 Tabitha Sen
Tabitha Sen Karen Spruyt
Karen Spruyt- 1School of Biomedical Sciences, Queensland University of Technology, Brisbane, QLD, Australia
- 2Lyon Neuroscience Research Center, INSERM U1028-CNRS UMR 5292, University Claude Bernard, School of Medicine, Lyon, France
Since a thorough review in 2011 by Spruyt, into the integral pitfalls of pediatric questionnaires in sleep, sleep researchers worldwide have further evaluated many existing tools. This systematic review aims to comprehensively evaluate and summarize the tools currently in circulation and provide recommendations for potential evolving avenues of pediatric sleep interest. 144 “tool”-studies (70 tools) have been published aiming at investigating sleep in primarily 6–18 years old per parental report. Although 27 new tools were discovered, most of the studies translated or evaluated the psychometric properties of existing tools. Some form of normative values has been established in 18 studies. More than half of the tools queried general sleep problems. Extra efforts in tool development are still needed for tools that assess children outside the 6-to-12-year-old age range, as well as for tools examining sleep-related aspects beyond sleep problems/disorders. Especially assessing the validity of tools has been pursued vis-à-vis fulfillment of psychometric criteria. While the Spruyt et al. review provided a rigorous step-by-step guide into the development and validation of such tools, a pattern of steps continue to be overlooked. As these instruments are potentially valuable in assisting in the development of a clinical diagnosis into pediatric sleep pathologies, it is required that while they are primary subjective measures, they behave as objective measures. More tools for specific populations (e.g., in terms of ages, developmental disabilities, and sleep pathologies) are still needed.
Introduction
There is significant power in the efficiency and cost-effective nature of questionnaires and surveys as contributors to aetiological discoveries of a wide range of medical disorders. These instruments however, do not always possess the objective nature of medically advised and established tools, e.g., polysomnography, and can become a hindrance to adequate diagnoses, particularly when neglecting recommendations of their development (1). Despite these problems, there has been considerable effort to transform the structure of health questionnaires, specifically in the field of pediatric sleep, to reflect a systematic approach of the highest concordance to medical diagnostic standards. The systematic review by Spruyt et al. (2, 3) in 2011, publicly summarized the shortcomings of questionnaires and their developmental standards while advising a thorough procedure in which to follow to adequately evaluate or develop a tool.
Since this time, a variety of tools have been established, both adhering to and overlooking the recommended steps. More detailed information on the 11 steps can be found in Spruyt et al. (3). Briefly, Step 1 is to reflect on the variable(s) of interest and targeted sample(s). Step 2 is to consider the research question that the instrument will be used to address. Thus, the goal of this step is to reflect on whether the tool will be suitable to collect the type of data required to address your hypothesis. Steps 3 (response format) and Step 4 (items) build on the two preceding steps. They allow us to reflect not only on “which” questions and “which’” answers assesses the variable(s) of interest, but also on “how” a question is formulated and “how” it can be answered. The common goal of steps 1–4 is that we want the underlying “concepts” and/or “assumptions” contained in the questions, such as language (e.g., jargon), meaning and interpretation of the wording to be identically understood by all respondents. Getting as close as this ideal as possible will minimize errors of comprehension and completion. Step 5 involves piloting of your drafted tools. Piloting also prevents disasters with the actual data collection. In fact, Steps 2–5 should be an iterative process, meaning that we do them repeatedly, until a consensus has been reached among experts and/or respondents with descriptive statistics underpinning those decisions. Assessing the performance of individual test items, separately and as a whole, is Step 6 (item analysis). There are two main approaches to item analysis: classical test theory and the item-response theory, either of which should be combined with missing data analysis. The next step is about identifying the underlying concepts of the tool (Step 7 Structure) because only rarely is a questionnaire unidimensional. Steps 8 and 9 are about assessing the reliability and validity, respectively. Reliability does not imply validity, although a tool cannot be considered valid if it is not reliable! Several statistical, or psychometric, tests allow us to assess a tool’s reliability and validity (cfr. textbooks written on this topic). For instance, validation statistics of the tool may involve content validity, face validity, criterion validity, concurrent validity or predictive validity. Step 10 is about verifying the stability, or robustness, of the aforementioned steps. It is the step in which you assess the significance, inference, and confidence (i.e., minimal measurement error) of your tool, using the sample(s) for which it was designed. Step 11 involves standardization and norm development, allowing large-scale usage of your tool.
This review aims to conclude the trends associated with these questionnaires, and reinforce the importance of certain stages of tool development and highlight the direction of research that would be ideal to follow.
Materials and Methods
To achieve consistency and retrieve relevant studies to the Spruyt (2, 3) review, the search terms(*) and databases were mirrored; “Sleep” AND (“infant” OR “child” OR “adolescent”) AND (“questionnaire,” “instrument,” “scale,” “checklist,” “assessment,” “log,” “diary,” “record,” “interview,” “test,” “measure”). The databases included PubMed, Web of Science (WOS), and EBSCOHOST (per PRISMA guidelines). Additional limitations to the search criteria were applied for date and age range of the respective study populations. Database-wide searches were conducted between 18th of April 2010 (Spruyt, 2011 publication date of search) and 1st of January 2020. Age categories listed in PubMed filters between 0 and 18 years were also applied to restrict the search to pediatric populations alone. Contrastingly, language criteria were not specified but post hoc constrained to English. Papers in other languages could not be evaluated by one of the authors, in case a consensus on the psychometric evaluation was needed. The search for relevant studies extended to authors in listserver groups PedSleep2.0 and the International Pediatric Sleep Association (IPSA) in order to achieve maximal inclusion. The refinement of these study characteristics ensured that the systematic review would evaluate relevant studies in pediatric tool development, adaptation, and validation. Final search count was sizeable (refer to Figure 1).
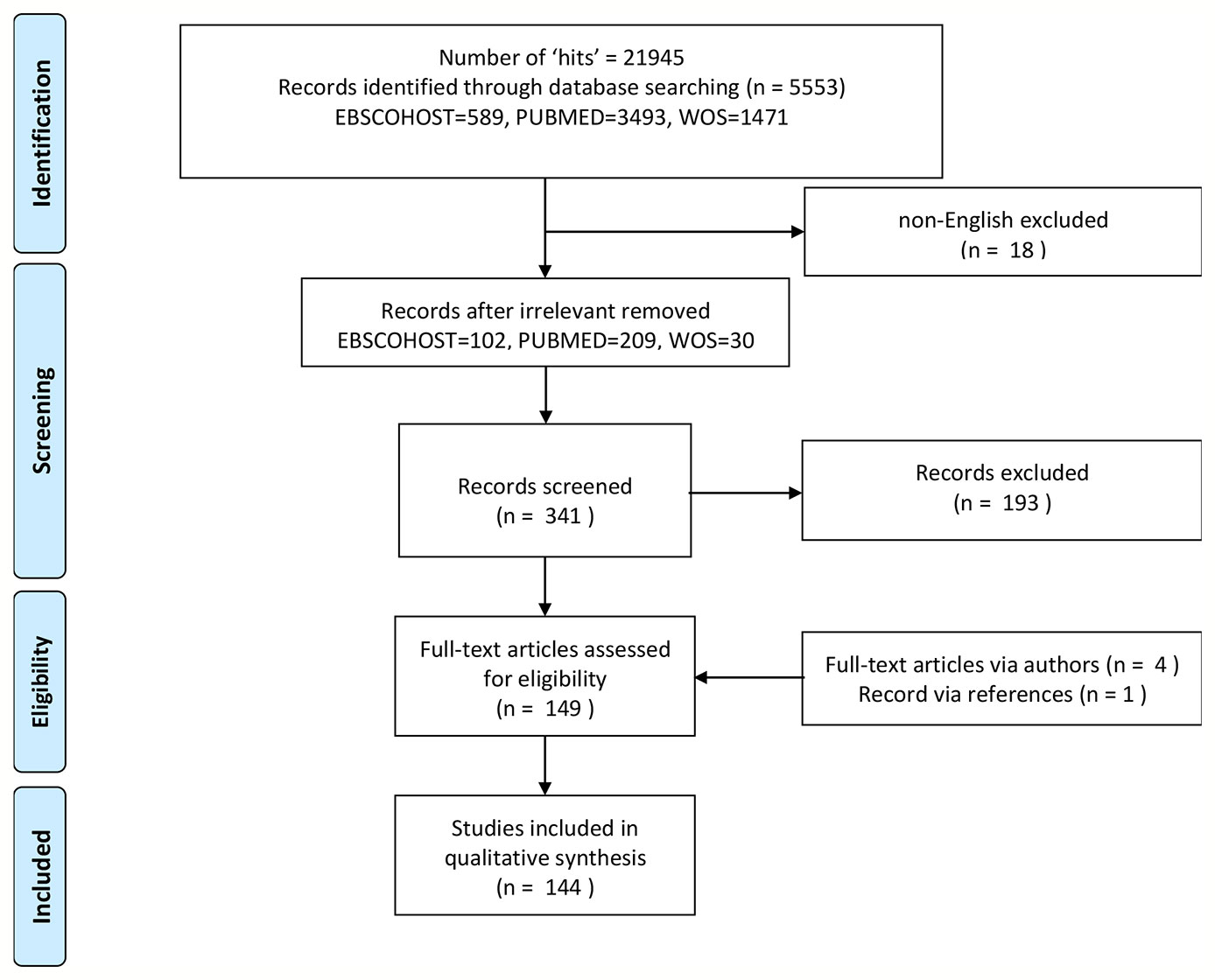
Figure 1 Flowchart of studies included.
Full-text access was achieved through the literary database “Library Genesis” or author contact if necessary (see Acknowledgments). All flagged citations were then manually screened for relevant keywords in their respective titles, abstracts and methods to further refine studies relevant to the systematic review—these being 11 psychometric steps (2, 3) and 7 sleep categories (sleep quantity, sleep quality, sleep regularity, sleep hygiene, sleep ecology, and sleep treatment) (4). Consequently, independent studies were highlighted and screened, and each study’s descriptive variables were extracted and collated. Any absence of indispensable information regarding the tools use was addressed through contact of authors.
Statistical Analysis
A total of 11 steps (2) and 7 sleep categories (4) were extracted and were statistically analyzed for frequency and descriptive assessment (refer to Tables 1 and 2). Any variables unmentioned or neglected were described as “empty,” and tabulated as such in the forthcoming interpretations. Continuous variables will be described as mean values (± standard deviation) and categorical variables will be shown as absolute and relative values. Statistical analyses were performed with Statistica version 13 (StatSoft, Inc. (2009), STATISTICA, Tulsa, OK).

Table 1 Basic information of studies evaluated.
Results
Studies Included
As described by Figure 1, the total number of studies generated from the database search was sizeable, at n=341. Key emphasis of a pediatric diagnostic tools’ use, development or validation deemed it eligible for review, as well as the general translation and consequent adaptation of any pediatric questionnaire, survey, log, diary, etc. The titles and abstracts of each report were screened accordingly, resulting in the omission of 193 articles and final inclusion of 144 articles. Exported abstracts were then assigned their respective full-text. Complete text access was not available for 14, while retrieved from either the literature database “Library Genesis” or via author permission (n=4, see Acknowledgments), leaving 144 or 70 tools eligible for review based on the search conducted.
A more thorough examination of methodological processes was then executed to reveal categories to which each article was suitably assigned for ease of future assessment (refer to Table 1); “New Development (N),” “Psychometric Analysis (P),” and “Translation (T)/Adaptation (A),” or a combination thereof. Each paper was assigned to the appropriate criteria; “Development” if the report’s main purpose was to produce an unprecedented tool, “Psychometric Analysis” if the explicit objective was to assess the reliability and validity of said tool, and “Translation and/or Adaptation” for all studies that in any way translated or altered a tool to suit a specific population, culture, and/or nation. Overall (Table 2), 36.8% of the studies aimed to merely psychometrically evaluate a pediatric sleep tool, while 9% additionally translated it. 24.3% of the studies aimed to independently translate while 4.2% additionally adapted their tool. As for lone adaptations, there were 4.2% of studies that performed this, while 18.8% created an entirely new tool. 1.4% of the studies conducted both a new tool development and translation and alike, 0.7% of studies adapted their new tool to particular population, culture, or other.

Table 2 Overview of psychometric analyses performed.
Study Characteristics
The structural organization and publication features of each study are detailed in Table 1. In the Appendix are the acronyms for each tool reviewed. Since the 2011 Spruyt review on pediatric diagnostic and epidemiological tools, approximately 144 “tool”-studies have been published. The focus into pediatric tool evaluation peaked in 2014 where 16.7% of all studies were conducted, closely followed by 2017 (13.9%), and 2016 and 2019, each at 13.2% as well as 2015 at 12.5%. As for the remaining years of this decade, between 2010 and 2014, 2018 , the percentage of total studies published ranged from 0.7%–9.7% (n=1–10) per year. Over a third of the total studies were published in Europe (38.9%), followed by North America (25%), Asia (18.1%), Middle East (2.8%), South America (7.6%), Australia and Oceania (6.3%), and the United Kingdom (1.4%).
Across all 144 studies evaluated, it was evident that sleep tools were predominantly developed and evaluated for a combination of children and adolescents between the ages of 6–18 years (27.1%), followed closely by tools for adolescents 13–18 years at 22.2% and children 6–12 years alone at 16.7%. Only 10 studies covered the 0–18 years age range, and one did not define its range (82). Meanwhile, only 5.6% of all the studies assessed tools for preschool-aged children (2–5 years) alone and 1.4% for infants (0–23 months) alone. As for the studies remaining, a combination of age ranges was investigated with the most predominant combination being both preschool children and children (ages of 2–12 years) at 8.3% of the total studies. The lesser frequent combinations of age ranges for which tools were assessed in these studies, ranged from 0.7–7.6% per combination.
As for the sample size, this ranged between 20 and 11,626 children inclusive of adult (6–13) participants across all publications, where 15.6% of all studies used a sample size >1,000 participants large (Table 2). Of these study samples, approximately 46.5% of respondents were parents, 41% were self-report, and 11.1% either a combination of experts, children, mothers, and parents. For two, the respondent is primarily a professional (17, 95).
Sleep Categories
As exemplified in Table 2, the overall focus of these studies was overwhelmingly directed at tools measuring the quality of sleep or identification of sleep pathologies in all pediatric age classifications (68.1%), followed by the levels of sleepiness (55.6%) and duration of sleep (48.6%). Various secondary coobjectives of these studies were to investigate tools measuring the sleep regularity (46.5%) and sleep hygiene practices (29.2%). Rarely but in existence, was the singular assessment of sleep ecology and treatment around sleep pathologies at a frequency of 21.5% and 0.7%, respectively. About 19 studies (13.2%) queried simultaneously nearly all categories (except treatment).
The 11 Steps
Regarding the psychometric evaluation step-by-step guide proposed by Spruyt (2, 3), less than half the required 11 steps (chiefly 1, 2, 6, 8, and 9 were done) were fulfilled across all studies. Steps 3 and 10 were often not reported (i.e., 84.7% and 63.2%, respectively). Three studies reported all steps (2.1%), three only lack step 11 (2.1%), and four (2.8%) only lack steps 10 and 11. The most common combination of steps (7.7%) reported are 1, 2, and 4 joined with 5, 6, 7, 8, 9 or 5, 6, 8, 9 or 6, 7, 8, 9, 10. After a decade, only 18 papers (12.5%) reported some form of norms. An in-depth description of the steps fulfilled is described in the categorically-divided (per purpose, see Methods) results below.
Tools Newly Developed
According to our search criteria, a total of 27 novel pediatric sleep tools were developed between 2010 and 2020 (refer to Table 2 and shaded). Of these, approximately eight were published in Europe (29.6%), eight in North America (29.6%), four in Asia (14.8%), three in South America (11.1%), two in Australia and Oceania (7.4%), and two in the United Kingdom (7.4%). The majority were developed for child-adolescent age ranges (66.7%), while one for preschool children (2–5 years) and one for all three aforementioned ages (2–18 years). All newly developed tools possessed a multipurpose objective, most of which assessed sleep quality (77.8%), followed by the assessment of sleepiness (51.9%) and sleep regularity (41.7%) and sleep quantity (41.7%), while more rarely assessing hygiene (25%), ecology (12.5%), and treatment (4.2%).
In addition, three tools being newly created are an English translation of the NARQoL-21 (70) and YSIS (140), and also an adaptation, the nighttime sleep diary (NSD) (71). The latter being a diary adapted to monitor nighttime fluctuations in young children with asthma.
Only two tools were developed according to the 11 aforementioned steps required for psychometric validation of a tool; the NARQoL-21 (70) and SNAKE (129) (refer to Table 2). One other tool, OSPQ (83) also developed normative scores for widespread usage while fulfilling most steps but steps 3 and 9. Whereas the CSAQ (27) fulfilled all steps except step 11, and the BRIAN-K (16), PADSS (84), and SDSC* (125) except steps 10 and 11. The outstanding tools were mostly absent of steps 5, 7, 8, 9, and 10. For the newly developed diary, NSD (71) steps 1–6 were fulfilled.
Almost half of the tools queried general sleep problems (41.7%). Twenty-five percent aimed at surveying sleep disordered breathing. While others such as sleep bruxism (128), PADSS (84), P-RLS-SS (98), RLS (117), NARQoL-21(70), YSIS (140), and NSD (71) focused on a specific sleep problem (16.7%). Tools aimed at investigating sleep complaints in children with (developmental) disabilities are besides NSD (71), the OSA Screening Questionnaire (73), Pediatric Sleep CGIs (90), SHIP (127), and SNAKE (129).
Tools Translated
In total, 35 out of the total 144 studies primarily aimed to translate an existing tool alone (refer to Table 2). Namely, 17 tools have been translated: BISQ (15), CCTQ (19), CSHQ (29, 33, 34, 40–43), CSM (45), CSRQ (46), DBAS (49), ISI (56, 57), MEQ (62), OSA-18 (74–79), OSD-6 (81), PDSS (85–87), PosaST (96), PSQ (105–107, 110, 111, 113), PSQI (115), SDSC (120–122), SHI (126), and SSR (43, 133). The most frequently translated tools were: OSA-18 (17.1%), CSHQ (14.3%), and PSQ (11.4%). The most common translation was to Portuguese (n=4), Spanish (n=4), and Turkish (n=4), followed by Brazilian Portuguese (n=3), Chinese (n=3), and Dutch (n=3). Less often, tools were translated to German, Persian, and Greek as well as English, Italian, Polish, Swedish, Japanese, French, Malay, and Thai. Again, primarily tools for child/adolescent age ranges as parental reports have been translated. Of these, the main categorical foci, and often overlapping, were sleep quality (77.1%), quantity (48.6%), and sleepiness (48.6%).
When ranked from most to least prevalent step, apart from steps 1 and 2, we found: step 8 (97.1%), step 4 (91.4%), step 9 (88.6%), step 6 (85.7%), step 5 (57.1%), step 7 (51.4%), and step 10 (34.3%) being performed across the studies. The CSHQ (34) and SDSC (120, 121) included norm development (step 11). Step 3 is missing in all translations. Only the translation of the SDSC fulfilled nearly all steps with (121) missing step 3 and (120) missing steps 3 and 9. Receiver Operator Curve (ROC) analyses were performed in five : OSA-15 (74), PosaST (96), PSQ (106, 111), and CSHQ (43).
Tools Adapted
Moreover, six studies (see Table 2) specifically aimed to adapt a tool from a preexisting one, most notably the Children’s Sleep Habits Questionnaire (CSHQ) (66.7%), among these a shortened version and infant adaptation, along with the BEDS (14) (16.7%) adapted toward children with Down syndrome, and the OSA-18 Questionnaire (16.7%), which was also shortened [toward OSA-5 (80)] to suit the sample of interest. Although the number of items may have changed, no substantial changes to the answer categories could be noted. Only 33.3% reported steps 3, 4, 5, 7, 10 yet steps 6, 8, 9 were analyzed in 83.3%. None developed norms. In two studies (38, 44) ROC analyses were pursued for the CSHQ.
Tools Adapted and Translated
Six studies adapted and also translated existing tools (see Table 2): CSHQ (29), PedsQL (91, 92), SQS-SVQ (131), TuCASA (139), and NSS (72). The CSQH and TuCASA were adapted and translated to Portuguese, the PedsQL to Arabic and Chinese, while SQS-SVQ to Turkish and NSS to Chinese. The adaptations involved an infant version of CSHQ and child-sample for NSS, the PedsQL to children with cancer and acute leukemia, and the TuCasa was adapted toward children of low socioeconomic status. Regarding the SQS-SVQ it was modified based on personal communication with the authors of the original version. That is, four items were added.
For these tools Steps 3 and 11 were not performed, while Steps 8 and 9 were performed in all. About half (50%) did steps 5, 6, and more than half step 7 (66.7%) and less than half did step 10. Some aspects of step 4 were inconsistently applied across 83.3% of the studies (e.g., expert perspective).
Tools Psychometrically Evaluated
Approximately 53 studies were published that focused solely on psychometric evaluation of questionnaires between 2010 and 2020 (refer to Table 2). Of these, commonly investigated were CSHQ (11.3%), CRSP, and PSQ (each 7.5%), followed by SDSC and PROMIS (each 5.7%). The greatest number were printed in 2014 (15.1%), as well as 2018 and 2019 (each 13.2%) and 2015, 2016, 2017 (each 11.3%), and a lesser number of instruments were evaluated in the other years. In terms of location, the majority were published in North America (43.4%) followed by Europe (22.6%) and Asia (18.9%), Australia and Oceania (11.3%), and the South America (3.8%). Especially tools for adolescent age ranges (34%) were psychometrically evaluated, followed by child-adolescent age range (22.6%). 9.4% involved tools for preschoolers (2–5 years) and 15.1% are for child (6–12 years) alone. The remainder are combinations: preschooler child (3.8%), preschool to adolescent (9.4%), and all (0–18 years; 3.8%).
Ranked on sleep category, the tools examined: 64.2% sleep quality; 58.5% sleep quantity; 47.2% sleep regularity; 58.5% sleepiness; 35.8% sleep hygiene, 20.8% sleep ecology but none for treatment. Among all 53-instrument validations, none adhered to all eleven recommended steps of tool evaluation. Besides steps 1 and 2, especially steps 9 (90.6%) and 8 (75.5%), 6 (64.2%) have been reported upon psychometrically evaluating tools, and less common have been steps 7 (54.7%), 10 (41.5%), and 4 (34%). Least common in psychometric screening were steps 5 (13.2%), 3 (13.2%), and again 11 (15.1%). ROC analyses were performed in 11 studies (20.8%): ESS (52), AIS and SQI (5), JSQ (58, 59), PSQ (108, 109, 112), CAS-15 (17), CSRQ (47), and Comics (138). Almost fulfilling all steps were: CAS-15 (Goldstein et al., 2012) and Comics (137, 138).
Tools Psychometrically Evaluated and Adaptations
Three tools underwent evaluation but were simultaneously modified: FoSI was adapted for adolescents (54), and a reduced itemset was suggested for aMEQ-R (65) and PROMIS (102).
Tools Psychometrically Evaluated and Translated
In addition to the 53 instruments validated, there were 13 studies flagged that additionally translated their respective tools (refer to Table 2); the ASHS to Persian, the BEARS to Spanish, CCTQ to Chinese, the CSHQ to German and Spanish, the ESS to Tamil, the MEQ to European Portuguese, the MESSi to Turkish, the PSQ to Chinese, Portuguese and French, and the PedsQL to Brazilian Portuguese. Step 9 was performed in all studies, closely followed by steps 4, 6, and 8 (93.3% each). Step 7 (69.2%) and 5 (53.8%) and 10 (46.2% each) were not as frequently pursued. Again, steps 3 and 11 (15.4%) were nearly absent in the psychometric evaluation. Of these, the ESS (51) underwent all steps.
Tools Psychometrically Evaluated, Translated With Adaptations
The Russian version of the PDSS (89) did not report step 3, but executed to a certain extent all the steps to psychometrically evaluate a translated tool to its population. Based on the advice of the area specialist and the focus group of children questions #3 (Trouble getting out of bed in the morning), 4 (Fall asleep/drowsy during class), 7 (Fall back to sleep after being awakened), and 8 (Usually alert during the day (reverse coded)) were modified for better understanding.
Some Extra Remarks
Translations of Tools
Although the studies reported here are English papers, popular translations are Chinese, Portuguese, Spanish, and Turkish. The CSHQ, PSQ, and OSA-18 were the most frequently translated tools.
Tools With Norm Scores
Psychometric studies of particular interest are those that developed normative values or clinical/community cutoff scores for widespread usage, of which there were overall 18. Norms have been developed for CAS-15 (17), ESS (51, 52), JSQ (58, 59), SDSC (120, 121), CSHQ and CRSP (25, 34), CSRQ (47), MEQ (64, 65), NARQoL-21 (70), OSPQ (83), PSQ (108), SNAKE (129), Comic (138), and YSIS (140) (refer to Table 2).
The CAS-15, PSQ, CSRQ, and ESS studies provided “normative” ROC cutoff scores, with the Krishnamoorthy et al. (51) providing cutoffs for moderate and high excessive sleepiness.
Population-based norms were developed for preschoolers and school-aged children of JSQ. Average T-scores for all as well as for boys/girls in age bands of 2–3, 4, 5–6 years separately are available for each subscale: restless legs syndrome, sensory; obstructive sleep apnea syndrome; morning symptoms; parasomnias; insomnia or circadian rhythm disorders; daytime excessive sleepiness; daytime behaviors; sleep habit; insufficient sleep; and restless legs syndrome, motor. For school-aged median T-scores are available for 1st–2nd, 3rd–4th,5th–6th grade per the following subscales: restless legs syndrome, sleep disordered breathing, morning symptoms, nighttime awakenings, insomnia, excessive daytime sleepiness, daytime behavior, sleep habit, and irregular/delayed sleep phase.
Regarding the SDSC, French (France and French speaking Switzerland) as well as Chinese T-scores are available. The Chinese study reports average T-scores per the subscales sleep–wake transition disorders; disorders of initiating and maintaining sleep; disorders of excessive somnolence; disorders of arousal; sleep hyperhidrosis; and sleep breathing disorders. Whereas the French study copied the approach of the original report, i.e., tabulated the full T-score range from 31 to 100 including marks for clinical ranges.
The CSHQ study aimed to validate the Dutch version of the tool for toddlers while developing norms due to the current inaccessibility of the CSHQ in this age group. Norm values were decidedly the mean total score in the sample population and while the factor-structure was unsupported, the normative score developed was still representative of the presence and severity of sleep problems in 25% of toddlers. Authors report the mean total score for lower/higher socioeconomic status, 2 and 3 year olds, girls and boys, yes/no problem sleepers. The authors similarly provided means and standard deviations for the 23 items of the CRSP.
The MEQ studies are comparable providing means and standard deviations as well as percentiles. Also percentiles are reported in the YSIS study.
For the NARQoL-21 a comparison was made with a validated health-related quality of life tool, and a cutoff of <42 was deemed as sensitive and specific, supplementary available are cutoff scores for differentiating between optimal and suboptimal quality of life.
T-scores for subscales by gender and age (5–7 and 8–10 years old) are provided for OSPQ: sleep routine, bedtime anxiety, morning tiredness, night arousals, sleep disordered breathing and restless sleep.
For SNAKE a t-distribution was generated for Disturbances going to sleep, Disturbances remaining asleep, Arousal disorders, Daytime sleepiness, and Conduct disorders for children in ages between 1 and 25 years old. For the Children’s Sleep Comic (ages 5 to 11) stanines were generated for the raw intensity of sleep problem score.
Tools With ROC Analyses
Twenty-eight (19.4%) studies reported ROC findings. This was primarily done for (refer to Table 2) CSHQ (n=4) and PSQ (n=5). That is, in 20% the ROC was calculated given clinical versus control/community samples, while in 48% of the papers a PSG parameter was used (e.g., apnea-hypopnea index, obstructive index). Another criterion was used in 32% of the cases (e.g., validated questionnaire, parental report, or optimal cutoff from original paper).
Papers With Questionnaires Available
In Table 1, the studies (32.6%) that printed or made available their questionnaire in supplementary files or appendix are shown.
Use of Classification Systems
Primarily the ICSD classification system was used to generate/mimic items for the following new tools: the Pediatric Sleep CGIs (90), RLS (117), SDSC* (125), SNAKE (129), the Children's Sleep Comic (137), and YSIS (140). When tools were psychometrically evaluated and/or translated/modified such as the CSHQ or the SDSC the classification system upon which their original items were generated remains.
Tools Used in Specific Populations
The SNAKE has been specifically developed for children with psychomotor disabilities, and hence serves as a good example of tool development. Whereas the vast majority of studies involved tools that are modifications or compilations, as well as a psychometric evaluation of the tool utility in an “atypical” population.
Discussion
Since the 2011 Spruyt (2, 3) review, it has been encouraged that further psychometric validation is pursued for all questionnaires to develop a broader and more reliable range of tools. While “tools do not need to be perfect or even psychometrically exceptional, they need to counterpart clinical decision-making and reduce errors of judgment when screening for poor sleep,” suggested Spruyt (personal communication). This is done through the descriptive, iterative process of a tool protocol and often requires all steps of psychometric evaluation. Without this we have observed that tools rely on minor aspects of their psychometric validity for (clinical) application when this is often fallacious and nonspecific to the study population. Following the systematic review however, a dramatic increase in tool translations and adaptations has been observed which is to be irrefutably applauded. Nonetheless, it is important to develop standardized tests that are culture-free and fair in order to identify sleep issues across the board based on an unbiased testing process.
Twenty-seven new tools have been developed, while most of the papers published reported translations/adaptations or a psychometric evaluation of an existing tool. More than half of the tools queried general sleep problems. Irrespective of the infrequency of tools developed in categories like sleep ecology and treatment, there is an emerging need for further research into these areas given the environmental impact of technology on pediatric sleep in the 21st century (141, 142).
The two new tools that underwent all 11 steps aimed at investigating sleep problems either in terms of a quality of life tool for narcoleptics (NARQoL-21) (70) or as a sleep disorder tool for children with severe psychomotor impairment (SNAKE) (129). Several other tools accomplished nearly all steps (see Tables: OSPQ, CSAQ, BRIAN-K, PADSS, SDSC*, NSD, and YSIS).
Since the 2011 review, tools for specific populations (e.g., in terms of ages, developmental disabilities, sleep pathologies) are still needed. Epidemiological tools assessing sleep in adolescents specifically have received some focus, where they were second in publication frequency. This dramatic influx of relevant research can be a result of the rising sleep-reduction epidemic in teenage populations influenced by biological, psychological and sociocultural factors. In addition, the investigation into the effects of sleep hygiene and ecology (143), which are heavily influenced by sociocultural phenomena, have slowly presented themselves across children and adolescents (6–18 years). With the introduction of technology at the forefront of childhood influence (144, 145), pediatric sleep habits and consequently quality is slowly gaining traction where studies flagged here are acknowledging the underlying weight of sleep hygiene on sleep quality and sleep quantity. Although at present, these tools are still demanding attention for further psychometric validation. An urgent call for tools with adequate psychometric properties is concluded in several recent reviews (146–148).
Especially assessing the factor structure of tools toward construct validation has been pursued, while other steps continue to be overlooked. Similarly, general tools to screen for sleep pathologies remain preponderant since the 2011 review. Alternatively, a file-drawer problem can be expected. Combined with the difficulty of finding a suitable journal to publish a tool validation study, this may lead to a skewed scientific literature toward commonly published and used tools. This is potentially echoed in atypical populations as seen by the influx of psychometric evaluations of existing tools. Undoubtedly, more studies are needed in an era where sleep is rapidly gaining public interest, and the need for a scientifically sound answer on the consequences of a “poor sleep” endemic is pressing.
Several tools pop out for diverse reasons. The first tool of note is the JSQ (58, 59) validated for Japanese children investigating sleep in a large population-based sample flagged by our search and developing normative values for this tool at a 99% confidence interval. This tool is notable in that given its statistical validity and reliability in a large population sample, the plausibility of this being mirrored in other cultures is possible. Important to note however, is that sleeping habits in Japanese children may vary greatly to those in western countries. Therefore, the changes in sociocultural sleep habits when adapting for other populations should be considered. Secondly, SNAKE the sleep questionnaire for children with severe psychomotor impairment underwent all 11 steps and was uniquely developed (hence not modified) for a specific population. More alike are needed (149). Thirdly, PADSS, and BRIAN-K both newly developed tools drew our attention because they examine arousal level and biological rhythm. Although the PADSS may need some further validation studies toward diagnosing, monitoring, and assessing the effects of treatment in arousal disorders in childhood particularly, it addresses the need for more specialized tools. Whereas the BRAIN-K being a modification of an adult version may benefit from additional psychometric evaluations beyond the current age range. Also, the FoSI, measuring fear, being based on the adult version assessing fear in a rural trauma-exposed sample (150) warrants further psychometric scrutiny. In contrast to others, the RLS (117) proposes a difference in scores between two time points 14 days apart to identify RLS-related symptoms. Lastly, addressing the need for tools allowing the child to express themselves regarding sleep is the Children's Sleep Comic, being an adapted version of the unpublished German questionnaire “Freiburger Kinderschlafcomic” and providing pictures for items and responses. Hence, pinpointing to the “un”published tools in the field and a welcomed child’s perspective regarding inquiring about sleep in an alternative way.
Adhering to the words of Spruyt, that instruments should be enhancing clinical decision-making and significantly reducing errors of judgment, the study by Soh et al. identified, developed, and abbreviated the OSA-5 questionnaire after recognising preexisting faults in the original 18-item version. It was identified that the OSA-18 was initially designed as a disease-specific quality of life tool that does not predict obstructive sleep apnea (OSA) symptoms consistent with the gold-standard PSG. Recently Patel et al. (151) scrutinized the accuracy of such clinical scoring tools. Additionally, the study by Soh et al. (80) acknowledged that there exists a lack of parental understanding of some items and their wording in the original instrument. As a result, the OSA-18 was abbreviated to 11-items and then to 5- so that ultimately it would “perform better as a screening tool for use in triage and referral planning.” Our review also revealed other tools addressing this sleep problem: I’m sleepy (55). While OSA is increasingly relevant in pediatric epidemiology due to the rise in obesity, parental knowledge of the condition and consequent treatment options is imperative. A recent 2017 study regarding the development of a questionnaire informing parents of this treatment was designed by Links et al. (82). The tool aims to alleviate parental conflict around the choice for or against this treatment in children and is a first in its approach as a questionnaire focusing on medical treatment decision making. Like the objectives of OSA-5, this tool is notable in that it aims to “improve the quality and impact of patient and family decisions about OSA diagnosis and treatment” (82). As part of the personalized/precision medicine era, the CAS-15 (17) and PROMIS-papers pop out. The CAS-15 is one of the few tools where the respondent is the professional. The PROMIS, although presented as a potential screening/diagnostic tool, recently underwent several psychometric evaluations. It involves an item bank of Patient Reported Outcomes Measurement, or better it is intended to measure the subject’s “view” of their health status (e.g. sleep). Although these patients reported outcome measures (PROM) adhere to the same psychometric characteristics as diagnostic/screening tools, the scope of a PROM is very different. Namely, PROMs allow the efficacy of a clinical “intervention” to be measured from the patients’ perspective. Unfortunately, these specific instruments have not undergone all steps, accordingly, they would benefit from further validation and possible cultural/linguistic adaptation to achieve a more widespread use in the future.
As for the majority of tools that lack the detailed mention above, there is need for comment on the gradually increasing recognition for disease-specific instruments or instruments for specific populations. Alternatively, measuring the severity of sleep conditions over the frequency is still much needed. It was observed by Spruyt that nearly all questionnaires up until the 2010 search, focused on the frequency of sleep problems, however since then, several tools have aimed to increase the specificity and sensitivity of sleep tools to the severity of common pediatric illnesses and specific age groups associated with them e.g. Down syndrome, Narcolepsy (148), infancy, etc. This specificity of condition severity and age may help to refine treatment measures and streamline clinical interventions.
Additionally, in contrast to our review in 2011, the studies reported here are English papers, although popular translations are Chinese, Portuguese, Spanish, and Turkish. That is, between 2010 and 2020 especially the CSHQ, PSQ, and OSA-18 were translated. This is likely an approximation due to the exclusion of non-English papers and of dissertations etc. In 2011, we observed that the development or modification of tools may not always evolve into a scientific paper.
Vis-à-vis fulfillment of psychometric criteria, preliminary and confirmative factor analysis methods have been included in the scope of, and completed in either partially or completely, most the studies which was lacking prior. Primarily construct and content validity via factor structure or item correlation, and Cronbach alpha statistics are noticed. Standardized scoring and item generation however, is still ill-managed as a requirement and is an important step in developing a diagnostic tool or adapting/translating an existing one. Nonetheless, generally, it can be said that much of the studies into tool-psychometrics deserve recognition for endeavoring to adhere to steps 1 through 11. But the overarching suggestion thus far, is to more thoroughly fulfill the facets of validation; i.e. content, convergence, discriminative, and criterion-related validity (steps 8 and 9), pilot questionnaires in the event of an adaptive change made (step 5), examine the underlying factors to ensure (uni)dimensional structure of a said tool (steps 7 and 10) and develop norms alongside cutoff scores (step 11). Furthermore, although several tools mimic classification systems a more thorough psychometric scrutiny thereof is still needed. As a consequence, to date, the vast majority of tools reflect an appraisal of the frequency of a sleep complaint.
Several limitations should be noted. We post hoc limited our flagged studies to only English language given that they reach the broader scientific community. Furthermore, several of the tools included are not 100% sleep tools (e.g. health related). In addition, our way of presenting being “New Development (N),” “Psychometric Analysis (P),” and “Translation (T)/Adaptation (A),” or a combination thereof, involved overlaps in descriptive analyses. Contrary to the original paper by Spruyt, this one did not apply searches in Dissertations and Theses, Google Scholar (Web crawling), ebooks and conference Sleep abstract books, and as a consequence might not be an exhaustive list of tools. Alternatively, studies involving app’s did “hit” our search terms yet were not retained during further screening toward our aims. Lastly, given that this is a systematic review we didn’t pursue a quality assessment of study designs investigating sleep tools. Nevertheless, in Spruyt et al. (2) each of the necessary steps are stipulated.
Recommendations
It is recommended that future tools further the investigation into sleep hygiene, ecology [see (143)] and schedules of pediatric populations as this is becoming a highly relevant field of research upon the introduction of technology into sleeping habits and routines. The increasing prevalence of sleep deprivation in children (152–155) requires in depth discovery as to what damage or lack thereof is being done as a result of a 21st century society.
In addition to this, it is suggested that pediatric tools should be further introduced and adapted or validated for reporting by children older than 8 years of age. Since there is evidence to suggest that children as young as eight years can report information critical to their own health, it is recommended that a large proportion of questionnaires be designed for children in this age category as well as parents (1). Conjunctional use of these however, is advised to develop any diagnosis.
Although several tools listed mimic classification systems, or were psychometrically evaluated in samples that underwent clinical diagnoses upon a classification system, there is still room for improvement. Combined with primarily convenience samples such as clinical referrals and lack of details on (at risk of being poor) sampling techniques, the internal and external validity of studies might be seriously jeopardized.
Sensitivity and specificity are key in differencing screening versus diagnostic tools. Yet also, the sample on which this difference is determined plays a key role, where the diagnostic tools chiefly aims at subjects believed to have the problem. Thus, screening tests are chosen toward high sensitivity while diagnostic tests are chosen toward high specificity (true negatives).
Lastly, caution is warranted upon a general positive score regarding reliability and validity assessment, and readers are advised to remain critical concerning the statistical techniques applied in the individual studies. Several recommendations for future tool development or evaluation have been listed in Box 1. Tool development and evaluation, as mentioned in the past is time and labor-intensive (2). In short, scientific copycats (i.e. replication studies) are needed!
Box 1. Research agenda: a need for
● Tools assessing sleep ecology, sleep routines/hygiene, regularity, treatment
● Psychometric evaluation of apps
● Tools for daytime sleep
● Tools per sleep pathology
● Tools for specific populations
● Tools sensitive and specific regards classification systems
● Tools adept to developmental changes
● Tools differentiating between school days and nonschool days
● Tools as a PROM, Patient-Reported Outcome Measures
● A venue to publish psychometric evaluations of tools
● Methodologic scrutiny regarding sampling (patient/population), statistical techniques, the aim(s), and type of study
● Availability of the tools published, especially translations
● Equal attention to all 11 steps; e.g. step 3 such as answer but also time format
● Replication studies
● Self-reporting tools for school-aged children
● Question and/or Response formats beyond frequency
● Sleep duration not being a categorical answer
● Caution regarding “child”-modifications of adult tools or applications beyond the intended age range
● Culture-free or fair tools
● Reviews and meta-analyses on criterion validity of subjective tools
Author Contributions
TS performed first search, extracted data, and wrote the first draft during her internship. Her work was updated, verified and finalized by KS.
Conflict of Interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Acknowledgments
We would like to thank and acknowledge listservers PedSleep2.0 and IPSA for distributing the request for relevant additional literature and the following authors to whom expressed interest, to our review: Candice A. Alfano, Annie Bernier, Kelly Byars, Daniel A. Combs, and Jodi Mindell. Additionally, we would like to thank the following people for providing information and/or complete access to a pdf copy of their study: Annie Links, Beth Malow, Serge Brand, Robert Bozidis, Rocío De la Vega, and Valerie Crabtree.
Abbreviations
AAP, American Academy of Pediatrics; ADHD, attention deficit hyperactivity disorder; ASDC, Association of Sleep Disorders Centers classification; DSM, Diagnostic and Statistical Manual of Mental Disorders; ICD, International Classification of Diseases; ICSD, International Classification of Sleep Disorders; PSG, polysomnography; RLS, Restless Legs Syndrome; ROC, Receiver Operating Characteristic curve.
References
1. Eaden J, Mayberry MK, Mayberry JF. Questionnaires: the use and abuse of social survey methods in medical research. Postgraduate Med J (1999) 75(885):397–400. doi: 10.1136/pgmj.75.885.397
2. Spruyt K, Gozal D. Development of pediatric sleep questionnaires as diagnostic or epidemiological tools: a brief review of dos and don’ts. Sleep Med Rev (2011) 15(1):7–17. doi: 10.1016/j.smrv.2010.06.003
3. Spruyt K, Gozal D. Pediatric sleep questionnaires as diagnostic or epidemiological tools: a review of currently available instruments. Sleep Med Rev (2011) 15(1):19–32. doi: 10.1016/j.smrv.2010.07.005
4. Spruyt K, Braam W, Curfs LM. Sleep in Angelman syndrome: A review of evidence. Sleep Med Rev (2018) 37:69–84. doi: 10.1016/j.smrv.2017.01.002
5. Chung K-F. Assessing Insomnia in Adolescents: Comparison of Insomnia Severity Index, Athens Insomnia Scale and Sleep Quality Index. Sleep Med (2011) 12:463–70. doi: 10.1016/j.sleep.2010.09.019
6. Storfer-Isser A, Lebourgeois MK, Harsh J, Tompsett CJ, Redline S. Psychometric properties of the Adolescent Sleep Hygiene Scale. J Sleep Res (2013) 22(6):707–16. doi: 10.1111/jsr.12059
7. de Bruin EJ, van Kampen RKA, van Kooten T, Meijer AM. Psychometric properties and clinical relevance of the Adolescent Sleep Hygiene Scale in Dutch adolescents. Sleep Med (2014) 15(7):789–97. doi: 10.1016/j.sleep.2014.03.015
8. Chehri A, Khazaie H, Eskandari S, Khazaie S, Holsboer-Trachsler E, Brand S, et al. Validation of the Farsi version of the revised Adolescent Sleep Hygiene Scale (ASHSr): a cross-sectional study. BMC Psychiatry (2017) 17(1):408. doi: 10.1186/s12888-017-1578-6
9. Lin CY, Strong C, Siu AMH, Jalilolghadr S, Nilsen P, Brostrom A, et al. Validating the Persian Adolescent Sleep Hygiene Scale-Revised (ASHSr) using comprehensive psychometric testing methods. Sleep Med (2018) 50:63–71. doi: 10.1016/j.sleep.2018.05.036
10. Arroll B, Fernando A, Falloon K, Warman G, Goodyear-Smith F. Development, validation (diagnostic accuracy) and audit of the Auckland Sleep Questionnaire: a new tool for diagnosing causes of sleep disorders in primary care. J Primary Health Care (2011) 3(2):107–13. doi: 10.1071/HC11107
11. Sufrinko AM, Valrie CR, Lanzo L, Bond KE, Trout KL, Ladd RE, et al. Empirical validation of a short version of the Adolescent Sleep-Wake Scale using a sample of ethnically diverse adolescents from an economically disadvantage community. Sleep Med (2015) 16(10):1204–6. doi: 10.1016/j.sleep.2015.07.002
12. Essner B, Noel M, Myrvik M, Palermo T. Examination of the Factor Structure of the Adolescent Sleep–Wake Scale (ASWS). Behav Sleep Med (2015) 13(4):296–307. doi: 10.1080/15402002.2014.896253
13. Bastida-Pozuelo MF, Sanchez-Ortuno MM. Preliminary analysis of the concurrent validity of the Spanish translation of the BEARS sleep screening tool for children. J Psychiatr Ment Health Nurs (2016) 23(8):513–20. doi: 10.1111/jpm.12338
14. Esbensen AJ, Hoffman EK. Reliability of parent report measures of sleep in children with Down syndrome. J Intellectual Disability Res (2017) 61(3):210–20. doi: 10.1111/jir.12315
15. Cassanello P, Diez-Izquierdo A, Gorina N, Matilla-Santander N, Martinez-Sanchez JM, Balaguer A. Adaptation and study of the measurement properties of a sleep questionnaire for infants and pre-school children. Anales pediatria (Barcelona Spain : 2003) (2018) 89(4):230–7. doi: 10.1016/j.anpedi.2017.12.003
16. Berny T, Jansen K, Cardoso T, Mondin TC, Silva R, Souza L, et al. Construction of a biological rhythm assessment scale for children. Trends Psychiatry Psychother (2018) 40(1), 53–60. doi: 10.1590/2237-6089-2017-0081
17. Goldstein NA, Stefanov DG, Graw-Panzer KD, Fahmy SA, Fishkin S, Jackson A, et al. Validation of a clinical assessment score for pediatric sleep-disordered breathing. Laryngoscope (2012) 122(9):2096–104. doi: 10.1002/lary.23455
18. Becker SP, Ramsey RR, Byars KC. Convergent validity of the Child Behavior Checklist sleep items with validated sleep measures and sleep disorder diagnoses in children and adolescents referred to a sleep disorders center. Sleep Med (2015) 16(1):79–86. doi: 10.1016/j.sleep.2014.09.008
19. Dursun OB, Ogutlu H, Esin IS. Turkish Validation and Adaptation of Children ‘s Chronotype Questionnaire (CCTQ)/Cocukluk Donemi Kronotip Anketi’nin Turkce Gecerlilik ve Guvenilirligi. Eurasian J Med (2015) 47(1):56–61. doi: 10.5152/eajm.2014.0061
20. Ishihara K, Doi Y, Uchiyama M. The reliability and validity of the Japanese version of the Children’s ChronoType Questionnaire (CCTQ) in preschool children. Chronobiol Int (2014) 31(9):947–53. doi: 10.3109/07420528.2014.933841
21. Yeung WF, Yu BYM, Ho YS, Ho FYY, Chung KF, Lee RLT, et al. Validation of the Chinese Version of the Children?s ChronoType Questionnaire (CCTQ) in school-aged children. Chronobiol Int (2019) 36(12):1681–90. doi: 10.1080/07420528.2019.1673769
22. Cordts KP, Steele RG. An Evaluation of the Children’s Report of Sleep Patterns Using Confirmatory and Exploratory Factor Analytic Approaches. J Pediatr Psychol (2016) 41(9):993–1001. doi: 10.1093/jpepsy/jsw013
23. Meltzer LJ, Avis KT, Biggs S, Reynolds AC, Crabtree VM, Bevans KB. The Children’s Report of Sleep Patterns (CRSP): a self-report measure of sleep for school-aged children. J Clin Sleep Med (2013) 9(3):235–45. doi: 10.5664/jcsm.2486
24. Meltzer LJ, Brimeyer C, Russell K, Avis KT, Biggs S, Reynolds AC, et al. The Children’s Report of Sleep Patterns: validity and reliability of the Sleep Hygiene Index and Sleep Disturbance Scale in adolescents. Sleep Med (2014) 15(12):1500–7. doi: 10.1016/j.sleep.2014.08.010
25. Steur LMH, Grootenhuis MA, Terwee CB, Pillen S, Wolters NGJ, Kaspers GJL, et al. Psychometric properties and norm scores of the sleep self report in Dutch children. Health Qual Life Outcomes (2019) 17(1):15. doi: 10.1186/s12955-018-1073-x
26. Meltzer LJ, Biggs S, Reynolds A, Avis KT, Crabtree VM, Bevans KB. The Children’s Report of Sleep Patterns – Sleepiness Scale: A self-report measure for school-aged children. Sleep Med (2012) 13(4):385–9. doi: 10.1016/j.sleep.2011.12.004
27. Chuang HL, Kuo CP, Liu CC, Li CY, Liao WC. The Development and Psychometric Properties of the Children’s Sleep Assessment Questionnaire in Taiwan. J Pediatr Nurs (2016) 31(6):e343–e52. doi: 10.1016/j.pedn.2016.07.008
28. Markovich AN, Gendron MA, Corkum PV. Validating the Children’s Sleep Habits Questionnaire against polysomnography and actigraphy in school-aged children. Front Psychiatry (2015) 5:188. doi: 10.3389/fpsyt.2014.00188/full10.3389/fpsyt.2014.00188
29. Dias CAC, Figueiredo B, Pinto TM. Children’s Sleep Habits Questionnaire - Infant Version. J Pediatr (Rio J) (2018) 94(2):146–54. doi: 10.1016/j.jped.2017.05.012
30. Ren F, Wang G, Wang M, Zhang J. A taxometric analysis of the children’s sleep habits questionnaire. Sleep Med (2013) 14(Supplement 1):e241–e2. doi: 10.1016/j.sleep.2013.11.584
31. Liu Z, Wang G, Tang H, Wen F, Li N. Reliability and validity of the Children’s Sleep Habits Questionnaire in preschool-aged Chinese children. Sleep Biol Rhythms (2014) 12(3):187–93. doi: 10.1111/sbr.12061
32. Tan TX, Wang Y, Cheah CSL, Wang G-H. Reliability and construct validity of the Children’s Sleep Habits Questionnaire in Chinese kindergartners. Sleep Health (2018) 4:104–9. doi: 10.1016/j.sleh.2017.10.008
33. Waumans RC, Terwee CB, Van den Berg G, Knol DL, Van Litsenburg RR, Gemke RJ. Sleep and sleep disturbance in children: Reliability and validity of the Dutch version of the Child Sleep Habits Questionnaire. Sleep (2010) 33(6):841–5. doi: 10.1093/sleep/33.6.841
34. Steur LMH, Visser EH, Grootenhuis MA, Terwee CB, Kaspers GJL, van Litsenburg RRL. Psychometric properties and Dutch norm values of the Children’s Sleep Habits Questionnaire in toddlers. Sleep Med (2017) 34:57–63. doi: 10.1016/j.sleep.2017.01.022
35. Mavroudi A, Chrysochoou EA, Boyle RJ, Trypsianis G, Xinias I, Cassimos D, et al. Validation of the Children’s Sleep Habits Questionnaire in a sample of Greek children with allergic rhinitis. Allergologia Immunopathol (2018) 46(4):389–93. doi: 10.1016/j.aller.2017.09.016
36. Johnson CR, DeMand A, Lecavalier L, Smith T, Aman M, Foldes E, et al. Psychometric properties of the children’s sleep habits questionnaire in children with autism spectrum disorder. Sleep Med (2016) 20:5–11. doi: 10.1016/j.sleep.2015.12.005
37. Sneddon P, Peacock GG, Crowley SL. Assessment of Sleep Problems in Preschool Aged Children: An Adaptation of the Children’s Sleep Habits Questionnaire. Behav Sleep Med (2013) 11(4):283–96. doi: 10.1080/15402002.2012.707158
38. Masakazu O, Shingo K, Yoshitaka I, Hisateru T, Yuichi K, Shigekazu H, et al. Reliability and validity of a brief sleep questionnaire for children in Japan. J Physiol Anthropol (2017) 36(1):1–8. doi: 10.1186/s40101-017-0151-9. (1):1.
39. Schlarb AA, Schwerdtle B, Hautzinger M. Validation and psychometric properties of the German version of the Children’s Sleep Habits Questionnaire (CSHQ-DE). Somnologie - Schlafforschung und Schlafmedizin (2010) 14(4):260–6. doi: 10.1007/s11818-010-0495-4
40. Silva FG, Cláudia Rocha S, Lígia Barbosa B, Ana Serrão N. Portuguese Children’s Sleep Habits Questionnaire - validation and cross-cultural comparison. Jornal Pediatria (2014) 90(11):78–84:78. doi: 10.1016/j.jped.2013.06.009
41. Lucas-de la Cruz L, Martinez-Vizcaino V, Alvarez-Bueno C, Arias-Palencia N, Sanchez-Lopez M, Notario-Pacheco B. Reliability and validity of the Spanish version of the Children’s Sleep Habits Questionnaire (CSHQ-SP) in school-age children. Child: care Health Dev (2016) 42(5):675–82. doi: 10.1111/cch.12357
42. Fallahzadeh H, Etesam F, Asgarian FS. Validity and reliability related to the Persian version of the Children’s Sleep Habits Questionnaire. Sleep Biol Rhythms (2015) 13(3):271–8. doi: 10.1111/sbr.12114
43. Loureiro HC. Validation of the Children Sleep Habits Questionnaire and the Sleep Self Report for portugese children. Sleep Sci (2013) 6(4):151–8.
44. Bonuck KA, Goodlin-Jones BL, Schechter C, Owens J. Modified Children’s sleep habits questionnaire for behavioral sleep problems: A validation study. Sleep Health (2017) 3:136–41. doi: 10.1016/j.sleh.2017.03.009
45. Jankowski KS. Composite Scale of Morningness: psychometric properties, validity with Munich ChronoType Questionnaire and age/sex differences in Poland. Eur Psychiatry (2015) 30(1):166–71. doi: 10.1016/j.eurpsy.2014.01.004
46. Dewald JF, Short MA, Gradisar M, Oort FJ, Meijer AM. The Chronic Sleep Reduction Questionnaire (CSRQ): a cross-cultural comparison and validation in Dutch and Australian adolescents. J Sleep Res (2012) 21(5):584–94. doi: 10.1111/j.1365-2869.2012.00999.x
47. Dewald-Kaufmann JF, Bruin EJ, Smits M, Zijlstra BJH, Oort FJ, Meijer AM. Chronic sleep reduction in adolescents—clinical cut-off scores for the Chronic Sleep Reduction Questionnaire (CSRQ). J Sleep Res (2018) 27(3):e12653. doi: 10.1111/jsr.12653
48. LeBourgeois MK, Harsh JR. Development and psychometric evaluation of the Children’s Sleep-Wake Scale. Sleep Health (2016) 2:198–204. doi: 10.1016/j.sleh.2016.04.001
49. Lang C, Brand S, Holsboer-Trachsler E, Puhse U, Colledge F, Gerber M. Validation of the German version of the short form of the dysfunctional beliefs and attitudes about sleep scale (DBAS-16). Neurological Sci (2017) 38(6):1047–58. doi: 10.1007/s10072-017-2921-x
50. Blunden SL, Crawford M, Gregory AM. Development of a short version of the dysfunctional beliefs about sleep questionnaire for use with children (DBAS-C10). Sleep (2012) 35:A364–A5. doi: 10.4172/2325-9639.1000115
51. Krishnamoorthy Y, Sarveswaran G, Sakthivel M, Kalaiselvy A, Majella MG, Lakshminarayanan S. Construct Validation and Reliability Assessment of Tamil Version of Epworth Sleepiness Scale to Evaluate Daytime Sleepiness among Adolescents in Rural Puducherry, South India. J Neurosci Rural Pract (2019) 10(1):89–93. doi: 10.4103/jnrp.jnrp_168_18
52. Crabtree VM, Klages KL, Sykes A, Wise MS, Lu ZH, Indelicato D, et al. Sensitivity and Specificity of the Modified Epworth Sleepiness Scale in Children With Craniopharyngioma. J Clin Sleep Med (2019) 15(10):1487–93. doi: 10.5664/jcsm.7982
53. Janssen KC, Phillipson S, O’Connor J, Johns MW. Validation of the Epworth Sleepiness Scale for Children and Adolescents using Rasch analysis. Sleep Med (2017) 33:30–5. doi: 10.1016/j.sleep.2017.01.014
54. Brown TSH, Garcia E, Akeeb A, Lynch-Jiles AC, White D, Young M. Adolescent Nocturnal Fears: a psychometric evaluation of the fear of sleep inventory (FoSI). Behav Sleep Med (2019) 17(6):721–8. doi: 10.1080/15402002.2018.1469495
55. Kadmon G, Chung SA, Shapiro CM. I’M SLEEPY: A short pediatric sleep apnea questionnaire. Int J Pediatr Otorhinolaryngol (2014) 78:2116–20. doi: 10.1016/j.ijporl.2014.09.018
56. Kanstrup M, Holmstrom L, Ringstrom R, Wicksell RK. Insomnia in paediatric chronic pain and its impact on depression and functional disability. Eur J Pain (London England) (2014) 18(8):1094–102. doi: 10.1002/j.1532-2149.2013.00450.x
57. Gerber M, Lang C, Lemola S, Colledge F, Kalak N, Holsboer-Trachsler E, et al. Validation of the German version of the insomnia severity index in adolescents, young adults and adult workers: results from three cross-sectional studies. BMC Psychiatry (2016) 16:174. doi: 10.1186/s12888-016-0876-8
58. Kuwada A, Mohri I, Asano R, Matsuzawa S, Kato-Nishimura K, Hirata I, et al. Japanese Sleep Questionnaire for Elementary Schoolers (JSQ-ES): validation and population-based score distribution. Sleep Med (2018) 41:69–77. doi: 10.1016/j.sleep.2017.07.025
59. Shimizu S, Kato-Nishimura K, Mohri I, Kagitani-Shimono K, Tachibana M, Ohno Y, et al. Psychometric properties and population-based score distributions of the Japanese Sleep Questionnaire for Preschoolers. Sleep Med (2014) 15:451–8. doi: 10.1016/j.sleep.2013.05.020
60. Garmy P, Jakobsson U, Nyberg P. Development and psychometric evaluation of a new instrument for measuring sleep length and television and computer habits of Swedish school-age children. J school Nurs (2012) 28(2):138–43. doi: 10.1177/1059840511420878
61. Roenneberg T. Life Between Clocks: daily Temporal Patterns of Human Chronotypes. J Biol Rhythms (2003) 18(1):80–90. doi: 10.1177/0748730402239679
62. Cavallera GM, Boari G. Validation of the Italian Version of the Morningness-Eveningness Questionnaire for Adolescents by A. Lancry and Th. Arbault. Med Sci Monitor (2015) 21:2685–93. doi: 10.12659/msm.894091
63. Danielsson K, Sakarya A, Jansson-Frojmark M. The reduced Morningness-Eveningness Questionnaire: Psychometric properties and related factors in a young Swedish population. Chronobiol Int (2019) 36(4):530–40. doi: 10.1080/07420528.2018.1564322
64. Rodrigues PFS, Pandeirada JNS, Marinho PI, Bem-Haja P, Silva CF, Ribeiro L, et al. Morningness–eveningness preferences in Portuguese adolescents: Adaptation and psychometric validity of the H&O questionnaire. Pers Individ Dif (2016) 88:62–5. doi: 10.1016/j.paid.2015.08.048
65. Rodrigues PFS, Pandeirada JNS, Bem-Haja P, Marinho PI, Fernandes NL, Ribeiro L, et al. Assessing circadian preferences in Portuguese adolescents: development and preliminary validation of a reduced Morningness-Eveningness Questionnaire. Biol Rhythm Res (2019) 50(6):916–26. doi: 10.1080/09291016.2018.1512291
66. Díaz-Morales JF. Morningness–Eveningness Scale for Children (MESC): Spanish normative data and factorial invariance according to sex and age. Pers Individ Dif (2015) 87:116–20. doi: 10.1016/j.paid.2015.07.027
67. Demirhan E, Onder I, Horzum MB, Masal E, Besoluk S. Adaptation of the Morningness-Eveningness Stability Scale improved (MESSi) into Turkish. Chronobiol Int (2019) 36(3):427–38. doi: 10.1080/07420528.2018.1560307
68. Weidenauer C, Tauber L, Huber S, Rimkus K, Randler C. Measuring circadian preference in adolescence with the Morningness-Eveningness Stability Scale improved (MESSi). Biol Rhythm Res (2019) 0:1–3. doi: 10.1080/09291016.2019.1600268
69. Pinto TR, Pinto JC, Pinto HR, Paiva T. Validation of a three-dimensional model about sleep: habits, personal factors and environmental factors. Sleep Sci (2014) 7(4):197–202. doi: 10.1016/j.slsci.2014.12.002.
70. Chaplin JE, Szakacs A, Hallbook T, Darin N. The development of a health-related quality-of-life instrument for young people with narcolepsy: NARQoL-21. Health Qual Life Outcomes (2017) 15(1):135. doi: 10.1186/s12955-017-0707-8
71. Yoshihara S, Kanno N, Fukuda H, Yamada Y, Fukuda N, Tsuchiya T, et al. Development and validation of a nighttime sleep diary in asthmatic children. Pediatr Allergy Immunol (2011) 22(7):667–70. doi: 10.1111/j.1399-3038.2011.01164.x
72. Ouyang H, Han F, Zheng Q, Zhang J. Chinese version of narcolepsy severity scale: a validation study. BMC Neurol (2019) 19(1):334. doi: 10.1186/s12883-019-1570-5
73. Sanders E, Hill CM, Evans HJ, Tuffrey C. The development of a screening questionnaire for obstructive sleep apnea in children with Down syndrome. Front Psychiatry (2015) 6:147. doi: 10.3389/fpsyt.2015.00147
74. Huang YS, Hwang FM, Lin CH, Lee LA, Huang PY, Chiu ST. Clinical manifestations of pediatric obstructive sleep apnea syndrome: Clinical utility of the Chinese-version Obstructive Sleep Apnea Questionaire-18. Psychiatry Clin Neurosci (2015) 69(12):752–62. doi: 10.1111/pcn.12331
75. Kang KT, Weng WC, Yeh TH, Lee PL, Hsu WC. Validation of the Chinese version OSA-18 quality of life questionnaire in Taiwanese children with obstructive sleep apnea. J Formosan Med Assoc = Taiwan yi zhi (2014) 113(7):454–62. doi: 10.1016/j.jfma.2012.10.002
76. Bannink N, Maliepaard M, Raat H, Joosten KF, Mathijssen IM. Reliability and validity of the obstructive sleep apnea-18 survey in healthy children and children with syndromic craniosynostosis. J Dev Behav Pediatr : JDBP (2011) 32(1):27–33. doi: 10.1097/DBP.0b013e3181fa579f
77. Mousailidis GK, Lachanas VA, Skoulakis CE, Sakellariou A, Exarchos ST, Kaditis AG, et al. Cross-cultural adaptation and validation of the Greek OSA-18 questionnaire in children undergoing polysomnography. Int J Pediatr Otorhinolaryngol (2014) 78:2097–102. doi: 10.1016/j.ijporl.2014.09.013
78. Fernandes FM, Teles Rda C. Application of the Portuguese version of the Obstructive Sleep Apnea-18 survey to children. Braz J Otorhinolaryngol (2013) 79(6):720–6. doi: 10.5935/1808-8694.20130132
79. Chiner E, Landete P, Norberto Sancho-Chust J, Angel Martinez-Garcia M, Perez-Ferrer P, Pastor E, et al. Adaptation and Validation of the Spanish Version of OSA-18, a Quality of Life Questionnaire for Evaluation of Children with Sleep Apnea-Hypopnea Syndrome. Archivos Bronconeumol (2016) 52(11):553–9. doi: 10.1016/j.arbres.2016.04.003
80. Soh HJ, Rowe K, Davey MJ, Horne RS, Nixon GM. The OSA-5: Validation of a brief questionnaire screening tool for obstructive sleep apnoea in children. Int J Pediatr Otorhinolaryngol (2018) 27113:62–6. doi: 10.1016/j.ijporl.2018.07.029
81. Lachanas VA, Mousailidis GK, Skoulakis CE, Papandreou N, Exarchos S, Alexopoulos EI, et al. Validation of the Greek OSD-6 quality of life questionnaire in children undergoing polysomnography. Int J Pediatr Otorhinolaryngol (2014) 78:1342–7. doi: 10.1016/j.ijporl.2014.05.024
82. Links AR, Tunkel DE, Boss EF. Stakeholder-Engaged Measure Development for Pediatric Obstructive Sleep-Disordered Breathing: The Obstructive Sleep-Disordered Breathing and Adenotonsillectomy Knowledge Scale for Parents. JAMA Otolaryngol - Head Neck Surg (2017) 143(1):46. doi: 10.1001/jamaoto.2016.2681
83. Biggs SN, Kennedy JD, Martin AJ, van den Heuvel CJ, Lushington K. Psychometric properties of an omnibus sleep problems questionnaire for school-aged children. Sleep Med (2012) 13(4):390–5. doi: 10.1016/j.sleep.2011.12.005
84. Arnulf I, Zhang B, Uguccioni G, Flamand M, Noel de Fontreaux A, Leu-Semenescu S, et al. A scale for assessing the severity of arousal disorders. Sleep (2014) 37(1):127–36. doi: 10.5665/sleep.3322
85. Felden EP, Carniel JD, Andrade RD, Pelegrini A, Anacleto TS, Louzada FM. Translation and validation of the Pediatric Daytime Sleepiness Scale (PDSS) into Brazilian Portuguese. Jornal pediatria (2016) 92(2):168–73. doi: 10.1016/j.jped.2015.05.008
86. Komada Y, Breugelmans R, Drake CL, Nakajima S, Tamura N, Tanaka H, et al. Social jetlag affects subjective daytime sleepiness in school-aged children and adolescents: A study using the Japanese version of the Pediatric Daytime Sleepiness Scale (PDSS-J). Chronobiol Int (2016) 33(10):1311–9. doi: 10.1080/07420528.2016.1213739
87. Bektas M, Bektas I, Ayar D, Selekoglu Y, Ayar U, Kudubes AA, et al. Psychometric Properties of Turkish Version of Pediatric Daytime Sleepiness Scale (PDSS-T). Asian Nurs Res (2016) 10(1):62–7. doi: 10.1016/j.anr.2016.01.002
88. Ferrari Junior GJ, Drake CL, Barbosa DG, Diego Andrade R, Santos Silva DA, Erico Pereira GF. Factor structure of the Brazilian version of Pediatric Daytime Sleepiness Scale. Chronobiol Int (2018) 35(8):1088–94. doi: 10.1080/07420528.2018.1458732
89. Randler C, Kolomeichuk SN, Morozov AV, Petrashova DA, Pozharskaya VV, Martynova AA, et al. Psychometric properties of the Russian version of the Pediatric Daytime Sleepiness Scale (PDSS). Heliyon (2019) 5(7):e02134. doi: 10.1016/j.heliyon.2019.e02134
90. Malow BA, Connolly HV, Weiss SK, Halbower A, Goldman S, Hyman SL, et al. The Pediatric Sleep Clinical Global Impressions Scale-A New Tool to Measure Pediatric Insomnia in Autism Spectrum Disorders. J Dev Behav Pediatr : JDBP (2016) 37(5):370–6. doi: 10.1097/dbp.0000000000000307
91. Al-Gamal E, Long T. The Psychometric Properties of an Arabic version of the PedsQL Multidimensional Fatigue Scale Tested for Children with Cancer. Compr Child Adolesc Nurs (2017) 40(3):188. doi: 10.1080/24694193.2017.1316791
92. Qimeng Y, Ke L, Jun W, Xiuqing B, Lili Z. Reliability and validity of the Chinese version of the PedsQL Multidimensional Fatigue Scale in children with acute leukemia. IJNSS (2016) 3(2), 146–52. doi: 10.1016/j.ijnss.2016.04.001
93. Nascimento LC, Nunes MD, Rocha EL, Bomfim EO, Floria-Santos M, Dos Santos CB, et al. High validity and reliability of the PedsQL Multidimensional Fatigue Scale for Brazilian children with cancer. J Pediatr Oncol Nurs (2015) 32(1):57–64. doi: 10.1177/1043454214554656
94. Byars KC, Simon SL, Peugh J, Beebe DW. Validation of a Brief Insomnia Severity Measure in Youth Clinically Referred for Sleep Evaluation. J Pediatr Psychol (2017) 42(4):466–75. doi: 10.1093/jpepsy/jsw077
95. Whiteside-Mansell L, Nabaweesi R, Caballero AR, Mullins SH, Miller BK, Aitken ME. Assessment of Safe Sleep: Validation of the Parent Newborn Sleep Safety Survey. J Pediatr Nurs (2017) 35:30–5. doi: 10.1016/j.pedn.2017.02.033
96. Pires PJS, Mattiello R, Lumertz MS, Morsch TP, Fagondes SC, Nunes ML, et al. Validation of the Brazilian version of the “pediatric obstructive sleep apnea screening tool” questionnaire. J Pediatr (Rio J) (2019) 95(2):231–7. doi: 10.1016/j.jped.2017.12.014
97. Finimundi M, Barin I, Bandeira D, Souza DO. Validity of a circadian rhythm scale - Sleep/wake cycle for adolescents. Rev Paul Pediatr (2012) 30(3):409–14. doi: 10.1590/S0103-05822012000300016
98. Arbuckle R, Abetz L, Durmer JS, Ivanenko A, Owens JA, Croenlein J, et al. Development of the Pediatric Restless Legs Syndrome Severity Scale (P-RLS-SS): a patient-reported outcome measure of pediatric RLS symptoms and impact. Sleep Med (2010) 11(9):897–906. doi: 10.1016/j.sleep.2010.03.016
99. van Kooten JA, Terwee CB, Kaspers GJ, van Litsenburg RR. Content validity of the Patient-Reported Outcomes Measurement Information System Sleep Disturbance and Sleep Related Impairment item banks in adolescents. Health Qual Life Outcomes (2016) 14:92. doi: 10.1186/s12955-016-0496-5
100. van Kooten JAMC, van Litsenburg RRL, Yoder WR, Kaspers GJL, Terwee CB. Validation of the PROMIS Sleep Disturbance and Sleep-Related Impairment item banks in Dutch adolescents. Qual Life Res (2018) 27(7):1911–20. doi: 10.1007/s11136-018-1856-x
101. Forrest CB, Meltzer LJ, Marcus CL, de la Motte A, Kratchman A, Buysse DJ, et al. Development and validation of the PROMIS Pediatric Sleep Disturbance and Sleep-Related Impairment item banks. Sleep (2018) 41(6):zsy054. doi: 10.1093/sleep/zsy054
102. Bevans KB, Meltzer LJ, De La Motte A, Kratchman A, Viel D, Forrest CB. Qualitative Development and Content Validation of the PROMIS Pediatric Sleep Health Items. Behav Sleep Med (2019) 17(5):657–71. doi: 10.1080/15402002.2018.1461102
103. Smith VC, Leppert KA, Alfano CA, Dougherty LR. Construct validity of the Parent-Child Sleep Interactions Scale (PSIS): associations with parenting, family stress, and maternal and child psychopathology. Sleep Med (2014) 15(8):942–51. doi: 10.1016/j.sleep.2014.04.002
104. Ishman S, Heubi C, Jenkins T, Michalsky M, Simakajornboon N, Inge T. OSA screening with the pediatric sleep questionnaire for adolescents undergoing bariatric surgery in teen-LABS. Obesity (19307381) (2016) 24(11):2392. doi: 10.1002/oby.21623
105. Yuksel H, Sogut A, Yilmaz O, Kutluay E. Reliability and validity of the Turkish version of the pediatric sleep questionnaire: a tool for prediction of sleep related breathing disorder. Tuberkuloz ve toraks (2011) 59(3):236–41. doi: 10.5578/tt.2467
106. Bertran K, Mesa T, Rosso K, Jose Krakowiak M, Pincheira E, Brockmann PE. Diagnostic accuracy of the Spanish version of the Pediatric Sleep Questionnaire for screening of obstructive sleep apnea in habitually snoring children. Sleep Med (2015) 16(5):631–6. doi: 10.1016/j.sleep.2014.10.024
107. Hasniah AL, Jamalludin AR, Norrashidah AW, Norzila MZ, Asiah K, Anida AR, et al. Cross-cultural adaptation and reliability of pediatric sleep questionnaire in assessment of sleep-disordered breathing in the Malay speaking population. World J Pediatr (2012) 8(1):38–42. doi: 10.1007/s12519-011-0279-3
108. Chan A, Chan CH, Ng DK. Validation of sleep-related breathing disorder scale in Hong Kong Chinese snoring children. Pediatr Pulmonol (2012) 47(8):795–800. doi: 10.1002/ppul.22505
109. Ehsan Z, Kercsmar CM, Collins J, Simakajornboon N. Validation of the pediatric sleep questionnaire in children with asthma. Pediatr Pulmonol (2017) 52(3):382–9. doi: 10.1002/ppul.23568
110. Li X, Tai J, Xu Z, Ma J, Peng X, Pan Y, et al. Systematic investigation of childhood sleep-disordered breathing (SDB) in Beijing: validation of survey methodology. BMJ Open (2018) 8(8):1. doi: 10.1136/bmjopen-2017-021097
111. Longlalerng K, Sonsuwan N, Uthaikhup S, Kumsaiyai W, Sitilertpisan P, Traisathit P, et al. Translation, cross-cultural adaptation and psychometric properties of the Sleep-Related Breathing Disordered-Pediatric Sleep Questionnaire for obese Thai children with obstructive sleep apnea. Sleep Med (2018) 53:45–50. doi: 10.1016/j.sleep.2018.08.033
112. Raman VT, Splaingard M, Tumin D, Rice J, Jatana KR, Tobias JD. Utility of screening questionnaire, obesity, neck circumference, and sleep polysomnography to predict sleep-disordered breathing in children and adolescents. Pediatr Anesthesia (2016) 26(6):655–64. doi: 10.1111/pan.12911
113. Certal V, de Lima FF, Winck JC, Azevedo I, Costa-Pereira A. Translation and cross-cultural adaptation of the Pediatric Sleep Questionnaire into Portuguese language. Int J Pediatr Otorhinolaryngol (2015) 79:175–8. doi: 10.1016/j.ijporl.2014.12.002
114. Jordan L, Beydon N, Razanamihaja N, Garrec P, Carra MC, Fournier BP, et al. Translation and cross-cultural validation of the French version of the Sleep-Related Breathing Disorder scale of the Pediatric Sleep Questionnaire. Sleep Med (2019) 58:123–9. doi: 10.1016/j.sleep.2019.02.021
115. Passos MH, Silva HA, Pitangui AC, Oliveira VM, Lima AS, Araujo RC. Reliability and validity of the Brazilian version of the Pittsburgh Sleep Quality Index in adolescents. Jornal pediatria (2017) 93(2):200–6. doi: 10.1016/j.jped.2016.06.006
116. Raniti MB, Waloszek JM, Schwartz O, Allen NB, Trinder J. Factor structure and psychometric properties of the Pittsburgh Sleep Quality Index in community-based adolescents. Sleep (2018) 41(6):zsy066. doi: 10.1093/sleep/zsy066
117. Schomoller A, Weis K, von Barby R, Hubler A, Mayer F, Erler T. Restless legs syndrome in childhood and adolescence: Applicability of aquestionnaire designed to assess disease-related symptoms. Somnologie (2019) 23(2):104–8. doi: 10.1007/s11818-018-0188-y
118. Graef DM, Byars KC. Utility of the Sleep Disorders Inventory for Students in Clinically Referred Youth With Insomnia: Risk Identification and Relationship With Polysomnographic Measures. Behav Sleep Med (2020), 18(2):249–61. doi: 10.1080/15402002.2019.1578770
119. Daniel LC, Schwartz LA, Mindell JA, Tucker CA, Barakat LP. Initial Validation of the Sleep Disturbances in Pediatric Cancer Model. J Pediatr Psychol (2016) 41(6):588–99. doi: 10.1093/jpepsy/jsw008
120. Huang MM, Qian Z, Wang J, Vaughn MG, Lee YL, Dong GH. Validation of the sleep disturbance scale for children and prevalence of parent-reported sleep disorder symptoms in Chinese children. Sleep Med (2014) 15(8):923–8. doi: 10.1016/j.sleep.2014.03.023
121. Putois B, Leslie W, Gustin MP, Challamel MJ, Raoux A, Guignard-Perret A, et al. The French Sleep Disturbance Scale for Children. Sleep Med (2017) 32:56–65. doi: 10.1016/j.sleep.2016.12.008
122. Saffari M, Gholamrezaei A, Saneian H, Attari A, Bruni O. Linguistic validation of the Sleep Disturbance Scale for Children (SDSC) in Iranian children with Persian language. Sleep Med (2014) 15:998–1001. doi: 10.1016/j.sleep.2014.03.021
123. Cordts KMP, Hall TA, Hartman ME, Luther M, Wagner A, Piantino J, et al. Sleep Measure Validation in a Pediatric Neurocritical Care Acquired Brain Injury Population. Neurocrit Care (2019). doi: 10.1007/s12028-019-00883-5
124. Mancini VO, Rudaizky D, Pearcy BTD, Marriner A, Pestell CF, Gomez R, et al. Factor structure of the Sleep Disturbance Scale for Children (SDSC) in those with Attention Deficit and Hyperactivity Disorder (ADHD). Sleep Med X (2019) 1:100006. doi: 10.1016/j.sleepx.2019.100006
125. Moo-Estrella JA. Develoment and validation of the Sleep Disturbances Scale for School-age children. Acta Pediatr Mex (2018) 39:(2):121–33. doi: 10.18233/APM39No2pp121-1331573
126. Ozdemir PG, Boysan M, Selvi Y, Yildirim A, Yilmaz E. Psychometric properties of the Turkish version of the Sleep Hygiene Index in clinical and non-clinical samples. Compr Psychiatry (2015) 59:135–40. doi: 10.1016/j.comppsych.2015.02.001
127. Rabner J, Kaczynski KJ, Simons LE, Lebel AA. The Sleep Hygiene Inventory for Pediatrics: Development and Validation of a New Measure of Sleep in a Sample of Children and Adolescents With Chronic Headache. J Child Neurol (2017) 32(13):1040–6. doi: 10.1177/0883073817726679
128. Restrepo C, Manfredini D, Castrillon E, Svensson P, Santamaria A, Alvarez C, et al. Diagnostic accuracy of the use of parental-reported sleep bruxism in a polysomnographic study in children. Int J Paediatric Dentist (2017) 27(5):318–25. doi: 10.1111/ipd.12262
129. Blankenburg M, Tietze AL, Hechler T, Hirschfeld G, Michel E, Koh M, et al. Snake: the development and validation of a questionnaire on sleep disturbances in children with severe psychomotor impairment. Sleep Med (2013) 14(4):339–51. doi: 10.1016/j.sleep.2012.12.008
130. Maas APHM, Didden R, Korzilius H, Braam W, Collin P, Smits MG, et al. Psychometric properties of a sleep questionnaire for use in individuals with intellectual disabilities. Res Dev Disabil (2011) 32(6):2467–79. doi: 10.1016/j.ridd.2011.07.013
131. Önder İ, Masal E, Demirhan E, Horzum MB, Beşoluk Ş. Psychometric properties of sleep quality scale and sleep variables questionnaire in Turkish student sample. Int J Psychol Educ Stud (2016) 3(3):9–21. doi: 10.17220/ijpes.2016.03.002.
132. van Maanen A, Dewald-Kaufmann JF, Oort FJ, de Bruin EJ, Smits MG, Short MA, et al. Screening for Sleep Reduction in Adolescents Through Self-report: Development and Validation of the Sleep Reduction Screening Questionnaire (SRSQ). Child Youth Care Forum (2014) 43(5):607–19. doi: 10.1007/s10566-014-9256-z
133. Orgiles M, Owens J, Espada JP, Piqueras JA, Carballo JL. Spanish version of the Sleep Self-Report (SSR): factorial structure and psychometric properties. Child: care Health Dev (2013) 39(2):288–95. doi: 10.1111/j.1365-2214.2012.01389.x
134. Yamakita M, Sato M, Ando D, Suzuki K, Yamagata Z. Availability of a simple self-report sleep questionnaire for 9- to 12-year-old children. Sleep Biol Rhythms (2014) 12(4):279–88. doi: 10.1111/sbr.12072
135. Tait AR, Voepel-Lewis T, Christensen R, O’Brien LM. The STBUR questionnaire for predicting perioperative respiratory adverse events in children at risk for sleep-disordered breathing. Pediatr Anesthesia (2013) 23(6):510–6. doi: 10.1111/pan.12155
136. Tremaine RB, Dorrian J, Blunden S. Measuring sleep habits using the Sleep Timing Questionnaire: A validation study for school-age children. Sleep Biol Rhythms (2010) 8(3):194. doi: 10.1111/j.1479-8425.2010.00446.x
137. Schwerdtle. Children’s Sleep Comic: development of a new diagnostic tool for children with sleep disorders. Nat Sci Sleep (2012) 4:97–102. doi: 10.2147/NSS.S33127
138. Schwerdtle B, Kanis J, Kübler A, Schlarb A, Kübler A, Schlarb AA. The Children’s Sleep Comic: Psychometrics of a Self-rating Instrument for Childhood Insomnia. Child Psychiatry Hum Dev (2016) 47(1):53–63. doi: 10.1007/s10578-015-0542-2
139. Leite JM, Ferreira VR, do Prado LF, do Prado GF, de Morais JF, de Carvalho LB. TuCASA questionnaire for assessment of children with obstructive sleep apnea: validation. Sleep Med (2015) 16(2):265–9. doi: 10.1016/j.sleep.2014.09.013
140. Liu XC, Yang YY, Liu ZZ, Luo YC, Fan F, Jia CX. Psychometric properties of Youth Self-Rating Insomnia Scale (YSIS) in Chinese adolescents. Sleep Biol Rhythms (2019) 17(3):339–48. doi: 10.1007/s41105-019-00222-3
141. LeBourgeois MK, Hale L, Chang AM, Akacem LD, Montgomery-Downs HE, Buxton OM. Digital Media and Sleep in Childhood and Adolescence. Pediatrics (2017) 140(Suppl 2):S92–s6. doi: 10.1542/peds.2016-1758J
142. Woods HC, Scott H. Sleepyteens: Social media use in adolescence is associated with poor sleep quality, anxiety, depression and low self-esteem. J Adolesc (2016) 51:41–9. doi: 10.1016/j.adolescence.2016.05.008
143. Spruyt K, Anguh I, Nwabara OU. Sleep behavior of underrepresented youth. J Public Health (2014) 22(2):111–20. doi: 10.1007/s10389-013-0602-7
144. Bozzola E, Spina G, Ruggiero M, Memo L, Agostiniani R, Bozzola M, et al. Media devices in pre-school children: the recommendations of the Italian pediatric society. Ital J Pediatr (2018) 44(1):69. doi: 10.1186/s13052-018-0508-7
145. Anderson DR, Subrahmanyam K. Digital Screen Media and Cognitive Development. Pediatrics (2017) 140(Suppl 2):S57–s61. doi: 10.1542/peds.2016-1758C
146. Ji X, Liu J. Subjective sleep measures for adolescents: a systematic review. Child: care Health Dev (2016) 42(6):825–39. doi: 10.1111/cch.12376
147. Nascimento-Ferreira MV, Collese TS, de Moraes ACF, Rendo-Urteaga T, Moreno LA, Carvalho HB. Validity and reliability of sleep time questionnaires in children and adolescents: A systematic review and meta-analysis. Sleep Med Rev (2016) 30:85–96. doi: 10.1016/j.smrv.2015.11.006
148. Benmedjahed K, Wang YG, Lambert J, Evans C, Hwang S, Black J, et al. Assessing sleepiness and cataplexy in children and adolescents with narcolepsy: a review of current patient-reported measures. Sleep Med (2017) 32:143–9. doi: 10.1016/j.sleep.2016.12.020
149. Bautista M, Whittingham K, Edwards P, Boyd RN. Psychometric properties of parent and child reported sleep assessment tools in children with cerebral palsy: a systematic review. Dev Med Child Neurol (2018) 60(2):162–72. doi: 10.1111/dmcn.13609
150. Pruiksma KE, Taylor DJ, Ruggero C, Boals A, Davis JL, Cranston C, et al. A psychometric study of the Fear of Sleep Inventory-Short Form (FoSI-SF). J Clin Sleep Med (2014) 10(5):551–8. doi: 10.5664/jcsm.3710
151. Patel AP, Meghji S, Phillips JS. Accuracy of clinical scoring tools for the diagnosis of pediatric obstructive sleep apnea. Laryngoscope (2020) 130(4):1034–43. doi: 10.1002/lary.28146
152. Matricciani LA, Olds TS, Blunden S, Rigney G, Williams MT. Never enough sleep: a brief history of sleep recommendations for children. Pediatrics (2012) 129(3):548–56. doi: 10.1542/peds.2011-2039
153. Matricciani L, Olds T, Williams M. A review of evidence for the claim that children are sleeping less than in the past. Sleep (2011) 34(5):651–9. doi: 10.1093/sleep/34.5.651
154. Matricciani L, Olds T, Petkov J. In search of lost sleep: secular trends in the sleep time of school-aged children and adolescents. Sleep Med Rev (2012) 16(3):203–11. doi: 10.1016/j.smrv.2011.03.005
155. Matricciani L, Blunden S, Rigney G, Williams MT, Olds TS. Children’s sleep needs: is there sufficient evidence to recommend optimal sleep for children? Sleep (2013) 36(4):527–34. doi: 10.5665/sleep.2538
Appendix
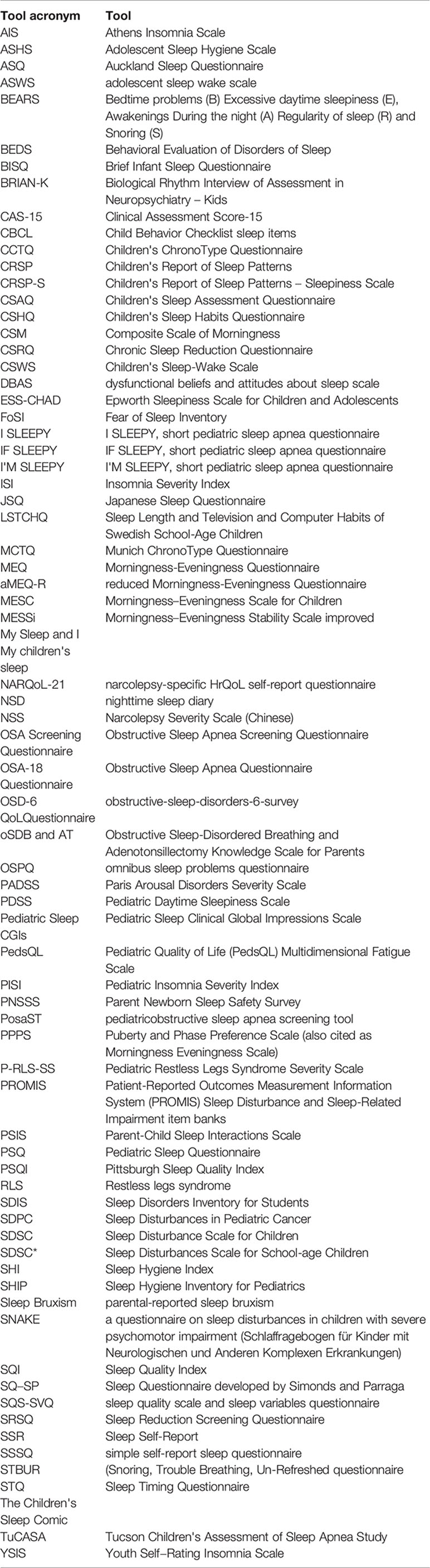
Keywords: sleep duration, sleep quality, sleep hygiene, questionnaire, child, review
Citation: Sen T and Spruyt K (2020) Pediatric Sleep Tools: An Updated Literature Review. Front. Psychiatry 11:317. doi: 10.3389/fpsyt.2020.00317
Received: 16 October 2019; Accepted: 31 March 2020;
Published: 23 April 2020.
Edited by:
Maurice M. Ohayon, Stanford University, United StatesReviewed by:
Thomas Penzel, Charité – Universitätsmedizin Berlin, GermanyAxel Steiger, Ludwig Maximilian University of Munich, Germany
Sejal V. Jain, University of Arizona, United States
Copyright © 2020 Sen and Spruyt. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Karen Spruyt, karen.spruyt@inserm.fr; karen.spruyt@univ-lyon1.fr