Parent Questionnaires in Screening for Developmental Language Disorder Among Bilingual Children in Speech and Language Clinics
 Hadar Abutbul-Oz
Hadar Abutbul-Oz Sharon Armon-Lotem
Sharon Armon-Lotem- 1Department of English Literature and Linguistic, Faculty of Humanities, Bar-Ilan University, Ramat Gan, Israel
- 2Gonda Multidisciplinary Brain Research Center, Bar-Ilan University, Ramat Gan, Israel
Screening for Developmental Language Disorder (DLD) among bilingual children in Speech and Language Clinics is challenged by the use of Societal Language (SL) monolingual norms and by the absence of knowledge about children’s performance in the Home Language (HL) leading to over diagnosis of DLD among bilingual children. The current study examined how bilingual parents’ questionnaire can contribute to a more accurate clinical protocol that can help mitigate the diagnosis difficulties and help disentangle the impact of bilingualism from DLD. Parents of 75 bilingual children (ages 48–82 months) participated in this study. Forty six children were referred to Speech and Language Pathologists (SLPs) due to language performance difficulties (Clinically Referred- CR) and 29 were never referred to a SLP (Non-referred- NR). Of the CR group only 19 were diagnosed by the SLP with DLD using dynamic assessment (CR-DLD), while 27 were diagnosed as having typical language development (CR-TLD). Parents of all children filled a Bilingual Parent Questionnaire (BIPAQ), developed from a SLP’s perspective, ith information in five domains: (a) Demographic Information, (b) Developmental background, (c) HL abilities, (d) SL abilities, and (e) Quantity and quality of exposure to both HL and SL. Significantly lower scores were observed for the CR-DLD group compared to the other groups on Developmental background, HL abilities, and SL abilities as well as on the total score. Sentence complexity, difference from other children in language development, and family history significantly distinguished between the CR-DLD and CR-TLD groups. Sentence complexity, difference from other children in language development, and confidence speaking freely distinguished between CR-DLD and NR children. No significant difference was observed between CR-TLD and NR children. A comparison of the CR- DLD and the CR-TLD bilinguals using a ROC curve analysis yielded good sensitivity and specificity, as well as good accuracy (AUC = 0.869). Our findings show that parent questionnaires can be a valuable part of diagnosis protocol and provide missing information needed for more accurate diagnosis before treatment commences, allowing clinicians alternative options of treatment as well as reducing caseloads at clinics.
Introduction
Difficulties or delays in the acquisition of the Societal Language (SL) lead to many referrals of bilingual children to Speech and Language Pathologists (SLPs). Yet, screening for Developmental Language Disorder (DLD) among bilingual children in Speech and Language Clinics is challenged by the use of SL monolingual norms and by the absence of knowledge on children’s performance in the Home Language (HL). Usage of SL monolingual norms to assess the linguistic performance of bilingual children can be misleading since their chronological age does not reflect the amount of exposure to SL Hebrew. The absence of standardized tests in the children’s home language (HL), and the limited availability of SLPs who know the different HLs, often make identification even more challenging, as assessment should be done in both languages. These caveats result in over diagnosis of Developmental Language Disorder (DLD) among bilingual children (see, for example, Armon-Lotem, 2010; Armon-Lotem et al., 2021 for Israel; Grimm and Schulz, 2014 for Germany; Paradis et al., 2010 for Canada and Scheidnes and Tuller, 2016 for France). The present study demonstrates how the use of a bilingual parent questionnaire yields differential profiles for bilingual children in the clinic and contributes to a more accurate clinical process that can help mitigate the diagnosis difficulties and disentangle the impact of bilingualism from DLD.
Diagnosing Developmental Language Disorder Among Bilingual Children
According to the Diagnostic and Statistical Manual of Mental Disorders, Fifth Edition (American Psychiatric Association, 2013), Language Impairment will be diagnosed when one experiences persistent difficulties in comprehension and expression of language, oral and/or written, in the absence of neurological, cognitive or conceptual factors such as hearing impairment or neurological damage. Language Impairment affects approximately 7% of the general population (Tomblin et al., 1997; Norbury et al., 2016). It is a neuro-developmental disorder with a hereditary component manifested mainly in morphology and syntax (Rice, 2004; Bishop, 2006; Rice et al., 2008; Leonard, 2014). Genetic aspects and family history predicted diagnosis in previous studies with different degrees of accuracy (Bishop et al., 1995, 2012; Leonard, 1998; Restrepo, 1998).
Bishop et al. (2017) introduced the term Developmental Language Disorder (DLD) following the CATALIZE consensus, a diagnostic label was embraced by international community referring to a language disorder unrelated to a biological condition and experienced in the course of language development. Subsequently, DLD could co-occur with other neurobiological disorders, environmental risk factors and does not require a gap between verbal and non-verbal IQ. For the remaining of this paper the term DLD will be used regardless of other terms previously mentioned to maintain a consistent and unified clarity.
Given that DLD is a neuro-developmental disorder (Leonard, 1998; Lee et al., 2020) it is expected to appear in both languages in a bilingual child. The official recommendation of the American Speech and Hearing Association (ASHA, 2004) and the IALP (International Association of Logopedics and Phoniatrics [IALP], 2020) is to assess a bilingual child’s ability in both languages for the purpose of diagnosing Developmental Language Disorder (see also RCSLT, 2019). Yet, often this recommendation cannot be adhered to due to lack of standardized tests in the various HLs present in addition to absence of SLPs who are native speakers of the HL. Translation of standardized tests is not recommended since each language assessment targets the language specific linguistic markers which indicate high risk for DLD.
Assessment of a bilingual child that includes a formal standardized test in the SL only leaves the SLPs with an incomplete description of the child’s language abilities and environment. Assessment in the SL only could result in over-diagnosis of DLD when the SL evaluation alone does not match the expectations from a monolingual child of the same chronological age (Peña et al., 2020; Armon-Lotem et al., 2021). Over diagnosis of DLD can lead to inadequate placement of children with typical language development (TLD) in special education preschools for children with DLD (see Iluz-Cohen, 2008; Armon-Lotem, 2010; Ruiz-Felter et al., 2016). As these educational settings are numbered and in high demand, this phenomenon has a negative impact on children with DLD who are denied access due to limited availability. Over-diagnosis results in overloading both healthcare system and educational resources in preschool and kindergarten years whereas underdiagnosis has a similar negative effect in school years. Therefore, it is necessary to make the diagnostic process of DLD among young bilingual children more accurate and beneficial for all parties involved.
DLD in monolinguals is diagnosed through testing the linguistic abilities of the child compared to age matched peers, however, when a child is exposed to two or more languages diagnostic process can be impacted by many additional factors such as: amount of exposure to each language, personal language aptitude, motivation, richness of language, exposure in an educational setting, verbal short-term memory etc. (Paradis, 2011; Paradis et al., 2016, 2017). With the large migration waves of the past decades, the number of children growing up with more than one language at home has increased dramatically. Some of these children are simultaneous bilinguals, exposed to more than one language from birth in various settings, while others are sequential bilinguals who acquire a SL when they enter preschool past the age of three (Thordardottir, 2019). Simultaneous bilingual children often reveal a similar rate of acquisition to monolinguals showing independent grammatical acquisitions in each language (Paradis and Genesee, 1996; Genesee and Nicoladis, 2007) with the possible exception of receptive vocabulary size (Paradis et al., 2003). By contrast, sequential bilinguals show a delay in the SL that reflects their length and amount of exposure to the SL (Paradis, 2009, 2010; Bohman et al., 2010; Armon-Lotem et al., 2021). The relatively low linguistic abilities in the SL when compared to age-matched monolingual peers and the impact of the HL are responsible for over-diagnosis of bilingual children with TLD as having DLD (Meir et al., 2016). Examining a young bilingual child in the SL only is not a reliable assessment of the linguistic skills due to influence of exposure to the SL or the influence of the HL (Iluz-Cohen, 2008; Nayeb et al., 2021). Gillam et al. (2013) used the EpiSLI model (Tomblin et al., 1996) deigned to identify children with language impairment among second language learners. They concluded an accurate use of the model can be achieved only when children attended an English-speaking public school and used English 30% of the time.
The Challenge of Diagnosing Developmental Language Disorder Among Bilingual Children in Israel
Israel is a multilingual-multicultural country in which 50% of the population are native speakers of HLs other than Hebrew, Israel’s official language and one out of five children in Israel speaks a language different than Hebrew at home (Robnov, 2006).
Speech and language clinics as well as Child Developmental Centers admit many children to their caseloads and waiting time for treatment vary between 3 and 12 months and sometimes even more in rural districts of the country. A national screening program has been operating since 2004 with the main purpose of identifying developmental delays at an early age allowing early intervention (Novogrodsky and Kreiser, 2019). The program is being operated by expert nurses for all children from birth till the age of five. Nurses meet every child in special child care units called “Tipat Xalav” (translates as “Drop of Milk”) located in every city where free services are offered for children and mothers (Tasher et al., 2016). In terms of language and communication skills, nurses are required to administrate a protocol designed to observe delays in expected milestones of language and communication skills. In case of an apparent delay or difficulty the nurses can refer the child for a full assessment by an SLP in Child Developmental Centers operated by one of Israel’s Health Maintenance Organizations (HMO) or by the Ministry of Health (Novogrodsky and Kreiser, 2019).
Referral to SLP can also be provided by the child’s pediatrician on his initiative or following a request from parents or teacher who are familiar with the child’s abilities. Parents are requested to provide a series of questionnaires filled out by them and by the educational staff (if the child attends a day care, preschool, kindergarten, or school). The questionnaires relate to all areas of developmental milestones, communication, social, and behavioral aspects. Those questionnaires, along with the doctor’s observation are sent to the Child Developmental Center of the –child’s HMO. A representative of a team of multi-disciplinary professionals reviews the questionnaire and summons the child for assessment according to her areas of difficulties. Waiting time for an assessment cannot exceed 3 months by law, however, in practice, it is often longer. Private clinics can also provide services of assessment and intervention; however, the costs are high and not all families can afford such services. Assessment is held in one or two sessions, using formal tests normed with monolingual Hebrew speakers, as well as intake data from parents. Once the initial assessment is completed by the SLP, a recommendation for intervention will be provided according to the child’s performance in those session/s along with “Language Difficulty” or definition if the child’s language formal test results were 1.25 SD below the average expected at that age (Ministry of Health, n.d. SLPs in Child Development).
Identification and diagnostic label of DLD will be determined after the age of three and only when a child demonstrates persistent difficulties in language acquisition despite consistent therapy, meaning, after a series of intervention sessions, which include dynamic assessment. Number of sessions varies by age and severity of the problem, leading to a large number of patients, 10% of children population (The State Comptroller Report, 2016), under the care of Child Developmental Centers, Developmental unites and private clinics associated with one of the four HMOs in the country. Yet, no specific attention is paid to the differences between bilinguals and monolinguals leading to overdiagnosis of bilinguals with DLD (Meir et al., 2016). Using parent questionnaires geared for bilingual development as a part of the protocol of bilingual children in Child Developmental Centers could have a potential impact on accuracy of assessment and treatment availability as efficient initial screening will reduce the number of children referred for individual intervention.
The process of assessment for a bilingual child in Israel relies on a formal standardized test in Israel’s SL Hebrew or its informal adaptation to Arabic, leaving the SLPs with an incomplete description of the child’s language abilities and environment. In Israel two standardized tests developed in Hebrew are used for DLD diagnosis in preschool years: (1) The Goralnik Screening Test for Hebrew (Goralnik Screening Test for Hebrew. Matan: Even Yehuda, Israel, Goralnik, 1995), includes six subtests: pronunciation, expressive vocabulary, comprehension, sentence repetition, expression, and storytelling. This test can be used from the age of 2:7 till the age of 6. (2) katzenberger Hebrew Language Assessment (Katzenberger and Meilijson, 2014), designed for older preschoolers at the ages of 4:00–5:11 includes six subtests as well: Auditory Processing, Lexicon, Grammar, Phonological Awareness, Semantic Categorization, and narrative expression. For older ages, SLPs often use the school- age version of the katzenberger Hebrew Language Assessment for ages 6–9 (Katzenberger and Meilijson, 2018).
All of the mentioned tests are widely used in clinics and educational settings in Israel and SLPs use one or more in the process of assessment according to the age of the child and her level of language performance. Limitations of availability or budget can influence the choice as well. All three language assessments were developed and standardized for Hebrew, targeting specific linguistic structures proven to distinguish between children with typical development and children with DLD.
Armon-Lotem et al. (2021) demonstrated the inadequacy of using formal tests developed for monolingual English speakers in measuring English used as a heritage language among bilingual children in Israel. Analyzing the performance of 240 bilingual English-Hebrew speaking children, ages 5–6; 6, on the Clinical Evaluation of Language Fundamentals, Preschool-2 (CELF Preschool-2; Wiig et al., 2004), they report a 10-point gap from the expected monolingual norm. Likewise, Altman et al. (2021) presented results from 397 typically developed bilingual children tested in the SL showing a consistent gap of more than 1 SD below the norm for their chronological age when using monolingual norms when testing in SL. Both studies demonstrate the difficulties of using monolingual standardized tests for English-Hebrew bilingual children suggesting that a combination of chronological age with age of onset of bilingualism might yield better assessment. Yet, English is only one of the HLs spoken in Israel, and an alternative for assessing children with other HLs in their HL is missing.
Thus, SLPs in Israel often rely on informal interviews to elicit background information from the parents but there is no official research-based protocol to follow. Moreover, these informal interviews hardly address the HL and mostly focus on parental concern. The Israeli case is far from unique and demonstrates the need for a practical solution for assisting this problematic diagnostic process found in many clinical settings. Parent questionnaires can offer such a solution as demonstrated in Boerma and Blom (2017). Boerma and Blom (2017) emphasized the clinical context as such in need for practical solutions in distinguishing between bilingual children with typical development and bilingual children with DLD and examined the use of parental questionnaire with standardized tests designed for bilingual context. Their results strengthen the possible value of using parental questionnaires in a diverse bilingual context as the combination of instruments presented enabled a differentiation between children with and without language impairment regardless of their linguistic background In this study we aim to offer an additional possible combination of informal tools or perhaps a suitable alternative by itself, available for every SLP, in our joined endeavors for making DLD identification among bilinguals more accurate.
Parent Questionnaires
Since the recommendation to diagnose and assess a bilingual child’s language ability in both languages cannot be followed as often as desired in a clinical setting, there is an increasing need for more practical tools and protocol to be implemented in clinics. The present study explores the possibility of adapting parent questionnaires, often used in research for collecting background information, in a clinical setting to complement the formal assessment protocol of young bilingual children. Parent questionnaires focusing on language related measures can offer a parental perspective on the child development, the essential insight into the HL abilities of the child, and observational comparison with other bilingual children in the use of the SL.
The use of parental reports about their children’s abilities is not uncommon. Parents certainly have extensive knowledge about their child in his/her natural environment and context. Thus, parental reports may have some advantages over an artificial testing situation. For example, questionnaires have been used to gather data regarding children’s vocabulary (Fenson et al., 1993), amount and quality of exposure to languages, including interactions with various interlocutors (Marchman and Martínez-Sussman, 2002; Bedore et al., 2012), assessing home literacy environment (Tambyraja et al., 2017) and early literacy (Boudreau, 2005).
Among parent questionnaires, the MacArthur-Bates Communicative Developmental Inventories (M-CDI, Fenson et al., 1994) is the best-known and most widely used parental report of the child’s linguistic abilities. Adapted for over 50 languages, the M-CDI is used to describe the expressive (and sometimes receptive) vocabulary of young children ages 8–30 months. Used for language evaluation of children with language delay (Thal et al., 1999), children with autism (Nordahl-Hansen et al., 2013), and bilingual speakers of various languages including Spanish-English bilingual children (Marchman et al., 2004), Irish-English (O’Toole and Hickey, 2017) and English-Hebrew Bilingual children (Armon-Lotem and Ohana, 2017). The M-CDI has become an established and valid source of young children’s linguistic profiles among monolinguals and bilinguals. In the bilingual context the M-CDI has been used successfully to assess the vocabulary in the HL, the SL, and in both languages together (Armon-Lotem and Ohana, 2017; Gatt, 2017; O’Toole et al., 2017).
Other parent questionnaires have been used for discriminating between children with and without DLD in monolingual (Callu et al., 2003, cited in Tuller, 2015) and multilingual contexts (Restrepo, 1998; Paradis, 2010; and also see Kašćelan et al., 2021 for an extensive review). ALDeQ, the Alberta Language and Development Questionnaire, was developed with the objective of creating a parental report containing information regarding the child’s HL development. More importantly, it was designed to differentiate English learners who are typically developing from those with DLD (Paradis et al., 2010). The ALDeQ includes four sections: (a) early milestones, (b) current Home Language abilities, (c) behavior patterns and activity preferences, and (d) family history. Two groups of bilingual children with various minority languages participated in that study: 139 with typical language development and 29 with Developmental Language Disorder. The study reports a significant difference between the two groups; the early milestones section emerged as the best discriminator and the current HL abilities the next best. The results of Paradis’ study demonstrate the potential of a questionnaire like the ALDeQ as a clinical tool, especially when information regarding the child’s HL cannot be obtained. Parental questionnaires have been used successfully as a part of a screening protocol for various conditions such as: gender identity development (Johnson et al., 2004), young children’s internalizing difficulties (Andrijic et al., 2013), and Autism (Mattila et al., 2012; Abbas et al., 2017). Mixed results were presented when screening for developmental delays in pediatrics’ clinics (Rydz et al., 2006; Kim and Sung, 2007). ALDeQ has been frequently used in research (Bonifacci et al., 2016; Hong and Yim, 2020) but seldom in a clinical setting (but see Karimijavan et al., 2021).
To complement ALDeQ and provide background information regarding the bilingual child’s linguistic experience and demographic environment in order to understand developmental patterns in the SL, Paradis (2011) designed the ALEQ, Alberta Language Environment Questionnaire. Using the ALEQ, Paradis (2011) showed a mixed influence of internal (e.g., chronological age or language aptitude) and external (e.g., mothers’ education or patterns of SL exposure) factors on the acquisition of English as the SL, measured by English standardized measures. Length of exposure to English and richness of English environment emerged as the two strongest predictors for performance on measures of verbal morphology and vocabulary. Unlike previous studies (Paradis, 2009, 2010), mothers’ education had marginal influence on vocabulary and accuracy in verbal morphology; and use of SL at home showed no influence on the child’s SL acquisition in general. Child-internal factors, as one factor, predicted more variation in children’s acquisition rates than external factors. In a more recent study, Paradis et al. (2017) presented findings regarding production of complex syntactic structures by L2-English children influenced by longer exposure to English in a school setting and richer English environments among the prominent predictors, using the ALEQ for data collection. Studies like this one reveal the potential power of parent questionnaires in providing valuable information when a standard assessment protocol cannot be used.
To further explore bilingual children’s risk factors for DLD, and Grimm and Schulz (2014) also used a parent questionnaire. They identified four factors: (a) late onset of single word stage, (b) late onset of multi-word stage, (c) family history of DLD, and (d) family history of difficulties with written language. Late onset of multi-word stage and family history of DLD were more prevalent among children with DLD and a moderate positive correlation was found between those risk factors and the SLPs’ evaluation. Thus, Grimm and Schulz (2014) suggested that the use of parent questionnaires could complement standardized language tests.
This suggestion has already been tested by Bishop and McDonald (2009), for example, in a study of monolingual children, where they explored the possibility of using the parent report “The children’s Communication Checklist” (CCC-2) for complementing formal assessment of Specific Language Impairment (currently known as DLD). 245 twin children (9–10 years old) participated in their study, 52 of them were referred to speech and language pathologists (CR-Clinically referred) as the rest were not (NR-Non-referred). A vast battery of tests was administrated to all participants and compared to CCC-2 ratings revealing that parent report managed to distinguish between children with and without language impairment both in the CR group and the NR group, similarly or better than formal tests.
The current study focused on CR and NR bilingual children in order to explore the potential of parental questionnaire for creating linguistic profiles for children in a clinical setting, distinguishing between clinically referred children with typical development (CR-TLD) and clinically referred children with DLD (CR-DLD). The aims of this study are to examine whether a parental questionnaire can be used as a screener for DLD among clinically referred bilingual children when standardized tests are unavailable. In addition, we aimed to discover what are the characteristics of children who were referred to SLP vs. the bilinguals who were not referred, as well as referred bilinguals who were not diagnosed as having DLD as oppose to the ones who were diagnosed with DLD.
The following questions will be addressed
1. Can parental questionnaires distinguish, between children with and without DLD? Which information (early milestones, HL skills, or SL skills) provides a better distinction within the CR group, and between the CR groups and the NR group?
2. Which specific questions tease apart the characteristics of children who were referred to SLP (CR) vs. the bilinguals who were not referred (NR), and which specific questions distinguish between those diagnosed the DLD and those who are not in clinical setting?
3. How accurate, in terms of sensitivity and specificity, are parental questionnaires among clinically referred bilingual children when standardized tests are unavailable? Can they be used for initial screening?
In light of the cited literature as well as the language context in Israel, where the study has been conducted, we shall be testing the following hypotheses:
1. Parental questionnaire can provide the information needed to differentiate between bilingual children with and without DLD even among children who have already been referred to the clinic. We expect this hypothesis to be borne out since referral by preschool teachers and even by pediatricians, is based on impressions of the SL abilities of the child, and does not take into consideration early milestone, family history, or HL abilities, domains which have been found to distinguish between children with TLD and children with DLD (Restrepo, 1998; Paradis et al., 2010; Grimm and Schulz, 2014). We further expect that SL abilities will distinguish between the NR group and the SR-TLD group, while HL abilities will be the same for these two groups.
2. Turning to the specific questions, we hypothesize that the questionnaire will assist in creating specific profiles that tease apart the three groups of children, distinguishing between bilingual children who were referred to SLP (CR) vs. the bilinguals who were not referred (NR), and between children who were identified as having DLD (CR-DLD) and those who were not (CR-TLD and NR). Previous study demonstrated higher presence of parental concern when it comes to language development among bilingual children as oppose to monolingual children (Boerma and Blom, 2017), thus is could be that such concerns might have brought the children to the clinic in the first place. If this is the case, parental concerns are not expected to distinguish the two clinical groups, but family history, as an independent measure might distinguish the groups (Leonard, 1998; Restrepo, 1998; Bishop et al., 2012). Similar differences are expected between the non-referred group and the children who have been diagnosed with DLD. Yet, children who were never referred to the clinic, might have a disorder that went undiagnosed, due to the assumption that bilingualism might be the cause of an observed delay. Thus, we expect less of a distinction on background information and family history, while the gap in HL abilities will remain distinctive (Paradis et al., 2010). Even if no significant differences are found in SL abilities, we anticipate that children who were referred to the clinic might have been less linguistically active in the SL than children who have never been referred.
3. We hypothesize that beyond the significant difference between the groups, a diagnostic accuracy will be attainable for the clinically referred children.
If these hypotheses are born out, drawing differential profiles for the different populations, is expected to contribute to a better screening process in our journey for an accurate identification of DLD. Moreover, if diagnostic accuracy is obtained, is expected to provide a tool for SLPs to better identify children with DLD and assist in determining the treatment goals and course of action.
Materials and Methods
Participants
Parents of 75 bilingual children (ages 48–82 months) participated in this study. 46 children were referred to SLPs by expert nurses, kindergarten teachers or doctors due to language performance difficulties (Clinically Referred- CR) and 29 were never referred to SLP (Non-referred- NR). NR children were recruited from public preschools in the center of Israel in which language of instruction is the SL-Hebrew. Most children spoke at home Russian (52) or English (18), with a few children in the clinics using other HLs French (3), Spanish (1), and Romanian (1). We have excluded children who meet the exclusionary criteria for DLD, having hearing impairment, repeated ear infections or language difficulties associated with ASD or another syndrome affecting cognitive development.
Due to the unreliability of the standardized assessment protocol in which bilingual children are assessed only in the SL, the SLPs were asked to reassess the children through Dynamic Assessment (DA). DA is a protocol based on Vygotsky’s concept of “zone of proximal development (ZPD)” which is defined as the distance between the “actual developmental level as determined by independent problem solving and the level of potential development as determined through problem solving under adult guidance or in collaboration with more capable peers” (Vygotsky, 1978, p. 86). In this protocol a base line assessment will be administered, determining the knowledge of the child in one or more domains followed by a teaching phase in which the focus is on the child’s learning potential accompanied by assessing the results of those efforts. Dockrell (2001), who reviewed several methods of possible language development evaluations, suggested that using process-based assessments could better assist us in comprehending the child’s difficulties and strategies when approaching a task, thus, giving us an insight to her learning potential rather than current ability which can be affected by multiple factors such as shyness and attention deficits (Camilleri and Law, 2007). In the case of multilingual children, the added language and culture differences can enhance the difficulty of obtaining reliable assessment based on one static evaluation as oppose to a process involving learning opportunities such as DA (Camilleri and Botting, 2013).
Multiple studies have demonstrated DA value in differentiating children with DLD and children with typical development in the process of learning a second language (Peña and Iglesias, 1992; Gutiérrez-Clellen and Peña, 2001; Peña et al., 2006; Hasson and Joffe, 2007; Kapantzoglou et al., 2012). In terms of language assessment in a clinical setting, it is widely used among SLPs to determine the presence of DLD among bilingual children in the absence of standardized tests (Hasson and Botting, 2010). The clinical framework, described in this study, provided a variety of linguistic abilities tested and evaluated as expected in such realistic situation. All SLPs evaluated expressive grammar tasks suitable to the child’s linguistic level. Progress was determined by measuring the child’s ability to acquire and use the grammatical rules taught during the period of assessment. SLP’s were able to diagnose the presence or absence of DLD according to their evaluation of a poor prognosis with persistent linguistic difficulties (Bishop et al., 2017).
According to SLPs’ dynamic assessment, only 19 of the children were identified as having DLD (CR-DLD) consequently, participants were divided into three groups based on the SLPs’ evaluation: clinically referred children diagnosed with DLD (CR-DLD), clinically referred children defined as having typical language development (CR-TD) and Non-referred bilinguals. Demographic data of the three groups are presented in Table 1.
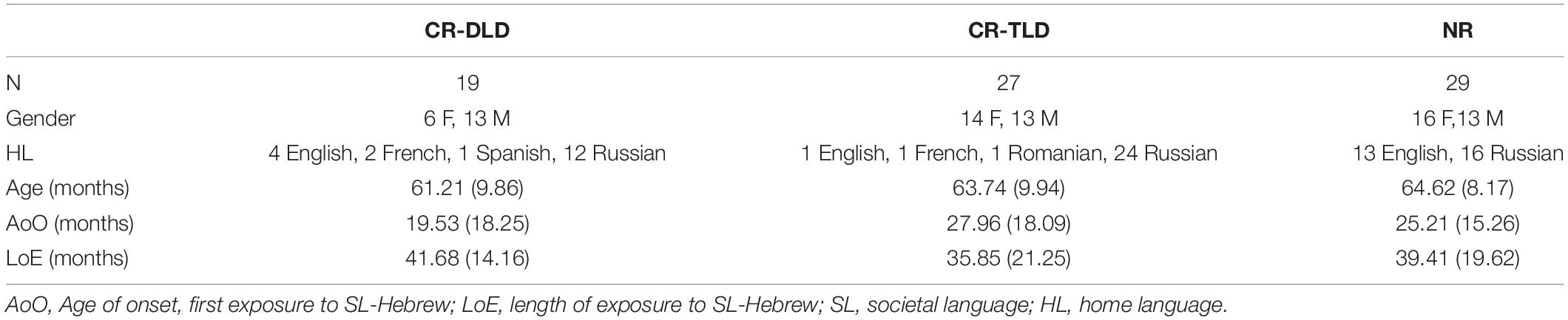
Table 1. Demographic data of the three groups.
Univariate GLMs showed no significant differences between the groups in Chronological age, Age of onset of SL (AoO) and Length of Exposure to SL (LoE).
Tools
Dynamic Assessment (Post-treatment Evaluation Form)
As the children with DLD were recruited from clinics, different standardized tests were used by the SLPs as part of their assessment (see section “The Challenge of Diagnosing DLD Among Bilingual Children in Israel”). All these tests were designed to evaluate language performance in Hebrew in monolinguals and are not reliable for use with bilingual children as mentioned above. Thus, the clinical diagnosis within the CR group was based on dynamic assessment procedure performed by the treating SLP and the standardized test results are not reported. The SLPs were asked to rely on their dynamic assessment conclusion and fill out a post-treatment questionnaire 3 months after treatment started detailing their professional expert diagnosis. The post treatment questionnaire also required the SLPs to provide information as to the length of treatment and the SLP’s opinion regarding the absence or presence of DLD following the treatment, including a detailed explanation for their response. This was complemented by questions on the child’s initial language standardized test results, a question about who referred the child and the reason for the referral, as well as general details concerning the child’s age, date of initial diagnosis done by the same SLP as well as the SLP’s work place and seniority.
Parental Report
The Bilingual Parent Questionnaire (BIPAQ), used in this paper, was developed from an SLP’s perspective, and is designed to serve as a protocol for soliciting background information in five domains: (a) Demographic Information, (b) Developmental background, (c) HL abilities, (d) SL abilities, and (e) Quantity and quality of exposure to both HL and SL. An SLP’s perspective includes needs, dilemmas and limitations arising in the clinic every day (e.g., time limitations) when different families from different cultures approach SLPs for assistance with the potential of being used as an accurate screener in a clinical setting. BIPAQ was developed alongside with the Parental Bilingual Questionnaire, PaBiQ (Tuller, 2015), within the European network COST Action IS0804 “Language Impairment in a Multilingual Society: Linguistic Patterns and the Road to Assessment.”1,2
To meet the needs of SLPs for a practical tool that can be used for soliciting background information on early milestones, the HL, and the SL with a clear scoring system, that can be used for creating a treatment plan, questions were selected from the ALDeQ (Paradis et al., 2010) and ALEQ (Paradis, 2011). The questions were adapted to the clinical setting in Israel adding questions that address everyday life in Israel, and integrated into one focused Bilingual Parent Questionnaire (BIPAQ, Abutbul-Oz et al., 2012). BIPAQ has three main advantages, that make it different from ALDeQ (Paradis et al., 2010) and ALEQ (Paradis, 2011) and more suitable for clinical setting:
Content
BIPAQ solicits information about both languages—for the HL to fill the gap created by the absence of standardized tests and SLPs who can test in the HL, and for the SL in order to cover for the absence of norms for bilinguals by obtaining the parents’ perspective of the ways in which their child compares with other children. In addition to the language-oriented questions for each language, BIPAQ also solicits information regarding quantity and quality of exposure to both languages. The information for SL-Hebrew was obtained in order to provide the SLP a better understanding of the linguistic environment of the child which will assist in reaching a more accurate diagnosis and treatment plan when needed.
Scoring
In order to pinpoint the source of difficulty, scoring was compartmentalized by the following sections: Early milestones and family history, HL abilities and SL abilities. Bilingual children with typical language development (TLD) and bilingual children with DLD often present different patterns of development in those domains despite similar language environment (Leonard, 1998; Restrepo, 1998; Paradis et al., 2010; Armon-Lotem and Meir, 2016). Difficulties in one language only are more typical bilingual development while difficulties in both languages are anticipated for bilingual children with DLD. Thus, for example, low score in the HL section as oppose to high score in SL section could be evidence for HL attrition.
Administration
To address the time limitations in the clinic, BIPAQ was designed to be used by parents independently before clinical evaluation, rather than as an interview.
The questionnaire begins with a short positioning to the parents explaining the complex situation of evaluating the language of a bilingual child and requesting their assistance in providing valuable data regarding their child’s linguistic abilities and environment. This came to address parents’ occasional feeling that they need to defend their choice to speak HL exclusively. Explaining the purpose of the questionnaire established the parents’ role as the best source of information regarding their children and requesting their assistance in the process of diagnosing the child.
The introduction is followed by 49 questions presented in the five separate sections: (a) Demographic Information—10 questions, (b) Developmental background—8 questions, (c) HL abilities—8 questions, (d) SL abilities—8 questions, and (e) Quantity and quality of exposure to both HL and SL—15 questions. The current study reports on findings for the first four sections. Findings from Section E are beyond the scope of the present study (see Supplementary Appendix A for the sections A–D). The use of BIPAQ was approved by the Bar-Ilan University Faculty of Humanities IRB committee and by the Ministry of Education.
Procedure
Parents of Non-referred bilinguals who attended regular preschools in multiple settings in the center of Israel were asked to fill out the BIPAQ. All parents signed an informed consent form and were asked to return the questionnaire by mail or email to the first author. The questionnaire was available for the parents in Hebrew, English and Russian.
Clinically referred bilinguals’ data collection was conducted in several private clinics servicing different locations in the center of Israel. Though the clinics are private businesses, they provide services through the major healthcare providers, ensuring that the referred population is representative of the bilingual population in Israel and not only of middle to high SES. All parents signed an informed consent form and were asked to fill out the BIPAQ and return it to the first author. The questionnaire was available for the parents in Hebrew, English, and Russian. Speakers of languages other than Russian or English used the Hebrew version. The version of the questionnaire that was used by the parents had no scoring information on it to ensure as much authentic responses as possible from the parents.
All questionnaires were analyzed and scored by the first author and not by the treating SLP in order to avoid any bias by parents’ input in the dynamic assessment.
Scoring and Analysis
All questionnaires were analyzed and scored according to BIPAQ’s scoring system detailed in Supplementary Appendix B. Maximum score is 63 points constructed from sections B to D. Section B of developmental milestones and family history contains 8 questions. Six questions used a 0-1-2 scale for age related developmental milestones and two were rated by the parents on a 0-1-2-3 Likert scale. Better outcomes (e.g., earlier age of walking or no acquisition difficulties) received a higher score to the maximum of 18 points. Sections C of HL abilities contained originally 8 questions as well, but one of them—about difficulties in learning the HL—was not answered by over 30% of the parents and was excluded from the scoring. Thus, the score was based on 7 questions, all scored on the same 4 points Likert scale (with max score of 3) to a total score of 21 points. Finally, Section D of SL abilities contains the same 8 questions as in Section C that, using the same scale, totaled in 24 points. The score obtained in each part was then converted to percentages out of the total score for that part and the total score obtained was then converted to percentages out of the total BIPAQ score. For example: if a child received 10 points in section B, 20 points in section C and 16 points in section D, the total score would be: (10 + 20 + 16)/63*100 = 73.01%. Lower score indicates a higher risk for DLD. The score in percentages, for each part and for the total score is used for further statistical analyses. Section E, Quantity and quality of exposure, is beyond the focus of the current paper.
The questionnaire has a fixed scoring system that leaves no space for the scorer’s judgment making the scoring simple and reliable. Thus, there was no need for inter or intra rater reliability measures. Cronbach’s Alphas was performed to evaluate internal consistency of the questionnaire, showing good to high reliability. The Developmental milestones and family history section (B) consisted of 8 items (α = 0.74), the HL abilities evaluation section (C) consisted of 7 items (α = 0.88), and the SL abilities evaluation section (D) consisted of 8 items (α = 0.85). The total evaluation was found to be highly reliable (23 items; α = 0.88).
Analysis commenced with descriptive statistic and GLMs comparing the Non-referred (NR), clinically referred DLD (CR-DLD) and clinically referred typically developing (CR-TLD) groups’ linguistic abilities as evaluated by parents. Analyses were applied to each part separately and to the total score. These were followed by post hoc Tukey HSD tests. In order to identify questions that better discriminate between the groups, Kruskal-Wallis Test was used for each question separately, since the scoring for the questions was either categorical or ordinal. These were followed by Mann-Whitney Tests for between group comparisons. The differential performance of the three groups on the different questions is used to identify the different profiles of children in the three groups. A ROC analysis is then conducted for the Clinically referred children only to identify the best cut-off point that distinguishes the two clinical groups (CR-TLD and CR-DLD) for which an SLP assessment is available. The ROC results are next applied to the NR group to explore if there are children in this group who might be at risk for DLD. Once identified, the differential performance of these on the different questions will be used to identify the different profiles of these children. This profiling process is expected to yield various characteristics of participants and contribute to the unique identifying bilinguals with high risk for DLD.
Results
Bilingual Parent Questionnaire Sections and Total Score
To address the first research question examining whether a parental questionnaire can distinguish between bilingual children with and without DLD and which information is more differential, Table 2 presents descriptive statistics for Sections B–D as well as the total score of the BIPAQ for the three groups of children. Univariate GLMs with Tukey HSD post-hoc tests were used to test for between group significance. Results are presented for each group of children in percentage (Mean, SD, and Range) followed by the statistical outcomes. Small superscript is used to indicate significant differences between the groups.
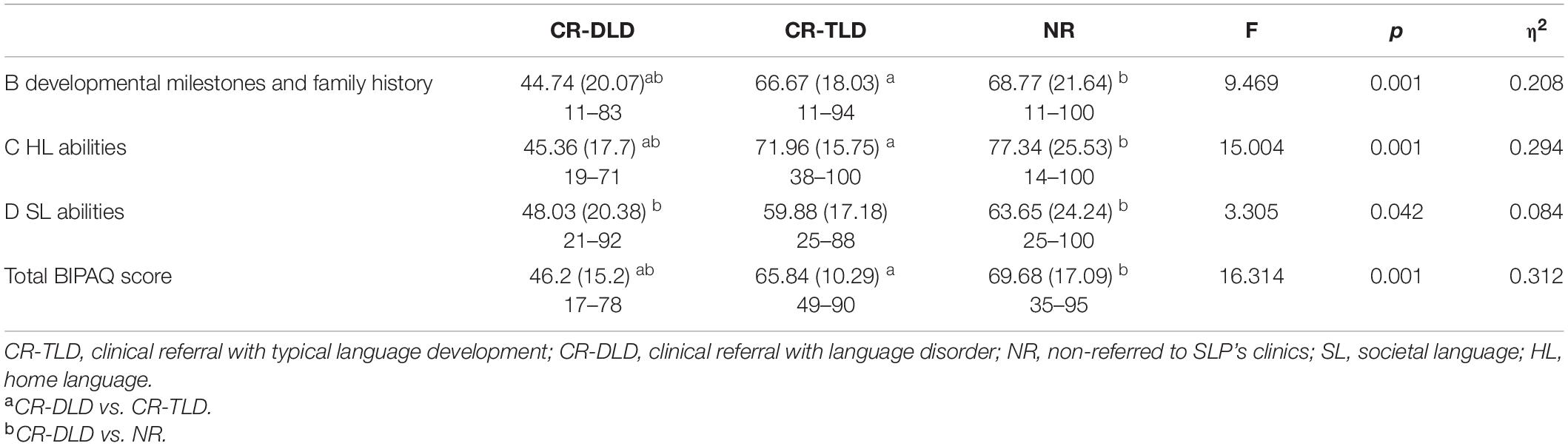
Table 2. Scores of BIPAQ: CR-DLD, CR-TLD, NR in percentage [Mean (SD), Range].
Table 2 shows a significant difference between groups for the three sections and the total score alike. Developmental milestones and family history, and HL abilities were more predictive of the difference between the groups than SL abilities (adjusted R2 = 0.186, adjusted R2 = 0.275, adjusted R2 = 0.059, respectively). The total score was the most predictive of the difference with adjusted R2 showing that group explains 29.31% of the variance in total BIPAQ scores. Tukey HSD post hoc tests indicates that the score for CR-DLD is significantly lower than the other two groups (ps < 0.001) but no difference was found between CR-TLD and NR children (p = 0.58).
Since all three sections came from the same participants, a GLM with Section as a Repeated Measures and Group as an Independent Variable was performed. A significant difference was observed on the Mauchly’s test of Sphericity (p = 0.01). Therefore, Greenhouse-Geisser was used to test within subjects’ effect of Section. A significant difference was observed, F(1.7, 128.5) = 3.522, p = 0.037, with no interaction between Section and Group, suggesting that the difference between the sections is the same for all groups.
Following the GLMs reported in Table 2, Tukey HSD post hoc tests were conducted for each section of the BIPAQ separately. In Section B, exploring developmental milestones and family history significant differences were observed between the CR-DLD and CR-TLD groups (p < 0.001) as well as between CR-DLD and NR children (p < 0.001), with no significant difference between CR-TLD and NR children (p = 0.918). Likewise, in Section C, HL abilities, significant differences were observed between CR-DLD and CR-TLD groups (p < 0.001) as well as between CR-DLD and NR children (p < 0.001), with no significant difference between CR-TLD and NR children (p = 0.592). By contrast, in Section D, a significant difference was found between CR-DLD and NR children (p < 0.036), but no significant difference was documented between CR-DLD and CR-TLD children (p = 0.149), nor between the CR-TLD and NR children (p = 0.780). The implications of this later finding for the differential profiles of bilingual children and its explanatory value for understanding why the CR-TLD were initially referred to the clinic will be addressed in the discussion.
Developing Differential Profiles—Analysis by Question
Further analyses by questions are next presented to address our second research question, and discover the characteristics of children who were referred to SLP (CR) vs. the bilinguals who were not referred (NR) as well as referred bilinguals who were not identified as having DLD (CR-TLD) as oppose to the ones who were identified as having DLD (CR-DLD). The analysis by specific questions will further contribute to shortening the questionnaire to meet the time constraints in the clinic.
To explore the effect of group on the different questions of the BIPAQ, a GLM with Question as Repeated Measure and Group as an Independent Variable was performed for each section. In Section B, a significant difference was observed on Mauchly’s test of Sphericity (p < 0.001). Therefore, Greenhouse-Geisser was used to test for effect of questions within subjects, showing a significant difference for Question, F(5,248) = 25.684, p < 0.001, as well as an interaction between Question and Group, F(10, 496) = 2.922, p = 0.001, suggesting that the difference between the questions is not similar for all groups. In Section C, a significant difference was observed on Mauchly’s test of Sphericity (p < 0.001). Therefore, Greenhouse-Geisser was used to test for effect of questions within subjects, showing a significant difference for Question, F(4, 691) = 18.441, p < 0.001, but no interaction between Question and Group, F(9, 382) = 1.154, p = 0.323, suggesting that the difference between the questions is similar for all groups. In Section D, a significant difference was observed on Mauchly’s test of Sphericity (p < 0.001). Therefore, Greenhouse-Geisser was used to test for effect of questions within subjects, showing a significant difference for Question, F(3, 779) = 20,534, p < 0.001, but no interaction between Question and Group, F(7, 559) = 1.850, p = 0.072, suggesting that the difference between the questions is similar for all groups.
Section B: Developmental Background and Family History
Table 3 presents descriptive results by Group for responses to questions presented in section B, in Means (SD) and Mean Rank, as well as the Kruskal-Wallis Test results. Small superscripts are used to indicate significant differences between two groups following a Mann-Whitney Tests.
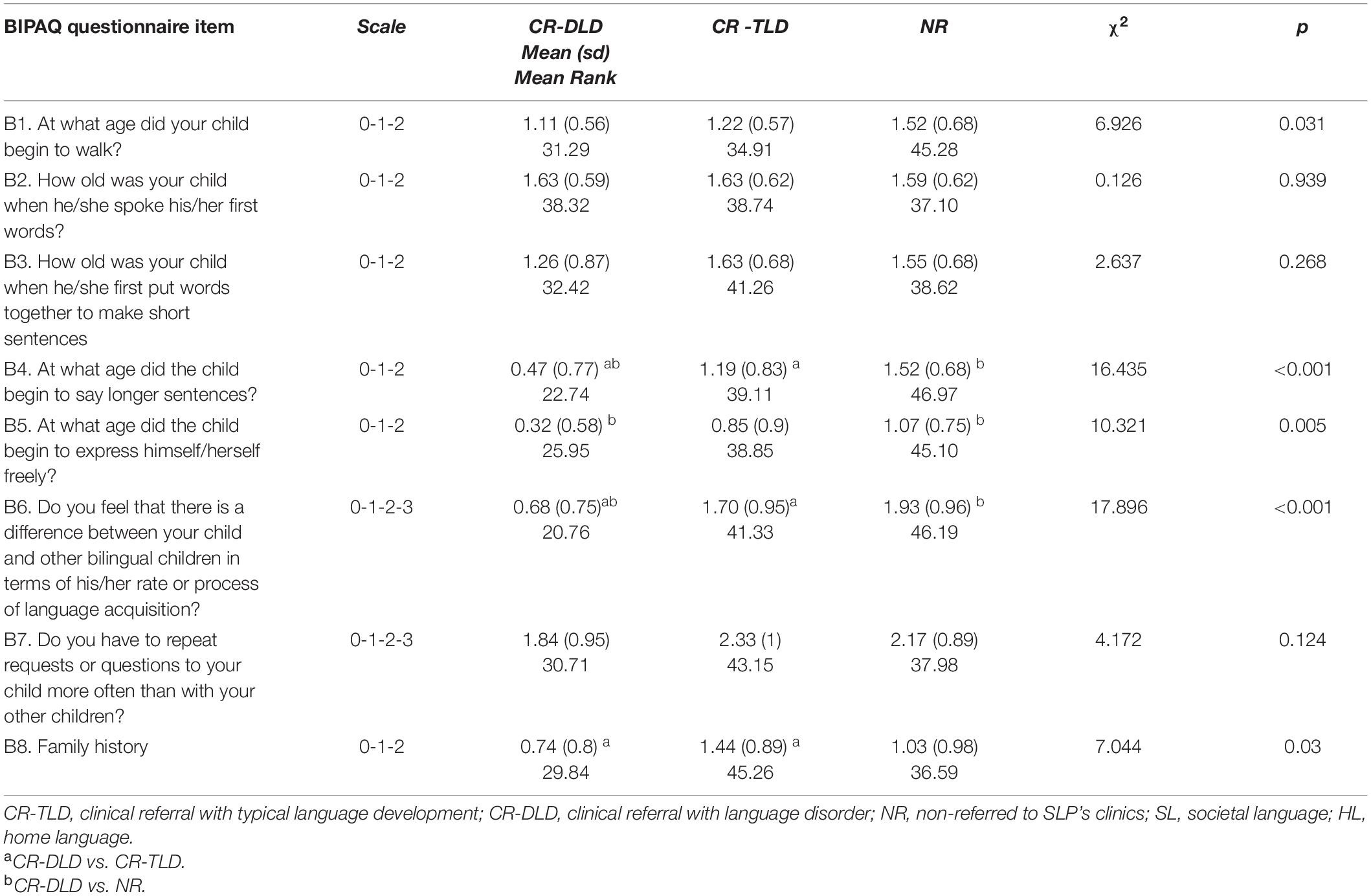
Table 3. Questions Section B: developmental background and family history.
Table 3 presents an effect of Group on age of walking (B1, p = 0.031), age of using longer sentences (B4, p < 0.001), age of being able to express oneself freely (B5, p = 0.005), difference from other bilingual children (B6, p < 0.001), and family history of disorders (B8, p = 0.03). Age of first of first words, age of word combinations and need to repeat requests did not yield a significant difference.
Mann-Whitney Tests used for post hoc analyses show significant differences between CR-DLD and CR-TLD groups in age of using longer sentences (B4, p = 0.006), age of being able to express oneself freely (B5, p = 0.041), difference from other bilingual children (B6, p = 0.001), need to repeat requests (B7, p = 0.043), and family history of disorders (B8, p = 0.007). Using the Holm’s Sequential Bonferroni Procedure to avoid familywise error, only age of using longer sentences, difference from other bilingual children, and family history remain significant.
For the CR-DLD and NR groups, an effect of group was found for age of walking (B1, p = 0.018), age of using longer sentences (B4, p < 0.001), age of being able to express oneself freely (B5, p = 0.001), and difference from other bilingual children (B6, p < 0.001). Using the Holm’s Sequential Bonferroni Procedure to avoid familywise error, only the last three remained significant. In contrast to the CR-DLD vs. CR-TLD comparison, family history did not come out significant. No significant differences were observed between the CR-TLD and NR children in any of the questions in Part B.
Section C: Home Language Abilities
Table 4 presents descriptive results by Group for response to questions presented in Section C, providing Means (SD) and Mean Rank as well as the Kruskal-Wallis Test results. Small superscripts are used to indicate significant differences between every two groups using Mann-Whitney Tests.
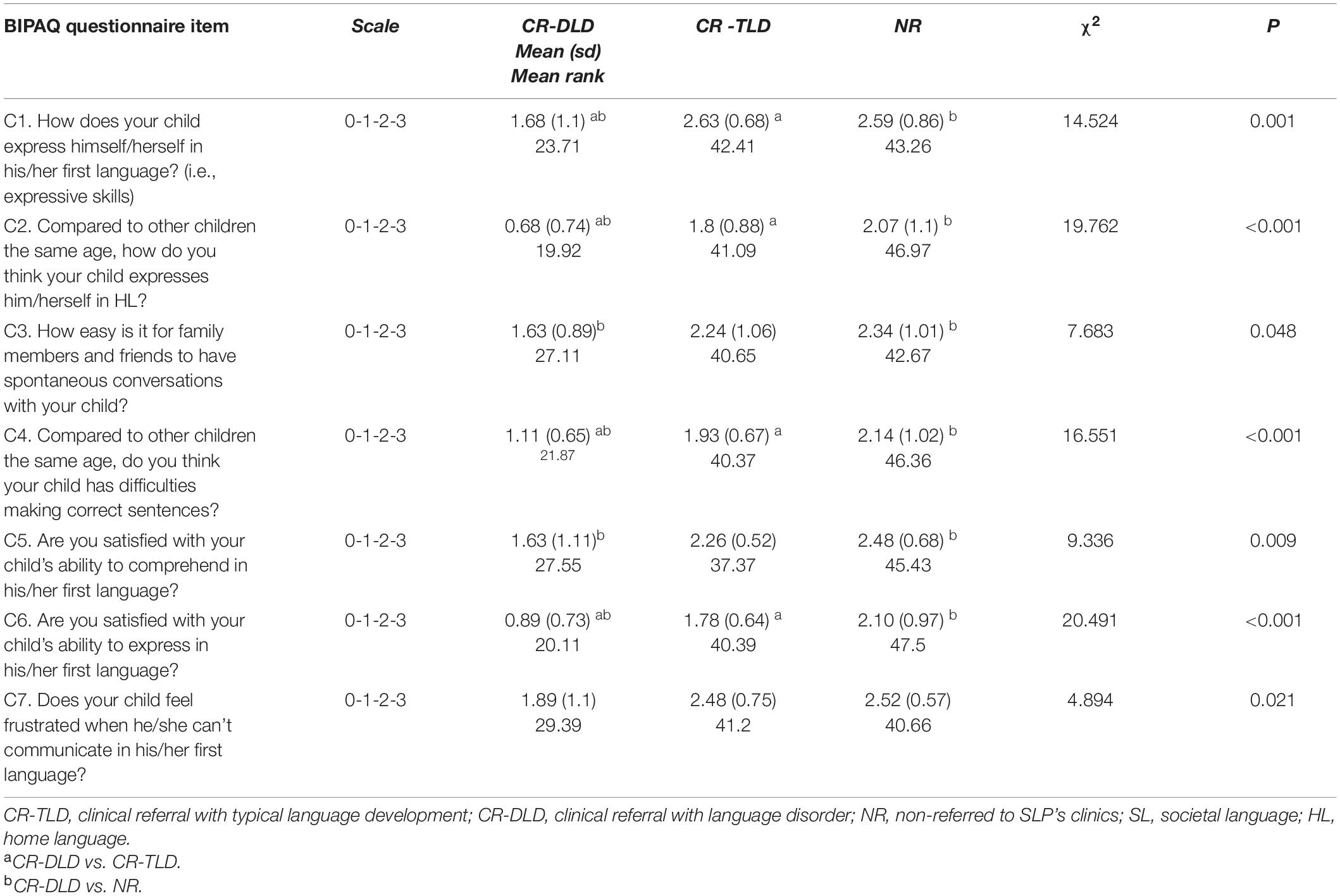
Table 4. Questions Section C: HL Language abilities.
Table 4 presents an effect of Group for all questions. Mann-Whitney Tests used for post hoc analyses show significant differences between CR-DLD and CR-TLD groups in expressive skills of HL (C1, p = 0.001), expression of HL in comparison to other bilinguals (C2, p < 0.001), spontaneous conversation fluency in HL (C3, p = 0.027), using correct sentences in HL (C4, p < 0.001) and satisfaction from HL expression (C6, p = 0.001). Using the Holm’s Sequential Bonferroni Procedure to avoid familywise error, all but spontaneous conversation fluency in HL remains significant.
For the CR-DLD and NR groups, an effect of group was found for expressive of HL (C1, p = 0.001), expression of HL in comparison to other bilinguals (C2, p < 0.001), spontaneous conversation fluency in HL (C3, p = 0.01), using correct sentences in HL (C4, p < 0.001), satisfaction from HL comprehension (C5, p = 0.005) and satisfaction from HL expression (C6, p < 0.001) Using the Holm’s Sequential Bonferroni Procedure to avoid familywise error, all question apart from frustration when communicating in HL remain significant.
In contrast to the CR-DLD vs. CR-TLD comparison, C5- satisfaction from HL comprehension and C7- frustration when communicating in HL come out significant. No significant differences were observed between the CR-TLD and NR children in any of the questions in section C.
Section D: Societal Language-Hebrew Language Abilities
Table 5 presents descriptive results by Group for response to questions presented in Section C, providing Means (SD) and Mean Rank as well as the Kruskal-Wallis Test results. Small superscripts are used to indicate significant differences between every two groups using Mann-Whitney Tests.
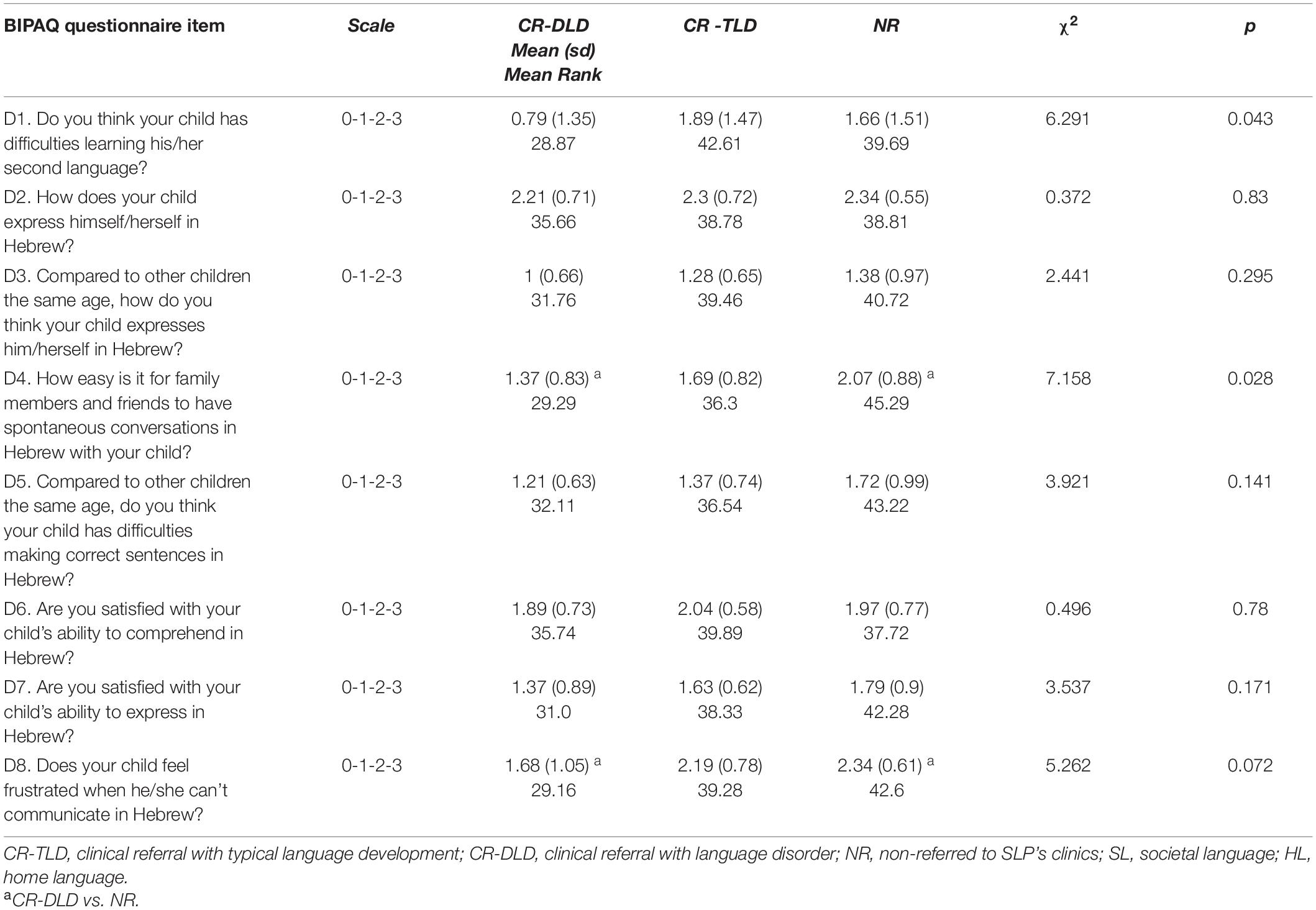
Table 5. Questions Section D: SL-Hebrew Language abilities.
Table 5 presents an effect of Group on difficulties in learning SL-Hebrew (D1, p = 0.043) and spontaneous conversation fluency in SL-Hebrew (D4, p = 0.028).
Mann-Whitney Tests used for post hoc analyses show significant differences between CR-DLD and CR-TLD groups only in difficulties in learning SL-Hebrew (D1, p = 0.015). Using the Holm’s Sequential Bonferroni Procedure to avoid familywise error, this difference is not significant anymore. For the CR-DLD and NR groups, an effect of group was found for spontaneous conversation fluency in SL-Hebrew (D4, p = 0.011) and frustration when communicating in SL-Hebrew (D7, p = 0.026). Yet, using the Holm’s Sequential Bonferroni Procedure to avoid familywise error none of these differences is significant. No significant differences were observed between the CR-TLD and NR children in any of the questions in section D.
Accuracy, Specificity, and Sensitivity of Bilingual Parent Questionnaire
Accuracy, specificity, and sensitivity were examined to assess whether BIPAQ can provide a tool for SLPs for screening bilingual children with DLD in a clinical setting. Thus, this part applies only to the CR group. Implications of this analysis to the NR group will be discussed.
To check the accuracy of the BIPAQ as a potential clinical tool, sensitivity and specificity, traditional measures of diagnostic accuracy, were explored. Using a ROC analysis, the predictive accuracy of a test can be measured by the area under the curve (AUC), representing the overall accuracy of a test: an area of 1 indicates a perfect test; an area of 0.90–1 indicates excellent accuracy; an area of 0.80–0.90 signifies good accuracy; an area of 0.70–0.80 exemplifies fair accuracy; and an area of 0.60–0.70 indicates poor accuracy. Sensitivity of a clinical tool refers to how well it diagnoses a true positive condition, in the present context, children with DLD as being impaired whereas specificity refers to how many true negative conditions are identified as such, that is, children with TD (Hajian-Tilaki, 2013). Figure 1 presents the ROC results for the clinical group.
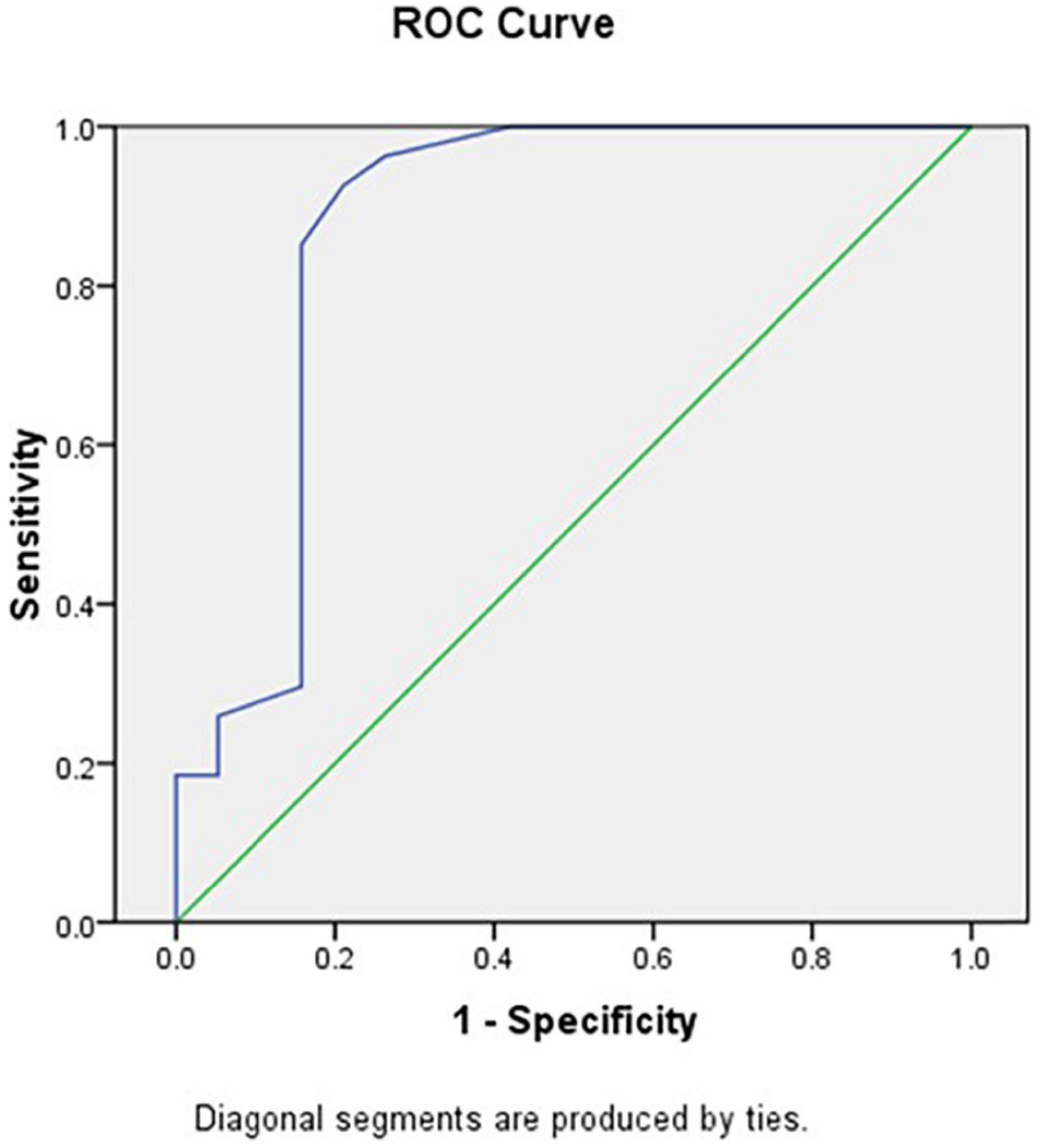
Figure 1. ROC curve analysis of total BIPAQ scores.
The total score of the BIPAQ was calculated from the sum of sections B–D divided by 63 points and converted into percentages. The ROC analysis of the total BIPAQ score yielded a score of 56.35% as the cut-off point with the best balance of sensitivity (0.852) and specificity (0.842). The area under the curve is 0.869, signifying good accuracy (Dunn, 2014). That is, the total BIPAQ score shows good sensitivity and specificity and good accuracy.
Discussion
Using parent questionnaire for evaluating their children’s language skills is an increasingly growing method, assisting in providing valuable data regarding the child’s developmental background and linguistic environment. However, it was mainly used in studies in research settings. In this study we attempted to examine whether a parent questionnaire can distinguish between clinical and non-clinical groups. Furthermore, we aimed to discover what are the characteristics of bilingual children referred to SLPs as oppose to the ones who were not, in an attempt to possibly create profiles identified with each group. Finally, we tested whether such a questionnaire can be used as a screener for DLD as a part of a diagnosis process in a clinical setting.
The Differential Power of Parental Questionnaires
CR-DLD group presented lower scores in all three sections as well as the total BIPAQ score. Total score of the BIPAQ for CR-DLD is significantly lower than the other two groups but no difference was found between CR-TLD and NR children. Similar results were presented for sections B- developmental milestones and family history and section C- HL abilities describing significant differences between CR-DLD group and both CR-TLD and NR groups but no difference between CR-TLD and NR groups. The difference in the total BIPAQ score as well as sections B and C is highly significant indicating that parental questionnaire data can differentiate between bilingual children with and without DLD. CR-DLD children were reported by their parents to have low language proficiency in both HL and SL-Hebrew in addition to delays in acquiring developmental milestones and family history of language related difficulties. The consistent differences between the results of the CR-DLD group and the CR-TLD and NR groups, emphasizes the fact that Developmental Language Disorder is indeed apparent in both HL and SL regardless of age, AoO or quantity and quality of exposure. These findings emphasize the importance of obtaining information relating to the child’s history and most importantly, HL abilities, as we can witness the tremendous value of this knowledge in distinguishing between TLD bilinguals and children with DLD.
When a bilingual child arrives to the clinic, SLP’s are required to determine a possible risk for DLD and provide a recommendation for intervention after one or two sessions. Adding to that challenge, using monolingual norms of standardized tests in the SL, would inevitably lead to more assessments of possible risk for DLD resulting in much more recommendation for further treatment. In the absence of standardized tests in the HL or available norms for bilingual children the SLPs are in need of information about the HL abilities to better assess the risk for DLD (Thordardottir, 2015). As mentioned before, an accurate identification of DLD among bilingual children requires evaluation of both languages (Nayeb et al., 2021) which is rarely possible, leading the SLPs to use a dynamic assessment model as was done by the SLPs whose patients took part in this study. The high correlation between the results of the BIPAQ and the identification of DLD post DA could outline a possible path for a better diagnostic protocol combining the two measures. The possible use of a parent questionnaire as a screener for DLD would benefit SLPs if the following conditions are met: (a) a unified questionnaire is available consisting of the most indicative questions to differentiate typical bilingual development from DLD markers; (b) the questionnaire must be easy to use in a clinical setting which has time limitations, that is, the questionnaire should be short, self-explanatory and available in multiple languages; and (c) the questionnaire cannot be language dependent, that is, it should be possible to use it to gather information on many different languages or dialects encountered in clinics.
Language Profiles Bilingual Children
Our second aim was to discover what are the characteristics of children who were referred to SLP vs. the bilinguals who were not referred but more importantly, we wanted to try and differentiated between the referred bilinguals who were not identified as having DLD as oppose to the ones who were identified as having DLD. To achieve that goal a Mann-Whitney Tests used for post hoc analyses of each question was performed yielding the following conclusions:
Group Profiles for Clinically Referred With Developmental Language Disorder vs. Clinically Referred With Typical Language Development
CR-DLD bilingual demonstrated later age of using longer sentences, larger difference from other bilingual children in language acquisition process leading to parental concern as well as more cases of family history when compared with CR-TLD children. Parental concerns are often considered as risk factors in the process of evaluating risk for DLD (Klee et al., 2000; Bishop et al., 2006; Tuller, 2015), and indeed, a close observation of the distribution of responses shows that only 3 of the parents in the CR-DLD group (16%) were satisfied with their children’s language development compared to 16 of the parents of CR-TLD children (60%), of whom 6 actually reported that they believed their children were better than other bilinguals of the same age. This definitely raises the question of why they were even referred to the clinic. Clearly, the answer to this does not lay in their HL abilities, since CR-DLD children demonstrated lower performance than CR-TLD bilinguals in all questions relating their HL abilities, apart from spontaneous conversation fluency in HL, stressing the importance of receiving information of HL language performance of children referred to the clinic for DLD assessment. Is the difficulty in spontaneous conversation fluency in HL enough to explain the referral?
Another most striking difference between these two groups is in terms of family history. While 15 of the 19 children in the CR-DLD group (79%) had at least one family member with language or learning disorders, only 8 of the 27 children in the CR-TLD group (less than 30%) had a family member with a language or learning disorder. While the percentage observed in the CR-TLD group is similar to what is expected in the general population, the findings for the CR-DLD group are reminiscent of those reported in previous studies of disordered populations (Bishop et al., 2006; Conti-Ramsden et al., 2006; Grimm and Schulz, 2014; Rudolph, 2017).
As these two groups are significantly different on both B- developmental milestones and family history and section C- HL abilities, the reason for referral must lay in their performance in SL. And indeed, the two groups show no significant difference in this respect. The only marginal difference in difficulty learning the SL emerges with parents of 17 of the children in the CR-TLD group reported no difficulty in acquiring the SL, while 14 of the parents in the CR-DLD group reported difficulties in acquiring the SL. But despite this difference in terms of the parents’ perception of their children acquisition process, the outcome was similar in the two groups, suggesting that referral was based on SL performance. This, as has often been noted, leads to over representation of bilingual children in clinical setting due to over diagnosis.
Group Profiles for Clinically Referred With Language Disorder vs. Non-referred
To better understand what it is that led to the referral of the CR-TLD group, we turn next to the comparison between the CR-DLD and NR group, in hope to learn what in the profile of children in the NR group distinguished them from the CR-DLD children. Similar difference to those observed between CR-DLD and CR-TLD children are found between the CR-DLD and NR children. Yet, several interesting differences emerged. Like the CR-TLD group, children in the NR group present earlier age of using longer sentences, and lower difference from other bilingual children in language acquisition when compared to the CR-DLD. Yet, the children in the NR group also present an earlier age of being able to express oneself freely. More specifically, of the 29 parents of the NR group, 21 (72%) reported that their children were fluent before the age of three, compared with only five parents (36%) in the CR-DLD group (and only one before the age of two and a half). The CR-TLD group is in-between with 14 out of the 27 children (52%) being fluent before the age of three. Could fluency explain why children were referred or not referred to the clinic? We return to this point below when discussing the abilities of the NR children in the SL.
While early fluency differentiated the children in the CR-DLD group and those in the NR-group, family history, which was significant for the CR-TLD did not emerge as a predictor of the difference between the CR-DLD and NR groups. This luck of significance difference from the CR-DLD group on this question is likely to be indicative of the heterogeneous nature of the NR group, as observed in Bishop and McDonald (2009), and will be further discussed below (section “Parent Questionnaire as a Screener for DLD in a Clinical Setting”).
Turning to language abilities in both languages, parents of CR-DLD children reported lower HL abilities than NR bilinguals in all questions, apart from spontaneous conversation fluency in HL, stressing, yet again the importance of receiving information on the HL language performance of children referred to the clinic for DLD assessment (Rudolph, 2017). As for SL use, no significant differences were observed between the groups, as predicted by previous studies that showed that bilingual children may show delays and characteristics that are also markers of atypical development during early stages of acquisition (Paradis, 2005; Paradis et al., 2008). Yet, parents did report lower, marginally significant, ability to engage in a fluent spontaneous conversation in SL-Hebrew and experiencing more frustration when communicating in SL-Hebrew for the CR-DLD group compare to the NR group. These results suggest that children might have been referred to the clinic due to more general language related behavior as they were probably less active in language related activities in the SL and thus more frustrated, rather than due to presenting a different linguistic profile in SL.
Group Profiles for Clinically Referred With Typical Language Development vs. Non-referred
Since both the CR-TLD group and the NR group are significantly different from the CR-DLD group in rather similar way, the question remains, why were the children in the CR-TLD referred to the clinic in the first place, and what was the reason for the luck of referral among the NR group. No significant differences were found between CR-TLD group and NR group in any of the questions in sections B–D. While both engaging in conversation in the SL and frustration emerged as questions that might explain why the CR-DLD children were referred, this does not seem to explain the referral of the CR-TLD children. Further observation of individual data on the one hand, and other background variables, on the other, might provide a better explanation.
Comparing the Three Groups
Close observation of the questions in section B presented an interaction between Section and Group suggesting that the profile of responses was different across the group. This is also apparent when comparing two groups at a time. To further compare the profiles of the three group, Figure 2 presents stacked bars for section B questions for the ratio of participants who received each score by groups, where higher scores are indicative of typical development.
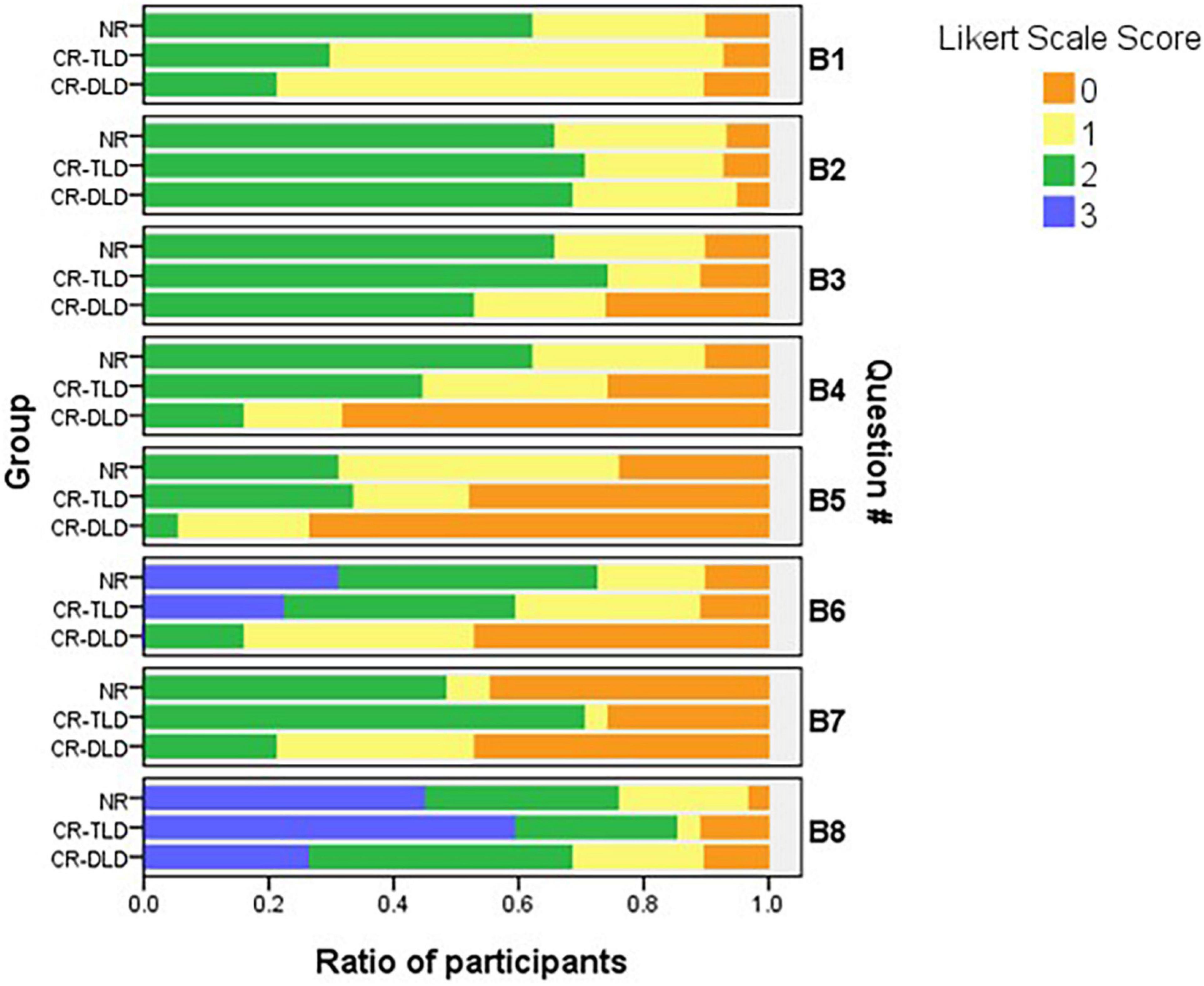
Figure 2. A comparison of the responses to Section B questions within each group.
A comparison of the stacked bars for three groups by questions demonstrates that the CR-DLD group presents the majority of the scores at the lower end on questions B4—age of producing sentences, B5—expressing oneself freely, B6—parental concern due to different acquisition, and B8—family history, while the scores of the other two groups are mostly in the middle range for these same questions. Questions B4 and B5 show distribution in the lower range for the CR-DLD group, in the lower and middle for the CR-TLD group and in the middle range for the NR group. That is, asking directly about expressive skills can explain why children in the CR-TLD group were clinically referred to start with, being in-between the two other groups. When turning to parental concern (Question B6), responses are in the lower range for the CR-DLD, in the middle range for CR-TLD group and in the middle and higher range for the NR group, showing again a similar gradation. Crucially the middle range already indicates that the parents did not notice a difference from other children. Finally, the responses on question B8 are in the lower range for the CR-DLD while the range of responses of the other two group is widely spread, with the majority of the responses being in the upper end indicating no family history.
Sections C and D were less informative for identifying different profiles, as there was no interaction between questions and group. Children in the CR-DLD were reported to perform low on all questions in section C, while the children in the CR-TLD group were scored in the middle and upper ranges for all questions, whereas a wide range of response was reported for section D, with relatively similar distribution for the questions in the three groups and no distinct profiles.
Parent Questionnaire as a Screener for Developmental Language Disorder in a Clinical Setting
A ROC analysis of the total BIPAQ score for all the Clinically Referred children (both CR-DLD and CR-TLD) yielded a score of 56.35% as the cut-off point with the best balance of sensitivity (0.852) and specificity (0.842). ROC Curve analysis presented an area under the curve of 0.869, signifying good accuracy. In comparison, the use of monolingual norms in SL-Hebrew for bilinguals yields 15–72% of over diagnosis of DLD, manifested in a specificity value of 77% when comparing to a result −2 SD below the expected mean at the same chronological age (Altman et al., 2021). These results illustrate the potential of using a parent questionnaire as a screener during DLD diagnosis protocol in a clinical setting, thus addressing the last research question.
The observed cut-off point further offers an opportunity for an exploration of the individual children in order to understand how they perform in comparison with this threshold, with the possibility of qualifying the different profiles. Of a particular interest in the NR group as previous studies report underdiagnoses of DLD among bilinguals. Figure 3 presents a scatterplot summarizing individual reported scores organized by age (X-axis) and BIPAQ total score (Y-axis). It shows how each child is reported to perform compared to the cut-off point.
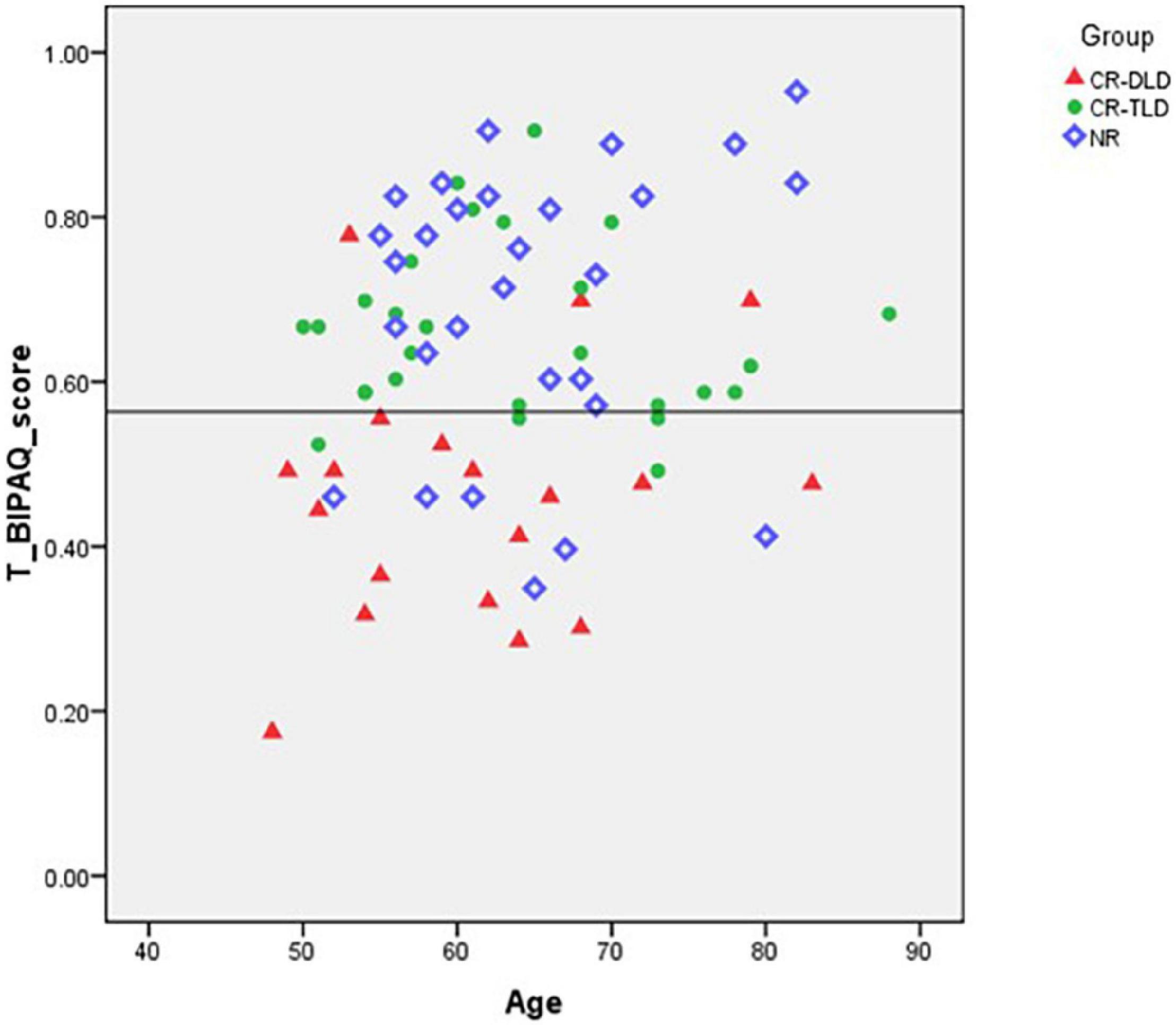
Figure 3. Reported performance by age, for individual children within each group.
As can be seen in Figure 3, most of the CR-TLD and NR bilinguals are above the 56.35% cut-off point defined by our ROC analysis. However, there are six children of the NR group who scored lower than 56.35%. Reviewing those participants’ questionnaires reveals parental concern regarding their language acquisition process, four parents indicated their children’s language acquisition process as “a little less good than others” and two referred to it as “not at all like others.” Parental concern emerged as a prominent indicative measure for establishing a risk for DLD in previous studies (Klee et al., 2000; Bishop et al., 2006; Tuller, 2015), and significantly distinguished between the CR-DLD and CR-TLD children in the present study. This supports previous suggestions to include it as a valuable part of assessment protocol, especially among bilingual children who might demonstrate misleading results in standardized tests using monolingual norms (Klee et al., 2000; Tuller, 2015). Another pattern that emerged from this analysis is that of HL attrition, as one of the children who scored low, presented a low score in the total score due to very low scores in the HL, however, his score for section D-SL abilities was high.
The presence of children who are at risk for DLD in the NR sample is not unreasonable and these finding from the BIPAQ might pick it up, while explaining the heterogeneous profile of the NR group. Bishop and McDonald (2009) related to this phenomenon in this cohort as 44 of the 82 children diagnosed with DLD in their study were never referred to SLP assessment, mostly attributed to the low socio-economic status of the family.
Clinical Implications
Identification of DLD among bilingual children presents a challenge for SLPs given the multiple factors influencing possible diagnosis. Parental questionnaire can provide valuable data to complement various formal and informal tests allowing accurate identification of DLD for the benefit of bilingual children (Paradis et al., 2013; Boerma and Blom, 2017).
The data presented in this study emphasize the importance of evaluating the child’s abilities in her Home Language for identification of DLD. The high accuracy of the total score of the BIPAQ as well as the significant between group difference of the separate scores of sections B and C suggest that SLPs might be able to use the BIPAQ in a clinical setting to complement the clinical tools (when available) and provide a more accurate and complete assessment before treatment begins. Each section of the BIPAQ measures different risk factors for DLD, while enabling evaluation of the child’s HL which is not obtained currently in any other way. This information obtained by BIPAQ is relevant both for initial assessment to determine whether intervention or further assessment is needed and later when identification and diagnosis of DLD is given.
Furthermore, our study demonstrates which type of information is particularly helpful and which particular questions work best. The statistical analyses indicate that questions dealing with Family history, milestones in using grammar and expressive skills of the HL are valuable for SLPs in providing accurate diagnosis of DLD. These results could be used to reduce the length of the BIPAQ, possibly making it more practical for clinical use.
Limitations of the Study
The present study, with its heterogenous cohort and unique setting, presents several limitations. First, the current findings reflect an atypically large proportion of children with DLD as the clinical group was the focus of the study. The number of participants allowed us to obtain a cut-off point, however, despite strong specificity and sensitivity, more data from non-referred population is needed to verify this and determine whether the cut-off point identified in the present study within the clinic, can be used among bilingual children in the general population before referral to the clinics in order to identify children at risk. Furthermore, we should consider the fact that the cut-off point presented here was the most balanced for research purposes but is not necessarily the best for a clinical setting in which we aim to have less under-diagnosis. In such a setting we might consider using a higher level of sensitivity at the expense of a lower level of specificity. Second, we acknowledge the fact that parents who are native HL speakers were asked to evaluate their children SL abilities, which might constitute a challenge for those parents and effect the results. Yet, most heritage speakers in Israel have good command of the SL, and this was also evident for the current cohort who rated their SL skills on the higher side of the scale. The authors also aim to provide translation of BIPAQ in multiple languages for future use. Finally, the results of the present study, while carrying promise for a more accurate diagnosis upon arrival at the clinic, raises an ethical question. It is not clear how those children who are experiencing SL functional difficulties to the degree that someone thought it necessary to refer them to an SLP should receive intervention once it is clear that they do not have a DLD. The authors believe that intervention, possibly of a different magnitude, could definitely benefit these children for two major reasons: (a) second generation bilingual children are often not legally defined as immigrants and therefore do not qualify for language assistance at school (which is clearly the case in the Israeli context) and (b) when a child experiences language and communication difficulties upon entering a SL educational system it may very well influence social, emotional, and learning abilities with meaningful consequences that cannot be ignored. This calls for further solutions within clinics and in the school system.
Conclusion
Substantial numbers of bilingual children are referred to SLPs by expert nurses, educational staff, pediatricians, and parents. Yet, they are mostly assessed using monolingual language tests. Parent questionnaires are often used in research settings, to complement missing information on bilingual background and home language, but are seldom used in clinical setting. Our study demonstrated that when looking for an accurate and professional way to assess language abilities among bilingual children in a clinical setting, we should definitely consider using parent questionnaires to complement formal and informal tests as a tool for gathering much needed information regarding the child’s developmental milestones, family history, and HL abilities. Our study showed that a parent questionnaire can distinguish between children identified with DLD and children who were never referred to the clinic. The use of more complex sentences, confidence in speaking freely and higher similarity in language development to other children characterize children who were never referred to the clinic. Our profiling process further showed that clinically referred children who were assessed as having typical language development, were also characterized by the use of more complex sentences, and higher similarity in language development to other children, when compared to children diagnosed with DLD. Moreover, within the clinically referred group, lack of family history highly characterized the children who showed typical language development. As expected, information on the home language distinguished between children with DLD and the other two groups, while information on the societal language did not. Crucially, the questionnaire was not only able to distinguish the groups but also showed good sensitivity and specificity within the Clinically Referred children. These findings show that such questionnaires can provide differential profiles for children both within the clinics and in the non-referred population, yielding better screening and treatment.
Data Availability Statement
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
Ethics Statement
The studies involving human participants were reviewed and approved by the Bar-Ilan University Faculty of Humanities IRB Committee. Written informed consent to participate in this study was provided by the participants’ legal guardian/next of kin.
Author Contributions
HA-O and SA-L contributed equally to the design and implementation of the research, to the analysis of the results and to the writing of the manuscript. HA-O was in charge of data collection and coding. SA-L supervised, supported, and guided this research project from beginning to end. Both authors contributed to the article and approved the submitted version.
Conflict of Interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher’s Note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Acknowledgments
BIPAQ was developed in collaboration with Joel Walters within COST Action IS0804 “Language Impairment in a Multilingual Society: Linguistic Patterns and the Road to Assessment (http://www.bi-sli.org)”. We would like to acknowledge German-Israel Foundation-GIF 1113/2010, Israel Science Foundation-ISF 779/10 and the Israeli Speech and Hearing Association (ISHLA) for supporting part of the data collection.
Supplementary Material
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/feduc.2022.846111/full#supplementary-material
Footnotes
References
Abbas, H., Garberson, F., Glover, E., and Wall, D. P. (2017). “Machine learning for early detection of autism (and other conditions) using a parental questionnaire and home video screening,” in Proceedings of the 2017 IEEE International Conference on Big Data (Big Data). (Piscataway, NJ: IEEE). doi: 10.1109/BigData.2017.8258346
Abutbul-Oz, H., Armon-Lotem, S., and Walters, J. (2012), BIPAQ- Bilingual Parent Questionnaire. Israel: Bar-Ilan University.
Altman, C., Harel, E., Meir, N., Iluz-Cohen, P., Walters, J., and Armon-Lotem, S. (2021). Using a monolingual screening test for assessing bilingual children. Clin. Linguistics Phonet. Online ahead of print doi: 10.1080/02699206.2021.2000644
American Psychiatric Association (2013). DSM 5 Diagnostic and Statistical Manual of Mental Disorders. Virginia, VA: American Psychiatric Association.
Andrijic, V., Bayer, J., and Bretherton, L. (2013). Validity of the children’s moods, fears and worries questionnaire in a clinical setting. Child Adolescent Mental Health 18, 11–17. doi: 10.1111/j.1475-3588.2012.00655.x
Armon-Lotem, S., and Meir, N. (2016). Diagnostic accuracy of repetition tasks for the identification of specific language impairment (SLI) in bilingual children: evidence from Russian and Hebrew. Int. J. Lang. Commun. Disord. 51, 715–731 doi: 10.1111/1460-6984.12242
Armon-Lotem, S., and Ohana, O. (2017). A CDI study of bilingual English-Hebrew children–frequency of exposure as a major source of variation. Int. J. Bilingual Educ. Bilingualism 20, 201–217. doi: 10.1080/13670050.2016.1179257
Armon-Lotem, S., Rose, K., and Altman, C. (2021). The development of English as a heritage language: the role of chronological age and age of onset of bilingualism. First Lang. 41, 67–89. doi: 10.1177/0142723720929810
ASHA (2004). Knowledge and Skills Needed by Speech-language Pathologists and Audiologists to Provide Culturally and Linguistically Appropriate Services. ASHA Supplement 24. Rockville, MD: ASHA
Bedore, L., Pena, E., Summers, C., Boerger, K., Resendiz, M., Greene, K., et al. (2012). The measure matters: language dominance profiles across measures in Spanish English bilingual children. Bilingualism: Lang. Cogn. 15, 616–629. doi: 10.1017/S1366728912000090
Bishop, D. V. (2006). What causes specific language impairment in children?. Curr. Direct. Psychol. Sci. 15, 217–221. doi: 10.1111/j.1467-8721.2006.00439.x
Bishop, D. V., and McDonald, D. (2009). Identifying language impairment in children: combining language test scores with parental report. Int. J. Lang. Commun. Disord. 44, 600–615. doi: 10.1080/13682820802259662
Bishop, D. V., Holt, G., Line, E., McDonald, D., McDonald, S., and Watt, H. (2012). Parental phonological memory contributes to prediction of outcome of late talkers from 20 months to 4 years: a longitudinal study of precursors of specific language impairment. J. Neurodev. Disord. 4, 1–12. doi: 10.1186/1866-1955-4-3
Bishop, D. V., Maybery, M., Wong, D., Maley, A., and Hallmayer, J. (2006). Characteristics of the broader phenotype in autism: a study of siblings using the children’s communication checklist-2. Am. J. Med. Genet. Part B: Neuropsychiatric Genet. 141, 117–122. doi: 10.1002/ajmg.b.30267
Bishop, D. V., North, T., and Donlan, C. (1995). Genetic basis of specific language impairment: evidence from a twin study. Dev. Med. Child Neurol. 37, 56–71. doi: 10.1111/j.1469-8749.1995.tb11932.x
Bishop, D. V., Snowling, M. J., Thompson, P. A., Greenhalgh, T., Adams, C., and Boyle, C. (2017). Phase 2 of CATALISE: a multinational and multidisciplinary Delphi consensus study of problems with language development: terminology. J. Child Psychol. Psychiatry 58, 1068–1080. doi: 10.1111/jcpp.12721
Boerma, T., and Blom, E. (2017). Assessment of bilingual children: what if testing both languages is not possible?. J. Commun. Disord. 66, 65–76. doi: 10.1016/j.jcomdis.2017.04.001
Bohman, T. M., Bedore, L. M., Peña, E. D., Mendez-Perez, A., and Gillam, R. B. (2010). What you hear and what you say: language performance in Spanish–English bilinguals. Int. J. Bilingual Educ. Bilingualism 13, 325–344. doi: 10.1080/13670050903342019
Bonifacci, P., Mari, R., Gabbianelli, L., Ferraguti, E., Montanari, F., Burani, F., and Porrelli, M. (2016). Sequential bilingualism and specific language impairment: the Italian version of ALDeQ parental questionnaire. Applied Psychology Bulletin. 64, 50–63.
Boudreau, D. (2005). Use of parent questionnaire in emergent and early literacy assessment of preschool children. Lang. Speech Hear. Services Schools 36:33. doi: 10.1044/0161-1461(2005/004)
Camilleri, B., and Botting, N. (2013). Beyond static assessment of children’s receptive vocabulary: the dynamic assessment of word learning (DAWL). Int. J. Lang. Commun. Disord. 48, 565–581. doi: 10.1111/1460-6984.12033
Camilleri, B., and Law, J. (2007). Assessing children referred to speech and language therapy: static and dynamic assessment of receptive vocabulary. Adv. Speech Lang. Pathol. 9, 312–322. doi: 10.1080/14417040701624474
Conti-Ramsden, G., Simkin, Z., and Botting, N. (2006). The prevalence of autistic spectrum disorders in adolescents with a history of specific language impairment (SLI). J. Child Psychol. Psychiatry 47, 621–628. doi: 10.1111/j.1469-7610.2005.01584.x
Dockrell, J. E. (2001). Assessing language skills in preschool children. Child Psychol. Psychiatry Rev. 6, 74–85. doi: 10.1017/S1360641701002532
Dunn, G. (2014). “Statistics in psychiatry,” in International Encyclopedia of Statistical Science ed M. Loveric (California, CA: Arnold).
Fenson, L., Dale, P. S., Reznick, J. S., Bates, E., Thal, D. J., Pethick, S. J., et al. (1994). Variability in early communicative development. Monogr. Soc. Res. Child Dev. 59:1-173; discussion 174-85
Fenson, L., Dale, P. S., Reznick, J. S., Thal, D., Bates, E., Hartung, J., et al. (1993). Guide and Technical Manual for the MacArthur Communicative Development Inventories. San Diego, CA: Singular Press.
Gatt, D. (2017). Bilingual vocabulary production in young children receiving maltese-dominant exposure: individual differences and the influence of demographic and language exposure factors. Int. J. Bilingual Educ. Bilingualism 20, 163–182. doi: 10.1080/13670050.2016.1179255
Genesee, F., and Nicoladis, E. (2007). “Bilingual first language acquisition,” in Blackwell Handbook of Language Development, eds E. Hoff and M. Shatz (West Sussex: Wiley–Blackwell), 324–342.
Gillam, R. B., Peña, E. D., Bedore, L. M., Bohman, T. M., and Mendez-Perez, A. (2013). Identification of specific language impairment in bilingual children: I. assessment in English. J. Speech Lang. Hear. Res. 56, 1813–1823 doi: 10.1044/1092-4388(2013/12-0056)
Grimm, A., and Schulz, P. (2014). Specific language impairment and early second language acquisition: the risk of over-and underdiagnosis. Child Indicators Res. 7, 821–841. doi: 10.1007/s12187-013-9230-6
Gutiérrez-Clellen, V. F., and Peña, E. (2001). Dynamic assessment of diverse children: a tutorial. Lang. Speech Hear. Services Schools 32, 212–224. doi: 10.1044/0161-1461(2001/019)
Hajian-Tilaki, K. (2013). Receiver operating characteristic (ROC) curve analysis for medical diagnostic test evaluation. Caspian J. Int. Med. 4:627
Hasson, N., and Botting, N. (2010). Dynamic assessment of children with language impairments: a pilot study. Child Lang. Teach. Therapy 26, 249–272. doi: 10.1177/0265659009349982
Hasson, N., and Joffe, V. (2007). The case for dynamic assessment in speech and language therapy. Child Lang. Teach. Therapy 23, 9–25 doi: 10.1177/0265659007072142
Hong, S., and Yim, D. (2020). Discriminant analysis of assessment tools in identifying language impairment in Korean-English bilingual children. Commun. Sci. Disorders 25, 531–545. doi: 10.12963/csd.20724
Iluz-Cohen, P. (2008). Language Proficiency, Language Control and Executive Control in Bilingual Children. Israel: Bar-Ilan University. Unpublished undergraduate thesis
International Association of Logopedics and Phoniatrics [IALP] (2020). Common Questions by Speech and Language Therapists Speech-Language Pathologists about Bilingual Multilingual Children and Informed, Evidence-based Answers. Available online at: https://ialpasoc.info/wp-content/uploads/2017/10/FAQ_ENGLISH_Common-Questions-by-Parents-and-Caregivers-of-Billingual-Multilingual-Children-and-Informed-Evidence-Based-Answers.pdf
Johnson, L. L., Bradley, S. J., Birkenfeld-Adams, A. S., Kuksis, M. A. R., Maing, D. M., Mitchell, J. N., et al. (2004). A parent-report gender identity questionnaire for children. Arch. Sex. Behav. 33, 105–116. doi: 10.1023/B:ASEB.0000014325.68094.f3
Kapantzoglou, M., Restrepo, M. A., and Thompson, M. S. (2012). Dynamic assessment of word learning skills: identifying language impairment in bilingual children. Lang. Speech Hear. Serv. Schools 43, 81–96 doi: 10.1044/0161-1461(2011/10-0095)
Karimijavan, G., Ebadi, A., Yadegari, F., Dastjerdi Kazemi, M., Darouie, A., and Karimi, S. E. (2021). Sequential bilingualism and language impairment: the persian version of ALDeQ parental questionnaire. Early Child Dev. Care 191, 815–826. doi: 10.1080/03004430.2019.1647192
Kašćelan, D., Prévost, P., Serratrice, L., Tuller, L., Unsworth, S., and De Cat, C. (2021). A review of questionnaires quantifying bilingual experience in children: do they document the same constructs?. Bilingualism: Lang. Cogn. 1–13. doi: 10.1017/S1366728921000390
Katzenberger, I., and Meilijson, S. (2018). ‘Language assessment of Hebrew-speaking children aged 6-9 years old: a comparison between typically developing children and children with specific language-learning impairment’, DaSH BaReShet. Israeli J. Speech Hear. Swallow. Acquisition Lang. Commun. 36, 51–74.
Katzenberger, I., and Meilijson, S. (2014). ‘Hebrew language assessment measure for preschool children: a comparison between typically developing children and children with specific language impairment’. Lang. Test. 31, 19–38 doi: 10.1177/0265532213491961
Kim, E. Y., and Sung, I. K. (2007). The ages and stages questionnaire: screening for developmental delay in the setting of a pediatric outpatient clinic. Korean J. Pediatrics 50, 1061–1066.
Klee, T., Pearce, K., and Carson, D. K. (2000). Improving the positive predictive value of screening for developmental language disorder. J. Speech Lang. Hear Res. 43, 821–833. doi: 10.1044/jslhr.4304.821
Lee, J. C., Nopoulos, P. C., and Tomblin, J. B. (2020). Procedural and declarative memory brain systems in developmental language disorder (DLD). Brain Lang. 205:104789. doi: 10.1016/j.bandl.2020.104789
Lotem-Armon, S. (2010). Instructive bilingualism: can bilingual children with specific language impairment rely on one language in learning a second one? Appl. Psycholinguistics 31, 253–260 doi: 10.1017/s0142716409990385
Marchman, V. A., Martínez-Sussmann, C., and Dale, P. S. (2004). The language-specific nature of grammatical development: evidence from bilingual language learners. Dev. Sci. 7, 212–224. doi: 10.1111/j.1467-7687.2004.00340.x
Marchman, V., and Martínez-Sussman, C. (2002). Concurrent validity of caregiver/parent report measures of language for children who are learning both English and Spanish. J. Speech Lang. Hear Res. 45, 983–997 doi: 10.1044/1092-4388(2002/080)
Mattila, M. L., Jussila, K., Linna, S. L., Kielinen, M., Bloigu, R., Kuusikko-Gauffin, S., et al. (2012). Validation of the Finnish Autism Spectrum Screening Questionnaire (ASSQ) for clinical settings and total population screening. J. Autism. Dev. Disord. 42, 2162–2180. doi: 10.1007/s10803-012-1464-5
Meir, N., Walters, J., and Armon-Lotem, S. (2016). Disentangling SLI and bilingualism using sentence repetition tasks: the impact of L1 and L2 properties. Int. J. Bilingualism 20, 421–452 doi: 10.1177/1367006915609240
Ministry of Health (n.d.). Speech and Language Pathology in Child Development Available online at: https://www.health.gov.il/Subjects/KidsAndMatures/child_development/professionals/Pages/ST.aspx
Nayeb, L., Lagerberg, D., Sarkadi, A., Salameh, E. K., and Eriksson, M. (2021). Identifying language disorder in bilingual children aged 2.5 years requires screening in both languages. Acta Paediatrica 110, 265–272. doi: 10.1111/apa.15343
Norbury, C. F., Gooch, D., Wray, C., Baird, G., Charman, T., Simonoff, E., et al. (2016). The impact of nonverbal ability on prevalence and clinical presentation of language disorder: evidence from a population study. J. Child Psychol. Psychiatry 57, 1247–1257. doi: 10.1111/jcpp.12573
Nordahl-Hansen, A., Kaale, A., and Ulvund, S. E. (2013). Inter-rater reliability of parent and preschool teacher ratings of language in children with autism. Res. Autism Spectrum Disord. 7, 1391–1396. doi: 10.1016/j.rasd.2013.08.006
Novogrodsky, R. and Kreiser, V. (2019). “Children with developmental language disorders (DLD) in israel - assessment and intervention,” in The Theory and Practice of Managing the Child with Language Impairment- Across Europe and Beyond, eds J. Law, C., Murphy, C., McKean, and E., Thordardottir (Abingdon-on-Thames: Routledge Publication). doi: 10.4324/9780429455308
O’Toole, C., and Hickey, T. M. (2017). Bilingual language acquisition in a minority context: using the Irish–English communicative development inventory to track acquisition of an endangered language. Int. J. Bilingual Educ. Bilingualism 20, 146–162. doi: 10.1080/13670050.2016.1179256
O’Toole, C., Gatt, D., Hickey, T. M., Miȩkisz, A., Haman, E., Armon-Lotem, S., et al. (2017). Parent report of early lexical production in bilingual children: a cross-linguistic CDI comparison. Int. J. Bilingual Educ. Bilingualism 20, 124–145. doi: 10.1080/13670050.2016.1179258
Paradis, J. (2005). Grammatical morphology in children learning English as a second language: implications of similarities with specific language impairment. Lang. Speech Hear. Serv. Sch. 36, 172–187 doi: 10.1044/0161-1461(2005/019)
Paradis, J. (2009). Oral Language Development in French and English and the Role of Home Input Factors. Edmonton, EDM: Conseil Scolarie Centre-Nord.
Paradis, J. (2010). The interface between bilingual development and specific language impairment. keynote article for special issue with peer commentaries. Appl. Psycholinguistics 31, 3–28. doi: 10.1017/S0142716409990373
Paradis, J. (2011). Individual differences in child English second language acquisition: comparing child-Internal and child-external factors. Linguistic Approaches Bilingualism 1, 213–237. doi: 10.1075/lab.1.3.01par
Paradis, J., and Genesee, F. (1996). Syntactic acquisition in bilingual children: autonomous or interdependent? Stud. Second Lang. Acquisition 18, 1–25. doi: 10.1017/S0272263100014662
Paradis, J., Crago, M., Genesee, F., and Rice, M. (2003). Bilingual children with specific language impairment: how do they compare with their monolingual peers. J. Speech Lang. Hear. Res. 46, 113–127. doi: 10.1044/1092-4388(2003/009)
Paradis, J., Emmerzael, K., and Sorenson Duncan, T. (2010). Assessment of english language learners: using parent report on first language. J. Commun. Disord. 43, 474–497. doi: 10.1016/j.jcomdis.2010.01.002
Paradis, J., Rice, M., Crago, M., and Marquis, J. (2008). The acquisition of tense in English: distinguishing child L2 from L1 and SLI. Appl. Psycholinguistics 29, 1–34. doi: 10.1017/S0142716408080296
Paradis, J., Rusk, B., Duncan, T. S., and Govindarajan, K. (2017). Children’s second language acquisition of English complex syntax: the role of age, input, and cognitive factors. Ann. Rev. Appl. Linguistics 37, 148–167. doi: 10.1017/S0267190517000022
Paradis, J., Schneider, P., and Duncan, T. S. (2013). Discriminating children with language impairment among English-language learners from diverse first-language backgrounds. J. Speech Lang. Hear. Res. 56, 971–981 doi: 10.1044/1092-4388(2012/12-0050)
Paradis, J., Tulpar, Y., and Arppe, A. (2016). Chinese L1 children’s English L2 verb morphology over time: individual variation in long-term outcomes. J. Child Lang. 43, 553–580. doi: 10.1017/S0305000915000562
Peña, E. D., Gillam, R. B., Malek, M., Ruiz-Felter, R., Resendiz, M., Fiestas, C., et al. (2006). Dynamic assessment of school-age children’s narrative ability: an experimental investigation of classification accuracy. J Speech Lang Hear Res. 49, 1037–1057 doi: 10.1044/1092-4388(2006/074)
Peña, E., and Iglesias, A. (1992). The application of dynamic methods to language assessment: a nonbiased procedure. J. Special Educ. 26, 269–280. doi: 10.1177/002246699202600304
Peña, E. D., Bedore, L. M., Lugo-Neris, M. J., and Albudoor, N. (2020). Identifying developmental language disorder in school age bilinguals: semantics, grammar, and narratives. Lang. Assess. Quarterly 2020, 541–558. doi: 10.1080/15434303.2020.1827258
Restrepo, M. A. (1998). Identifiers of predominantly Spanish-speaking children with language impairment. J. Speech Lang. Hear Res. 41, 1398–1411. doi: 10.1044/jslhr.4106.1398
Rice, M. L. (2004). “Growth models of developmental language disorders,” in Developmental Language Disorders: From Phenotypes to Etiologies, Eds M. L. Rice and S. F. Warren (Mahwah, NJ: Lawrence Erlbaum Associates Publishers).
Rice, M. L., Taylor, C. L., and Zubrick, S. R. (2008). Language outcomes of 7-year-old children with or without a history of late language emergence at 24 months. J. Speech Lang. Hear. Res. 51, 394–407. doi: 10.1044/1092-4388(2008/029)
Robnov, D. (2006). Talmidim Olim Be’mosdot Chinuch [Immigrant students in educational institutions]. Israel: Central bureau of Statistics.
Rudolph, J. M. (2017). Case history risk factors for specific language impairment: a systematic review and meta-analysis. Am. J. Speech Lang. Pathol. 26, 991–1010. doi: 10.1044/2016_AJSLP-15-0181
Ruiz-Felter, R., Cooperson, S. J., Bedore, L. M., and Peña, E. D. (2016). Influence of current input– output and age of first exposure on phonological acquisition in early bilingual Spanish–Englishspeaking kindergarteners. Int. J. Lang. Commun. Disord. 51, 368–383. doi: 10.1111/1460-6984.12214
Rydz, D., Srour, M., Oskoui, M., Marget, N., Shiller, M., Birnbaum, R., et al. (2006). Screening for developmental delay in the setting of a community pediatric clinic: a prospective assessment of parent-report questionnaires. Pediatrics 118, e1178–e1186. doi: 10.1542/peds.2006-0466
Scheidnes, M., and Tuller, L. (2016). Assessing successive bilinguals in two languages: a longitudinal look at English-speaking children in France. J. Commun. Disord. 64, 45–61. doi: 10.1016/j.jcomdis.2016.10.001
Tambyraja, S. R., Schmitt, M. B., Farquharson, K., and Justice, L. M. (2017). Home literacy environment profiles of children with language impairment: associations with caregiver- and child-specific factors. Int. J. Lang. Commun. Disord. 52, 238–249. doi: 10.1111/1460-6984.12269
Tasher, D., Rubin, L., Grossman, Z., Grotto, I., Dahan, D., Berlowitz, Y., et al. (2016). Child health care in Israel. J. Pediatr. 177, S107–S115. doi: 10.1016/j.jpeds.2016.04.047
Thal, D. J., O’Hanlon, L., Clemmons, M., and Fralin, L. (1999). Validity of a parent report measure of vocabulary and syntax for preschool children with language impairment. J. Speech Lang. Hear Res. 42, 482–496. doi: 10.1044/jslhr.4202.482
The State Comptroller Report (2016). Ministry of Health – Treatments in the field of Child-development. Available online at: https://www.mevaker.gov.il/he/Reports/Report_587/64b6f5c4-a435-48c2-b62c-d213ec85783c/N205-child.docx
Thordardottir, E. (2015). The relationship between bilingual exposure and morphosyntactic development. Int. J. Speech-lang. Pathol. 17, 97–114. doi: 10.3109/17549507.2014.923509
Thordardottir, E. (2019). Amount trumps timing in bilingual vocabulary acquisition: effects of input in simultaneous and sequential school-age bilinguals. Int. J. Bilingualism 23, 236–255. doi: 10.1177/1367006917722418
Tomblin, J. B., Records, N. L., and Zhang, X. (1996). A system for the diagnosis of specific language impairment in kindergarten children. J. Speech Lang. Hear Res. 39, 1284–1294. doi: 10.1044/jshr.3906.1284
Tomblin, J. B., Records, N. L., Buckwalter, P. R., Zhang, X., Smith, E., and O’Brien, M. (1997). Prevalence of specific language impairment in kindergarten children. J. Speech Lang. Hear Res. 40, 1245–1260. doi: 10.1044/jslhr.4006.1245
Tuller, L. (2015). “Clinical use of parental questionnaires in multilingual contexts,” in Assessing Multilingual Children eds S. Armon-Lotem, J. de Jong, and N. Meir (Bristol: Disentangling bilingualism from language impairment).
Vygotsky, L. S. (1978). Mind in Society: Development of Higher Psychological Processes. Cambridge, MA: Harvard university press.
Keywords: DLD, bilingual children, clinical setting, parent questionnaire, diagnosis protocol, language profile
Citation: Abutbul-Oz H and Armon-Lotem S (2022) Parent Questionnaires in Screening for Developmental Language Disorder Among Bilingual Children in Speech and Language Clinics. Front. Educ. 7:846111. doi: 10.3389/feduc.2022.846111
Received: 30 December 2021; Accepted: 02 May 2022;
Published: 13 June 2022.
Edited by:
Alexandra Prentza, University of Ioannina, GreeceReviewed by:
Juan-José Navarro, University of Seville, SpainAngela Grimm, Goethe University Frankfurt, Germany
Stanislava Antonijevic-Elliott, National University of Ireland Galway, Ireland
Copyright © 2022 Abutbul-Oz and Armon-Lotem. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Hadar Abutbul-Oz, hadaroz.keshet@gmail.com