 Renata Lazari Sandoval1*
Renata Lazari Sandoval1* Natalia Polidorio1
Natalia Polidorio1 Ana Carolina Rathsam Leite1
Ana Carolina Rathsam Leite1 Mariana Cartaxo2
Mariana Cartaxo2 Janina Pontes Pisani3Carla Vanessa Quirino3Loureno Cezana4
Janina Pontes Pisani3Carla Vanessa Quirino3Loureno Cezana4 Natálya Gonçalves Pereira5
Natálya Gonçalves Pereira5 Allan Andresson Lima Pereira1
Allan Andresson Lima Pereira1 Benedito Mauro Rossi3,5
Benedito Mauro Rossi3,5 Maria Isabel Achatz3
Maria Isabel Achatz3- 1Oncology Center, Hospital Sírio-Libanês, Brasília, Brazil
- 2Oncology Center, Hospital Nossa Senhora das Neves, João Pessoa, Brazil
- 3Oncology Center, Hospital Sírio-Libanês, São Paulo, Brazil
- 4Oncology Center, Hospital Santa Rita de Cássia, Vitoria, Brazil
- 5Genetics and Genomics Department, Beneficência Portuguesa, São Paulo, Brazil
Breast cancer (BC) is the most prevalent malignancy in women with Li-Fraumeni syndrome (LFS). The literature on BC in LFS is limited due to its rarity worldwide. A TP53 founder pathogenic variant (c.1010G>A; p.R337H) is responsible for the higher prevalence of this syndrome among women of Brazilian ancestry.
Purpose: The aim of the study was to describe the BC phenotype expressed by Brazilian female LFS carriers and compare the data between p.R337H and other TP53 germline pathogenic/likely pathogenic variants (non-p.R337H carriers).
Methods: We searched for cases of TP53 germline pathogenic/likely pathogenic variant carriers affected by BC included between 2015 and 2020 in the BLiSS (Brazilian Li-Fraumeni Study) registry at the Sírio-Libanês Hospital.
Results: Among 163 adult female carriers from the registry, 91 (56%) had received a BC diagnosis, including 72 p.R337H carriers. BC was the first cancer diagnosed in 90% of cases. Early onset BC (age ≤45 years) was diagnosed in 78.2% of cases (11.5% <31 years; 66.7% 31–45 years; 21.8% >45 years). The median age of BC diagnosis for p.R337H carriers was 39.5 years (range 20–69 years) compared to 34 years (range 21–63 years) for non-p.R337H carriers (p = 0.009). In total, 104 breast tumors were observed in 87 women. Bilateral BC was observed in 29.3% of cases. Histology was available for 96 tumors, comprising 69 invasive breast carcinomas, which were mostly invasive ductal carcinomas (95.6%), 25 ductal in situ carcinomas and 2 soft-tissue sarcomas. Overall, 90.5% of invasive breast carcinomas were hormone receptor (HR)-positive, 39.5% were human epidermal growth factor receptor 2 (HER2)-positive, and 32.8% showed HR and HER2 co-expression. In addition, 55.4% of patients opted for contralateral prophylactic mastectomy after a first BC diagnosis. There were no significant differences in the risk of developing contralateral BC or in the immunohistochemical profile between p.R337H and non-p.R337H groups.
Conclusions: The expressed phenotype of p.R337H is similar to that of other TP53 pathogenic/likely pathogenic variants, except for an average older age at the onset of disease; however, this is still younger than the general population.
Introduction
Li-Fraumeni syndrome (LFS; OMIM 151623) is an autosomal dominant condition that is associated with an increased risk of developing cancer. It is caused by TP53 germline pathogenic/likely pathogenic (P/LP) variants. Breast cancer (BC) is the most common cancer diagnosed in women with LFS (1–6). The lifetime risk of BC in women with LFS has been estimated to range 54–85% (7). The risk of BC increases from 20 years of age and peaks at approximately 40 years (7, 8). The median age for the onset of BC is approximately 32–34 years (2, 6, 9).
LFS is highly prevalent in the Southern and Southeastern areas of Brazil, due to the presence of the TP53 founder variant c.1010G>A (p.Arg337His), also known as variant p.R337H (10, 11). The p.R337H is a missense pathogenic variant (substitution of arginine for histidine at codon 337), located in exon 10, in the oligomerization domain of the protein p53. The frequency of TP53 p.R337H variant carriers among Brazilian women diagnosed with BC varies from 0.9 to 12%, depending on the geographical region of the studied population and age of BC onset (12–17).
It has been suggested that LFS caused by the TP53 variant p.R337H has a moderate penetrance when compared to that caused by other TP53 germline P/LP variants (non-p.R337H) (10, 18, 19). The majority of p.R337H carriers do not fulfill the classic clinical criteria for LFS (20), whereas the frequency of BC in this population is similar to that described in non-p.R337H carriers (10). Nevertheless, age-dependent penetrance seems to be different, less than 20% of p.R337H carriers develop BC before 30 years of age compared to 50% of non-p.R337H carriers, suggesting an age-related penetrance (21).
TP53 carriers usually have hormone receptor (HR)-positive and human epidermal growth factor receptor 2 (HER2)-positive BCs (22–27). Fitarelli-Kiehl et al. (25) suggested that in p.R337H carriers with BC, there are less HER2-positive tumors. However, there is a lack of available literature that focuses on p.R337H carriers. This information may impact strategic planning for chemoprevention, treatment, and surveillance in this high-risk population.
In this study, we sought to describe the BC phenotype of Brazilian female carriers of LFS and compare the BC features displayed between carriers of the p.R337H and other TP53 P/LP variants.
Materials and Methods
Study Design
All study subjects were participants of the BLiSS (Brazilian Li-Fraumeni Study) registry at the Sírio-Libanês Hospital, Brazil. The eligibility criteria for the current analysis included a confirmed germline P/LP variant in the gene TP53 and a personal history of BC. Germline testing was performed by commercial laboratories determined by health insurance coverage agreements or out of pocket payment. Cases were ascertained by Sanger sequencing and MLPA (Multiplex Ligation-dependent Probe Amplification), multigene next generation sequencing panels or point mutation sequencing. This study was approved by the Research Ethics Committee of Sírio-Libanês Hospital and the Brazilian Research Ethics Committee (CAAE: 02433418.5.0000.5461). All participants provided informed consent.
Ductal carcinoma in situ (DCIS), invasive breast carcinoma (IBC), and breast soft-tissue sarcoma (STS) cases were included. Carriers of more than one P/LP germline variant for an autosomal dominant BC susceptibility gene, possibly mosaic TP53 P/LP carriers and carriers of TP53 variants with conflicting data of pathogenicity were excluded from the analysis (Supplementary Figure 1).
All personal and family history data were ascertained by certified medical geneticists. All clinical and molecular data were de-identified before data sharing and analysis. The collected data included description of the TP53 germline P/LP variant, age at BC diagnosis, history of unilateral or bilateral BC (synchronous or metachronous), histological subtype and tumor immunohistochemical (IHC) profile, surgical management (lumpectomy vs. mastectomy), contralateral risk reduction mastectomy (CRRM) uptake after a first BC diagnosis, number of primary cancers, and family history of cancer (first, second, or third degree relatives).
All pathology and IHC reports were re-examined. The HR status of the tumor was considered positive if nuclei staining for the estrogen receptor and/or progesterone receptor was greater than or equal to 1%, according to ASCO/CAP guidelines (28). Estrogen receptor (ER) expression of 1–10% was considered ER-low-positive. Additional data based on updated clinical guidelines for BC subtype classification (29) are also available in the supplementary material (Supplementary Table 1).
The HER2 expression was recorded using the following scale; 0 for no staining, 1+ for weak cytoplasmic membrane staining in any proportion of tumor cells, 2+ for moderate cytoplasmic membrane staining in at least 10% of tumor cells, and 3+ for intense cytoplasmic membrane staining in at least 30% of tumor cells. Scores of 0 and 1+ were considered negative for HER2 expression. In case of equivocal HER2 expression (score 2+), only samples that had data showing positive detection for HER2 by fluorescent in situ hybridization (FISH) were included in the analysis.
Statistical Analysis
Data were tested for normality using the Kolmogorov–Smirnov and Shapiro–Wilk tests. Values were expressed as medians and percentiles for non-normal continuous variables, and as means and standard deviations for normal continuous variables. Categorical data were presented as absolute values and percentages and were tested using the Pearson χ2 and Fisher exact tests, where applicable. Quantitative data were compared by applying Student’s t-test for comparison of the two groups for normally distributed variables and Mann–Whitney U test for non-normally distributed ones. Statistical significance was set at p ≤0.05. Analyses were performed using the SPSS version 21.0 (IBM, NY, USA) software.
Results
A total of 91 out of 163 (56%) female TP53 germline P/LP variant carriers had a personal history of BC, and of these, 82 (90%) had BC as the first type of cancer presentation. Furthermore, 72 of the carriers with a personal history of BC harbored the TP53 p.R337H variant. Other 14 distinct germline TP53 P/LP variants were identified in the non-p.R337H carriers. To reduce possible bias, carriers of the variants p.D49H, p.R156H, and p.V147A were excluded from the analysis because of conflicting data on pathogenicity (30), which left 15 carriers (17.2%) in the non-p.R337H group (Supplementary Table 2). Geographic information about the cohort is detailed in the supplementary material (Supplementary Table 3), most of the participants (57/87, 65.5%) lived in the states of São Paulo and Distrito Federal.
The median age at BC diagnosis in the overall cohort was 38 years (range 20–69 years). In addition, 11% (10/87) of the patients were diagnosed under the age of 31, 66.7% (58/87) between 32 and 45 years, and 21.8% above 45 years old. The median age at BC diagnosis in the p.R337H group was 39.5 years (range 20–69 years), which was significantly higher than that observed in the non-p.R337H group (median age 34 years; range 21-63 years; p = 0.009). Furthermore, 43% (31/72) of the p.R337H carriers with BC fulfilled the revised Chompret criteria for LFS (31), in comparison to 60% (9/15) of the non-p.R337H carriers with BC (p = 0.231). All collected data and subgroup analyses are presented in Table 1.
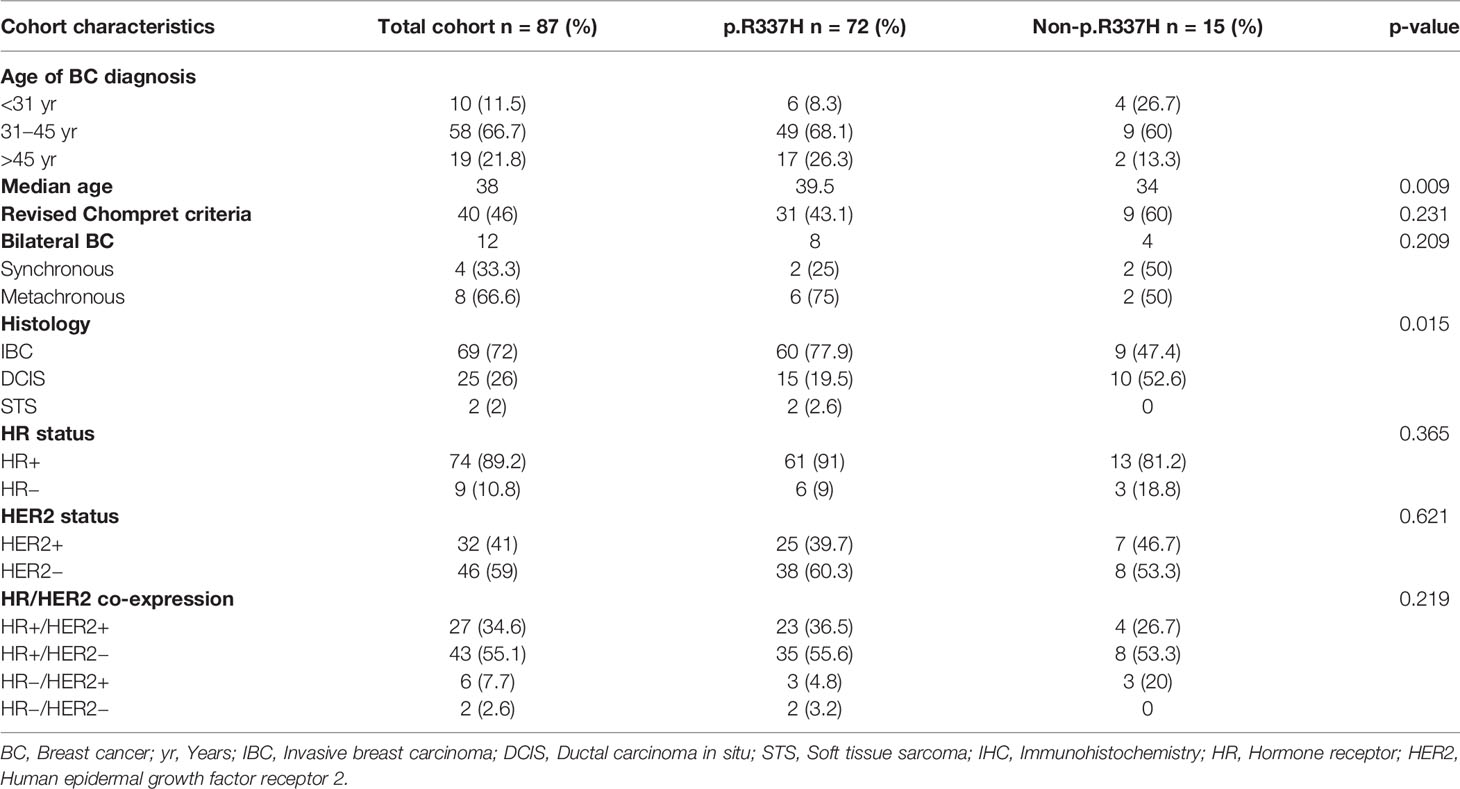
Table 1 Clinical and pathological characteristics of p.R337H and non-p.R337H carriers.
The type of breast surgery was available for 76 patients; 38% of the patients had undergone lumpectomies and 62% had undergone mastectomies. There were 46 patients that had opted for CRRM after a first BC diagnosis, which represented 55.4% of the patients. Cases of synchronous bilateral BC were excluded from the CRRM analysis. Only one patient (1/46, 2.1%) developed BC in the residual breast tissue after prophylactic mastectomy.
There were 17 patients that developed more than one primary BC and the interval between the first and second BC diagnosis ranged from 0 to 21 years. Moreover, 29.3% of the patients (12/41) were affected by bilateral BC, which included four cases of synchronous BC and eight cases of metachronous BC. Cases of CRRM after the first BC diagnosis were excluded from the bilateral breast cancer analysis.
A total of 104 breast tumors were described in the 87 LFS carriers. Pathology reports were available for 96 cases, including 69 IBCs (66 invasive ductal carcinomas and 3 invasive lobular carcinomas), 25 DCISs, and 2 breast STSs. Only 2 patients were diagnosed with invasive lobular carcinomas, out of which, one patient was diagnosed with bilateral synchronous disease at the age of 42. The other patient underwent bilateral mastectomy after a first DCIS diagnosis at the age of 56, but later developed axillary lymph node metastasis from an occult breast carcinoma in the contralateral breast at the age of 63. Both patients were p.R337H carriers.
Among DCIS cases with available HR status, from the total cohort, 85% (17/20) were HR-positive (HR+). The majority of tumors from non-p.R337H carriers were DCIS (p = 0.015). In addition, 90.5% of the total IBCs with available HR status (57/63) were HR+ and 39.5% (24/61) were HER2-positive (HER2+). HR/HER2 co-expression analysis in invasive tumors showed that 57.4% (35/61) were HR+/HER2−, 32.8% were HR+/HER2+, 6.5% were HR−/HER2+, and 3.3% were HR−/HER2−. There were no significant differences found between the p.R337H and non-p.R337H variants groups with regard to HR, HER2 status and HR/HER2 co-expression (Table 1). Forty-five IBCs had detailed information about percentage of estrogen receptor expression (>1%, 1–10%, >10%). ER-low-positive IBC represented 6.5% (3/45) of the total IBC samples. According to the St Gallen consensus (29), 33.5% (15/45) of the tumors were luminal A, 31% luminal B-HER2 positive, 20% luminal B-HER2 negative, 13.5% HER2 enriched, 2.2% triple negative (Supplementary Table 1).
Discussion
BC is the most common malignancy in women worldwide. It is the most frequent tumor diagnosed in women with LFS (2–6). LFS carriers have a higher risk of BC, young-onset cancers, multiple primary cancers, and radioinduced tumors (5–8). Therefore, providing adequate screening and follow-up appointments according to the Toronto protocol may enable early cancer detection and reduce cancer morbidity and mortality (32, 33).
Women with LFS should start BC awareness at the age of 18 years and have regular breast MRIs from the age of 20 years or at least 5 years before the earliest diagnosis of BC in the family if this is younger than 20 years of age (34). Risk-reduction mastectomy is an option for primary prevention (35). Early stage disease can be treated with total mastectomy instead of lumpectomy to avoid radiation exposure. Despite these options, there is still limited data available on BCs in LFS patients, especially in relation to p.R337H carriers.
Brazilian LFS carriers are mostly represented by p.R337H carriers, even though other TP53 germline variants are also found in this population (25, 36, 37). Likewise, although the majority of the LFS carriers in this study harbored the p.R337H variant, 17.2% of the cohort harbored other TP53 germline P/LP variants. The median age for BC onset in p.R337H carriers was significantly higher (p = 0.009) than the median age of diagnosis in the non-p.R337H group (39.5 versus 34 years, respectively). Similar results have been reported in other studies (9, 23, 25–27, 36). However, it is important to highlight that p.R337H carriers are affected in a lower age than that expected for the general population. Approximately three quarters of our p.R337H cohort with BC were diagnosed before the age of 45 years, and therefore, early high risk screening should be offered to p.R337H carriers.
In this study, almost 60% of the p.R337H group and 40% of the non-p.R337H group failed to fulfill the revised Chompret criteria for LFS. This finding may reflect the suboptimal sensitivity and specificity of LFS clinical criteria (3, 31). A new LFS classification was recently proposed by Kratz et al. (38), which states that TP53 germline P/LP variant carriers who do not meet the LFS classic or Chompret testing criteria should be defined as attenuated LFS. However, the impact of the new classification in the screening and management of LFS has not yet been determined.
In Brazil, it is estimated that between 0.9 and 12% of women diagnosed with BC carry a germline pathogenic variant of the gene TP53 (12–17). As clinical criteria are not sufficient to identify all carriers, the cost-effectiveness of universal TP53 testing in the Brazilian BC population should be evaluated. The same reasoning has previously been applied to pathogenic founder variants detected in the Ashkenazi Jewish population, where BRCA universal screening has already been validated (39).
The risk of developing bilateral/contralateral BC ranges between 4 and 70% for LFS female carriers (9, 23, 26, 27, 35, 40). The wide range of this percentage is thought to be due to differences in sample size, study design, and follow-up period between investigations. Furthermore, an association has been made between patient age at the first BC diagnosis and the risk of developing metachronous contralateral BC (40). Bougeard et al. (5) examined the clinical findings recorded from a large cohort of 214 families with LFS, including 415 TP53 pathogenic variant carriers (non-p.R337H), who were monitored over a 20 year period. The study found that the risk of developing contralateral BC in non-p.R337H LFS carriers was 31%, which is close to the 29.3% risk observed in the p.R337H enriched cohort in the current study.
After the first BC diagnosis, 55% of the cohort opted for CRRM. Therefore, it is proposed that knowledge of TP53 germline status may influence surgical decision making, although whether genetic testing was performed before or after BC diagnosis was not addressed in the present study. Siegel et al. (35) observed a high uptake (65%) of CRRM in women diagnosed with LFS, particularly in those with an early diagnosis. This corroborates the statistics recorded for CRRM in BRCA positive patients (41, 42).
Immunohistochemical features of BC are used routinely to predict prognosis, determine treatment, and plan chemoprevention; and hence, studies incorporating these data are important in the context of LFS. Indeed, it has been shown that HR+ tumors are common in sporadic BC and in BC diagnosed in LFS carriers (9, 22, 23, 26, 27, 43); and the results from this study are in accordance with those of previous studies. It is possible that chemoprevention through hormonal therapy may play a role in preventing BC in LFS carriers, and future studies should evaluate this as a potential preventive treatment. Treatment-oriented classification of subgroups of BC has evolved in the last decade (28, 29, 44, 45). Previous published LFS BC studies considered ER-positive cut off greater than or equal to 1% (9, 25–27), nevertheless, updated guidelines (28, 29) incorporated the concept of ER-low-positive due to its potential impact in prognosis and predictive role in neoadjuvant chemotherapy response (44). Our study observed 6.5% (3/45) of ER-low-positive IBCs. The retrospective design of our study imposed some limitations regarding missing/not available data. The frequency of ER-low-positive tumors should be systematically assessed in prospective LFS BC studies.
HER2+ tumors are associated with higher mortality (43), and TP53 P/LP variant carriers are more likely to have HER2+ breast tumors (9, 22–24, 26, 27). According to some studies, BCs that are found in p.R337H carriers are less likely to be HER2+ than those detected in non-R337H TP53 P/LP variant carriers (24, 25). It can be noted that although Fortuno et al. (24) observed a lower proportion of HER2+ breast tumors in p.R337H carriers when compared to non-R337H TP53 P/LP variant carriers, this difference was only significant for the age group of 40–49 years. Furthermore, another study that reported similar findings had included BC samples with equivocal HER2 amplification that had not been confirmed by FISH analysis in the test set (25). The current study showed that 41.5% of IBCs from p.R337H carriers were HER2+. Special attention should be made when comparing LFS BC published data in relation to HER2 status. The clinical relevance of HER2 positivity is well established for IBC (45). The significance of HER2 overexpression in DCIS is not well defined (46). Packwood et al. (26) and Kuba et al. (27) have included IBCs and DCISs to calculate overall HER2 positivity. Other studies used the term ‘breast tumors’ but were not clear about the inclusion of IBCs and/or DCISs (24, 25).
In the present study there was a recruitment bias. The majority of the participants were carriers of the founder pathogenic variant p.R337H and lived in the Southeast and Central-West of the country (Supplementary Table 3). Although this founder variant was initially found to be present in the Brazilian population from the South and Southeastern areas, the existence of p.R337H variant carriers in the Central-West of the country suggests that internal migrations may be responsible for the spread of the founder variant through different regions of Brazil.
Although the present study included the largest BC cohort of p.R337H carriers to date (n = 72), the retrospective design of the study imposed a few limitations. It would be beneficial to establish a Brazilian prospective cohort with cancer affected and unaffected LFS carriers in order to identify potential risk modifiers of BC, such as environmental exposures, breast feeding, previous cancer treatment, and family history of BC. In addition, it would be useful to examine the consequences of the TP53 germline status on oncological treatment approaches and the effects of intensive surveillance on morbidity. The Brazilian population offers a unique opportunity for a better understanding of LFS in the context of TP53 p.R337H variant carriers. Therefore, Brazilian academic and medical institutions should add efforts for the creation of a National LFS Registry.
Finally, female carriers of the LFS TP53 p.R337H variant have a high risk of BC and bilateral disease. The p.R337H variant has a similar phenotype to TP53 non-R337H P/LP variants, except for a slightly older onset age for BC (which is still considered a young age for BC onset). For these reasons, carriers of the p.R337H variant should follow the same management guidelines as TP53 non-R337H P/LP carriers.
Data Availability Statement
The original contributions presented in the study are included in the article/Supplementary Material, further inquiries can be directed to the corresponding author.
Ethics Statement
The studies involving human participants were reviewed and approved by the Ethics Committee of Hospital Sírio-Libanês and the Brazilian Research Ethics Committee (CAAE: 02433418.5.0000.5461). The patients/participants provided their written informed consent to participate in this study.
Author Contributions
Concept and Design: RLS. Acquisition, analysis, or interpretation of data: RLS, NP, MC, JPP, CVQ, ACRL, LC, NGP, AALP, BMR, and MIA. Drafting of the manuscript: RLS and MIA. Critical revision of the manuscript for important intellectual content: RLS, NP, MC, JPP, CVQ, ACRL, LC, NGP, AALP, BMR, and MIA. Supervision: RLS and MIA. All authors listed have made a substantial, direct, and intellectual contribution to the work and approved it for publication.
Funding
We received financial support from the Stand Up to Cancer (SU2C) for this study.
Conflict of Interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher’s Note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Supplementary Material
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fonc.2022.836937/full#supplementary-material
References
1. Garber JE, Goldstein AM, Kantor AF, Dreyfus MG, Fraumeni JF Jr, Li FP. Follow-Up Study of Twenty-Four Families With Li–Fraumeni Syndrome. Cancer Res (1991) 51(22):6094–7.
2. Olivier M, Goldgar DE, Sodha N, Ohgaki H, Kleihues P, Hainaut P, et al. Li–Fraumeni and Related Syndromes: Correlation Between Tumor Type, Family Structure, and TP53 Genotype. Cancer Res (2003) 63(20):6643–50.
3. Gonzalez KD, Noltner KA, Buzin CH, Gu D, Wen-Fong CY, Nguyen VQ, et al. Beyond Li Fraumeni Syndrome: Clinical Characteristics of Families With P53 Germline Mutations. J Clin Oncol (2009) 27(8):1250–6. doi: 10.1200/JCO.2008.16.6959
4. Ruijs MW, Verhoef S, Rookus MA, Pruntel R, van der Hout AH, Hogervorst FB, et al. TP53 Germline Mutation Testing in 180 Families Suspected of Li–Fraumeni Syndrome: Mutation Detection Rate and Relative Frequency of Cancers in Different Familial Phenotypes. J Med Genet (2010) 47(6):421–8. doi: 10.1136/jmg.2009.073429
5. Bougeard G, Renaux-Petel M, Flaman JM, Charbonnier C, Fermey P, Belotti M, et al. Revisiting Li–Fraumeni Syndrome From TP53 Mutation Carriers. J Clin Oncol (2015) 33(21):2345–52. doi: 10.1200/JCO.2014.59.5728
6. Amadou A, Achatz MIW, Hainaut P. Revisiting Tumor Patterns and Penetrance in Germline TP53 Mutation Carriers: Temporal Phases of Li–Fraumeni Syndrome. Curr Opin Oncol (2018) 30(1):23–9. doi: 10.1097/CCO.0000000000000423
7. Mai PL, Best AF, Peters JA, DeCastro RM, Khincha PP, Loud JT, et al. Risks of First and Subsequent Cancers Among TP53 Mutation Carriers in the National Cancer Institute Li–Fraumeni Syndrome Cohort. Cancer (2016) 122(23):3673–81. doi: 10.1002/cncr.30248
8. Shin SJ, Dodd-Eaton EB, Gao F, Bojadzieva J, Chen J, Kong X, et al. Penetrance Estimates Over Time to First and Second Primary Cancer Diagnosis in Families With Li–Fraumeni Syndrome: A Single Institution Perspective. Cancer Res (2020) 80(2):347–53. doi: 10.1158/0008-5472.CAN-19-0725
9. Masciari S, Dillon DA, Rath M, Robson M, Weitzel JN, Balmana J, et al. Breast Cancer Phenotype in Women With TP53 Germline Mutations: A Li–Fraumeni Syndrome Consortium Effort. Breast Cancer Res Treat (2012) 133(3):1125–30. doi: 10.1007/s10549-012-1993-9
10. Achatz MI, Olivier M, Le Calvez F, Martel-Planche G, Lopes A, Rossi BM, et al. The TP53 Mutation, R337H, is Associated With Li-Fraumeni and Li-Fraumeni-Like Syndromes in Brazilian Families. Cancer Lett (2007) 245(1-2):96–102. doi: 10.1016/j.canlet.2005.12.039
11. Garritano S, Gemignani F, Palmero EI, Olivier M, Martel-Planche G, Le Calvez-Kelm F, et al. Detailed Haplotype Analysis at the TP53 Locus in P.R337H Mutation Carriers in the Population of Southern Brazil: Evidence for a Founder Effect. Hum Mutat (2010) 31(2):143–50. doi: 10.1002/humu.21151
12. Assumpção JG, Seidinger AL, Mastellaro MJ, Ribeiro RC, Zambetti GP, Ganti R, et al. Association of the Germline TP53 R337H Mutation With Breast Cancer in Southern Brazil. BMC Cancer (2008) 8:357. doi: 10.1186/1471-2407-8-357
13. Giacomazzi J, Graudenz MS, Osorio CA, Koehler-Santos P, Palmero EI, Zagonel-Oliveira M, et al. Prevalence of the TP53 P.R337H Mutation in Breast Cancer Patients in Brazil. PloS One (2014) 9(6):e99893. doi: 10.1371/journal.pone.0099893
14. Hahn EC, Bittar CM, Vianna FSL, Netto CBO, Biazús JV, Cericatto R, et al. TP53 P.Arg337His Germline Mutation Prevalence in Southern Brazil: Further Evidence for Mutation Testing in Young Breast Cancer Patients. PloS One (2018) 13(12):e0209934. doi: 10.1371/journal.pone.0209934
15. Mathias C, Bortoletto S, Centa A, Komechen H, Lima RS, Fonseca AS, et al. Frequency of the TP53 R337H Variant in Sporadic Breast Cancer and its Impact on Genomic Instability. Sci Rep (2020) 10(1):16614. doi: 10.1038/s41598-020-73282-y
16. Sandoval RL, Leite ACR, Barbalho DM, Assad DX, Barroso R, Polidorio N, et al. Germline Molecular Data in Hereditary Breast Cancer in Brazil: Lessons From a Large Single-Center Analysis. PloS One (2021) 16(2):e0247363. doi: 10.1371/journal.pone.0247363
17. Felix GE, Abe-Sandes C, Machado-Lopes TM, Bomfim TF, Guindalini RS, Santos VC, et al. Germline Mutations in BRCA1, BRCA2, CHEK2 and TP53 in Patients at High-Risk for HBOC: Characterizing a Northeast Brazilian Population. Hum Genome Var (2014) 1:14012. doi: 10.1038/hgv.2014.12
18. Ribeiro RC, Sandrini F, Figueiredo B, Zambetti GP, Michalkiewicz E, Lafferty AR, et al. An Inherited P53 Mutation That Contributes in a Tissue-Specific Manner to Pediatric Adrenal Cortical Carcinoma. Proc Natl Acad Sci U S A (2001) 98(16):9330–5. doi: 10.1073/pnas.161479898
19. Pinto EM, Zambetti GP. What 20 Years of Research has Taught Us About the TP53 P.R337H Mutation. Cancer (2020) 126(21):4678–86. doi: 10.1002/cncr.33143
20. Li FP, Fraumeni JF Jr, Mulvihill JJ, Blattner WA, Dreyfus MG, Tucker MA, et al. A Cancer Family Syndrome in Twenty-Four Kindreds. Cancer Res (1988) 48(18):5358–62.
22. Wilson JR, Bateman AC, Hanson H, An Q, Evans G, Rahman N, et al. A Novel HER2-Positive Breast Cancer Phenotype Arising From Germline TP53 Mutations. J Med Genet (2010) 47(11):771–4. doi: 10.1136/jmg.2010.078113
23. Melhem-Bertrandt A, Bojadzieva J, Ready KJ, Obeid E, Liu DD, Gutierrez-Barrera AM, et al. Early Onset HER2-Positive Breast Cancer is Associated With Germline TP53 Mutations. Cancer (2012) 118(4):908–13. doi: 10.1002/cncr.26377
24. Fortuno C, Mester J, Pesaran T, Weitzel JN, Dolinsky J, Yussuf A, et al. Suggested Application of HER2+ Breast Tumor Phenotype for Germline TP53 Variant Classification Within ACMG/AMP Guidelines. Hum Mutat (2020) 41(9):1555–62. doi: 10.1002/humu.24060
25. Fitarelli-Kiehl M, Giacomazzi J, Santos-Silva P, Graudenz MS, Palmero EI, Michelli RA, et al. The Breast Cancer Immunophenotype of TP53-P.R337H Carriers is Different From That Observed Among Other Pathogenic TP53 Mutation Carriers. Fam Cancer (2015) 14(2):333–6. doi: 10.1007/s10689-015-9779-y
26. Packwood K, Martland G, Sommerlad M, Shaw E, Moutasim K, Thomas G, et al. Breast Cancer in Patients With Germline TP53 Pathogenic Variants Have Typical Tumour Characteristics: The Cohort Study of TP53 Carrier Early Onset Breast Cancer (COPE Study). J Pathol Clin Res (2019) 5(3):189–98. doi: 10.1002/cjp2.133
27. Kuba MG, Lester SC, Bowman T, Stokes SM, Taneja KL, Garber JE, et al. Histopathologic Features of Breast Cancer in Li-Fraumeni Syndrome. Mod Pathol (2021) 34(3):542–8. doi: 10.1038/s41379-020-0610-4
28. Allison KH, Hammond MEH, Dowsett M, McKernin SE, Carey LA, Fitzgibbons PL, et al. Estrogen and Progesterone Receptor Testing in Breast Cancer: ASCO/CAP Guideline Update. J Clin Oncol (2020) 38(12):1346–66. doi: 10.1200/JCO.19.02309
29. Coates AS, Winer EP, Goldhirsch A, Gelber RD, Gnant M, Piccart-Gebhart M, et al. Tailoring Therapies–Improving the Management of Early Breast Cancer: St Gallen International Expert Consensus on the Primary Therapy of Early Breast Cancer 2015. Ann Oncol (2015) 26(8):1533–46. doi: 10.1093/annonc/mdv221
30. Fortuno C, Lee K, Olivier M, Pesaran T, Mai PL, de Andrade KC, et al. ClinGen TP53 Variant Curation Expert Panel. Specifications of the ACMG/AMP Variant Interpretation Guidelines for Germline TP53 Variants. Hum Mutat (2021) 42(3):223–36. doi: 10.1002/humu.24152
31. Tinat J, Bougeard G, Baert-Desurmont S, Vasseur S, Martin C, Bouvignies E, et al. Version of the Chompret Criteria for Li Fraumeni Syndrome. J Clin Oncol (2009) 27(26):e108–9; author reply e110. doi: 10.1200/JCO.2009.22.7967
32. Villani A, Shore A, Wasserman JD, Stephens D, Kim RH, Druker H, et al. Biochemical and Imaging Surveillance in Germline TP53 Mutation Carriers With Li-Fraumeni Syndrome: 11 Year Follow-Up of a Prospective Observational Study. Lancet Oncol (2016) 17(9):1295–305. doi: 10.1016/S1470-2045(16)30249-2
33. Tak CR, Biltaji E, Kohlmann W, Maese L, Hainaut P, Villani A, et al. Cost-Effectiveness of Early Cancer Surveillance for Patients With Li-Fraumeni Syndrome. Pediatr Blood Cancer (2019) 66(5):e27629. doi: 10.1002/pbc.27629
34. Frebourg T, Bajalica Lagercrantz S, Oliveira C, Magenheim R, Evans DG. European Reference Network GENTURIS. Guidelines for the Li–Fraumeni and Heritable TP53-Related Cancer Syndromes. Eur J Hum Genet (2020) 28(10):1379–86. doi: 10.1038/s41431-020-0638-4
35. Siegel A, Bremer RC, Klein WMP, Savage SA, Loud JT, Khincha PP. Uptake and Timing of Bilateral and Contralateral Risk-Reducing Mastectomy in Women With Li-Fraumeni Syndrome. Breast Cancer Res Treat (2022) 191(1):159–67. doi: 10.1007/s10549-021-06410-5
36. Petry V, Bonadio RC, Cagnacci AQC, Senna LAL, Campos RDNG, Cotti GC, et al. Radiotherapy-Induced Malignancies in Breast Cancer Patients With TP53 Pathogenic Germline Variants (Li-Fraumeni Syndrome). Fam Cancer (2020) 19(1):47–53. doi: 10.1007/s10689-019-00153-5
37. Matzenbacher Bittar C, de Araújo Rocha YM, Vieira IA, Rosset C, Andreis TF, Sartor ITS, et al. Clinical and Molecular Characterization of Patients Fulfilling Chompret Criteria for Li-Fraumeni Syndrome in Southern Brazil. PloS One (2021) 16(9):e0251639. doi: 10.1371/journal.pone.0251639
38. Kratz CP, Freycon C, Maxwell KN, Nichols KE, Schiffman JD, Evans DG, et al. Analysis of the Li-Fraumeni Spectrum Based on an International Germline TP53 Variant Data Set: An International Agency for Research on Cancer TP53 Database Analysis. JAMA Oncol (2021) 28:e214398. doi: 10.1001/jamaoncol.2021.4398
39. Manchanda R, Legood R, Burnell M, McGuire A, Raikou M, Loggenberg K, et al. Cost-Effectiveness of Population Screening for BRCA Mutations in Ashkenazi Jewish Women Compared With Family History-Based Testing. J Natl Cancer Inst (2015) 107(1):380. doi: 10.1093/jnci/dju380
40. Hyder Z, Harkness EF, Woodward ER, Bowers NL, Pereira M, Wallace AJ, et al. Risk of Contralateral Breast Cancer in Women With and Without Pathogenic Variants in BRCA1, BRCA2, and TP53 Genes in Women With Very Early-Onset (<36 Years) Breast Cancer. Cancers (Basel) (2020) 12(2):378. doi: 10.3390/cancers12020378
41. Segerer R, Peschel C, Kämmerer U, Häussler S, Wöckel A, Segerer S. Factors Impacting on Decision-Making Towards Prophylactic Surgeries in BRCA Mutation Carriers and Women With Familial Predisposition. Breast Care (Basel) (2020) 15(3):253–9. doi: 10.1159/000503370
42. Yadav S, Reeves A, Campian S, Sufka A, Zakalik D. Preoperative Genetic Testing Impacts Surgical Decision Making in BRCA Mutation Carriers With Breast Cancer: A Retrospective Cohort Analysis. Hered Cancer Clin Pract (2017) 15:11. doi: 10.1186/s13053-017-0071-z
43. Harbeck N, Penault-Llorca F, Cortes J, Gnant M, Houssami N, Poortmans P, et al. Breast Cancer. Nat Rev Dis Primers (2019) 5(1):66. doi: 10.1038/s41572-019-0111-2
44. Paakkola NM, Karakatsanis A, Mauri D, Foukakis T, Valachis A. The Prognostic and Predictive Impact of Low Estrogen Receptor Expression in Early Breast Cancer: A Systematic Review and Meta-Analysis. ESMO Open (2021) 6(6):100289. doi: 10.1016/j.esmoop.2021.100289
45. Choong GM, Cullen GD, O’Sullivan CC. Evolving Standards of Care and New Challenges in the Management of HER2-Positive Breast Cancer. CA Cancer J Clin (2020) 70(5):355–74. doi: 10.3322/caac.21634
Keywords: Li-Fraumeni syndrome, TP53, R337H, hereditary breast cancer, early-onset breast cancer
Citation: Sandoval RL, Polidorio N, Leite ACR, Cartaxo M, Pisani JP, Quirino CV, Cezana L, Pereira NG, Pereira AAL, Rossi BM and Achatz MI (2022) Breast Cancer Phenotype Associated With Li-Fraumeni Syndrome: A Brazilian Cohort Enriched by TP53 p.R337H Carriers. Front. Oncol. 12:836937. doi: 10.3389/fonc.2022.836937
Received: 16 December 2021; Accepted: 14 February 2022;
Published: 16 March 2022.
Edited by:
Karen Hubbard, City College of New York (CUNY), United StatesReviewed by:
Natalija Dedić Plavetić, University Hospital Centre Zagreb, CroatiaGilda Alves Brown, Rio de Janeiro State University, Brazil
Copyright © 2022 Sandoval, Polidorio, Leite, Cartaxo, Pisani, Quirino, Cezana, Pereira, Pereira, Rossi and Achatz. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Renata Lazari Sandoval, rsandoval.med@gmail.com