 Alexandre Vallée
Alexandre Vallée- Department of Epidemiology and Public Health, Foch Hospital, Suresnes, France
The COVID-19 pandemic showed major impacts, on societies worldwide, challenging healthcare systems, economies, and daily life of people. Geoepidemiology, an emerging field that combines geography and epidemiology, has played a vital role in understanding and combatting the spread of the virus. This interdisciplinary approach has provided insights into the spatial patterns, risk factors, and transmission dynamics of the COVID-19 pandemic at different scales, from local communities to global populations. Spatial patterns have revealed variations in incidence rates, with urban-rural divides and regional hotspots playing significant roles. Cross-border transmission has highlighted the importance of travel restrictions and coordinated public health responses. Risk factors such as age, underlying health conditions, socioeconomic factors, occupation, demographics, and behavior have influenced vulnerability and outcomes. Geoepidemiology has also provided insights into the transmissibility and spread of COVID-19, emphasizing the importance of asymptomatic and pre-symptomatic transmission, super-spreading events, and the impact of variants. Geoepidemiology should be vital in understanding and responding to evolving new viral challenges of this and future pandemics.
Introduction
The COVID-19 pandemic showed a profound impact on societies worldwide, challenging healthcare systems, economies, and daily life (1–3). To effectively understand and combat the spread of pandemic, a multidisciplinary approach that incorporates both epidemiology and geography required (4, 5). This emerging field, known as geoepidemiology, examines the spatial patterns, risk factors, and transmission dynamics of COVID-19, for example, at various scales, from local communities to global populations (6–9). Geoepidemiology combines the power of spatial analysis, data science, and public health to gain insights into how the virus spreads, clusters in specific regions, and affects different populations (10–13). By analyzing the geographic distribution of COVID-19 cases, researchers and public administrations can identify hotspots, understand the influence of environmental factors, and develop specific strategies for prevention and control the pandemic (14, 15).
This interdisciplinary approach has revealed valuable information about the transmissibility and spread of COVID-19 pandemic (16, 17). It has shed light on determinants, such as urban-rural divides, regional hotspots, cross-border transmission, disparities in healthcare access, neighborhood-level variations, seasonal influences, and the role of behavioral patterns in the spread of the virus (18–21). Moreover, studies have explored the impact of risk determinants such as age, underlying health conditions, socioeconomic factors, occupation, demographics, and behavior on the vulnerability and outcomes of individuals and communities (22, 23).
National and international open data have allowed researchers to generate comprehensive insights and inform evidence-based response strategies (24, 25). Lessons learned from successful interventions, as well as failures, have shaped the global response to the pandemic and provided valuable insights for future preparedness efforts (26).
In this context, the exploration of the geoepidemiology aspect of the COVID-19 pandemic allows public policies to enhance more effective strategies to mitigate transmission (27), protect vulnerable populations (28, 29), allocate resources efficiently (30), and ultimately reduce the impact of the COVID-19 pandemic on public health and societies worldwide. Thus, this review focused on the interest and applications of geoepidemiology analyses during the COVID-19 pandemic.
Search strategy
PubMed Medline database was used for the research, with only articles in English language, using the following terms: “COVID-19,” “geo-epidemiology” and “spatial epidemiology.” Articles included in this review were both, original research, review, viewpoint, and case reports. Literature was searched from inception to 2023.
Spatial patterns
Identification of hotspots and the implementation of targeted control measures to minimize the spread of the virus
Studies have revealed stark spatial variations in COVID-19 incidence and mortality rates (31, 32). Factors such as population density, urbanization (33, 34), and transportation networks have a major role in virus transmission (35, 36). Dense urban areas with high population mobility have often experienced higher infection rates (37, 38). Moreover, regional variations in healthcare infrastructure, socioeconomic conditions, and public health interventions contribute to varying outcomes (39, 40). One prominent spatial pattern observed in the geoepidemiology of COVID-19 pandemic is the contrast between urban and rural areas (41, 42). Urban centers, characterized by high population density, extensive transportation networks, and frequent social interactions, have often experienced higher infection rates compared to rural regions (42). The concentration of cases in urban areas can be attributed to factors such as increased population mobility, crowded living conditions, and higher levels of economic activity (43). COVID-19 pandemic has exhibited the tendency to cluster in specific geographic areas, giving rise to regional hotspots (44, 45). These hotspots can be influenced by several factors, such as international travel hubs, densely populated neighborhoods, and areas with a high prevalence of risk factors such as poverty or comorbidities (37, 46, 47). Thus, identified hotspots around the world remains major to allow authorities to allocate resources, to implement targeted interventions, and to enforce localized lockdown measures to contain the spread (48, 49).
Moreover, peri-urban areas became marginal and degraded with a high rate of criminality, unemployment and in general low level of development indexes (50). Recent investigation have shown that the lockdown's impact on livelihoods was more severe in peri-urban areas than in urban areas (51). This could be consistent with the consensus that the pandemic hit small businesses, daily-wage earners, and low-wage earners, leaving them with no jobs or reduced incomes (52).
Highlight the importance of travel restrictions and coordinated public health responses to prevent cross-border transmission
The spread of COVID-19 pandemic has also been influenced by cross-border transmission patterns (53, 54). Proximity to international borders, transportation routes, and global migration patterns have facilitated the introduction and dissemination of the virus across different regions (55). Spatial patterns in COVID-19 cases have revealed disparities in healthcare access (56). Regions with limited healthcare infrastructure, fewer healthcare professionals, and inadequate testing and treatment facilities have often experienced higher case burdens and poorer outcomes (57). These disparities can exacerbate the impact of the virus, particularly in marginalized communities and underserved areas (29, 58, 59). Within cities and towns, the distribution of COVID-19 cases has exhibited neighborhood-level variations (60). Socioeconomic factors, housing conditions, and access to healthcare services can vary significantly across different neighborhoods, leading to differential vulnerability and infection rates (61).
Risk factors
By analyzing the relationship between COVID-19 pandemic and various risk factors, geoepidemiology has provided valuable insights into the disease's dynamics (62, 63). Studies have shown that age, gender, and underlying health conditions significantly affect vulnerability to infection and disease severity (64, 65). Additionally, socioeconomic factors, such as poverty, overcrowding, and access to healthcare, have been identified as determinants of COVID-19 outcomes (66).
Age has emerged as a significant risk factor in the transmission and severity of COVID-19. Older individuals, particularly those over the age of 65, are more susceptible to severe illness and mortality (67). Age-related physiological changes weakened immune systems, and a higher prevalence of underlying health conditions contribute to increased vulnerability (67). This ensures targeted protection measures for older populations, including prioritized vaccination campaigns and enhanced healthcare support (68, 69).
Socioeconomic determinants have a crucial role in the determination of COVID-19 risk (70). Individuals from lower socioeconomic backgrounds, who may have limited access to healthcare, live in crowded housing, or have occupations that do not allow for remote work, face heightened exposure risks (71, 72). They may also have challenges in accessing testing, treatment, and adhering to preventive measures due to economic constraints.
Certain occupations, such as healthcare workers, frontline workers, and those in essential services, face an increased risk of exposure to COVID-19 due to close contact with infected individuals or the public (73, 74). Workplaces that involve enclosed spaces, limited ventilation, and crowded conditions, such as factories, meatpacking plants, and prisons, have been associated with outbreaks (75–77). Thus, recent studies have highlighted the importance of workplace safety measures, including personal protective equipment (PPE) (78), physical distancing, and regular testing, to mitigate transmission risks (79, 80).
Demographic determinants, such as gender and ethnicity, have been observed to influence COVID-19 outcomes (81, 82). Men have been found to be more susceptible to severe illness and higher mortality rates compared to women (83). Furthermore, certain ethnic and racial groups, including Black, Indigenous, and minority populations, have experienced higher infection rates and worse outcomes due to systemic health disparities, socioeconomic factors, and structural inequities (84).
Individual behaviors have significant roles in COVID-19 transmission (85, 86). Determinants such as adherence to preventive measures (mask-wearing, hand hygiene, physical distancing), participation in social gatherings, travel, and compliance with public health guidelines influence the risk of COVID-19 infection and transmission (87–89). This knowledge can inform targeted public health messaging, community engagement strategies, and interventions to promote safe behaviors.
The COVID-19 pandemic has had far-reaching effects on mental health, livelihoods, and food security, pushing many individuals and families into poverty (90, 91). As the pandemic unfolded, it brought about a surge in stress, anxiety, and depression among people worldwide. The uncertainty surrounding the virus, fear of infection, isolation due to lockdowns, and loss of loved ones have taken a toll on mental wellbeing (92).
At the same time, the pandemic led to widespread job losses, reduced work hours, and business closures, particularly in sectors heavily affected by restrictions and social distancing measures. Many people found themselves without income or faced significant reductions in earnings, making it challenging to meet basic needs and maintain their livelihoods (93).
As the economic situation worsened, food security became a major concern. Disruptions in supply chains, rising food prices, and limited access to food resources exacerbated existing vulnerabilities, especially among low-income and marginalized populations (93).
The combination of mental health challenges, economic hardships, and food insecurity has forced many individuals and families into poverty (94). People living on the brink of poverty before the pandemic found themselves pushed over the edge due to the loss of income and access to essential resources (95).
The impact has been particularly severe in developing countries and marginalized communities, where the social safety net may be inadequate to address the growing needs (96). Vulnerable populations have been disproportionately affected, as they lack job security, social protection, and access to healthcare (97). Thus, addressing the mental health implications of the pandemic is crucial to mitigating its impact on livelihoods and food security. Providing mental health support and resources can help individuals cope with stress and anxiety, enabling them to better navigate the challenges posed by the pandemic.
Transmissibility and spread
Geoepidemiological investigations have shed light on the transmission dynamics of COVID-19 pandemic, elucidating how the virus spreads within and between communities (98, 99). By examining patterns of mobility, social interactions, and travel, researchers have quantified the impact of human behavior on virus transmission (100, 101). Furthermore, the integration of geographic information systems (GIS) and mathematical modeling has facilitated the prediction of future outbreaks and the evaluation of the effectiveness of control measures (62, 102). These insights have been instrumental in guiding public health responses and policy decisions (5, 103).
COVID-19 pandemic can be transmitted by individuals who are either asymptomatic (showing no symptoms throughout the infection) or pre-symptomatic (infected but not yet showing symptoms) (104). This characteristic of the virus poses challenges in identifying and containing transmission chains. This type of research has highlighted the significance of widespread testing, contact tracing, and quarantine measures to control the spread, even among individuals who do not exhibit symptoms (105).
COVID-19 pandemic has exhibited a pattern of super-spreading events, where a small number of individuals infect a disproportionately large number of people (106, 107). These events typically occur in crowded settings, such as social gatherings, religious ceremonies, and mass gatherings, where close contact and inadequate preventive measures facilitate rapid transmission (108). Thus, underscoring the importance of avoiding large gatherings is major for implementing targeted interventions in high-risk settings.
Travel restrictions, quarantine measures, and testing protocols have been implemented to mitigate travel-related spread (109). Additionally, contact tracing of individuals with travel history has played a crucial role in identifying and containing clusters of cases (110).
The emergence and spread of SARS-CoV-2 variants have further influenced the transmissibility and spread of COVID-19 (111). Variants with increased transmissibility, such as the Alpha, Beta, Gamma, and Delta variants, have led to more rapid spread in certain regions (112). Recent studies have monitored the circulation and impact of these variants, highlighting the need for genomic surveillance, early detection, and adaptive public health strategies to address emerging viral evolution (113, 114).
The spatio-temporal tracking of changed COVID dynamics based on genomic analysis is a cutting-edge approach in understanding the evolving nature of the SARS-CoV-2 virus (115). By analyzing the genetic sequences of the virus collected from different regions and at different time points, scientists can identify genetic mutations and variations that occur over time (116). This allows them to track the spread and transmission patterns of specific viral lineages across geographic areas. Moreover, the identification of new variants and their prevalence in different regions helps to assess their potential impact on disease severity, transmissibility, and vaccine effectiveness (117). This valuable information aids public health authorities in tailoring targeted interventions, optimizing testing strategies, and guiding vaccination efforts to effectively control and respond to the changing dynamics of the COVID-19 pandemic. The spatio-temporal genomic analysis could become an indispensable tool in the global effort to combat the pandemic and mitigate its effects on communities worldwide (118, 119). Nevertheless, this type of analysis needs to access of open and comprehensive data (120).
Countries disparities, the specific case of African countries
During the initial stages of the pandemic, the number of COVID-19 cases in African countries closely correlated with the volume of international flights into the continent. South Africa and Egypt, with their busiest international airports, experienced the highest case numbers (121). Conversely, countries with limited business and tourism connections to other continents reported lower case numbers.
A significant contributing factor to the relatively lower-case numbers in Africa was the early closure of airports in many countries, particularly those with prior experience in managing epidemic infectious diseases such as Ebola, Tuberculosis, and Lassa fever (122). These nations-initiated disease surveillance and contact tracing at airports much earlier than many other countries, thereby limiting the introduction of COVID-19 cases into the continent. Consequently, the “seeding” of cases was restrained, leading to a delayed onset and slower growth of infections, effectively “flattening the curve” in many African countries (123).
Testing capacity played a crucial role in shaping the reported case numbers. The top testing countries, e.g., USA and Europe, globally conducted significantly higher numbers of RT-PCR tests compared to African nations (57, 124). Limited testing resources, high costs, and the scarcity of necessary equipment and trained personnel hampered extensive testing in Africa. As a result, many cases might have been missed, and some antibody testing suggested that a substantial portion of the population may have already contracted and recovered from the disease (57). Furthermore, the absence of widespread testing might have resulted in some deaths being erroneously attributed to other causes when they were, in fact, due to COVID-19.
The lower population density in Africa compared to other continents played a favorable role in slowing the spread of the virus (125). Rural and widely dispersed communities contributed to limiting the rapid transmission of the disease, as observed in USA (126).
The youthfulness of the African population was also a protective factor. With a less median age in Sub-Saharan Africa compared to Europe, younger individuals were four times less likely to acquire severe symptoms or fatalities from COVID-19 (127). Conversely, countries with slightly older populations, like Egypt and South Africa, had higher case numbers and greater case fatality rates, partially due to higher prevalence of comorbidities associated with severe illness and mortality (128).
Exposure to previous infections, including other coronaviruses and endemic diseases like malaria, tuberculosis, and HIV, may have conferred relative immunity, and contributed to milder COVID-19 presentations in Africa (129, 130). Countries with higher Human Development Index tended to have higher case numbers and worse outcomes, suggesting that healthcare development and access influenced the pandemic's impact in countries (131).
Global collaboration and lessons learned
Recently it has been highlighted the importance of global collaboration in responding to a pandemic (132, 133). Through the sharing of data, expertise, and best practices, researchers and policymakers have been able to develop a more comprehensive understanding of the COVID-19 pandemic (134). Moreover, investigations have shown the need for improved surveillance systems, data harmonization, and standardized reporting methods for effective global monitoring and response (135).
The complexity of the COVID-19 pandemic has underscored the need for multidisciplinary collaboration (136) (Table 1). Thus, geoepidemiology brings together experts from various fields, including epidemiology, geography, data science, and public health, to analyze spatial patterns, risk factors, and transmission dynamics (137). By integrating diverse perspectives and expertise, researchers have been able to generate comprehensive insights, develop innovative methodologies, and formulate evidence-based strategies to combat the pandemic.
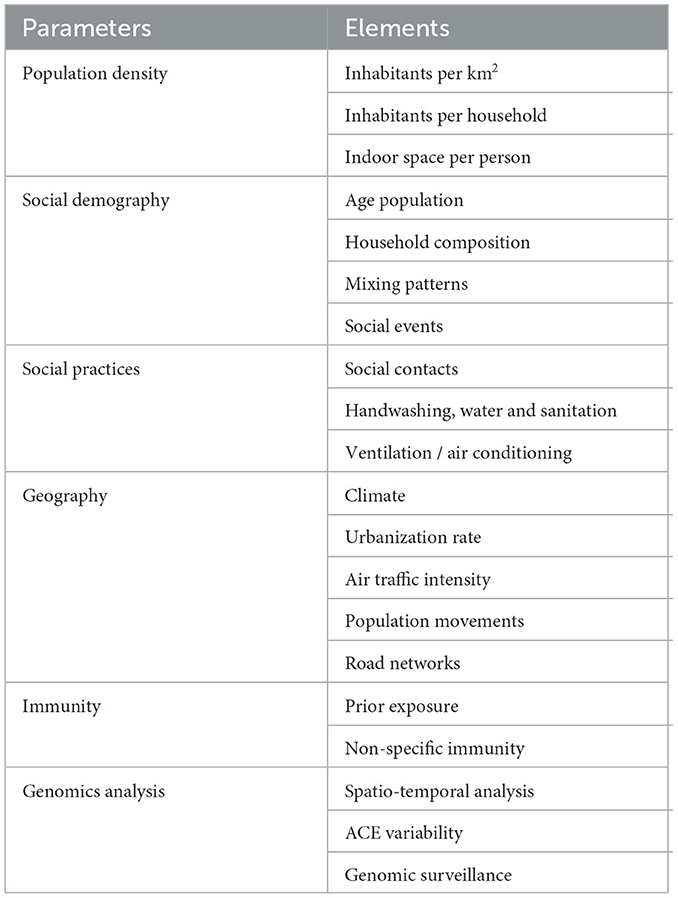
Table 1. Contextual parameters potentially influencing COVID-19 transmission.
The COVID-19 pandemic has emphasized the critical role of rapid information dissemination in effective response efforts (138). Studies have relied on real-time data sharing, open-access publications, and online platforms to disseminate findings promptly (139). Rapid dissemination of accurate information is crucial for guiding public health decision-making, enabling policymakers and healthcare professionals to implement evidence-based interventions, and fostering public trust and compliance with preventive measures (140, 141).
The development and distribution of vaccines against COVID-19 have shown the importance of global solidarity and equitable access (142). Global collaboration has emphasized the need for fair vaccine distribution, support for low-income countries, and collaborative efforts to ensure that no one is left behind in the global vaccination campaign (143).
Conclusion
In conclusion, this study can statute that geoepidemiology has provided invaluable insights into the global impact of the COVID-19 pandemic. By analyzing spatial patterns, risk factors, and transmission dynamics, this interdisciplinary field has contributed to the development of targeted interventions, efficient resource allocation, and informed decision-making. As the pandemic may continue to evolve, geoepidemiological research will have a major role in understanding and responding to these new emerging challenges. Moreover, geo-epidemiology cannot be a stand-alone field but should seek to work with other disciplines and fields in the delivery of its mandate and contribution to infectious disease epidemiology.
Author contributions
AV: conceptualization, formal analysis, and writing—original draft preparation.
Conflict of interest
The author declares that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher's note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
References
1. Sawicka B, Aslan I, Della Corte V, Periasamy A, Krishnamurthy SK, Mohammed A, et al. The coronavirus global pandemic and its impacts on society. Coronavirus Drug Discov. (2022) 4:267–311. doi: 10.1016/B978-0-323-85156-5.00037-7
2. Hiscott J, Alexandridi M, Muscolini M, Tassone E, Palermo E, Soultsioti M, et al. The global impact of the coronavirus pandemic. Cytok Growth Factor Rev. (2020) 53:1–9. doi: 10.1016/j.cytogfr.2020.05.010
3. Miyah Y, Benjelloun M, Lairini S, Lahrichi A. COVID-19 impact on public health, environment, human psychology, global socio economy, and education. Sci World J. (2022) 2022:5578284. doi: 10.1155/2022/5578284
4. Parajuli RR, Mishra B, Banstola A, Ghimire BR, Poudel S, Sharma K, et al. Multidisciplinary approach to COVID-19 risk communication: a framework and tool for individual and regional risk assessment. Sci Rep. (2020) 10:21650. doi: 10.1038/s41598-020-78779-0
5. Smith CD, Mennis J. Incorporating geographic information science and technology in response to the COVID-19 pandemic. Prev Chronic Dis. (2020) 17:E58. doi: 10.5888/pcd17.200246
6. Andersen LM, Harden SR, Sugg MM, Runkle JD, Lundquist TE. Analyzing the spatial determinants of local COVID-19 transmission in the United States. Sci Total Environ. (2021) 754:142396. doi: 10.1016/j.scitotenv.2020.142396
7. Gu L, Yang L, Wang L, Guo Y, Wei B, Li H. Understanding the spatial diffusion dynamics of the COVID-19 pandemic in the city system in China. Soc Sci Med. (2022) 302:114988. doi: 10.1016/j.socscimed.2022.114988
8. Vallée A. Geo-epidemiological approach of the COVID-19 pandemic in France and in Europe for public health policies. J Pub Health Policy. (2023) 44:255–63. doi: 10.1057/s41271-023-00402-z
9. Vallée A. Heterogeneity of the COVID-19 pandemic in the United States of America: a geo-epidemiological perspective. Front Public Health. (2022) 10:818989. doi: 10.3389/fpubh.2022.818989
10. Moroni L, Bianchi I, Lleo A. Geoepidemiology, gender and autoimmune disease. Autoimmun Rev. (2012) 11:A386–392. doi: 10.1016/j.autrev.2011.11.012
11. Pellegrino P, Radice S, Clementi E. Geoepidemiology of acute disseminated encephalomyelitis. Epidemiol Camb Mass. (2014) 25:928–9. doi: 10.1097/EDE.0000000000000176
12. Landier J, Bassez L, Bendiane M-K, Chaud P, Franke F, Nauleau S, et al. Social deprivation and SARS-CoV-2 testing: a population-based analysis in a highly contrasted southern France region. Front Public Health. (2023) 11:1162711. doi: 10.3389/fpubh.2023.1162711
13. Marianelli C, Verrubbi V, Pruiti Ciarello F, Ippolito D, Pacciarini ML, Di Marco Lo Presti V. Geo-epidemiology of animal tuberculosis and Mycobacterium bovis genotypes in livestock in a small, high-incidence area in Sicily, Italy. Front Microbiol. (2023) 14:1107396. doi: 10.3389/fmicb.2023.1107396
14. Ahasan R, Alam MdS, Chakraborty T, Hossain MdM. Applications of GIS and geospatial analyses in COVID-19 research: a systematic review. F1000Research. (2022) 9:1379. doi: 10.12688/f1000research.27544.2
15. Hass FS, Jokar Arsanjani J. The geography of the COVID-19 pandemic: a data-driven approach to exploring geographical driving forces. Int J Environ Res Public Health. (2021) 18:2803. doi: 10.3390/ijerph18062803
16. Bontempi E, Vergalli S, Squazzoni F. Understanding COVID-19 diffusion requires an interdisciplinary, multi-dimensional approach. Environ Res. (2020) 188:109814. doi: 10.1016/j.envres.2020.109814
17. Mol A, Hardon A. What COVID-19 may teach us about interdisciplinarity. BMJ Glob Health. (2020) 5:e004375. doi: 10.1136/bmjgh-2020-004375
18. Gupta D, Biswas D, Kabiraj P. COVID-19 outbreak and urban dynamics: regional variations in India. GeoJournal. (2022) 87:2719–37. doi: 10.1007/s10708-021-10394-6
19. Callaghan T, Lueck JA, Trujillo KL, Ferdinand AO. Rural and urban differences in covid-19 prevention behaviors. J Rural Health. (2021) 37:287–95. doi: 10.1111/jrh.12556
20. Arsenault C, Gage A, Kim MK, Kapoor NR, Akweongo P, Amponsah F, et al. COVID-19 and resilience of healthcare systems in ten countries. Nat Med. (2022) 28:1314–24. doi: 10.1038/s41591-022-01750-1
21. Carrión D, Colicino E, Pedretti NF, Arfer KB, Rush J, DeFelice N, et al. Neighborhood-level disparities and subway utilization during the COVID-19 pandemic in New York City. Nat Commun. (2021) 12:3692. doi: 10.1038/s41467-021-24088-7
22. Abrams EM, Szefler SJ. COVID-19 and the impact of social determinants of health. Lancet Respir Med. (2020) 8:659–61. doi: 10.1016/S2213-2600(20)30234-4
23. Mena GE, Martinez PP, Mahmud AS, Marquet PA, Buckee CO, Santillana M. Socioeconomic status determines COVID-19 incidence and related mortality in Santiago, Chile. Science. (2021) 372:eabg5298. doi: 10.1126/science.abg5298
24. Huston P, Edge V, Bernier E. Reaping the benefits of Open Data in public health. Can Commun Dis Rep. (2019) 45:252–6. doi: 10.14745/ccdr.v45i10a01
25. Titler MG. The Evidence for Evidence-Based Practice Implementation. In: Hughes RG, editor. Patient Safety and Quality: An Evidence-Based Handbook for Nurses. Advances in Patient Safety. Rockville, MD: Agency for Healthcare Research and Quality (US) (2008).
26. Marcassoli A, Leonardi M, Passavanti M, De Angelis V, Bentivegna E, Martelletti P, et al. Lessons learned from the lessons learned in public health during the first years of COVID-19 pandemic. Int J Environ Res Pub Health. (2023) 20:1785. doi: 10.3390/ijerph20031785
27. Anderson RM, Heesterbeek H, Klinkenberg D, Hollingsworth TD. How will country-based mitigation measures influence the course of the COVID-19 epidemic? Lancet. (2020) 395:931–4. doi: 10.1016/S0140-6736(20)30567-5
28. Holmes EA, O'Connor RC, Perry VH, Tracey I, Wessely S, Arseneault L, et al. Multidisciplinary research priorities for the COVID-19 pandemic: a call for action for mental health science. Lancet Psychiatry. (2020) 7:547–60. doi: 10.1016/S2215-0366(20)30168-1
29. Zucman D, Rasnaama A, Majerholc C, Vallée A. The COVID-19 pandemic and the migrant population for HIV diagnosis and care follow-up: they are left behind. Healthc Basel Switz. (2022) 10:1607. doi: 10.3390/healthcare10091607
30. Yuk-Chiu Yip J. Healthcare resource allocation in the COVID-19 pandemic: Ethical considerations from the perspective of distributive justice within public health. Pub Health Pract. (2021) 2:100111. doi: 10.1016/j.puhip.2021.100111
31. Bossak BH, Turk CA. Spatial variability in COVID-19 mortality. Int J Environ Res Public Health. (2021) 18:5892. doi: 10.3390/ijerph18115892
32. Thomas LJ, Huang P, Yin F, Luo XI, Almquist ZW, Hipp JR, et al. Spatial heterogeneity can lead to substantial local variations in COVID-19 timing and severity. Proc Natl Acad Sci U S A. (2020) 117:24180–7. doi: 10.1073/pnas.2011656117
33. Yu D, Li X, Yu J, Shi X, Liu P, Tian P. Whether urbanization has intensified the spread of infectious diseases-renewed question by the COVID-19 pandemic. Front Public Health. (2021) 9:699710. doi: 10.3389/fpubh.2021.699710
34. Carozzi F, Provenzano S, Roth S. Urban density and COVID-19: understanding the US experience. Ann Reg Sci. (2022) 12:1–32. doi: 10.1007/s00168-022-01193-z
35. Lu J, Lin A, Jiang C, Zhang A, Yang Z. Influence of transportation network on transmission heterogeneity of COVID-19 in China. Transp Res Part C Emerg Technol. (2021) 129:103231. doi: 10.1016/j.trc.2021.103231
36. Silva GC, Ribeiro EMS. The impact of Brazil's transport network on the spread of COVID-19. Sci Rep. (2023) 13:2240. doi: 10.1038/s41598-022-27139-1
37. Khavarian-Garmsir AR, Sharifi A, Moradpour N. Are high-density districts more vulnerable to the COVID-19 pandemic? Sustain Cities Soc. (2021) 70:102911. doi: 10.1016/j.scs.2021.102911
38. Jo Y, Hong A, Sung H. Density or Connectivity: What Are the Main Causes of the Spatial Proliferation of COVID-19 in Korea? Int J Environ Res Public Health. (2021) 18:5084. doi: 10.3390/ijerph18105084
39. Strully K, Yang T-C, Liu H. Regional variation in COVID-19 disparities: connections with immigrant and Latinx communities in U.S. counties. Ann Epidemiol. (2021) 53:56–62. doi: 10.1016/j.annepidem.2020.08.016
40. Bollyky TJ, Castro E, Aravkin AY, Bhangdia K, Dalos J, Hulland EN, et al. Assessing COVID-19 pandemic policies and behaviours and their economic and educational trade-offs across US states from Jan 1, 2020, to July 31, 2022: an observational analysis. Lancet Lond Engl. (2023) 401:1341–60. doi: 10.1016/S0140-6736(23)00461-0
41. Monnat SM. Rural-Urban Variation in COVID-19 Experiences and Impacts among U.S. working-age adults. Ann Am Acad Pol Soc Sci. (2021) 698:111–36. doi: 10.1177/00027162211069717
42. Greteman BB, Garcia-Auguste CJ, Gryzlak BM, Kahl AR, Lutgendorf SK, Chrischilles EA, et al. Rural and urban differences in perceptions, behaviors, and healthcare disruptions during the COVID-19 pandemic. J Rural Health Off J Am Rural Health Assoc Natl Rural Health Care Assoc. (2022) 38:932–44. doi: 10.1111/jrh.12667
43. Yao Y, Liu L. Research on population mobility and sustainable economic growth from a communication perspective. Front Psychol. (2022) 13:935606. doi: 10.3389/fpsyg.2022.935606
44. Gohari K, Kazemnejad A, Sheidaei A, Hajari S. Clustering of countries according to the COVID-19 incidence and mortality rates. BMC Public Health. (2022) 22:632. doi: 10.1186/s12889-022-13086-z
45. Darques R, Trottier J, Gaudin R, Ait-Mouheb N. Clustering and mapping the first COVID-19 outbreak in France. BMC Public Health. (2022) 22:1279. doi: 10.1186/s12889-022-13537-7
46. Lak A, Sharifi A, Badr S, Zali A, Maher A, Mostafavi E, et al. Spatio-temporal patterns of the COVID-19 pandemic, and place-based influential factors at the neighborhood scale in Tehran. Sustain Cities Soc. (2021) 72:103034. doi: 10.1016/j.scs.2021.103034
47. Gurram MK, Wang MX, Wang Y-C, Pang J. Impact of urbanisation and environmental factors on spatial distribution of COVID-19 cases during the early phase of epidemic in Singapore. Sci Rep. (2022) 12:9758. doi: 10.1038/s41598-022-12941-8
48. Stobart A, Duckett S. Australia's response to COVID-19. Health Econ Policy Law. (2022) 17:95–106. doi: 10.1017/S1744133121000244
49. Emmanuel F, Hassan A, Ahmad A, Reza TE. Pakistan's COVID-19 Prevention and control response using the world health organization's guidelines for epidemic response interventions. Cureus. (2023) 15:e34480. doi: 10.7759/cureus.34480
50. Corsi S, Dell'Ovo M, Dezio C, Longo A, Oppio A. Beyond food: framing ecosystem services value in peri-urban farming in the post-COVID era with a multidimensional perspective the case of Cascina biblioteca in Milan (Italy). Cities. (2023) 137:104332. doi: 10.1016/j.cities.2023.104332
51. Padmaja R, Nedumaran S, Jyosthnaa P, Kavitha K, Abu Hatab A, Lagerkvist C-J. COVID-19 impact on household food security in urban and peri-urban areas of Hyderabad, India. Front Public Health. (2022) 10:814112. doi: 10.3389/fpubh.2022.814112
52. Sharma GD, Mahendru M. Lives or livelihood: insights from locked-down India due to COVID19. Soc Sci Humanit Open. (2020) 2:100036. doi: 10.1016/j.ssaho.2020.100036
53. Arora P, Mrig S, Goldust Y, Kroumpouzos G, Serap Karadag A, Rudnicka L, et al. New coronavirus (SARS-CoV-2) crossing borders beyond cities, nations, and continents: impact of international travel balk. Med J. (2021) 38:205–11. doi: 10.5152/balkanmedj.2021.21074
54. Xiang L, Ma S, Yu L, Wang W, Yin Z. Modeling the global dynamic contagion of COVID-19. Front Public Health. (2022) 9:809987. doi: 10.3389/fpubh.2021.809987
55. Findlater A, Bogoch II. Human mobility and the global spread of infectious diseases: a focus on air travel. Trends Parasitol. (2018) 34:772–83. doi: 10.1016/j.pt.2018.07.004
56. Garcia-Morata M, Gonzalez-Rubio J, Segura T, Najera A. Spatial analysis of COVID-19 hospitalised cases in an entire city: the risk of studying only lattice data. Sci Total Environ. (2022) 806:150521. doi: 10.1016/j.scitotenv.2021.150521
57. Vallée A. Underestimation of the number of COVID-19 cases, an epidemiological threat. Epidemiol Infect. (2022) 150:e191. doi: 10.1017/S0950268822001728
58. Kantamneni N. The impact of the COVID-19 pandemic on marginalized populations in the United States: a research agenda. J Vocat Behav. (2020) 119:103439. doi: 10.1016/j.jvb.2020.103439
59. Lopez L, Hart LH, Katz MH. Racial and ethnic health disparities related to COVID-19. JAMA. (2021) 325:719–20. doi: 10.1001/jama.2020.26443
60. Gu A, Shafeeq H, Chen T, Gadhoke P. Factors associated with COVID-19 infection, hospitalization and death in New York City neighborhoods. Innov Pharm. (2021) 12:3379. doi: 10.24926/iip.v12i3.3379
61. Mongin D, Cullati S, Kelly-Irving M, Rosselet M, Regard S, Courvoisier DS. Neighbourhood socio-economic vulnerability and access to COVID-19 healthcare during the first two waves of the pandemic in Geneva, Switzerland: a gender perspective. EClinicalMedicine. (2022) 46:101352. doi: 10.1016/j.eclinm.2022.101352
62. Arutkin M, Faranda D, Alberti T, Vallée A. Delayed epidemic peak caused by infection and recovery rate fluctuations. Chaos Woodbury N. (2021) 31:101107. doi: 10.1063/5.0067625
63. Vallée A, Faranda D, Arutkin M. COVID-19 epidemic peaks distribution in the United-States of America, from epidemiological modeling to public health policies. Sci Rep. (2023) 13:4996. doi: 10.1038/s41598-023-30014-2
64. Lecarpentier Y, Vallée A. The key role of the level of ACE2 gene expression in SARS-CoV-2 infection. Aging. (2021) 13:14552–6. doi: 10.18632/aging.203181
65. Favas C, Jarrett P, Ratnayake R, Watson OJ, Checchi F. Country differences in transmissibility, age distribution and case-fatality of SARS-CoV-2: a global ecological analysis. Int J Infect Dis IJID Off Publ Int Soc Infect Dis. (2022) 114:210–8. doi: 10.1016/j.ijid.2021.11.004
66. Green H, Fernandez R, MacPhail C. The social determinants of health and health outcomes among adults during the COVID-19 pandemic: a systematic review. Public Health Nurs Boston Mass. (2021) 38:942–52. doi: 10.1111/phn.12959
67. Chen Y, Klein SL, Garibaldi BT Li H, Wu C, Osevala NM Li T, Margolick JB, et al. Aging in COVID-19: vulnerability, immunity and intervention. Ageing Res Rev. (2021) 65:101205. doi: 10.1016/j.arr.2020.101205
68. Wouters OJ, Shadlen KC, Salcher-Konrad M, Pollard AJ, Larson HJ, Teerawattananon Y, et al. Challenges in ensuring global access to COVID-19 vaccines: production, affordability, allocation, and deployment. Lancet Lond Engl. (2021) 397:1023–34. doi: 10.1016/S0140-6736(21)00306-8
69. Williams V, Edem B, Calnan M, Otwombe K, Okeahalam C. Considerations for establishing successful coronavirus disease vaccination programs in Africa. Emerg Infect Dis. (2021) 27:2009–16. doi: 10.3201/eid2708.203870
70. Ehlert A. The socio-economic determinants of COVID-19: a spatial analysis of German county level data. Socioecon Plann Sci. (2021) 78:101083. doi: 10.1016/j.seps.2021.101083
71. Gama A, Alves J, Costa D, Laires PA, Soares P, Pedro AR, et al. Double jeopardy from the COVID-19 pandemic: risk of exposure and income loss in Portugal. Int J Equity Health. (2021) 20:231. doi: 10.1186/s12939-021-01569-1
72. Mishra V, Seyedzenouzi G, Almohtadi A, Chowdhury T, Khashkhusha A, Axiaq A, et al. Health inequalities during COVID-19 and their effects on morbidity and mortality. J Healthc Leadersh. (2021) 13:19–26. doi: 10.2147/JHL.S270175
73. St-Denis X. Sociodemographic determinants of occupational risks of exposure to COVID-19 in Canada. Can Rev Sociol. (2020) 57:399–452. doi: 10.1111/cars.12288
74. Hawkins D. Differential occupational risk for COVID-19 and other infection exposure according to race and ethnicity. Am J Ind Med. (2020) 63:817–20. doi: 10.1002/ajim.23145
75. Klein MD, Sciaudone M, Richardson D, Lacayo R, McClean CM, Kharabora O, et al. SARS-CoV-2 seroprevalence and risk factors among meat packing, produce processing, and farm workers. PLOS Glob Public Health. (2022) 2:e0000619. doi: 10.1371/journal.pgph.0000619
76. Zhao X, Liu S, Yin Y, Zhang T, Chen Q. Airborne transmission of COVID-19 virus in enclosed spaces: An overview of research methods. Indoor Air. (2022) 32:e13056. doi: 10.1111/ina.13056
77. Beaudry G, Zhong S, Whiting D, Javid B, Frater J, Fazel S. Managing outbreaks of highly contagious diseases in prisons: a systematic review. BMJ Glob Health. (2020) 5:e003201. doi: 10.1136/bmjgh-2020-003201
78. Battista RA, Ferraro M, Piccioni LO, Malzanni GE, Bussi M. Personal protective equipment (PPE) in COVID 19 pandemic. J Occup Environ Med. (2021) 63:e80–5. doi: 10.1097/JOM.0000000000002100
79. Kucharski AJ, Klepac P, Conlan AJK, Kissler SM, Tang ML, Fry H, et al. CMMID COVID-19 working group. Effectiveness of isolation, testing, contact tracing, and physical distancing on reducing transmission of SARS-CoV-2 in different settings: a mathematical modelling study. Lancet Infect Dis. (2020) 20:1151–60. doi: 10.1016/S1473-3099(20)30457-6
80. Talic S, Shah S, Wild H, Gasevic D, Maharaj A. Effectiveness of public health measures in reducing the incidence of COVID-19, SARS-CoV-2 transmission, and COVID-19 mortality: systematic review and meta-analysis. BMJ. (2021) 375:n2997. doi: 10.1136/bmj.n2997
81. Pan D, Sze S, Minhas JS, Bangash MN, Pareek N, Divall P, et al. The impact of ethnicity on clinical outcomes in COVID-19: a systematic review. EClinicalMedicine. (2020) 23:100404. doi: 10.1016/j.eclinm.2020.100404
82. Kopel J, Perisetti A, Roghani A, Aziz M, Gajendran M, Goyal H. Racial and Gender-Based Differences in COVID-19. Front Public Health. (2020) 8:418. doi: 10.3389/fpubh.2020.00418
83. Jin J-M, Bai P, He W, Wu F, Liu X-F, Han D-M, et al. Gender differences in patients with COVID-19: focus on severity and mortality. Front Public Health. (2020) 8:152. doi: 10.3389/fpubh.2020.00152
84. Tai DBG, Sia IG, Doubeni CA, Wieland ML. Disproportionate impact of COVID-19 on racial and ethnic minority groups in the United States: a 2021 update. J Racial Ethn Health Disparities. (2022) 9:2334–9. doi: 10.1007/s40615-021-01170-w
85. West R, Michie S, Rubin GJ, Amlôt R. Applying principles of behaviour change to reduce SARS-CoV-2 transmission. Nat Hum Behav. (2020) 4:451–9. doi: 10.1038/s41562-020-0887-9
86. Agusto FB, Erovenko IV, Fulk A, Abu-Saymeh Q, Romero-Alvarez D, Ponce J, et al. To isolate or not to isolate: the impact of changing behavior on COVID-19 transmission. BMC Public Health. (2022) 22:138. doi: 10.1186/s12889-021-12275-6
87. Dzisi EKJ, Dei OA. Adherence to social distancing and wearing of masks within public transportation during the COVID 19 pandemic. Transp Res Interdiscip Perspect. (2020) 7:100191. doi: 10.1016/j.trip.2020.100191
88. Kale D, Herbec A, Beard E, Gold N, Shahab L. Patterns and predictors of adherence to health-protective measures during COVID-19 pandemic in the UK: cross-sectional and longitudinal findings from the HEBECO study. BMC Public Health. (2022) 22:2347. doi: 10.1186/s12889-022-14509-7
89. Shushtari ZJ, Salimi Y, Ahmadi S, Rajabi-Gilan N, Shirazikhah M, Biglarian A, et al. Social determinants of adherence to COVID-19 preventive guidelines: a comprehensive review. Osong Public Health Res Perspect. (2021) 12:346–60. doi: 10.24171/j.phrp.2021.0180
90. Bwala DG, Otekunrin OA, Adebowale OO, Fasina MM, Odetokun IA, Fasina FO. COVID-19 pandemic impacted food security and caused psychosocial stress in selected states of Nigeria. Int J Environ Res Public Health. (2023) 20:4016. doi: 10.3390/ijerph20054016
91. Kakaei H, Nourmoradi H, Bakhtiyari S, Jalilian M, Mirzaei A. Effect of COVID-19 on food security, hunger, and food crisis. COVID-19 Sustain Dev Goals. (2022) 4:3–29. doi: 10.1016/B978-0-323-91307-2.00005-5
92. Singh S, Roy D, Sinha K, Parveen S, Sharma G, Joshi G. Impact of COVID-19 and lockdown on mental health of children and adolescents: a narrative review with recommendations. Psychiatry Res. (2020) 293:113429. doi: 10.1016/j.psychres.2020.113429
93. Workie E, Mackolil J, Nyika J, Ramadas S. Deciphering the impact of COVID-19 pandemic on food security, agriculture, and livelihoods: a review of the evidence from developing countries. Curr Res Environ Sustain. (2020) 2:100014. doi: 10.1016/j.crsust.2020.100014
94. Wolfson JA, Garcia T, Leung CW. Food insecurity is associated with depression, anxiety, and stress: evidence from the early days of the COVID-19 pandemic in the United States. Health Equity. (2021) 5:64–71. doi: 10.1089/heq.2020.0059
95. Ibn-Mohammed T, Mustapha KB, Godsell J, Adamu Z, Babatunde KA, Akintade DD, et al. A critical analysis of the impacts of COVID-19 on the global economy and ecosystems and opportunities for circular economy strategies. Resour Conserv Recycl. (2021) 164:105169. doi: 10.1016/j.resconrec.2020.105169
96. Rasul G, Nepal AK, Hussain A, Maharjan A, Joshi S, Lama A, et al. Socio-economic implications of COVID-19 pandemic in south Asia: emerging risks and growing challenges. Front Sociol. (2021) 6:629693. doi: 10.3389/fsoc.2021.629693
97. Barron GC, Laryea-Adjei G, Vike-Freiberga V, Abubakar I, Dakkak H, Devakumar D, et al. Safeguarding people living in vulnerable conditions in the COVID-19 era through universal health coverage and social protection. Lancet Public Health. (2022) 7:e86–92. doi: 10.1016/S2468-2667(21)00235-8
98. Fang Y, Nie Y, Penny M. Transmission dynamics of the COVID-19 outbreak and effectiveness of government interventions: a data-driven analysis. J Med Virol. (2020) 92:645–59. doi: 10.1002/jmv.25750
99. Brand SPC, Ojal J, Aziza R, Were V, Okiro EA, Kombe IK, et al. COVID-19 transmission dynamics underlying epidemic waves in Kenya. Science. (2021) 374:989–94. doi: 10.1126/science.abk0414
100. Boto-García D. Investigating the two-way relationship between mobility flows and COVID-19 cases. Econ Model. (2023) 118:106083. doi: 10.1016/j.econmod.2022.106083
101. Kellermann R, Sivizaca Conde D, Rößler D, Kliewer N, Dienel H-L. Mobility in pandemic times: Exploring changes and long-term effects of COVID-19 on urban mobility behavior. Transp Res Interdiscip Perspect. (2022) 15:100668. doi: 10.1016/j.trip.2022.100668
102. Wang P, Zheng X, Liu H. Simulation and forecasting models of COVID-19 taking into account spatio-temporal dynamic characteristics: a review. Front Public Health. (2022) 10:1033432. doi: 10.3389/fpubh.2022.1033432
103. Huang X, Zhang R, Li X, Dadashova B, Zhu L, Zhang K, et al. Health-based geographic information systems for mapping and risk modeling of infectious diseases and COVID-19 to support spatial decision-making. Adv Exp Med Biol. (2022) 1368:167–88. doi: 10.1007/978-981-16-8969-7_8
104. Subramanian R, He Q, Pascual M. Quantifying asymptomatic infection and transmission of COVID-19 in New York City using observed cases, serology, and testing capacity. Proc Natl Acad Sci U S A. (2021) 118:e2019716118. doi: 10.1073/pnas.2019716118
105. Bracis C, Burns E, Moore M, Swan D, Reeves DB, Schiffer JT, et al. Widespread testing, case isolation and contact tracing may allow safe school reopening with continued moderate physical distancing: a modeling analysis of King County, WA data. Infect Dis Model. (2020) 6:24–35. doi: 10.1016/j.idm.2020.11.003
106. Wang L, Didelot X, Yang J, Wong G, Shi Y, Liu W, et al. Inference of person-to-person transmission of COVID-19 reveals hidden super-spreading events during the early outbreak phase. Nat Commun. (2020) 11:5006. doi: 10.1038/s41467-020-18836-4
107. Deslandes A, Calba C, Mahdjoub S, Zhu-Soubise A, Mathey D, Ardoin A. Superspreading events of SARS-CoV-2 in Paris: a retrospective analysis of data from the first wave of COVID-19 in 2020. J Infect Public Health. (2021) 14:1733–8. doi: 10.1016/j.jiph.2021.10.001
108. Liu C, Huang J, Chen S, Wang D, Zhang L, Liu X, et al. The impact of crowd gatherings on the spread of COVID-19. Environ Res. (2022) 213:113604. doi: 10.1016/j.envres.2022.113604
109. Movsisyan A, Burns J, Biallas R, Coenen M, Geffert K, Horstick O, et al. Travel-related control measures to contain the COVID-19 pandemic: an evidence map. BMJ Open. (2021) 11:e041619. doi: 10.1136/bmjopen-2020-041619
110. Hossain AD, Jarolimova J, Elnaiem A, Huang CX, Richterman A, Ivers LC. Effectiveness of contact tracing in the control of infectious diseases: a systematic review. Lancet Public Health. (2022) 7:e259–73. doi: 10.1016/S2468-2667(22)00001-9
111. Yi H, Wang J, Wang J, Lu Y, Zhang Y, Peng R, et al. The emergence and spread of novel SARS-CoV-2 variants. Front Public Health. (2021) 9:696664. doi: 10.3389/fpubh.2021.696664
112. Alizon S, Haim-Boukobza S, Foulongne V, Verdurme L, Trombert-Paolantoni S, Lecorche E, et al. Rapid spread of the SARS-CoV-2 Delta variant in some French regions, June 2021. Eurosurveillance. (2021) 26:2100573. doi: 10.2807/1560-7917.ES.2021.26.28.2100573
113. Tosta S, Moreno K, Schuab G, Fonseca V, Segovia FMC, Kashima S, et al. Global SARS-CoV-2 genomic surveillance: what we have learned (so far). Infect Genet Evol. (2023) 108:105405. doi: 10.1016/j.meegid.2023.105405
114. Ramazzotti D, Maspero D, Angaroni F, Spinelli S, Antoniotti M, Piazza R, et al. Early detection and improved genomic surveillance of SARS-CoV-2 variants from deep sequencing data. iScience. (2022) 25:104487. doi: 10.1016/j.isci.2022.104487
115. Wang P, Liu H, Zheng X, Ma R. A new method for spatio-temporal transmission prediction of COVID-19. Chaos Solitons Fractals. (2023) 167:112996. doi: 10.1016/j.chaos.2022.112996
116. Almubaid Z, Al-Mubaid H. Analysis and comparison of genetic variants and mutations of the novel coronavirus SARS-CoV-2. Gene Rep. (2021) 23:101064. doi: 10.1016/j.genrep.2021.101064
117. Singh H, Dahiya N, Yadav M, Sehrawat N. Emergence of SARS-CoV-2 new variants and their clinical significance. Can J Infect Dis Med Microbiol J Can Mal Infect Microbiol Médicale. (2022) 2022:7336309.
118. da Silva CC, de Lima CL, da Silva ACG, Silva EL, Marques GS, de Araújo LJB, et al. COVID-19 dynamic monitoring and real-time spatio-temporal forecasting. Front Public Health. (2021) 9:641253. doi: 10.3389/fpubh.2021.641253
119. Bollen N, Artesi M, Durkin K, Hong SL, Potter B, Boujemla B, et al. Exploiting genomic surveillance to map the spatio-temporal dispersal of SARS-CoV-2 spike mutations in Belgium across 2020. Sci Rep. (2021) 11:18580. doi: 10.1038/s41598-021-97667-9
120. Hamdi A, Shaban K, Erradi A, Mohamed A, Rumi SK, Salim F. Spatiotemporal data mining: a survey on challenges and open problems. Artif Int Rev. (2022) 55:1441–88. doi: 10.1007/s10462-021-09994-y
121. Bamgboye EL, Omiye JA, Afolaranmi OJ, Davids MR, Tannor EK, Wadee S, et al. COVID-19 pandemic: is Africa different? J Natl Med Assoc. (2021) 113:324–35. doi: 10.1016/j.jnma.2020.10.001
122. Wamai RG, Hirsch JL, Van Damme W, Alnwick D, Bailey RC, Hodgins S, et al. What could explain the lower COVID-19 burden in Africa despite considerable circulation of the SARS-CoV-2 virus? Int J Environ Res Public Health. (2021) 18:8638. doi: 10.3390/ijerph18168638
123. Tang JW, Caniza MA, Dinn M, Dwyer DE, Heraud J-M, Jennings LC, et al. An exploration of the political, social, economic and cultural factors affecting how different global regions initially reacted to the COVID-19 pandemic. Interf Focus. (2022) 12:20210079. doi: 10.1098/rsfs.2021.0079
124. Mboussou F, Impouma B, Farham B, Wolfe CM, Williams GS, Ngom R, et al. Analysing the reported incidence of COVID-19 and factors associated in the world health organization African region as of 31 December 2020. Epidemiol Infect. (2021) 149:e256. doi: 10.1017/S095026882100193X
125. Tcheutchoua DN, Tankeu AT, Angong DLW, Agoons BB, Nguemnang NYY, Djeunga HCN, et al. Unexpected low burden of coronavirus disease 2019 (COVID-19) in sub-Saharan Africa region despite disastrous predictions: reasons and perspectives. Pan Afr Med J. (2020) 37:352. doi: 10.11604/pamj.2020.37.352.25254
126. Schuchat A. Public health response to the initiation and spread of pandemic COVID-19 in the United States, February 24–April 21, 2020. MMWR Morb Mortal Wkly Rep. (2020) 69: e2. doi: 10.15585/mmwr.mm6918e2
127. Impouma B, Carr ALJ, Spina A, Mboussou F, Ogundiran O, Moussana F, et al. Time to death and risk factors associated with mortality among COVID-19 cases in countries within the WHO African region in the early stages of the COVID-19 pandemic. Epidemiol Infect. (2022) 12:1–29. doi: 10.1017/S095026882100251X
128. Njenga MK, Dawa J, Nanyingi M, Gachohi J, Ngere I, Letko M, et al. Why is there low morbidity and mortality of COVID-19 in Africa? Am J Trop Med Hyg. (2020) 103:564–9. doi: 10.4269/ajtmh.20-0474
129. Tso FY, Lidenge SJ, Peña PB, Clegg AA, Ngowi JR, Mwaiselage J, et al. High prevalence of pre-existing serological cross-reactivity against severe acute respiratory syndrome coronavirus-2 (SARS-CoV-2) in sub-Saharan Africa. Int J Infect Dis. (2021) 102:577–83. doi: 10.1016/j.ijid.2020.10.104
130. Osei SA, Biney RP, Anning AS, Nortey LN, Ghartey-Kwansah G. Low incidence of COVID-19 case severity and mortality in Africa: could malaria co-infection provide the missing link? BMC Infect Dis. (2022) 22:78. doi: 10.1186/s12879-022-07064-4
131. Heo M-H, Kwon YD, Cheon J, Kim K-B, Noh J-W. Association between the human development index and confirmed COVID-19 cases by country. Healthcare. (2022) 10:1417. doi: 10.3390/healthcare10081417
132. Kokudo N, Sugiyama H. Call for international cooperation and collaboration to effectively tackle the COVID-19 pandemic. Glob Health Med. (2020) 2:60–2. doi: 10.35772/ghm.2020.01019
133. Bernardo T, Sobkowich KE, Forrest RO, Stewart LS, D'Agostino M, Perez Gutierrez E, et al. Collaborating in the time of COVID-19: the scope and scale of innovative responses to a global pandemic. JMIR Public Health Surveill. (2021) 7:e25935. doi: 10.2196/25935
134. Dron L, Kalatharan V, Gupta A, Haggstrom J, Zariffa N, Morris AD, et al. Data capture and sharing in the COVID-19 pandemic: a cause for concern. Lancet Digit Health. (2022) 4:e748–56. doi: 10.1016/S2589-7500(22)00147-9
135. Kostkova P, Saigí-Rubió F, Eguia H, Borbolla D, Verschuuren M, Hamilton C, et al. Data and digital solutions to support surveillance strategies in the context of the COVID-19 pandemic. Front Digit Health. (2021) 3:707902. doi: 10.3389/fdgth.2021.707902
136. Montani D, Savale L, Beurnier A, Colle R, Noël N, Pham T, et al. Multidisciplinary approach for post-acute COVID-19 syndrome: time to break down the walls. Eur Respir J. (2021) 58:2101090. doi: 10.1183/13993003.01090-2021
137. Rezaeian M, Dunn G, St Leger S, Appleby L. Geographical epidemiology, spatial analysis and geographical information systems: a multidisciplinary glossary. J Epidemiol Commun Health. (2007) 61:98–102. doi: 10.1136/jech.2005.043117
138. Selerio E, Caladcad JA, Catamco MR, Capinpin EM, Ocampo L. Emergency preparedness during the COVID-19 pandemic: modelling the roles of social media with fuzzy DEMATEL and analytic network process. Socioecon Plann Sci. (2022) 82:101217. doi: 10.1016/j.seps.2021.101217
139. Brownson RC, Eyler AA, Harris JK, Moore JB, Tabak RG. Getting the word out: new approaches for disseminating public health science. J Public Health Manag Pract. (2018) 24:102–11. doi: 10.1097/PHH.0000000000000673
140. Chirico F, Teixeira da Silva JA. Evidence-based policies in public health to address COVID-19 vaccine hesitancy. Future Virol. (2023) 18:261–73 doi: 10.2217/fvl-2022-0028
141. Tricco AC, Langlois EV, Straus SE. Rapid Reviews to Strengthen Health Policy and Systems: A Practical Guide. Geneva: World Health Organization (2017).
142. Singh B, Chattu VK. Prioritizing “equity” in COVID-19 vaccine distribution through global health diplomacy. Health Promot Perspect. (2021) 11:281–7. doi: 10.34172/hpp.2021.36
Keywords: COVID-19, SARS-CoV-2, pandemic, geoepidemiology, epidemiology, public health, spatio-temporal epidemiology
Citation: Vallée A (2023) Geoepidemiological perspective on COVID-19 pandemic review, an insight into the global impact. Front. Public Health 11:1242891. doi: 10.3389/fpubh.2023.1242891
Received: 19 June 2023; Accepted: 02 October 2023;
Published: 19 October 2023.
Edited by:
Chiara de Waure, University of Perugia, ItalyReviewed by:
Umme Raihan Siddiqi, Shaheed Suhrawardy Medical College and Hospital, BangladeshFolorunso Oludayo Fasina, University of Pretoria, South Africa
Copyright © 2023 Vallée. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Alexandre Vallée, al.vallee@hopital-foch.com