 Dehao Chen1,2†
Dehao Chen1,2† Sarah L. McKune1,3†
Sarah L. McKune1,3† Nitya Singh2,4
Nitya Singh2,4 Jemal Yousuf Hassen5
Jemal Yousuf Hassen5 Wondwossen Gebreyes6Mark J. Manary7
Wondwossen Gebreyes6Mark J. Manary7 Kevin Bardosh8
Kevin Bardosh8 Yang Yang2,9Nicholas Diaz3Abdulmuen Mohammed10
Yang Yang2,9Nicholas Diaz3Abdulmuen Mohammed10 Yitagele Terefe11Kedir Teji Roba12Mengistu Ketema13Negassi Ameha14
Yitagele Terefe11Kedir Teji Roba12Mengistu Ketema13Negassi Ameha14 Nega Assefa12
Nega Assefa12 Gireesh Rajashekara6
Gireesh Rajashekara6 Loïc Deblais6
Loïc Deblais6 Mostafa Ghanem6‡Getnet Yimer15
Mostafa Ghanem6‡Getnet Yimer15 Arie H. Havelaar2,4,16*
Arie H. Havelaar2,4,16*- 1Department of Environmental and Global Health, College of Public Health and Health Professions, University of Florida, Gainesville, FL, United States
- 2Emerging Pathogens Institute, University of Florida, Gainesville, FL, United States
- 3Center for African Studies, University of Florida, Gainesville, FL, United States
- 4Department of Animal Sciences, Institute of Food and Agricultural Sciences, University of Florida, Gainesville, FL, United States
- 5Department of Rural Development and Agricultural Extension, Haramaya University, Dire Dawa, Ethiopia
- 6Department of Veterinary Preventive Medicine, The Ohio State University, Columbus, OH, United States
- 7Department of Pediatrics, Washington University in St. Louis, St. Louis, MO, United States
- 8Department of Anthropology, University of Florida, Gainesville, FL, United States
- 9Department of Biostatistics, College of Public Health and Health Professions & College of Medicine, University of Florida, Gainesville, FL, United States
- 10Office of Research Affairs, Haramaya University, Dire Dawa, Ethiopia
- 11College of Veterinary Medicine, Haramaya University, Dire Dawa, Ethiopia
- 12College of Health and Medical Sciences, Haramaya University, Dire Dawa, Ethiopia
- 13School of Agricultural Economics and Agribusiness, Haramaya University, Dire Dawa, Ethiopia
- 14School of Animal and Range Science, Haramaya University, Dire Dawa, Ethiopia
- 15Global One Health initiative, Office of International Affairs, The Ohio State University, Eastern Africa Regional Office, Addis Ababa, Ethiopia
- 16Institute for Sustainable Food Systems, University of Florida, Gainesville, FL, United States
Livestock farming provides a possible mechanism by which smallholder farmers can meet their household need for animal source foods (ASF), which may reduce the risk of stunting. However, direct/indirect contacts with domestic animals may increase colonization by Campylobacter spp., which has been associated with Environmental Enteric Dysfunction (EED) and stunting. A cross-sectional study involving 102 randomly selected children between 12 and 16 months of age was conducted in rural eastern Ethiopia to establish prevalence rates of Campylobacter colonization, EED, and stunting, and evaluate potential risk factors. Data were collected between September and December 2018. The prevalence of EED and stunting was 50% (95% CI: 40–60%) and 41% (95% CI: 32–51%), respectively. Among enrolled children, 56% had consumed some ASF in the previous 24 h; 47% had diarrhea and 50% had fever in the past 15 days. 54, 63, 71 or 43% of households owned at least one chicken, cow/bull, goat, or sheep; 54 (53%) households kept chickens indoors overnight and only half of these confined the animals. Sanitation was poor, with high levels of unimproved latrines and open defecation. Most households had access to an improved source of drinking water. The prevalence of Campylobacter colonization was 50% (95% CI: 41–60%) by PCR. In addition to the thermotolerant species Campylobacter jejuni, Campylobacter coli and Campylobacter upsaliensis, non-thermotolerant species related to Campylobacter hyointestinalis and Campylobacter fetus were frequently detected by Meta-total RNA sequencing (MeTRS). Current breastfeeding and ASF consumption increased the odds of Campylobacter detection by PCR, while improved drinking water supply decreased the odds of EED. No risk factors were significantly associated with stunting. Further studies are necessary to better understand reservoirs and transmission pathways of Campylobacter spp. and their potential impact on child health.
Introduction
Undernutrition has been identified as an underlying cause in 45% of under-five mortality globally (1). In Africa, an average of 31.2% of children under-five are stunted, which indicates chronic undernutrition and is represented by length/height for age Z-scores (LAZ/HAZ) of −2 or more standard deviations below median length/height for age of a reference population. Stunted children are short in stature for their age, at increased risk of infectious diseases and vaccine failures, have poor cognitive development, resulting in increased morbidity and mortality and lower lifetime productivity, and income (2–5). In Ethiopia, rates of stunting among children under-five are alarmingly high—up to 38% based on a 2018 report (6). A recent study indicates that average LAZ in a large sample (N = 1,750) of Ethiopian children decreased from −0.7 to −2.0 between 6 and 18 months of age (7). Linear growth faltering during this time period in a child's life therefore not only significantly contributes to the stunting events but also to the overall health status later in life.
Animal-source foods (ASF), including milk, meat, and eggs, have been shown to dramatically decrease undernutrition in children under-five (4, 8). The demand for ASF in Africa is growing rapidly alongside population growth, with projected increases of 145 and 155%, respectively in the demand for meat and milk, between 2005 and 2050 (9). In 2030, egg consumption is projected to be increased by 155% in comparison to 2000 (10). Considering the large increases in the demand of ASF for improving nutritional status and generating income opportunities, the Ethiopian Livestock Master Plan (LMP) aims to significantly increase livestock production in the country (11). However, successful implementation of the LMP will also lead to higher livestock densities in human dwellings and more frequent exposure of human populations to zoonotic pathogens, including Campylobacter spp. Next to food and water mediated transmission, direct fecal-oral transmission pathways of zoonotic pathogens to humans are known, mainly through direct contact with animal excreta and contaminated objects in the environment. Occurrence of zoonotic infections may limit the potential benefits of livestock production (7, 12). In Ethiopia, especially the eastern part, chickens, cows, goats, and sheep have close interaction with family members in the homestead. An ethnographic study in the Haramaya woreda (district) in eastern Ethiopia found that chickens and small ruminants are frequently housed in the home overnight with a half-wall barrier separating the livestock animals and the sleeping place of the family members, and frequent contacts between children and farm animals and their contaminated environments occur (13). This cohabitation with livestock creates a distinct opportunity for transmission of zoonotic pathogens from livestock to children (13).
Research highlights that the presence of livestock and their feces may be important risk factors for child malnutrition, particularly stunting (14, 15). The importance of animal feces as a source of exposure to enteric pathogens, causing diarrhea and EED, has been well-documented in recent years. Studies have indicated a strong correlation between poultry ownership and linear growth faltering among children under-five at households. In particular, the overnight presence of chickens within the household was associated with a decrease in HAZ in several countries including Ethiopia (14, 16). A 2017 study found the presence of animal feces to be significantly associated with a lower HAZ score in children 6–24 months of age in Ethiopia (7).
Stunting cannot be completely reversed by optimized diet and reduced diarrhea, leading to the hypothesis that a primary underlying cause of stunting is subclinical gut disease, known as environmental enteric dysfunction (EED) (14). EED is associated with unsanitary disposal of feces, contaminated water supplies, and the presence of domesticated animals in or around the home (14). Increasing evidence suggests that repeated or persistent asymptomatic (i.e., without diarrheal illness) colonization with enteric pathogens may result in EED and stunting (15, 17). Therefore, assessment of the colonization of children with enteric pathogens, or more broadly full characterization of the gut microbiota, is critical to further understanding the complex interactions between pathogens, the environment, and human hosts ultimately leading to malnutrition and other poor health outcomes in children.
Poultry and other warm-blooded animals are the natural reservoirs of thermophilic Campylobacter spp. (18). Humans and other higher primates may develop disease after intestinal colonization with Campylobacter spp. (19). Diarrheal disease (the most commonly observed), and autoimmune diseases, as well as digestive disorders, may be triggered after infection with Campylobacter spp. (20). A study in Peru indicated that asymptomatic and symptomatic Campylobacter infections were associated with reduced weight gain over a three-month period, and symptomatic Campylobacter infections were marginally associated with reduced linear growth over a nine-month period (21). A recent multi-center study identified a high prevalence of Campylobacter spp. in stool samples of primarily asymptomatic children in low-resource settings being associated with a lower LAZ score and increased level for markers of EED (intestinal permeability and intestinal and systemic inflammation) at 24 months of age (15). Thermotolerant species including Campylobacter jejuni and Campylobacter coli are the most frequent causes of bacterial enteritis globally (22). Non-thermotolerant Campylobacter species (e.g., Campylobacter hyointestinalis, Campylobacter fetus, and Candidatus Campylobacter infans) are a diverse group of bacteria, whose pathogenic mechanism is not-well-established (23). In a follow-up study, fecal samples were tested with quantitative polymerase chain reaction (PCR) for a large array of enteropathogenic organisms, and C. jejuni/C. coli were among a limited number of pathogens significantly associated with decreased LAZ, and the only pathogens maintaining this consistent trend in a longitudinal model (17). A causal role of Campylobacter spp. in the pathology of EED has been recently observed in a mouse model. When diets were deficient in zinc, consistent bloody diarrhea and weight loss were observed, as well as elevation of fecal inflammation markers of EED including fecal myeloperoxidase (MPO) in mice infected by C. jejuni (24).
These lines of evidence converge to suggest that Campylobacter species, a natural inhabitant of the gastrointestinal tract of livestock and poultry, are among the main pathogenic bacteria involved in the causal chain of stunting. Nevertheless, in Ethiopia, little research has been conducted to estimate the reservoirs or transmission pathways of Campylobacter colonization. The association of Campylobacter with EED and stunting, due to young children's direct or indirect exposure to feces of these animals, and socio-demographic factors that may affect this association are not well-understood. To fill these knowledge gaps, the formative research of the project, Campylobacter Genomics and Environmental Enteric Dysfunction (CAGED), includes a cross-sectional epidemiological investigation involving young children to estimate the prevalence and species diversity of Campylobacter spp. in gut microbiota in relation to the prevalence of EED and stunting. Results of PCR and metagenomic analyses of gut microbiota, reflecting Campylobacter species prevalence along with microbial diversity among the young children are presented in a companion manuscript (25). Here we aim to better understand the relationships of Campylobacter colonization in the intestine of children with the occurrence of EED and stunting and divulge potential risk factors in their socio-demographic context.
Materials and Methods
Study Design and Population
A community-based cross-sectional study, including a questionnaire-based surveillance of the households and collection of child growth data, child urine, and fecal samples were performed in the Haramaya woreda (district), East Hararghe Zone, Oromia Region, Ethiopia. Beginning in 2018, Haramaya University (HU) initiated a full household enumeration of 12 kebeles (wards) within Haramaya woreda using methods developed for the Kersa Health and Demographic Surveillance System (26). For this cross-sectional study, five out of the 12 kebeles were selected in a way to capture the spatial heterogeneities in the landscape (e.g., land use, land cover, altitude, agricultural practices) that could influence risk factors contributing to health outcomes.
Eligibility criteria of this study were designed to enroll children receiving traditional maternal care and without underlying health conditions that might affect the primary study outcomes. Previous studies (MAL-ED) have indicated that the prevalence of Campylobacter spp. in children in low- and middle-income countries (LMIC) increases linearly in the first year of life and then reaches a steady state or slow decline with peak levels occurring around 12 months of age (15). A child was included in the study if he/she was 11–13 months of age when consent was given, and if the child's mother was the caretaker. The child was excluded from the study if he/she presented visible congenital abnormality or had serious medical illnesses, or the child or his/her mother required extended stay in hospital after birth. Households with at least three chickens within the homestead (defined as the small collection of households that are physically connected to one another), willing to participate and conform to the requirements of the study were included. Families not residing in Haramaya woreda for at least 3 months, currently participating in another study on animal husbandry, or with a mother who did not live in Haramaya woreda when the child was born were excluded.
The sample size of this study considered estimation of the three primary outcomes: Campylobacter colonization, EED, and stunting. Based on a binomial distribution, a sample size of 100 for the whole study population allowed estimation of a 50% prevalence with precision of 10 at 95% confidence (R function binom:: binom.confint).
While adjusting for population weight of kebeles, 102 children (one child from each household) were randomly selected from the sampling frame of the selected five kebeles. Field work started on October 16, 2018 and continued for 10 weeks until December 21, 2018. The enrolled children and their mothers were invited to come to a local health post or administration office for anthropometric measurements, administration of a sugar solution, and collection of a urine sample for each child for later measurement of lactulose excretion (a marker for EED in urine), as well as completion of interviews and providing a fecal sample for each child.
Field Activities
Questionnaires were developed in collaboration with the Haramaya University (HU) field team using validated indices whenever possible, such as minimum dietary diversity of infant and young children (MDD-IYC). In consultation with social scientists and field workers, the study questionnaire was finalized so that it was culturally appropriate and locally adapted. In the local language (Afan Oromo), bilingual data collectors collected information on demographics, livelihoods, wealth, animal ownership, animal management and disease, water, sanitation and hygiene, health, and nutrition. Study data were collected and managed using REDCap electronic data capture tools hosted at the University of Florida Clinical and Translational Science Institute (27).
Collection and Analyses of Stool and Urine Samples
During the implementation of household surveillance, stool samples from the selected children were also collected aseptically in a sterile plastic sheet for EED and PCR analyses, and meta-total RNA sequencing (MeTRS, a culture-independent sequencing method that profiles the presence and quantity of RNA transcripts in a sample). Samples were flash-frozen in the field using liquid nitrogen and stored at −80°C until further use. Genomic DNA and RNA were extracted for conventional PCR and MeTRS, respectively (25). Details of laboratory procedures on PCR and MeTRS were described in Terefe et al. (25). For the dual sugar absorption test, an oral solution consisting of 200 mg L-rhamnose and 1000 mg lactulose in 10 mL sterile water was prepared as previously described (28). Study personnel administered the entire solution to each child over a period of 5 min. A urine bag was then placed on the child 30 min after consuming the solution and all urine collected over the subsequent 60 min was returned to the data collector. Analysis of lactulose and rhamnose was conducted according to a previously described procedure (29, 30). In stool samples, myeloperoxidase (MPO) was measured using a commercially available enzyme-linked immunosorbent assay (MPO RUO, Alpco, Salem, NH). One child had severe diarrhea and difficulty in producing feces, we were unable to collect a fecal sample from him; another child produced a small amount of feces that was only sufficient for PCR testing. The samples sizes for PCR, MeTRS, and MPO analyses were therefore 101, 100, and 100, respectively.
Threshold cutoffs for moderate and severe EED based on the dual sugar absorption test and fecal MPO were defined following previously described methods (31, 32). As reported by Ordiz et al. (31), urinary excretion of lactulose and rhamnose were highly correlated as illustrated in Supplementary Figure 1, and following these authors, we adopted the percentage of lactulose excretion as a biomarker for gut permeability associated with EED. Cutoff values for the percentage of lactulose (%L) were as suggested by Agapova et al. (33): 0.2 < %L ≤ 0.45% for moderate EED, and %L > 0.45 for severe EED. Following Kosek et al. (32), we defined a threshold for fecal MPO of 2,000 ng/ml for gut inflammation and the third quartile of the observed data (11,000 ng/ml in our cohort) as a threshold for severe inflammation.
Anthropometric Measurements
The child's weight, recumbent length, and Mid-Upper Arm Circumference (MUAC) measurements were collected by trained caregivers using Seca 334 baby scales, Seca 417 length boards (Itin Scale Co., Inc., Brooklyn, NY), and MUAC tape precise to 0.01 kg, 0.1, and 0.2 cm, respectively. Length measurements were taken three times. The average length was calculated by taking the arithmetic mean of the data after outlier removal as described in Supplementary Appendix 1. Length-for-age, weight-for-age, and weight-for-length Z scores (LAZ, WAZ, and WLZ, respectively) were calculated according to WHO Child Growth Standards using R package anthro. Severe acute malnutrition was defined according to Ethiopian clinical standards (MUAC <110 mm and length >65 cm or a WLZ ≤ −3) (34).
A total of 12 children with one (or more) of the following medical condition(s) were referred to a healthcare facility, including four cases of dehydration, five cases of diarrhea and fever, and six cases of diarrhea. Two children were referred to a health post for additional follow-up for severe acute malnutrition.
Data Analysis
Primary outcome variables of interest were Campylobacter colonization (by PCR), EED, and stunting. Descriptive analysis was undertaken to explore background features of the study population. 95% binomial proportion confidence intervals for prevalence were based on Wilson score. Explanatory variables potentially associated with the outcome variables were selected based on a priori knowledge (1–4, 7, 8, 10, 12, 13, 16). All data analyses were performed in the statistical language R version 3.5.1 (35).
Composite variables were generated to assist in analyzing the sociodemographic data. We created Water, Sanitation, and Hygiene (WASH) ladder variables (i.e., drinking water, sanitation, and hygiene ladders) based on the Joint Monitoring Program (JMP) by WHO and UNICEF (22, 36). Tropical livestock unit (TLU), a composite metric for quantifying all farming animals in a household, was calculated following published literature (37).
Bivariate and multivariate analyses were conducted to explore associations between the three outcome variables and potential explanatory variables using unadjusted and adjusted logistic regression models [controlling for child's age (in days), sex, and kebele of residence]. To strengthen the robustness of the models, continuous [i.e., child's and mother's age, TLU, household wealth (asset and income)] and ordinal explanatory variables were, respectively dichotomized by medians or generally accepted cut-offs (i.e., minimum dietary diversity score of 5). We established multiple exposure models by including the three confounders (child's age group, sex, and kebele of residence) and candidate variables with p-values < 0.20 from the adjusted single exposure models (Supplementary Tables 4–6), and backward stepwise selections were conducted to sort out the significant explanatory variables (38). Given the small sample size, all p-values and 95% confidence intervals (CIs) were estimated by likelihood-ratio (LR) test, and we did not include interaction between the explanatory variables in the models. Observations with missing values were excluded from the analyses.
Results
Sociodemographic Characteristics
Child Health and Diet
At the time of data collection, the mean age of children was 428 days (SD = 31, range 360–498 days). As reported by mothers, nearly half (47%) of children had experienced diarrhea (defined as three or more loose or watery stools) in the previous 15 days, while 12% currently had diarrhea in the previous 24 h; half (50%) of children experienced fever in the previous 15 days, with 5% currently having fever in the previous 24 h (Table 1). Based on the caregiver survey, 35% of the children encountered both fever and diarrhea in the previous 15 days, and 3% currently had both symptoms.
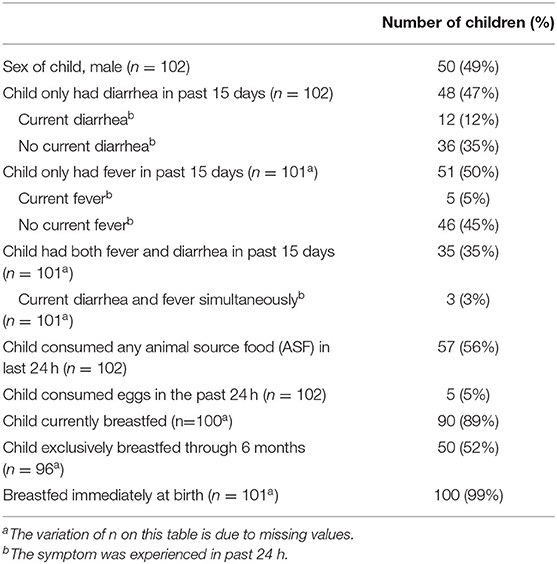
Table 1. Child health and diet in five rural kebeles in Haramaya woreda, Eastern Ethiopia.
Within the sample population, 99% of children were breastfed at birth and 89% were still breastfed at the time of data collection (Table 1). The rate of exclusive breastfeeding through 6 months was low, at 52%, indicating that just under half of the children had received supplementary food other than breastmilk to eat or drink prior to 6 months of age (36) (Table 1).
According to 24-h food recall by mothers, only 9% of children met the minimum dietary diversity threshold for infants and young children (MDD – IYC) of consuming five out of eight food groups (note: breastmilk is included in this measure). However, 56% (57/102) of children had consumed animal source food, of whom a strong majority (93%, 53/57) consumed milk and relatively few (9%, 5/57) consumed eggs. Consumption of goat's milk by children is not very common in the area and heat treatment of milk is uncommon in rural areas. Thus, reports of milk being consumed by young children are most likely unpasteurized cow's milk, though this was not specified in the questionnaire. No child was reported to have consumed any animal meat or flesh product. Most children consumed 3–4 food groups (range 1–6 food groups), mainly from the food groups of (1) grains, roots, and tubers, (2) legumes and nuts, and (3) breastmilk.
Water, Sanitation, and Hygiene (WASH)
Sanitation, drinking water, and hygiene ladders indicate very low levels of WASH conditions. Only 23% of households used improved sanitation facilities shared between households (limited), and 77% of households practiced open defecation (Sanitation Ladder, Table 2). We observed 56% of respondents reported drinking water from an improved source that required <30 min for a roundtrip collection. 42% of respondents also had access to an improved source, however it required more than 30 min to collect, while only 2% reported having access to a safely managed drinking water source located on premises, available when needed, and not contaminated by fecal and chemical pollutants (see Drinking Water Ladder, Table 2). Among women, 93% reported having no place to wash their hands, while 7% had a facility, but without soap and water.
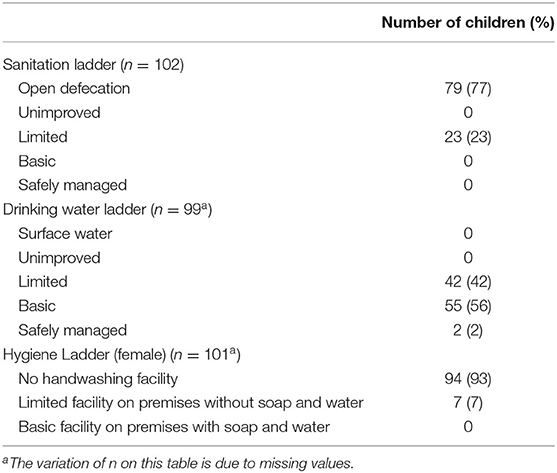
Table 2. Water, sanitation and hygiene indicators in five rural kebeles in Haramaya woreda, Eastern Ethiopia.
Animal Husbandry
Most families (94%) owned some livestock, typically the equivalent of 2-3 TLU, and 54, 63, 71, and 43% of households had at least one chicken (range 0–15 chicken), one cow/bull (range 0–7 cattle), one goat (range 0–10 goat), and one sheep (range 0–7 sheep), respectively. Very few other animals were reported, including cats, dogs, camels, and others.
Of the 54% of households who reported owning chickens, all but one respondent reported keeping their chicken(s) within the house at night. To characterize the increasing likelihood of contact between chickens and study participants based on poultry management practices, we defined a Chicken Nighttime Location risk score as elucidated in Table 3. Households who either had no chickens or did not keep them in the home at night (46%) were assigned a chicken nighttime risk score of 0; another 26%, who kept their chickens in the home at night but reported confining the chicken within the household, were assigned a risk score of 1; and the remaining 28%, who kept their chicken in the home without confinement, were assigned a risk score of 2 (Table 3).
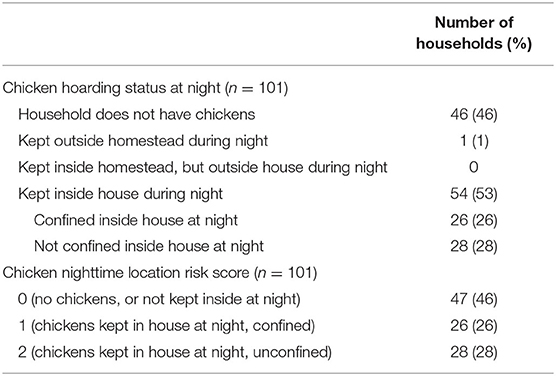
Table 3. Chicken husbandry for sampled households in five rural kebeles in Haramaya woreda, Eastern Ethiopia.
Campylobacter Colonization
Campylobacter prevalence in child fecal samples was 50% (95% CI: 41–60%, n = 101) as deduced from PCR-based detection (23), and 12% of the children were reported to have current diarrhea. MeTRS revealed 88% (95% CI: 80–93%, n = 100) prevalence of the genus Campylobacter among the studied samples. Eight Campylobacter species showed the highest prevalence: C. jejuni, C. hyointestinalis, C. coli, Campylobacter sp. RM6137, C. upsaliensis, an uncultured Campylobacter sp. and Campylobacter sp. RM12175 (Table 4). Interestingly, most of the children (82%, n = 100) were observed to be infected with multiple species of Campylobacter.
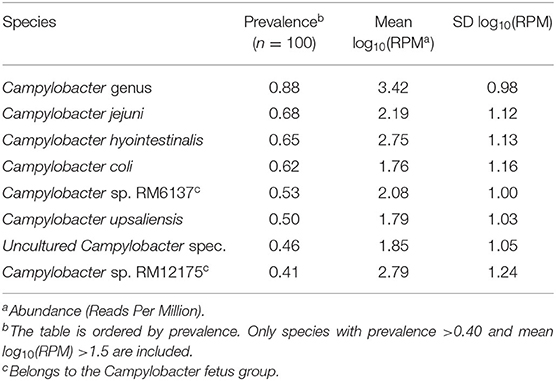
Table 4. Campylobacter species detected in child fecal samples by Meta-total RNA sequencing (MeTRS) in five rural kebeles in Haramaya woreda, Eastern Ethiopia.
EED
As expected, absorption of lactulose ( = 0.27) and rhamnose ( = 4.03) are highly correlated (Pearson's ρ= 0.44, P-value < 0.01) (Supplementary Table 1 and Supplementary Figure 1). Based on the specified threshold cutoffs for MPO and %L biomarkers, the prevalence of EED in the study children was deduced to be 50% (95% CI: 40–60%, n = 100), among whom 17% (95% CI: 11–26%) had severe EED (Supplementary Table 2).
Anthropometry
Comparing with the reference distribution of LAZ and WLZ (both with a mean = 0 and SD = 1), the full distribution of LAZ values was shifted to the left, while the distribution of WLZ had a mode at 0 but was tailed to the left (Figure 1). The means for LAZ, WAZ, WLZ, and MUAC were −1.88 (SD = 1.56), −1.25 (SD = 1.18), −0.42 (SD = 0.91), and 130 mm (SD = 11), respectively (Supplementary Table 3). Stunting was observed in 41% (95% CI: 32–51%) of the study population, while severe stunting occurred in 19% (95% CI: 12–27%) of the children (Table 5). Wasting and severe wasting were observed in 5% (95% CI: 2–11%) and 1% (95% CI: 0–5%) of the population, respectively, and 3% (1–8%) of children were both stunted and wasted (Table 5).
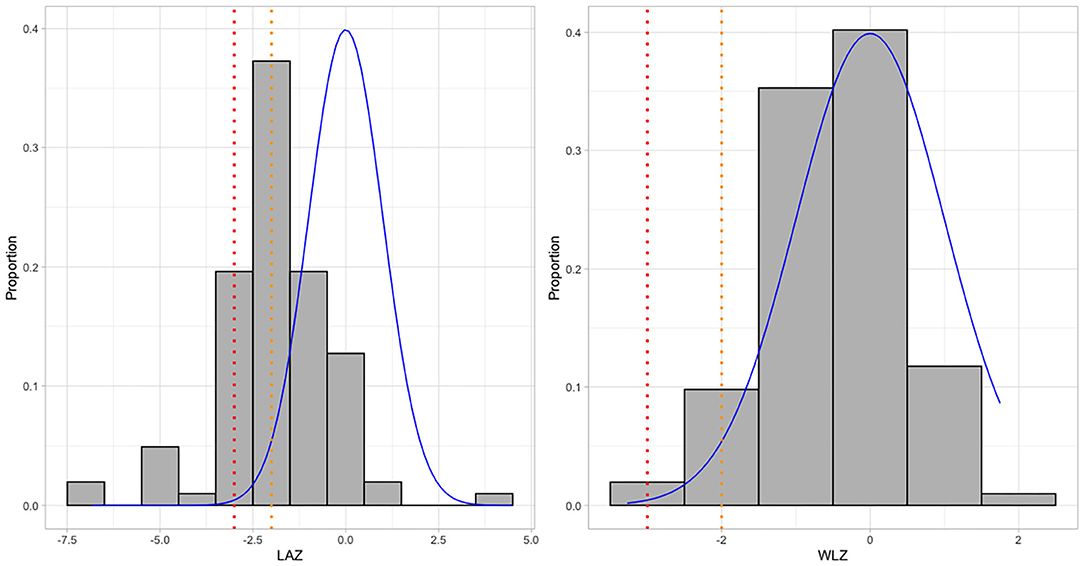
Figure 1. Distribution of LAZ & WLZ compared to WHO normal growth standards in five rural kebeles in Haramaya woreda, Eastern Ethiopia. The histograms show the distribution of LAZ and WLZ in the sample; the blue curve shows a standard normal distribution of WHO growth reference (μ = 0, σ = 1). Orange and red dotted lines indicate thresholds for stunting/wasting (Z score <-2) and severe stunting/wasting (Z score <-3), respectively.
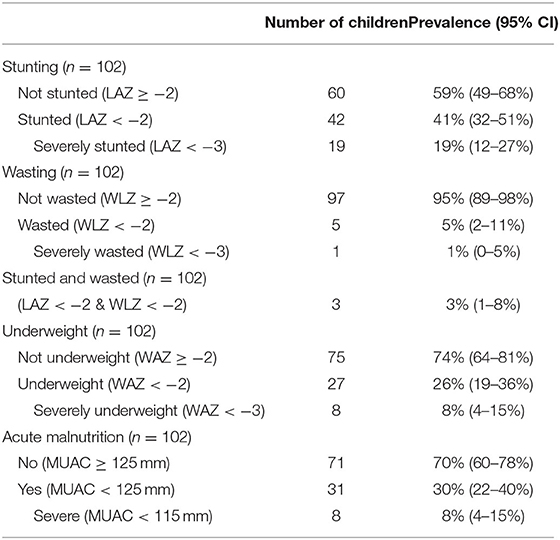
Table 5. Stunting and wasting levels in five rural kebeles in Haramaya woreda, Eastern Ethiopia.
Risk Factor Analyses
Supplementary Tables 4–6 present crude and adjusted odd ratios, and Table 6 depicts the models with single (with p [probability]-values <0.2) and multiple risk factor(s), i.e., the Campylobacter model considering children's current breastfeeding and animal source food consumption practices as risk factors. The five kebeles could be categorized into three sets by assembling the three kebeles with similar prevalence of Campylobacter (by PCR) into a new group as a confounder for kebele effect in Campylobacter models (Supplementary Table 4). Given this three-level kebele effect did not yield statistically different prevalence of EED and stunting (Supplementary Tables 5, 6), this scheme was kept in the models of these two outcomes (i.e., EED and stunting) to account for spatial heterogeneity. Statistical analysis showed that the group of children who are being breastfed and also currently consuming ASF had significantly higher odds for the presence of Campylobacter spp. when adjusting for confounders and other risk factors at the 5% level (Table 6). EED was treated as a binary variable by combining categories of moderate and severe EED as listed in the Supplementary Table 2. The household's access to a basic or safely managed drinking water source significantly reduced the odds of EED at the 5% level (Table 6). No significant crude or adjusted associations were found between stunting and any of the explanatory variables (Supplementary Table 6), hence multiple exposure models were not constructed. Also, the aforementioned associations (measured through the logistic regressions) between the explanatory factors and the three health endpoints (i.e., colonization with Campylobacter spp., EED, and stunting) and their prevalence estimates are depicted in Figure 2.
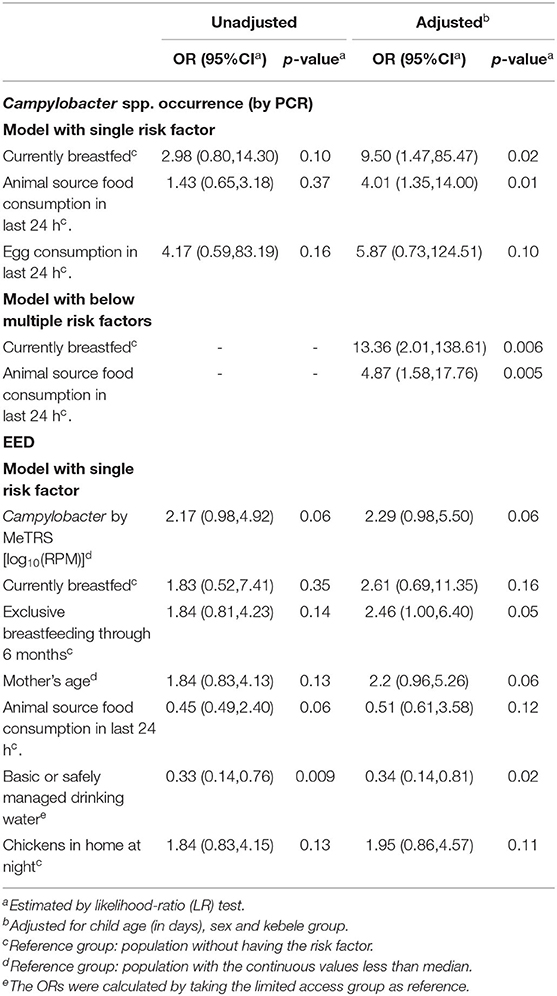
Table 6. Univariate and multivariate models for Campylobacter and EED outcomes of children in Haramaya woreda, Eastern Ethiopia.
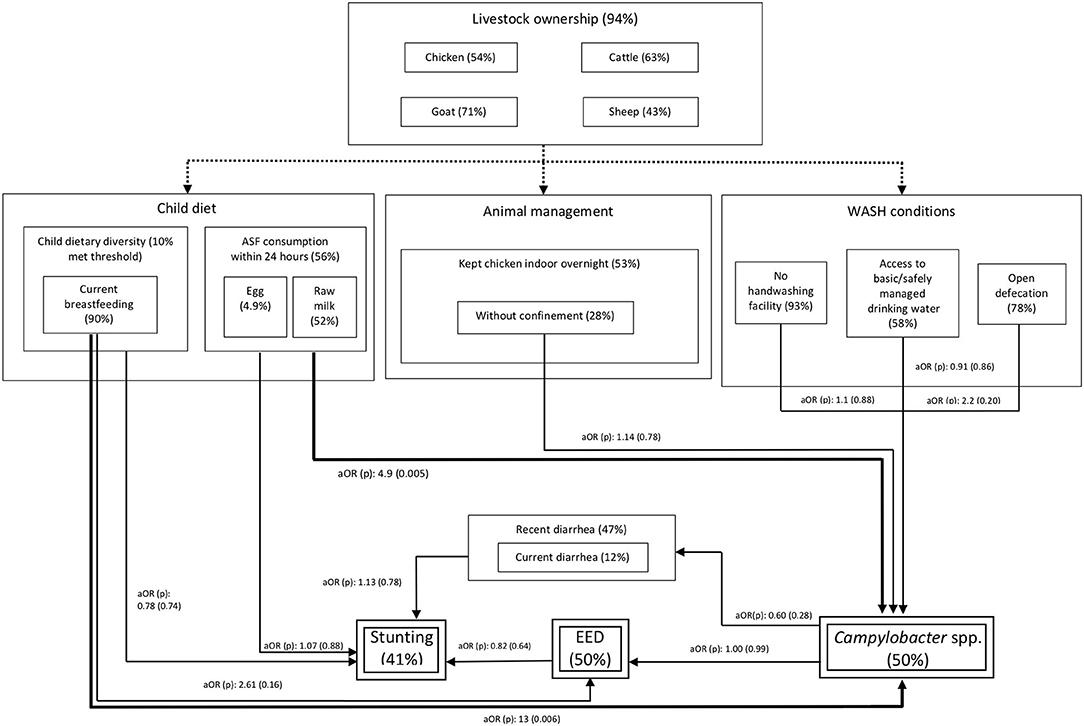
Figure 2. Putative relationships between animal ownership and management, WASH conditions, diets and the main outcome variables in this study: colonization of children with Campylobacter spp., environmental enteric dysfunction (EED) and stunting. The rounded-dot dash lines represent the complex interactions between livestock ownership and risk factors explored in this study. The thick bold lines represented significant (p < 0.05) associations in the multivariate models. The thinner lines represent tested associations in the single exposure models. aOR: adjusted odds ratio (p-value in parenthesis).
Discussion
The socio-demographic context in rural Ethiopia and the complex, multifactorial eco-pathological processes that influence the colonization by Campylobacter, occurrence of EED, and impaired growth among children make it challenging to identify causative factors and exposure routes of the pathogen. Nevertheless, the findings from the household surveys are useful in understanding the high prevalence of malnutrition, poor gut health, and Campylobacter colonization of young children. Within the complex network of pathogens exposures, animal husbandry and the presence of domestic animals have been shown to be associated with higher burdens of Campylobacter colonization, acute disease (e.g., diarrhea, fever), and chronic outcomes such as EED and stunting. The results of this study also indicate that the detrimental effects to child health of insufficient WASH and poor animal husbandry conditions are likely exacerbated by poor diets. The strengths of our study include the application of mixed-method and following of the “One Health” approaches, allowing transdisciplinary and multisectoral teams to collaborate.
Undernutrition
According to the 2018 Global Hunger Index, Ethiopia ranks 93rd out of 199 qualifying low/middle income countries and suffers from a level of hunger that is considered serious (39). The prevalence of stunting in children under 5 years of age has decreased from 57.4% in 2000 to 38.4% in 2018. In the study area, we found that the prevalence of stunting among children 12–16 month of age is 41% (95% CI: 32–51%), which is higher than a 2020 study in southern rural Ethiopia (31.4%) (40). Conversely, our study found a lower rate of wasting 5% (2–11%) compared to the southern rural region in this country (14.3%) (40). On the other hand, in rural Ethiopia, average HAZ value has been reported to be −1.7 at approximately 9.6–20 months of age (7), whereas the average LAZ in our setting at that age was −1.9. Hence, chronic malnutrition in the area of this study appears to be more serious than the country's rural average.
Campylobacter Species Diversity and Risk Factors
The prevalence of Campylobacter spp. among almost 50% of the under-five children in our setting is similar to Tanzania from the MAL-ED study and another recent surveillance study conducted in southern rural Ethiopia (15, 40), when measured by PCR, confirming a high burden of Campylobacter colonization. High exposure to pathogenic microorganisms is also indicated by high prevalence of diarrhea and fever (41, 42). The results of this study aligns with findings from previous studies that indicate a considerable number of diarrheal episodes can be associated with Campylobacter spp., which is one of the most commonly detected species in stool samples in Peru, South Africa, Brazil, and Nepal (41, 42). The metagenomic results confirmed that the thermotolerant C. jejuni and C. coli, which are commonly associated with chickens and livestock, are frequently colonizing at high abundance levels in the gut of young children, that we have also presented in more details (18). Notably, we observed the presence of C. upsaliensis, which is a member of the C. jejuni group but commonly associated with cats and dogs. An important finding of our study is the occurrence of a large number of other, non-thermotolerant Campylobacter species known to be highly diverse. Their reservoirs are poorly characterized, especially in low- and middle-income countries. The frequent presence of these non-thermotolerant species, including C. hyointestinalis, showing higher abundance than C. jejuni/C. coli, indicates a salient impact of various animals on child health in Ethiopia. Previous studies have shown that intestinal colonization of C. upsaliensis, C. fetus, and C. hyointestinalis can induce gastroenteritis in humans (43–45). Apart from human isolates, C. hyointestinalis subsp. hyointestinalis has been mainly isolated from ruminants while C. hyointestinalis subsp. lawsonii has been isolated from pigs (46). The primary reservoirs of C. fetus subsp. fetus include cattle and sheep, but this subspecies has also been isolated from the feces of other animal species. Among the Campylobacter spp. identified by MeTRS in this study, C. fetus subsp. venerealis is a cause of infection in cows (44), and Campylobacter sp. RM 6137 and Campylobacter sp. RM12175 are unnamed novel species in the C. fetus group that have been isolated from feces of wild pigs and cows, respectively (47). Therefore, frequent occurrence of C. jejuni/C. coli in children supports the hypothesis that chickens are a main reservoir of these bacteria. The presence of other species of Campylobacter implies that domestic and farmed animals other than poultry may also significantly contribute to environmental exposure and colonization of children. This inference is further supported by the increased risk of Campylobacter colonization associated with ASF consumption, which in this region mainly includes raw cow's milk (Table 6).
The observed significantly increased risk of Campylobacter colonization associated with current breastfeeding, which is in accordance with a growing body of evidence indicating that exclusive breastfeeding may provide a gut environment, more favorable to growth of (certain species) of Campylobacter (23, 48). It is currently not clear how breastfeeding provides a competitive advantage to Campylobacter species in the infant gut (23). Nonetheless, the significance and importance of breastfeeding for overall child infant nutrition, development, and protection against infectious diseases is well-documented (48). Our findings should not be interpreted as to discourage breastfeeding of infants and young children but underscore the importance of controlling Campylobacter exposure, as well as overall gut health, to protect and ensure proper growth of children.
EED
There is no gold standard for classifying EED based on biomarkers, and different approaches have been used to define this endpoint (28, 32). We adopted the Lactulose: Rhamnose test, which is now considered more appropriate than the Lactulose: Mannitol test as a marker for intestinal permeability, and MPO as a well-established marker of neutrophil activity and gut inflammation (28). A classification based on these two markers was then used to define moderate and severe EED and revealed a high burden of EED in our study area. Fecal MPO results are known to be strongly variant within and between populations geographically. The median MPO concentration in our setting is lower than the median of all sites in the MAL-ED cohort (32). This does not necessarily imply a lower EED burden in our study population, because the variance of MPO may be due to different age of children in the two studies, since MPO is age-dependent (49).
Child Health and Nutrition
Typically, the diarrheal prevalence has been reported to be 20–25% among the under-five children in the study region (50, 51). However, the mother interviewed in our study have reported a higher prevalence (48%) of recent diarrhea (in the previous 15 days) among the children aged between 12 and 16 months. A high prevalence of recent diarrhea in children, as reported by their mothers, has also reported from Pakistan (63%), Bangladesh (53%), and Peru (53%), whereas lower prevalence was reported in India (21%), Nepal (27%), South Africa (4%), Tanzania (6%), and Brazil (5%) (15). These differences in diarrheal prevalence might be due to variations in selection criteria, geo-climatic conditions, and WASH and feeding practices. For example, in congruence to our study, increased diarrhea has been found in populations consuming more milk in southeast Asia (52). Further investigation of the microbial content of ASF, as well as more careful characterization of symptomatic diarrhea would aid in better understanding this potential driver of stunting among different child cohorts.
Only 9% of children in our study population met the MDD-IYC of five out of eight food groups (53). While intake of diverse ASF can significantly improve child diet quality, no child consumed any animal flesh, only about half of children consumed dairy products, and very few of them consumed eggs. Though seasonality of diet may vary significantly in parts of Ethiopia (54), evidence does not suggest that these data reflect lower than normal rates of MDD-IYC than would otherwise be observed in the study area. Moreover, increased diversity in ASF for younger children may vary seasonally with parents income (55), which was not captured in this study.
Influence of WASH Status and Livestock Management
Our fieldwork indicated that people in the Haramaya woreda do not consider exposure to animal feces a public health issue, and household members in the community had little knowledge or concern about the risks of zoonotic exposure. In the study region, access to or use of proper sanitation facilities was observed to be very poor and human and/or animal excreta were found scattered in most homesteads. Despite the general suboptimal drinking water supply, we found access to the basic or safely managed source of drinking water was associated with reduced odds of EED. This emphasizes the necessity of improving the drinking water supply in the study region. Moreover, people's perception of the significance and adequate practice of hand-washing was low in general. The above contexts of WASH practices could not only induce microbial exposure (e.g., Campylobacter spp.) to the mothers but also to their children.
Most of the study families had their own livestock and poultry, and most animals were freely roaming around without proper management of animal droppings. As observed, most of the families kept the smaller animals in house overnight due to security concerns; in over half of households, chickens roamed freely within household compounds during nighttime. This kind of animal husbandry, in addition to the poor status of WASH practices, place human populations at high risk of exposure to zoonotic pathogens and may explain the observed high prevalence of Campylobacter and EED in children. Nonetheless, other research underlines the difficulty of unraveling these complex networks: despite multiple observational studies that found household-level WASH to be strongly associated with child linear growth, three landmark randomized clinical trials found WASH interventions had no statistically significant impact on the linear growth, even though effective behavior change and prevalence reduction for some enteric pathogens were achieved (56, 57).
Limitations
Only a few significant associations between explanatory variables and stunting, EED, and Campylobacter colonization among young children could be ascertained, which might be due to relatively small sample size of this study. Other limitations of this study included the use of the cross-sectional survey data to evaluate variation in health status as a consequence of multiple factors interacting on different time scales, including children's diet and breastfeeding practices, and their health conditions (diarrhea and fever statuses), which are complex interactions particularly susceptible to recall bias (58).
Conclusion
Our study reveals high burdens of Campylobacter colonization, EED, and stunting in the traditional rural Ethiopian settings of smallholder farmers. Results of this study indicate that child health in this rural setting may be negatively influenced by poor diversity of diet despite high level of breastfeeding, low level of WASH, in combination with poor livestock management. Common occurrence of emerging Campylobacter spp. was also observed. High prevalence of stunting and undernutrition among young children in this region may be due to chronic exposure to Campylobacter infection. A variety of Campylobacter spp., including thermotolerant C. jejuni, C. coli, and C. fetus and non-thermotolerant C. hyointestinalis species, which commonly occur in not only poultry and livestock but also in pets and wild animals, were observed to occur in high prevalence among young children, many of whom suffering from frequent diarrhea. Our study contributes to a body of literature underscoring the necessity of considering “transformative WASH” in future research to decipher the multifaceted causal pathways between zoonotic pathogens and child growth faltering and better understand how the colonization of children with Campylobacter spp. is related to EED and stunting, against a background of poor WASH and nutritional conditions. Further, a longitudinal study is planned to better understand animal reservoirs and transmission pathways for colonization of children with Campylobacter spp., inducing EED and stunting, against a background of poor WASH and nutritional conditions. In the same study population, an exposure assessment investigation following the Sanipath methodology will be embedded within the longitudinal study to strengthen our collective understanding of children's exposure pathways to these pathogens (59).
Data Availability Statement
Study data are available at https://dataverse.harvard.edu/dataset.xhtml?persistentId=doi:10.7910/DVN/CPCK91.
Ethics Statement
All the study procedures were performed in accordance with the Declaration of Helsinki and ethical approvals were obtained from the Haramaya University Institutional Health Ethics Research Review Committee (Ref. No. IHRERC/152/2018), the Ethiopia National Research Ethics Review Committee (Ref. No. MoST/3-10/168/2018), the Institutional Review Board at the University of Florida (UF) (Ref. No. 201703252), and Washington University School of Medicine (Protocol No. 201806021). The operational district officers and local village chiefs were informed about the objectives of the study, and their consent was obtained through a Community Advisory Board established for the study (60). Written consents were also obtained from both the child's mother/caregiver and father. Material and Data Transfer Agreements (MDTA) were signed between HU and all US-based partners. Export permits to ship biological specimens from Ethiopia to the U.S.A were approved by the Ministry of Science and Higher Education of Ethiopia (Ref. No. SHE/SSM/19.1/008/11/19).
Author Contributions
AH, SM, JY, WG, MM, KB, YY, and GR conceived and designed the study. SM, NS, AM, and KR designed and implemented the survey. AM, MK, NAm, NAs, and YT supervised sample collection, data collection, and laboratory analysis. YT, LD, and MG the samples. DC and ND cleaned and processed the data. DC analyzed the data, with supervision from AH, SM, and YY. DC, SM, and AH wrote the manuscript. All authors contributed to the revision of the manuscript.
Funding
The University of Florida was funded by the Bill & Melinda Gates Foundation to research and address food insecurity issues in Ethiopia and Burkina Faso through the project Equip—Strengthening Smallholder Livestock Systems for the Future (Grant Number: OPP11755487). These funds are administered by the Feed the Future Innovation Lab for Livestock Systems, which was established by funding from the United States Agency for International Development (USAID) and is co-led by the University of Florida's Institute of Food and Agricultural Sciences and the International Livestock Research Institute. Support for the Feed the Future Innovation Lab for Livestock Systems is made possible by the generous support of the American people through USAID. The contents are the responsibility of the authors and do not necessarily reflect the views of USAID or the United States Government.
Conflict of Interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Acknowledgments
We thank Beyan Abdullahi, Yeharerwork Abebaw, Elias Ahmed, Ibsa Ahmed, Jafer Amin, Bahar Mummed, Seyum Tezera, Ibsa Usmane (Haramaya University), Isabel Ordiz (Washington University in St. Louis), Yosra Mohamed (Ohio State University), Jenna Daniels, and Anna Rabil (University of Florida) for their contributions to the project. We thank Srevi Devaraj (Clinical Chemistry and POCT, Texas Children's Hospital, Baylor College of Medicine, Houston, TX) for analysis of sugars in the dual sugar absorption test and Vida Ahyong and Katrina Kalantar (Chan Zuckerberg Biohub, San Francisco, CA) for their support in performing and interpreting the shotgun sequence analysis. The CAGED project was supported by a Technical Advisory Group consisting of Eric Fèvre (University of Liverpool and Ineternational Livestock Research Institute), Nigel French (Massey University), Aulo Gelli (International Food Policy Research Institute), Andrew Jones (University of Michigan), Vivek Kapur, (Penn State University), Nick Juleff and Supriya Kumar (Bill & Melinda Gates Foundation) and James Platts-Mills (University of Virginia). Research reported in this publication was supported by the University of Florida Clinical and Translational Science Institute, which was supported in part by the NIH National Center for Advancing Translational Sciences under award number UL1TR001427. The content is solely the responsibility of the authors and does not necessarily represent the official views of the National Institutes of Health. The study would not have been possible without cooperation of study communities and local administration of the study kebeles. We would like to express our appreciation for the study households and all who supported the study directly or otherwise.
Supplementary Material
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fpubh.2020.615793/full#supplementary-material
References
1. Black RE, Victora CG, Walker SP, Bhutta ZA, Christian P, De Onis M, et al. Maternal and child undernutrition and overweight in low-income and middle-income countries. Lancet. (2013) 382:427–51. doi: 10.1016/S0140-6736(13)60937-X
2. Nahar B, Hossain M, Mahfuz M, Islam MM, Hossain MI, Murray-Kolb LE, et al. Early childhood development and stunting: findings from the MAL-ED birth cohort study in Bangladesh. Matern. Child Nutr. (2020) 16:e12864. doi: 10.1111/mcn.12864
3. Murray-Kolb LE, Acosta AM, De Burga RR, Chavez CB, Flores JT, Olotegui MP, et al. Early childhood cognitive development is affected by interactions among illness, diet, enteropathogens and the home environment: findings from the MAL-ED birth cohort study. BMJ Glob. Health. (2018) 23:e000752. doi: 10.1136/bmjgh-2018-000752
4. Iannotti LL, Lutter CK, Stewart CP, Riofrío CAG, Malo C, Reinhart G, et al. Eggs in early complementary feeding and child growth: a randomized controlled trial. Pediatrics. (2017) 140:e20163459. doi: 10.1542/peds.2016-3459
5. Alderman H. The economic cost of a poor start to life. J. Dev. Orig. Health Dis. (2010) 1:19–25. doi: 10.1017/S2040174409990158
6. von Grebmer K, Bernstein J, Hammond L, Patterson F, Sonntag A, Klaus L, et al. Global Hunger Index: Forced Migration and Hunger. Bonn: Welt Hunger Hilfe Concern Worldwide (2018).
7. Headey D, Nguyen P, Kim S, Rawat R, Ruel M, Menon P. Is exposure to animal feces harmful to child nutrition and health outcomes? a multicountry observational analysis. Am. J. Trop. Med. Hyg. (2017) 96:961–9. doi: 10.4269/ajtmh.16-0270
8. Neumann CG, Murphy SP, Gewa C, Grillenberger M, Bwibo NO. Meat supplementation improves growth, cognitive, and behavioral outcomes in Kenyan children. J. Nutr. (2007) 137:1119–23. doi: 10.1093/jn/137.4.1119
9. World Bank, The Food and Agriculture Organization of the United Nations (FAO), International Livestock Research Institute (ILRI), Interafrican Bureau for Animal Resources (AU-IBAR). Investing in African Livestock: Business Opportunities in 2030-2050 (2013).
10. Food and Agriculture Organization. Mapping Supply and Demand for Animal Source Foods in 2030. Animal Production and Health Working Paper 2. (2011). Available online at: http://www.fao.org/3/i2425e/i2425e00.htm (accessed October 02, 2020).
11. Shapiro B, Gebru G, Desta S, Negassa S, Nigussie K, Aboset G Others. Ethiopia Livestock Master Plan, Roadmap for Growth and Transformation. (2015). Available online at: https://cgspace.cgiar.org/bitstream/handle/10568/68037/lmp_roadmaps.pdf?sequence=1 (accessed October 02, 2020).
12. Kaur M, Graham JP, Eisenberg JNS. Livestock ownership among rural households and child morbidity and mortality: an analysis of demographic health survey data from 30 sub-Saharan African countries (2005-2015). Am. J. Trop. Med. Hyg. (2017) 96:741–8. doi: 10.4269/ajtmh.16-0664
13. Bardosh KL, Hussein JW, Sadik EA, Hassen JY, Ketema M, Ibrahim AM, et al. Chicken eggs, childhood stunting and environmental hygiene: an ethnographic study from the Campylobacter genomics and environmental enteric dysfunction (CAGED) project in Ethiopia. One Health Outlook. (2020) 2:5. doi: 10.1186/s42522-020-00012-9
14. Owino V, Ahmed T, Freemark M, Kelly P, Loy A, Manary M, et al. Environmental enteric dysfunction and growth failure/stunting in global child health. Pediatrics. (2016) 138:e20160641. doi: 10.1542/peds.2016-0641
15. Amour C, Gratz J, Mduma E, Svensen E, Rogawski ET, McGrath M, et al. Epidemiology and Impact of Campylobacter infection in children in 8 low-resource settings: results from the MAL-ED study. Clin. Infect. Dis. (2016) 63:1171–9. doi: 10.1093/cid/ciw542
16. Headey D, Hirvonen K. Is exposure to poultry harmful to child nutrition? An observational analysis for rural Ethiopia. PLoS ONE. (2016) 11:e0160590. doi: 10.1371/journal.pone.0160590
17. Rogawski ET, Liu J, Platts-Mills JA, Kabir F, Lertsethtakarn P, Siguas M, et al. Use of quantitative molecular diagnostic methods to investigate the effect of enteropathogen infections on linear growth in children in low-resource settings: longitudinal analysis of results from the MAL-ED cohort study. Lancet Glob. Health. (2018) 6:e1319–28. doi: 10.1016/S2214-109X(18)30351-6
18. Newell DG. The ecology of Campylobacter jejuni in avian and human hosts and in the environment. Int. J. Infect. Dis. (2002) 6:S16–21. doi: 10.1016/S1201-9712(02)90179-7
19. Jones FR, Baqar S, Gozalo A, Nunez G, Espinoza N, Reyes SM, et al. New world monkey Aotus nancymae as a model for Campylobacter jejuni infection and immunity. Infect. Immun. (2006) 74:790–3. doi: 10.1128/IAI.74.1.790-793.2006
20. Mølbak K, Havelaar A. Burden of illness of campylobacteriosis and sequelae. In: Nachamkin I, Szymanski, CM, Blaser MJ, editors. Campylobacter. 3rd ed. Washington, DC: American Society of Microbiology (2014). p. 3151–162. doi: 10.1128/9781555815554.ch8
21. Lee G, Pan W, Penataro Yori P, Paredes Olortegui M, Tilley D, Gregory M, et al. Symptomatic and asymptomatic Campylobacter infections associated with reduced growth in Peruvian children. PLoS Negl. Trop. Dis. (2013) 7:e2036. doi: 10.1371/journal.pntd.0002036
22. Havelaar AH, Kirk MD, Torgerson PR, Gibb HJ, Hald T, Lake RJ, et al. World Health Organization global estimates and regional comparisons of the burden of foodborne disease in 2010. PLoS Med. (2015) 12:e1001923. doi: 10.1371/journal.pmed.1001923
23. Bian X, Garber JM, Cooper KK, Huynh S, Jones J, Mills MK, et al. Campylobacter abundance in breastfed infants and identification of a new species in the global enterics multicenter study. mSphere. (2020) 5. doi: 10.1128/mSphere.00735-19
24. Giallourou N, Medlock GL, Bolick DT, Medeiros PH, Ledwaba SE, Kolling GL, et al. A novel mouse model of Campylobacter jejuni enteropathy and diarrhea. PLoS Pathog. (2018) 14:e1007083. doi: 10.1371/journal.ppat.1007083
25. Terefe Y, Deblais L, Ghanem M, Helmy YA, Mummed B, Chen D, et al. Co-occurrence of Campylobacter species in children from eastern Ethiopia, and their association with environmental enteric dysfunction, diarrhea, and host microbiome. Front. Public Health. (2020) 8:99. doi: 10.3389/fpubh.2020.00099
26. Assefa N, Oljira L, Baraki N, Demena M, Zelalem D, Ashenafi W, et al. HDSS profile: the Kersa health and demographic surveillance system. Int. J. Epidemiol. (2016) 45:94–101. doi: 10.1093/ije/dyv284
27. Harris PA, Taylor R, Thielke R, Payne J, Gonzalez N, Conde JG. Research electronic data capture (REDCap)–a metadata-driven methodology and workflow process for providing translational research informatics support. J. Biomed. Inf. (2009) 42:377–81. doi: 10.1016/j.jbi.2008.08.010
28. Faubion WA, Camilleri M, Murray JA, Kelly P, Amadi B, Kosek MN, et al. Improving the detection of environmental enteric dysfunction: a lactulose, rhamnose assay of intestinal permeability in children aged under 5 years exposed to poor sanitation and hygiene. BMJ Glob. Health. (2016) 1:e000066. doi: 10.1136/bmjgh-2016-000066
29. Weisz AJ, Manary MJ, Stephenson K, Agapova S, Manary FG, Thakwalakwa C, et al. Abnormal gut integrity is associated with reduced linear growth in rural malawian children. J. Pediatr. Gastroenterol. Nutr. (2012) 55:747–50. doi: 10.1097/MPG.0b013e3182650a4d
30. Trehan I, Shulman RJ, Ou CN, Maleta K, Manary MJ. A randomized, double-blind, placebo-controlled trial of rifaximin, a nonabsorbable antibiotic, in the treatment of tropical enteropathy. Am. J. Gastroenterol. (2009) 104:2326–33. doi: 10.1038/ajg.2009.270
31. Ordiz MI, Davitt C, Stephenson K, Agapova S, Divala O, Shaikh N, et al. EB 2017 article: interpretation of the lactulose: mannitol test in rural Malawian children at risk for perturbations in intestinal permeability. Exp. Biol. Med. (2018) 243:677–83. doi: 10.1177/1535370218768508
32. Kosek M, Haque R, Lima A, Babji S, Shrestha S, Qureshi S, et al. Fecal markers of intestinal inflammation and permeability associated with the subsequent acquisition of linear growth deficits in infants. Am. J. Trop. Med. Hyg. (2013) 88:390–6. doi: 10.4269/ajtmh.2012.12-0549
33. Agapova SE, Stephenson KB, Divala O, Kaimila Y, Maleta KM, Thakwalakwa C, et al. Additional common bean in the diet of malawian children does not affect linear growth, but reduces intestinal permeability. J. Nutr. (2018) 148:267–74. doi: 10.1093/jn/nxx013
34. World Health Organization. Standard Treatment Guidelines for Primary Hospitals, Ethiopia. 3rd ed. Jeneva: World Health Organization (WHO) (2014). Available online at: http://www.fmhaca.gov.et/wp-content/uploads/2019/03/STG-Primary-Hospital.pdf (accessed October 02, 2020).
36. World Health Organization. Progress on Drinking Water, Sanitation and Hygiene: 2017 Update and SDG Baselines (2017).
37. Jahnke HE. Livestock Production Systems and Livestock Development in Tropical Africa. (1982). Available online at: https://pdf.usaid.gov/pdf_docs/pnaan484.pdf (accessed October 02, 2020).
38. Hosmer Jr DW, Lemeshow S, Sturdivant RX. Applied Logistic Regression. New York, NY: John Wiley & Sons (2013). doi: 10.1002/9781118548387
39. Concern Worldwide Welthungerhilfe. 2019 Global Hunger Index (Ethiopia). (2019). Available online at: https://www.globalhungerindex.org/ethiopia.html (accessed October 02, 2020).
40. Budge S, Barnett M, Hutchings P, Parker A, Tyrrel S, Hassard F, et al. Risk factors and transmission pathways associated with infant Campylobacter spp. prevalence and malnutrition: a formative study in rural Ethiopia. PLoS ONE. (2020) 15:e0232541. doi: 10.1371/journal.pone.0232541
41. Cardemil CV., Sherchand JB, Shrestha L, Sharma A, Gary HE, Estivariz CF, et al. Pathogen-specific burden of outpatient diarrhea in infants in Nepal: a multisite prospective case-control study. J. Pediatric Infect Dis. Soc. (2017) 6:e75–85. doi: 10.1093/jpids/pix009
42. Platts-Mills JA, Babji S, Bodhidatta L, Gratz J, Haque R, Havt A, et al. Pathogen-specific burdens of community diarrhoea in developing countries: a multisite birth cohort study (MAL-ED). Lancet Glob. Health. (2015) 3:e564–75. doi: 10.1016/S2214-109X(15)00151-5
43. Jaime AL, Joan S, Lee B, Nancy S, Sydney MH, Eleanor L, et al. Campylobacter upsaliensis: another pathogen for consideration in the United States. Clin. Infect Dis. (2002) 34:e59–e60. doi: 10.1086/340266
44. Wagenaar JA, van Bergen MA, Blaser MJ, Tauxe RV, Newell DG, van Putten JP. Campylobacter fetus infections in humans: exposure and disease. Clin. Infect Dis. (2014) 58:1579–86.doi: 10.1093/cid/ciu085
45. Edmonds P, Patton CM, Griffin PM, Barrett TJ, Schmid GP, Baker CN, et al. Campylobacter hyointestinalis. associated with human gastrointestinal disease in the United States. J. Clin. Microbiol. (1987) 25:685–91. doi: 10.1128/JCM.25.4.685-691.1987
46. Wilkinson DA, O'Donnell AJ, Akhter RN, Fayaz A, Mack HJ, Rogers LE, et al. Updating the genomic taxonomy and epidemiology of Campylobacter hyointestinalis. Sci. Rep. (2018) 8:2393. doi: 10.1038/s41598-018-20889-x
47. Miller WG, Yee E, Lopes BS, Chapman MH, Huynh S, Bono JL, Parker CT, et al. Comparative genomic analysis identifies a Campylobacter clade deficient in selenium metabolism. Genome Biol. Evol. (2017) 9:1843–58. doi: 10.1093/gbe/evx093
48. Le Doare K, Holder B, Bassett A, Pannaraj PS. Mother's milk: a purposeful contribution to the development of the infant microbiota and immunity. Front. Immunol. (2018) 9:361. doi: 10.3389/fimmu.2018.00361
49. Arndt MB, Richardson BA, Ahmed T, Mahfuz M, Haque R, John-Stewart GC, et al. Fecal markers of environmental enteropathy and subsequent growth in Bangladeshi children. Am. J. Trop. Med. Hyg. (2016) 95:694–701. doi: 10.4269/ajtmh.16-0098
50. Mengistie B, Berhane Y, Worku A. Prevalence of diarrhea and associated risk factors among children under-five years of age in Eastern Ethiopia: a cross-sectional study. Open J. Prev. Med. (2013) 3:446–53. doi: 10.4236/ojpm.2013.37060
51. Hashi A, Kumie A, Gasana J. Prevalence of diarrhoea and associated factors among under-five children in Jigjiga District, Somali Region, Eastern Ethiopia. Open J. Prev. Med. (2016) 6:233–46. doi: 10.4236/ojpm.2016.610022
52. Darapheak C, Takano T, Kizuki M, Nakamura K, Seino K. Consumption of animal source foods and dietary diversity reduce stunting in children in Cambodia. Int. Arch. Med. (2013) 6:29. doi: 10.1186/1755-7682-6-29
53. World Health Organization. Indicators for Assessing Infant and Young Child Feeding Practices: Part 2: Measurement. Jeneva: World Health Organization (WHO) (2010).
54. Hirvonen K, Taffesse AS, Worku Hassen I. Seasonality and household diets in Ethiopia. Publ. Health Nutr. (2016) 19:1723–30. doi: 10.1017/S1368980015003237
55. Roba KT, O'Connor TP, Belachew T, O'Brien NM. Variations between post- and pre-harvest seasons in stunting, wasting, and Infant and Young Child Feeding (IYCF) practices among children 6-23 months of age in lowland and midland agro-ecological zones of rural Ethiopia. Pan Afr. Med. J. (2016) 24:163. doi: 10.11604/pamj.2016.24.163.9387
56. Pickering AJ, Null C, Winch PJ, Mangwadu G, Arnold BF, Prendergast AJ, et al. The WASH benefits and SHINE trials: interpretation of WASH intervention effects on linear growth and diarrhoea. Lancet Glob. Health. (2019) 7:e1139–46. doi: 10.1016/S2214-109X(19)30268-2
57. Cumming O, Arnold BF, Ban R, Clasen T, Esteves Mills J, Freeman MC, et al. The implications of three major new trials for the effect of water, sanitation and hygiene on childhood diarrhea and stunting: a consensus statement. BMC Med. (2019) 17:173. doi: 10.1186/s12916-019-1410-x
58. Heidkamp RA, Ayoya MA, Teta IN, Stoltzfus RJ, Marhone JP. Complementary feeding practices and child growth outcomes in Haiti: an analysis of data from demographic and health surveys. Matern. Child Nutr. (2015) 11:815–28. doi: 10.1111/mcn.12090
59. Wang Y, Moe CL, Teunis PFM. Children are exposed to fecal contamination via multiple interconnected pathways: a network model for exposure assessment. Risk Anal. (2018) 38:2478–96. doi: 10.1111/risa.13146
Keywords: Campylobacter, environmental enteric dysfunction, undernutrition, cross-sectional study, Ethiopia, smallholder farming
Citation: Chen D, McKune SL, Singh N, Yousuf Hassen J, Gebreyes W, Manary MJ, Bardosh K, Yang Y, Diaz N, Mohammed A, Terefe Y, Roba KT, Ketema M, Ameha N, Assefa N, Rajashekara G, Deblais L, Ghanem M, Yimer G and Havelaar AH (2021) Campylobacter Colonization, Environmental Enteric Dysfunction, Stunting, and Associated Risk Factors Among Young Children in Rural Ethiopia: A Cross-Sectional Study From the Campylobacter Genomics and Environmental Enteric Dysfunction (CAGED) Project. Front. Public Health 8:615793. doi: 10.3389/fpubh.2020.615793
Received: 09 October 2020; Accepted: 17 December 2020;
Published: 21 January 2021.
Edited by:
Thandavarayan Ramamurthy, National Institute of Cholera and Enteric Diseases (ICMR), IndiaReviewed by:
Alison Parker, Cranfield University, United KingdomSucharit Basu Neogi, International Centre for Diarrhoeal Disease Research (ICDDR), Bangladesh
Copyright © 2021 Chen, McKune, Singh, Yousuf Hassen, Gebreyes, Manary, Bardosh, Yang, Diaz, Mohammed, Terefe, Roba, Ketema, Ameha, Assefa, Rajashekara, Deblais, Ghanem, Yimer and Havelaar. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Arie H. Havelaar, ariehavelaar@ufl.edu
†These authors have contributed equally to this work
‡Present address: Mostafa Ghanem, Department of Veterinary Medicine, University of Maryland, College Park, MD, United States