


See related practice article by Dubé at www.cmaj.ca/lookup/doi/10.1503/cmaj.080505.
A previously well 54-year-old woman was admitted to hospital for investigation of bilateral pain in her legs that prevented her from walking. She had a three-week history of pain, which started in the knees and progressed to involve the muscles of her lower limbs diffusely. This pain was associated with mild swelling and bruising. She also noted red dots on her legs. Review of systems was positive for a progressive history of fatigue and a 5-lb weight loss over two years.
The patient’s medical history included osteoarthritis and osteoporosis. Her medications were alendronate, calcium, vitamin D and acetaminophen. The patient reported allergies to sulfa, penicillin, codeine and nuts. She was a non-smoker, was employed in a full-time job and denied any social or financial stressors.
On presentation, the patient was mildly tachycardic (heart rate 103 beats/min) with a blood pressure reading of 100/67 mm Hg, but she was otherwise stable. Positive findings included small knee effusions and mild bilateral pitting edema of the lower limbs. Muscles of the lower limbs were very tender to palpation. Nonpalpable petechiae were present on the legs (Figure 1), and extensive ecchymosis could be seen on the posterior thighs and calves (Figure 2).

Leg of a 54-year-old woman with bilateral pain in her lower limbs and a diagnosis of scurvy showing purpuric lesions, petechial in appearance. We were unable to note the perifollicular nature of the lesions because the patient had recently shaved. A small-vessel vasculitis could have a similar appearance.

Posterior aspect of thighs and calves of the patient, 48 hours after vitamin C therapy was started, showing ecchymosis in various stages of resorption.
In hospital, progressive normocytic anemia was noted, with a drop in hemoglobin level from 96 g/L to 73 g/L (normal 115–155 g/L) over 72 hours. The reticulocyte count was elevated. The leukocyte count was 9.3 (normal 3.0–10.5) 109/L, with a normal differential. Platelets were slightly elevated at 498 (normal 125–400) 109/L. The erythrocyte sedimentation rate was mildly elevated, and the ferritin level was normal at 312 (normal 24–336) μg/L. Total bilirubin was 75 (normal 24–336) μmol/L, and all other liver enzymes were normal. Haptoglobin, international normalized ratio, creatinine, thyroid-stimulating hormone, creatine kinase, folate and vitamin B12 levels were normal, as was the partial thromboplastin time. Workup for infection, including serology for hepatitis B and C, was negative.
A chest radiograph was normal, as was a computed tomographic scan of the abdomen and pelvis. Further investigations included a normal electromyogram. A skin biopsy of the petechiae showed noninflammatory dermal hemorrhages.
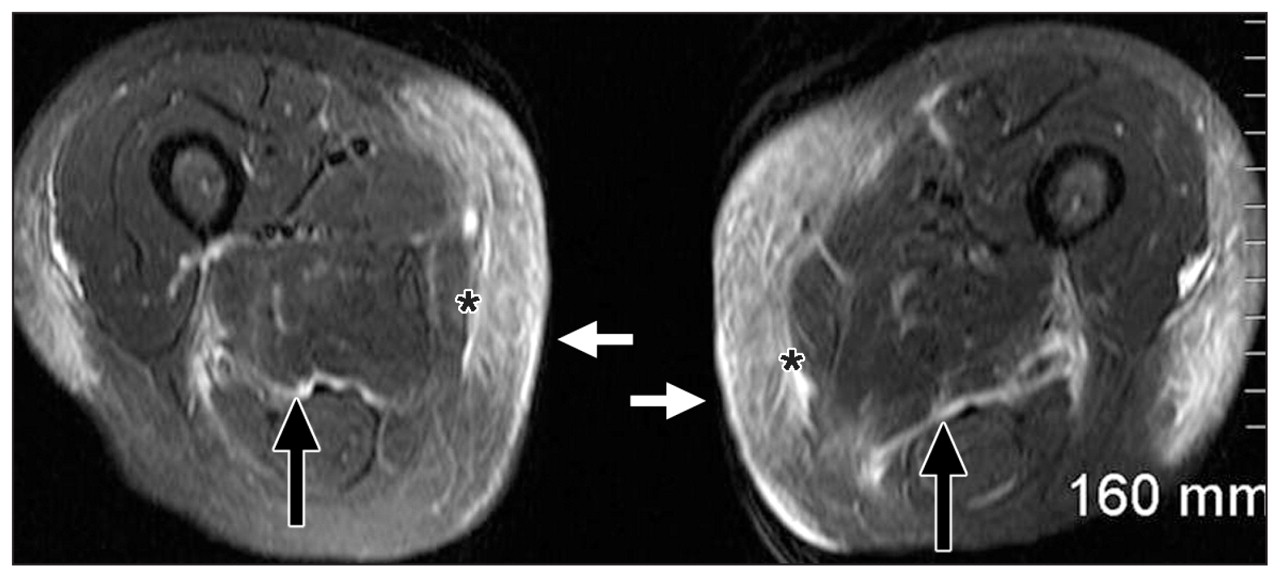
Subcutaneous edema was seen on a plain film of the femur. Magnetic resonance imaging (MRI) of the lower extremities showed mild peripheral increase in T2-weighted muscle signal in the distal vastus medialis and lateralis with more prominent bilateral dermal thickening, subcutaneous edema and deep fascial edema (Figure 3; Appendix 1, available at www.cmaj.ca/lookup/suppl/doi:10.1503/cmaj.091938/-/DC1). Similar findings were seen in the gastrocnemius muscles bilaterally (Appendix 2, available at www.cmaj.ca/lookup/suppl/doi:10.1503/cmaj.091938/-/DC1) and also in the calves with prominent subcutaneous and deep fascial edema. The medial gastrocnemius muscles also showed fatty infiltration but no atrophy. Focal enhancing marrow lesions in the right femur were felt to represent islands of red marrow.
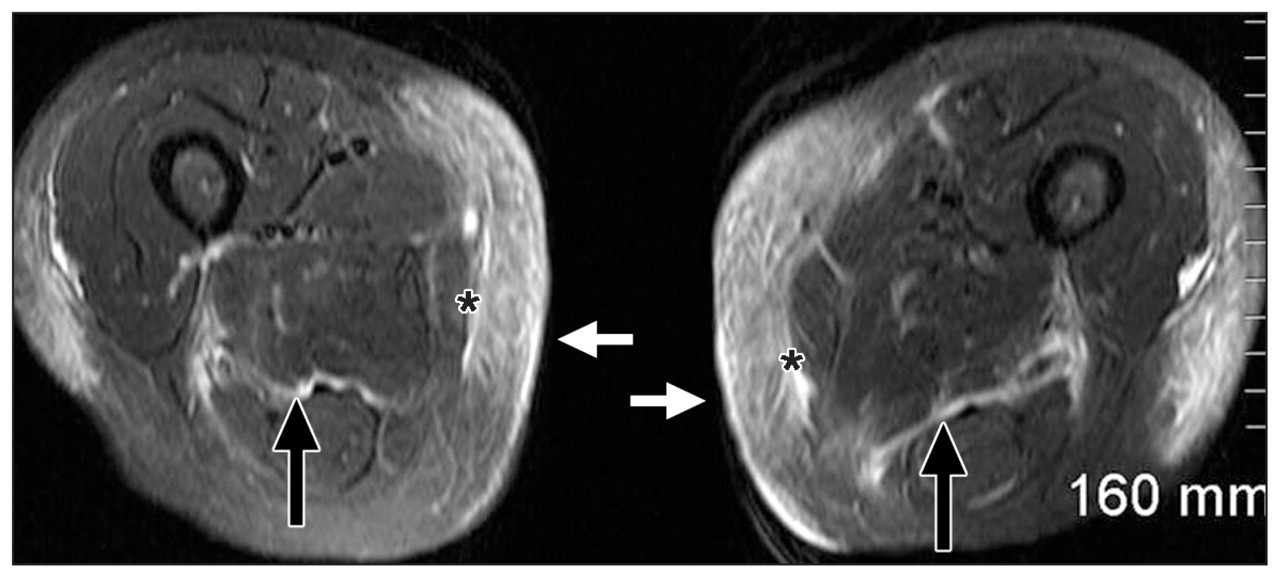
Axial T2-weighted fat-saturated magnetic resonance images of the thighs showing dermal thickening and subcutaneous edema (white arrows) with fascial edema underneath (asterisks) and deep fascial edema (black arrows).
Enhanced images did not show areas of muscle necrosis or fluid collections to suggest abscess. The findings of MRI were nonspecific and reported to be in keeping with an inflammatory process.
On further questioning, it became apparent that the patient had been restricting all fruits and most vegetables in an escalating fashion over the past two years because of a perceived allergy. Based on this information, the patient’s vitamin C level was tested, and she was given oral ascorbic acid, 100 mg orally three times per day. Her condition improved substantially within 48 hours. Subsequently, her vitamin C level was reported to be less than 10 (normal > 25) μmol/L, which confirmed the diagnosis of scurvy.
Discussion
Scurvy is a disease caused by vitamin C deficiency. Vitamin C, also known as ascorbic acid, is necessary in hydroxylation reactions, including procollagen production.
At one time, this disease was common among sailors, soldiers and others without access to fresh fruits and vegetables. The Scottish naval surgeon Sir James Lind first described the effective treatment of scurvy with citrus fruits in A Treatise of the Scurvy in 1753.1 With increased awareness for the necessity of fresh fruits and vegetables in one’s diet, the rate of scurvy declined through the 18th century.
It has generally been thought that scurvy is an uncommon disease in developed nations. However, a 2008 study found that 25% of men and 16% of women from low-income populations in the United Kingdom were deficient in vitamin C (< 11 μmol/L).2 A similar study completed in the United States in 2003/04 found that 7.1% of healthy middle-class participants were vitamin C deficient (< 11.4 μmol/L) and 13.7% were deplete (< 28 μmol/L).3 Thus, it is clear that even in industrialized populations with access to fresh food, vitamin C deficiency is present. Those who are elderly, alcoholics, smokers, mentally ill, and those with low socioeconomic status or restricted diets are particularly at risk for vitamin C deficiency.4,5
Clinical findings
Patients typically develop clinical findings one to three months after starting a diet void of ascorbic acid. Concentrations below 20 μmol/L may be associated with nonspecific symptoms, such as fatigue, loss of appetite and irritability. Serum concentrations of less than 11.4 μmol/L are considered to indicate substantial vitamin C deficiency.3
Musculoskeletal findings include joint pain, typically of the knees, ankles and wrists; as well as muscle pain and hemarthrosis.6 Skin findings can include petechia centred around hair follicles, corkscrew hairs, ecchymosis and hematomas. As in our patient, these changes typically occur first in the legs and buttocks, because these are regions of elevated hydrostatic pressures.
Oral manifestations are inconsistent, but can include hypertrophy and bleeding of gums.7 Teeth are required for these oral changes because the inflammation occurs in the supporting tissues of the teeth. It is presumed that teeth provide portals of entry for microbes into the gingiva.8
Anemia
A common laboratory finding in patients with deficiency in vitamin C is anemia. Vitamin C deficiency can present as an iron-deficiency anemia. It can also present with a normochromic–normocytic pattern.8 Most often the anemia can be attributed to acute blood loss resulting from defects in collagen synthesis. Blood loss can occur from the gastrointestinal tract, joints, muscles and many soft tissue sites. Intravascular hemolysis has also been reported, presumably due to a decreased life span of red cells.8
Vitamin C is important in the absorption and metabolism of many nutrients that affect production of red blood cells. For example, vitamin C aids in the conversion of iron from the ferric to ferrous form, which is required for iron absorption from the gastrointestinal tract. Scurvy can also be associated with folate deficiency. Vitamin C augments the effect of folate in production of red blood cells, and foods rich in vitamin C are often the same foods rich in folic acid.9
Imaging
There are few reports of MRI findings associated with scurvy. Because of our patient’s musculoskeletal complaints, MRI of the lower extremities was performed. In a previous case report of a 56-year-old man with scurvy, MRI of the leg showed multiple small areas of focal marrow edema.10 These T1-weighted images were noted to be in the distal metaphyseal region of the femur and proximal tibia, similar in location to our patient’s signal changes of the femur and tibia. These findings could represent areas of hemorrhage, infarct or islands of red marrow, all of which are nonspecific findings of scurvy on MRI.10 In another report, a 68-year-old woman was admitted to hospital with a similar presentation of progressive lower-extremity pain preventing ambulation.7 She was initially diagnosed with cellulitis and underwent an MRI to exlude myositis or osteomyelitis. The imaging showed nonspecific bone marrow edema and osteoporosis. As in our patient, the ultimate diagnosis of scurvy was made through further questioning and clinical examination; however, the MRI helped to rule out other diagnoses. A third case report of a five-year-old child noted diffuse marrow signal changes and subperiosteal fluid.11 This case also reported enhancement on T1-weighted images and abnormal signal on T2-weighted images of surrounding thigh muscles, particularly of the vastus medialis, which was seen in the imaging of our patient. Initially the subperiosteal changes were thought to represent osteomyelitis, but further investigation confirmed chronic inflammation and hemorrhage, in keeping with scurvy.
On review, our patient’s subcutaneous and deep muscle edema, and fluid and fatty infiltration were felt to be secondary to subcutaneous and fascial hemorrhages. These findings are consistent with the conclusion that the patient’s normocytic anemia was due to acute blood loss.
Diagnosis
The diagnosis of scurvy is made clinically, with evidence of inadequate intake of vitamin C based on a thorough dietary history and characteristic physical findings. Although a decreased ascorbic acid level can be used as an indicator for scurvy, it is not a sensitive test and can be normal in a patient with vitamin C deficiency. Other laboratory results, such as evidence of anemia, provide support for the diagnosis. Findings on imaging are nonspecific and will not lead to the diagnosis, but may serve to rule out other potential etiologies, particularly in those who present with musculoskeletal complaints. A practical clinical indicator for scurvy is a rapid response to oral vitamin C.9
Treatment
If vitamin C deficiency is suspected based on a history of poor nutrition or physical examination, oral vitamin C should be started immediately. Symptoms of scurvy have improved with varying doses of ascorbic acid, and one review found as little as 6.5 mg daily improved symptoms.8 However, expert opinion recommends oral supplementation of 300 mg daily in divided doses of ascorbic acid for at least one month or until body stores are replenished, indicated by serum levels.9 Patients’ subjective complaints can improve within 24 hours of starting treatment.8 As with our patient, objective findings, such as ecchymosis resorption, can begin to improve within only 48 hours of treatment. After serum levels are replenished, patients should ensure they are meeting the estimated daily requirement of vitamin C. In US recommendations, the estimated average requirement for women is 60 mg/d for nonsmokers and 95 mg/d for smokers (75 mg/d and 110 mg/d, respectively, in male populations).3 The recommended dietary allowance for vitamin C in Canada is 75 mg/d in women and 90 mg/d in men; the daily allowance varies with age and sex, and in pregnancy or breastfeeding.12
Key points-
Scurvy exists in the developed world and remains a clinical diagnosis, based on a thorough dietary history and characteristic physical findings.
-
Patients may present with nonspecific complaints such as fatigue, loss of appetite and pain in the joints or muscles.
-
Scurvy can result in catastrophic illness, and empiric oral treatment with vitamin C should be started when scurvy is suspected.
-
Treatment with vitamin C leads to prompt resolution of symptoms within days.
The section Cases presents brief case reports that convey clear, practical lessons. Preference is given to common presentations of important rare conditions, and important unusual presentations of common problems. Articles start with a case presentation (500 words maximum), and a discussion of the underlying condition follows (1000 words maximum). Generally, up to five references are permitted and visual elements (e.g., tables of the differential diagnosis, clinical features or diagnostic approach) are encouraged. Written consent from patients for publication of their story is a necessity and should accompany submissions. See information for authors at www.cmaj.ca.
Footnotes
-
Competing interests: None declared.
-
This article has been peer reviewed.
-
Contributors: Alexa Smith drafted the manuscript, which Gina Di Primio and Susan Humphrey-Murto revised. All authors approved the final version submitted for publication.
In this issue

{kind=link}
{kind=link}
{kind=link}
Article tools






Jump to section
Related Articles
Cited By...
More in this TOC Section
Similar Articles
Collections

