | 8.8 | |
| Income insufficient to support self and family | Never | 3 | 5.3 |
| Almost never | 4 | 7.0 | |
| Sometimes | 12 | 21.1 | |
| Almost always | 11 | 19.3 | |
| Always | 25 | 43.9 |
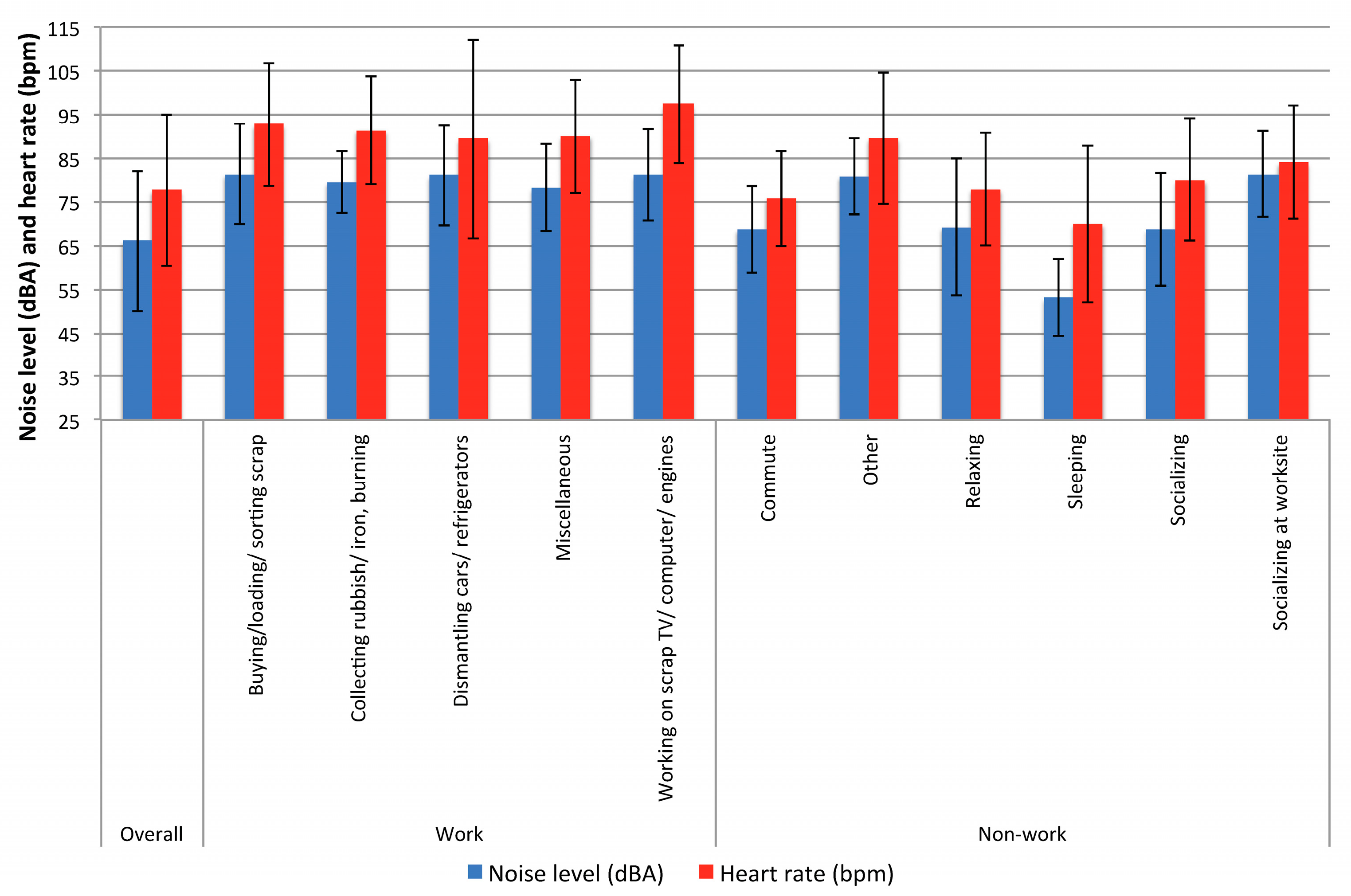
3.3. Noise Exposure and Heart Rate Measurements
| Activity | N Subjects Reporting | Duratio (min) | Subject Duration (min) | Subject Noise Level (dBA) ** | Heart Rate (bpm) | |||
|---|---|---|---|---|---|---|---|---|
| Mean | SD | Mean | SD | Mean | SD | |||
| Overall | 57 * | 45098 | 791.2 | 604.6 | 66.0 | 16.0 | 77.7 | 17.3 |
| Occupational | 20 | 4830 | 966 | 798.1 | 80.8 | 11.0 | 91.8 | 17.4 |
| Buying, loading, or sorting scrap | 5 | 1815 | 363 | 10.6 | 81.3 | 11.4 | 92.7 | 14.0 |
| Collecting rubbish or iron, burning | 3 | 274 | 91.3 | 29.2 | 79.6 | 7.2 | 91.4 | 12.5 |
| Dismantling cars or refrigerators | 10 | 1579 | 157.9 | 106.1 | 81.0 | 11.4 | 89.4 | 22.8 |
| Miscellaneous | 3 | 476 | 158 | 5.3 | 78.2 | 9.9 | 90.1 | 13.0 |
| Working on scrap TV/computer/car engines | 2 | 619.0 | 309.4 | 204.2 | 81.1 | 10.5 | 97.3 | 134. |
| Non-occupational | 53 | 30473 | 575 | 509 | 63.1 | 15.9 | 74.9 | 16.7 |
| Commute | 48 | 2974 | 48.0 | 40.0 | 68.7 | 10.0 | 75.7 | 10.9 |
| Other | 3 | 229 | 76.4 | 105.9 | 80.9 | 8.8 | 89.5 | 15.0 |
| Relaxing | 38 | 7549 | 199 | 66.0 | 69.2 | 15.6 | 78.0 | 13.0 |
| Sleeping | 41 | 15814 | 386 | 289 | 53.0 | 8.8 | 70.0 | 18.0 |
| Socializing | 10 | 1110 | 111 | 88.0 | 68.7 | 12.9 | 80.0 | 14.0 |
| Socializing at the work site | 32 | 5505 | 172 | 27.0 | 81.3 | 9.8 | 84.0 | 13.0 |

| Parameter | Model 1 | Model 2 | Model 3 | ||||||
|---|---|---|---|---|---|---|---|---|---|
| Coefficient | SE | p-Value | Coefficient | SE | p-Value | Coefficient | SE | p-Value | |
| Intercept | 52.5 | 5.1 | 0.001 | 52.2 | 17.2 | 0.00 | 88.1 | 34.4 | 0.01 |
| Around smokers | |||||||||
| No | 2.6 | 1.4 | 0.06 | −20.1 | 2.2 | 0.00 | 11.5 | 4.7 | 0.01 |
| Yes | Ref | Ref | Ref | Ref | Ref | Ref | Ref | Ref | Ref |
| Age (years) | −0.1 | 0.1 | 0.3 | 0.6 | 0.6 | 0.3 | 0.8 | 0.6 | 0.15 |
| Income (Cedis) | −1.4 | 0.8 | 0.07 | −0.3 | 2.3 | .0.9 | -2.8 | 1.9 | 0.13 |
| LEQ noise level (dBA) ** | 0.5 | 0.05 | 0.001 | 0.3 | 0.1 | 0.01 | 0.2 | 0.08 | 0.01 |
| Work activity | |||||||||
| Dismantling cars or refrigerators | −7.8 | 7.7 | 0.3 | −11.4 | 6.5 | 0.08 | |||
| Collecting rubbish or iron, burning | −0.3 | 6.1 | 1.0 | 4.1 | 6.2 | 0.51 | |||
| Buying, loading, or sorting scrap | −0.6 | 7.6 | 0.9 | −12.1 | 7.0 | 0.08 | |||
| Working scrap TV/computer/car engines | 17.0 | 5.4 | 0.00 | −4.1 | 7.2 | 0.60 | |||
| Miscellaneous | Ref | Ref | Ref | Ref | Ref | Ref | |||
| Noise away from work | |||||||||
| No | −30.5 | 6.7 | 0.001 | ||||||
| Yes | Ref | Ref | Ref | ||||||
| Exposed to unfavorable physical work conditions | |||||||||
| Sometimes | −20.2 | 3.4 | 0.001 | ||||||
| Almost always | −20.9 | 7.0 | 0.003 | ||||||
| Always | Ref | Ref | Ref | ||||||
| PSS score | −0.3 | 0.74 | 0.7 | ||||||
4. Discussion
Limitations
5. Conclusions
Acknowledgments
Author Contributions
Conflicts of Interest
References
- Kang, H.-Y.; Schoenung, J. M. Electronic waste recycling: A review of U.S. infrastructure and technology options. Resour. Conserv. Recycl. 2005, 45, 368–400. [Google Scholar] [CrossRef]
- Baldé, C.P.; Wang, F.; Kuehr, R.; Huisman, J. The Global E-Waste Monitor; UNU-IAS: Bonn, Germany, 2014. [Google Scholar]
- Kiddee, P.; Naidu, R.; Wong, M.H. Electronic waste management approaches: An overview. Waste Manag. 2013, 33, 1237–1250. [Google Scholar] [CrossRef] [PubMed]
- Yu, L.; He, W.; Li, G.; Huang, J.; Zhu, H. The development of WEEE management and effects of the fund policy for subsidizing WEEE treating in China. Waste Manag. 2014, 34, 1705–1714. [Google Scholar] [CrossRef] [PubMed]
- He, Y.; Xu, Z. The status and development of treatment techniques of typical waste electrical and electronic equipment in China: A review. Waste Manag. Res. 2014, 32, 254–269. [Google Scholar] [CrossRef] [PubMed]
- Itai, T.; Otsuka, M.; Asante, K.A.; Muto, M.; Opoku-Ankomah, Y.; Ansa-Asare, O.D.; Tanabe, S. Variation and distribution of metals and metalloids in soil/ash mixtures from Agbogbloshie e-waste recycling site in Accra, Ghana. Sci. Total Environ. 2014, 470–471, 707–716. [Google Scholar] [CrossRef] [PubMed]
- Feldt, T.; Fobil, J.N.; Wittsiepe, J.; Wilhelm, M.; Till, H.; Zoufaly, A.; Burchard, G.; Göen, T. High levels of PAH-metabolites in urine of e-waste recycling workers from Agbogbloshie, Ghana. Sci. Total Environ. 2014, 466–467, 369–376. [Google Scholar] [CrossRef] [PubMed]
- Song, Q.; Li, J. Environmental effects of heavy metals derived from the e-waste recycling activities in China: A systematic review. Waste Manag. 2014, 34, 2587–2594. [Google Scholar] [CrossRef] [PubMed]
- Schuelp, M.; Hagelueken, C.; Kuehr, R.; Magalini, F.; Maurer, C.; Meskers, C.; Mueller, E.; Wang, F. Recycling from E-Waste to Resources; Oktoberdruck AG: Berlin, Germany, 2009. [Google Scholar]
- Basner, M.; Babisch, W.; Davis, A.; Brink, M.; Clark, C.; Janssen, S.; Stansfeld, S. Auditory and non-auditory effects of noise on health. Lancet 2014, 383, 1325–1332. [Google Scholar] [CrossRef]
- Singhal, S.; Yadav, B.; Hashmi, S.F.; Muzammil, M. Effects of workplace noise on blood pressure and heart rate. Biomed. Res. 2009, 20, 122–126. [Google Scholar]
- Hohmann, C.; Grabenhenrich, L.; de Kluizenaar, Y.; Tischer, C.; Heinrich, J.; Chen, C. M.; Thijs, C.; Nieuwenhuijsen, M.; Keil, T. Health effects of chronic noise exposure in pregnancy and childhood: A systematic review initiated by ENRIECO. Int. J. Hyg. Environ. Health 2013, 216, 217–229. [Google Scholar] [CrossRef] [PubMed]
- Kraus, U.; Schneider, A.; Breitner, S.; Hampel, R.; Rückerl, R.; Pitz, M.; Geruschkat, U.; Belcredi, P.; Radon, K.; Peters, A. Individual daytime noise exposure during routine activities and heart rate variability in adults: A repeated measures study. Environ. Health Perspect. 2013, 121, 607–612. [Google Scholar] [PubMed]
- Sim, C.S.; Sung, J.H.; Cheon, S.H.; Lee, J.M.; Lee, J.W.; Lee, J. The effects of different noise types on heart rate variability in men. Yonsei Med. J. 2015, 56, 235–243. [Google Scholar] [CrossRef] [PubMed]
- Solenkova, N.V.; Newman, J.D.; Berger, J.S.; Thurston, G.; Hochman, J.S.; Lamas, G.A. Metal pollutants and cardiovascular disease: Mechanisms and consequences of exposure. Am. Heart J. 2014, 168, 812–822. [Google Scholar] [CrossRef] [PubMed]
- Wyss, S.; Ablordeppey, J.; Okrah, J.; Kyei, A. Reaching disenfranchised youth and mobile populations in Ghana through voluntary counselling and testing services for HIV. Afr. J. AIDS Res. 2007, 6, 121–128. [Google Scholar] [CrossRef] [PubMed]
- Grant, K.; Goldizen, F.C.; Sly, P.D.; Brune, M.-N.; Neira, M.; Van den Berg, M.; Norman, R.E. Health consequences of exposure to e-waste: A systematic review. Lancet. Glob. Heal. 2013, 1, 350–361. [Google Scholar] [CrossRef]
- Asampong, E.; Dwuma-Badu, K.; Stephens, J.; Srigboh, R.; Neitzel, R.; Basu, N.; Fobil, J.N. Health seeking behaviours among electronic waste workers in Ghana. BMC Public Health 2015. [Google Scholar] [CrossRef] [PubMed]
- Fogari, R.; Zoppi, A.; Vanasia, A.; Marasi, G.; Villa, G. Occupational noise exposure and blood pressure. J. Hypertens. 1994, 12, 475–479. [Google Scholar] [CrossRef]
- Chang, T.-Y.; Liu, C.-S.; Hwang, B.-F.; Hsieh, H.-H.; Bao, B.-Y.; Chen, C.-J.; Wang, V.-S.; Lai, J.-S. Acute effects of noise exposure on 24-h ambulatory blood pressure in hypertensive adults. J. Hypertens. 2015, 33, 507–514. [Google Scholar] [CrossRef] [PubMed]
- Kalantary, S.; Dehghani, A.; Yekaninejad, M.S.; Omidi, L.; Rahimzadeh, M. The effects of occupational noise on blood pressure and heart rate of workers in an automotive parts industry. ARYA Atheroscler. 2015, 11, 215–219. [Google Scholar] [PubMed]
- Cohen, S.; Kamarck, T.; Mermelstein, R. A global measure of perceived stress. J. Health Soc. Behav. 1983, 24, 385–396. [Google Scholar] [CrossRef] [PubMed]
- Neitzel, R.; Seixas, N.S.; Camp, J.; Yost, M. An assessment of occupational noise exposure in four construction trades. Am. Ind. Hyg. Assoc. J. 1999, 60, 807–817. [Google Scholar] [CrossRef] [PubMed]
- Neitzel, R.; Yost, M. Task-based assessment of occupational vibration and noise exposures in forestry workers. AIHA J. 2002, 63, 617–627. [Google Scholar] [CrossRef]
- Neitzel, R.; Seixas, N.; Olson, J.; Daniell, W.; Goldman, B. Nonoccupational noise: Exposures associated with routine activities. J. Acoust. Soc. Am. 2004, 115, 237–245. [Google Scholar] [CrossRef] [PubMed]
- Neitzel, R.L.; Svensson, E.B.; Sayler, S.K.; Ann-Christin, J. A comparison of occupational and nonoccupational noise exposures in Sweden. Noise Health 2014, 16, 270–278. [Google Scholar] [CrossRef] [PubMed]
- IEC. Electroacoustics—Sound Level Meters—Part 1: Specifications. Available online: https://webstore.iec.ch/publication/5708 (accessed on 10 October 2015).
- WHO Guidelines for Community Noise. Available online: http://www.quietskiescoalition.org/files/WHO_Guidelines_for_Community_Noise.pdf (accessed on 10 October 2015).
- Hornung, R.W.; Reed, L.D. Estimation of average concentration in the presence of nondetectable values. Appl. Occup. Environ. Hyg. 1990, 5, 46–51. [Google Scholar] [CrossRef]
- NIOSH. Criteria for a Recommended Standard: Occupational Noise Exposure. Available online: http://www.cdc.gov/niosh/docs/98-126/pdfs/98-126.pdf (accessed on 10 October 2105).
- Association, A.H. Target Heart Rates. Available online: http://www.heart.org/HEARTORG/GettingHealthy/PhysicalActivity/FitnessBasics/Target-Heart-Rates_UCM_434341_Article.jsp#.VkSRpcrgQ5g (accessed on 11 November 2015).
- Pan, W. Akaike’s information criterion in generalized estimating equations. Biometrics 2001, 57, 120–125. [Google Scholar] [CrossRef] [PubMed]
- Fox, K.; Borer, J.S.; Camm, A.J.; Danchin, N.; Ferrari, R.; Lopez Sendon, J.L.; Steg, P.G.; Tardif, J.C.; Tavazzi, L.; Tendera, M. Resting Heart Rate in Cardiovascular Disease. J. Am. Coll. Cardiol. 2007, 50, 823–830. [Google Scholar] [CrossRef] [PubMed]
- Caetano, J.; Delgado Alves, J. Heart rate and cardiovascular protection. Eur. J. Intern. Med. 2015, 26, 217–222. [Google Scholar] [CrossRef] [PubMed]
- Akormedi, M.; Asampong, E.; Fobil, J.N. Working conditions and environmental exposures among electronic waste workers in Ghana. Int. J. Occup. Environ. Health 2013, 19, 278–286. [Google Scholar] [CrossRef] [PubMed]
- Asante, K.A.; Agusa, T.; Biney, C.A.; Agyekum, W.A.; Bello, M.; Otsuka, M.; Itai, T.; Takahashi, S.; Tanabe, S. Multi-trace element levels and arsenic speciation in urine of e-waste recycling workers from Agbogbloshie, Accra in Ghana. Sci. Total Environ. 2012, 424, 63–73. [Google Scholar] [CrossRef] [PubMed]
- Asante, K.A.; Adu-Kumi, S.; Nakahiro, K.; Takahashi, S.; Isobe, T.; Sudaryanto, A.; Devanathan, G.; Clarke, E.; Ansa-Asare, O.D.; Dapaah-Siakwan, S.; et al. Human exposure to PCBs, PBDEs and HBCDs in Ghana: Temporal variation, sources of exposure and estimation of daily intakes by infants. Environ. Int. 2011, 37, 921–928. [Google Scholar] [CrossRef] [PubMed]
- Allsop, M.; Santillo, D.; Johnston, P. Environmental and Human Health Concerns in the Processing of Electrical and Electronic Waste; Report GRL-TN-04-2006; University of Exeter: Exeter, UK, 2006. [Google Scholar]
- Asante, K.A.; Takahashi, S.; Itai, T.; Isobe, T.; Devanathan, G.; Muto, M.; Agyakwah, S.K.; Adu-Kumi, S.; Subramanian, A.; Tanabe, S. Occurrence of halogenated contaminants in inland and coastal fish from Ghana: levels, dietary exposure assessment and human health implications. Ecotoxicol. Environ. Safety 2013, 94, 123–130. [Google Scholar] [CrossRef] [PubMed]
- Atiemo, S.M.; Ofosu, F.G.; Aboh, I.J.K. Assessing the heavy metals contamination of surface dust from waste electrical and electronic equipment (e-waste) recycling site in Accra, Ghana. Res. J. Env. Earth Sci. 2012, 4, 605–611. [Google Scholar]
- Gioia, R.; Eckhardt, S.; Breivik, K.; Jaward, F.M.; Prieto, A.; Nizzetto, L.; Jones, K.C. Evidence for major emissions of PCBs in the west African region. Environ. Sci. Technol. 2011, 45, 1349–1355. [Google Scholar] [CrossRef] [PubMed]
- May, J.J. Occupational hearing loss. Am. J. Ind. Med. 2000, 37, 112–120. [Google Scholar] [CrossRef]
- Cantley, L.; Galusha, D.; Cullen, M.; Dixon-Ernst, C.; Rabinowitz, P.; Neitzel, R. Association between ambient noise exposure, hearing acuity, and risk of acute occupational injury. Scand. J. Work Environ. Health 2015, 41, 75–83. [Google Scholar] [CrossRef] [PubMed]
- Kjellberg, A.; Muhr, P.; Skoldstrom, B. Fatigue after work in noise—An epidemiological survey study and three quasi—Experimental field studies. Noise Health 1998, 1, 47–55. [Google Scholar] [PubMed]
- Muzammil, M.; Khan, A.A.; Hasan, F.; Hasan, S.N. Effect of noise on human performance under variable load in a die casting industry—A case study. J. Environ. Sci. Eng. 2004, 46, 49–54. [Google Scholar] [PubMed]
- Basu, N.; Clarke, E.; Green, A.; Calys-Tagoe, B.; Man Chan, L.; Dzodzomenyo, M.; Fobil, J.; Long, R.; Quansah, R.; Neitzel, R.; et al. Integrated assessment of artisanal and small-scale gold mining in Ghana—Part 1: Human health review. Int. J. Env. Res. Public Health 2015, 12, 5143–5176. [Google Scholar] [CrossRef] [PubMed]
- Green, A.; Jones, A.D.; Sun, K.; Neitzel, R.L. The Association between noise, cortisol and heart rate in a small-scale gold mining community—A pilot study. Int. J. Environ. Res. Public Health 2015, 12, 9952–9966. [Google Scholar] [CrossRef] [PubMed]
- Kudielka, B.M.; Buske-Kirschbaum, A.; Hellhammer, D.H.; Kirschbaum, C. Differential heart rate reactivity and recovery after psychosocial stress (TSST) in healthy children, younger adults, and elderly adults: The impact of age and gender. Int. J. Behav. Med. 2004, 11, 116–121. [Google Scholar] [CrossRef] [PubMed]
- Pejtersen, J.H.; Burr, H.; Hannerz, H.; Fishta, A.; Eller, N.H. Update on work-related psychosocial factors and the development of ischemic heart disease. A systematic review. Cardiol. Rev. 2014, 23, 4–6. [Google Scholar]
- Liakios, C.; Karpanou, E.; MI, M.; Grassos, C.; Vyssoulis, G. Correlation of 24-h blood pressure and heart rate variability to renal function parameters in hypertensive patients. Eff. Smoking. J. Clin. Hypertens. 2015, 17, 938–943. [Google Scholar] [CrossRef] [PubMed]
- Linneberg, A.; Jacobsen, R.K.; Skaaby, T.; Taylor, A.E.; Fluharty, M.E.; Jeppesen, J.L.; Bjørngaard, J.H.; Åsvold, B.O.; Gabrielsen, M.E.; Campbell, A.; et al. Effect of smoking on blood pressure and resting heart rate: A mendelian randomisation meta-analysis in the CARTA consortium. Circ. Cardiovasc. Genet. 2015, 8, 832–841. [Google Scholar] [CrossRef] [PubMed]
- Vrijkotte, T.G.; van Doornen, L.J.; de Geus, E.J. Effects of work stress on ambulatory blood pressure, heart rate, and heart rate variability. Hypertension 2000, 35, 880–886. [Google Scholar] [CrossRef] [PubMed]
- Dishman, R.K.; Nakamura, Y.; Garcia, M.E.; Thompson, R.W.; Dunn, A.L.; Blair, S.N. Heart rate variability, trait anxiety, and perceived stress among physically fit men and women. Int. J. Psychophysiol. 2000, 37, 121–133. [Google Scholar] [CrossRef]
- Levine, M.E.; Crimmins, E.M. Evidence of resiliency among long-lived smokers. Vienna Yearb. Popul. Res. 2014, 11, 205–218. [Google Scholar] [CrossRef]
- Liu, Q.; Shi, S.J.; Du, L.Q.; Wang, Y.; Cao, J.; Xu, C.; Fan, F.Y.; Giesy, J.P.; Hecker, M. Environmental and health challenges of the global growth of electronic waste. Environ. Sci. Pollut. Res. Int. 2012, 19, 2460–2462. [Google Scholar] [CrossRef] [PubMed]
- Neitzel, R.L.; Daniell, W.E.; Sheppard, L.; Davies, H.W.; Seixas, N.S. Evaluation and comparison of three exposure assessment techniques. J. Occup. Environ. Hyg. 2011, 8, 310–323. [Google Scholar] [CrossRef] [PubMed]
- Sookan, T.; McKune, A.J. Heart rate variability in physically active individuals: Reliability and gender characteristics. Cardiovasc. J. Afr. 2012, 23, 67–72. [Google Scholar] [PubMed]
- Unosson, J.; Blomberg, A.; Sandström, T.; Muala, A.; Boman, C.; Nyström, R.; Westerholm, R.; Mills, N.L.; Newby, D.E.; Langrish, J.P.; et al. Exposure to wood smoke increases arterial stiffness and decreases heart rate variability in humans. Part. Fibre Toxicol. 2013. [Google Scholar] [CrossRef] [PubMed]
- Park, S.K.; O’Neill, M.S.; Vokonas, P.S.; Sparrow, D.; Wright, R.O.; Coull, B.; Nie, H.; Hu, H.; Schwartz, J. Air pollution and heart rate variability: Effect modification by chronic lead exposure. Epidemiology 2008, 19, 111–120. [Google Scholar] [CrossRef] [PubMed]
- Xhyheri, B.; Manfrini, O.; Mazzolini, M.; Pizzi, C.; Bugiardini, R. Heart rate variability today. Prog. Cardiovasc. Dis. 2012, 55, 321–331. [Google Scholar] [CrossRef] [PubMed]
- Romanowicz, M.; Schmidt, J.E.; Bostwick, J.M.; Mrazek, D.A.; Karpyak, V.M. Changes in heart rate variability associated with acute alcohol consumption: Current knowledge and implications for practice and research. Alcohol. Clin. Exp. Res. 2011, 35, 1092–1105. [Google Scholar] [CrossRef] [PubMed]
© 2016 by the authors; licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons by Attribution (CC-BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Burns, K.N.; Sun, K.; Fobil, J.N.; Neitzel, R.L. Heart Rate, Stress, and Occupational Noise Exposure among Electronic Waste Recycling Workers. Int. J. Environ. Res. Public Health 2016, 13, 140. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph13010140
Burns KN, Sun K, Fobil JN, Neitzel RL. Heart Rate, Stress, and Occupational Noise Exposure among Electronic Waste Recycling Workers. International Journal of Environmental Research and Public Health. 2016; 13(1):140. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph13010140
Chicago/Turabian StyleBurns, Katrina N., Kan Sun, Julius N. Fobil, and Richard L. Neitzel. 2016. "Heart Rate, Stress, and Occupational Noise Exposure among Electronic Waste Recycling Workers" International Journal of Environmental Research and Public Health 13, no. 1: 140. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph13010140