

Abstract
Background: Patients with schizophrenia show elevated brain levels of the neuroactive tryptophan metabolite kynurenic acid (KYNA). This astrocyte-derived mediator acts as a neuroprotectant and modulates sensory gating and cognitive function. We measured the levels of KYNA in the cerebrospinal fluid (CSF) of patients with bipolar disorder and healthy volunteers to investigate the putative involvement of KYNA in bipolar disorder.
Methods: We obtained CSF by lumbar puncture from 23 healthy men and 31 euthymic men with bipolar disorder. We analyzed the samples using high-performance liquid chromatography.
Results: Patients with bipolar disorder had increased levels of KYNA in their CSF compared with healthy volunteers (1.71 nM, standard error of the mean [SEM] 0.13 v. 1.13 nM, SEM 0.09; p = 0.002. The levels of KYNA were positively correlated with age among bipolar patients but not healthy volunteers.
Limitations: The influence of ongoing drug treatment among patients cannot be ruled out. We conducted our study during the euthymic phase of the disease.
Conclusion: Brain KYNA levels are increased in euthymic men with bipolar disorder. In addition, KYNA levels increased with age in these patients. These findings indicate shared mechanisms between bipolar disorder and schizophrenia. Elevated levels of brain KYNA may provide further insight to the pathophysiology and progression of bipolar disorder.
Introduction
Bipolar disorder is characterized by recurrent episodes of mania and depression, interspersed with euthymic periods when depressive or manic symptoms are absent. Severe manic episodes often feature psychotic symptoms, such as hallucinations and delusions that may be indistinguishable from acute psychosis in schizophrenia. Cognitive impairments of executive function, attention and memory are evident in all states of bipolar disorder,1,2 and cognitive deficits are also regarded as core symptoms in schizophrenia. These and other similarities in clinical characteristics are indicative of a partially shared pathophysiology of these disorders. Indeed, several common susceptibility genes have been identified,3 and a recent population study including more than 2 million Swedish families revealed a substantial genetic association between schizophrenia and bipolar disorder.4 Despite much effort, our knowledge about the causes and underlying mechanisms of bipolar disorder and related psychiatric disorders is still unsatisfactory. Although excessive dopamine activity is proposed in the manic state,5 no biological markers have yet been identified that correspond with the disease.
Kynurenic acid (KYNA) is a tryptophan metabolite of the kynurenine pathway that acts as an endogenous antagonist on both the glycine site of the N-methyl-D-aspartate6,7 receptor and on the nicotinergic α7* acetylcholine receptor.8 The compound is synthesized in and released by astrocytes in the brain.9,10 Elevated levels of KYNA have previously been observed in patients with schizophrenia, both in the cerebrospinal fluid (CSF)11,12 and postmortem prefrontal cortex.13 Interestingly, KYNA tonically modulates midbrain dopamine activity,14–20 indicating a potential role of this compound in dopamine-related diseases.21
Our objective was to test the hypothesis that KYNA plays a role in the pathophysiology of bipolar disorder, by analyzing the concentration of KYNA in the CSF of patients with bipolar disorder and controls.
Methods
Participants
We recruited patients from December 2005 to April 2008 from a long-term follow-up program at a bipolar outpatient unit at the Northern Stockholm psychiatric clinic, Stockholm, Sweden. Consecutive new outpatients referred for treatment and continuing patients at the bipolar outpatient unit were invited to participate, provided that they were at least 18 years old and met the DSM-IV criteria for bipolar disorder type I or II.
A complete account of the clinical investigation procedure has been previously published.22 Briefly, the clinical diagnosis of bipolar disorder was established according to the Affective Disorder Evaluation,22 which was previously used in the STEP-BD project.23 With the permission of its originator Gary S. Sachs, the ADE was translated and modified to suit Swedish conditions. To minimize interrater variability, the collected information was presented at a diagnostic case–conference, and a consensus panel of experienced board-certified psychiatrists who specialize in bipolar disorder made the final diagnostic decision at this conference.
We collected CSF samples when the patients were symptom free and in a stable euthymic mood, as judged by a physician. For ethical reasons, the patients continued to take their prescribed medication.
We recruited 36 healthy male volunteers from among medical students, hospital staff members and their relatives. They all underwent a medical check-up including laboratory tests (electrolytes, blood, thyroid, kidney and liver) and a physical examination. The volunteers had to have been free of medication for at least 1 month and free from any form of substance abuse. We included those who smoked or consumed coffee.
The volunteers underwent a semistructured interview using the Structured Clinical Interview for DSM-IV Axis I disorders (SCID-I).24 The interview was directed toward affective disorders, anxiety disorders and drug abuse. The volunteers also completed the SCID-II questionnaire for personality disorders.25 We considered 30 healthy volunteers to be eligible for inclusion in the study with respect to the clinical interview and SCID results. All were considered healthy by the psychiatrist performing the examinations and showed no signs of psychiatric or somatic illness or had any laboratory test results outside of the standardized reference ranges. None of the volunteers had a family history of major psychosis or suicide in first- or second-degree relatives.
This study was carried out in accordance with the Declaration of Helsinki for experiments involving humans. All patients and healthy volunteers received verbal and written information and gave their written informed consent. Patients were excluded if they were unable to complete the standard clinical assessment or were incapable of providing informed consent. The study was approved by the Ethical Committees of the University Hospital in Linköping, the Karolinska Institutet and the Medical Faculty of Uppsala University, Sweden.
Analysis of KYNA
We drew CSF from the L4–L5 interspace between 9 and 11 am after a night of fasting and bed rest. In total, 12 mL CSF was collected, inverted to avoid gradient effects, divided into aliquots and frozen at −870°C until assayed. Data from a subset of the control samples have previously been published.12
We performed the analysis of KYNA using an isocratic reversed-phase high-performance liquid chromatography (HPLC) system, including a dual-piston, high-liquid delivery pump (Bischoff Chromatography), a ReproSil-Pur C18 column (4 × 150 mm, Dr. Maisch GmbH ) and a fluorescence detector (Jasco Ltd.) with an excitation wavelength of 344 nm and an emission wavelength of 398 nm (18 nm bandwidth), essentially as previously described.26 A mobile phase of 50 mM sodium acetate (pH 6.2, adjusted with acetic acid) and 7.0% acetonitrile was pumped through the reversed-phase column at a flow rate of 0.5 mL/min. Samples of 50 μL were manually injected (Ecom). Zinc acetate (0.5 M not pH adjusted) was delivered after the column by a peristaltic pump (P-500; Pharmacia) at a flow rate of 0.10 mL/min. Signals from the fluorescence detector were transferred to a computer for analysis with Datalys Azur (version 4.6.0.0; http://datalys.net). The retention time of KYNA was about 7–8 minutes. Initially, the sensitivity of the system was verified by analysis of a standard mixture of KYNA with concentrations from 0.5 to 30 nM, which resulted in a linear standard plot. To verify the reliability of this method, some samples were analyzed in duplicate, and the mean intraindividual variation was below 5%.
Statistical analysis
The KYNA values are given as mean and standard errors of the mean (SEM). Differences in the levels of KYNA were established using the Mann–Whitney U test. We performed linear regression analysis using the least squares method to study the relation between KYNA level and age. We tested for a normal distribution of residuals with the Anderson–Darling test for each of the groups and none of the groups deviated from normality (p > 0.25). We assumed significance for all values with p < 0.05.
Results
We included 31 men with bipolar disorder and 23 healthy male volunteers. The mean age of the men with bipolar disorder was 36.3 (standard deviation [SD] 9.2, range 20–52 yr), and the mean age of the healthy men was 33.1 (SD 6.9, range 24–51 yr). Of the included men, 18 met the DSM-IV criteria for bipolar disorder type I (mean age 37.3, SD 10.5 yr) and 13 met the criteria for type II (mean age 34.8, SD 7.1 yr). Because there were a limited number of female healthy volunteers, we did not include female patients in this study.
All but 2 patients with bipolar disorder were taking medication at the time of sampling. The most commonly used treatments were as follows: lithium (n = 21), lamotrigine (n = 7), quetiapine (n = 5), mirtazapine (n = 4), propiomazine (n = 4) and valproate (n = 3). Some of these patients were taking more than one drug: lithium and lamotrigine (n = 5) lithium and propiomazine (n = 3), lithium and mirtazapine (n = 2), lithium, lamotrigine and quetiapine (n = 2), lamotrigine and valproate (n = 1), valproate and quetiapine (n = 1), valproate and mirtazapine (n = 1), lamotrigine and propiomazine (n = 1), lithium, lamotrigine and mirtazapine (n = 1) and lithium, quetiapine and propiomazine (n = 1).
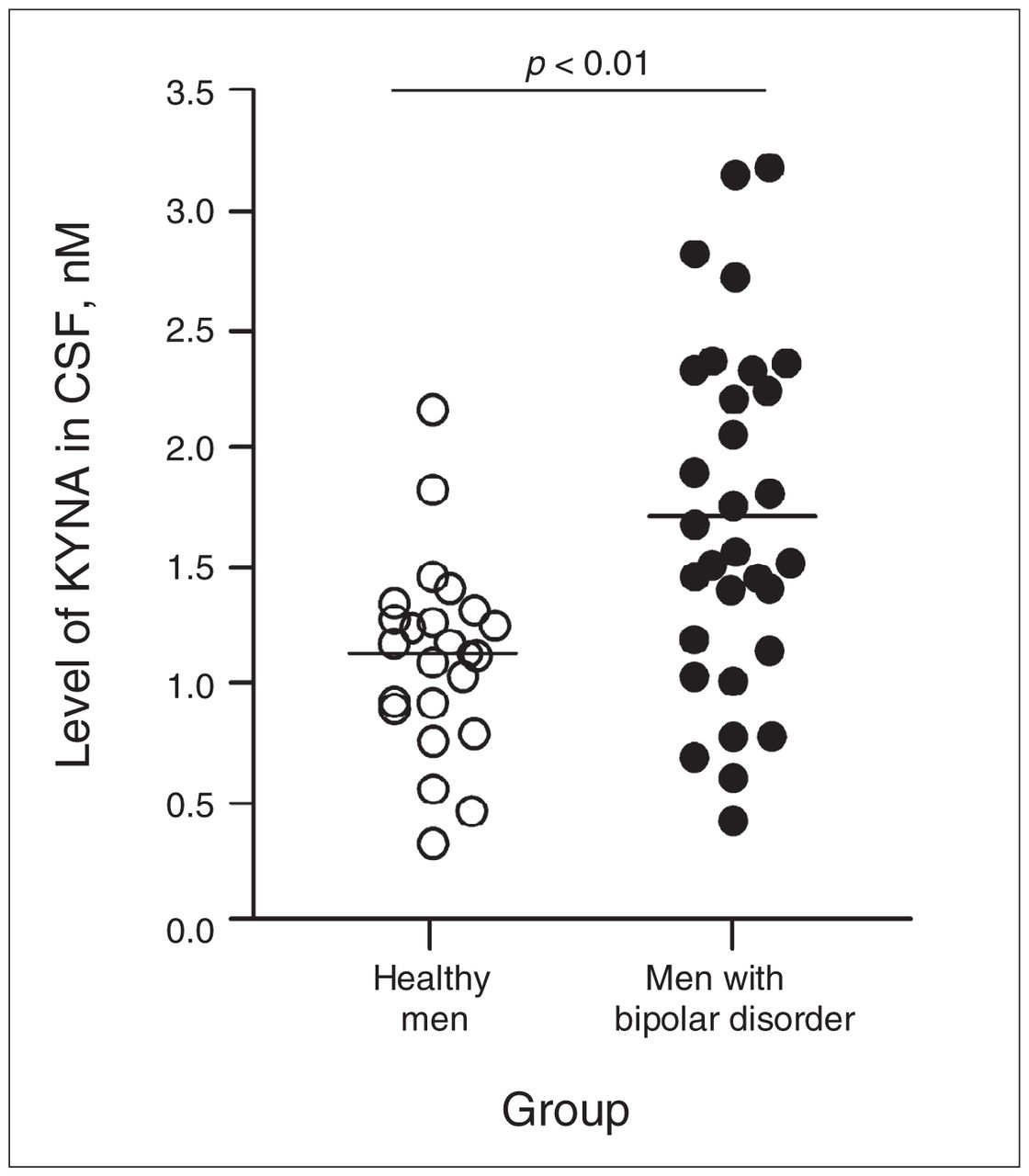
The KYNA levels in the CSF of patients with bipolar disorder were significantly higher (1.71 nM, SEM 0.13 nM, range 0.45–3.19 nM, n = 31) than in the healthy volunteers (1.13 nM, SEM 0.09 nM, range 0.34–2.17 nM, n = 23, U = 181, p = 0.002, Fig. 1). There was no difference in KYNA levels between patients with bipolar disorder I and II (type I: 1.77 nM, SEM 0.17 nM, n = 18; type II: 1.63 nM, SEM 0.21 nM, n = 13). The level of KYNA was significantly correlated with age in patients (r = 0.49, p = 0.005, y = 0.0397x + 0.274) but not in healthy volunteers (r = 0.23, p = 0.29, y = 0.0135x + 0.686; Fig. 2).
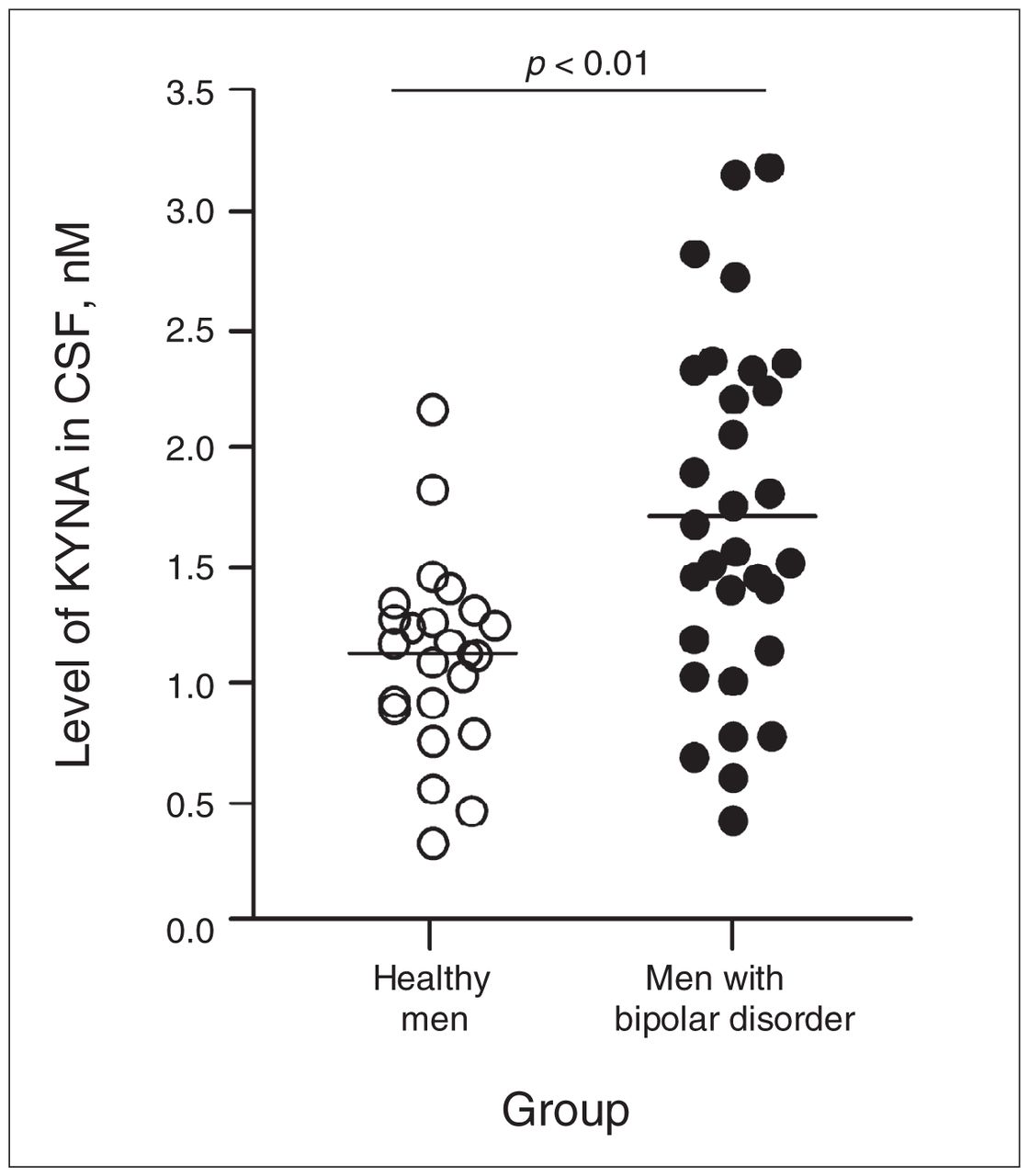
Kynurenic acid (KYNA) in the cerebrospinal fluid (CSF) of healthy men and men with bipolar disorder. Each point represents the concentration of KYNA in a single CSF sample. The mean of each group is indicated by the line. Mann–Whitney U test, U = 181.
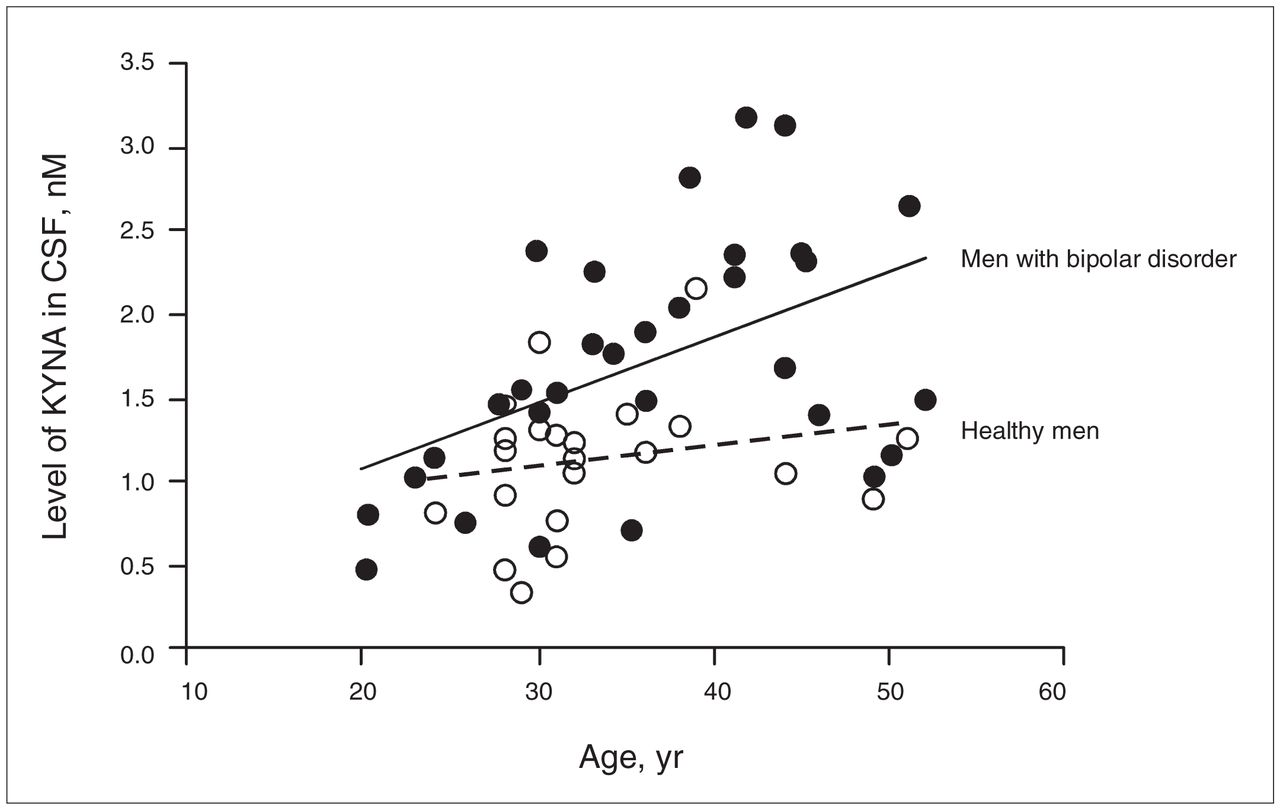
Linear regression analysis of the amount of kynurenic acid (KYNA) in the cerebrospinal fluid (CSF) and age of healthy men (open circles) and in men with bipolar disorder (closed circles). A significant correlation between KYNA and age was observed in male patients with bipolar disorder (r = 0.49, p = 0.005, y = 0.0397x + 0.274).
Discussion
We found that KYNA levels in the CSF were higher in euthymic men with bipolar disorder than in healthy men. Furthermore, KYNA levels were positively correlated with age in the patient group. These results are similar to our previous studies, in which we found increased levels of KYNA in the CSF of patients with schizophrenia.11,12 In the present study, there was no correlation between age and KYNA level in healthy men. An age-related increase in KYNA concentration has previously been reported in rats27,28 but not in healthy volunteers.11,12,29–31 Because our samples were limited by a rather narrow age range (20–52 yr), we cannot ruled out that brain KYNA may increase with age in older healthy individuals.
Kynurenic acid is an astrocyte-derived antagonist that inhibits brain glutamatergic and cholinergic transmission. The functional significance of the observed elevation in brain KYNA levels (about 50%) is unclear. Notably though, experimental studies reported that elevations of KYNA in the rat brain, within the same order of magnitude, are associated with a marked activation of the firing of midbrain dopamine neurons.14–20 Thus, the elevation of brain KYNA in bipolar disorder likely functionally influences glutamatergic, cholinergic and dopaminergic neurotransmission in these patients.
Limitations
A major limitation of our study is that most of the patients were taking psychotropic drugs during CSF sampling. However, several animal studies have shown that some of the drugs used by the patients, such as valproate and lamotrigine, do not affect brain KYNA concentration when administered to animals at clinically relevant concentrations.32 Further, chronic treatment with antipsychotic drugs reduces brain KYNA levels in rats,33 a finding also supported by postmortem findings in patients with schizophrenia,34 thus arguing against an influence of these drugs on the present results. Although we did not perform a complete correlation analysis between KYNA levels and medication status, KYNA levels did not differ between patients taking antipsychotic drugs or lithium as compared with the rest of the group (data not shown). The observation that KYNA in CSF increases with age, despite similar medication doses given to all patients regardless of age, further argues against any direct influence of ongoing medication. Taken together, the observed elevation of KYNA in the CSF of bipolar patients is more likely the result of underlying processes that might be linked to the progression of the disease. Our findings are in agreement with those of a postmortem study of patients with bipolar disorder showing increased levels of brain kynurenine, the immediate precursor of KYNA, and increased expression of the tryptophan-degrading enzyme tryptophan 2,3-dioxygenase (TDO2).34
The observed elevation of KYNA levels in the CSF of bipolar patients is important in light of the fact that cognitive dysfunctions are present in all states of the disease, including the euthymic state. Furthermore, these dysfunctions are known to progress with the course and severity of the disease.35–37 Numerous studies have shown an intimate relation between cognitive function and glutamatergic and cholinergic neurotransmission.38,39 Indeed, a large body of studies has demonstrated that KYNA is involved in the modulation of behaviour and cognition. Thus, in rodents, pharmacologically increased levels of KYNA have been found to disrupt prepulse inhibition,40 a feature also observed in patients with bipolar disorder during both acute psychotic mania41 and euthymia,42 as well as in patients with schizophrenia.43 Furthermore, pharmacologically elevated KYNA levels impair contextual learning and working memory in rats.44,45 Accordingly, kynurenine aminotransferase II knockout mice, which have low levels of endogenous KYNA, show increased performance in passive avoidance T-maze tests.46,47 Taken together, these findings suggest that KYNA might causally contribute to the development of the decline in cognitive function during the progression of bipolar disorder.
Conclusion
Men with bipolar disorder have increased levels of KYNA in their CSF compared with healthy men. Because experimental studies have described the important role of KYNA in learning and memory,21 KYNA may be involved in the mechanisms leading to cognitive deficits in bipolar disorder.
Acknowledgements
We dedicate this article to the memory of our dear friend Conny Nordin, who died July 5, 2008. We thank the health professionals who facilitated this study. In particular, we thank study coordinator Mrs. Martina Wennberg and research nurses Mrs. Agneta Carswärd-Kjellin, Mrs. Stina Stadler, Mrs. Hazel Holmberg-Forsyth and Mrs. Margareta Krona. We also thank Dr. Christian Johansson.
Footnotes
Competing interests: None declared.
Contributors: Drs. Engberg, Erhardt, Nordin and Landén designed the study. Drs. Samuelsson, Lindström, Jönsson, Nordin and Landén acquired the data, which Drs. Saetre, Erhardt, Nordin and Landén and Ms. Olsson analyzed. Drs. Saetre, Engberg, Erhardt, Nordin and Landén and Ms. Olsson wrote the article. All authors reviewed the article and approved its publication.
Funding: Financial support for this study was provided through the regional agreement on medical training and clinical research between Stockholm County Council and the Karolinska Institutet, and through grants from the Hållstens Forskningsstiftelse, Swedish Brain Foundation, the Östergötland County Council, Svenska Läkaresällskapet, Karolinska Institutet, Torsten och Ragnar Söderbergs stiftelse and the Swedish Research Council (no. 2009-4046 to S.E., 2008-3822 and 2009-3068 to G.E., K2008-62x-14647-06-3 to M.L., and 2006-986 and 2006-2992 to E.G.J.). No funding sources had any role in study design, in the collection, analysis and interpretation of data, in the writing of the report, or in the decision to submit the paper for publication.
- Received December 10, 2009.
- Revision received February 2, 2010.
- Accepted February 2, 2010.
References
In this issue

{kind=link}
{kind=link}
Article tools






Related Articles
Cited By...
- The steroid hormone ADIOL promotes learning by reducing neural kynurenic acid levels
- Quantitative Translational Analysis of Brain Kynurenic Acid Modulation via Irreversible Kynurenine Aminotransferase II Inhibition
- Acute intermittent porphyria: comorbidity and shared familial risks with schizophrenia and bipolar disorder in Sweden