Introduction
Anterior cruciate ligament (ACL) injuries are common among adolescent athletes.1 Surgical reconstruction of the ACL is recommended for athletes who intend to return to sport.2 Unfortunately, the risk of sustaining another ACL injury is high among adolescent athletes.3 In fact, it has been reported that approximately 25% of adolescent athletes will suffer a second ACL injury in the first year after they return to sport following ACL reconstruction.4 These alarmingly poor outcomes highlight the urgent need to improve rehabilitation and return-to-sport decision making after ACL reconstruction.
Athletes who have undergone ACL reconstruction often demonstrate marked inter-limb asymmetries in impact forces during landing, even after they have returned to sport.5–10 This persistent asymmetry in limb loading may contribute to the relatively high incidence of ACL injuries in athletes who return to sport following ACL reconstruction.11 The typical pattern of asymmetry involves athletes landing with greater loads on their uninvolved limb, vs. their limb that underwent ACL reconstruction.12 This apparent shift in loading away from the ACL-reconstructed limb could help to explain why ACL injuries are common for the previously uninjured limb in adolescent athletes following return to sport,12 as higher impact forces during landing correspond with greater ACL loading13,14 and appear to be a risk factor for primary ACL injury.15,16
Considering that athletes often demonstrate persistent inter-limb asymmetries in impact forces, and the potential relevance of these kinetic asymmetries to their risk of a second ACL injury, it seems likely that information regarding inter-limb impact force symmetry would be of value to sports medicine professionals involved in post-operative rehabilitation and return-to-sport decision making.7,12,17,18 Unfortunately, information of this nature is typically not available to clinicians, as the force plate technology required to record ground reaction forces has traditionally been confined to a laboratory setting. However, the development of portable force plate systems that are more conducive to testing outside of a laboratory, may provide opportunities to begin to assess inter-limb kinetic symmetry throughout rehabilitation in order to guide treatment and return-to-sport decision making.
While advances in technology create opportunities to enhance post-operative rehabilitation and return-to-sport testing, there is still the challenge of determining if an athlete has returned to a ‘normal’ level of inter-limb kinetic symmetry, since some degree of inter-limb asymmetry is typically observed, even in uninjured athletes.19,20 This makes it difficult to determine if the asymmetry exhibited by an athlete who has undergone ACL reconstruction is excessive or within a range that is similar to uninjured athletes. The purpose of this study was to establish normative values for inter-limb impact force symmetry in uninjured adolescent athletes. An example is also provided of how a clinical team could use these normative values to identify athletes who exhibit atypically high levels of asymmetry following ACL reconstruction.
Methods
One hundred thirty-six (86 males, 50 females) uninjured competitive adolescent athletes and 11 competitive adolescent athletes (6 males, 5 females) who had recently undergone ACL reconstruction (ACLR group) participated in this cross-sectional study. The uninjured athletes’ data were used to establish normative values, while the data from the athletes who had undergone ACL reconstruction were used to provide an example of how a clinical team could use these normative values to identify athletes who exhibit an atypically high level of asymmetry. All athletes were between 14-18 years of age and competed at the high school level. Athletes in the uninjured group needed to have competed in sports that involve frequent landing, jumping, and cutting within the prior year and not have a history of significant lower extremity injury or surgery, or an injury in the previous six months that limited their ability to train or compete. Athletes in the ACLR group needed to have undergone successful unilateral ACL reconstruction within the previous 18 months, completed conventional post-operative rehabilitation, and been cleared to resume landing and jumping activities. Athletes were excluded from the ACLR group if they had a history of significant injury in their uninvolved limb. The ACLR group’s data was collected at the time of their return-to-sport testing session. The median number of days since their ACL reconstruction at the time of testing was 191 days (range: 162 to 237 days), which appears to be consistent with the typical timing of return-to-sport testing.21 Ten athletes in the ACLR group had received bone-patellar tendon-bone autografts, while one had received a hamstrings tendon autograft. Six athletes in the ACLR group had suffered a concomitant injury to their meniscus, while five sustained isolated ACL injuries. The athletes in the uninjured and ACLR groups competed in basketball, football, rugby, soccer, tennis, and/or volleyball. Table 1 includes demographic information for the athletes. All athletes provided informed consent or assent prior to enrollment, and a parent or guardian provided consent for athletes younger than 18 years of age. This study was approved by the Lutheran Hospital Institutional Review Board.
All athletes completed the same testing protocol. After a standardized warm-up, athletes performed drop vertical jumps (DVJs) and countermovement jumps (CMJs) while two adjacent portable force plates simultaneously recorded three-dimensional ground reaction forces at 600 Hz (AccuPower, Advanced Mechanical Technology, Inc., Watertown, MA, USA). These force plates are designed for testing outside of the laboratory setting.22 For the DVJ task, the athletes dropped from a 31 cm high plyometric box, landed with their feet on separate force plates (initial landing), immediately performed a maximal vertical jump, and landed again.15 For the CMJ task, the athletes performed a quick squat (countermovement), followed by a maximal vertical jump, and then landed with their feet on separate force plates.23 Foot position was monitored visually by an investigator during testing and trials were re-collected if an athlete’s feet did not appear to contact separate force plates. Athletes were encouraged to focus on jumping as high as possible during performance of the tasks. Arm movement was not restricted for either task. The DVJ and CMJ tasks were analyzed because they are both commonly used for ACL injury risk screening15,16,24 and to evaluate inter-limb symmetry in athletes post-ACLR.9,10,23 Athletes performed four trials for each task; however, only the final three trials were analyzed.9,10,15,23 The first trial was included to allow athletes to become accustomed to the tasks and/or be cued to correct their technique. The order of the DVJ and CMJ tasks was randomized. Athletes were given a 10 second rest period between trials. Athletes wore their own footwear and athletic apparel during testing.
The ground reaction force data from each force plate were filtered using a 4th order, zero lag, recursive Butterworth filter with a cutoff frequency of 50 Hz.25 Peak vertical ground reaction forces (‘impact forces’) were identified from each force plate during the initial landing phase. The initial landing phase was defined as the initial 150 ms after athletes contacted each respective force plate during landing. Initial contact was defined as the frame where the vertical ground reaction force first exceeded a threshold of 10 N. Inter-limb impact force symmetry was captured for each trial via a symmetry index (SI),23 which was calculated by finding the absolute percent difference in impact forces between the limbs using Equation 1, where Xright represents the impact force from the force plate contacted by the right foot and Xleft represents the impact force from the force plate contacted by the left foot.
SI (%)=100∗ |Xright − Xleft|0.5∗(Xright+Xleft)
Since this SI captures the absolute difference between the limbs, a value of 0% reflects perfect symmetry in limb loading, while higher values correspond with greater inter-limb asymmetry.25 Although this SI does not provide information about the direction of asymmetry (i.e. which limb is being loaded more during a trial), the absolute differences between the limbs were analyzed to prevent positive and negative SI values from canceling each other out when averaged. All preliminary data processing was completed via a custom MATLAB script (The MathWorks Inc., Natick, MA, USA).
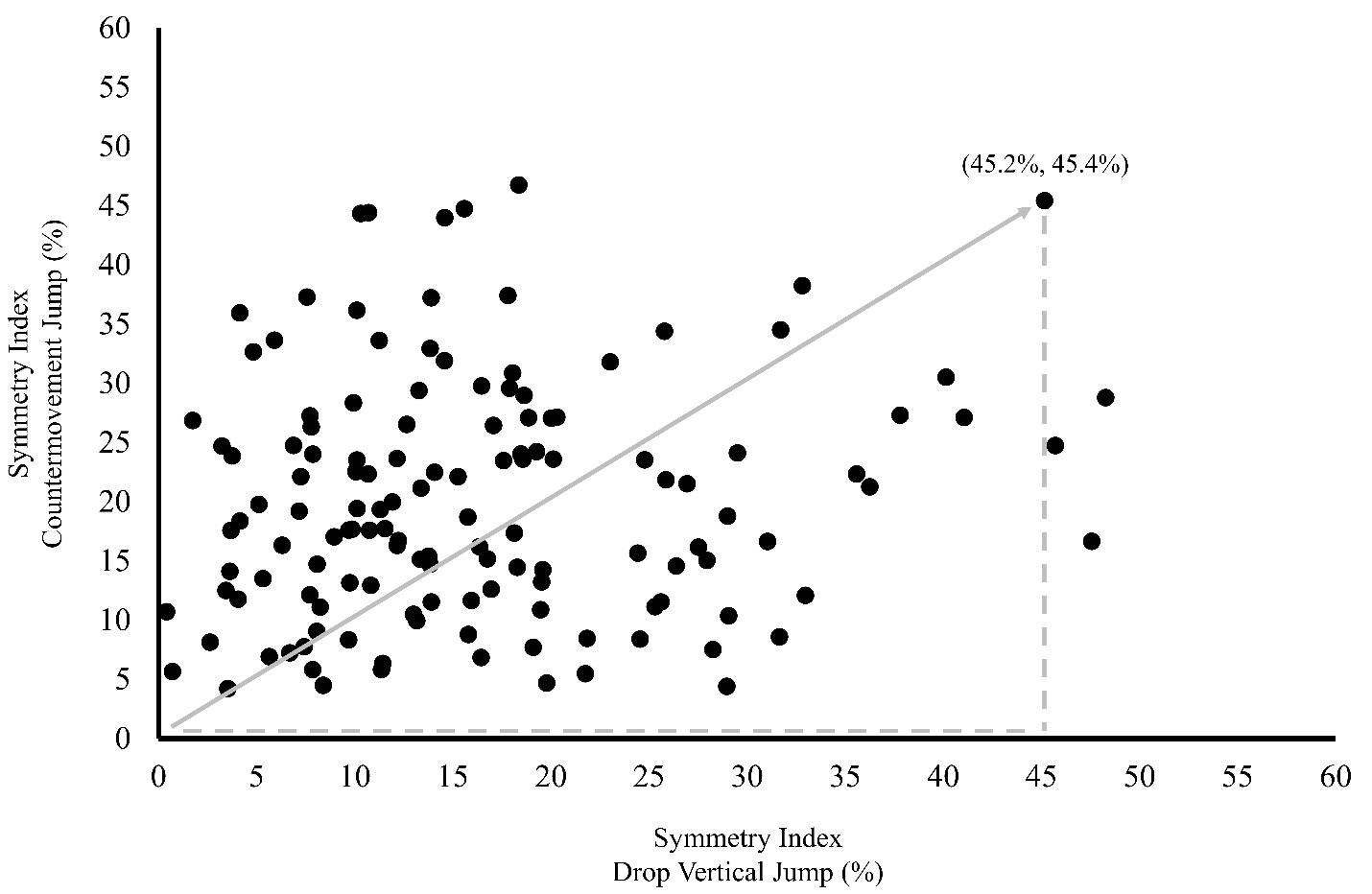
The three-trial average of the SIs from the DVJ task and CMJ task were calculated for each athlete. While the primary objective of this study was to establish normative values for the individual tasks, the SI values were also combined into a novel metric that captures inter-limb symmetry across both tasks. To create this metric, the SI values from the DVJ task (SIDVJ) and CMJ task (SICMJ) were plotted onto a plane where the origin represented perfect inter-limb symmetry for both tasks (0%, 0%), the SIDVJ values were on the horizontal axis, and the SICMJ values were on the vertical axis. For each point on the coordinate system, the resultant vector from the origin was calculated using Equation 2 (Figure 1). This vector (SIDVJ+CMJ) reflects the combined degree of asymmetry across both tasks.
SIDVJ+CMJ (%)= √SI2DVJ+ SI2CMJ

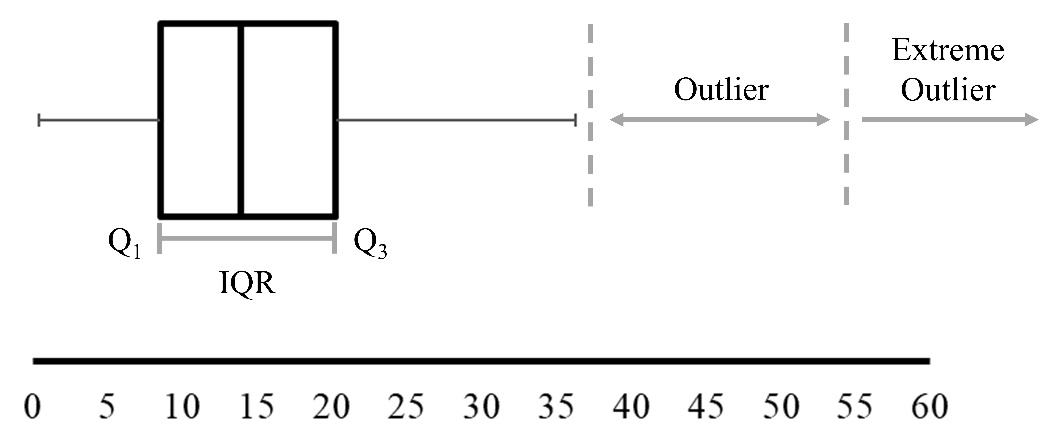
Normative values were established for the SIDVJ, SICMJ, and SIDVJ+CMJ variables. For each SI, the mean, standard deviation, minimum value, first quartile (Q1), median, third quartile (Q3), maximum value, 50th percentile, 75th percentile, 85th percentile, and 95th percentile were calculated/identified. In addition, threshold values (‘fences’) were established based on the inter-quartile range (IQR) for each of the distributions in order to identify SI values that would be considered ‘outliers’ (Equation 3) and ‘extreme outliers’ (Equation 4) in the distribution of observations for the uninjured athletes.
Outlier (%)= Q3+1.5 ×IQR
Extreme Outlier (%)= Q3+3 ×IQR
This approach is commonly used to identify outliers in a distribution26 and can help to determine the threshold values that reflect mildly atypical (outlier) and extremely atypical (extreme outlier) performance (Figure 2). Data analysis was performed using R software (The R Foundation, Vienna, AUT).

A secondary objective of this study was to provide an example of how these normative values could be used to identify athletes who exhibit atypically high levels of inter-limb asymmetry following ACL reconstruction. When examining inter-limb impact force symmetry in injured athletes, an initial screening can be conducted to determine if an athlete exhibits asymmetry that exceeds what is typically observed in uninjured athletes. Then each trial can explored in order to determine if there is a consistent pattern to the asymmetry (i.e. an athlete consistently placing greater load on a specific limb vs. more random trial-to-trial variation in the limb experiencing greater loading). This information can then be shared among the members of a clinical team (physical therapist, strength and conditioning specialist, surgeon) so that they can consider it when making rehabilitation and return-to-sport decisions. For this study, the SIDVJ+CMJ values for the athletes in the ACLR group were initially examined to determine where they fell within the distribution of SI values based on the uninjured athletes’ data. Athletes in the ACLR group who exceeded the 75th percentile were considered to be exhibiting atypically high levels of inter-limb asymmetry. For the athletes identified as ‘atypical’, the impact forces for the uninvolved and ACL-reconstructed limbs were examined for each trial in order to determine which limb was being loaded more during the landings, since the SI values are absolute values and only reflect the magnitude of asymmetry. It should be noted that clinicians could certainly use different cutoff points to identify athletes who exhibit varying levels of asymmetry. For instance, the 85th percentile could be used as the cutoff for identifying athletes exhibiting atypically high levels of asymmetry, instead of the 75th percentile. Using the 85th percentile would essentially result in a less stringent cutoff, where fewer athletes are essentially ‘flagged’ as exhibiting atypically high levels of asymmetry.
Results
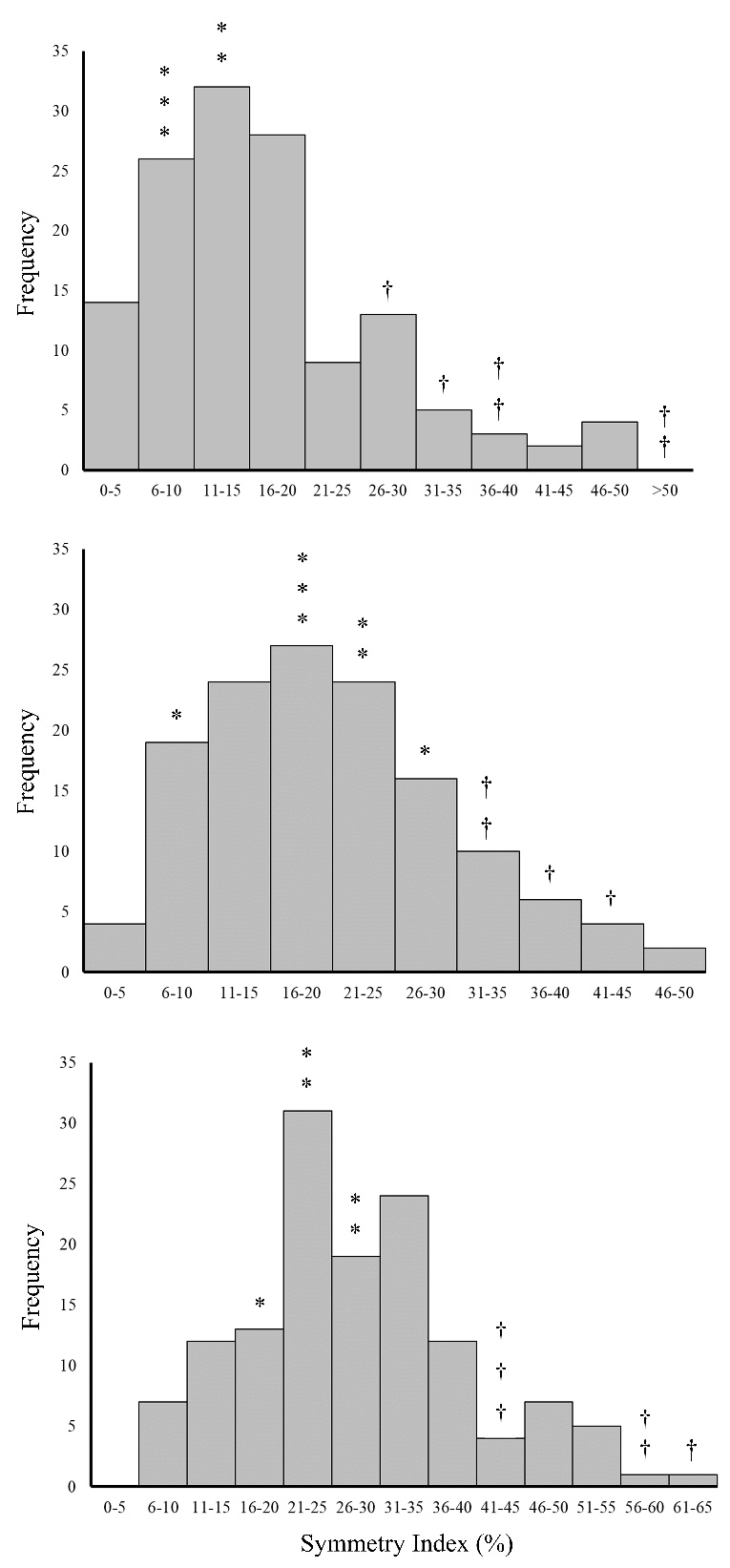
Table 2 includes descriptive statistics and Table 3 includes percentiles and thresholds for the outliers and extreme outliers for each of the symmetry indices. Figure 3 includes histograms for each of the symmetry indices. For the uninjured athletes, the means (± standard deviations) for the SIDVJ and SICMJ metrics were 16.4 ± 10.3% and 20.2 ± 10.2%, respectively. Indicating that, on average, uninjured athletes demonstrated inter-limb impact force asymmetries of approximately 16-20%.

Table 4 includes the three-trial mean SIDVJ and SICMJ values for each athlete in the ACLR group (ranked in descending order based on their SIDVJ+CMJ values), as well as the SI values for each trial (+/- signs used to denote which limb experienced greater loading). Six of the 11 athletes exhibited SIDVJ+CMJ values that were considered atypically high (>75th percentile - 34.6%) based on the threshold used for this study. In each case, it appeared that the atypical degree of inter-limb asymmetry was the result of the athlete landing with greater impact forces on their uninvolved limb, vs. their ACL-reconstructed limb, during performance of the CMJ task and/or DMJ task (based on analysis of the symmetry indices from each trial) (Table 4).
Discussion
The purpose of this study was to establish normative values for inter-limb impact force symmetry in uninjured adolescent athletes as they performed landing/jumping tasks that are commonly used for ACL injury risk screening. In addition, an example was provided of how clinicians could use these types of normative values to identify athletes who are exhibiting an atypically high level of asymmetry following ACL reconstruction.
From a clinical perspective, it is important to consider how the ability to identify athletes who are exhibiting an atypically high level of inter-limb impact force asymmetry could be used to guide rehabilitation. It appears that athletes tend to offload their ACL-reconstructed limb and place greater load on their uninvolved limb during landing after undergoing ACL reconstruction (based on our findings, as well as those of previous studies examining inter-limb kinetic symmetry in athletes post-ACL reconstruction9,10). There are a variety of factors that may contribute to this pattern of asymmetry, such as deficits in quadriceps strength for the ACL-reconstructed limb27 or fear of re-injury.28,29 In other cases, it may reflect a maladaptive change in an athlete’s motor pattern that has developed following injury.30 The ability to identify athletes who are exhibiting an atypically high level of inter-limb impact force asymmetry could help to guide clinicians to explore the underlying factors that are contributing to the asymmetry, allowing them to develop more targeted intervention strategies to address these factors. This type of targeted assessment/intervention is difficult when normative data is not available. The development of normative values for inter-limb impact force symmetry could also allow clinicians to establish rehabilitation goals for their patients. For instance, a reasonable goal for an injured athlete may be to exhibit asymmetry that is comparable to uninjured athletes. Again, this type of application is challenging unless normative values have been established.
Establishing normative values for inter-limb impact force symmetry could also facilitate the development of more comprehensive return-to-sport testing, where the degree of side-to-side asymmetry in limb loading is considered. At this time, decisions regarding an athlete’s readiness to return to sport are typically based on the time since surgery, knee motion/strength, self-reported knee function, and/or performance on various clinical assessments of sport-related knee function.31 Information of this nature can be readily collected during a clinical examination; however, a recent meta-analysis found that athletes who meet conventional return-to-sport testing criteria are at similar risk for sustaining a second ACL injury, compared to athletes who fail to meet these criteria.32 This appears to indicate that information collected during conventional return-to-sport testing may provide limited insight into an athlete’s readiness to safely resume sports participation. As a result, it may be critical for sports medicine professionals to continue to explore novel ways to evaluate readiness to return to sport following ACL reconstruction. Perhaps the ability to identify athletes who exhibit an atypically high level of inter-limb impact force asymmetry could augment conventional return-to-sport testing.
Future studies could also use the normative values provided in this study to examine the proportion of adolescent athletes who exhibit atypically high levels of inter-limb impact force asymmetry following ACL reconstruction. While previous studies have found that, in general, athletes tend to offload their ACL-reconstructed limb during landing, these studies have examined average performance across all subjects.9,10 What this type of analysis does not provide, is an indication of whether inter-limb differences are the result of most athletes exhibiting inter-limb asymmetries or only a few athletes exhibiting marked inter-limb asymmetries (thus creating a mean difference between the limbs). Although it was not a primary purpose of this study, it was interesting to note that six of the 11 athletes examined as part of ACLR group exhibited atypically high levels of inter-limb impact force asymmetry across both tasks (SIDVJ+CMJ >75th percentile). In each of these six cases, the athlete tended to offload their ACL-reconstructed limb. This appears to indicate that inter-limb asymmetries may be quite pervasive in athletes who have undergone ACL reconstruction; however, examination of a larger sample is certainly warranted.
While the results of this study may be of value to clinicians involved in rehabilitation and return-to-sport decision making, there are limitations that should be considered. First, at this time, most clinics do not have access to a portable or laboratory-based force plate system with the specifications (e.g. sensor range, sampling rate) or durability needed for assessment of dynamic tasks such as landing and jumping. However, it is likely that force plate systems will become more commonly used to assess landing/jumping mechanics in clinical settings as their clinical utility continues to be established. Also, only inter-limb symmetry in peak vertical ground reaction forces were examined. Additional insight could be gained from looking at joint-specific loading patterns (e.g. net joint moments or power), which requires data from a motion capture system that incorporates kinematic data. However, impact force symmetry during landing appears to be strongly related to knee joint kinetic symmetry in both uninjured athletes and athletes who have undergone ACL reconstruction.7,17,18 As a result, assessment of impact force symmetry may provide an indication of asymmetries proximally in the kinetic chain. In addition to loading, it is also critical to highlight the importance of assessing movement quality during testing, since this may also influence ACL injury risk. Finally, it is important to note that there are no well-established thresholds based on inter-limb impact force symmetry for determining if it is safe for an athlete to return to sport. A reasonable goal may be to return injured athletes to a level of symmetry that is comparable to what is observed in most uninjured athletes. However, at this time, it is impossible to determine if this will reduce their risk of re-injury or minimize long-term deficits in knee function. At this point, assessment of inter-limb impact force symmetry would simply provide another piece of information that could be considered when rehabilitating athletes. Although not a limitation to the primary purpose of this study, the amount of trial-to-trial variability in the SI values exhibited by some of the athletes in the ACLR group was notable (Table 4). Perhaps this high degree of variability reflects a relatively unstable motor pattern, which still needs to be refined. Variability in motor performance following ACL reconstruction should continue to be examined.
Conclusion
The normative values for landing forces during jumping tasks established as part of this study may serve as a basis for identifying adolescent athletes who exhibit an atypically high level of inter-limb impact force asymmetry following ACLR. It is possible that this type of assessment of inter-limb kinetic symmetry could help to improve rehabilitation and return-to-sport decision making for adolescent athletes.