 Laila Carolina Abu Esba
Laila Carolina Abu Esba Ghada Mardawi3,4
Ghada Mardawi3,4 Mohammad Al Deeb
Mohammad Al Deeb- 1King Abdulaziz Medical City, Ministry of National Guard, Health Affairs, Riyadh, Saudi Arabia
- 2King Saud Bin Abdulaziz University for Health Sciences, Riyadh, Saudi Arabia
- 3King Abdullah International Medical Research Centre, Riyadh, Saudi Arabia
- 4Pharmaceutical Care Services, King Abdulaziz Medical, Riyadh, Saudi Arabia
- 5Department of Emergency Medicine, Medical Toxicology division, King Abdulaziz Medical City, Riyadh, Saudi Arabia
- 6College of medicine, King Saud Bin Abdulaziz University for Health Sciences, King Abdullah International Medical Research Centre, Riyadh, Saudi Arabia
Background: In a series of cases that came to be recognized as a national methanol outbreak, an incident of delay in allocation and treatment with the antidote fomepizole is described with aim of sharing a learning experience.
Method: A team of 16 members was formed to conduct a Root Cause Analysis (RCA), which included multiple individual interviews with the stakeholders and inspection visits to the area.
Results: Root causes: The restocking process was unclear and inconsistent and specifically lacked a restocking policy for antidotes, inappropriate labeling and area design, and a sound-alike between fomepizole and omeprazole. Contributing factors included: unsuitable restocking practice and lack of training in using the pharmaceutical electronic inventory system. Corrective actions were recommended and implemented.
Conclusion: Management of antidotes in large healthcare systems requires a team effort to ensure appropriate and timely availability in emergency poisoning cases. This RCA identified important areas for improvement that could be insightful to other institutions in preventing similar vulnerabilities and is unique in describing the details of system improvements that can have a large impact on patient safety.
Background
Methanol toxicity is a serious poisoning that has high morbidity and mortality, which typically occurs in outbreaks in the community through ingestion of homemade or illegally produced alcoholic drinks. Despite that, the world health organization’s global report on health outcomes related to alcohol describes that methanol toxicity only accounted for less than 1% of all alcohol-attributable deaths (WHO, 2014). A study in the United States reported that the inpatient prevalence of methanol toxicity was 6.4 cases per 1,000,000 admissions. Nevertheless, these outbreaks are tragic events as methanol poisoning if not rapidly treated, causes retinal injury and eventually permanent blindness, as well as ischemic or hemorrhagic injury to the basal ganglia, renal failure, respiratory failure, and death (Kaewput et al., 2021).
In September 2020, we identified our first case of methanol toxicity which turned into a series of cases that came to be recognized as a national methanol outbreak, as other cases were reported at other hospitals. All these cases were linked to one source of poorly adulterated alcoholic beverages, distributed illegally. Familiarity with methanol toxicity is not common in our region. A retrospective review of methanol toxicity cases received over the past decade using data from our pharmacy showed that only 15 vials of fomepizole were dispensed over 10 years, with a zero consumption over the past 3 years ahead of this outbreak, compared to 95 vials utilized since the outbreak.
A literature search of methanol toxicity cases in Saudi Arabia (SA) revealed only four cases (Algahtani et al., 2018; Althwanay et al., 2020; Owolabi et al., 2020). However, Galvez-Ruiz et al. described outcomes of optic disk cupping following methanol poisoning in a series of 50 cases presenting at two large hospitals in Riyadh between 2008 and 2014, possibly indicating a higher incidence of methanol toxicity than perceived (Galvez-Ruiz et al., 2015). A recent study that used the United States National Inpatient Sample database reported 6.4 cases per 1,000,000 inpatient prevalence of methanol toxicity (Kaewput et al., 2021).
Insufficient stocking and availability of antidotes have been reported as a worldwide problem (Dart et al., 1996; Al-Sohaim et al., 2012; Gasco et al., 2013; Thanacoody et al., 2013). The Institute of Safe Medication Practice (ISMP-Canada) in a safety bulletin recognized the inaccessibility to antidotes and availability of information resources to guide timely use as main vulnerabilities in dealing with toxicity cases (Ismp-canada, 2018).
This paper aims to share a learning experience as we describe the incidence of delay in allocation and treatment with the antidote fomepizole in the first cases of methanol toxicity presented at our facility. We also describe the root cause analysis (RCA) of the incidence and the measures taken to ensure patient safety and prevent a recurrence.
No patient or case details are described in this paper, the aim is to share barriers to proper medication management of antidotes to promote patient safety.
Event summary
In 2020, around the beginning of the autumn season and just as COVID-19 lockdown and restrictions on gatherings were eased in SA, the first case in a series of cases of methanol toxicity presented to the emergency room (ER) during the weekend. With classic signs and symptoms of methanol toxicity including metabolic acidosis and changes in the level of consciousness. The diagnosis was confirmed with methanol blood levels. At this point, dialysis and intravenous (IV) fomepizole were ordered.
The order for fomepizole was entered in the computerized physician order entry (CPOE) as a STAT order, which was verified by the ER satellite pharmacy within 2 mins; however, no stocks of fomepizole were available in the ER satellite pharmacy. The pharmacy technician proceeded to check the pharmacy’s electronic inventory system, which indicated that stocks were available in the pharmacy warehouse. The technician called and paged the on-call pharmacist in charge of the pharmacy main store but no one answered.
The pharmacy technician also called the intensive care unit (ICU) satellite pharmacy in another attempt to locate stocks of fomepizole, as satellite pharmacy stocks are not linked to the electronic inventory system, and thus, stocks need to be checked manually. Over the phone, the pharmacist misheard fomepizole IV as omeprazole IV, which is not a formulary item at the hospital, and therefore, the pharmacist provided a negative response, replying that no stocks are available. The technician also contacted the IV room pharmacy but they also had no stock.
Five hours from the initial order the on-call pharmacist in charge of the pharmacy main store answered, but replied that no stocks are available in the pharmacy warehouse.
The patient was then transferred to the ICU where a new order for fomepizole was made. The ICU pharmacy technician was also unable to locate the stock of fomepizole, but a senior pharmacy technician was aware of its presence. The first dose of fomepizole was finally administered to the patient 6 hours after the initial order.
During that time, the pharmacy director and director of pharmaceutical planning who were off-duty were informed by hospital staff about the unavailability of fomepizole and began efforts in borrowing stocks from other hospitals. The director of pharmaceutical planning requested from one of his off-duty staff to physically check the pharmacy warehouse for stocks of fomepizole, which were available and delivered to the ICU-satellite pharmacy within 7 hours from the initial fomepizole order for the index case. Figure 1 outlines the pharmaceutical distribution process at our institution.
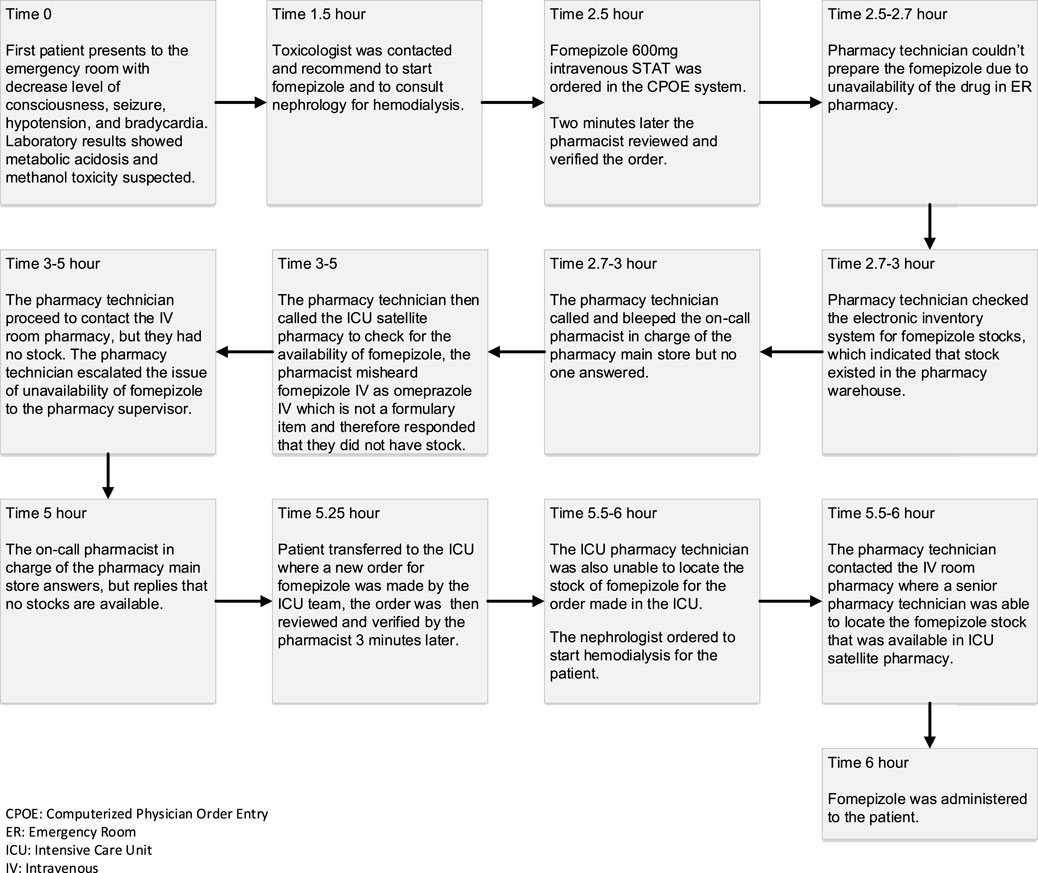
FIGURE 1. Timeline and sequence of the event.
The toxicologists overseeing the patient had also inquired the pharmacy about the availability of ethanol (an alternative antidote for methanol toxicity), which was unfortunately not listed as a formulary item and was only stocked in the narcotic pharmacy in small quantities for other uses, and pharmacy staff were not aware of its availability. Figure 2 outlines the timeline and sequence of the event.

FIGURE 2. Pharmaceutical Distribution Process at MNGHA.
Method
Setting: King Abdulaziz Medical City (KAMC) is a 1500-bed tertiary care hospital in Riyadh, Saudi Arabia, and is under the umbrella of the large integrated health system of the Ministry of National Guard Health Affairs, which includes six medical cities. The hospital has emergency services, specialized toxicology physicians, a drug and poison information center (DPIC) and its laboratory service is well equipped to perform all necessary toxicology testing.
The medication safety program is a well-established division of the quality and patient safety department at KAMC, and is responsible for monitoring and analyzing all reported medication adverse events, regularly conducts RCA and identifies areas for improvement, and recommends actions to prevent patient harm. All recommendations are discussed in a collective corporate meeting including all regional hospitals, and agreed-upon recommendations are implemented in all hospitals.
The root cause analysis process
The delay in allocation and treatment of patients presenting with methanol toxicity was discussed in our pharmacy and therapeutics committee and a memo was sent to our quality and patient safety department to officially conduct an RCA and respond to our committee with results for improvement and actions to be taken.
A team of 16 members was formed to conduct the RCA and included: medication safety officers (team leader), quality improvement specialists, ER consultant, a toxicologist, a nursing medication safety representative, the DPIC pharmacist, director of the pharmaceutical planning department, and the director of warehousing and distribution. In addition to the main RCA meeting, multiple individual interviews with the stakeholders and inspection visits to the area were conducted.
The institutional review board (IRB) at King Abdullah International Medical Research Center (KAIMRC) (Protocol NRC21R/520/12) approved this study. No consent form was required by the Ministry of National Guard Health Affairs ethics committee.
Results of the RCA
The event was deemed preventable by the task force evaluating the incidence. The family was disclosed about the event.
The RCA elucidated the fundamental error in this event to be the failure to locate the available stocks of fomepizole within the hospital by pharmacy staff, resulting in a 6-hours delay in the administration of the antidote. On further analysis, this error of medication administration delay was attributed to the following three root causes:
Root-causes identified
1) Distribution of Supplies Factors: Before the event occurred the ER satellite pharmacy requested stocks of fomepizole from the pharmacy warehouse; however, as the request was submitted on the last business day (i.e. before the weekend), the ER pharmacy was not re-supplied, which resulted in a zero stock over the weekend. The pharmacy main store did not stock all medications and fomepizole as a low-consumed drug was not stored. In addition, the pharmacy technician was unaware of the process of responding to zero stock issues and escalating it to the supervisors. The restocking process was unclear and inconsistent and specifically lacked a restocking policy for antidotes including fomepizole injection, with no clear guidance on communication with senior staff in an emergency situation.
2) Work Environment Factors: The allocated space for the ICU satellite pharmacy was small, with limited shelves and space, as a result, fomepizole as a drug rarely dispensed, was stored on a lower and not so visible shelf. It was also stored following no specific alphabetic or therapeutic class order (e.g., antidote shelf), which made it impossible for the junior staff to find, and only the senior pharmacy technician knew where it was stocked. Therefore, the ICU satellite pharmacy was unable to supply the ER satellite pharmacy with the available stocks. Hence, the root cause of this deviation was inappropriate area design.
3) Communication factors: The sound-alike between fomepizole and omeprazole led the ICU pharmacist to inform the ER pharmacy technician that fomepizole was not available in stock; this was a verbal miscommunication over the phone. The delay in response from the on-call pharmacist in the pharmacy main store and the misinformation about the availability of stocks in the pharmacy warehouse led the rest of the efforts to focus on borrowing from other hospitals, while stocks were available in the pharmacy warehouse.
Contributing factors
1) Distribution of Supplies Factors: The system of restocking implemented by pharmaceutical planning was based on the average monthly usage (AMU), which in cases of medications with unclear trends in consumption (i.e. no average monthly use) required a justification from the pharmacy technician to be approved for restocking. This led the first request sent from the ER satellite pharmacy for fomepizole stocks to be rejected, while the second request was approved just before the weekend but not executed. The contributing factor to this deviation was guidelines do not enable one to carry out the task promptly.
2) Education & Training: The lack of competency of pharmacy staff in using the pharmaceutical electronic inventory system resulted in incorrect information about stock availability.
Root‐cause analysis: Recommendations & improvements
After multiple meetings with the stakeholders and parties involved the RCA team agreed on a list of recommendations, and the team is continuously working on these recommendations and has been able to implement changes to improve patient safety. Table 1 summarizes these recommendations and improvements achieved. Table 2 lists the antidotes added to the formulary after the RCA.
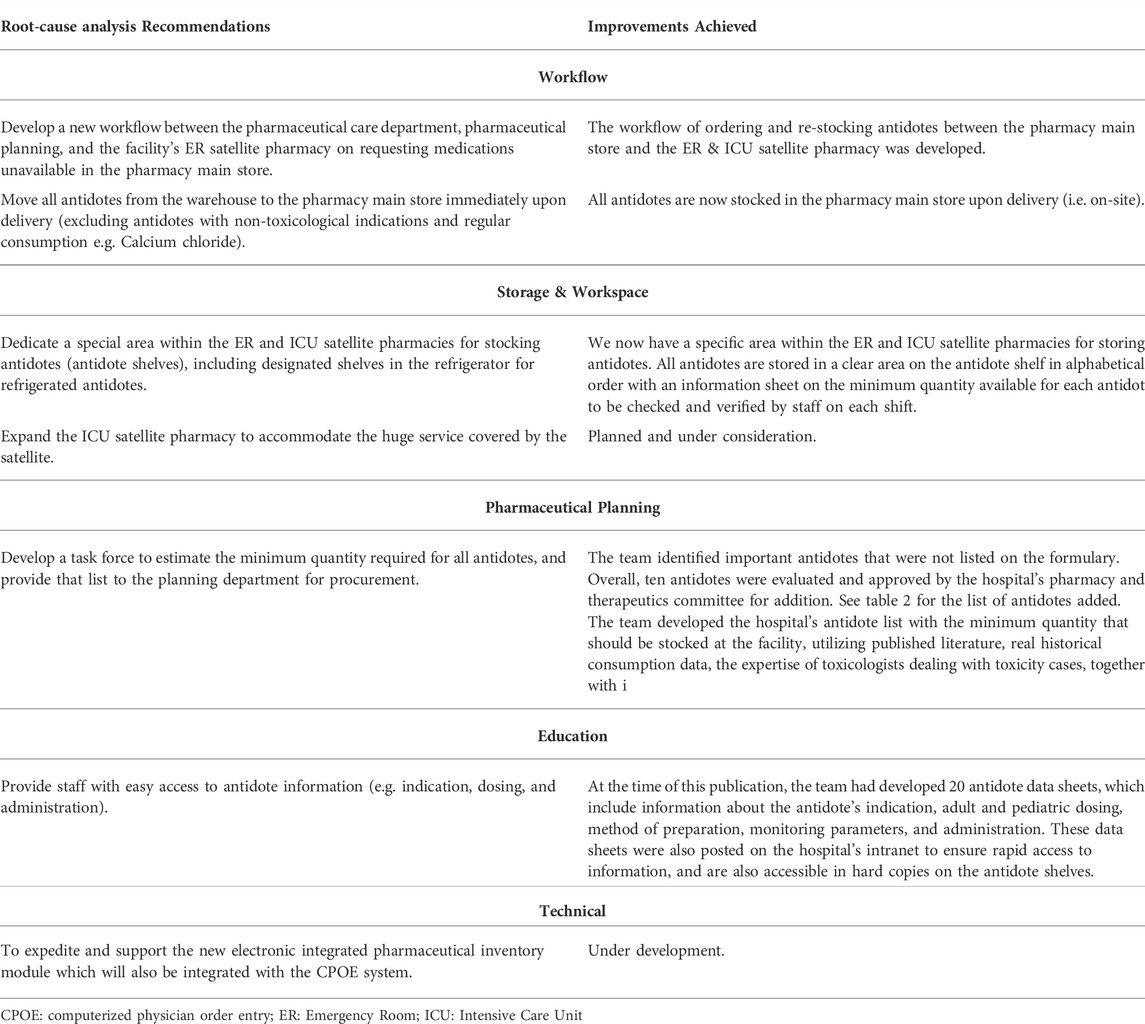
TABLE 1. Summary of the RCA Recommendations and Improvements Achieved.

TABLE 2. List of Antidotes on the Formulary before and after the RCA.
Discussion
Planning pharmaceutical inventory can be extremely challenging in such a dynamic setting of disease trends, drug discovery, and new clinical research, adding to these, the rarity of some indications and their therapeutic utilization makes it more challenging.
The outbreak of COVID-19 in 2020 and the shutdown of major pharmaceutical plants around the world added to the challenge of a well-planned secured drug supply in many healthcare settings (Abu Esba et al., 2020).
Poisoning cases vary in epidemiology and often lack good evidence on incidence, in addition to geographical differences in types and frequencies of occurrences. This makes local assessment and decisions on antidote stocking crucial (Azab et al., 2016; Sandilands and Bateman, 2016).
A national survey of antidote stocking in the United Kingdom revealed that atropine, calcium gluconate, and flumazenil were the only antidotes available in adequate stocks in all hospitals. They also reported that only (24.3%) of the hospitals held all antidotes that were recommended to be available immediately, which only improved to (47.9%) after auditing and introducing a national guideline. They concluded that more efforts are required to ensure timely access to other antidotes (Bailey et al., 2016).
This RCA triggered a holistic review of our antidote preparedness and identified areas of weakness in stocking and access that were important to be reassessed and modified to be prepared for any further poisoning cases presenting. Similar efforts have been shared by the Nova Scotia antidote program which demonstrated that adequate stocking is achievable through ongoing surveillance and maintenance by a multidisciplinary team (Murphy et al., 2019).
Pharmacists working in poison centers should be able to provide information on the appropriate use of antidotes including method of preparation, dosing, and monitoring in addition to advice on procurement and stocking of antidotes suitable to the size and area of their served community.
Cultural aspects and difference also unique to our setting was the unavailability of ethanol, which in other countries is readily available. Therefore, antidote stocking and planning should be tailored to address these differences.
Whatever the reasons for inadequate stocking of antidotes, be it cost, availability, infrequent use, or lack of awareness, institutions should make all efforts to regularly review and audit their antidote stocks.
Conclusion
Management of antidotes in large healthcare systems requires a team effort to ensure appropriate and timely availability in emergency poisoning cases. This RCA identified important areas for improvement that could be insightful to other institutions in preventing similar vulnerabilities. It provides details on operational level modifications that are needed to ensure safe access to antidotes when needed. The implemented measures require future analysis and assessment of their success in improving access to antidotes.
Author contributions
LA conceptualized this project and writing, GM led the RCA team, MD participated as an RCA member directly involved in the event, all three authors contributed in the RCA project and manuscript draft review and writing.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
References
Abu Esba, L. C., Al-Abdulkarim, H. A., Alrushidan, A., and Al Harbi, M. (2020). Pharmacy and therapeutics committee preparedness plan for COVID-19. Glob. J. Qual. Saf. Healthc. 3 (2), 55–64. doi:10.36401/JQSH-20-9
Al-Sohaim, S. I., Awang, R., Zyoud, S. H., Rashid, S. M., and Hashim, S. (2012). Evaluate the impact of hospital types on the availability of antidotes for the management of acute toxic exposures and poisonings in Malaysia. Hum. Exp. Toxicol. 31 (3), 274–281. doi:10.1177/0960327111405861
Algahtani, H., Shirah, B., Ahmad, R., Abobaker, H., and Hmoud, M. (2018). Transverse myelitis-like presentation of methanol intoxication: A case report and review of the literature. J. Spinal Cord. Med. 41 (1), 72–76. doi:10.1080/10790268.2016.1226005
Althwanay, A., Alharthi, M. M., Aljumaan, M., Almubarak, Y., and Alamri, A. (2020). Methanol, paracetamol toxicities and acute blindness. Cureus 12 (5), e8179. doi:10.7759/cureus.8179
Azab, S. M., Hirshon, J. M., Hayes, B. D., El-Setouhy, M., Smith, G. S., Tawfik, H., et al. (2016). Epidemiology of acute poisoning in children presenting to the poisoning treatment center at Ain Shams University in Cairo, Egypt, 2009-2013. Clin. Toxicol. 54 (1), 20–26. doi:10.3109/15563650.2015.1112014
Bailey, G. P., Rehman, B., Wind, K., Wood, D. M., Thanacoody, R., NaSh, S., et al. (2016). Taking stock: UK national antidote availability increasing, but further improvements are required. Eur. J. Hosp. Pharm. 23 (3), 145–150. doi:10.1136/ejhpharm-2015-000802
Dart, R. C., Stark, Y., Fulton, B., Koziol-McLain, J., and Lowenstein, S. R. (1996). Insufficient stocking of poisoning antidotes in hospital pharmacies. JAMA 276 (18), 1508–1510. doi:10.1001/jama.1996.03540180064034
Galvez-Ruiz, A., Elkhamary, S. M., Asghar, N., and Bosley, T. M. (2015). Cupping of the optic disk after methanol poisoning. Br. J. Ophthalmol. 99 (9), 1220–1223. doi:10.1136/bjophthalmol-2014-306354
Gasco, L., Rosbolt, M. B., and Bebarta, V. S. (2013). Insufficient stocking of cyanide antidotes in US hospitals that provide emergency care. J. Pharmacol. Pharmacother. 4 (2), 95–102. doi:10.4103/0976-500X.110875
Ismp-canada. Antidotes and related agents: Recognition of need, availability, and effective use. Available at: https://www.ismp-canada.org/download/safetyBulletins/2018/ISMPCSB2018-07-Antidotes.pdf. 2018. (Accessed April 22, 2022).
Kaewput, W., Thongprayoon, C., Petnak, T., Chewcharat, A., Boonpheng, B., Bathini, T., et al. (2021). Inpatient burden and mortality of methanol intoxication in the United States. Am. J. Med. Sci. 361 (1), 69–74. doi:10.1016/j.amjms.2020.08.014
Murphy, N. G., Bona, D. R., and Hurley, T. A. (2019). A system-wide solution to antidote stocking in emergency departments: The Nova Scotia antidote program. CJEM 21 (1), 37–46. doi:10.1017/cem.2017.400
Owolabi, L. F., Enwere, O. O., Ahmed Reda, A., Sayed Sayd, R. E., Elrazek, H., Adamu, B., et al. (2020). Methanol induced stroke: Report of cases occurring simultaneously in two biological brothers. J. Community Hosp. Intern. Med. Perspect. 10 (3), 265–268. doi:10.1080/20009666.2020.1766840
Sandilands, E., and Bateman, D. (2016). The epidemiology of poisoning. Med. Baltim. 44 (2), 76–79. doi:10.1016/j.mpmed.2015.11.015
Thanacoody, R. H., Aldridge, G., Laing, W., Dargan, P. I., Nash, S., Thompson, J. P., et al. (2013). National audit of antidote stocking in acute hospitals in the UK. Emerg. Med. J. 30 (5), 393–396. doi:10.1136/emermed-2012-201224
WHO. Global status report on alcohol and health 2014. Geneva, Switzerland: Who.int. Available at: https://www.who.int/publications-detail-redirect/global-status-report-on-alcohol-and-health-2014 2014. (Accessed June 1, 2022).
Keywords: antidotes, stocking, poisoning, methanol, fomepizol
Citation: Abu Esba LC, Mardawi G and Al Deeb M (2022) Can’t find the antidote: A root cause analysis. Front. Pharmacol. 13:895841. doi: 10.3389/fphar.2022.895841
Received: 14 March 2022; Accepted: 22 July 2022;
Published: 06 September 2022.
Edited by:
Kenneth McMartin, Ochsner LSU Health, United StatesReviewed by:
Jaroslav Pejchal, University of Defence, CzechiaOscar Medina-Contreras, Mexico Children’s Hospital, Mexico
Copyright © 2022 Abu Esba, Mardawi and Al Deeb. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Laila Carolina Abu Esba, abuesbala@ngha.med.sa