 Yike Chen1†
Yike Chen1† Xiaohui Xu2†Jing Cao3Yuanqing Jie4Linkai Wang1
Xiaohui Xu2†Jing Cao3Yuanqing Jie4Linkai Wang1 Feng Cai1
Feng Cai1 Sheng Chen1
Sheng Chen1 Wei Yan1
Wei Yan1 Yuan Hong1
Yuan Hong1 Jianmin Zhang1*
Jianmin Zhang1* Qun Wu1*
Qun Wu1*- 1Department of Neurosurgery, The Second Affiliated Hospital, School of Medicine, Zhejiang University, Hangzhou, China
- 2Department of Neurosurgery, The Fourth Affiliated Hospital, School of Medicine, Zhejiang University, Yiwu, China
- 3Department of Statistical Office, The Affiliated Changsha Central Hospital, Hengyang Medical School, University of South, Changsha, China
- 4Department of Neurosurgery, The Affiliated Quzhou People’s Hospital of Wenzhou Medical University, Quzhou, China
Background: Transsphenoidal surgery (TSS) is first-line treatment for giant pituitary adenomas (PAs). Although PA is a benign neuroendocrine tumor that originates from adenohypophysial cells, the surgical outcomes and prognosis of giant PAs differ significantly due to multiple factors such as tumor morphology, invasion site, pathological characteristics and so on. The aim of this study was to evaluate surgical outcomes of giant PAs in a single-center cohort.
Methods: The clinical features and outcomes of 239 patients with giant PA who underwent sphenoidal surgery at the Second Affiliated Hospital of Zhejiang University School of Medicine from January 2015 to October 2021 were collected from medical records. The basic clinical information (age, gender, function etc.), surgical procedure, imaging features (maximum diameter, invasion characteristics, tumor shape etc.) and histopathological characteristics (pathological results, Ki-67, P53 etc.) were retrospectively reviewed. SPSS 25.0 and Stata 12.0 software were used for statistical analysis.
Results: A total of 239 patients with giant PAs underwent TSS, of which 168 surgeries (70.29%) were endoscopic endonasal transsphenoidal (EETS) and 71 (29.71%) were microscopic transsphenoidal (MTS). The mean preoperative maximum diameter in the cohort was 45.64 mm. Gross-total resection was achieved in 46 patients (19.25%), near-total in 56 (23.43%), subtotal in 68 (28.45%), and partial in 69 (28.87%) patients. The maximum tumor diameter and Knosp grade were the significant factors that limited the extent of the resection of giant PAs. A total of 193 patients (80.75%) experienced surgical complications, and the most common complications were postoperative diabetes insipidus (DI) (91, 38.08%), intracranial infection (36, 15.06%) and cerebrospinal fluid (CSF) leaks (37, 15.48%). In addition, there was a significant difference in the incidence of CSF leaks between the neuroendoscopy group and the microscopic group (P < 0.05).
Conclusion: The management of giant PAs remains a therapeutic challenge due to their large size and postoperative complications. The maximum diameter and Knosp grade of giant PAs significantly limited the extent of resection, which warrants a reasonable surgical plan.
Introduction
Pituitary adenoma (PA) is a benign neuroendocrine tumor that originates from adenohypophysial cells, and accounts for 10%-20% of all primary intracranial tumors (1, 2). Giant PAs are defined as tumors with largest diameter ≥4 cm (3–5), and are characterized by high invasiveness and irregular growth. In addition, giant PAs tend to compresses the optic chiasm and third ventricle, encase the internal carotid artery, and affect hormone secretion from the pituitary gland and hypothalamus (6, 7).
Surgical resection is the first-line treatment for most giant PAs except prolactinoma. Either transcranial or transsphenoidal approaches can be adopted for the surgical removal of giant PAs. Since craniotomy causes greater damage to normal brain tissues and results in more postoperative complications, it is now gradually being replaced with the transnasal sphenoidal approach (8). However, the efficacy of transsphenoidal surgery (TSS) for giant adenomas is poor and is associated with a higher complication rate compared to the smaller PAs (9–11), which can be attributed to the intricate anatomy and secretory functions of the pituitary gland. In this study, we have reviewed the outcomes following TSS of 239 giant PAs from a single-center and analyzed the factors that limit the extent of resection.
Materials and Methods
Study Population
The clinical data of 239 patients with giant PAs who underwent TSS at The Second Affiliated Hospital Zhejiang University School of Medicine between January 2015 and October 2021 was retrospectively analyzed. The study was approved by the Research Ethics Committee of SAHZU. The inclusion criteria were as follows: 1) histologically confirmed PAs, 2) maximal diameter of PAs not less than 4 cm according to preoperative MRI, 3) tumor resection through TSS, and 4) regular follow-up for a minimum of 3 months. Patients were excluded if the medical records were not complete, or if the pathological report or follow-up data were missing.
Data Collection
The basic, surgical, radiological and pathological data was collected. Basic information included age, gender, functional status, clinical presentation. Radiological characteristics included maximum diameter (mm), tumor shape (rounded, dumbbell-shaped, multilobular), invasion characteristics and Knosp classification. Surgical procedures included the surgical method (microscopy or neuroendoscopy), unilateral/bilateral nostrils, the amount of blood loss, the duration of surgery, postoperative hospital stay, extent of resection (gross total resection, GTR (≥95%); near total resection, NTR (≥90%); subtotal resection, STR (≥70%); partial resection, PR [<70%) (12)], endocrine remission and surgical complications. The pathological classification, P53 and Ki-67 positive rates were also collected.
Tumor Volume Measurement
MRI was typically performed within 2 weeks before surgery and 3 months postoperatively at our institution. The imaging data were obtained through the imaging information-management system. The diameters of the tumors were measured in all direction using a measuring tool in the system, and the extent of resection was determined by comparing pre- and postoperative MRI data.
Surgical Approach
All patients underwent TSS, and the major surgical procedures were conducted by neurosurgeons with more than 15 years of experience. The objectives of the surgery were to: 1) achieve maximal resection and maximal remission of symptoms with least disturbance to neural and vascular structures, and 2) maintain or reinstate endocrine function.
Patients were positioned supine with the head raised and tilted back slightly. After the induction of general anesthesia, the nasal mucosa and skin of the surgical site was fully disinfected. The following operations are performed under an endoscope (with the aid of a 0° or 30° 4-mm endoscope) or microscope. To avoid nasal mucosal damage, a uninostril approach is used in most cases. Bilateral nostrils technique was performed if the operating space is too narrow. After covering the nasal mucosa with epinephrine cotton pad, the nasal turbinates are lateralized to expand the surgical space. The right pedicled nasoseptal flap was partially resected, then it was stored inferior the surgical channel and was fully harvested if an intraoperative CSF leak occurred. A high-speed drill or osteotome was used to open the sphenoid sinus and the sellar floor was removed. Once the tumor was fully exposed, the lesions localized in the intrasellar and suprasellar region was removed with suction and ring curettes first, then removed the residual lesions in cavernous sinus under direct vision. To protect the carotid arteries and other lateral structures, neuronavigation and Doppler ultrasound were used during resection. Finally, the skull base was reconstructed using the prepared autologous tissue and artificial materials after efficient hemostasis.
Data Analysis
SPSS 25.0 and STATA 12.0 software were used for statistical analysis. Continuous variables with normal distribution were expressed as mean ± SD and compared by one-way ANOVA. Mann-Whitney U test and Kruskal-Wallis H test were used for categorical variables. Enumeration data were compared using the chi-square and Fisher exact tests. Ordinal logistic regression model was used to identify factors affecting the extent of resection. Two-sided P values < 0.05 were considered statistically significant.
Results
General Characteristics
A total of 239 patients (137 females and 102 males) with pathologically confirmed PA were included. The mean age was 51.12 ± 13.8 years (range, 19-84 years). Non-functional PAs was detected in 158 patients (66.11%) and 81 patients (33.89%) had functional PAs. In this series, patients mainly presented with visual impairment 175 (73.22%), including visual acuity (162, 67.78%) and/or visual field (122, 51.05%) deficits. In addition, 67 patients (28.03%) presented with headache, and 41 patients (17.15%) exhibited symptoms of endocrine dysfunction prior to surgery, including irregular menstruation (13, 5.44%), galactorrhea (2, 0.84%), sexual dysfunction (3, 1.26%), acromegaly (6, 2.51%), concentric obesity (2, 0.84%) and thyroid dysfunction (15, 6.28%). Furthermore, 10 patients (4.18%) experienced diabetes insipidus and 23 (9.62%) had apoplexy (confirmed by radiographic and intraoperative findings) prior to surgery (Table 1).
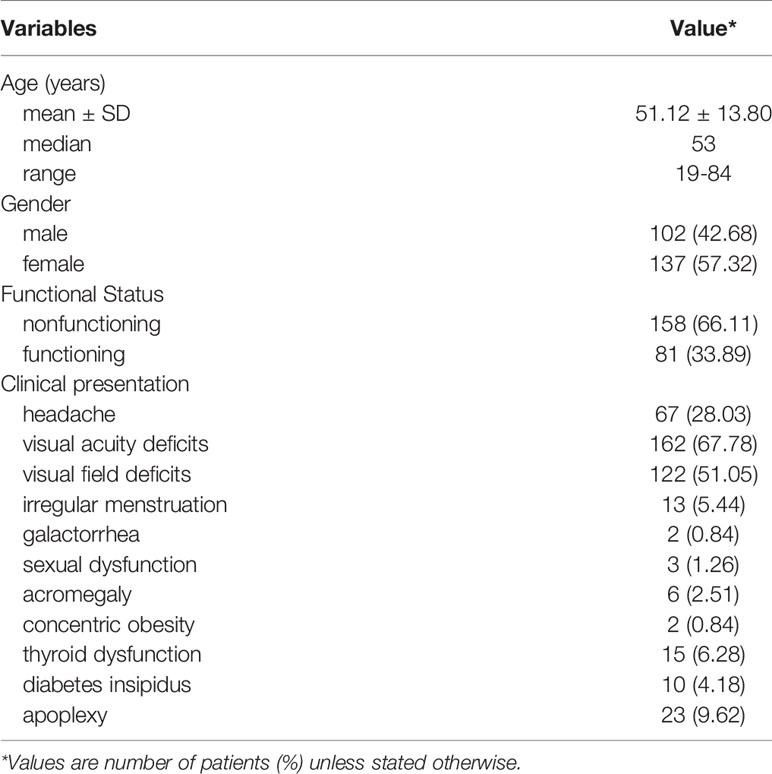
Table 1 General characteristics.
The average maximum diameter for the giant PAs was 45.64 ± 6.7 mm (range 40–75 mm). The tumors were round in 14 cases (5.86%), dumbbell shaped in 89 cases (37.24%), and multilobular in 136 cases (56.9%). Based on the preoperative MRI results and intraoperative observations, 220 cases (92.05%) had cavernous sinus invasion, 165 (69.04%) had sphenoid sinus invasion and 221 cases (92.47%) showed suprasellar invasion. The highest Knosp grade was 0-1 for 26 patients (10.88%), 2 for 46 patients (19.25%), 3A for 38 patients (15.90%), 3B for 21 patients (8.79%) and 4 for 108 patients (45.19%), which were indicative of the extent of cavernous sinus invasion and aggressiveness of the giant PAs (Table 2).
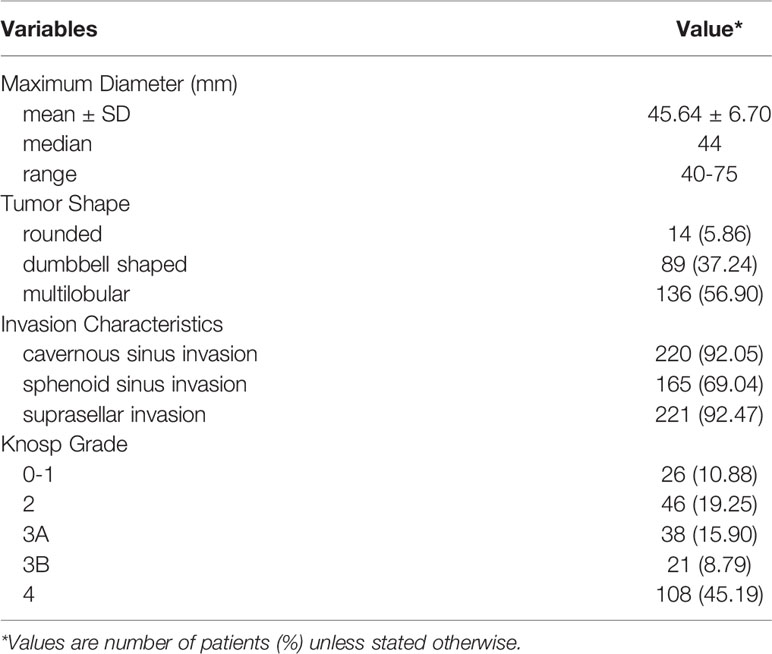
Table 2 Radiological characteristics.
As expected, the predominant pathological type of the giant PAs was gonadotrophic adenomas (76, 31.8%), followed by lactotroph adenomas (27, 11.3%), corticotroph adenomas (27, 11.3%), pluri-hormonal and double adenomas (22, 9.21%), null cell adenomas (20, 8.4%), and somatotroph adenomas (3, 1.26%). 64 pathological results that were not based on latest WHO criteria and lack of transcription factors evaluation were excluded. Furthermore, Ki-67 labeling index was ≥ 5% in 19 patients (7.95%), < 3% in 178 patients (74.48%) and 3%-5% in 42 patients (17.57%). Positive staining for P53 was 14.64%, and 200 patients (83.68%) were negative and 4 patients (1.67%) had weak staining (Table 3).
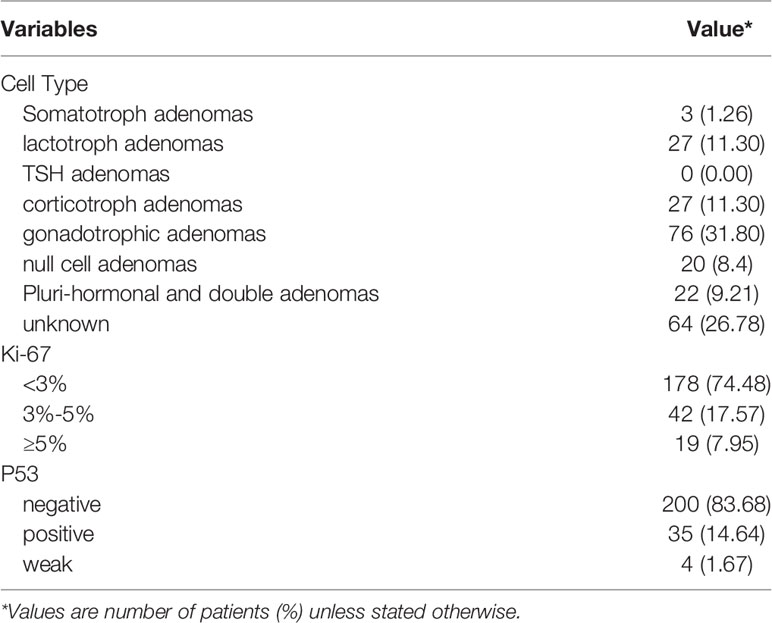
Table 3 Pathological characteristics.
Surgical Procedure
All patients underwent TSS, of which 168 patients (70.29%) were treated with neuroendoscopy and 71 (29.71%) with microscopy. The average operating duration was 143.18 ± 80.26 minutes (range, 46-475 minutes) and the mean intraoperative blood loss was 160.46 ± 285.71ml (range, 10-3500 ml). Four cases had more than 1000 ml of intraoperative blood loss. In addition, the two-nostril approach was taken in 39 cases and 200 patients were treated with the one-nostril approach. The mean length of stay after surgery was 9.59 ± 7.52 days and 7 patients were hospitalized for more than 1 month, mainly because of endocrine dysfunction and intracranial infection. According to postoperative MRI, GTR was achieved in 46 cases (19.25%), NTR in 56 cases (23.43%), STR in 68 cases (28.45%) and PR in 69 cases (28.87%). Improvement of vision was achieved in 133 patients (76.00%). Endocrine tests were performed 3 days, 1 week, and 3 months postoperatively. Sixty-five patients with functional giant PAs achieved endocrine remission after TSS. All details are summarized in Table 4.
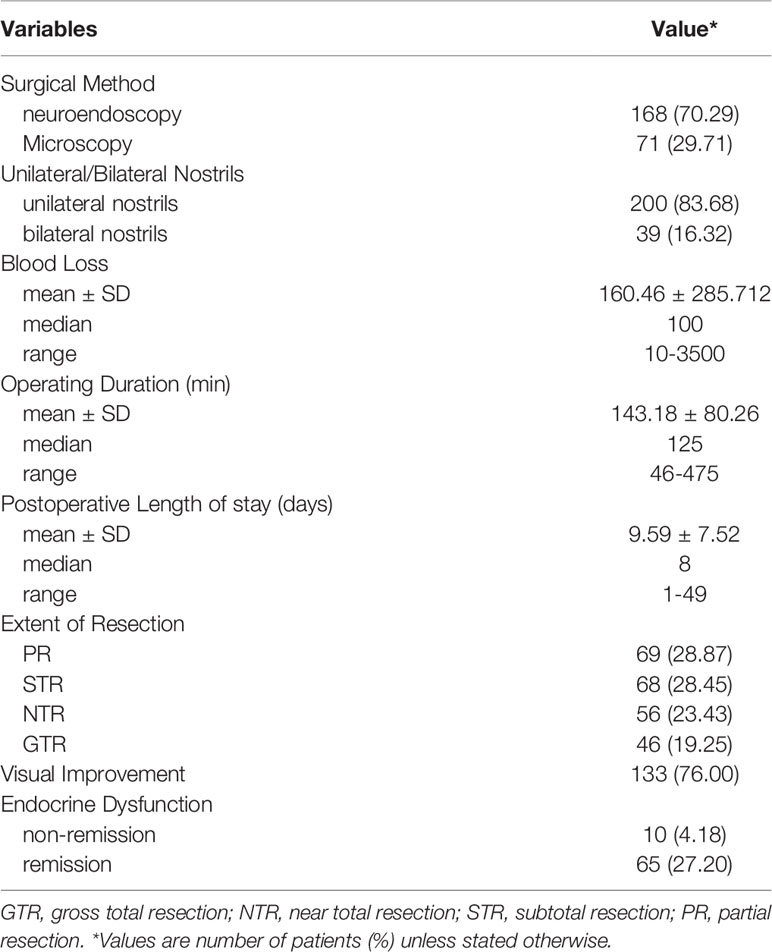
Table 4 Surgical characteristics.
A total of 193 patients (80.75%) experienced surgical complications (Table 5), and the most common complication was postoperative diabetes insipidus (DI), which occurred in 91 patients (38.08%). The incidence of intracranial infection and cerebrospinal fluid (CSF) leaks was 15.48% (13) and 15.06% (14) respectively. Furthermore, 18 patients with CSF leaks developed secondary intracranial infections, and 8 patients experienced postoperative intracranial hemorrhage due to abundant tumor blood supply and inadequate hemostasis of residual tumor. Cranial nerve palsies were observed in 5 cases, all of whom experienced impaired visual field and limited eye movement. One patient experienced intraoperative internal carotid artery injury and was discharged after interventional therapy. Two patients died of intracranial infection and multiorgan failure. In addition, there was a significant difference in the incidence of CSF leaks between the neuroendoscopy and the microscopy groups (P < 0.05) (Table 6).
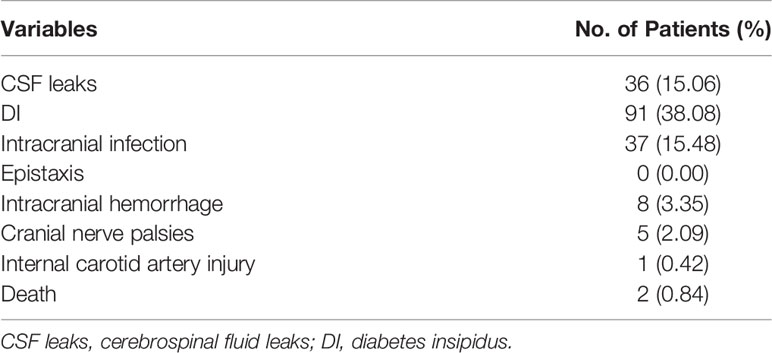
Table 5 Surgical complications.

Table 6 Complications comparison of ETTS and MTTS.
Risk Factors of Extent of Resection
The effect of various tumor characteristics on the extent of resection are outlined in Table 7, factors (P > 0.05) including age, gender, functional status, surgical method, unilateral/bilateral nostrils, tumor shape, invasion characteristics, Ki-67 labeling index, P53 were not significantly correlated with the extent of resection. Univariate analysis showed the maximum diameter of giant PAs maybe a significant factor limiting the extent of resection (P < 0.05). In the ordinal logistic regression model, the OR of maximum diameter was 0.95 (P < 0.05; 95%CI: 0.92-0.98) (Table 8). The Knosp grade was showed a significant effect on the extent of resection (P < 0.001). GTR was more likely achieved in giant PAs with lower Knosp grade, especially Knosp grade 0-1 (P < 0.05; OR: 2.96; 95%CI: 1.27, 6.90) (Table 8).
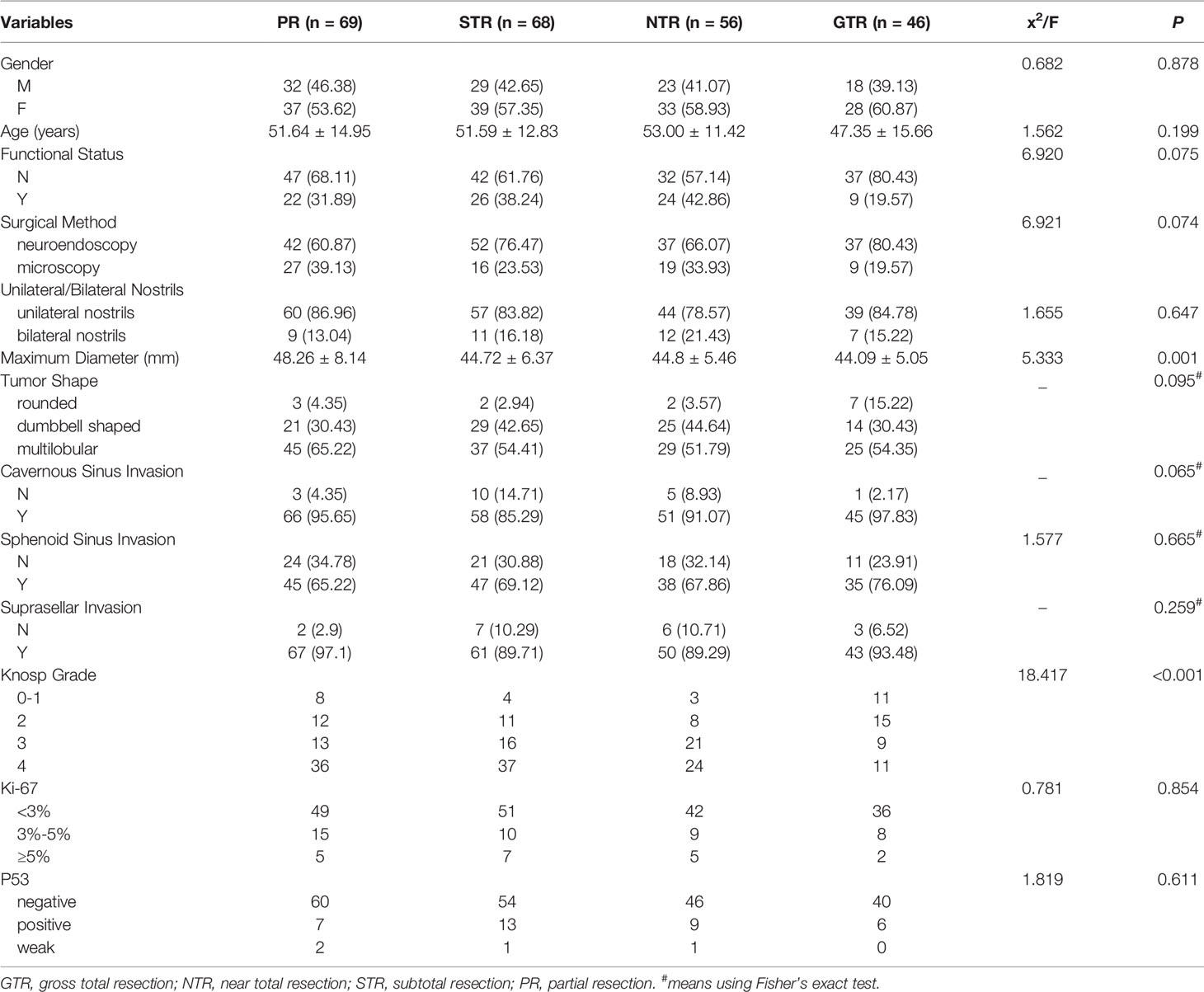
Table 7 The effect of various tumor characteristics on the extent of resection.
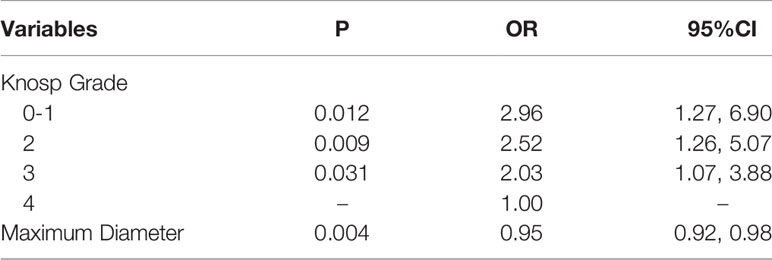
Table 8 Ordinal logistic regression for factors of GTR.
Discussion
Although relatively rare, giant PAs present significant challenges in terms of surgical resection and postoperative management on account of their size and frequent invasion into the surrounding normal tissues. In this study, we retrospectively analyzed the clinical data and surgical outcomes of 239 patients with giant PAs, and identified risk factors for the extent of resection.
Around 6-10% of PAs are defined as giant PAs based on their largest diameter (15, 16). A total of 2829 patients with PAs were treated at our center from January 2015 to October 2021, of which 8.4% had giant PAs. The frequency of the clinically non-functioning giant PAs (158; 66.11%) was twice as high as that of the functioning adenomas (81; 33.89%). This finding is consistent with that reported by Pedro et al. (6). This could be due to the difficulty in detecting silent PAs till they grow to a certain size and become symptomatic. Furthermore, 16 cases of clinically non-functioning giant PAs were confirmed as corticotroph adenomas, which are commonly found in large size of PAs and have been recognized as a more aggressive subtype of pituitary adenomas (17).
TSS is the first-line treatment for giant PAs (18) except the prolactinomas that can be effectively treated with dopamine agonists. The main goals of surgical resection of PAs are the restoration of normal pituitary function, nerve and vascular decompression, and minimal damage to the surrounding tissues. Since the 1990s, the endoscopic endonasal transsphenoidal (EETS) approach has been widely practiced for its improved surgical visualization (19–22), since endoscopes with angled lenses can be used to access areas that are not visible under a microscope. Komotar et al. conducted a systematic review (1995–2010) to compare the outcomes of EETS and microscopic transsphenoidal approach (MTS), and found the EETS group had higher rates of GTR (47.2%) compared to the MTS group (30.9%) (23). Michael et al. further reported significantly higher mean reduction of tumor volume with EETS (91%) compared to MTS (63%) in a cohort of 72 patients with giant PAs (21). In this study, the extent of resection in the EETS group was higher than that in the MTS group, albeit without statistical significance.
Giant PAs are associated with a higher surgical complication rate compared to normal PAs, and the most common complications are DI, CSF leaks, postoperative intracranial hemorrhage, intracranial infections, cranial nerve palsies, hypopituitarism and epistaxis (12, 24, 25). Consistent with previous reports (25–28), the three most frequent complications in our cohort were DI (91, 38.08%) and 6 patients developed permanent DI, CSF leaks (36, 15.06%), and intracranial infection (37, 15.48%). DI is caused by posterior pituitary disfunction, and its incidence rate typically ranges from 9% to 22%, and may increase up to 53% at some centers (29–34). Nevertheless, only 2-7% of the patients develop permanent DI (35,36). PA patients with visual abnormalities, suprasellar extension or large tumors are at a higher risk of developing DI postoperatively (36), which could be the reason for the high incidence of DI in our cohort.
CSF leaks are generally the result of surgical injury and tumor invasion, especially in case of giant PAs with anterior cranial fossa extension (37) and suprasellar expansion (14). In our cohort, most cases of CSF leaks occurred during tumor removal. After reconstructing the skull base with the vascularized nasoseptal flap or the fascia and subcutaneous fat of the thigh, the CSF leaks in most patients receded within 3-6 days. In addition, we found that the rate of CSF leaks was higher in the EETS group than in the MTS group, which was consistent with the results of Yoshua et al. (13). This may be related to the imaging features of neuroendoscopy, which only provides 2D images without the important depth and three-dimensional sense. A previous study reported a significant association between CSF leak and postoperative intracranial infection (38), indicating that despite advanced skull base reconstruction and antibiotic treatment, some patients with CSF leaks may still develop intracranial infection. In this study, 37 patients experienced intracranial infection and 2 patients died as a result. Therefore, intracranial infection still represents a common and feared complication of this approach.
In our cohort, postoperative intracranial hemorrhage was reported in 8 (3.35%) cases. This is a terrible postoperative complication, which can cause great risk to the patient’s life and economic pressure. Residual tumor and inadequate hemostasis were main reasons for this complication, so extreme caution should be exercised after giant PAs surgery. Once a hematoma in the operative cavity is found, an early evacuation of the hematoma and decompression of cranial nerve are urgent needed.
Internal carotid artery rupture is a rare complication but carries the greatest risk of short-term mortality, and there are reports describing fatal bleeds from damaged carotid arteries (39–41). In this study, one patient experienced internal carotid artery damage and formed a false aneurysm, which was managed by interventional endovascular treatment. In addition, cranial nerves are easily damaged during resection of tumors invading the cavernous sinus. Therefore, maintaining a strictly midline approach, familiarity with MRI results and the use of Doppler ultrasound is essential for neurovascular protection.
Since gross total resection is the optimal surgical outcome of giant PAs, we identified independent risk factors of the extent of resection in order to plan a suitable surgical strategy. Tumor size and the invasiveness of giant PAs into surrounding structures are key factors that limit the extent of resection. In our study, we found that each 1 mm increase in tumor diameter corresponded to a 5% decrease in the chance of achieving a GTR. Likewise, giant PAs with Knosp grades 0-1, 2 and 3 were more than twice as likely to achieve GTR compared to those with grade 4 (Table 8). Therefore, both the maximum diameter and the Knosp grade are independent factors of the extent of resection. Sanmillan et al. (42) also identified tumor volume and the Knosp grade as independent risk factors of the extent of resection in a study conducted on 294 patients with PAs, and found that the Knosp grade had a greater impact. Consistent with this, we found that some giant PAs with low Knosp grade could be satisfactorily removed despite their large size. Thus, cavernous sinus invasion of the PAs is crucial for planning surgical procedures, and tumor size can provide complementary information.
The primary aim of identifying risk factors limiting the extent of resection is to guide the neurosurgeons to distinguish the operation terminal and avoid complex complications rather than achieve complete removal of giant PAs. Therefore, the ultimate goals of the surgical resection of giant PAs are decompression of neurovascular structures, especially the optic nerve and internal carotid artery, relieving endocrine dysfunction and controlling the tumor progression, instead of gross total resection of the giant PAs. However, this study has certain limitations that are largely related to its single-center retrospective nature, and a longer follow-up and multicenter cohort are needed to validate our results.
Data Availability Statement
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
Ethics Statement
The studies involving human participants were reviewed and approved by Ethics Committee of Second Affiliated Hospital, School of Medicine, Zhejiang University. Written informed consent for participation was not required for this study in accordance with the national legislation and the institutional requirements.
Author Contributions
YC and XX performed the analysis and co-wrote the manuscript. LW, XX, YJ, FC, SC, and JC collected the patient information. WY and YH revised paper. QW and JZ supervised the project, conceived the study, and guided the editing of the manuscript. YC and XX contributed equally to the manuscript. QW and JZ are corresponding authors. All authors contributed to the article and approved the submitted version.
Conflict of Interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher’s Note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
References
1. Ostrom QT, Gittleman H, Truitt G, Boscia A, Kruchko C, Barnholtz-Sloan JS. CBTRUS Statistical Report: Primary Brain and Other Central Nervous System Tumors Diagnosed in the United States in 2011-2015. Neuro Oncol (2018) 20(suppl_4):iv1–iv86. doi: 10.1093/neuonc/noy131
2. Chen Y, Wang CD, Su ZP, Chen YX, Cai L, Zhuge QC, et al. Natural History of Postoperative Nonfunctioning Pituitary Adenomas: A Systematic Review and Meta-Analysis. Neuroendocrinology (2012) 96(4):333–42. doi: 10.1159/000339823
3. Raverot G, Jouanneau E, Trouillas J. Management of Endocrine Disease: Clinicopathological Classification and Molecular Markers of Pituitary Tumours for Personalized Therapeutic Strategies. Eur J Endocrinol (2014) 170(4):R121–32. doi: 10.1530/EJE-13-1031
4. Müslüman AM, Cansever T, Yılmaz A, Kanat A, Oba E, Çavuşoğlu H, et al. Surgical Results of Large and Giant Pituitary Adenomas With Special Consideration of Ophthalmologic Outcomes. World Neurosurg (2011) 76(1-2):141–8; discussion 63-6. doi: 10.1016/j.wneu.2011.02.009
5. Chen Y, Cai F, Cao J, Gao F, Lv Y, Tang Y, et al. Analysis of Related Factors of Tumor Recurrence or Progression After Transnasal Sphenoidal Surgical Treatment of Large and Giant Pituitary Adenomas and Establish a Nomogram to Predict Tumor Prognosis. Front Endocrinol (2021) 12:793337. doi: 10.3389/fendo.2021.793337
6. Iglesias P, Rodríguez Berrocal V, Díez JJ. Giant Pituitary Adenoma: Histological Types, Clinical Features and Therapeutic Approaches. Endocrine (2018) 61(3):407–21. doi: 10.1007/s12020-018-1645-x
7. Fallah N, Taghvaei M, Sadaghiani S, Sadrhosseini SM, Esfahanian F, Zeinalizadeh M. Surgical Outcome of Endoscopic Endonasal Surgery of Large and Giant Pituitary Adenomas: An Institutional Experience From the Middle East. World Neurosurg (2019) 132:e802–e11. doi: 10.1016/j.wneu.2019.08.004
8. Pratheesh R, Rajaratnam S, Prabhu K, Mani SE, Chacko G, Chacko AG. The Current Role of Transcranial Surgery in the Management of Pituitary Adenomas. Pituitary (2013) 16(4):419–34. doi: 10.1007/s11102-012-0439-z
9. de Paiva Neto MA, Vandergrift A, Fatemi N, Gorgulho AA, Desalles AA, Cohan P, et al. Endonasal Transsphenoidal Surgery and Multimodality Treatment for Giant Pituitary Adenomas. Clin Endocrinol (2010) 72(4):512–9. doi: 10.1111/j.1365-2265.2009.03665.x
10. Goel A, Nadkarni T, Muzumdar D, Desai K, Phalke U, Sharma P. Giant Pituitary Tumors: A Study Based on Surgical Treatment of 118 Cases. Surg Neurol (2004) 61(5):436–45; discussion 45-6. doi: 10.1016/j.surneu.2003.08.036
11. Mortini P, Barzaghi R, Losa M, Boari N, Giovanelli M. Surgical Treatment of Giant Pituitary Adenomas: Strategies and Results in a Series of 95 Consecutive Patients. Neurosurgery (2007) 60(6):993–1002; discussion 3-4. doi: 10.1227/01.NEU.0000255459.14764.BA
12. Juraschka K, Khan OH, Godoy BL, Monsalves E, Kilian A, Krischek B, et al. Endoscopic Endonasal Transsphenoidal Approach to Large and Giant Pituitary Adenomas: Institutional Experience and Predictors of Extent of Resection. J Neurosurg (2014) 121(1):75–83. doi: 10.3171/2014.3.JNS131679
13. Esquenazi Y, Essayed WI, Singh H, Mauer E, Ahmed M, Christos PJ, et al. Endoscopic Endonasal Versus Microscopic Transsphenoidal Surgery for Recurrent and/or Residual Pituitary Adenomas. World Neurosurg (2017) 101:186–95. doi: 10.1016/j.wneu.2017.01.110
14. do Amaral LC, Reis BL, Ribeiro-Oliveira A Jr., da Silva Santos TM, Giannetti AV. Comparative Study of Complications After Primary and Revision Transsphenoidal Endoscopic Surgeries. Neurosurg Rev (2021) 44(3):1687–702. doi: 10.1007/s10143-020-01360-w
15. Mohr G, Hardy J, Comtois R, Beauregard H. Surgical Management of Giant Pituitary Adenomas. Can J Neurol Sci Le J Canadien Des Sci Neurol (1990) 17(1):62–6. doi: 10.1017/s0317167100030055
16. Trouillas J, Roy P, Sturm N, Dantony E, Cortet-Rudelli C, Viennet G, et al. A New Prognostic Clinicopathological Classification of Pituitary Adenomas: A Multicentric Case-Control Study of 410 Patients With 8 Years Post-Operative Follow-Up. Acta Neuropathol (2013) 126(1):123–35. doi: 10.1007/s00401-013-1084-y
17. Cho HY, Cho SW, Kim SW, Shin CS, Park KS, Kim SY. Silent Corticotroph Adenomas Have Unique Recurrence Characteristics Compared With Other Nonfunctioning Pituitary Adenomas. Clin Endocrinol (Oxf) (2010) 72(5):648–53. doi: 10.1111/j.1365-2265.2009.03673.x
18. Wang WF, Yang LH, Han L, Li MJ, Xiao JQ. Efficacy of Transsphenoidal Surgery for Pituitary Tumor: A Protocol for Systematic Review. Medicine (2019) 98(6):e14434. doi: 10.1097/MD.0000000000014434
19. Jho HD, Carrau RL. Endoscopic Endonasal Transsphenoidal Surgery: Experience With 50 Patients. J Neurosurg (1997) 87(1):44–51. doi: 10.3171/jns.1997.87.1.0044
20. Cappabianca P, Alfieri A, de Divitiis E. Endoscopic Endonasal Transsphenoidal Approach to the Sella: Towards Functional Endoscopic Pituitary Surgery (FEPS). Minim Invasive Neurosurg: MIN (1998) 41(2):66–73. doi: 10.1055/s-2008-1052019
21. Cusimano MD, Kan P, Nassiri F, Anderson J, Goguen J, Vanek I, et al. Outcomes of Surgically Treated Giant Pituitary Tumours. Can J Neurol Sci Le J Canadien Des Sci Neurol (2012) 39(4):446–57. doi: 10.1017/s0317167100013950
22. Sanchez MM, Karekezi C, Almeida JP, Kalyvas A, Castro V, Velasquez C, et al. Management of Giant Pituitary Adenomas: Role and Outcome of the Endoscopic Endonasal Surgical Approach. Neurosurg Clin N Am (2019) 30(4):433–44. doi: 10.1016/j.nec.2019.05.004
23. Komotar RJ, Starke RM, Raper DM, Anand VK, Schwartz TH. Endoscopic Endonasal Compared With Microscopic Transsphenoidal and Open Transcranial Resection of Giant Pituitary Adenomas. Pituitary (2012) 15(2):150–9. doi: 10.1007/s11102-011-0359-3
24. Koutourousiou M, Gardner PA, Fernandez-Miranda JC, Paluzzi A, Wang EW, Snyderman CH. Endoscopic Endonasal Surgery for Giant Pituitary Adenomas: Advantages and Limitations. J Neurosurg (2013) 118(3):621–31. doi: 10.3171/2012.11.JNS121190
25. Gondim JA, Almeida JP, Albuquerque LA, Gomes EF, Schops M. Giant Pituitary Adenomas: Surgical Outcomes of 50 Cases Operated on by the Endonasal Endoscopic Approach. World Neurosurg (2014) 82(1-2):e281–90. doi: 10.1016/j.wneu.2013.08.028
26. Xue-Fei S, Yong-Fei W, Shi-Qi L, Jing-Song W, Yao Z, Ying M, et al. Microsurgical Treatment for Giant and Irregular Pituitary Adenomas in a Series of 54 Consecutive Patients. Br J Neurosurg (2008) 22(5):636–48. doi: 10.1080/02688690802346083
27. Sinha S, Sharma BS. Giant Pituitary Adenomas–an Enigma Revisited. Microsurgical Treatment Strategies and Outcome in a Series of 250 Patients. Br J Neurosurg (2010) 24(1):31–9. doi: 10.3109/02688690903370305
28. Rahimli T, Hidayetov T, Yusifli Z, Memmedzade H, Rajabov T, Aghayev K. Endoscopic Endonasal Approach to Giant Pituitary Adenomas: Surgical Outcomes and Review of the Literature. World Neurosurg (2021) 149:e1043–e55. doi: 10.1016/j.wneu.2021.01.019
29. Devin JK. Hypopituitarism and Central Diabetes Insipidus: Perioperative Diagnosis and Management. Neurosurg Clinics North Am (2012) 23(4):679–89. doi: 10.1016/j.nec.2012.06.001
30. Kadir ML, Islam MT, Hossain MM, Sultana S, Nasrin R, Hossain MM. Incidence of Diabetes Insipidus in Postoperative Period Among the Patients Undergoing Pituitary Tumour Surgery. Mymensingh Med J: MMJ (2017) 26(3):642–9.
31. Nemergut EC, Zuo Z, Jane JA Jr., Laws ER Jr. Predictors of Diabetes Insipidus After Transsphenoidal Surgery: A Review of 881 Patients. J Neurosurg (2005) 103(3):448–54. doi: 10.3171/jns.2005.103.3.0448
32. Qari FA, AbuDaood EA, Nasser TA. Diabetes Insipidus Following Neurosurgery at a University Hospital in Western Saudi Arabia. Saudi Med J (2016) 37(2):156–60. doi: 10.15537/smj.2016.2.12848
33. Zhan R, Ma Z, Wang D, Li X. Pure Endoscopic Endonasal Transsphenoidal Approach for Nonfunctioning Pituitary Adenomas in the Elderly: Surgical Outcomes and Complications in 158 Patients. World Neurosurg (2015) 84(6):1572–8. doi: 10.1016/j.wneu.2015.08.035
34. Constantino ER, Leal R, Ferreira CC, Acioly MA, Landeiro JA. Surgical Outcomes of the Endoscopic Endonasal Transsphenoidal Approach for Large and Giant Pituitary Adenomas: Institutional Experience With Special Attention to Approach-Related Complications. Arq Neuropsiquiatr (2016) 74(5):388–95. doi: 10.1590/0004-282X20160042
35. Vance ML. Perioperative Management of Patients Undergoing Pituitary Surgery. Endocrinol Metab Clinics North Am (2003) 32(2):355–65. doi: 10.1016/s0889-8529(03)00003-3
36. Nayak P, Montaser AS, Hu J, Prevedello DM, Kirschner LS, Ghalib L. Predictors of Postoperative Diabetes Insipidus Following Endoscopic Resection of Pituitary Adenomas. J Endocr Soc (2018) 2(9):1010–9. doi: 10.1210/js.2018-00121
37. Karnezis TT, Baker AB, Soler ZM, Wise SK, Rereddy SK, Patel ZM, et al. Factors Impacting Cerebrospinal Fluid Leak Rates in Endoscopic Sellar Surgery. Int Forum Allergy Rhinol (2016) 6(11):1117–25. doi: 10.1002/alr.21783
38. Parikh A, Adapa A, Sullivan SE, McKean EL. Predictive Factors, 30-Day Clinical Outcomes, and Costs Associated With Cerebrospinal Fluid Leak in Pituitary Adenoma Resection. J Neurol Surg Part B Skull Base (2020) 81(1):43–55. doi: 10.1055/s-0039-1679896
39. Ahuja A, Guterman LR, Hopkins LN. Carotid Cavernous Fistula and False Aneurysm of the Cavernous Carotid Artery: Complications of Transsphenoidal Surgery. Neurosurgery (1992) 31(4):774–8; discussion 8-9. doi: 10.1227/00006123-199210000-00025
40. Kachhara R, Menon G, Bhattacharya RN, Nair S, Gupta AK, Gadhinglajkar S, et al. False Aneurysm of Cavernous Carotid Artery and Carotid Cavernous Fistula: Complications Following Transsphenoidal Surgery. Neurol India (2003) 51(1):81–3. doi: 10.1179/016164103101201247
41. Reddy K, Lesiuk H, West M, Fewer D. False Aneurysm of the Cavernous Carotid Artery: A Complication of Transsphenoidal Surgery. Surg Neurol (1990) 33(2):142–5. doi: 10.1016/0090-3019(90)90024-j
Keywords: giant pituitary adenoma, transsphenoidal surgery, CSF leak, Knosp grade, extent of resection
Citation: Chen Y, Xu X, Cao J, Jie Y, Wang L, Cai F, Chen S, Yan W, Hong Y, Zhang J and Wu Q (2022) Transsphenoidal Surgery of Giant Pituitary Adenoma: Results and Experience of 239 Cases in A Single Center. Front. Endocrinol. 13:879702. doi: 10.3389/fendo.2022.879702
Received: 20 February 2022; Accepted: 08 April 2022;
Published: 06 May 2022.
Edited by:
Congxin Dai, Capital Medical University, ChinaReviewed by:
Andrea Glezer, University of São Paulo, BrazilGao Dakuan, The Fourth Military Medical University, China
Copyright © 2022 Chen, Xu, Cao, Jie, Wang, Cai, Chen, Yan, Hong, Zhang and Wu. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Qun Wu, 2192010@zju.edu.cn; Jianmin Zhang, zjm135@zju.edu.cn
†These authors have contributed equally to this work and share first authorship