
Patients’ decision-making in the informed consent process in a hierarchical and communal culture

Published online: 3 September, TAPS 2019, 4(3), 57-66
DOI: https://doi.org/10.29060/TAPS.2019-4-3/OA2085
Astrid Pratidina Susilo1, Brahmaputra Marjadi2,3, Jan van Dalen4& Albert Scherpbier4
1Faculty of Medicine, University of Surabaya, Indonesia; 2Faculty of Medicine, Universitas Wijaya Kusuma Surabaya, Indonesia; 3School of Medicine, Western Sydney University, Australia; 4Faculty of Health, Medicine, and Life Sciences, Maastricht University, The Netherlands
Abstract
Objective: To investigate patients’ decision-making in the informed consent process in a hierarchical and communal culture.
Methods: This qualitative study took place in an Indonesian hospital and was conducted in line with the Grounded Theory approach. Fifteen patients and twelve family members were interviewed to understand the patients’ decision-making process and factors that contributed to this process. Interview transcripts were analysed using the constant comparison method.
Results: Patients used information to develop an explanation of their illness and treatment. They consented to a medical procedure if information from their physicians matched their own explanation. An increasing severity of the disease urged patients to decide, even when a satisfying explanation had not been developed. A hierarchical relationship between physicians and patients hampered patients’ discussing concerns or sharing emotions with their physicians. To maintain a harmonious relation with their physicians, patients accepted that some questions remained unanswered even after a decision had been made.
Conclusion: The strong hierarchical and communal context added to the complexity in the physician-patient relationship and consequently influenced patients’ decision-making. In addition to strengthening physicians’ communication skills, involving other health professionals as patient advocates or mediators is recommended to ensure patients make voluntary and informed decisions.
Keywords: Decision-making, Informed Consent, Hierarchical Culture, Communal Culture, Grounded Theory
Practice Highlights
- Patients consent to a proposed procedure if information from the physicians match their own.
- Patients’ perception of the information from their physician is influenced by the doctor-patient relation.
- The hierarchical and communal culture hinder patients to discuss their concern with physicians.
- Skills of exploration and facilitation should be strengthened for all health professionals.
- Involvement of other health professionals as advocates may help patients’ make voluntary and informed decisions.
I. INTRODUCTION
Underlying the informed consent process is the patient’s decision-making which is a reflection of patient’s autonomy. Patients have the right to make a voluntary decision about a medical procedure after obtaining adequate information from the physician (King & Moulton, 2006).
In Western settings, decision-making is reported to be both an analytical and intuitive process (Broadstock & Michie, 2000; Power, Swartzman, & Robinson, 2011). Studies which assumed that decision-making was analytical and rational saw decision-making as weighing benefits and risks. Proper information provision, e.g., on the adequacy of information received in an informed consent process was measured by the patients’ recall of information or by their level of satisfaction (Burns, Keogh, & Timon, 2005; Howlader et al., 2004; McGaughey, 2004; McKeague & Windsor, 2003). Patients could not always recall the information, which suggested inadequacy of information (Burns et al., 2005; McGaughey, 2004). Recommendations focused on improvement ofinformation-delivery, for example by using decision aids (Brehaut, Saginur, & Elwyn, 2009; Burns et al., 2005; Schenker, Fernandez, Sudore, & Schillinger, 2011). The more naturalistic paradigm argued that decision-making was also intuitive, with interplays between cognition and emotion (Broadstock & Michie, 2000). Patients dynamically form a representation of their illnesses as the obtained information changes. A decision is made based on this representation adjusted to patients’ belief and experience. Options are accepted if they are satisfactory although not necessarily optimal (Broadstock & Michie, 2000; Power et al., 2011).
As decision-making is context-based (Blank, Graves, Sepucha, & Llewellyn-Thomas, 2006; Broadstock & Michie, 2000), the process in Asia may differ from that in the West. Asian cultures tend to be strongly hierarchical, where large power distance among people is pervasive (Hofstede, Hofstede, & Minkov, 2010). The physician-patient relationship in Asia also tends to be hierarchical (Claramita & Susilo, 2014). Many Asian cultures are also strongly communal, where personal decision-making is heavily influenced by the community (Hofstede et al., 2010) including family members (Pun, Chan, Wang, & Slade, 2018; Susilo, Nurmala, van Dalen, & Scherpbier, 2012; Susilo et al., 2013). Patients’ involvement in health decision-making is often low regardless of their level of education (Claramita, van Dalen, & van der Vleuten, 2011). Patients let physicians make decisions for them to avoid confrontation and/or because of the trust patients have in physicians on medical issues (Lin, Huang, Chiang, & Chen, 2012). Unfortunately, studies on patient decision-making in Asia have been sparse and provide limited insight due to narrow selection of patients (Lin et al., 2012; Sekimoto et al., 2004) or clinicians (Slingsby, 2004).
We conducted this study to expand the evidence in an Asian context. Our research question is: How is the process of patients’ decision-making for informed consent in Indonesia related to the hierarchical and communal Indonesian culture? We investigated the role of information given to patients during the informed consent process in their medical decision-making, and the factors influencing this process unique for the Indonesian context. Insights from this study could assist in preparing health professionals to better support patients’ decision-making and maintain respect for patients’ autonomy.
II. METHODS
As we aimed to understand less known phenomena, this study was conducted in line with the Grounded Theory approach (Corbin & Strauss, 2008; Kennedy & Lingard, 2006). A theoretical framework was developed based on interviews with patients and their families.
A. Study Participants
This study was conducted at an Indonesian hospital with around 300 beds and multi-specialist services. The study population was all former adult in-patients who had been hospitalised up to one year prior to the study. Eligible patients had been offered a diagnostic or therapeutic procedure that required written informed consent. Participants were selected purposively from a list of eligible patients compiled by the Medical Record Department. The sample selection process aimed for diversity (Fraenkel, Wallen, & Hyun, 2012) with regard to medical procedure, age, sex, and educational attainment. Participants had to be fluent in the Indonesian language and be accessible for interviews. Eligible patients were contacted by phone and were provided with verbal information about the study. Those who were interested to participate were invited to give a face-to-face interview. Written information about the study was given to participants prior to obtaining their written informed consent for the study. Family members who were identified as important stakeholders, involved in the decision-making process, were also interviewed with the patients’ approval.
A two-stage sampling process (Kennedy & Lingard, 2006) was employed. The initial sample consisted of elective and urgent patients only. After analysis of seven interviews, a theoretical sampling was derived from the preliminary data and used to expand the sample by including patients with repeated procedures and life-threatening conditions.
B. Data Collection
Semi-structured interviews were conducted to explore the patients’ decision-making process, factors that contributed to the decision, and sources of information used by patients. The interview guide is provided in the Appendix. Interviews were conducted by APS at a location of participants’ choice, mostly in their residence. Each interview took approximately one hour. BM joined one interview session to confirm interview techniques. APS and BM are native Indonesian physicians with no involvement in the care for these patients. Both were trained in qualitative research. Interviews were audio-recorded and notes were handwritten as a backup. When data were considered sufficiently saturated, i.e. when no new information emerged during the interviews, no further interviews were conducted.
C. Data Analysis
The audio recordings were transcribed verbatim and combined with handwritten notes. APS and BM separately conducted open coding on the transcripts of five interviews. Coding categories were then compared and differences were discussed until consensus was reached. APS coded the remainder of the transcripts. The coding categories were sharpened during this iterative process and emerging themes identified and discussed among the authors. Axial coding was performed by comparing similar codes in different interviews in line with the constant comparative method as a necessary component of Grounded Theory (Corbin & Strauss, 2008; Kennedy & Lingard, 2006). The authors discussed the final integration of the themes to the theoretical framework to achieve consensus.
D. Rigour
In order to ensure quality and rigour, we triangulated different data sources (patients and their family) and different researchers. Researchers’ reflections throughout the project were recorded as memos to support data interpretation. Member-checking was conducted by summarising important issues at several points during the interviews (Fraenkel et al., 2012).
E. Ethical Consideration
No physical risk was identified. To avoid influencing the patients’ medical decision-making, only discharged patients were selected for this study. All participants were given oral and written information before being asked for consent. Participants were assured that their decision for participation was voluntary and had no repercussions on their current and future medical opportunities and quality of their care. Identities of participants, physicians, and hospital were kept confidential.
III. RESULTS
Twenty-seven participants (fifteen patients and twelve family members) consented to the study and were interviewed (Table 1). Eleven patients had consented to the proposed medical procedures and four refused to give consent. Ten of the 15 patients had tertiary education. Patients had various health problems and were treated by different physicians.
| No | Sex | Age | Education | Ethnicity | Other people interviewed | Medical condition | Consent |
| P1 | Female | 41 | High school | Javanese | None | Pleural effusion | Consented to pleural puncture |
| P2 | Female | 23 | Tertiary education | Javanese | Sister | Closed fracture of elbow |
Consented to CT-scan and insertion of K-wire |
| P3 | Male | 40 | High school | Javanese | None | Tonsillitis | Requested medication first, then consented to tonsillectomy |
| P4 | Male | 71 | Tertiary education | Chinese | Daughter | Inguinal hernia | Consented to herniotomy |
| P5 | Male | 21 | Tertiary education | Javanese | None | Pleural effusion | Consented to pleural puncture |
| P6 | Female | 35 | High school | Chinese | Husband | Uterine inertia | Requested medication first, then consented to caesarean section |
| P7 | Male | 77 | Tertiary education | Javanese | Daughter, wife, daughter-in-law | Head trauma and vertigo |
Consented to CT-scan, requested early discharge |
| P8 | Female | 38 | High school | Javanese | Husband | Gastritis | Consented to gastroscopy, requested early discharge |
| P9 | Female | 32 | High school | Javanese | None | Spontaneous abortion | Consented to emergency curettage |
| P10 | Male | 31 | Tertiary education | Javanese | Mother | Internal bleeding | Consented to emergency laparotomy |
| P11 | Male | 24 | Tertiary education | Javanese | None | Liver dysfunction | Refused USG and requested early discharge |
| P12 | Female | 48 | Tertiary education | Chinese | None | Anaemia and uterine myoma | Consented to hysterectomy |
| P13 | Male | 67 | Tertiary education | Javanese | Wife | Polycythaemia | Consented to repeated phlebotomy |
| P14 | Male | 68 | Tertiary education | Javanese | Wife | Coronary heart disease |
Refused insertion of cardiac stent and echocardiography, requested early discharge |
| P15 | Female | 57 | Tertiary education | Javanese | Husband, daughter | Pneumonia and hypoglycaemia | Consented to emergency mechanical ventilation |
Table 1. Basic information of participants
A. Emerging Themes
The emerging themes are reported under five major themes, with ‘P(number, diagnosis/procedure)’ denoting a patient, ‘F(number)’ a family member and ‘A’ APS, the interviewer.
1) Decision-making as an evolving process:All interviewed patients reported attempting to develop an ‘explanation’ of what was happening to them and what should be done to rectify their health problem. Each explanation was highly influenced by the patient’s beliefs, values, emotion, and own and others’ past experiences. These explanations helped them to understand and cope with their illness. Some explanations were close to the biomedical concept; for example, P9 (spontaneous abortion) described the objective of curettage as “to clean the remaining blood that was still in the tummy, so… in the next few months it is possible to get [pregnant] straightaway”. Other explanations were not as clear, such as from P8 (gastritis): “I was ill. I didn’t know what the illness was. Someone ‘made’ it, [it’s] my neighbour. I couldn’t walk. I couldn’t do anything”.
Patients’ explanations evolved with the changes in their health conditions. The explanations also evolved as patients obtained further information, either actively sought or passively received. Along this process, patients identified gaps in their explanations and attempted to fill those to develop a satisfactory explanation for their conditions. For instance, P6 (uterine inertia) was informed that the condition of the baby in the womb was worsening as shown as a weakening activity in a Non-Stress Test. The physician suggested a caesarean section. However, P6 did not want surgery and developed her own explanation that the weakening activity was due to her baby being asleep during the test.
The information patients used to develop their explanations came from their physician and various other sources: media, family and friends. Other health professionals (like other physicians approached for a second opinion) were also sources of information. Nurses were sometimes consulted, although not frequently.
Some patients – notably those with chronic conditions – had been contemplating their health problem and the necessary medical procedure(s) prior to being offered the procedure in question. Such patients had had ample time to incorporate alternative treatment options into their explanations. Some patients reported having tried several alternative methods, such as traditional medicine. If outcomes were unsatisfactory, the patient would try another treatment while revising their explanations to incorporate this negative experience. For example, P4 (inguinal hernia) contemplated for four years and tried different solutions before consenting to surgery.
2) Matching own explanation with the information from the physicians:Patients compared formally obtained information from their physician in the informed consent process, particularly about the proposed treatment with their existing explanations. Regardless of the comprehensiveness of the physician’s information (which assessment was beyond the scope of this study), as long as this information matched the patient’s explanation, the patient tended to readily consent to the proposed medical procedure.
[I would prefer] to avoid surgery, [because] it would be much more comfortable to have simple drug treatments. That’s what I thought, and as it turned out my idea matched with Dr X… I felt it click in my heart, because the doctor said, “Let’s treat this with drugs first, okay?”
(P3, chronic tonsillitis)
A match between physician’s information and patient’s explanations led patients to perceive that the information was adequate at the time of decision. If the physician’s information did not match the patient’s explanations, the patients tended to continue to develop explanations and fill the gaps. This process included seeking more information from their physician or others. For example, P12 (myoma) consulted three other physicians despite having had much information from her attending physician.
In searching for more information, patients tended to focus mostly on the gaps or discrepancies in their explanations based on prior knowledge, experience, belief, and value, instead of seeking an overall completeness of information. The husband of P6 (caesarean section) explained why he requested a printout but did not feel the need to ask about the risks of surgery:
Since I am used to dealing with data, naturally I would like to see the data… so I had the graphs printed. My questioning stopped after I got the data… I wasn’t told about the risks of surgery, but I believe… as long as the quality is good, the drugs are good, because the condition of [the patient] was without hypertension, without [other] risks for pregnancy, so I thought there would be no problem… I have studied about high risks in pregnancy, for example if she had had prior surgery… and in several mother and child health books, the risks include for example high blood pressure… but I saw there was none of those risks in [the patient].
On the other hand, when patients had other concerns, they paid less attention to physicians’ information. The mother of P10 (internal bleeding) hardly remembered what the physician had discussed as she was worried about the cost of the surgery during the encounter.
3) Changing severity of the disease disrupts the development of the explanation:Increasing severity of the disease tended to push patients toward consenting to the proposed procedure regardless of their satisfaction with the information they had obtained at that stage. The severity changed influenced patients’ emotion and the patients’ ability to comprehend the information they received. The feelings of confusion, fear, and/or anxiety seemed to be stronger than the patients’ desire to search for more information.
P5: I was also afraid, I was down. I didn’t ask whether there were other alternatives. I trusted the physician.
A: If you look back now, do you think it was a correct decision to have the fluid removed?
P5: Well, quite correct. However, we also don’t know whether there were other solutions or not. Because we didn’t ask. We just trusted the physician.
(P5, pleural effusion)
In contrast to those with severe or emergency conditions, patients who considered their conditions not severe or diminished tended to postpone or refuse a proposed treatment.
P11: I thought my condition was not too severe, so [ultrasonography] was not necessary… because in those two to three days I was actually feeling better.
(P11, liver dysfunction)
4) Influence of physician-patient relation in the decision-making process:When patients trusted their physician and/or the hospital, they tended to consent more readily to the proposed medical procedure regardless of the perceived adequacy of information. The trust also led the participants to give a positive evaluation of the decision despite their lack of knowledge about the condition and/or procedure.
F15: [The decision for the medical procedure] can be considered correct because I had no medical knowledge. I only think that the physician has given the best decision, that’s all… because I know that [the hospital] sincerely gives help to patients who need it.
(Husband of P15, pneumonia and hypoglycaemia)
In contrast, distrust with the physician seemed to influence patients to refuse consent. P14 (coronary heart disease) refused an intervention and asked for early discharge, a decision which he linked to his perception of the physician. He suspected a commercial motive by the physician, as the procedure was expensive. He did not discuss his concern further as he considered the physician not approachable.
The physician-patient relations also influenced the way patients sought information from their physicians. Some patients admitted to having had concerns that they did not express to their physicians. These patients were hesitant to bother their physicians further. Even when their physicians invited patients to ask questions, these patients felt it was inappropriate to ask, or they did not want to offend the physician by expressing their doubts; they chose to maintain a harmonious relation with their physicians. F13 (polycythaemia) did not ask for more information for fear that the physician would see the questions as an attempt to outsmart him and this would be considered as inappropriate behaviour. Furthermore, patients did not always share their emotions openly with their physicians although during the interviews many reported the emotional impact of their illness. P3 (chronic tonsillitis) reported that his physician asked if he was afraid of the surgery and he denied, although he was actually rather afraid.
5) Closing the event:Once the medical procedure had been undertaken, many patients decided not to seek further information regardless of whether there were still gaps in their explanation. This decision seemed to reflect their acceptance of the explanation. For example, when asked whether she still had any unresolved questions about her procedure, P12 (myoma) said: “No, and I also don’t want to know… It will make me think of bad things”. The wife of P13 (polycythaemia), who happened to be a nurse in the same hospital, admitted:“I am actually [still] curious about the [causal] factor… Because Dr Z said it could be due to food, it could be due to excessive intake…”. However, she decided not to pursue her questions any further to avoid making her husband anxious about his condition. For some participants, the event was not as easily closed. For example, P8 (gastritis) went to a traditional healer after discharge and only closed the event when she believed that the healer extracted needles, stones, and cloths (alleged signs of black magic) from her body.
B. Theoretical Framework Describing Patients’ Decision-Making Process
The dynamic process of patients’ decision-making, including the interplaying components within, is depicted in Figure 1. The grey box represents the decision-making of the patient as an evolving process. This consists of several small processes; each is represented by a blue box. First, the process is initiated when the patients feels their first symptoms. Patients build an explanation of their illness and how to treat it, and this explanation evolves over time. Second, during the informed consent process patients assess the match between the information from their physician and their explanation at the time; the degree of match determines the patient’s response to the proposed medical procedure. Third, the culmination of the process is the decision. In the informed consent process, this can be the moment the patient signs the consent form. Fourth, finally the patient will close the event after a medical procedure or non-alternatives by accepting whatever stage their explanation is at the moment, including the fact that some questions may remain unanswered.
This evolution is influenced by external factors outside the grey box; pictured with black arrows. Along the process, patient receives information from different sources including the attending physician. The disease severity modulates the development of the explanation as well as the final decision-making process. Patients’ perception of the information from their physician is influenced by the physician-patient (and/or hospital-patient) relationship.
Finally, the outermost box showed that the whole process is inseparable from the societal culture, which in this context tended to be strongly hierarchical and communal.
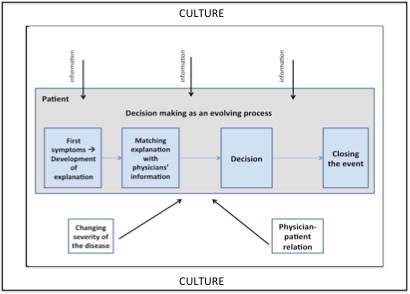
Figure 1. The theoretical framework of patient’s decision-making process
IV. DISCUSSION
The decision-making process of patients in a hierarchical and communal culture is a development of an explanation about their illness and the treatment which evolves as the severity of the disease changes. This explanation is shaped by the information they obtain from different sources. This general pathway of decision is in line with the naturalistic paradigm from Western studies (Broadstock & Michie, 2000; Little, 2009). Similarly to Western findings, we found that many patients still had concerns although they have consented (McKeague & Windsor, 2003; Schenker et al., 2011). These similarities indicate that some phenomena in patient’s decision-making are universal.
Other findings were specific to our Indonesian context. Our participants reported feeling uncomfortable to discuss their concerns or share their emotion with their physicians. This feeling is likely to be stronger in our culture of hierarchy and communality (Hofstede et al., 2010). As physicians occupy a much higher hierarchical position (Claramita & Susilo, 2014), patients do not want to be seen as outsmarting them. Patients also do not want to upset their relation with the physician, a typical feature of a communal culture that upholds harmony, (Hofstede et al., 2010) also reported from a similar culture in Taiwan (Lin et al., 2012). Patients seemed to be willing to assume a passive role and accepted that some concerns were left unanswered.
Our finding of patients’ submissive role confirmed previous studies from this cultural context which showed that patients generally have low involvement in health consultations (Claramita et al., 2011; Kim, Kols, Bonnin, Richardson, & Roter, 2001). However, patients in the hierarchical context also desire a more partnership-style relation with their physicians in which they could have more involvement (Claramita, Nugraheni, van Dalen, & van der Vleuten, 2013). Patients’ effort to gather information from different sources may have indicated that they do have a desire to actively participate in the health decision. Yet, the effort to gather information can also be interpreted as an attempt to make meaning of their illness experience, which is a common adjustment process (Park, 2010). The making of both meanings and decisions seem to be interlinked. In a communal culture information from family and friends is prominent (Hofstede et al., 2010). Patients incorporate information from non-physician sources to develop an explanation about their illness and the treatment although such information is not necessarily in line with that from a physician and could enhance patients’ concern.
When a hierarchical relation hinders patients to discuss their unspoken concern with their physicians, patients may accept underdeveloped or unmatched explanations of their illness at the time of consent. Such patients may experience a higher level of regret than those who were actively involved in the decision (Sawka et al., 2012). If undesired outcomes ensue, patients may blame themselves or the health care system for making the ‘wrong’ decision (Brehaut et al., 2003; Little, 2009).
To face these cultural challenges, we propose some measures to improve patients’ decision-making. Provision of additional information with printed media or decision aids (Brehaut et al., 2009; Burns et al., 2005; Schenker et al., 2011) could support patients to obtain basic information necessary in the informed consent process. Strengthening communication skills of physicians is strongly suggested (Silverman, Kurtz, & Draper, 2013). A guideline tailored to the Southeast Asian culture is available. It may be used to train health professionals to strengthen their skills in exploration, tailoring information and, especially, interpreting subtle non-verbal gestures (Claramita, Susilo, Rosenbaum, & van Dalen, 2016).
As direct confrontation is undesirable in a strong communal culture (Hofstede et al., 2010), patients may not raise their concerns despite exploration by the physician. Therefore, merely training physicians might be insufficient to ensure that patients make voluntary informed decisions. Other studies from similar contexts emphasised the involvement of non-physician health professionals (e.g. nurses) to relay patients’ concerns to the physicians (Lee, Lee, Kong, Kim, & Kim, 2009; Lin et al., 2012; Susilo et al., 2013).
Strengthening the communication skills of health professionals should be started at their education. The informed consent process can serve as a valuable topic to learn communication skills together with the legal, ethical, and cultural aspects in an integrated fashion (Susilo et al., 2013). The insight from this study can inform the development of communication skills training in health professions education. This education should emphasise the importance of understanding the cultural context and tailoring the communication competence of health professionals according to these cultural characteristics (Claramita et al., 2016).
Our study had a few limitations. First, our choice to look at decision-making contexts may have predisposed our data analysis toward decision-making. This subjectivity is an inherent nature of qualitative studies that we need to be aware of (Fraenkel et al., 2012).
Second, from the point of view of qualitative study, there is a limitation in the variation of our sampling. This study was conducted at a single hospital, whose particular setting may have influenced the results of the study. For example, the ethnicities of the patients are Javanese and Chinese and the levels of education of the patients are high school or tertiary education. These categories of patients are the most prevalent ethnic and level of education in this hospital. What we meant with Chinese in this study is Indonesian Chinese who have lived in this country for generations and assimilated with local culture (Urban, 2013). Although Indonesia has diverse ethnicities, similar to other ethnics in Indonesia, both Javanese and Indonesian Chinese hold strong hierarchical and communal culture (Hofstede et al., 2010). There are also some variations of educational attainment in our sampling although this is not the representation of the whole spectrum of education.
Nevertheless, we managed to vary the sampling according to sex, age, and medical procedures. Within the medical procedures, there were also variations based on the type of the health problem or specialisation involved (pulmonology, internal medicine, surgery, obstetrics) and the decision (consent and refusal). We also have representation of emergency and elective procedures, as well as one-time procedure and repeated ones (phlebotomy).
Despite these sampling constraints, the theoretical framework arising from this study was adequate to explain the stories of all participants, thus supporting the comprehensiveness of the framework (Corbin & Strauss, 2008).
Third, since the interviews were conducted a few months after the decision was made, participants may have had inaccurate and/or selective recollection of their decision-making experience. To reduce this phenomenon, which is analogous with ‘recall bias’ in retrospective quantitative studies (Althubaiti, 2016), family members who were involved in the decision-making process were also interviewed (either together or separately) and their accounts were triangulated.
Finally, considering that some phenomena in the decision-making process are universal, we notice the potential of our theoretical model to be applied in other cultural settings. Our data were not adequate to detail this issue because our participants came from one cultural context. It would be interesting to test the applicability of our theoretical model by comparing this result to others from different cultural settings.
V. CONCLUSION
The decision-making process in a hierarchical and communal context resembled that of the Western world. The highlighted differences were in the physician-patient relation and the prominent non-physician source of information. The hierarchical and communal social cultures added to the complexity of this relation and hindered patients to discuss their concerns with the physician in the informed consent process. Our findings could help inform education for health professional. It is important to include the understanding of patients’ decision-making processes in a hierarchical and cultural context to the training of communication skills of health professionals and develop the cultural competence. The awareness of these characteristics can help health professionals to ensure the voluntary nature of patients’ informed decisions.
Notes on Contributors
Astrid Pratidina Susilo is a researcher in health professions education and an anesthesiologist.
Brahmaputra Marjadi is a senior lecturer and researcher in public health and medical education.
Jan van Dalen is a researcher in health professions education.
Albert Scherpbier is a professor in quality improvement in medical education.
Ethical Approval
This study was approved by the hospital’s board of directors and ethics committee (Letter No. 277/SDM/IV-2007).
Acknowledgements
The authors wish to thank all participants in this study.
Funding
There is no external funding involved in this study.
Declaration of Interest
Authors have no conflict of interest, including financial, consultant, institutional and other relationships that might lead to bias.
References
Althubaiti, A. (2016). Information bias in health research: Definition, pitfalls, and adjustment methods. Journal of Multidisciplinary Healthcare, 9, 211-217.
Blank, T., Graves, K., Sepucha, K., & Llewellyn-Thomas, H. (2006). Understanding treatment decision making: Contexts, commonalities, complexities, and challenges. Annals of Behavioral Medicine, 32(3), 211-217.
Brehaut, J. C., O’Connor, A. M., Wood, T. J., Hack, T. F., Siminoff, L., Gordon, E., & Feldman-Stewart, D. (2003). Validation of a decision regret scale. Medical Decision Making, 23(4), 281-292.
Brehaut, J. C., Saginur, R., & Elwyn, G. (2009). Informed consent documentation necessary but not sufficient. Contemporary Clinical Trials, 30(5), 388-389.
Broadstock, M., & Michie, S. (2000). Processes of patient decision making: Theoretical and methodological issues. Psychology & Health, 15(2), 191-204.
Burns, P., Keogh, I., & Timon, C. (2005). Informed consent: A patients’ perspective. The Journal of Laryngology & Otology,119(1), 19-22.
Claramita, M., Nugraheni, M. D., van Dalen, J., & van der Vleuten, C. P. M. (2013). Doctor-patient communication in Southeast Asia: A different culture? Advances in Health Sciences Education Theory and Practice, 18(1), 15-31.
Claramita, M., & Susilo, A. P. (2014). Improving communication skills in the Southeast Asian health care context. Perspectives on Medical Education, 3(6), 474-479.
Claramita, M., Susilo, A. P., Rosenbaum, M., & van Dalen, J. (2016). Core communication skills for health professionals in Southeast Asian health care settings. In M. Claramita, A. P. Susilo, M. Rosenbaum, & J. van Dalen (Eds.), Communication of health care professionals and patients in the context of Southeast Asian culture(pp. 1-17). Jakarta, Indonesia: EGC.
Claramita, M., van Dalen, J., & van der Vleuten, C. P. M. (2011). Doctors in a Southeast Asian country communicate sub-optimally regardless of patients’ educational background. Patient Education and Counseling, 85(3), 169-174.
Corbin, J., & Strauss, A. (2008). Basics of qualitative research: Techniques and procedures for developing grounded theory(3rd ed.). Thousand Oaks, CA: SAGE Publications, Inc.
Fraenkel, J. R., Wallen, N. E., & Hyun, H. H. (2012). How to design and evaluate research in education(8th ed.). New York, NY: Mc-Graw Hill.
Hofstede, G., Hofstede, G. J., & Minkov, M. (2010). Cultures and organizations: Software of the mind: Intercultural cooperation and its importance for survival (3rd ed.). New York, NY: McGraw Hill.
Howlader, M. H., Dhanji, A. R., Uppal, R., Magee, P., Wood, A. J., & Anyanwu, A. C. (2004). Patients’ views of the consent process for adult cardiac surgery: Questionnaire survey. Scandinavian Cardiovascular Journal, 38(6), 363-368.
Kennedy, T. J., & Lingard, L. A. (2006). Making sense of grounded theory in medical education. Medical Education, 40(2), 101-108.
Kim, Y. M., Kols, A., Bonnin, C., Richardson, P., & Roter, D. (2001). Client communication behaviors with health care providers in Indonesia. Patient Education and Counseling, 45(1), 59-68.
King, J. S., & Moulton, B. W. (2006). Rethinking informed consent: The case for shared medical decision-making. Americal Journal of Law & Medicine, 32(4), 429-501.
Lee, S., Lee, W. H., Kong, B. H., Kim, I. S., & Kim, S. (2009). Nurses’ perceptions of informed consent and their related roles in Korea: An exploratory study. International Journal of Nursing Studies, 46(12), 1580-1584.
Lin, M. L., Huang, C. T., Chiang, H. H., & Chen, C. H. (2012). Exploring ethical aspect of elective surgery patients’ decision-making experiences. Nursing Ethics, 20(6), 672-683.
Little, M. (2009). The role of regret in informed consent. Journal of Bioethical Inquiry,6(1), 49-59.
McGaughey, I. (2004). Informed consent and knee arthroscopies: An evaluation of patient understanding and satisfaction. Knee, 11(3), 237-242.
McKeague, M., & Windsor, J. (2003). Patients’ perception of the adequacy of informed consent: A pilot study of elective general surgical patients in Auckland. The New Zealand Medical Journal,116(1170).
Park, C. L. (2010). Making sense of the meaning literature: An integrative review of meaning making and its effects on adjustment to stressful life events. Psychological Bulletin, 136(2), 257-301.
Power, T. E., Swartzman, L. C., & Robinson, J. W. (2011). Cognitive-emotional decision making (CEDM): A framework of patient medical decision making. Patient Education and Counseling, 83(2), 163-169.
Pun, J. K. H., Chan, E. A., Wang, S., & Slade, D. (2018). Health professional-patient communication practices in East Asia: An integrative review of an emerging field of research and practice in Hong Kong, South Korea, Japan, Taiwan, and Mainland China. Patient Education and Counseling, 101(7), 1193-1206.
Sawka, A. M., Straus, S., Gafni, A., Meiyappan, S., David, D., Rodin, G., … Goldstein, D. P. (2012).Thyroid cancer patients’ involvement in adjuvant radioactive iodine treatment decision-making and decision regret: An exploratory study. Supportive Care in Cancer, 20(3), 641-645.
Schenker, Y., Fernandez, A., Sudore, R., & Schillinger, D. (2011). Interventions to improve patient comprehension in informed consent for medical and surgical procedures: A systematic review. Medical Decision Making, 31(1), 151-173.
Sekimoto, M., Asai, A., Ohnishi, M., Nishigaki, E., Fukui, T., Shimbo, T., & Imanaka, Y. (2004). Patients’ preferences for involvement in treatment decision making in Japan. BMC Family Practice, 5, 1.
Silverman, J., Kurtz, S., & Draper, J. (2013). Skills for communicating with patients(3rd ed.). London, England: Radcliffe Publishing Ltd.
Slingsby, B. T. (2004). Decision-making models in Japanese psychiatry: Transitions from passive to active patterns. Social Science & Medicine, 59(1), 83-91.
Susilo, A. P., Nurmala, I., van Dalen, J., & Scherpbier, A. (2012). Patient or physician safety? Physicians’ views of informed consent and nurses’ roles in an Indonesian setting. Journal of Interprofessional Care, 26(3), 212-218.
Susilo, A. P., van Dalen, J., Scherpbier, A., Tanto, S., Yuhanti, P., & Ekawati, N. (2013). Nurses’ roles in informed consent in a hierarchical and communal context. Nursing Ethics, 20(4), 413-425.
Urban, G. S. (2013).The eternal newcomer: Chinese Indonesian identity from Indonesia to the United States. LUX: A Journal of Transdisciplinary Writing and Research from Claremont Graduate University,3(1), 19.
*Astrid Pratidina Susilo
University of Surabaya,
Jalan Raya Kali Rungkut,
Surabaya 60293, Indonesia
Tel: +62-31-298-1000
Email: astrid.pratidina@gmail.com
Announcements
- Fourth Thematic Issue: Call for Submissions
The Asia Pacific Scholar is now calling for submissions for its Fourth Thematic Publication on “Developing a Holistic Healthcare Practitioner for a Sustainable Future”!
The Guest Editors for this Thematic Issue are A/Prof Marcus Henning and Adj A/Prof Mabel Yap. For more information on paper submissions, check out here! - Best Reviewer Awards 2023
TAPS would like to express gratitude and thanks to an extraordinary group of reviewers who are awarded the Best Reviewer Awards for 2023.
Refer here for the list of recipients. - Most Accessed Article 2023
The Most Accessed Article of 2023 goes to Small, sustainable, steps to success as a scholar in Health Professions Education – Micro (macro and meta) matters.
Congratulations, A/Prof Goh Poh-Sun & Dr Elisabeth Schlegel! - Best Article Award 2023
The Best Article Award of 2023 goes to Increasing the value of Community-Based Education through Interprofessional Education.
Congratulations, Dr Tri Nur Kristina and co-authors! - Volume 9 Number 1 of TAPS is out now! Click on the Current Issue to view our digital edition.

- Best Reviewer Awards 2022
TAPS would like to express gratitude and thanks to an extraordinary group of reviewers who are awarded the Best Reviewer Awards for 2022.
Refer here for the list of recipients. - Most Accessed Article 2022
The Most Accessed Article of 2022 goes to An urgent need to teach complexity science to health science students.
Congratulations, Dr Bhuvan KC and Dr Ravi Shankar. - Best Article Award 2022
The Best Article Award of 2022 goes to From clinician to educator: A scoping review of professional identity and the influence of impostor phenomenon.
Congratulations, Ms Freeman and co-authors. - Volume 8 Number 3 of TAPS is out now! Click on the Current Issue to view our digital edition.

- Best Reviewer Awards 2021
TAPS would like to express gratitude and thanks to an extraordinary group of reviewers who are awarded the Best Reviewer Awards for 2021.
Refer here for the list of recipients. - Most Accessed Article 2021
The Most Accessed Article of 2021 goes to Professional identity formation-oriented mentoring technique as a method to improve self-regulated learning: A mixed-method study.
Congratulations, Assoc/Prof Matsuyama and co-authors. - Best Reviewer Awards 2020
TAPS would like to express gratitude and thanks to an extraordinary group of reviewers who are awarded the Best Reviewer Awards for 2020.
Refer here for the list of recipients. - Most Accessed Article 2020
The Most Accessed Article of 2020 goes to Inter-related issues that impact motivation in biomedical sciences graduate education. Congratulations, Dr Chen Zhi Xiong and co-authors.
