INTRODUCTION
Smoking is a significant public health challenge1, although recently there have been sizeable reductions in smoking rates as a result of government initiatives such as smoking bans, standardised packaging and advances in technology2-3. Such technological advancements include electronic nicotine delivery systems (ENDS), which are electronic devices that do not burn or use tobacco leaves but vaporise the content solution for the user to inhale4. The most common type of ENDS is the e-cigarette, which usually contains nicotine, propylene glycol sometimes with glycerol, and flavouring agents4. Though ENDS have been in existence since the 1930s, they became a commercial success in 20035, and were introduced to the United Kingdom around 20056.
In the UK, it has been suggested that the increase in e-cigarette use, especially by adults, is responsible for the reduction in traditional cigarette use7 because most adults use them as smoking cessation devices although they have not been licensed as such8. Furthermore, adults are being encouraged by health professionals to use e-cigarettes instead of traditional cigarettes as available scientific evidence has suggested there are less risks associated with e-cigarette use8-13. However, a recently updated meta-analysis of 27 studies, which reported a quantitative estimate of the association between e-cigarette use and smoking cessation with an appropriate control group, found the odds of quitting cigarettes were 28% lower in those who used e-cigarettes compared with those who did not (OR=0.73, 95% CI: 0.59–0.92). This conclusion did not significantly depend on differences in the study design14. This suggests that e-cigarettes may not be as helpful for quitting smoking as first thought.
Despite this, the use of e-cigarettes is becoming more acceptable worldwide, especially amongst smokers and ex-smokers15-17. E-cigarette use is also becoming increasingly popular among adolescents and young adults18-19. As a result, concerns are being raised by health professionals about e-cigarette use in the adolescent population20 as research from the USA suggests this trend is providing a window to adolescent traditional cigarette use and eventual nicotine addiction21-24. While early evidence of this association was cross-sectional in nature21 and therefore provided no evidence of a temporal relationship, more recent evidence is strengthened by systematic reviews with meta-analyses that include22 or are limited to24 longitudinal studies. Similar findings have also been revealed in qualitative research23.
The concept that drug use in weaker forms leads to stronger drug use rests at the centre of gateway theory25. Although widely debated, gateway theory has most recently been applied to the context of e-cigarettes25. Gateway effects are notoriously difficult to establish as studies need to be able to prove causality and may not be determined via observational studies that simply adjust for confounders26. Observational studies may, however, give an indication of an association between one drug and another.
In the USA, according to data released by the Centre for Disease Control and Prevention (CDC), the use of e-cigarettes almost doubled between 2010 and 2011 from 3.3% to 6.2% in the general population27. Moreover, the rate of e-cigarette use among middle and high school students increased alarmingly between 2017 and 2018 with a 78% increase in e-cigarette use among high school students (11.7% to 20.8%) and a 48% increase in e-cigarette use among middle school students (3.3% to 4.9%) between 2017 and 201828. In the UK, 6.2% of the adult population currently uses e-cigarettes alone or in combination with traditional cigarettes29. Additionally, an annual survey of e-cigarette use by Action on Smoking and Health (ASH) revealed a 4% increase in youth (aged 11–18 years) e-cigarette use in the UK from 7% to 11% between 2016 and 201730 while only 5% of adolescents aged 11–18 years said they had not heard of e-cigarettes18. It has also been identified that the pattern of adolescent nicotine product use is shifting towards e-cigarettes31-32, with the rate of adolescent experimentation (used at least once) with e-cigarettes at 22% overtaking adolescent traditional cigarette experimentation at 18% in 2014 in the UK33.
Public health concerns have been raised about the impact of e-cigarettes on adolescents due to increases in their use20,34 and concerns about their safety1,4,27,35. Despite a report claiming that e-cigarettes are 95% safer than traditional cigarettes10, a more recent study highlighted the tendency of e-cigarettes to damage cultured human DNA and reduce repair activities within lung and bladder cells when exposed to the equivalent of light e-cigarette use for 10 years36. While carcinogenic tobacco-specific nitrosamine levels in e-cigarette smokers are 97% lower than in tobacco smokers, nonetheless, it is significantly higher than in non-smokers36. Emissions from e-cigarettes can also contain chemicals that are considered toxic to the user when e-cigarettes are used regularly for longer than one month35. In the USA and some European countries, several studies have highlighted the potential damage that could result from the use of nicotine, such as brain damage37-38.
A number of studies have also reported an association between adolescent e-cigarette use and traditional cigarette smoking. For example, a systematic review and meta-analysis of longitudinal studies that assessed initial use of e-cigarettes and subsequent traditional cigarette smoking among adolescents and young adults (aged 14–30 years) by Soneji et al.24,39 showed strong and consistent evidence of an association between initial e-cigarette use and subsequent cigarette smoking initiation, however this review included studies only from the USA. Most recently in the UK, McNeil et al.11 addressed the issue of whether e-cigarette use contributed to the uptake of tobacco smoking in adolescents and concluded that e-cigarettes did not appear to be undermining the long-term decline in traditional cigarette smoking in the UK among young people. McNeil et al.11 suggested that the evidence needed constant review and that more research was needed, therefore the aim of our study was to systematically review the empirical evidence on whether adolescent e-cigarette use is associated with traditional cigarette smoking in the UK.
METHODS
This review aimed to investigate whether e-cigarette use is associated with traditional cigarette use in adolescents in the UK; it is reported according to the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) and registered with PROSPERO (CRD42018093019).
Search strategy
PICOS (Population, Intervention, Comparator, Outcome and Study) format was used to structure the search. Searches were made for peer reviewed empirical studies that focused on adolescent (males and females aged 10–19 years) e-cigarette use in the UK that also examined traditional smoking initiation or intention. Any study design was considered as there was no intervention or comparator. Studies were restricted to those written in English as translation services were not available. Studies were excluded if they were based outside the UK, were focussed on adults or very young children (<10 years old), or examined traditional cigarette use only. Editorials, opinion articles and systematic reviews were also excluded.
Study selection
PubMed, Medline via ProQuest, CINAHL with full text (Cumulative Index to Nursing and Allied Health), and Scopus were searched between January 2005 (when e-cigarettes became commercially available in the UK) and May 2018. Search terms were based on the concepts: adolescents, e-cigarettes, traditional cigarette smoking, and the UK (Supplementary file gives a search string example). All identified references were downloaded into Endnote citation management software where duplicate references were identified and removed. Initial study selection was carried out by the lead author (AA) and involved sifting title and abstract against the inclusion and exclusion criteria. In addition, the PubMed search (n=118) was also sifted by the second author (CH) and agreement compared using the Kappa coefficient. All full texts of selected studies were obtained and once again sifted by AA against the inclusion and exclusion criteria in order to determine the final studies for inclusion in the review. The first 10% of the second sift was checked by CH and any disagreement discussed and a decision agreed.
Quality assessment
The quality of all included studies was appraised using the most relevant CASP (Critical Appraisal Skill Programme) tool dependent on the study type40. A risk of bias assessment was carried out using ROBINS-I (Risk Of Bias In Non-randomised Studies of Interventions), which is appropriate for use with observational studies41. In order to assess risk of bias, the following confounding factors were considered important: demographic characteristics, socioeconomic status, family and friends smoking pattern, educational attainment, and other risk behaviours. Quality assessment and risk of bias was carried out by AA and checked by CH.
Data extraction
A detailed data extraction table was developed by adapting data extraction tables from similar studies22,24. Data were extracted under the following sub-headings: study year, source, participants (number of ever users of e-cigarettes), location, design, measures, adjusted variables, results and conclusion. Data extraction was carried out by AA with one full study checked by CH.
Data synthesis
A meta-analysis was carried out in RevMan V.5.3 from those included studies that were homogenous in terms of design and outcomes. The presence of heterogeneity was assessed statistically using chi-squared and the extent of heterogeneity using I2. A narrative synthesis was carried out on those studies that were not suitable for inclusion in the meta-analysis.
RESULTS
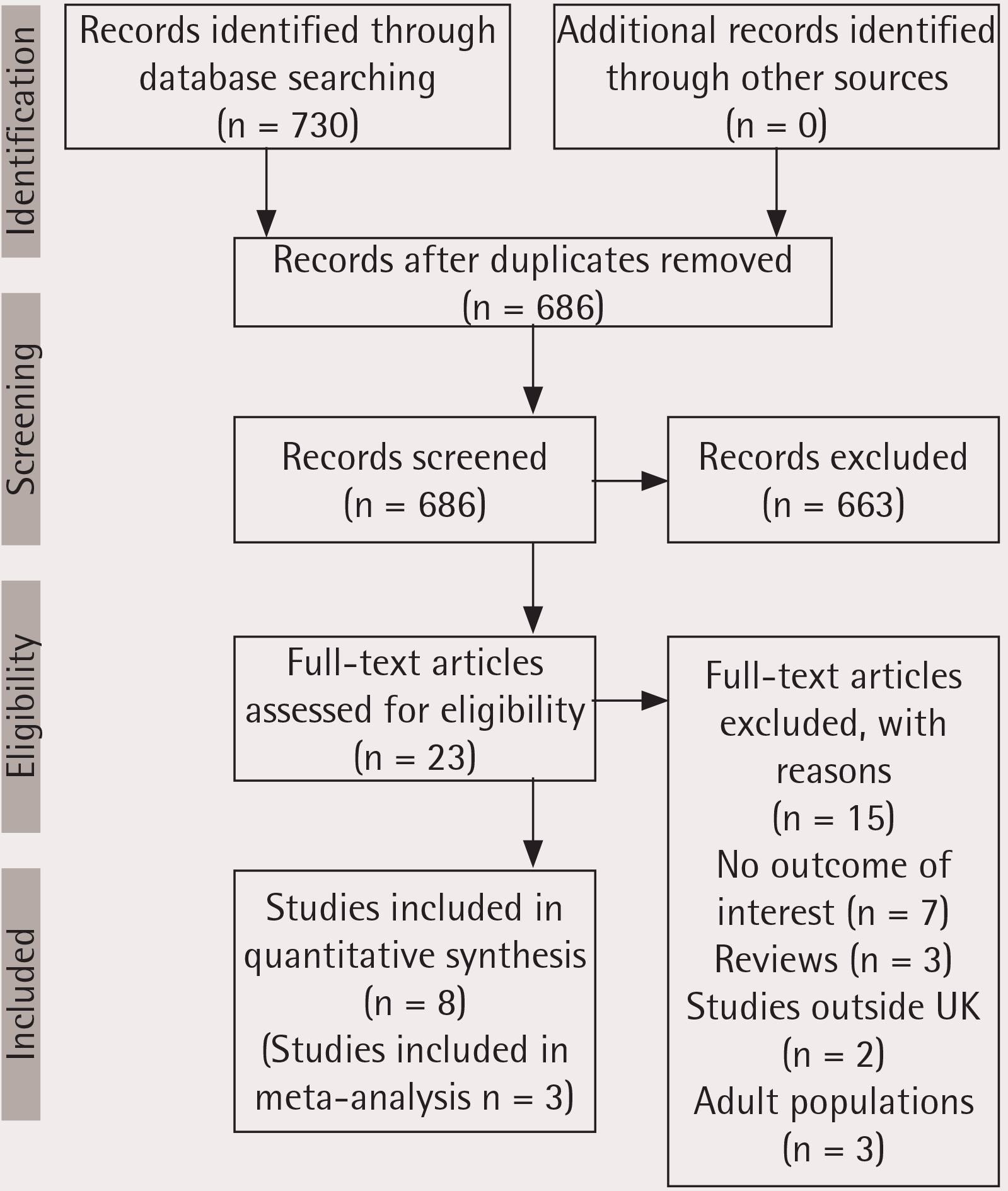
A total of 730 studies was generated from all the searched databases (CINAHL=110, Medline=368, PubMed=118 and Scopus=134). Fourty-four duplicate studies were removed, and 686 studies was screened for inclusion or exclusion through examining the titles and abstracts using the stated criteria. Overall, 663 studies was excluded and 23 studies were eligible for full text screening. Fifteen studies were exluded after full text screening and eight studies were included in this review (Figure 1). Using parameters from the CASP tool for cohort studies, the included studies were generally of good quality (Table 1) while risk of bias was mainly low (Table 2). Over all of the eight included studies20,42-48 there were a total of 73076 adolescents aged 10–19 years (Table 3). Five of the studies used a cross-sectional survey design20,45-48 while three42-44 were longitudinal (prospective) designs and were able to be included in a meta-analysis.
Table 1
Quality appraisal: using parameters from CASP (critical appraisal skill programme) tool for cohort studies
| Study/Study Characteristics | Best et al.422017 | Conner et al.432017 | East et al.442017 | Eastwood et al.472015 | Moore et al.452014 | Moore et al.462015 | de Lacy et al.202017 | Hughes et al.482015 |
|---|---|---|---|---|---|---|---|---|
| 1. Did the study address a clearly focused issue? | Y | Y | Y | Y | Y | Y | Y | Y |
| 2. Was the cohort recruited in an acceptable way? | Y | Y | Y | Y | Y | Y | Y | Y |
| 3. Was the exposure accurately measured to minimise bias? | Cannot tell | Y | Cannot tell | Cannot tell | Cannot tell | Cannot tell | Cannot tell | Cannot tell |
| 4. Was the outcome accurately measured to minimise bias? | Cannot tell | Y | Cannot tell | Cannot tell | Cannot tell | Cannot tell | Cannot tell | Cannot tell |
| 5. a. Have the authors identified all important confounding factors? | N | N | N | N | N | N | N | N |
| 6. b. Was confounding factors considered in the design and/or analysis? | Y | Y | Y | Y | Y | Cannot tell | Y | Y |
| 7. Was the follow up of subjects complete enough? | Y | N | N | N/A | N/A | N/A | N/A | N/A |
| 8. Was the follow up of subjects long enough? | Y | Y | N | N/A | N/A | N/A | N/A | N/A |
| 9. What are the results of this study? | See Table 1 | See Table 1 | See Table 1 | See Table 1 | See Table 1 | See Table 1 | See Table 1 | See Table 1 |
| 10. Was the result precise? | Y | Y | Y | Y | Y | Y | Y | Y |
| 11. Do you believe the results? | Y | Y | Y | Y | Y | Y | Y | Y |
| 12. Can the results be applied to the local population? | Y | Y | Y | Cannot tell | Y | Y | Y | Y |
| 13. Do the results of this study fit with other available evidence? | Y | Y | Y | Y | Y | Y | Y | Y |
| 14. Does this have implication for practice? | Y | Y | Y | Y | Y | Y | Y | Y |
Table 2
Risk of bias using parameters from ROBIN-I
| Studies/Questions | Best et al.42 2017 | East et al.44 2017 | Conner et al.43 2017 | de Lacy et al.20 2017 | Moore et al.45 2014 | Hughes et al.48 2015 | Eastwood et al.47 2015 | Moore et al.46 2015 |
|---|---|---|---|---|---|---|---|---|
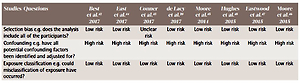
| Selection bias e.g. does the analysis include all of the participants? | Low risk | Low risk | Unclear risk | Low risk | Low risk | Low risk | Low risk | Low risk |
| Confounding e.g. have all potential confounding factors been identified and adjusted for? | High risk | High risk | High risk | High risk | High risk | High risk | High risk | High risk |
| Exposure classification e.g. could misclassification of exposure have occurred? | Low risk | Low risk | Low risk | Low risk | Low risk | Low risk | Low risk | Low risk |
| Performance bias e.g. were there systemic differences between groups? | Low risk | Low risk | Low risk | Low risk | Low risk | Low risk | Low risk | Low risk |
| Data attrition e.g. is follow up data missing? | Low risk | High risk | High risk | N/A | N/A | N/A | N/A | N/A |
| Outcome measurement e.g. could bias have been introduced via method of measurement of outcome measures? | Unclear risk | Unclear risk | Low risk | Unclear risk | Unclear risk | Unclear risk | Unclear risk | Unclear risk |
| Reporting bias e.g. was there selective reporting of results? | Unclear risk | Unclear risk | Unclear risk | Unclear risk | Unclear risk | Unclear risk | Unclear risk | Unclear risk |
Table 3
Characteristics of included studies
| Study | Location, setting and study | Population | Outcome measures | Design | Adjusted variable | Results | Conclusions |
|---|---|---|---|---|---|---|---|
| Best et al.42 2017 | UK (Scotland) Determining the Impact of Smoking Point-of-Sale Legislation Among Youth (DISPLAY) study. | 3807 high school students (aged 11–18 years). | Smoking status, e-cigarette use, susceptibility to smoking, family and friends smoking pattern and demographic characteristics. | Longitudinal (prospective) survey. | Demographic characteristic, deprivation, family and friends smoking pattern. | At baseline, 183 of 2125 (8.6%) never smokers had tried an e-cigarette. Of the young people who had not tried an e-cigarette at baseline, 249 (12.8%) went on to try smoking a cigarette by follow-up compared with 74 (40.4%) of those who had tried an e-cigarette at baseline (OR=4.62, 95% Cl: 3.34–6.38). This effect remained significant in a logistic regression model adjusted for smoking susceptibility, having friends who smoke, family members’ smoking status, age, sex, family affluence score, ethnic group and school (adjusted OR=2.42, 95% CI: 1.63–3.60). | Compared to non-smokers who had not tried e-cigarettes, young people who had tried e-cigarettes had greater odds of smoking traditional cigarette at follow-up. There was a significant interaction between e-cigarette use and smoking susceptibility and between e-cigarette use and smoking within the friendship group. |
| East et al.44 2017 | UK Action on Smoking and Health Great Britain Youth longitudinal survey 2016 | 1152 adolescents (aged 11–18 years). | Smoking and e-cigarette use pattern, smoking susceptibility and family and friend’s pattern of smoking. | Longitudinal (prospective) survey. | Age, parental smoking pattern, peers smoking. | At baseline, 19.8% were ever smokers and 11.4% were ever e-cigarette users. Respondents who were ever e-cigarette users vs. never users (53% vs 8%, OR=11.89, 95% CI: 3.56–39.72) and escalated their e-cigarette use vs did not (41% vs 8%, OR=7.89, 95% CI: 3.06–20.38) were more likely to initiate smoking. Respondents who were ever smokers vs never smokers (32% vs 4%, OR=3.54, 95% CI: 1.68–7.45) and escalated their smoking vs did not (34% vs 6%, OR=5.79, 95% CI: 2.55–13.15) were more likely to initiate e-cigarette use. There was a direct effect of ever e-cigarette use on smoking initiation (OR=1.34, 95% CI: 1.05–1.72) and ever smoking on e-cigarette initiation (OR=1.08, 95% CI: 1.01–1.17); e-cigarette and smoking escalation, respectively, did not mediate these effects. | E-cigarette use was associated with smoking initiation and vice-versa at follow-up. |
| Conner et al.43 2017 | UK (England) Do electronic cigarettes increase cigarette smoking in UK adolescent? 12-months prospective study. | 2836 adolescents (aged 13–14 years) in 20 English schools. | Breath carbon monoxide levels, self-reported e-cigarette and traditional cigarette use, sex, age, friends and family smoking, beliefs about cigarette use and percentage receiving free school meals at baseline. Self-reported cigarette use validated by breath carbon monoxide levels at 12 months follow-up. | Longitudinal (prospective) survey. | Family smoking, peers smoking, smoking habit and e-cigarette use habit, socio-economic status (based on free school meal status). | At baseline, 34.2% of adolescents reported ever using e-cigarettes (16% used only e-cigarettes). Baseline ever use of e-cigarettes was strongly associated with subsequent initiation (n=1726; OR=5.38, 95% Cl: 4.02–7.22). Controlling for covariates (OR=4.06, 95% Cl: 2.94–5.60). Escalation (n=318; OR=1.91, 95% Cl: 1.14–3.21) controlling for covariates, this effect of escalation became non-significant (OR=1.39, 95% Cl: 0.97–1.82). | Ever use of e-cigarettes was robustly associated with initiation but modestly related to escalation of cigarette use. |
| de Lacy et al.20 2017 | UK (Wales) 2013/2014 Welsh health behaviour in school-aged children (HBSC) survey. | 32479 students (aged 11–16 years) in 87 Welsh secondary schools. | Use of e-cigarettes and novel psychoactive substances. Frequency of smoking and sequencing of e-cigarette or tobacco use. Family Affluence Scale (FAS). | Cross–sectional survey. | Family Affluence Scale (FAS), smoking status, other substance use and frequency of substance use. | 18.5 % students reported ever using e-cigarettes compared to 10.5% smoking tobacco. 41.8% of daily smokers reported being regular e-cigarette users. Regular e-cigarette use was more prevalent among current cannabis users (relative risk ratio, RRR=41.82, 95% CI: 33.48–52.25), binge drinkers (RRR=47.88, 95% CI: 35.77–64.11), users of mephedrone (RRR=32.38, 95% CI: 23.05–45.52) and laughing gas users (RRR=3.71, 95% CI: 3.04–4.51). Multivariate analysis combining demographics and smoking status showed that only gender (being male) and tobacco use independently predicted regular use of e-cigarettes (p<0.001). Among weekly smokers who had tried tobacco and e-cigarettes (n=877), the vast majority reported that they tried tobacco before using an e-cigarette (n=727; 82.9%). | Experimentation with e-cigarettes has grown. Regular use has almost doubled, and is increasing among never and non-smokers. No evidence of e-cigarettes as a pathway into smoking. |
| Moore et al.45 2014 | UK (Wales) 2014 Child exposure to Environmental Tobacco Smoke (CHETS) 2. | 1500 Children (aged 10–11 years). | E-cigarette use, parental and peer smoking, intentions to smoke tobacco within the next 2 years. Family Affluence Scale (FAS). | Cross-sectional survey. | Parents smoke/use e-cigarettes, friends smoking, sex, Family Affluence Scale (FAS). | Children were most likely to have used an e-cigarette if parents used both tobacco and e-cigarettes (OR=3.40, 95% CI: 1.73–6.69). Having used an e-cigarette was associated with intentions to smoke (OR=3.21, 95% CI: 1.66–6.23). While few children reported that they would smoke in 2 years’ time, children who had used an e-cigarette were less likely to report that they definitely would not smoke tobacco in 2 years’ time and were more likely to say that they might. | Findings are consistent with a hypothesis that children use e-cigarettes to imitate parental and peer smoking behaviours, and that e-cigarette use is associated with weaker antismoking intentions. |
| Hughes et al.48 2015 | UK (North West England). 5th Iteration of the Trading Standards North West Alcohol and Tobacco Survey. | 18233 students (aged 14–17 years) in 114 schools. | Demographic characteristics, deprivation, smoking behaviour, alcohol and tobacco access methods, parental smoking, involvement in violence when drunk. The question on e-cigarette access asked participants “have you ever tried or purchased e-cigarettes” | Cross-sectional survey. | Socio-demographic, smoking and drinking behaviour. | One in five participants reported having accessed e-cigarettes (19.2%). Prevalence was highest among smokers (rising to 75.8% in those smoking >5 per day), although 15.8% of teenagers that had accessed e-cigarettes had never smoked traditional cigarettes (v.13.6% being ex-smokers). E-cigarette access was independently associated with male gender, having parents/guardians that smoke and students’ alcohol use. Compared with non-drinkers, teenagers that drank alcohol at least weekly and binge drank were more likely to have accessed e-cigarettes (adjusted OR=1.89, p<0.001), with this association particularly strong among never-smokers (adjusted OR=4.59, p<0.001). | Findings suggest that e-cigarettes are being accessed by teenagers more for experimentation than smoking cessation. |
| Eastwood et al.47 2015 | UK. A national survey by YouGov PLC, commissioned by Action against smoking (ASH) | 2062 participants (2013) and 1952 participants (2014) (aged: 11–18 years). | Traditional cigarette and e-cigarette use, frequency of use, combined use and which was initiated first. | Cross-sectional survey (two waves). | Age, smoking status, and e-cigarette use. | Ever-use of e-cigarettes increased significantly from 4.6% (95% CI: 3.8–5.7) in 2013 to 8.2% (95% CI: 7.0–9.6) in 2014. The proportion of young people who perceived e-cigarettes to be less harmful to users than cigarettes fell from 73.4% (95% CI: 71.0–75.8) to 66.9% (95% CI: 64.5–69.2). The proportion who considered e-cigarettes to cause similar levels of harm increased from 11.8% (95% CI: 10.0–13.5) to 18.2% (95% CI: 16.3–20.1). Of the 8.2% of e-cigarette ever-users in 2014, 69.8% (95% CI: 62.2–77.3) had smoked a cigarette prior to using an e-cigarette, while 8.2% (95% CI: 4.1–12.2) first smoked a cigarette after e-cigarette use. | Increase use of e-cigarette was mainly confined to the smoking adolescent population. |
| Moore et al.46 2015 | UK (Wales) 2014 Welsh Health Behaviour in School-aged Children survey (HSBC WALES) | 9055 participants (aged 11–16 years) from 82 secondary schools. | Cigarette smoking and e-cigarette smoking patterns, demographic characteristics, Family Affluence Scale (FAS) | Cross-sectional survey. | Gender, cannabis use, pattern of e-cigarette and cigarette smoking, Family Affluence Scale (FAS) | Almost half of those who had tried smoking had tried an e-cigarette. 42.8% of young people who had used e-cigarettes reported that they had never smoked tobacco. Regular e-cigarette use was more likely among those who had smoked tobacco, both in terms of relative risk ratio (66.30) and absolute values, with 80% of regular e-cigarette users reporting having also smoked tobacco. Current smoking was also strongly associated with e-cigarette use: Relative risk ratios for regular e-cigarette use among young people smoking weekly (RRR=121.15, 95% CI 57.56–254.97) or daily (115.38, 95% CI: 70.09–189.91). 72.1% of young people who had used an e-cigarette a few times, and 43.2% of regular e-cigarette users, were from the larger group of young people who were not current smokers (hence while current smoking is associated with a greater relative risk of e-cigarette use, most young people who have used an e-cigarette are not smokers). | Current cigarette smokers are more likely to smoke e-cigarette. |
Smoking initiation
Smoking initiation was assumed to be the best evidence of an association with e-cigarette use that could be generated from observational studies with short-term follow-up periods. Smoking initiation does not mean regular use, however it can be taken as a potential starting point that could easily progress to regular use of a substance49. Three longitudinal studies42-44 examined traditional smoking initiation in adolescent e-cigarette users compared to adolescents who had never used e-cigarettes.
Best et al.42 examined whether young never smokers who had tried an e-cigarette were more likely than those who had not tried an e-cigarette to have initiated traditional cigarette smoking by the following year. The study reported that young e-cigarette users had more than four times greater odds of initiating traditional smoking by the following year (OR=4.62, 95% Cl: 3.34–6.38) (Adjusted OR=2.42, 95% CI: 1.63–3.60). Conner et al.43 carried out a longitudinal study that investigated whether adolescent e-cigarette use was prospectively associated with initiation of traditional cigarette use. Baseline ever use of e-cigarettes was strongly associated with subsequent initiation of traditional cigarettes (OR=5.38, 95% Cl: 4.02–7.22) (Adjusted OR=4.06, 95% CI: 2.94–5.60). East et al.44 examined whether ever use of e-cigarettes by adolescents was associated with traditional cigarette initiation at follow-up. The odds of smoking initiation in ever users of e-cigarettes were significantly high (OR=12.31, 95% Cl: 5.06–29.94) (Adjusted OR=10.57, 95% CI: 3.33–33.50).
As the presence of heterogeneity (χ2=4.15), extent of heterogeneity (I2=52%) and risk of bias were relatively low, these studies were able to be included in a meta-analysis using a random effect model (Figure 2). The meta-analysis showed that the odds of smoking traditional cigarettes were increased up to six times in non-smoking adolescents who used e-cigarettes (OR=5.55, 95% Cl: 3.94–7.82).

This meta-analysis was based on number of events and therefore on unadjusted odds ratios. As the included studies were susceptible to confounding, we also performed a generic inverse variance meta-analysis based on unadjusted odds ratios (Figure 3). This meta-analysis also showed the odds of smoking traditional cigarettes were increased in non-smoking adolescents who used e-cigarettes (OR=26.01, 95% CI: 5.35–126.44).

Intent to smoke
Liberal attitudes towards smoking, or perceiving the risks associated with smoking as low, may indicate future susceptibility to smoking50. Although this may not necessarily lead to smoking, individuals who perceive low risk from a habit are more likely to engage in it50. Three studies42-43,45, two longitudinal42-43 and one cross-sectional45 reported increased intent to smoke or permissive attitude towards smoking associated with e-cigarette use. Conner et al.43 observed that ever use of e-cigarettes at baseline was statistically significant in predicting weakening smoking intentions (OR=0.7, 95% Cl: 0.52–0.96) and attitudes (OR=0.68, 95% Cl: 0.44–1.04). Participants with strong negative attitudes and intentions against smoking were less likely to initiate smoking at follow-up.
Moore et al.45 investigated the association between e-cigarette use in adolescents and their future intentions to smoke traditional cigarettes. The findings demonstrated a statistically significant increased willingness to smoke in the future in participants that had used e-cigarettes compared to those that had not (OR=3.21, 95% Cl: 1.66–6.23). Best et al.42 reported that susceptibility to smoking traditional cigarettes at follow-up was able to be predicted by e-cigarette use. However, the highest impact of e-cigarette use was observed in adolescents who expressed low susceptibility to smoking at baseline but had eventually used traditional cigarettes at follow-up (χ2=53.93, p<0.001).
Combined use of electronic and traditional cigarettes
Evidence of this nature simply shows that people who use e-cigarettes are likely to smoke or people who smoke are likely to use e-cigarettes. More so, it shows that using one of the products could reinforce the use of the other. Four cross-sectional studies20,46-48 found that in adolescents who have ever used e-cigarettes, current regular smokers were more likely to use e-cigarettes than other groups such as light smokers or ex-smokers showing an association of use. Furthermore, in longitudinal studies East et al.44 found that there was as much of a significant likelihood for an adolescent smoker to initiate e-cigarrete use as an adolescent e-cigarette user to initiate traditional smoking (OR=3.54, 95% CI: 1.68–7.45). In addition, East et al.44 and Conner et al.43 found that there was an increase in use of one of either e-cigarettes or traditional cigarettes when the alternate product was initiated, although Conner et al.43 found this became non-significant when covariates (socioeconomic status, sex, age, family smoking, friends’ smoking) were controlled for.
Reviewer agreement
Agreement between reviewers was compared using the Kappa coefficient, which was 0.936. This showed very good agreement, with an observed agreement of 99.15% (Tables 4a and 4b).
DISCUSSION
Summary of findings
Our meta-analysis, including three longitudinal (prospective) studies, showed that the odds of smoking traditional cigarettes were increased up to six times in non-smoking adolescents who used e-cigarettes in the UK. Longitudinal studies also reported an increase in use of one of either e-cigarettes or traditional cigarettes when the alternate product was initiated The remaining included studies employed cross-sectional surveys and therefore were only able to show an association between e-cigarette use and traditional cigarette smoking in British adolescents.
Comparison to the literature
Findings from this review corroborate results from Zhong et al.22 and Soneji et al.24,39 who also carried out systematic reviews on whether adolescent e-cigarette use was associated with traditional cigarette smoking. Soneji et al.24,39 showed strong and consistent evidence of an association between initial e-cigarette use and subsequent cigarette smoking initiation, while Zhong et al.22 reported e-cigarette use was associated with increased smoking intention. However, studies included in the Zhong et al.22 and the Soneji et al.24 reviews were predominatly from the USA while our review is set within the unique context and policies of the UK. In addition, the review by Zhong et al.22 focused on the influence of e-cigarette use on intent to smoke traditional cigarettes and Soneji et al.24 focused on initiation of traditional cigarette smoking while our review accomodated both. Hammond et al.17 also found similar results in their longitudinal study of electronic cigarette use and smoking initiation among youths (secondary school students in grades 9–12) in Canada. They concluded that past 30-day use of e-cigarettes at baseline was associated with initiation of smoking a traditional cigarette (adjusted OR=2.12, 95% CI: 1.68–2.66) and with initiation of daily smoking (adjusted OR=1.79, 95% CI: 1.41–2.28) at follow-up.
Limitations and strengths
This is the first systematic review to examine whether adolescent e-cigarette use is associated with smoking in the UK. The quality appraisal process and risk of bias revealed studies to be mainly of good quality and results from three studies were able to be combined in a meta-analysis, however there are some limitations to this review. Firstly, only three of the included studies were longitudinal in nature and were able to be combined in a meta-analysis. Given that the remainder of the included studies were cross-sectional, it cannot be concluded with certainty whether the association between e-cigarette use and traditional cigarette smoking initiation is causal or not, and as such, more longitudinal (prospective) studies are warranted. Secondly, only published peer-reviewed studies were included with the aim of identifying evidence of high quality, however it must be acknowldged that this could introduce publication bias. Furthermore, included studies are, in the main, reliant on self-reported data and limited length of follow-up. Finally, included studies were limited to those written in English so while there is potential that important studies could have been overlooked this is unlikely given the context of this review was the UK.
CONCLUSIONS
While emerging results from this review and similar studies from other countries are beginning to provide evidence regarding the association between e-cigarette and traditional cigarette use, public health policy makers in the UK still need clear conclusions about the effects and safety of e-cigarettes. In a recent qualitative study of GPs’ and nurses’ perceptions of electronic cigarettes in England, many practitioners reported uncertainties about the safety and long-term risks of e-cigarettes51. Health professionals wanted advice from healthcare regulators such as the National Institute for Health and Care Excellence to reassure them about the safety of e-cigarettes51.
To enhance clarity in future research studies, there is a need for standardised parameters for outcome measures when collecting data on smoking and e-cigarette use. The standardised parameters for outcome measures should address issues such as clear definition of regular use, past 30 days use and discrepancies in assessing binge smokers. Moreover, longitundinal study designs with longer follow-up periods should be used to research further the extent to which experimentation leads to continuous use.