Abstracts
OBJECTIVE:
To describe the prevalence of anemia and of its types in hospitalized patients with pulmonary tuberculosis.
METHODS:
This was a descriptive, longitudinal study involving pulmonary tuberculosis inpatients at one of two tuberculosis referral hospitals in the city of Rio de Janeiro, Brazil. We evaluated body mass index (BMI), triceps skinfold thickness (TST), arm muscle area (AMA), ESR, mean corpuscular volume, and red blood cell distribution width (RDW), as well as the levels of C-reactive protein, hemoglobin, transferrin, and ferritin.
RESULTS:
We included 166 patients, 126 (75.9%) of whom were male. The mean age was 39.0 ± 10.7 years. Not all data were available for all patients: 18.7% were HIV positive; 64.7% were alcoholic; the prevalences of anemia of chronic disease and iron deficiency anemia were, respectively, 75.9% and 2.4%; and 68.7% had low body weight (mean BMI = 18.21 kg/m2). On the basis of TST and AMA, 126 (78.7%) of 160 patients and 138 (87.9%) of 157 patients, respectively, were considered malnourished. Anemia was found to be associated with the following: male gender (p = 0.03); low weight (p = 0.0004); low mean corpuscular volume (p = 0.03);high RDW (p = 0; 0003); high ferritin (p = 0.0005); and high ESR (p = 0.004). We also found significant differences between anemic and non-anemic patients in terms of BMI (p = 0.04), DCT (p = 0.003), and ESR (p < 0.001).
CONCLUSIONS:
In this sample, high proportions of pulmonary tuberculosis patients were classified as underweight and malnourished, and there was a high prevalence of anemia of chronic disease. In addition, anemia was associated with high ESR and malnutrition.
Tuberculosis, pulmonary; Anemia; Malnutrition; Iron
OBJETIVO:
Descrever a prevalência de anemia e de seus tipos em pacientes internados com tuberculose pulmonar.
MÉTODOS:
Estudo descritivo e longitudinal com pacientes com tuberculose pulmonar hospitalizados em dois hospitais de referência na cidade do Rio de Janeiro (RJ). Foram avaliados o índice de massa corpórea (IMC), dobra cutânea tricipital (DCT), área muscular do braço (AMB), VHS, volume globular médio e red blood cell distribution width (RDW, índice de anisocitose eritrocitária), assim como os níveis de proteína C reativa, hemoglobina, transferrina e ferritina.
RESULTADOS:
Foram incluídos 166 pacientes, sendo 126 (75,9%) do sexo masculino. A média de idade foi de 39,0 ± 10,7 anos. Alguns dados não estavam disponíveis para todos os pacientes: 18,7% eram portadores de HIV; 64,7% eram etilistas; as prevalências de anemia da doença crônica e de anemia ferropriva foram, respectivamente, de 75,9% e 2,4%; e 68,7% apresentaram baixo peso (média do IMC = 18,21 kg/m2). Com base em DCT e AMB, respectivamente, 126/160 pacientes (78,7%) e 138/157 pacientes (87,9%) foram considerados desnutridos. A presença de anemia associou-se às seguintes variáveis: sexo masculino (p = 0,03), baixo peso (p = 0,0004), baixo volume globular médio (p = 0,03), alto RDW (p = 0,0003), alto nível de ferritina (p = 0,0005) e de VHS (p = 0,004). Houve diferenças significativas entre pacientes anêmicos e não anêmicos em relação a IMC (p = 0,04), DCT (p = 0,003) e VHS (p < 0,001).
CONCLUSÕES:
Nesta amostra, a proporção de pacientes com tuberculose pulmonar classificados com baixo peso e desnutrição foi elevada, assim como a prevalência de anemia da doença crônica. Além disso, a anemia associou-se a VHS elevada e desnutrição.
Tuberculose pulmonar; Anemia; Desnutrição; Ferro
Introduction
According to the World Health Organization, one third of the world population is
infected with Mycobacterium tuberculosis. It is estimated that
approximately 8.8 million new cases of tuberculosis occur each year; Brazil ranks 18th
among the 22 countries that collectively account for most such cases.(
11. World Health Organization [homepage on the Internet]. Geneva: World
Health Organization [cited 2013 April 4]. Global tuberculosis control: WHO report
2011. [Adobe Acrobat document, 258p.]. Available from:
http://www.who.int/tb/publications/global_report/2011/gtbr11_full.pdf
http://www.who.int/tb/publications/globa...
)
In Brazil, approximately 85,000 cases of tuberculosis occur each year, approximately 5,000 deaths being associated with the disease. The incidence rate of tuberculosis in the country has been estimated at 37.2/100,000 population. Among all Brazilian states, Rio de Janeiro has the highest annual incidence rate of tuberculosis (73.27/100,000 population) and the highest mortality rate (5.0/100,000 population).( 22. Piller RV. Epidemiologia da tuberculose. Pulmão RJ. 2012;21(1):4-9. )
According to the World Health Organization, the severity of the global tuberculosis
situation is primarily due to social inequality, population aging, large migration
flows, and the advent of AIDS in the 1980s.(
33. Ruffino-Netto A. Tuberculose: a calamidade negligenciada. Rev Soc
Bras Med Trop. 2002;35(1):51-58.
http://dx.doi.org/10.1590/S0037-86822002000100010
http://dx.doi.org/10.1590/S0037-86822002...
) In addition to AIDS, risk factors for tuberculosis include alcoholism,
smoking, history of tuberculosis, diabetes mellitus, malnutrition, and low socioeconomic
status.(
44. Zachariah R, Spielmann MP, Harries AD, Salaniponi FM. Moderate to
severe malnutrition in patients with tuberculosis is a risk factor associated with
early death. Trans R Soc Trop Med Hyg. 2002;96(3):291-4.
http://dx.doi.org/10.1016/S0035-9203(02)90103-3
http://dx.doi.org/10.1016/S0035-9203(02)...
)
The association between tuberculosis and malnutrition consists of two interactions: the
effect of tuberculosis on the nutritional status and the effect of malnutrition on the
clinical manifestations of tuberculosis, as a result of immunological
impairment.(
33. Ruffino-Netto A. Tuberculose: a calamidade negligenciada. Rev Soc
Bras Med Trop. 2002;35(1):51-58.
http://dx.doi.org/10.1590/S0037-86822002000100010
http://dx.doi.org/10.1590/S0037-86822002...
,
55. Macallan DC. Malnutrition in tuberculosis. Diagn Microbiol Infect
Dis. 1999;34(2):153-7.
http://dx.doi.org/10.1016/S0732-8893(99)00007-3
http://dx.doi.org/10.1016/S0732-8893(99)...
) Anemia has been observed in 32-94% of patients with tuberculosis
(
66. Lee SW, Kang YA, Yoon YS, Um SW, Lee SM, Yoo CG, et al. The
prevalence and evolution of anemia associated with tuberculosis. J Korean Med Sci.
2006;21(6):1028-32. http://dx.doi.org/10.3346/jkms.2006.21.6.1028
http://dx.doi.org/10.3346/jkms.2006.21.6...
7. Sahiratmadja E, Wieringa FT, van Crevel R, de Visser AW, Adnan I,
Alisjahbana B, et al. Iron deficiency and NRAMP1 polymorphisms (INT4, D543N and
3'UTR) do not contribute to severity of anaemia in tuberculosis in the Indonesian
population. Br J Nutr. 2007;98(4):684-90.
http://dx.doi.org/10.1017/S0007114507742691
http://dx.doi.org/10.1017/S0007114507742...
-
88. Isanaka S, Mugusi F, Urassa W, Willett WC, Bosch RJ, Villamor E, et
al. Iron deficiency and anemia predict mortality in patients with tuberculosis. J
Nutr. 2012;142(2):350-7. http://dx.doi.org/10.3945/jn.111.144287
http://dx.doi.org/10.3945/jn.111.144287...
)
Iron deficiency is the most common micronutrient deficiency in the world, and numerous
studies have evaluated the association between serum iron levels and iron-deficiency
anemia.(
99. Oppenheimer SJ. Iron and its relation to immunity and infectious
disease. J Nutr. 2001;131(2S-2):616S-633S. discussion 633S-635S.
,
1010. Abba K, Sudarsanam TD, Grobler L, Volmink J. Nutritional supplements
for people being treated for active tuberculosis. Cochrane Database Syst Rev.
2008;(4):CD006086. http://dx.doi.org/10.1002/14651858.CD006086.pub2
http://dx.doi.org/10.1002/14651858.CD006...
) However, there is controversy regarding the administration of iron; some
studies have shown that iron deficiency increases susceptibility to infectious
processes, whereas others have shown that excess iron is more harmful to the human body
than is iron deficiency, and that iron deficiency can protect against
infection.(
1111. Bricks LF. Ferro e infecções. Atualização. Pediat. (S.
Paulo).1994;16(1):34-43.
)
Among the anemias that are characterized by altered iron metabolism, iron-deficiency anemia and anemia of chronic disease are the most common.( 1212. Carvalho MC, Baracat EC, Sgarbieri VC. Anemia ferropriva e anemia da doença crônica: distúrbios do metabolismo de ferro. Segurança Alimentar e Nutricional. 2006;13(2):54-63. )
Iron-deficiency anemia is the most common nutritional deficiency worldwide, affecting primarily individuals residing in developing countries. It occurs as a result of chronic blood loss, urinary losses, poor iron intake/absorption, and increased blood volume. In individuals with iron-deficiency anemia, a decrease in plasma iron levels occurs, limiting erythropoiesis. The risk of developing iron-deficiency anemia is highest among infants, children under 5 years of age, and women of childbearing age.( 1212. Carvalho MC, Baracat EC, Sgarbieri VC. Anemia ferropriva e anemia da doença crônica: distúrbios do metabolismo de ferro. Segurança Alimentar e Nutricional. 2006;13(2):54-63. )
Anemia of chronic disease, also known as anemia of inflammation, is a clinical syndrome characterized by the development of anemia in patients with (fungal, bacterial, or viral) infectious diseases, such as tuberculosis, inflammatory diseases, autoimmune diseases, and neoplastic diseases.( 1313. Cançado RD, Chiattone CS. Anemia da doença crônica. Rev Bras Hematol Hemoter. 2002;24(2):127-36. ) It is characterized by mild to moderate normocytic hypochromic anemia, and hypochromia and microcytosis can occur in 20-30% of cases. However, when microcytosis occurs, it is not as pronounced as it is in iron-deficiency anemia.( 1212. Carvalho MC, Baracat EC, Sgarbieri VC. Anemia ferropriva e anemia da doença crônica: distúrbios do metabolismo de ferro. Segurança Alimentar e Nutricional. 2006;13(2):54-63. ) This type of anemia is associated with decreased serum iron levels and total iron binding capacity, as well as with increased ferritin levels.( 1313. Cançado RD, Chiattone CS. Anemia da doença crônica. Rev Bras Hematol Hemoter. 2002;24(2):127-36. )
In patients with active tuberculosis, few of the studies investigating the presence of
anemia have determined whether anemia is associated with iron deficiency or chronic
disease or have identified variables associated with its occurrence.(
66. Lee SW, Kang YA, Yoon YS, Um SW, Lee SM, Yoo CG, et al. The
prevalence and evolution of anemia associated with tuberculosis. J Korean Med Sci.
2006;21(6):1028-32. http://dx.doi.org/10.3346/jkms.2006.21.6.1028
http://dx.doi.org/10.3346/jkms.2006.21.6...
7. Sahiratmadja E, Wieringa FT, van Crevel R, de Visser AW, Adnan I,
Alisjahbana B, et al. Iron deficiency and NRAMP1 polymorphisms (INT4, D543N and
3'UTR) do not contribute to severity of anaemia in tuberculosis in the Indonesian
population. Br J Nutr. 2007;98(4):684-90.
http://dx.doi.org/10.1017/S0007114507742691
http://dx.doi.org/10.1017/S0007114507742...
-
88. Isanaka S, Mugusi F, Urassa W, Willett WC, Bosch RJ, Villamor E, et
al. Iron deficiency and anemia predict mortality in patients with tuberculosis. J
Nutr. 2012;142(2):350-7. http://dx.doi.org/10.3945/jn.111.144287
http://dx.doi.org/10.3945/jn.111.144287...
)
The objective of the present study was to describe the prevalence of anemia and of its types in hospitalized patients with pulmonary tuberculosis, as well as to examine the relationship between anemia and the clinical and nutritional status of anemic patients in comparison with non-anemic patients.
Methods
This was a prospective cross-sectional descriptive study, which included active pulmonary tuberculosis patients consecutively admitted to one of two tuberculosis referral hospitals in the state of Rio de Janeiro (namely Instituto Estadual de Doenças do Tórax Ary Parreiras and Hospital Estadual Santa Maria, both located in the city of Rio de Janeiro) and initiating antituberculosis treatment between March of 2007 and December of 2010. All participants gave written informed consent.
Patients under 18 years of age or over 60 years of age were excluded, as were those who had previously undergone tuberculosis treatment or who had been receiving treatment with antituberculosis drugs for more than seven days; those with diabetes mellitus receiving insulin therapy; those with renal failure on peritoneal dialysis or hemodialysis; those who had received blood transfusions in the 3 months preceding study entry; and those who were pregnant or lactating. For data collection, we used a standardized questionnaire and reviewed medical records. In addition, we collected blood samples and performed medical and nutritional assessment up to seven days after the initiation of pharmacological treatment. Alcohol abuse was defined as a daily intake of 30 g or more for males and of 24 g or more for females. The Cut down, Annoyed, Guilty, and Eye-opener (CAGE) questionnaire was used in order to identify alcohol abuse.( 1414. Mayfield D, McLeod G, Hall P. The GAGE questionnaire: validation of a new alcoholism screening instrument. Am J Psychiatry. 1974;131(10):1121-3. )
Nutritional assessment included measurements of weight, height, and body mass index
(BMI), in order to identify patients who were underweight,(
1515. Frisancho AR. New norms of upper limb fat and muscle areas for
assessment of nutritional status. Am J Clin Nutr.
1981;34(11):2540-5.
) as well as measurements of triceps skinfold thickness (TST) and arm muscle
area (AMA), in order to identify patients who were malnourished. (
1515. Frisancho AR. New norms of upper limb fat and muscle areas for
assessment of nutritional status. Am J Clin Nutr.
1981;34(11):2540-5.
,
1616. Metcalfe N. A study of tuberculosis, malnutrition and gender in Sri
Lanka. Trans R Soc Trop Med Hyg. 2005;99(2):115-9.
http://dx.doi.org/10.1016/j.trstmh.2004.06.007
http://dx.doi.org/10.1016/j.trstmh.2004....
)
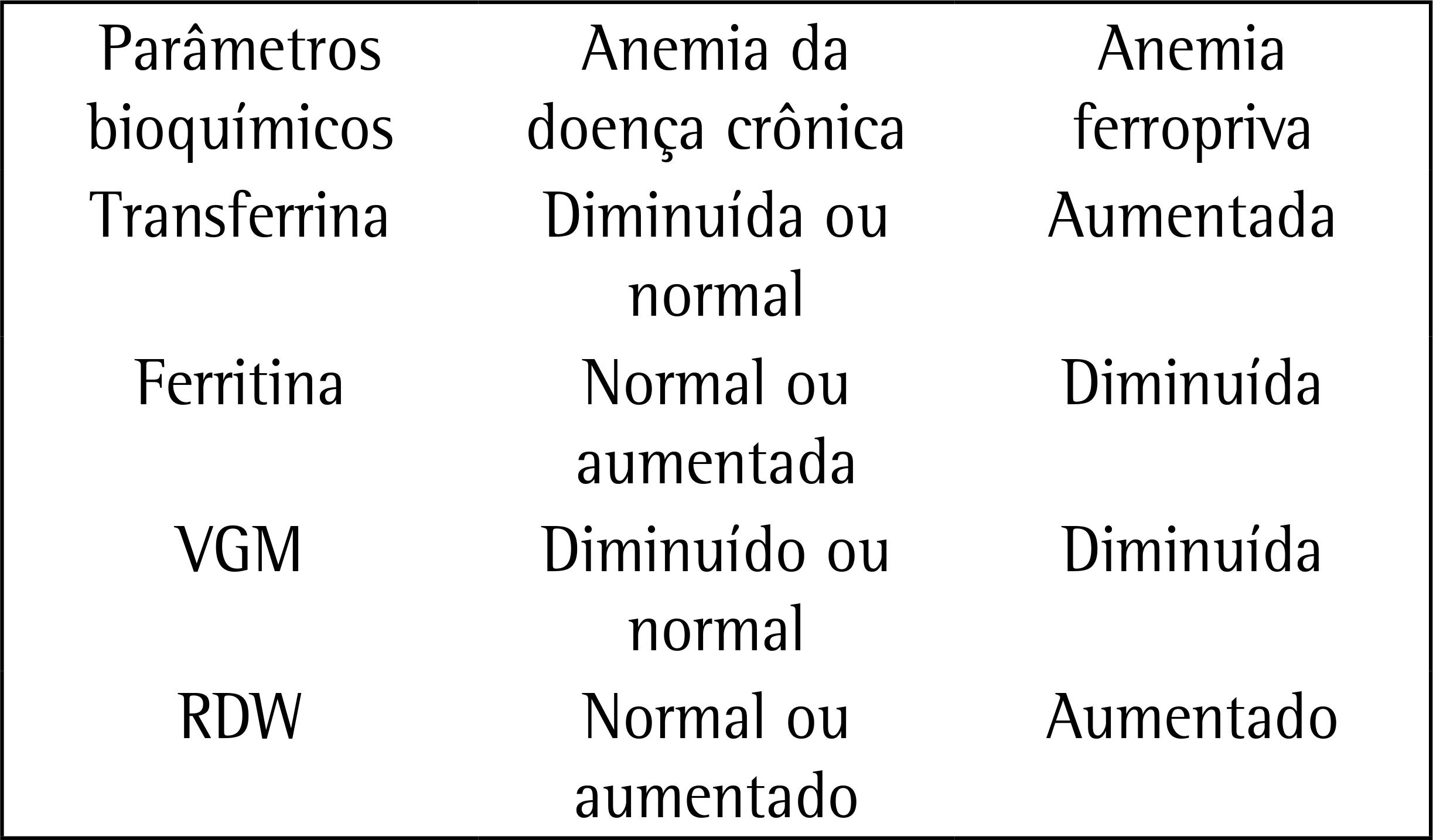
In order to classify anemia, we analyzed the following parameters: hemoglobin levels; transferrin levels; ferritin levels; and mean corpuscular volume (MCV). We used red blood cell distribution width (RDW) in order to assess the presence of anisocytosis. This classification is shown in Chart 1. In addition to the aforementioned measurements, we performed measurements of C-reactive protein (CRP) and ESR, as well as HIV testing. All tests were performed in a laboratory certified by the Brazilian Clinical Pathology Association Clinical Laboratory Accreditation Program. Iron-deficiency anemia was characterized by decreased levels of iron and ferritin and increased levels of transferrin, whereas anemia of chronic disease was characterized by decreased levels of iron and transferrin and increased levels of ferritin.( 1313. Cançado RD, Chiattone CS. Anemia da doença crônica. Rev Bras Hematol Hemoter. 2002;24(2):127-36. )
Parameters for the evaluation of the types of anemia studied. MCV: mean corpuscular volume; and RDW: red blood cell distribution width
For statistical analysis, we used descriptive statistics, including range (minimum and maximum values), mean, standard deviation, median, interquartile range, and 95% CI. We used the Kolmogorov-Smirnov test in order to test the normality of the variables and Levene's test in order to determine the equality of variances. We used the Student's t-test in order to compare means with normal distribution between the groups of patients with and without anemia. We used ANOVA in order to analyze the differences among quantitative variables and the chi-square test in order to identify associations among categorical variables. For the identification of variables associated with anemia, we used multivariate logistic regression analysis in order to assess the presence of confounding covariates. Covariates with values of p < 0.20 in the bivariate analysis were included in the model. Values of p < 0.05 were considered statistically significant. All analyses were performed with the Statistical Package for the Social Sciences, version 16.0 for Windows (SPSS Inc., Chicago, IL, USA).
The present study was approved by the Research Ethics Committee of the Federal University of Rio de Janeiro School of Medicine Clementino Fraga Filho University Hospital on April 28, 2005 (Protocol no. 004/05).
Results
We included 166 patients, 126 (75.9%) of whom were male. The mean age was 39.0 ± 10.7 years. In our sample, 95 (62.5%) of 152 patients were non-White; 18 (18.7%) of 96 patients were HIV-positive; 97 (64.7%) of 150 patients were considered alcoholic on the basis of the CAGE questionnaire; 118 (74.7%) of 158 patients were classified as smokers or former smokers; and 47 (30.1%) of 156 patients reported illicit drug use. Of the 166 patients, 18 (10.9%) had no anemia and 148 (89.1%) had anemia. Of those, 4 (2.4%) had iron-deficiency anemia and 126 (75.9%) had anemia of chronic disease; in the remaining 18 patients, it was impossible to distinguish between the two.
We found low hemoglobin levels (mean, 10.86 ± 2.04 g/dL) in 89.2% of patients; low transferrin levels (mean, 177.28 ± 58.71 mg/dL) in 65.3%; and low MCV (mean, 82.00 ± 7.77 fL) in 39.7%. In addition, we found high ferritin levels (mean, 520.68 ± 284.26 ng/mL) in 52.7% of patients; high RDW (mean, 16.36 ± 3.47%) in 55.4%; high CRP levels (mean, 5.84 ± 4.22 mg/dL) in 98.2%; and high ESR (mean, 60.30 ± 39.84 mm/h) in 84.3%.
On the basis of the BMI, 88 (68.7%) of 128 patients were underweight (mean, 18.21 ± 2.93 kg/m2). On the basis of the TST, 126 (78.7%) of 160 patients were mildly, moderately, or severely malnourished (mean, 6.16 ± 3.83 mm). On the basis of the AMA, 138 (87.9%) of 157 patients were mildly, moderately, or severely malnourished (mean, 24.41 ± 9.86 cm2).
When we compared the sociodemographic and clinical variables between the groups of patients with and without anemia, we found an association of anemia with the male gender (p = 0.03) and a trend toward an association of anemia with being a smoker or former smoker (p = 0.05; Tables 1 and 2). Table 3 shows a comparison of nutritional and laboratory variables between the groups of patients with and without anemia. Anemia was found to be associated with the following: BMI (p = 0.0004); MCV (p = 0.03); ferritin (p = 0.0005); RDW (p = 0.0003); and ESR (p = 0.004). After the multivariate analysis, ESR was the only independent variable that remained.
Table 4 shows the results of the correlation of nutritional and laboratory variables with the presence of anemia. Mean BMI and mean TST were significantly lower in the patients with anemia than in those without. However, high ESR values were significantly associated with anemia (p < 0.001). Nevertheless, there were no significant differences between the groups of patients with and without anemia regarding AMA, transferrin levels, ferritin levels, or MCV.
Discussion
In the present study, pulmonary tuberculosis was found to be more common in young adults, males, alcoholics, smokers, illicit drug users, and HIV-positive patients; this finding is similar to those reported in studies evaluating pulmonary tuberculosis inpatients at general and tuberculosis referral hospitals in Brazil.( 1717. Shah S, Whalen C, Kotler DP, Mayanja H, Namale A, Melikian G, et al. Severity of human immunodeficiency virus infection is associated with decreased phase angle, fat mass and body cell mass in adults with pulmonary tuberculosis infection in Uganda. J Nutr. 2001;131(11):2843-7. , 1818. Conde MB, Melo FA, Marques AM, Cardoso NC, Pinheiro VG, Dalcin Pde T, et al. III Brazilian Thoracic Association Guidelines on tuberculosis. J Bras Pneumol. 2009;35(10):1018-48. )
The prevalence of anemia in the present study (89.2%) was higher than was that in a
study conducted in South Korea (32%)(
66. Lee SW, Kang YA, Yoon YS, Um SW, Lee SM, Yoo CG, et al. The
prevalence and evolution of anemia associated with tuberculosis. J Korean Med Sci.
2006;21(6):1028-32. http://dx.doi.org/10.3346/jkms.2006.21.6.1028
http://dx.doi.org/10.3346/jkms.2006.21.6...
) and similar to that in studies conducted in Indonesia (63%),(
77. Sahiratmadja E, Wieringa FT, van Crevel R, de Visser AW, Adnan I,
Alisjahbana B, et al. Iron deficiency and NRAMP1 polymorphisms (INT4, D543N and
3'UTR) do not contribute to severity of anaemia in tuberculosis in the Indonesian
population. Br J Nutr. 2007;98(4):684-90.
http://dx.doi.org/10.1017/S0007114507742691
http://dx.doi.org/10.1017/S0007114507742...
) Tanzania (96%),(
88. Isanaka S, Mugusi F, Urassa W, Willett WC, Bosch RJ, Villamor E, et
al. Iron deficiency and anemia predict mortality in patients with tuberculosis. J
Nutr. 2012;142(2):350-7. http://dx.doi.org/10.3945/jn.111.144287
http://dx.doi.org/10.3945/jn.111.144287...
) and Malawi (88%).(
1919. Krapp F, Véliz JC, Cornejo E, Gotuzzo E, Seas C. Bodyweight gain to
predict treatment outcome in patients with pulmonary tuberculosis in Peru. Int J
Tuberc Lung Dis. 2008;12(10):1153-9.
) In the present study, the proportion of patients with anemia of chronic
disease was higher than was that of those with iron-deficiency anemia (75.9% vs. 2.4%),
a finding that was similar to those reported in other studies(
66. Lee SW, Kang YA, Yoon YS, Um SW, Lee SM, Yoo CG, et al. The
prevalence and evolution of anemia associated with tuberculosis. J Korean Med Sci.
2006;21(6):1028-32. http://dx.doi.org/10.3346/jkms.2006.21.6.1028
http://dx.doi.org/10.3346/jkms.2006.21.6...
,
77. Sahiratmadja E, Wieringa FT, van Crevel R, de Visser AW, Adnan I,
Alisjahbana B, et al. Iron deficiency and NRAMP1 polymorphisms (INT4, D543N and
3'UTR) do not contribute to severity of anaemia in tuberculosis in the Indonesian
population. Br J Nutr. 2007;98(4):684-90.
http://dx.doi.org/10.1017/S0007114507742691
http://dx.doi.org/10.1017/S0007114507742...
) but different from those reported in another study.(
88. Isanaka S, Mugusi F, Urassa W, Willett WC, Bosch RJ, Villamor E, et
al. Iron deficiency and anemia predict mortality in patients with tuberculosis. J
Nutr. 2012;142(2):350-7. http://dx.doi.org/10.3945/jn.111.144287
http://dx.doi.org/10.3945/jn.111.144287...
) In the bivariate analysis, anemia was found to be more common in males than
in females, a finding that is inconsistent with the literature.(
66. Lee SW, Kang YA, Yoon YS, Um SW, Lee SM, Yoo CG, et al. The
prevalence and evolution of anemia associated with tuberculosis. J Korean Med Sci.
2006;21(6):1028-32. http://dx.doi.org/10.3346/jkms.2006.21.6.1028
http://dx.doi.org/10.3346/jkms.2006.21.6...
7. Sahiratmadja E, Wieringa FT, van Crevel R, de Visser AW, Adnan I,
Alisjahbana B, et al. Iron deficiency and NRAMP1 polymorphisms (INT4, D543N and
3'UTR) do not contribute to severity of anaemia in tuberculosis in the Indonesian
population. Br J Nutr. 2007;98(4):684-90.
http://dx.doi.org/10.1017/S0007114507742691
http://dx.doi.org/10.1017/S0007114507742...
-
88. Isanaka S, Mugusi F, Urassa W, Willett WC, Bosch RJ, Villamor E, et
al. Iron deficiency and anemia predict mortality in patients with tuberculosis. J
Nutr. 2012;142(2):350-7. http://dx.doi.org/10.3945/jn.111.144287
http://dx.doi.org/10.3945/jn.111.144287...
) However, the association between anemia and the male gender was not
confirmed in the multivariate analysis; likewise, we found no association between anemia
and HIV infection, a finding that is in disagreement with those reported in other
studies.(
88. Isanaka S, Mugusi F, Urassa W, Willett WC, Bosch RJ, Villamor E, et
al. Iron deficiency and anemia predict mortality in patients with tuberculosis. J
Nutr. 2012;142(2):350-7. http://dx.doi.org/10.3945/jn.111.144287
http://dx.doi.org/10.3945/jn.111.144287...
,
1919. Krapp F, Véliz JC, Cornejo E, Gotuzzo E, Seas C. Bodyweight gain to
predict treatment outcome in patients with pulmonary tuberculosis in Peru. Int J
Tuberc Lung Dis. 2008;12(10):1153-9.
)
On the basis of the BMI, 68.7% of patients were found to be underweight, a proportion
that is higher than that reported in a study conducted in Peru (21%)(
2020. van Lettow M, West CE, van der Meer JW, Wieringa FT, Semba RD. Low
plasma selenium concentrations, high plasma human immunodeficiency virus load and
high interleukin-6 concentrations are risk factors associated with anemia in adults
presenting with pulmonary tuberculosis in Zomba district, Malawi. Eur J Clin Nutr.
2005;59(4):526-32. http://dx.doi.org/1602116A/sj.bjp.0704832
http://dx.doi.org/1602116A/sj.bjp.070483...
) and similar to those reported in studies conducted in Malawi(
44. Zachariah R, Spielmann MP, Harries AD, Salaniponi FM. Moderate to
severe malnutrition in patients with tuberculosis is a risk factor associated with
early death. Trans R Soc Trop Med Hyg. 2002;96(3):291-4.
http://dx.doi.org/10.1016/S0035-9203(02)90103-3
http://dx.doi.org/10.1016/S0035-9203(02)...
,
2121. Onwubalili JK. Malnutrition among tuberculosis patients in Harrow,
England. Eur J Clin Nutr. 1988;42(4):363-6.
) and England.(
2222. Harries AD, Nkhoma WA, Thompson PJ, Nyangulu DS, Wirima JJ.
Nutritional status in Malawian patients with pulmonary tuberculosis and response to
chemotherapy. Eur J Clin Nutr. 1988;42(5):445-50.
) This is probably due to the fact that those studies included high
proportions of HIV-positive inpatients.
On the basis of the TST and AMA, 126 (78.7%) of 160 patients and 138 (87.9%) of 157 patients, respectively, were considered malnourished. Similar results have been reported elsewhere.( 2222. Harries AD, Nkhoma WA, Thompson PJ, Nyangulu DS, Wirima JJ. Nutritional status in Malawian patients with pulmonary tuberculosis and response to chemotherapy. Eur J Clin Nutr. 1988;42(5):445-50. ) A 13% reduction in TST and a 20% reduction in AMA were reported in a case-control study,( 2222. Harries AD, Nkhoma WA, Thompson PJ, Nyangulu DS, Wirima JJ. Nutritional status in Malawian patients with pulmonary tuberculosis and response to chemotherapy. Eur J Clin Nutr. 1988;42(5):445-50. ) whereas a 35% reduction in TST and a 19% reduction in AMA were reported in another study.( 2121. Onwubalili JK. Malnutrition among tuberculosis patients in Harrow, England. Eur J Clin Nutr. 1988;42(4):363-6. )
Almost all of the patients included in our study were found to have elevated levels of
CRP and ESR, a finding that is similar to those reported in the literature.(
77. Sahiratmadja E, Wieringa FT, van Crevel R, de Visser AW, Adnan I,
Alisjahbana B, et al. Iron deficiency and NRAMP1 polymorphisms (INT4, D543N and
3'UTR) do not contribute to severity of anaemia in tuberculosis in the Indonesian
population. Br J Nutr. 2007;98(4):684-90.
http://dx.doi.org/10.1017/S0007114507742691
http://dx.doi.org/10.1017/S0007114507742...
,
2323. Peresi E, Silva SM, Calvi SA, Marcondes-Machado J. Cytokines and
acute phase serum proteins as markers of inflammatory regression during the treatment
of pulmonary tuberculosis. J Bras Pneumol. 2008;34(11):942-9.
http://dx.doi.org/10.1590/S1806-37132008001100009
http://dx.doi.org/10.1590/S1806-37132008...
,
2424. Grange JM, Kardjito T, Setiabudi I. A study of acute-phase reactant
proteins in Indonesian patients with pulmonary tuberculosis. Tubercle.
1984;65(1):23-39.
) We believe that CRP and ESR can be useful as markers of the effect of
treatment and of the resolution of inflammation, given that CRP and ESR levels decreased
during antituberculosis treatment, having normalized by the end of the treatment period
(data not shown).
The concentrations of most proteins are elevated in tuberculosis patients, the exception
being the concentrations of transferrin and hemoglobin, which are decreased.(
2525. Wong CT, Saha N. Changes in serum proteins (albumin, immunoglobulins
and acute phase proteins) in pulmonary tuberculosis during therapy. Tubercle.
1990;71(3):193-7.
) In our study, we found low concentrations of transferrin and high
concentrations of ferritin, a finding that is similar to those reported by other groups
of authors.(
66. Lee SW, Kang YA, Yoon YS, Um SW, Lee SM, Yoo CG, et al. The
prevalence and evolution of anemia associated with tuberculosis. J Korean Med Sci.
2006;21(6):1028-32. http://dx.doi.org/10.3346/jkms.2006.21.6.1028
http://dx.doi.org/10.3346/jkms.2006.21.6...
,
77. Sahiratmadja E, Wieringa FT, van Crevel R, de Visser AW, Adnan I,
Alisjahbana B, et al. Iron deficiency and NRAMP1 polymorphisms (INT4, D543N and
3'UTR) do not contribute to severity of anaemia in tuberculosis in the Indonesian
population. Br J Nutr. 2007;98(4):684-90.
http://dx.doi.org/10.1017/S0007114507742691
http://dx.doi.org/10.1017/S0007114507742...
,
2525. Wong CT, Saha N. Changes in serum proteins (albumin, immunoglobulins
and acute phase proteins) in pulmonary tuberculosis during therapy. Tubercle.
1990;71(3):193-7.
,
2626. Monteiro L. Valores de referência do RDW-CV e do RDW-SD e sua
relação com o VCM entre os pacientes atendidos no ambulatório do Hospital
Universitário Oswaldo Cruz- Recife, PE. Rev Bras Hematol Hemoter. 2009;32(1):34-9.
http://dx.doi.org/10.1590/S1516-84842010005000013
http://dx.doi.org/10.1590/S1516-84842010...
)
In conditions other than inflammatory conditions, determination of ferritin levels is the most sensitive method for the diagnosis of iron deficiency. However, in tuberculosis patients, determination of ferritin levels should be used with caution because ferritin levels do not accurately express the amount of iron in such patients. Therefore, patients can have iron deficiency even when they have normal or increased ferritin levels.( 1313. Cançado RD, Chiattone CS. Anemia da doença crônica. Rev Bras Hematol Hemoter. 2002;24(2):127-36. )
Given that microcytosis was observed in most of the patients in the present study,
increased RDW might be useful to demonstrate iron deficiency,(
2626. Monteiro L. Valores de referência do RDW-CV e do RDW-SD e sua
relação com o VCM entre os pacientes atendidos no ambulatório do Hospital
Universitário Oswaldo Cruz- Recife, PE. Rev Bras Hematol Hemoter. 2009;32(1):34-9.
http://dx.doi.org/10.1590/S1516-84842010005000013
http://dx.doi.org/10.1590/S1516-84842010...
) although its role remains controversial.(
2727. Corsonello A, Pedone C, Battaglia S, Paglino G, Bellia V, et al.
C-reactive protein (CRP) and erythrocyte sedimentation rate (ESR) as inflammation
markers in elderly patients with stable chronic obstructive pulmonary disease (COPD).
Arch Gerontol Geriatr. 2011;53(2):190-5.
http://dx.doi.org/10.1016/j.archger.2010.10.015
http://dx.doi.org/10.1016/j.archger.2010...
)
When we compared the groups of patients with and without anemia in terms of their
nutritional status, we found that malnutrition was more severe in the former, who had
low serum concentrations of transferrin and high serum concentrations of ferritin, as
reported in one study.(
77. Sahiratmadja E, Wieringa FT, van Crevel R, de Visser AW, Adnan I,
Alisjahbana B, et al. Iron deficiency and NRAMP1 polymorphisms (INT4, D543N and
3'UTR) do not contribute to severity of anaemia in tuberculosis in the Indonesian
population. Br J Nutr. 2007;98(4):684-90.
http://dx.doi.org/10.1017/S0007114507742691
http://dx.doi.org/10.1017/S0007114507742...
) Regarding the inflammatory state, the multivariate analysis showed that ESR
was higher in the patients with anemia than in those without, the difference being
significant. One group of authors(
2727. Corsonello A, Pedone C, Battaglia S, Paglino G, Bellia V, et al.
C-reactive protein (CRP) and erythrocyte sedimentation rate (ESR) as inflammation
markers in elderly patients with stable chronic obstructive pulmonary disease (COPD).
Arch Gerontol Geriatr. 2011;53(2):190-5.
http://dx.doi.org/10.1016/j.archger.2010.10.015
http://dx.doi.org/10.1016/j.archger.2010...
) found that ESR increases in response to anemia, a finding that corroborates
the results of the present study. However, although we excluded patients with a history
of tuberculosis, those receiving insulin therapy, those on peritoneal dialysis or
hemodialysis, and those who had received blood transfusions in the 3 months preceding
study entry, the associations of ESR and CRP with anemia in the present study should be
confirmed in studies investigating larger samples, preferably with a higher prevalence
of iron-deficiency anemia and without the presence of comorbidities such as HIV
infection, alcoholism, and smoking.
Given that it was impossible to use all of the recommended parameters for the
differential diagnosis between iron-deficiency anemia and anemia of chronic disease,
including transferrin receptor and bone marrow analysis,(
1313. Cançado RD, Chiattone CS. Anemia da doença crônica. Rev Bras Hematol
Hemoter. 2002;24(2):127-36.
) the criteria used in the present study resulted in a low frequency of
iron-deficiency anemia in isolation. However, we believe that some of the patients with
anemia of chronic disease also had iron-deficiency anemia, as reported in one
study.(
88. Isanaka S, Mugusi F, Urassa W, Willett WC, Bosch RJ, Villamor E, et
al. Iron deficiency and anemia predict mortality in patients with tuberculosis. J
Nutr. 2012;142(2):350-7. http://dx.doi.org/10.3945/jn.111.144287
http://dx.doi.org/10.3945/jn.111.144287...
) In such cases, not all patients benefit from iron
supplementation.(
1313. Cançado RD, Chiattone CS. Anemia da doença crônica. Rev Bras Hematol
Hemoter. 2002;24(2):127-36.
) In another study,(
77. Sahiratmadja E, Wieringa FT, van Crevel R, de Visser AW, Adnan I,
Alisjahbana B, et al. Iron deficiency and NRAMP1 polymorphisms (INT4, D543N and
3'UTR) do not contribute to severity of anaemia in tuberculosis in the Indonesian
population. Br J Nutr. 2007;98(4):684-90.
http://dx.doi.org/10.1017/S0007114507742691
http://dx.doi.org/10.1017/S0007114507742...
) after successful tuberculosis treatment, anemia was corrected without iron
supplementation in most patients.
In conclusion, high proportions of pulmonary tuberculosis patients were classified as underweight and malnourished on the basis of different parameters (BMI, AMA, and TST), and there was a high prevalence of anemia of chronic disease. In addition, the degree of malnutrition was higher in the patients with anemia than in those without.
References
-
1World Health Organization [homepage on the Internet]. Geneva: World Health Organization [cited 2013 April 4]. Global tuberculosis control: WHO report 2011. [Adobe Acrobat document, 258p.]. Available from: http://www.who.int/tb/publications/global_report/2011/gtbr11_full.pdf
» http://www.who.int/tb/publications/global_report/2011/gtbr11_full.pdf -
2Piller RV. Epidemiologia da tuberculose. Pulmão RJ. 2012;21(1):4-9.
-
3Ruffino-Netto A. Tuberculose: a calamidade negligenciada. Rev Soc Bras Med Trop. 2002;35(1):51-58. http://dx.doi.org/10.1590/S0037-86822002000100010
» http://dx.doi.org/10.1590/S0037-86822002000100010 -
4Zachariah R, Spielmann MP, Harries AD, Salaniponi FM. Moderate to severe malnutrition in patients with tuberculosis is a risk factor associated with early death. Trans R Soc Trop Med Hyg. 2002;96(3):291-4. http://dx.doi.org/10.1016/S0035-9203(02)90103-3
» http://dx.doi.org/10.1016/S0035-9203(02)90103-3 -
5Macallan DC. Malnutrition in tuberculosis. Diagn Microbiol Infect Dis. 1999;34(2):153-7. http://dx.doi.org/10.1016/S0732-8893(99)00007-3
» http://dx.doi.org/10.1016/S0732-8893(99)00007-3 -
6Lee SW, Kang YA, Yoon YS, Um SW, Lee SM, Yoo CG, et al. The prevalence and evolution of anemia associated with tuberculosis. J Korean Med Sci. 2006;21(6):1028-32. http://dx.doi.org/10.3346/jkms.2006.21.6.1028
» http://dx.doi.org/10.3346/jkms.2006.21.6.1028 -
7Sahiratmadja E, Wieringa FT, van Crevel R, de Visser AW, Adnan I, Alisjahbana B, et al. Iron deficiency and NRAMP1 polymorphisms (INT4, D543N and 3'UTR) do not contribute to severity of anaemia in tuberculosis in the Indonesian population. Br J Nutr. 2007;98(4):684-90. http://dx.doi.org/10.1017/S0007114507742691
» http://dx.doi.org/10.1017/S0007114507742691 -
8Isanaka S, Mugusi F, Urassa W, Willett WC, Bosch RJ, Villamor E, et al. Iron deficiency and anemia predict mortality in patients with tuberculosis. J Nutr. 2012;142(2):350-7. http://dx.doi.org/10.3945/jn.111.144287
» http://dx.doi.org/10.3945/jn.111.144287 -
9Oppenheimer SJ. Iron and its relation to immunity and infectious disease. J Nutr. 2001;131(2S-2):616S-633S. discussion 633S-635S.
-
10Abba K, Sudarsanam TD, Grobler L, Volmink J. Nutritional supplements for people being treated for active tuberculosis. Cochrane Database Syst Rev. 2008;(4):CD006086. http://dx.doi.org/10.1002/14651858.CD006086.pub2
» http://dx.doi.org/10.1002/14651858.CD006086.pub2 -
11Bricks LF. Ferro e infecções. Atualização. Pediat. (S. Paulo).1994;16(1):34-43.
-
12Carvalho MC, Baracat EC, Sgarbieri VC. Anemia ferropriva e anemia da doença crônica: distúrbios do metabolismo de ferro. Segurança Alimentar e Nutricional. 2006;13(2):54-63.
-
13Cançado RD, Chiattone CS. Anemia da doença crônica. Rev Bras Hematol Hemoter. 2002;24(2):127-36.
-
14Mayfield D, McLeod G, Hall P. The GAGE questionnaire: validation of a new alcoholism screening instrument. Am J Psychiatry. 1974;131(10):1121-3.
-
15Frisancho AR. New norms of upper limb fat and muscle areas for assessment of nutritional status. Am J Clin Nutr. 1981;34(11):2540-5.
-
16Metcalfe N. A study of tuberculosis, malnutrition and gender in Sri Lanka. Trans R Soc Trop Med Hyg. 2005;99(2):115-9. http://dx.doi.org/10.1016/j.trstmh.2004.06.007
» http://dx.doi.org/10.1016/j.trstmh.2004.06.007 -
17Shah S, Whalen C, Kotler DP, Mayanja H, Namale A, Melikian G, et al. Severity of human immunodeficiency virus infection is associated with decreased phase angle, fat mass and body cell mass in adults with pulmonary tuberculosis infection in Uganda. J Nutr. 2001;131(11):2843-7.
-
18Conde MB, Melo FA, Marques AM, Cardoso NC, Pinheiro VG, Dalcin Pde T, et al. III Brazilian Thoracic Association Guidelines on tuberculosis. J Bras Pneumol. 2009;35(10):1018-48.
-
19Krapp F, Véliz JC, Cornejo E, Gotuzzo E, Seas C. Bodyweight gain to predict treatment outcome in patients with pulmonary tuberculosis in Peru. Int J Tuberc Lung Dis. 2008;12(10):1153-9.
-
20van Lettow M, West CE, van der Meer JW, Wieringa FT, Semba RD. Low plasma selenium concentrations, high plasma human immunodeficiency virus load and high interleukin-6 concentrations are risk factors associated with anemia in adults presenting with pulmonary tuberculosis in Zomba district, Malawi. Eur J Clin Nutr. 2005;59(4):526-32. http://dx.doi.org/1602116A/sj.bjp.0704832
» http://dx.doi.org/1602116A/sj.bjp.0704832 -
21Onwubalili JK. Malnutrition among tuberculosis patients in Harrow, England. Eur J Clin Nutr. 1988;42(4):363-6.
-
22Harries AD, Nkhoma WA, Thompson PJ, Nyangulu DS, Wirima JJ. Nutritional status in Malawian patients with pulmonary tuberculosis and response to chemotherapy. Eur J Clin Nutr. 1988;42(5):445-50.
-
23Peresi E, Silva SM, Calvi SA, Marcondes-Machado J. Cytokines and acute phase serum proteins as markers of inflammatory regression during the treatment of pulmonary tuberculosis. J Bras Pneumol. 2008;34(11):942-9. http://dx.doi.org/10.1590/S1806-37132008001100009
» http://dx.doi.org/10.1590/S1806-37132008001100009 -
24Grange JM, Kardjito T, Setiabudi I. A study of acute-phase reactant proteins in Indonesian patients with pulmonary tuberculosis. Tubercle. 1984;65(1):23-39.
-
25Wong CT, Saha N. Changes in serum proteins (albumin, immunoglobulins and acute phase proteins) in pulmonary tuberculosis during therapy. Tubercle. 1990;71(3):193-7.
-
26Monteiro L. Valores de referência do RDW-CV e do RDW-SD e sua relação com o VCM entre os pacientes atendidos no ambulatório do Hospital Universitário Oswaldo Cruz- Recife, PE. Rev Bras Hematol Hemoter. 2009;32(1):34-9. http://dx.doi.org/10.1590/S1516-84842010005000013
» http://dx.doi.org/10.1590/S1516-84842010005000013 -
27Corsonello A, Pedone C, Battaglia S, Paglino G, Bellia V, et al. C-reactive protein (CRP) and erythrocyte sedimentation rate (ESR) as inflammation markers in elderly patients with stable chronic obstructive pulmonary disease (COPD). Arch Gerontol Geriatr. 2011;53(2):190-5. http://dx.doi.org/10.1016/j.archger.2010.10.015
» http://dx.doi.org/10.1016/j.archger.2010.10.015
-
Financial support: This study received financial support from the Brazilian Conselho Nacional de Desenvolvimento Científico e Tecnológico/Ministério da Ciência, Tecnologia e Inovação (CNPq/MCTI, National Council for Scientific and Technological Development/National Ministry of Science, Technology, and Innovation; Grant nos. CNPq/INCT 573548/2008-0 and 478033/2009-5) and the Foundation for the Support of Research in the State of Rio de Janeiro (Grant no. E26/110.974/2011).
-
*
Study carried out at the Tuberculosis Research Center, Clementino Fraga Filho University Hospital, Federal University of Rio de Janeiro School of Medicine, Rio de Janeiro, Brazil.
Publication Dates
-
Publication in this collection
Jul-Aug 2014
History
-
Received
03 Apr 2013 -
Accepted
27 June 2014