





Abstract
Biomarkers in chronic obstructive pulmonary disease may be useful in aiding diagnosis, defining specific phenotypes of disease, monitoring exacerbations and evaluating the effects of drugs. Exhaled breath condensate is a noninvasive means of sampling the airways, allowing biomarkers of airway inflammation and oxidative stress to be measured. In the present review, the use of exhaled breath condensate biomarkers in chronic obstructive pulmonary disease is explored and potential applications in diagnosis, disease phenotyping, exacerbation monitoring and clinical trials are considered. Exhaled breath condensate biomarkers are comprehensively reviewed in terms of method validation, reproducibility, disease specificity and sensitivity to detect changes in airway inflammation.
The commonly used exhaled breath condensate methodologies in chronic obstructive pulmonary disease patients are shown to have considerable variability, due to technical issues concerning both sample collection and analysis. Despite these issues, there is still data to support the use of exhaled breath condensate biomarkers for monitoring chronic obstructive pulmonary disease exacerbations and the response to pharmacological intervention. Further improvements to sample collection and analysis methods will improve the sensitivity of these biomarkers. The use of cytokine arrays, mass spectrometry and nuclear magnetic resonance profiling of exhaled breath condensate has opened a new avenue for analysis, as hypothesis generation from such profiling may lead to further selection of biomarkers for specific analysis.
Chronic obstructive pulmonary disease (COPD) is characterised by airway inflammation and progressive airflow limitation. Despite major advances in the symptomatic control of this disease, there is currently a lack of drugs that halt disease progression. There is a pressing need to develop drugs to modify the chronic inflammatory processes involved in this common disease and several classes of drug, with novel mechanisms of action, are now in clinical development. Validated methods are needed in order to assess short- and long-term efficacy of these new drugs.
There is currently a reliance on forced expiratory volume in one second (FEV1) to measure therapeutic effects in COPD clinical trials. While this may be appropriate for bronchodilators, the effects of anti-inflammatory drugs on pulmonary function may have a slow onset and so require long-term studies. Such studies are expensive and there may be safety issues during long-term exposure to drugs whose side-effects are not well understood. Shorter studies focusing on “proof of pharmacology” can show that the drug has the desired pharmacological action and can provide the confidence to perform larger studies. These studies need validated biomarkers in order to detect pharmacological actions. Such biomarkers should be related to the disease process, so that there is a possibility that a change in the biomarker may indicate a therapeutic benefit.
COPD is a heterogeneous disease and there is much interest in the use of biomarkers that can define specific disease subgroups with different long-term prognoses or responses to therapeutic intervention. Candidate biomarkers include sputum neutrophilia, which is predictive of decline in lung function 1 and sputum eosinophilia, which is predictive of response to corticosteroid therapy 2, 3. Other uses of biomarkers may be to aid in the diagnosis of COPD or to monitor exacerbations 4.
Exhaled breath condensate (EBC) is a noninvasive method of sampling the airways that can be repeated easily and is acceptable to patients. The use of EBC to monitor airway inflammation is based on the hypothesis that it contains aerosolised particles from the airway lining fluid (ALF). These aerosolised particles are generated from the entire respiratory tract (from mouth to alveolus) into air which is saturated with water vapour. As the expired air is cooled, this water vapour condenses around the aerosolised particles forming EBC. This process therefore traps nonvolatile substances contained within the ALF, such as proteins and water-soluble volatile substances. EBC is being increasingly used in respiratory medicine to measure biomarkers of airway inflammation and oxidative stress, and guidelines for its use have recently been published by a European Respiratory Society Task Force 5.
In the present review, the potential of EBC measurements to be used as biomarkers in COPD are reported. The ideal characteristics of a pulmonary biomarker in COPD are that it is: 1) reproducible; 2) disease specific, as it is related to the underlying pathophysiology of the disease; and 3) sensitive enough to detect changes in airway inflammation caused by exacerbations or therapeutic intervention. In this context, first the important methodological issues concerning EBC measurements in COPD that could influence reproducibility are reviewed, including: collection and storage; analytical techniques; variation of EBC biomarkers over time; and other factors affecting EBC composition, such as smoking and demographics. Secondly, a comprehensive evaluation of each current EBC biomarker is presented, focussing on potential applications in: 1) diagnosis; 2) disease stratification and phenotyping; 3) exacerbation monitoring; and 4) clinical trials of anti-inflammatory drugs. Finally, estimations of the number of subjects required in clinical trials of therapeutic interventions using EBC mediators as outcome measures are provided. Accordingly, the present review is structured in two main sections: first, methodological issues; and secondly, the use of EBC biomarkers in COPD. The review concludes with a critical summary of the existing data in COPD.
SEARCH STRATEGY
The present authors conducted a Medline search using the terms “exhaled breath condensate” or “expired breath condensate”. All references from the recent comprehensive EBC review 5 were also considered. All papers including EBC collected from subjects with COPD were included. Throughout the present review, papers from healthy subjects or patients with other respiratory diseases were used to provide supporting information, but the critical analysis of the potential of specific EBC biomarkers in COPD patients for diagnosis, phenotyping, exacerbation monitoring and in clinical trials is centred on published data from COPD patients. Papers using EBC collected from healthy subjects or subjects with respiratory diseases other than COPD were also included to provide supporting information if they contained relevant data related to methodological issues of EBC collection or analysis.
EBC COLLECTION
Collection device
Several different devices have been used to collect EBC. The commercially available EcoScreen (Jaeger, Wurzburg, Germany) and R-tubes (Respiratory Research Inc., Charlottesville, VA, USA) are commonly used, while some laboratories have used their own custom-made devices. Studies comparing collection devices have shown that there may be differences; in a mixed group of patients with asthma or allergic rhinitis and healthy volunteers, significantly higher pH levels were observed in EBC collected using EcoScreen compared to R-tubes 6. Significantly higher eotaxin and cysteinyl-leukotriene levels have also been observed using the EcoScreen compared to R-tubes 7. In contrast, studies including only healthy subjects have demonstrated no significant difference in the pH of EBC between the EcoScreen and R-tubes 7, 8 and no difference in aldehyde concentrations comparing the EcoScreen with a custom-made device 9. The possible differences between devices appear to vary with the biomarker measured and with the presence of disease.
The condenser coating used can influence the measurements obtained, due to the adhesive and electrical properties of the condensation equipment. Each EBC biomarker has specific physical and chemical properties resulting in a unique interaction with each condenser system. Rosias et al. 10 compared EBC collected using condensers with five different coatings and the EcoScreen in healthy volunteers. Use of condensers coated with silicone and glass resulted in significantly higher detection of 8-isoprostane and albumin than other coatings (Teflon, aluminium, polypropylene and EcoScreen). Measurement of nitrates (NO2-)/nitrites (NO3-) in EBC may also be affected by contamination of the sample from plastic and glass surfaces 11.
Vaughan et al. 12 observed that using the R-tube at different temperatures of collection had no effect on the pH of EBC in healthy subjects. This effect has not been investigated with the use of other devices, nor in COPD patients.
The different EBC collection devices in use have been well tolerated and found to be safe. While no formal safety studies have been performed in COPD patients, there have been no adverse effects reported in studies in which EBC has been successfully collected from patients with unstable and severe COPD 13, 14. Transmission of infection between subjects using nondisposable EBC collection systems is theoretically possible, although bacterial DNA cross-contamination was not observed in a study of EBC taken from patients with cystic fibrosis (CF) 15. Exhalation particle filters are not recommended as they may trap molecules in the expired air 5. Use of a one-way valve or disposable collection devices limits the infection risk.
Pattern of breathing
The volume of EBC obtained increases with higher minute ventilation and/or tidal volume 12, 16–18. This may simply reflect the increase in volume of air exhaled or be due to greater turbulence generating increased aerosolisation of ALF. Studies of EBC composition in COPD have not measured expiratory flow rates. However, disease severity in COPD patients affects expiratory flow rate, which may alter the concentration of biomarker. EBC hydrogen peroxide (H2O2) concentration is inversely proportional to the expiratory flow rate during collection in asthma patients and healthy subjects using resistors to generate flow rates of 140, 69 and 48 mL·s−1 17. In contrast, the pattern of breathing has no significant effect on concentrations of leukotriene (LT)B4, LTE4, prostaglandin (PG)E2 16, aldehydes 9, pH 12, 18, NO3- or total protein 18. The effect of breathing pattern is therefore dependent on the specific mediator examined. The effect of different breathing patterns on the concentration of EBC mediators should be investigated in COPD patients of different severities.
Nasal contamination
During exhaled nitric oxide (NO) measurement, nasal contamination is minimised by expiratory flow resistance, which ensures nasopharyngeal velum closure. The use of a resistor has also lead to more reproducible EBC NO3- concentrations 19. However, its use requires increased effort and does not prevent inspiratory nasal contamination. Contamination of EBC samples with nasal air is probably unavoidable in COPD patients.
The use of a nose peg opens the nasopharyngeal velum, resulting in nasal contamination of the exhaled air. In a study of pH of EBC in COPD patients and healthy subjects, similar variability between samples separated by 1 h without a nose peg, to that observed comparing collection with or without a nose peg was observed 20. This suggests that any effect of nose peg use is no greater than the natural changes in airway pH over time. The effect of nose peg use on the contribution of the nasal airway to other specific EBC constituents in COPD is largely unknown and requires further study.
Most EBC studies have used oral inhalation and exhalation during collection of EBC. One study in healthy subjects and patients with allergic rhinitis observed a significantly higher volume of EBC during oral compared with nasal inhalation, but no difference in levels of adenosine, ammonia and thromboxane (TX)B2 21.
Oral contamination
Studies comparing matched EBC samples obtained orally and from endotracheal or tracheostomy tubes found no difference in levels of pH, adenosine or TXB2 12, 21. However, higher concentrations of ammonia have been observed in EBC samples collected orally, suggesting that ammonia in EBC is mainly derived from the upper airways and oropharynx 21, 22. It has been argued that the pH of orally collected EBC is mainly driven by this high ammonia content 23. However, subsequent data has shown that the pH of EBC is not significantly affected by oral ammonia 24. Furthermore, the markedly higher variability in pH of EBC observed in COPD patients compared with healthy subjects 20 is more likely to be due to differences in airway pH between the groups than the degree of oral contamination with ammonia. Further support for the lack of contribution of mouth contamination to EBC measurements comes from the report of no relationship between the pH in saliva and EBC, in healthy subjects 12.
Oral contamination may also affect EBC NO metabolites, as nitrogen-rich meals were shown to boost levels of NO2- and NO3- in healthy subjects 25. A recent study of healthy subjects observed high levels of LTB4 in saliva. LTB4 levels were also raised in EBC samples that contained salivary amylase 26. The authors concluded that salivary contamination is a likely source of LTB4 detected in EBC. This is in contrast to previous studies, which have found salivary amylase to be undetectable in EBC samples 9, 16, 19, 27, 28. However, it has been argued that the analytical methods used may not have been sensitive enough to definitively exclude salivary contamination. The possible effect of oral contamination probably cannot be ignored if high levels of a specific mediator are present in saliva. Therefore, the contribution of oral contamination should be investigated with respect to each specific EBC mediator. In conclusion, the effects of oral contamination, pattern of breathing and the condenser device used must be standardised separately for each specific EBC mediator and in different diseases (table 1⇓).
Mediator-specific methodological issues in exhaled breath condensate collection
Concentration artefact
It can be hypothesised that any decrease in EBC solute concentration could be due to a corresponding decrease in ALF concentration or the presence of fewer aerosolised particles of ALF in the same volume of EBC (i.e. a dilutional effect). Attempts have been made to standardise EBC by using urea 29, protein 30, electrolytes 29, 31 or conductance of lyophilised samples 31. Whereas the ratio of aerosolised particles of ALF to water vapour may vary, the concentration of a dilution factor in EBC would enable calculation of the true concentration of a mediator in the ALF. However, for such calculations to be valid, the dilution factor must be of known concentration in serum, diffuse through cell membranes at a constant rate and not be produced in the airways themselves. So far, none of these methods has been validated and further research is required before such calculations can be made with accuracy. Such a dilution control factor would be particularly useful in COPD studies where between- and within-subject variability may be high, but it remains to be seen whether such methods can improve EBC reproducibility. An alternative strategy that may bypass errors caused by dilutional effects is to measure ratios between mediators. This approach has been used in induced sputum supernatant, i.e. measuring the ratio between matrix metalloproteinases and their inhibitors 32.
Storage
For practical reasons, EBC is usually frozen to be analysed later. However there are only limited reports of the effect of freezing on the composition of EBC. In analysing the pH of EBC using argon de-aeration to provide gas standardisation of the carbon dioxide (CO2) concentration in the sample, it has been shown that samples from healthy subjects frozen at -20°C for >1 yr 12 and from COPD patients at -80°C for ≤3 months 20 are stable. However, it has recently been shown that pH values obtained without gas standardisation after freezing EBC for 8 weeks were significantly higher than those obtained immediately after analysis 6. This may be due to the loss of CO2 from the sample, so the effect of freezing on other volatile substances should be investigated.
Other studies have shown no effect on 8-isoprostane 27, NO2-/NO3- 33, H2O2 34, interleukin (IL)-1β or tumour necrosis factor (TNF)-α levels 35 in EBC after freezing for periods varying from 3 weeks to 2 months. In conclusion, it is likely that freezing samples has little effect on EBC composition, with the exception of pH without gas standardisation.
EBC ANALYSIS
Gas standardisation
De-aeration of EBC samples using argon, otherwise referred to as gas standardisation, is commonly performed prior to pH measurement 12, 36, 37. This process causes a decrease in CO2 levels, which increases pH 38 and improves pH of EBC reproducibility 12. The pH has also been measured without gas standardisation, as it has been argued that the concentration of CO2 in the sample is important in itself 18, 39. However, non-de-aerated samples have unstable pH due to rapid interaction of the sample with ambient air and resulting change in CO2 concentration, making sample-analysis time crucial 40. The mean change in pH after gas standardisation is ∼1 20, 40, 41. However, whereas the effect of gas standardisation on samples with a pH >6 is predictable, it causes unpredictable pH changes in samples with pH <6 12, 40, 42. Acidic EBC samples that change little after gas standardisation may contain a low concentration of CO2, but high concentrations of other acids.
The process of gas standardisation causes an incomplete and variable reduction in CO2 levels over time 38. An alternative method to overcome this issue is CO2 standardisation by bubbling CO2 through EBC samples, which improves the reproducibility of EBC pH. Further studies are needed to assess the applicability of this method.
Immunoassays
ELISA is a common method for measuring inflammatory mediators in EBC. It is easy to perform, relatively inexpensive and studies have reported good intra-assay reproducibility 14, 43. However, despite the use of identical ELISA kits in similar patient groups, the levels of biomarkers quoted between different studies have varied considerably. For example, the mean values of LTB4 in COPD have varied 10-fold 13, 43. The specificities of the LTB4 ELISA and the 8-isoprostane radioimmunoassay have been confirmed using reverse-phase high-performance liquid chromatography (HPLC) 44, 45. However, the authors themselves conclude that further validation using mass spectrometry (MS) would provide more definitive quantitative analysis of the presence of these compounds in EBC.
It is probable that the sensitivity of the ELISA technique is inadequate for the measurement of some EBC mediators, as studies have reported individual levels below the limit of detection of the assay 13, 16. This suggests that the authors either diluted the standard below the recommended level or that they extrapolated the standard curve below the lowest concentration of standard. These are not standard practices and may lead to a loss of accuracy. The concentration of EBC samples by lyophilisation has been used by investigators prior to mediator measurement in an attempt to improve sensitivity and reproducibility 31.
Alternative analytical methods
The combination of gas chromatography (GC) or liquid chromatography (LC) and MS offer increased sensitivity for EBC analysis. However, these techniques are more complex, expensive and time consuming than ELISAs. Nevertheless, they may be valuable for validating ELISAs or enabling more accurate determination of the composition of EBC.
Using GC-MS, Cáp et al. 46 found detectable levels of LTs B4, D4 and E4 in all EBC samples from asthma patients and healthy subjects, suggesting that this technique may have improved sensitivity over ELISA. However, the use of arachidonic acid as the internal standard in the study may have lead to an overestimation of LTB4 concentrations. A subsequent study using LC-MS with LTB4 as the internal standard found detectable LTB4 levels only in steroid-naïve asthma patients, but not in healthy subjects or steroid-treated asthma 47. The detection limit of the assay was 100 pg·mL−1 (compared with ELISA which is 5 pg·mL−1), suggesting that the sensitivity of the assay needs to be improved. Furthermore, quantification of the within-subject reproducibility of these techniques has yet to be described.
LC-MS has also been used to measure aldehydes in a study of COPD patients, healthy smokers and nonsmoking controls 9. Malondialdehyde levels were increased in COPD patients compared with healthy smokers and in healthy smokers compared with healthy nonsmokers and other aldehydes were detectable in all subjects. The reproducibility of the measurements was assessed and reported as adequate, but the small sample sizes used may have made this conclusion unreliable. Adenosine has been measured in EBC from asthmatic patients and healthy subjects by HPLC 48. Levels were increased in steroid-naïve asthma patients compared to steroid-treated patients and healthy controls. The within-subject variability of this assay (limits of agreement) was shown to be 3.6 nM, with the majority of absolute measurements in patients ranging 5–35 nM, indicating that the variability was low compared with the absolute measurement obtained.
One recent study has used the technique of nuclear magnetic resonance-based metabolomic analysis to profile low molecular weight metabolites in EBC 49. Selected signals from this technique enabled more accurate differentiation between healthy children and those with asthma. This method has promise to generate hypotheses for new metabolic pathways, which may have a role in asthma, as well as identification of potential novel biomarkers.
WITHIN-SUBJECT VARIATION OVER TIME
It is important to quantify the changes in mediator concentrations observed over time (“within-subject variability”) in order to determine the natural variation of EBC composition. The reports of the within-subject variability of EBC biomarkers are outlined in table 2⇓.
Exhaled breath condensate(EBC) biomarker variability
The majority of these studies have reported variability as being “minimal”. However, there are several reasons why the variability of EBC mediators may have been underestimated. First, use of the coefficient of variation, group mean statistics or correlation coefficients may have underestimated individual variability 57. Such analyses provide information about overall group differences but not the potential for repeated samples from a single individual to vary over time. Studies using these methods to investigate variability may observe no significant change in mean group values over time, or report low coefficients of variation. However, this does not necessarily mean that the within-subject variability is low; the Bland–Altman method can show that while some individuals have highly reproducible measurements over time, considerable variation can exist in other subjects. The limits of agreement obtained by this method provide a numerical estimation expressed in the units of the measurement, of the maximum degree of variability expected within an individual during repeated sampling 57. Using a particular EBC biomarker to detect a significant biological change in an individual, such as after administration of a drug, would require a change greater than the limits of agreement. In contrast, coefficients of variation and correlation coefficients provide statistics using arbitrary values that do not relate to the units of the measurement being studied.
Several studies have investigated EBC mediator variability over time in healthy subjects. It is probable that within-subject variability in patients with disease will be higher due to changes in lung inflammation over time. Within-subject variability in healthy subjects was compared with COPD patients using the Bland–Altman method, and was demonstrated to have greater within-subject variability of pH of EBC in COPD patients over time, compared with that seen in healthy subjects 20. Bland–Altman analysis has also been used to assess within-subject variability for EBC LTB4 and H2O2 (table 2⇑). Within-subject variability of LTB4 was markedly higher in patients with disease compared with healthy subjects 51, 53, 54, similar to the findings for pH. In contrast, the within-subject variability of EBC H2O2 appears to be similar in patients and healthy subjects 27, 28, 34, suggesting that the variability of this mediator is not influenced by the development of lung disease. Further studies are required in order to confirm whether within-subject variability of other EBC mediators is higher in COPD than that observed in healthy subjects.
OTHER FACTORS INFLUENCING EBC COMPOSITION
Smoking has been found to cause an acute increase in EBC 8-isoprostane 58 and H2O2 levels 59, which may be useful biomarkers of oxidative stress in COPD. Balint et al. 60 showed that NO metabolites (NO2-/NO3-) were significantly increased 30 mins after smoking two cigarettes and had returned to baseline at 90 mins. Conversely, levels of EBC NO3- alone, s-nitrosothiols and nitrotyrosine were unchanged. Other authors have observed no difference in NO3-, IL-1β, TNF-α, total protein or aldehyde levels after smoking one cigarette 9, 35. No studies looking at the acute effects of smoking have included a placebo group, making it possible that the above observations were simply due to variation over time. However, due to the possible acute effects of cigarette smoke on certain EBC mediators, it is recommended that subjects should refrain from smoking for 3 h prior to EBC collection 5.
EBC H2O2 concentration exhibits significant diurnal variation in COPD patients 50 and in healthy subjects 59. The pH of EBC does not appear to exhibit this phenomenon in healthy subjects 12 but this has not been investigated in COPD patients. Compared with asthma, COPD is defined as having relatively low variation in airway calibre. However, the observed circadian variation in airflow 61, may affect the concentration of EBC mediators that are flow dependent. Further studies are needed in order to establish the presence of circadian rhythm of mediators in EBC from COPD patients.
In a study of healthy subjects and COPD patients it was observed that age, height and weight had no effect on EBC volume 30. However, the concentration of H2O2 in EBC increases with advancing age 59. In a large study of >400 healthy subjects, no differences in the pH of EBC were observed based on age, sex or race 62.
Carpagnano et al. 63 observed a significant increase in EBC IL-6 and TNF-α and a reduction in pH after sputum induction with hypertonic compared with isotonic saline solution. Antczak et al. 64 observed an increase in both LTB4 and 8-isoprostane levels in EBC collected following sputum induction in healthy subjects, which was not observed in asthma patients. These observations have implications for the order in which tests are performed during clinical trials, with EBC perhaps best performed before induced sputum.
USE OF EBC BIOMARKERS IN COPD
The potential of specific EBC biomarkers in COPD will now be considered systematically with respect to the following aspects. 1) Diagnosis. The ability of biomarkers to differentiate between health and disease and display specificity for COPD. 2) The ability of biomarkers to distinguish different severities and phenotypes of COPD. 3) The ability of biomarkers to monitor exacerbations of COPD. 4) The ability of biomarkers to monitor the effect of therapeutic interventions in COPD.
This part of the review uses subheadings (Diagnosis, Phenotyping, Exacerbations and Clinical trials) in order to critically and systematically appraise each of these points in turn. Where no subheading is presented, there is no published data in COPD or other patient groups concerning this area. The evidence for the potential of EBC biomarkers in COPD phenotyping, exacerbation monitoring and clinical trials is summarised in table 3⇓, while healthy controls are included in diagnosis by necessity.
Summary of the data available in chronic obstructive pulmonary disease(COPD) patients for each exhaled breath condensate (EBC) biomarker with respect to diagnosis, disease severity/phenotype, monitoring of exacerbations and therapeutic intervention
pH
Airway acidification and its regulation are thought to be implicated in the pathogenesis of obstructive lung disease 74. One potential mechanism is that protons cause the release of tachykinins, leading to bronchoconstriction and airway inflammation. Unlike other EBC mediators for which reported levels in similar subject groups may vary widely, the mean EBC pH observed in healthy subjects from different studies is similar. This “normal range” has been confirmed in a study of >400 healthy subjects where the median pH was 8.0 62. This important observation suggests that the pH of EBC is a reproducible measurement across different laboratories.
Diagnosis
Using EBC, studies have shown that patients with COPD 20, 37, acute and stable asthma 36, 75, bronchiectasis 37, chronic cough 41, CF 75 and patients on ventilators 42 have airway acidification. Figure 1⇓ summarises previous studies of EBC pH, showing marked overlap between the results obtained in different airway diseases. At first glance, this suggests that the pH of EBC is a general marker of airway inflammation rather than a disease-specific marker. However, closer inspection suggests that the pH of EBC in COPD patients exhibits certain unique characteristics. First, there is a clear differentiation between the pH “normal range” and the pH observed in COPD patients, which is not observed in other airway diseases. Secondly, a subgroup of patients with stable COPD exhibited very acidic pH, which is not observed in stable asthma. This subgroup of COPD patients may represent a specific disease phenotype and warrants further study.

Exhaled breath condensate pH, post gas standardisation, in healthy subjects and patients with disease. COPD: chronic obstructive pulmonary disease; CF: cystic fibrosis. ▴: data from 36; ▾: 37; ○: 42; •: 41; ▪: 66; □: 20; ▵: 62. Data are presented as mean for ▴, ▾, ○, ▪ and •, and median for □ and ▵.
Phenotyping
The mechanisms that contribute to airway acidity and its variability in COPD are unclear. Kostikas et al. 37 observed that EBC pH correlated with sputum neutrophilia and FEV1, although this FEV1 relationship was not confirmed in the present authors’ COPD population 20. Further investigation of the mechanisms involved in the generation and variation of acidic EBC pH, as well as the relationship between EBC pH and different COPD phenotypic characteristics, is required.
Clinical trials
An observational study in acute asthma, showing that EBC acidity improves with steroid treatment, was the first to suggest that this biomarker might be sensitive to treatment effects 36. A significant increase in the pH of EBC was also observed after 6 months’ steroid treatment in stable asthma 55. In a study of serial pH of EBC measurements in chronic cough, EBC acidification was significantly more common in those patients who subsequently responded symptomatically to proton pump inhibition, supporting the role of airway acidification in reflux-associated cough 76. However, another study showed no change in the pH of EBC after treatment with omeprazole, despite clinical improvement of reflux-associated cough 77. Studies examining the sensitivity of EBC pH to detect treatment effects in COPD are lacking.
LTB4
LTB4 is produced from arachidonic acid by 5-lipoxygenase. It is a potent neutrophil chemoattractant and therefore may have a role in the pathogenesis of COPD.
Diagnosis
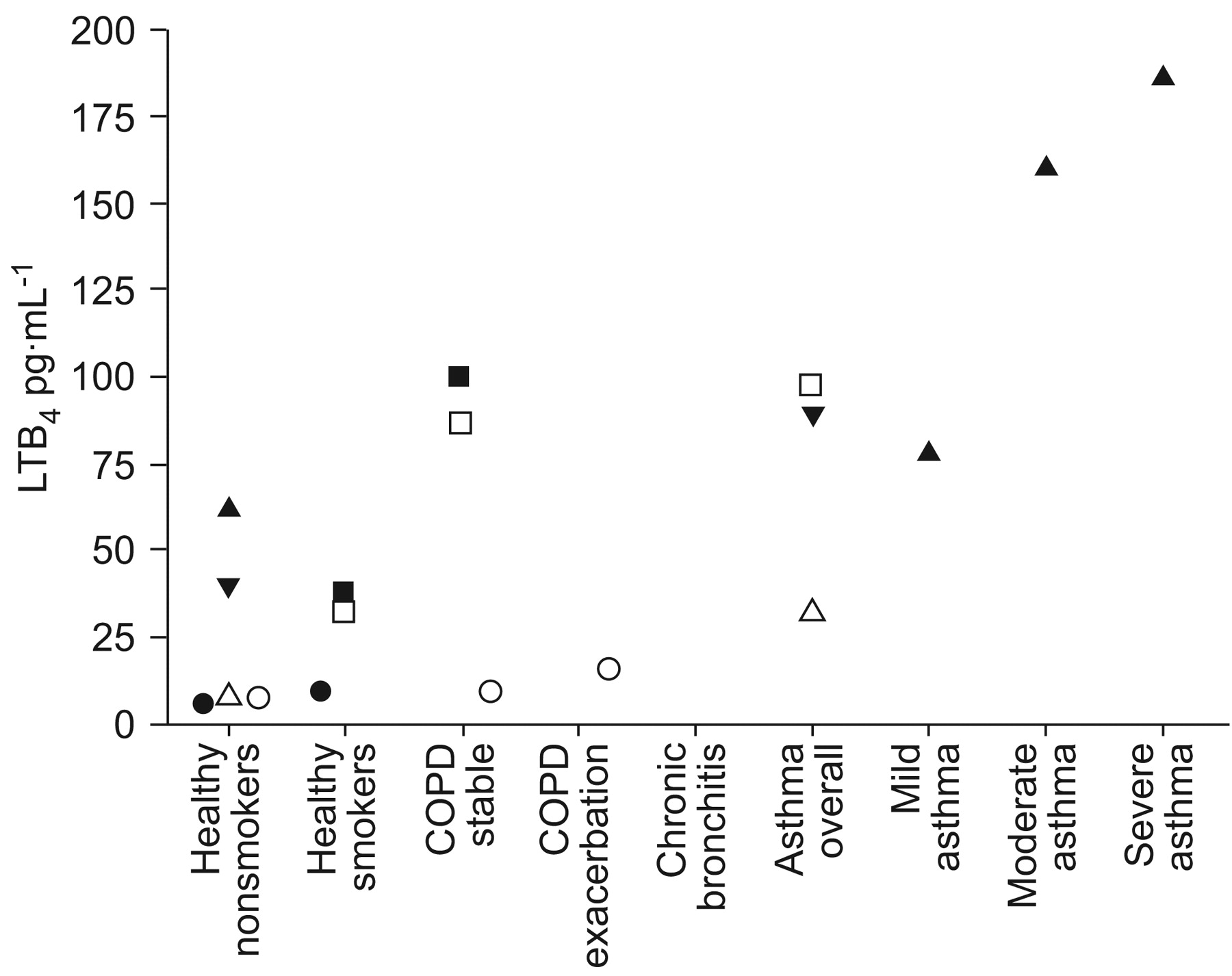
Increased levels of EBC LTB4 have been demonstrated in stable COPD patients compared with healthy smokers 43, 54, as well as in healthy smokers compared with nonsmokers 66. These studies suggest that EBC LTB4 measurements may be used to aid the diagnosis of COPD. However, a different picture emerges when the results of all studies investigating levels of EBC LTB4 in adults are viewed at the same time (fig. 2⇓). There is a wide variation in absolute levels of EBC LTB4 between studies, despite the use of the same breath condenser and ELISA kit; values in COPD patients range from 10 13 to 100 pg·mL−1 43. Furthermore, there is an overlap of EBC LTB4 levels between patients and controls, which argues against the ability of this biomarker to be used in COPD diagnosis. The potential methodological pitfalls associated with LTB4 collection and measurement, including oral contamination and lack of ELISA sensitivity, have already been reviewed. These methodological issues lead to considerable variability of LTB4 measurements in COPD patients 51 and probably contribute to the lack of reproducibility of data between laboratories.
Phenotyping
Despite the methodological issues, there are data to support the use of EBC LTB4 measurements in COPD patients, as it is correlated with sputum neutrophilia and may, therefore, be a useful biomarker of the degree of neutrophilic inflammation 54.
Exacerbations
EBC LTB4 has also been observed to increase during COPD exacerbations and fall during recovery, suggesting that this biomarker is an indicator of the inflammatory burden in the airways 13. Airway neutrophilia is known to increase during COPD exacerbations 80 and further studies are needed to confirm that LTB4 is a biomarker of neutrophilic inflammation during exacerbations.
Cinical trials
The potential of LTB4 as a biomarker in clinical trials has been explored; Montuschi et al. 65 performed a randomised placebo-controlled trial with ibuprofen in 14 patients with COPD, and a follow up open-label uncontrolled study using the COX-2 inhibitor rofecoxib in a separate group of 16 COPD patients. Whereas ibuprofen caused a significant increase in EBC LTB4 compared to placebo, rofecoxib did not, suggesting that this biomarker may sensitively differentiate between selective and nonselective COX inhibition in COPD patients. The mechanism behind this effect is not clear but may indicate that in COPD, COX-1 inhibition can divert arachidonic acid metabolism to produce LTs whereas COX-2 inhibition does not. However, placebo-controlled studies are needed in order to confirm these observations. There is also evidence from asthma trials that LTB4 can be used as a biomarker to detect drug effects, as LTB4 and cysteinyl-LTs were reduced by montelukast, which was associated with improvement in quality-of-life scores 79. These results require validation in a randomised placebo-controlled trial setting. Reduction in EBC cysteinyl-LTs has also been demonstrated following the treatment of allergic rhinitis with inhaled corticosteroids 81. No difference in EBC LTB4 levels was observed between steroid-treated and steroid-naïve COPD patients in a study by Montushci et al. 43, as the cross-sectional design of the study could not definitively exclude an effect of steroids on LTB4.
Prostaglandins
Diagnosis
EBC PGE2 is increased in stable COPD patients 43 and in smokers with asthma 56 but not in nonsmokers with asthma 16, 56. Conversely, TXB2 is increased in EBC in asthma but is not detectable in patients with COPD 16, 43. These observations suggest that the profile of EBC prostaglandins may differ in asthma and COPD.
Clinical trials
It has been shown that ibuprofen significantly reduced EBC PGE2 compared with placebo in COPD patients, whereas rofecoxib did not, suggesting that this biomarker can sensitively differentiate between selective and nonselective COX inhibition in COPD patients 65. More studies are needed in order to properly evaluate the potential of EBC PGE2 as a biomarker of drug effects. Such data should include the definition of normal range and methodological validation, including reproducibility.
Cytokines
Diagnosis
COPD is associated with the upregulation of the activity of a complex network of proinflammatory cytokines in the airways. Increased levels of EBC IL-6 and TNF-α (pro-inflammatory cytokines) and IL-10 (a regulatory cytokine), have been reported in COPD and healthy smokers, albeit at very low concentrations near or below the limit of the standard curve of the ELISA methods used 63, 66. Garey et al. 35 demonstrated higher levels of protein in EBC from smokers compared with nonsmokers, but no difference in the levels of IL-1β or TNF-α between the groups.
Phenotyping
IL-6 concentrations were found to correlate with smoking history and FEV1 in healthy smokers 66.
Exacerbations
More recently, a study using a multiplex array kit observed an increase in EBC cytokines (IL-1β, IL-6, IL-8, IL-10, IL-12p70 and TNF-α) in COPD patients with acute exacerbation compared with stable patients 67. That study suggests that EBC cytokines may be useful biomarkers of COPD exacerbations. This multiplex array technique shows promise but optimisation of sensitivity and reproducibility is required if this method is to be used with more confidence.
Clinical trials
There is evidence from asthma studies that EBC cytokine measurements (IL-4, IL-8, IL-17, TNF-α, chemokine (C-C motif) ligand 5 and transforming growth factor-β) are elevated in patients compared with controls 82 and that inhaled corticosteroids reduce EBC IL-4, but not IL-6, in asthma patients, although the lack of a placebo control means these results should be interpreted with caution. 55.
H2O2
Airway H2O2 is produced by superoxide dismutase-mediated conversion of superoxide anions. EBC H2O2 is measured by a spectrophotometric method using horseradish peroxidase.
Diagnosis
Figure 3⇓ shows that there is some differentiation between EBC H2O2 levels observed in disease and those observed in healthy subjects, as well as between healthy smokers and COPD patients 68, 69. However, overlap exists between observed levels in COPD and asthma patients, indicating that this biomarker is not disease specific.

Phenotyping
In COPD patients, correlations were observed between EBC H2O2 and FEV1, sputum neutrophils and dyspnoea score, indicating that this mediator reflects disease activity 27.
Exacerbations
In cross-sectional and longitudinal studies, increased H2O2 levels have been observed during COPD exacerbations 14, 68. There is promise for this biomarker for monitoring the burden of oxidative stress associated with exacerbations.
Clinical trials
There is evidence that EBC H2O2 can be used as a biomarker in clinical trials. In a double-blind, randomised, placebo-controlled parallel group study, the effect of N-acetylcysteine, an antioxidant mucolytic, was studied in 44 COPD patients 70. There was no change between placebo and treatment groups after 6 months, but after 9 and 12 months, the treatment group exhaled significantly less H2O2 than the placebo group. The effects of inhaled corticosteroids on EBC H2O2 is unclear, as both inhaled beclomethasone and fluticasone propionate reduced H2O2 after 4 weeks’ treatment, but there was no placebo control to compare 71, while EBC H2O2 did not change after 2 weeks’ treatment with inhaled beclomethasone compared with placebo in a cross-over study in COPD patients 72. Overall, these intervention studies suggest promise for EBC H2O2 measurements to be used to sensitively detect treatment effects in COPD, although further well-designed studies are needed to prove this.
8-Isoprostane
8-Isoprostane is formed by the free radical peroxidation of arachidonic acid and is a putatative marker of oxidative stress levels in the lungs.
Diagnosis
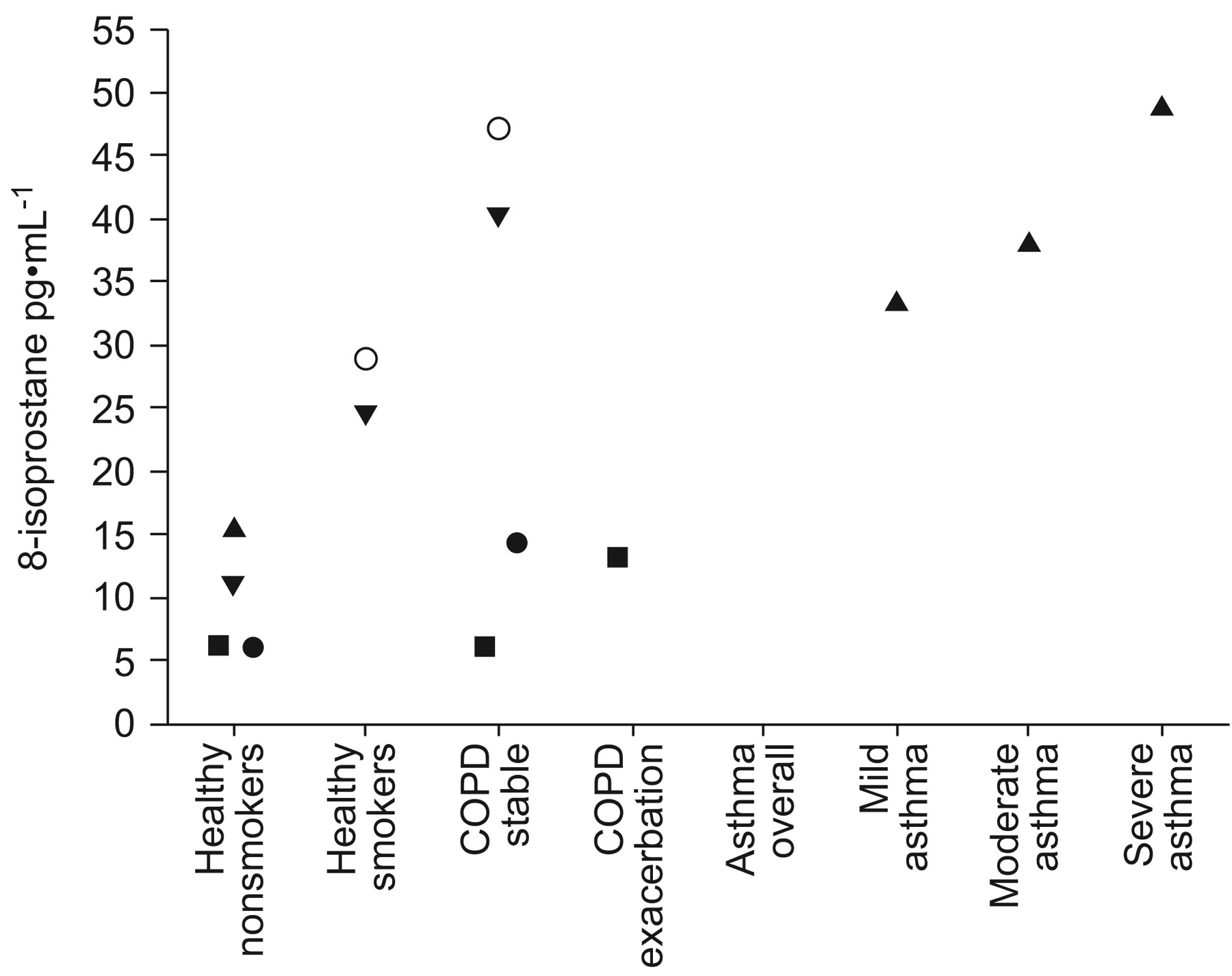
Individual studies have shown higher levels of EBC 8-isoprostane in stable COPD patients compared with healthy controls 27, 58, 84 and in healthy smokers compared with nonsmokers 58. However, mean values of 8-isoprostane in COPD patients have varied across studies ranging from 9 13 to 47 pg·mL−1 27, despite the use of identical methods (fig. 4⇓). This may be attributable to differences in condenser coatings or ELISA-sensitivity issues already discussed. Patients with asthma also have elevated EBC 8-isoprostane, indicating that it is not a disease-specific biomarker of oxidative stress 86.
Phenotyping
No correlations have been observed between 8-isoprostane and FEV1, smoking history, sputum cells or dyspnoea score in COPD studies 27, 58. However, Ko et al. 85 observed significantly higher concentrations of EBC 8-isoprostane in those with severe compared with mild-to-moderate COPD.
Exacerbations
There is evidence that EBC 8-isoprostane levels are raised during exacerbations 13.
Clinical trials
There are no published clinical trials in COPD to evaluate EBC 8-isoprostane measurements in this setting, although no reduction in this biomarker was observed when patients with asthma were treated with inhaled corticosteroids 87.
Other markers of oxidative stress
Diagnosis
Lipid peroxidation results in the production of aldehydes that can be measured in EBC by LC-tandem MS. Levels of hexanal and heptanal were increased in stable COPD compared with nonsmoking controls, and malondialdehyde was increased compared with smoking controls 9. Further studies of these EBC biomarkers are needed to address the issues of reproducibility and changes caused by exacerbations or therapeutic interventions.
Nitrogen oxides
NO is a highly reactive free radical that is stabilised ultimately as NO2- and NO3- (nitrogen oxides (NOx)) or in biological complexes with thiols to form nitrosothiols (RS-NO). In the presence of oxidative stress, the reaction between NO and superoxide anions yields peroxynitrite, which in turn leads to the formation of harmful nitrotyrosine (NT) 88. NOx are commonly measured by the Greiss reaction 89, which is a diazotisation reaction using the reagents sulphanilamide and naphthylethyllene dihydrochloride under acidic conditions (usually phosphoric acid) to detect NO2- spectophotometrically. NO3- is quantitated after enzymatic reduction to NO2- and then measured as described. Other less-commonly used assays include the fluorimetric 2,3-diaminonapthalene method 60, 90, chemiluminescence and ion chromatography 89, 91, 92.
Diagnosis
Table 4⇓ summarises the studies that have examined levels of NO2- and/or NO3- in EBC. There is inconsistency between study results in smokers with normal lung function, as both increased 35, 93 and normal 60, 73 NOx levels have been observed in smokers compared with nonsmoking controls. Higher levels of NO2- were observed in COPD patients compared with smoking and nonsmoking controls 73, whereas NO3- levels in COPD have been found to be similar 93. In asthma, higher NO2- 33, 93, total NO2-/NO3- and NO3- 93 levels have been observed.
Nitrate(NO3-) and nitrite (NO2-) levels in exhaled breath condensate
In suppurative conditions such as CF 39 and COPD 94 where mucus production can cause reduced exhaled NO levels, measuring EBC NOx may have advantages 19, 33, 39, 73 as gaseous NO is encouraged to interact with aqueous ALF giving rise to NOx 95.
Clinical trials
Exhaled NO levels have been widely used to measure inhaled corticosteroid effects in patients with asthma, and also in ex-smokers with COPD 72. Similarly, in patients with asthma, budesonide caused a significant reduction in EBC NOx levels compared with placebo 87. The potential use of EBC NOx measurements as biomarkers of drug effects needs to be further studied in COPD, perhaps in specific subgroups, such as ex-smokers.
Nitrotyrosine
Diagnosis
EBC studies have measured NT using a specific enzyme immunoassay kit with a detection limit of 3.9 ng·mL−1. Mild steroid-naïve asthmatics had significantly higher levels of NT than healthy controls but levels were reduced in those treated with ICS with moderate and severe disease 78. Although NT measurements have been performed in induced sputum of COPD patients, with increased levels compared with controls and inhibition by the xanthine oxidase inhibitor allopurinol, there have been no studies using this method in EBC from COPD patients 96.
Nitrosothiols
Diagnosis
Nitrosothiols (RS-NO) are measured using a commercially available assay (Oxonon; detection limit 0.025 μM) based on the cleavage of RS-NO to release NO, which upon rapid oxidation forms NO2- and is detected colourimetrically. Higher RS-NO levels were observed in smokers compared with nonsmokers in one study 73 but this was not confirmed in another study 60. Corradi et al. 73 also observed significantly higher levels of RS-NO in COPD ex-smokers, CF and severe asthma patients, compared with healthy nonsmokers. More studies using this measurement in COPD patients are needed in order to properly define reproducibility and the potential of this biomarker as a clinical tool, for example, in monitoring exacerbations or in clinical trials.
Power calculations
The between-subject variability can be used for power calculations to estimate the number of subjects required in clinical trials of therapeutic interventions. EBC pH, LTB4 and 8-isoprostane variability data 20, 51 were used, to estimate the number of subjects that would be required to obtain an estimated 80 or 90% power in order to detect certain effect sizes (table 5⇓). The clinically important effect size for EBC biomarkers is not known. Therefore, effect sizes were determined from the literature as described in table 6⇓.
Biomarker power calculations
Clinically important effect sizes for exhaled breath condensate biomarkers
DISCUSSION
In the present review the potential of EBC mediators to be used as biomarkers in COPD has been explored. Initially, methodological issues were considered. The present authors conclude that each potential EBC mediator must be subject to separate and meticulous method validation. Many issues regarding the collection of EBC, including pattern of breathing 9, 12, 16–18, collection device used 6–10, and the effect of oral contamination 12, 25, 26 are mediator specific. For certain EBC mediators, particularly cytokines, the ELISA method has been associated with inadequate assay sensitivity and specificity. Methods such as GC/MS may prove more successful but require further validation 44–49.
A high degree of within-subject variability has been demonstrated for many EBC mediators, which can be more pronounced in COPD patients compared with healthy subjects 20, 51, 53, 54. This is an important observation as it indicates an increased tendency for EBC composition to vary over time in COPD patients.
In terms of method validation, pH has been the most extensively studied EBC mediator. Mean pH levels are consistent in healthy subjects 64 and there is good differentiation between health and disease 20, 37. Furthermore, a subset of COPD patients exhibit a very low pH, of EBC which may be indicative of a specific COPD phenotype 20, 37. However, the pH of EBC is significantly more variable in COPD patients than in healthy subjects and the reasons for this are unknown 20. There is currently little published information regarding the identity of the acids that cause low pH values in EBC samples. Further research is warranted to explore the mechanisms generating acidic pH in the airways and to examine the sensitivity of the pH of EBC to detect exacerbation and treatment effects in COPD.
The mediators 8-isoprostane and LTB4 have been extensively reported in EBC but levels have varied considerably within the same subject groups, despite the use of identical analytical methods 13, 27, 43. This is likely to be due to methodological issues, such as condenser coatings, mouth contamination and assay sensitivity. The lack of differentiation of levels of these mediators between disease groups and healthy subjects clearly limits their use in COPD diagnosis. However, despite the methodological issues, there is some evidence supporting the role of EBC 8-isoprostane and LTB4 as markers of exacerbations in COPD patients 13 and some promising preliminary data showing the utility of EBC LTB4 as a biomarker in clinical trials 65. Improvements to the collection and analysis methods for 8-isoprostane and LTB4 may improve their potential as biomarkers in COPD.
With regard to COPD, EBC H2O2 perhaps shows the most evidence for use as a biomarker for monitoring exacerbations, as well as in clinical trials 14, 68, 70. Studies have shown relatively good reproducibility in both healthy subjects and COPD patients, if constant minute ventilation is maintained 27, 34. EBC H2O2 levels exhibit marked overlap between diseases, indicating a lack of disease specificity, again precluding its use as a diagnostic biomarker in COPD 28, 68, 69, 84. However, this lack of disease specificity may not adversely affect its potential as a biomarker of treatment response in COPD.
The use of ELISA for measuring cytokines in EBC has been hampered by assay sensitivity. The use of cytokine arrays has proved more promising, as biomarkers of COPD exacerbations can be detected 67. Further methodological optimisation of this technique is warranted.
The study of EBC biomarkers is a rapidly evolving field and the present evaluation at this point in time could easily change with new findings. It can be seen in table 3⇑ that there is much information still needed to complete the evaluation of the potential of EBC biomarkers in COPD. It should also be stressed that biomarkers showing potential for exacerbation monitoring or response to treatment intervention may be different to those useful in diagnosis or disease phenotyping.
The use of mass spectrometry or nuclear magnetic resonance profiling of exhaled breath condensate may allow hypothesis-free profiling of biomarkers, rather than a traditional hypothesis-driven approach 49. These techniques have the advantage of increased sensitivity but require complex data analysis in order to identify single mediators or patterns of mediators linked to clinical status. Hypothesis generation from such profiling may lead to more rational selection of biomarkers for specific analysis.
Statement of interest
None declared.
- Received September 4, 2007.
- Accepted February 13, 2008.
- © ERS Journals Ltd











{kind=link}
{kind=link}
{kind=link}
{kind=link}