 Annie C. H. Fung1†
Annie C. H. Fung1† Gary Tse1,2†
Gary Tse1,2† Hiu Lam Cheng3Eric S. H. Lau1Andrea Luk1,2,4Risa Ozaki1Tammy T. Y. So1Rebecca Y. M. Wong1Joshua Tsoh3Elaine Chow1
Hiu Lam Cheng3Eric S. H. Lau1Andrea Luk1,2,4Risa Ozaki1Tammy T. Y. So1Rebecca Y. M. Wong1Joshua Tsoh3Elaine Chow1 Yun Kwok Wing5Juliana C. N. Chan1,2,4
Yun Kwok Wing5Juliana C. N. Chan1,2,4 Alice P. S. Kong1,2,4*
Alice P. S. Kong1,2,4*
- 1Department of Medicine and Therapeutics, The Chinese University of Hong Kong, Shatin, Hong Kong
- 2Li Ka Shing Institute of Health Sciences, The Chinese University of Hong Kong, Shatin, Hong Kong
- 3School of Public Health and Primary Care, The Chinese University of Hong Kong, Shatin, Hong Kong
- 4Hong Kong Institute of Diabetes and Obesity, The Chinese University of Hong Kong, Shatin, Hong Kong
- 5Department of Psychiatry, The Chinese University of Hong Kong, Shatin, Hong Kong
Background and objectives: Undiagnosed depression is an important comorbidity in type 2 diabetes (T2D) which can be detected using the Geriatric Depression Scale (GDS-15) questionnaire. In this cross-sectional study, we examined the associations of depression using GDS score with control of cardiometabolic risk factors and health status in elderly patients with T2D.
Setting and participants: Between February and December 2013, patients aged ≥65 years who underwent structured comprehensive assessment as a quality improvement program at the Diabetes Center of a teaching hospital were invited to complete the GDS-15 questionnaire.
Main outcome measures: Depression was defined as a GDS score ≥7. Demographic data, prior history of co-morbidities, frequency of self-reported hypoglycemia, and attainment of treatment targets defined as HbA1c, <7%, blood pressure <130/80 mmHg, and LDL-C <2.6 mmol/L were documented.
Results: Among 325 participants (65% male, median [interquartile range] age: 69 [8] years), 42 (13%) had depression. Patients with depression had longer disease durations (mean ± SD: 15.1 ± 9.1 vs. 11.6 ± 8.1 years, P = 0.02), more frequent self-reported hypoglycemic events (17 vs. 6%, P = 0.03) and were less likely to attain all three treatment targets (0 vs. 16%, P = 0.004) than those without depression. On multivariable analysis, patients with depression had an odds ratio of 2.84 (95% confidence intervals: 1.35–6.00, P = 0.006) of reporting prior history of co-morbidities.
Conclusion: In elderly patients with T2D, depression was not uncommon especially in those with poor control of risk factors, hypoglycemia, and co-morbidities. Inclusion of GDS-15 questionnaire during structured assessment for complications and risk factors can identify these high-risk patients for more holistic management of their physical and mental health.
Introduction
Depression is an important but frequently undiagnosed comorbidity in type 2 diabetes (T2D). As a result, the impacts of mental health on self-management and quality of care are often overlooked. A previous meta-analysis reported higher odds of depression (odds ratio: 1.24–2.90) in subjects with T2D than those without T2D (1, 2), while another meta-analysis demonstrated increased risk of depression in people with diabetic complications, including retinopathy, nephropathy, macrovascular, and sexual dysfunction (3).
Depression and diabetes are complex conditions with multi-factorial etiologies. The co-existence of depression and diabetes has been associated with poor self-management and twofold increased risk of cardiovascular events, notably stroke, and premature mortality (4, 5). In Chinese adults with T2D, depression was also associated with hypoglycemia and hyperglycemia, the latter being attenuated after adjusting for suboptimal treatment adherence (6). Age is a common risk factor for both depression and diabetes (7). Thus, with increasing life expectancies, these two conditions represent major burdens on the healthcare system. Given the age-sensitive nature of depression, the Geriatric Depression Scale (GDS-15) is a screening tool that has been tailored and validated for use in the elderly population. In this study, we conducted a cross-sectional analysis from a Diabetes Register to test the utility of GDS-15 and its associations with health status and control of cardiometabolic risk factors in Chinese elderly patients with T2D.
Materials and Methods
Study Population and Setting
Since 1995, the Prince of Wales Hospital, the teaching hospital of the Chinese University of Hong Kong, initiated a research-driven quality improvement program, where 30–50 patients with diabetes underwent periodic structured comprehensive assessment of risk factors and complications to form the Hong Kong Diabetes Register (8). Using a unique identifier and hospitalization data, a series of risk equations were subsequently derived and validated. In 2007, together with other risk parameters, these risk scores were incorporated into the web-based Joint Asia Diabetes Evaluation (JADE) Technology for data integration, risk stratification, and issue of a personalized report to inform patients and care providers for promoting self management and individualized treatment (9). The JADE Portal was subsequently used to establish a JADE Register in Asia to improve quality of care and promote collaborative research (10).
Between February and December 2013, elderly patients aged 65 years or above diagnosed with T2D were invited to complete GDS-15 for screening of depression. The exclusion criteria included: (1) non-Chinese descent, (2) age less than 65 years old, (3) diagnosis of type 1 diabetes (acute presentation with ketosis or continuous requirement of insulin within 1 year of diagnosis of diabetes), (4) inability or refusal to provide informed consent, or (5) incomplete GDS-15 or clinical data. Ethical approval was obtained from the Chinese University of Hong Kong Clinical Research Ethics Committee with informed written consent from all participants.
Clinical Assessment
All data were collected during a 4-h structured assessment performed by trained nurses and health care assistants after an overnight fast of at least 8 h using published protocol. These included history taking, clinical assessment, eye and feet examination, and blood and urine collection (6). Clinical data included current age and age of diagnosis for calculation of disease duration, social habits, education, family history, and frequency of self-reported hypoglycemia in the last 3 months. History of co-morbidities included history of coronary artery disease, stroke, peripheral vascular disease, chronic kidney disease, and malignancy with validation by doctors or cross-checking with the Clinical Management System. Treatment targets were adapted from the American Diabetes Association recommendations (11) and defined as HbA1c <7.0%, blood pressure <130/80 mmHg, and LDL-C <2.6 mmol/L.
Depression was assessed using the Traditional Chinese version of the 15-item GDS, which has been validated in outpatient clinic settings among Hong Kong older population ≥60 years with chronic disease (12). The items involved dichotomous “yes/no” answers that make the GDS-15 easier for elderly to complete, and for scoring by clinicians administering the questionnaires. A cutoff of 7 out of 15 was defined as clinically significant depression (13, 14).
Statistical Analysis
Data analysis was performed using the Statistical Package for Social Science software (SPSS Inc., Version 23, Chicago, IL, USA). Continuous variables were expressed as mean ± SD or median (interquartile range, IQR) and categorical variables were expressed in number (percentage). Student’s t-test, Chi-squared test, and Mann–Whitney U-test were used for group comparisons. Linear and logistic regression was performed to adjust for independent variables significantly associated with depression on univariable analysis with reporting of odds ratio (OR) and 95% confidence intervals (CI). A P-value <0.05 (two-tailed) was considered as statistically significant.
Results
Between February and December 2013, 405 elderly patients with T2D provided informed consent. Of these, 53 patients who did not complete the GDS-15 questionnaire and 27 patients with incomplete clinical data were excluded from the analysis. In the remaining 325 eligible patients, 65% were male (n = 211) with a median age of 69 years (IQR = 8 years). The mean duration of diabetes was 12.0 ± 8.3 years and the mean HbA1c was 7.2 ± 1.1%.
Table 1 compares the demographic and clinical characteristics of the study population categorized by depression defined by a validated GDS-15 score ≥7. The mean GDS-15 score of the study cohort was 3.26 ± 3.12 (range 0–15) with 13% (n = 42) of them reporting significant depressive symptoms based on the GDS-15 score. The depressed group had a mean GDS score of 9.71 ± 0.28 compared to 2.31 ± 1.81 in the non-depressed group. Both groups had similar distribution in term of gender, use of tobacco, and alcohol as well as use of medications for control of blood glucose, blood lipids, and blood pressure. Patients with depression had longer disease duration (15.1 ± 9.1 vs. 11.6 ± 8.1 years, P = 0.02) and tended to be more obese, reaching significance for waist circumference among the males (97.9 ± 8.5 vs. 91.9 ± 8.7 cm, P = 0.001). The depression group tended to have higher fasting plasma glucose and HbA1c levels, albeit short of significance and were more likely to report hypoglycemic events within the past 3 months than the non-depressed group (17 vs. 6%, P = 0.030). Patients with depression had higher systolic blood pressure (145 ± 17 vs. 137 ± 19 mmHg, P = 0.01) with similar control in diastolic blood pressure and blood lipid values. Patients with depression were also more likely to have a prior history of diabetes-related comorbidities. When analyzed by individual events, there was a tendency for patients with depression to report a history of cardiovascular disease more frequently than the non-depression group, albeit short of significance (36 vs. 28%, P = 0.28).
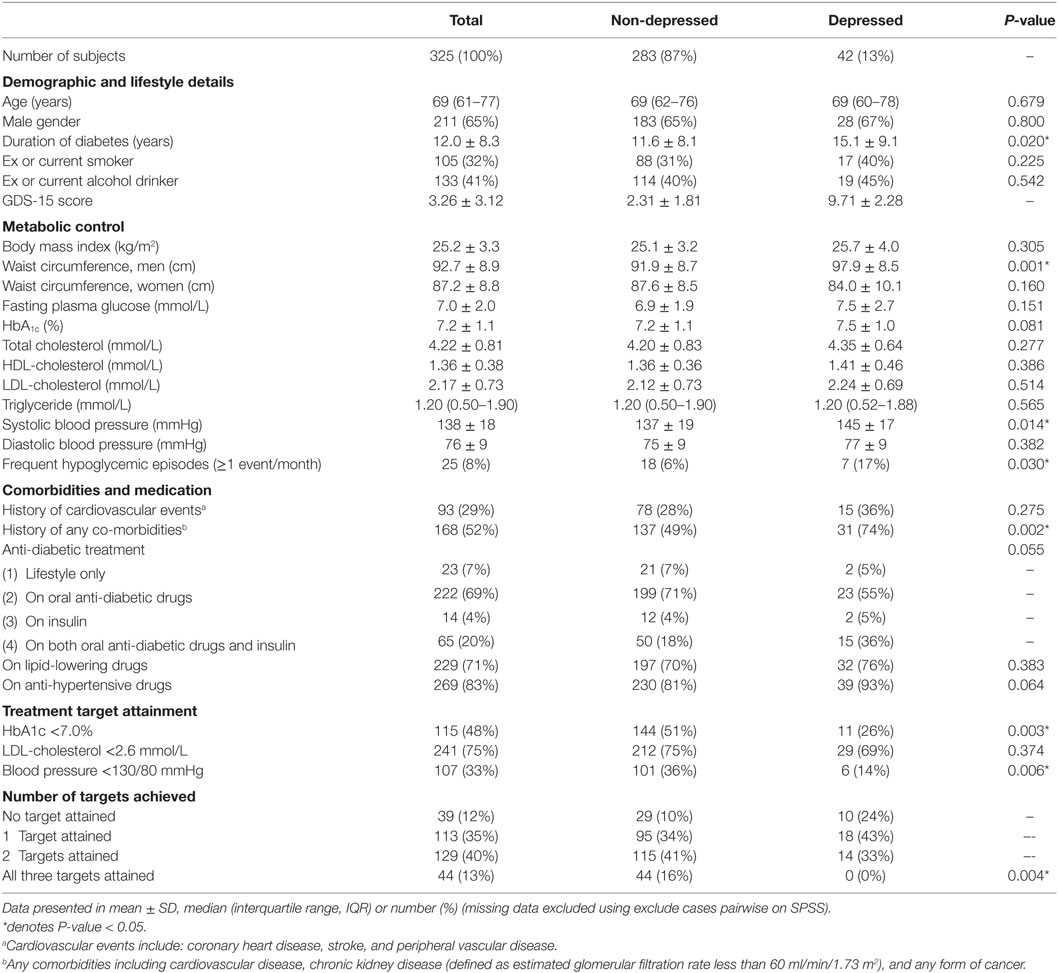
Table 1. Demographic and clinical characteristics of Chinese elderly patients with type 2 diabetes with or without depression defined by Geriatric Depression Score (GDS score ≥7).
Patients with depression were less likely to achieve individual treatment target [HbA1c <7.0% (26 vs. 51%, P = 0.003); blood pressure <130/80 mmHg (14 vs. 36%, P = 0.006); and LDL-C <2.6 mmol/L (69 vs. 75%, P = 0.37)]. Logistic regression analysis showed that depression was associated with a lower OR of attainment for blood pressure (OR: 0.33, 95% CI: 0.13–0.82, P = 0.017) and HbA1c targets (OR: 0.35, 95% CI: 0.17–0.72, P = 0.005) and higher odds for having a prior history of diabetes-related complications (OR = 2.85, 95% CI: 1.35–6.00, P = 0.006) after adjusting for age, gender, and disease duration (Table 2). None of the patients with depression attained all three treatment targets of HbA1c, LDL-C, and blood pressure versus those without depression (0 vs. 16%, P = 0.004). On linear regression analysis, after adjustment for confounders, depressed subjects had a lower OR for attaining all three treatment targets than those without depression (Table 3).
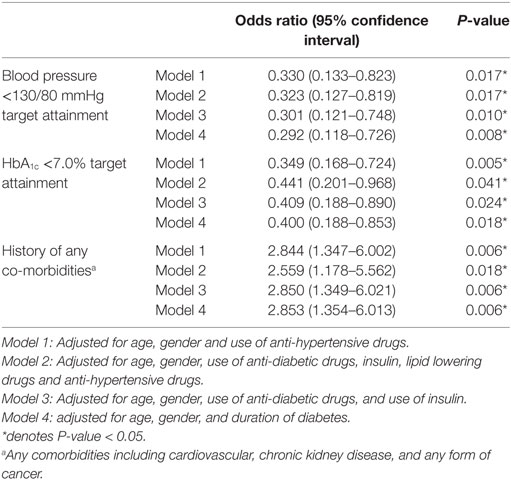
Table 2. Logistic regression analysis for risk association between depression (GDS score ≥7) and control of cardiometabolic risk factors and co-morbidities in Chinese elderly patients with type 2 diabetes.
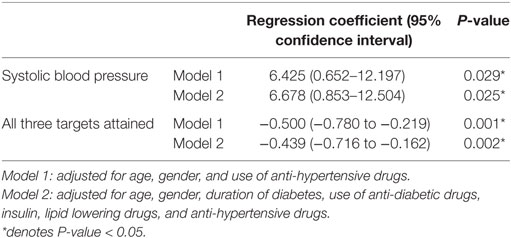
Table 3. Linear regression analysis for risk association of depression (GDS score ≥7) with control of cardiometabolic risk factors in Chinese elderly patients with type 2 diabetes.
Discussion
In this cross-sectional analysis of Chinese elderly patients with T2D, 13% of them had depression which was associated with longer disease durations, more frequent self-reported hypoglycemic events, reduced likelihood of attaining all three treatment targets, and increased odds of having co-morbidities compared to those without depression.
The Bidirectional Association Between Depression and Diabetes
Depression and diabetes exhibit bidirectional relationships (7) and share pathophysiological mechanisms, such as increased oxidative stress, low grade inflammation, and hypercortisolemia (15–17). Depression has been suggested as a risk factor for diabetes for several reasons. First, impaired mental health and lack of motivation might worsen medication adherence and obesity due to suboptimal lifestyle factors, such as physical inactivity and smoking (18). Second, increased activation of the hypothalamic–pituitary–adrenal axis, sympathetic nervous and immune systems in response to stress could lead to hypercortisolemia, increased gluconeogenesis, and reduced insulin secretion (7).
On the other hand, patients with diabetes are prone to develop depression. The emotional burden of a diabetes diagnosis and possible development of complications can lead to rumination and failure to concentrate, which may result in memory, cognitive, and functional impairment. In elderly patients, dependency of daily activities may result in poor self-perception of health, social withdrawal, fear of falling, sense of loneliness, and reflection of past life events which may worsen depressive symptoms. These negative moods can be further aggravated by the co-occurrence of diabetes (19–21).
Depression in the Elderly
In elderly, emotional and somatic symptoms of depression may be concealed by or mistaken for cognitive impairment or dementia making an accurate diagnosis of depression challenging. Yet, even in primary care settings, depression is treatable using psychoeducation, psychotherapy, and medications, followed by monitoring and referral when necessary. There is also evidence suggesting that relief from depression could improve glycemic control (1), but the converse has not been reported. In a randomized controlled trial conducted in primary care setting, integrated care of diabetes and depression in adults improved adherence to oral antidiabetic medications and antidepressants with improved glycemic control and reduced depressive symptoms compared to usual care (22). In “Diabetes, depression, and death: a randomized controlled trial of a depression treatment program for older adults based in primary care” (PROSPECT), depressed elderly patients with diabetes who received intervention were less likely to die during a 5-year period compared to the usual care group with an adjusted hazard ratio of 0.49 (95% CI [0.24–0.98]) (23).
The GDS-15 is a shortened version of GDS-30 and can be self-administered. It is widely accepted by elderly patients and healthcare professionals for its brevity, simplicity, and sensitivity with dichotomous items of “yes or no.” Previous studies using GDS-15 in Hong Kong Chinese population mainly focused on patients with stroke or suicide ideation (24). Our results confirmed the utility of GDS-15 in identifying patients with diabetes and comorbid depression which was associated with complications and poor control of cardiometabolic risk factors.
In our study cohort, 13% of patients had depression. Earlier studies conducted in Hong Kong Chinese reported higher prevalence of depression in elderly with T2D (12.2%) than those without diabetes (9%) (25). In most surveys, depression is more common in women than men. An earlier study in Hong Kong also reported a female preponderance of depression in elderly population (14.5 vs. 11%) (26). Possible reasons for this gender difference included higher levels of psychological stress, somatic complaints, and poor self-rated health in females (27). However, we did not find this gender difference which might be due to the male predominance and small sample size of our study cohort.
Depression Is Associated With Co-Morbidities and Poor Control of Cardiometabolic Risk Factors
In agreement with the literature (28), Chinese elderly patients with T2D were more likely to report prior history of co-morbidities. Although we did not measure treatment adherence in this study, we have reported its association with depression using PHQ9 in a separate cohort with broader age range (6). In a review article, the authors highlighted that comorbid depression might increase disease burden of T2D due to poor self-management, increased risk of dementia and healthcare expenditure (28). Besides, aging and diabetes are both linked to dependency, psychosocial, and physical changes, which can be exacerbated under the synergistic effect of depression (29). Functional disability, defined as difficulty performing routine activities of daily living or social activities, can be both a consequence of and a risk factor for developing chronic diseases. In this light, patients with comorbid depression and diabetes were more likely to experience functional disability than those with either diabetes or depression alone (30). In our analysis, elderly patients with diabetes and depression were more likely to have co-morbidities, including cardiovascular disease, chronic kidney disease, and cancer, which was likely to result in functional disability although this was not formally documented.
In agreement with our previous report (31), elderly patients with depression had higher HbA1c and frequency of hypoglycemic episodes than those without depression. This combined trait of hyperglycemia and hypoglycemia can lead to glycemic variability which has been shown to predict depressive symptoms in Israeli elderly patients with T2D (32). In the same study, the association was observed in patients irrespective of attainment of HbA1c target <7% although the effect size was more evident in those who were not at target. In a recent prospective analysis of the Hong Kong Diabetes Register, we have reported a hazard ratio of 1.5 of cardiovascular-renal disease for every 1 SD in HbA1c (33). In this cross-sectional study, we only used the HbA1c value and self-reported hypoglycemic events in the past 3 months collected during the comprehensive assessment for analysis. Thus we were not able to examine the association between depression and HbA1c variability which requires prospective evaluation.
Apart from poor glycemic control, none of our elderly patients with diabetes and depression had attained any of the three treatment targets compared to 16% in those without depression. Attainment of these treatment targets had prognostic significance for future clinical outcomes. In this light, we have reported that patients who attained two or more treatment targets had 50% lower risk of incident cardiovascular disease than who were not at any target (34). These constellations of poor control of cardiometabolic risk factors, frequent hypoglycemia, co-morbidities, poor self management, and functional disability might contribute to the 1.5-fold increased risk of mortality in patients with diabetes and depression compared to diabetes alone (35), thus highlighting the importance in identifying these high risk patients for holistic management.
Social Support and Multidisciplinary Care in Elderly Patients With Diabetes and Depression
Achieving optimal glycemic control is more challenging in elderly than younger patients for many reasons. Age-related functional, cognitive, and physical impairments can hinder an individual’s ability to remember and comply with complex self-management regimens including changes to their accustomed lifestyles (25). A holistic approach addressing the biopsychosocial needs in elderly patients with comorbid depression could improve quality of care and reduce the burden on their family members and healthcare services. In this light, satisfaction of elderly patients toward family and social support has been shown to protect against development of depressive symptoms (36, 37).
In Hong Kong, since 2000, periodic comprehensive assessment for risk factors and complications performed by trained nurses is a standard service in the public healthcare institutions in both hospital and primary care settings (38). Our results suggested that inclusion of GDS-15, especially in those with poor control of risk factors and/or co-morbidities might identify elderly patients with depression, who would benefit from intensive health and social care support by a multi-disciplinary team, including endocrinologists, primary care doctors, and psychiatrists and other professional and community care workers to address these multiple needs.
Study Limitations
Several limitations of this study should be noted. First, the study cohort was relatively small, and all patients were recruited from a single hospital. Second, screening of depression was based solely upon GDS score without confirmation using standard instruments such as the Mini International Neuropsychiatric Interview or clinical diagnosis by a psychiatrist. While we were unable to comment on the diagnostic performance of GDS-15 for depression, the tool was useful in identifying a subgroup of patients with unmet needs. Third, we did not document the personal or family history of depression or administration of any psychotropic medications. The latter could be retrieved from the Clinical Management System of the hospital but this was outside the scope of this study. Besides, many of these electronic medical records were used to collect data and not designed to establish a register for quality improvement or monitoring purpose, making data-mining, data-cleaning, and data-analysis extremely labor-intensive. Our experience of redesigning the workflow for systematic collection of data periodically to establish a Register could combine research and practice to address multiple purposes including quality assurance, providing feedback to care providers, and patients with ongoing evaluation to identify unmet needs (9). Finally, these cross-sectional data are only hypothesis-generating. Longitudinal and interventional studies are needed to confirm whether alleviation of depression could improve risk factor control and clinical outcomes in elderly patients with T2D and depression.
Implications for Clinical Practice
In elderly Chinese people with T2D, 13% had depression which was associated with long disease duration, poor control of cardiometabolic risk factors, frequent hypoglycemia and co-morbidities. Patients harboring these traits would benefit for screening for depression using GDS-15. Based on prior work, these patients had high risk for functional disability and death. Thus, upon identification, these patients would require detailed cognitive, psychological, and behavioral assessments followed by holistic health and social care in order to improve psychological health, self management, drug adherence, control of cardiometabolic risk factors, and clinical outcome.
Conclusion
In hospital clinic setting, depression affects 13% of Chinese elderly patients with T2D. Patients with long disease duration, poor control of cardiometabolic risk factors, frequent hypoglycemia and comorbidities are high risk individuals for having comorbid depression. Given the silent nature of these risk factors and depression, periodic comprehensive assessment of risk factors, and complications including the use of GDS-15 may identify high risk patients for early intervention in order to reduce the disease burden on patients, their families, and healthcare services.
Ethics Statement
This study received approval from the Chinese University of Hong Kong (CUHK) Clinical Research Ethics Committee and informed written consent was obtained from all participants.
Author Contributions
AF: data collection, analysis, manuscript drafting, and critical revision. GT: data interpretation, analysis, and manuscript critical revision. HC and EL: data collection, interpretation, and analysis. AL, RO, TS, RW, JT, and EC: data interpretation, manuscript critical revision. YW, JC, and AK: data interpretation, manuscript critical revision, and project supervision.
Conflict of Interest Statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Funding
We thank the medical and nursing staff at the Prince of Wales Hospital Diabetes Centre for their help in recruitment of subjects for this study. GT is supported by a Research Fellowship from the Croucher Foundation of Hong Kong.
References
1. Anderson RJ, Freedland KE, Clouse RE, Lustman PJ. The prevalence of comorbid depression in adults with diabetes: a meta-analysis. Diabetes Care (2001) 24:1069–78. doi:10.2337/diacare.24.6.1069
2. Nouwen A, Winkley K, Twisk J, Lloyd CE, Peyrot M, Ismail K, et al. Type 2 diabetes mellitus as a risk factor for the onset of depression: a systematic review and meta-analysis. Diabetologia (2010) 53:2480–6. doi:10.1007/s00125-010-1874-x
3. de Groot M, Anderson R, Freedland KE, Clouse RE, Lustman PJ. Association of depression and diabetes complications: a meta-analysis. Psychosom Med (2001) 63:619–30. doi:10.1097/00006842-200107000-00015
4. Ting RZ, Lau ES, Ozaki R, Lau WW, Kong AP, Luk AO, et al. High risk for cardiovascular disease in Chinese type 2 diabetic patients with major depression – a 7-year prospective analysis of the Hong Kong Diabetes Registry. J Affect Disord (2013) 149:129–35. doi:10.1016/j.jad.2013.01.012
5. Tse G, Lai ET, Tse V, Yeo JM. Molecular and electrophysiological mechanisms underlying cardiac arrhythmogenesis in diabetes mellitus. J Diabetes Res (2016) 2016:2848759. doi:10.1155/2016/2848759
6. Zhang Y, Ting RZ, Yang W, Jia W, Li W, Ji L, et al. Depression in Chinese patients with type 2 diabetes: associations with hyperglycemia, hypoglycemia, and poor treatment adherence. J Diabetes (2015) 7:800–8. doi:10.1111/1753-0407.12238
7. Tabak AG, Akbaraly TN, Batty GD, Kivimaki M. Depression and type 2 diabetes: a causal association? Lancet Diabetes Endocrinol (2014) 2:236–45. doi:10.1016/S2213-8587(13)70139-6
8. Chan JCN, So W, Ma RCW, Tong PCY, Wong R, Yang X. The complexity of vascular and non-vascular complications of diabetes: the Hong Kong Diabetes Registry. Curr Cardiovasc Risk Rep (2011) 5:230–9. doi:10.1007/s12170-011-0172-6
9. Chan JC, Ozaki R, Luk A, Kong AP, Ma RC, Chow FC, et al. Delivery of integrated diabetes care using logistics and information technology – the Joint Asia Diabetes Evaluation (JADE) program. Diabetes Res Clin Pract (2014) 106(Suppl 2):S295–304. doi:10.1016/S0168-8227(14)70733-8
10. Chan J, So W, Ko G, Tong P, Yang X, Ma R, et al. The Joint Asia Diabetes Evaluation (JADE) Program: a web-based program to translate evidence to clinical practice in type 2 diabetes. Diabet Med (2009) 26:693–9. doi:10.1111/j.1464-5491.2009.02751.x
11. Monnier L, Colette C. Target for glycemic control: concentrating on glucose. Diabetes Care (2009) 32(Suppl 2):S199–204. doi:10.2337/dc09-S310
12. Chan AC. Clinical validation of the Geriatric Depression Scale (GDS): Chinese version. J Aging Health (1996) 8:238–53. doi:10.1177/089826439600800205
13. Lee H-CB, Chiu HFK, Kwok WY, Leung CM. Chinese elderly and the GDS short form: a preliminary study. Clin Gerontol (1993) 14:37–42.
14. Cheng ST, Yu EC, Lee SY, Wong JY, Lau KH, Chan LK, et al. The geriatric depression scale as a screening tool for depression and suicide ideation: a replication and extention. Am J Geriatr Psychiatry (2010) 18:256–65. doi:10.1097/JGP.0b013e3181bf9edd
15. Michel TM, Pulschen D, Thome J. The role of oxidative stress in depressive disorders. Curr Pharm Des (2012) 18:5890–9. doi:10.2174/138161212803523554
16. Palta P, Samuel LJ, Miller ER III, Szanton SL. Depression and oxidative stress: results from a meta-analysis of observational studies. Psychosom Med (2014) 76:12–9. doi:10.1097/PSY.0000000000000009
17. Tse G, Yan BP, Chan YW, Tian XY, Huang Y. Reactive oxygen species, endoplasmic reticulum stress and mitochondrial dysfunction: the link with cardiac arrhythmogenesis. Front Physiol (2016) 7:313. doi:10.3389/fphys.2016.00313
18. Chau J, Martin CR, Thompson DR, Chang AM, Woo J. Factor structure of the Chinese version of the Geriatric Depression Scale. Psychol Health Med (2006) 11:48–59. doi:10.1080/13548500500093688
19. Lou VW, Chi I, Kwan CW, Leung AY. Trajectories of social engagement and depressive symptoms among long-term care facility residents in Hong Kong. Age Ageing (2013) 42:215–22. doi:10.1093/ageing/afs159
20. Leung DY, Bai X, Leung AY, Liu BC, Chi I. Prevalence of medication adherence and its associated factors among community-dwelling Chinese older adults in Hong Kong. Geriatr Gerontol Int (2015) 15:789–96. doi:10.1111/ggi.12342
21. Moreira Bde S, Dos Anjos DM, Pereira DS, Sampaio RF, Pereira LS, Dias RC, et al. The geriatric depression scale and the timed up and go test predict fear of falling in community-dwelling elderly women with type 2 diabetes mellitus: a cross-sectional study. BMC Geriatr (2016) 16:56. doi:10.1186/s12877-016-0234-1
22. Bogner HR, Morales KH, De Vries HF, Cappola AR. Integrated management of type 2 diabetes mellitus and depression treatment to improve medication adherence: a randomized controlled trial. Ann Fam Med (2012) 10:15–22. doi:10.1370/afm.1344
23. Bogner HR, Morales KH, Post EP, Bruce ML. Diabetes, depression, and death: a randomized controlled trial of a depression treatment program for older adults based in primary care (PROSPECT). Diabetes Care (2007) 30:3005–10. doi:10.2337/dc07-0974
24. Tang WK, Ungvari GS, Chiu HF, Sze KH. Detecting depression in Chinese stroke patients: a pilot study comparing four screening instruments. Int J Psychiatry Med (2004) 34:155–63. doi:10.2190/9YJ9-NNXA-RJCY-2DYP
25. Chau PH, Woo J, Lee CH, Cheung WL, Chen J, Chan WM, et al. Older people with diabetes have higher risk of depression, cognitive and functional impairments: implications for diabetes services. J Nutr Health Aging (2011) 15:751–5. doi:10.1007/s12603-011-0071-z
26. Chi I, Yip PS, Chiu HF, Chou KL, Chan KS, Kwan CW, et al. Prevalence of depression and its correlates in Hong Kong’s Chinese older adults. Am J Geriatr Psychiatry (2005) 13:409–16. doi:10.1097/00019442-200505000-00010
27. Boey KW, Chiu HF. Life strain and psychological distress of older women and older men in Hong Kong. Aging Ment Health (2005) 9:555–62. doi:10.1080/13607860500193351
28. Park M, Reynolds CF III. Depression among older adults with diabetes mellitus. Clin Geriatr Med (2015) 31:117–137,ix. doi:10.1016/j.cger.2014.08.022
29. Trief PM. Depression in elderly diabetes patients. Diabetes Spectrum (2007) 20:71–5. doi:10.2337/diaspect.20.2.71
30. Egede LE. Diabetes, major depression, and functional disability among U.S. adults. Diabetes Care (2004) 27:421–8. doi:10.2337/diacare.27.2.421
31. Zhang Y, Ting R, Lam M, Lam J, Nan H, Yeung R, et al. Measuring depressive symptoms using the Patient Health Questionnaire-9 in Hong Kong Chinese subjects with type 2 diabetes. J Affect Disord (2013) 151:660–6. doi:10.1016/j.jad.2013.07.014
32. Ravona-Springer R, Heymann A, Schmeidler J, Moshier E, Guerrero-Berroa E, Soleimani L, et al. Hemoglobin A1c variability predicts symptoms of depression in elderly individuals with type 2 diabetes. Diabetes Care (2017) 40:1187–93. doi:10.2337/dc16-2754
33. Luk AO, Ma RC, Lau ES, Yang X, Lau WW, Yu LW, et al. Risk association of HbA1c variability with chronic kidney disease and cardiovascular disease in type 2 diabetes: prospective analysis of the Hong Kong Diabetes Registry. Diabetes Metab Res Rev (2013) 29:384–90. doi:10.1002/dmrr.2404
34. Kong AP, Yang X, Ko GT, So WY, Chan WB, Ma RC, et al. Effects of treatment targets on subsequent cardiovascular events in Chinese patients with type 2 diabetes. Diabetes Care (2007) 30:953–9. doi:10.2337/dc06-2443
35. van Dooren FE, Nefs G, Schram MT, Verhey FR, Denollet J, Pouwer F. Depression and risk of mortality in people with diabetes mellitus: a systematic review and meta-analysis. PLoS One (2013) 8:e57058. doi:10.1371/journal.pone.0057058
36. Chan SW, Chiu HF, Chien WT, Goggins W, Thompson D, Hong B. Predictors of change in health-related quality of life among older people with depression: a longitudinal study. Int Psychogeriatr (2009) 21:1171–9. doi:10.1017/S1041610209990950
37. Nan H, Lee PH, Mcdowell I, Ni MY, Stewart SM, Lam TH. Depressive symptoms in people with chronic physical conditions: prevalence and risk factors in a Hong Kong community sample. BMC Psychiatry (2012) 12:198. doi:10.1186/1471-244X-12-198
Keywords: diabetes, depression, elderly, GDS-15, hypoglycaemia, comorbidities
Citation: Fung ACH, Tse G, Cheng HL, Lau ESH, Luk A, Ozaki R, So TTY, Wong RYM, Tsoh J, Chow E, Wing YK, Chan JCN and Kong APS (2018) Depressive Symptoms, Co-Morbidities, and Glycemic Control in Hong Kong Chinese Elderly Patients With Type 2 Diabetes Mellitus. Front. Endocrinol. 9:261. doi: 10.3389/fendo.2018.00261
Received: 18 February 2018; Accepted: 07 May 2018;
Published: 29 May 2018
Edited by:
Åke Sjöholm, Gävle Hospital, SwedenReviewed by:
Rebecca Thwing Emeny, Geisel School of Medicine, United StatesAmer Hayat Khan, University of Science, Malaysia, Malaysia
Copyright: © 2018 Fung, Tse, Cheng, Lau, Luk, Ozaki, So, Wong, Tsoh, Chow, Wing, Chan and Kong. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Alice P. S. Kong, alicekong@cuhk.edu.hk
†These authors have contributed equally to this work.