 Kristian Egebjerg1*
Kristian Egebjerg1* Cecilie Dupont Harwood2
Cecilie Dupont Harwood2 Nina Claire Woller3
Nina Claire Woller3 Claus Andrup Kristensen1Morten Mau-Sørensen1
Claus Andrup Kristensen1Morten Mau-Sørensen1- 1Department of Oncology, Copenhagen University Hospital, Rigshospitalet, Copenhagen, Denmark
- 2Department of Otorhinolaryngology, Head & Neck Surgery and Audiology, Copenhagen University Hospital, Rigshospitalet, Copenhagen, Denmark
- 3Department of Pathology, Copenhagen University Hospital, Rigshospitalet, Copenhagen, Denmark
Background: HER2 aberrations in salivary gland carcinomas (SGC) as well as benefit of HER2 directed therapy have been reported in small studies. However, reliable estimates of the prevalence of HER2 positivity in SGC and its various histological subtypes are lacking.
Objective: To assess the prevalence of HER2 positivity in histological subtypes of salivary gland carcinomas (SGC).
Methods: Studies were identified by a systematic review of the literature. Data on in situ hybridization (ISH) and immunohistochemistry (IHC) were extracted to derive pooled prevalence estimates calculated by a random effects model. Characteristics of the studies were extracted for subgroup analysis.
Results: Fifty studies including 3372 patients were identified, providing data on sixteen histological subtypes. Based on the meta-analysis, the estimated prevalence of HER2 positivity were 43% (95% CI: 36% – 51%) in salivary duct carcinoma (SDC), 39% (95% CI: 32% – 45%) in carcinoma ex pleomorphic adenoma (CEP), 17% (95% CI: 7.5% – 33%) in squamous cell carcinoma (SCC), 13% (95% CI: 7.6% – 21%) in adenocarcinoma NOS (ADC), 6.7% (95% CI: 0.17%-32%) in poorly differentiated carcinoma, 5.5% (95% CI: 2.9% – 9.6%) in mucoepidermoid carcinoma, 4.3% (95% CI: 1.4% – 13%) in myoepithelial carcinoma, 1.8% (95% CI: 0.04%-9.6%) in epithelial-myoepithelial carcinoma, 0.45% (95% CI: 0.0097% – 18%) in acinic cell carcinoma and 0.15% (0.037% – 5.4%) in adenoid cystic carcinoma. Estimates for five additional subtypes were assessed.
Conclusion: Prevalence of HER 2 positivity in SGC varies greatly based on histological subtype, with SDC, CEP, SCC, and ADC displaying the highest rates.
Introduction
Salivary gland carcinomas (SGC) are relatively rare tumors with an annual worldwide incidence of 0.07% corresponding to 52,799 cases each year according to the Global Cancer Observatory (1). The most recent WHO classification divide SGC into 21 histological subtypes (2). The incidence of the most common histopathological subtypes vary between countries, but mucoepidermoid carcinoma is the most prevalent subtype making up 12%-29% of the total cases, adenoid cystic carcinomas accounts for 10%-22%, acinic cell carcinoma for 8%-14%, while salivary duct carcinomas (SDC) only account for 5%-10%. SDC represents the most aggressive type (3–5). The prognosis of metastasizing SGC remains poor, and response rates to chemotherapy are modest (4). Consequently, oncologists and patients alike are faced with a clear unmet medical need for improvements in the treatment of this disease (6).
HER2 is a human epidermal receptor 2 tyrosine kinase of the epidermal growth factor receptor (EGFR) class coded by an oncogene ERBB2 located on chromosome 17. HER2 is overexpressed in various subtypes of SGC, but clinical trials on HER2 targeted therapy with trastuzumab or lapatanib without chemotherapy in SGC have failed to show significant clinical benefit, maybe because only a subset of the lapatinib treated patients harbored tumors with HER2 overexpression (7, 8). However, a Japanese study combining trastuzumab and docetaxel found an overall response rate of 70% in patients with HER2 positive SDC defined as IHC3+ or gene amplification by FISH (9). Recently, novel HER2 targeted therapies such as ado-trastuzumab emtansine and combinations of trastuzumab and pertuzumab have reached relevant response rate of 90% and 60%, respectively (10, 11).
HER2 protein overexpression is measured semi-quantitatively by immunohistochemistry (IHC) and gene amplification is measured by fluorescence/silver/dual in situ hybridization (FISH, SISH and DISH). Various scoring systems exist for other cancer types, such as breast carcinoma and gastric esophageal adenocarcinoma (12, 13). Although specific criteria for SGC have been proposed, the breast cancer carcinoma criteria are the most commonly used for scoring HER2 expression in SGC (14). This is partially due to morphological similarities to invasive ductal carcinoma of the breast and molecular resemblance with apocrine breast cancer and because studies validating HER2 scoring systems in SGC are lacking (15).
HER2 overexpression or gene amplification seems to be a prerequisite for response to trastuzumab. Currently there is no systematic review or meta-analysis investigating the prevalence of HER2 in SGC. The aims of this review and meta-analysis are to evaluate the literature and provide prevalence estimates for HER2 in various histological subtypes of SGC.
Methods
PRISMA Reporting guidelines were used.
Eligibility
Inclusion Criteria: Only studies examining human SGC tissue were included. Studies allowed were clinical trials, prospective and retrospective observational studies provided the study population was not a preselected HER2 positive cohort. HER2 status had to be evaluated by either IHC reporting semi-quantitative scores of 0, 1+, 2+, 3+ or quantitative ratios of HER2 gene copy number relative to chromosome 17 by ISH or by both IHC and ISH. Studies reporting HER2 status dichotomously (HER2 positive/negative) using the above mentioned semi-quantitative or quantitative data were eligible.
Exclusion criteria: Studies not listing which quantitative scoring methods of IHC 0 to 3+ or ISH were used to define HER2 positivity were not included. Studies not discriminating between histological subtype and HER2 status were not included. If the same dataset of patients was reported by the same author in two different publications only the newest was included. Studies reported in languages other than English, unpublished studies, case studies, conference abstracts, cell line and animal studies were all considered ineligible.
Rationale for criteria: The above-mentioned inclusion criteria were chosen to gather sufficient data to evaluate HER2 positivity in specific histological subtypes, and to assess whether criteria of HER2 positivity affect the prevalence estimates.
Identifying Studies
PubMed, Embase, Web of Science were searched up to September 19th, 2020 using the search string ((salivary gland tumor[Title/Abstract] OR carcinoma of the salivary gland[Title/Abstract] OR salivary gland cancer[Title/Abstract])) AND (HER2 or c-ERB2). The search syntaxes were adapted to those used by each respective search engine. All time periods were included. Exact search-syntax used for each search engine can be seen in Supplemental S2. No limitations were set regarding the date of coverage. In addition, hand searching of references list of obtained articles was conducted.
Study Selection Process
Titles were identified by the above-mentioned search strategy, screened and assessed for inclusion in the final meta-analysis independently by KE and CDH. Discrepancies were solved by consensus. A full list of texts screened but not included as well as the reason for exclusion is listed in Supplement S3.
Risk of Bias in the Individual Studies and Across Studies
The eligibility criteria were designed to minimize risk of bias – especially selection bias, across studies.
As the studies included are observational and not randomized controlled trials or interventional in nature, risks of bias were assessed using recommendations from COSMOS-E (Conducting Systematic Reviews and Meta-Analyses of Observational Studies of Etiology) (16).
Information bias was assessed by registering methods potentially affecting how frequently the outcome were registered: Prospectively collected or archival samples, HER2 positivity criteria, IHC assay and ISH probe type. The latter were also treated as confounders together with Geographic Region.
Data Items and Collection
A data extraction form was used to extract equivalent information from each paper. First author, published year, geographical region, prospectively collected or archival samples, HER2 positivity criteria, IHC assay, ISH probe type and ISH type: FISH, DISH, SISH. In addition, number of patients with each histological subtype and number of HER2 positive patients as well as data on, IHC0, IHC1+, IHC2+, IHC3+, and HER2 amplification were collected.
Specification of Endpoints
The following endpoints were predefined:
The primary endpoint was HER2 positivity for each SGC histological subtype. Specific IHC data (0, 1+, 2+, 3+) and gene amplification status was extracted when possible. During the data collection it became clear that this specific data was only available for SDC.
Analysis and Statistics and Synthesis Methods
Studies were included in each respective meta-analysis depending on the available data. Meta-analyses were conducted using a random effects model. The Wilson score interval method was used to calculate confidence intervals. Maximum likelihood estimator was used to estimate between study variance tau2 with the inverse variance method. Generalized linear mixed models were used for pooled prevalence estimates, forest plots were created and sorted based on number of patients included. Whenever sufficient data were available, subgrouping based on HER2 definition was plotted, and subgroup analysis based on probe, assay, geographical region was also conducted.
A threshold of n>60 patients was chosen for each tissue type to conduct meta-analysis, as we believe a lower number of patients would not yield a meaningful meta-analysis.
The Clopper-Pearson interval was used to calculate 95% confidence intervals in tissue types not eligible for inclusion in meta-analysis.
R version 4.0.0 and package meta was used.
HER2 Positivity
Various criteria were employed by studies to characterize tumor tissue as “HER2 positive”, and each study was labelled according to criteria employed. When data on both IHC and FISH status were reported, IHC2+ confirmed by gene amplification or IHC3+ was preferentially defined as HER2 positive.
IHC and FISH Prevalence Among SDC
Data for SDC, both de novo and carcinoma ex pleomorphic adenoma were sufficient to conduct analysis for specific IHC status sand gene amplification. Two studies (17, 18) reported combined estimates of IHC0 and IHC1+; this estimate was divided by two and each half was included in the IHC0 and IHC1+ analysis respectively.
Results
By the indicated method of study selection (Figure 1), 50 studies were identified including a total number of 3,372 patients to study the prevalence of HER2 positivity in SGC (Table 1, full characteristics of studies, Supplemental S1). Archival tissue was used in all studies except one; in this study information about tissue sampling was not available. Nineteen studies were conducted in Europe, 12 studies in the Americas, eight in Asia, two in Oceania and one study conducted in both Europe and the Americas. The following criteria were used in the studies included to define HER2 positivity: (1) IHC2+ or IHC3+, (2) IHC3+, (3) IHC2+ and HER2 amplification assessed by ISH or IHC3+, (4) IHC2+ or IHC3+ or HER2 amplification assessed by ISH, (5) IHC3+ or HER2 amplification assessed by ISH, (6) HER2 amplification assessed by ISH, (7) IHC2+ and ISH or IHC3 and ISH.
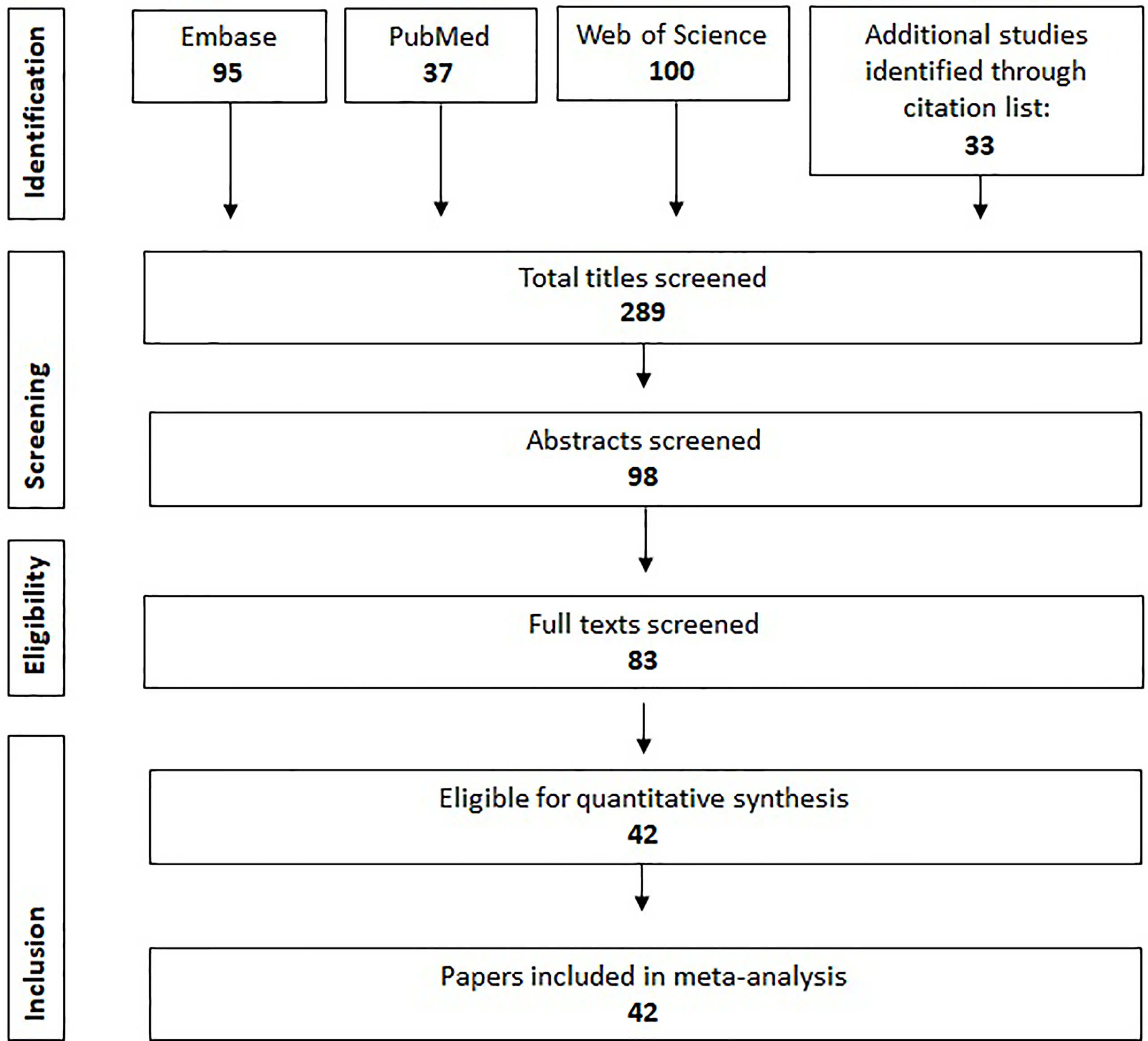
Figure 1 Flowchart describing the methodology of article selection.
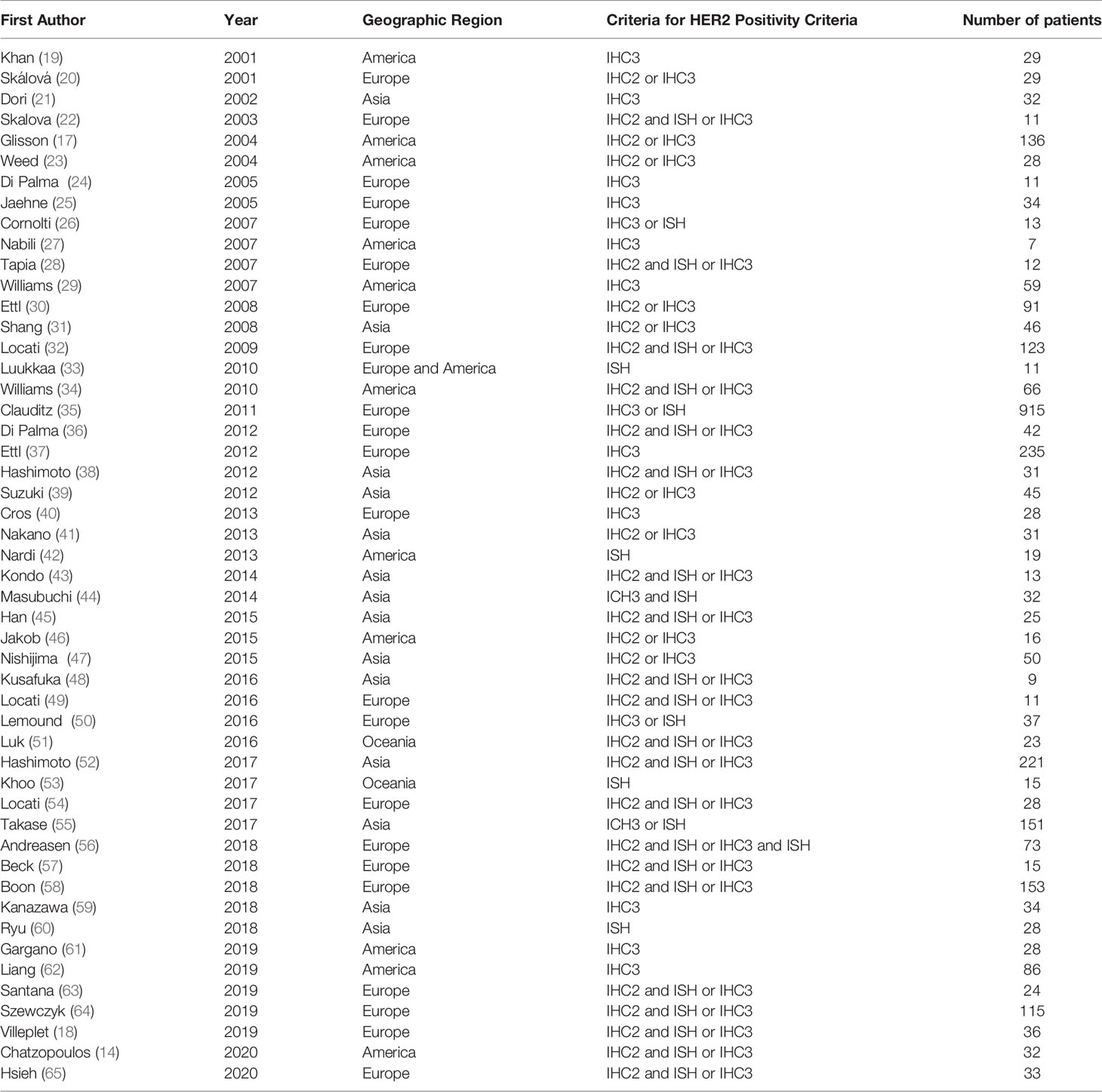
Table 1 Studies included in the meta-analysis.
Salivary Duct Carcinoma: IHC
Eighteen studies were included in the analysis of prevalence of protein expression as assessed by IHC in SDC patients. The estimated prevalence of HER2 scores of IHC0 was 31% (95% CI: 21% - 44%), IHC1+ 10% (95% CI: 6.4% – 15%), IHC2+ 14% (95% CI: 8.9%-20%), and IHC3+ 37% (95% CI: 28%-47%) as presented in Figure 2. There was significant (p<0.01) and marked heterogeneity in the IHC0 and IHC3+ data with I2 of 59% and 67%, respectively, but no significant heterogeneity in the IHC1+ and IHC2+ data. There was significant difference between assays used for all four IHC HER2 scores, for further information see Supplemental S4.
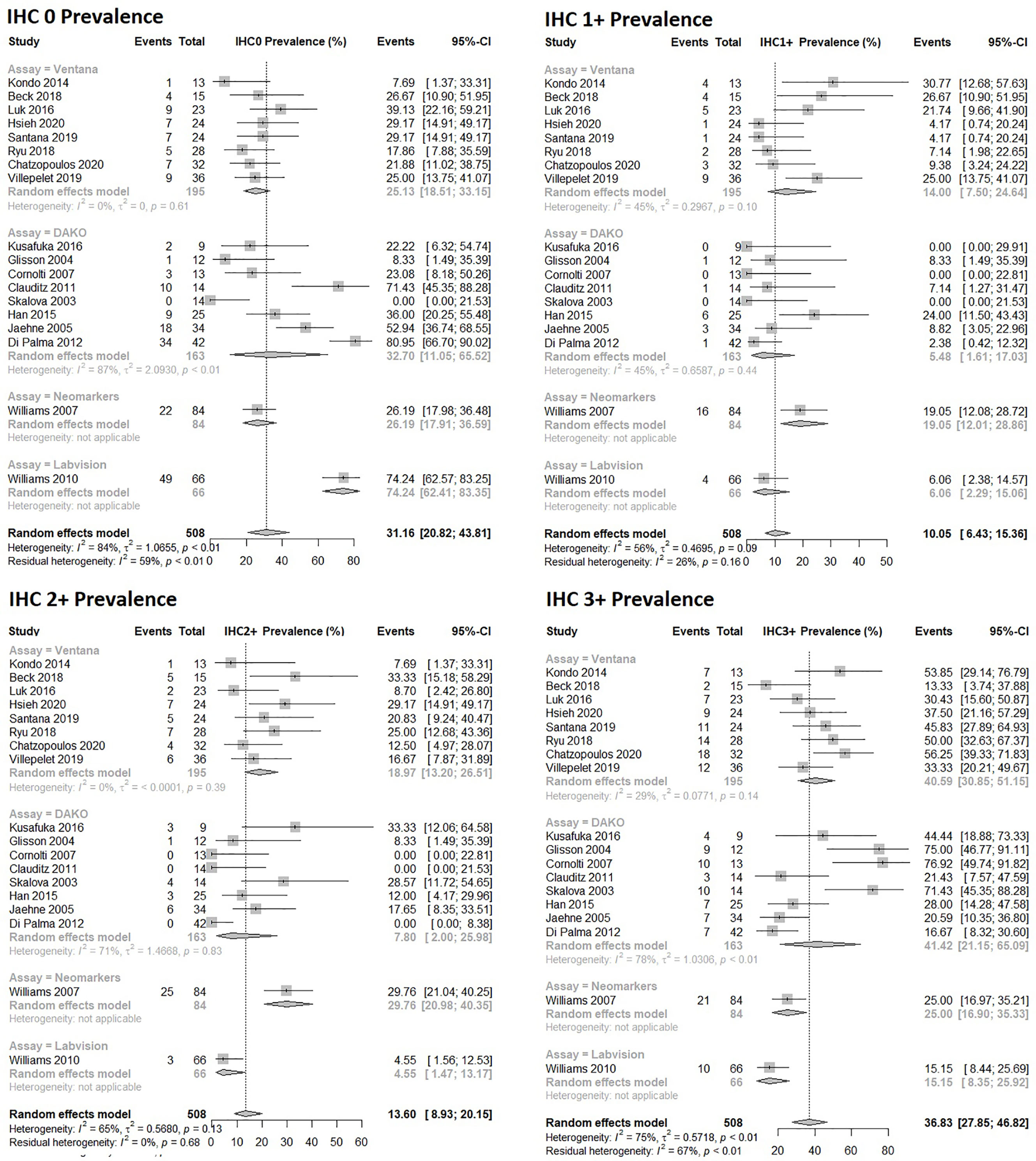
Figure 2 Forrest plot of prevalence estimates for HER2 protein expression assessed by IHC in salivary duct carcinomas.
Salivary Duct Carcinoma: HER2 Gene Amplification
Eighteen studies were included in the analysis. HER2 amplification rate in SDC was found to be 39% (95% CI: 31-49) as shown in Figure 3. There was significant (p<0.01) and marked (I2 66%) heterogeneity between studies. There was no significant difference in the estimated prevalence between studies applying various probes (p=0.12).
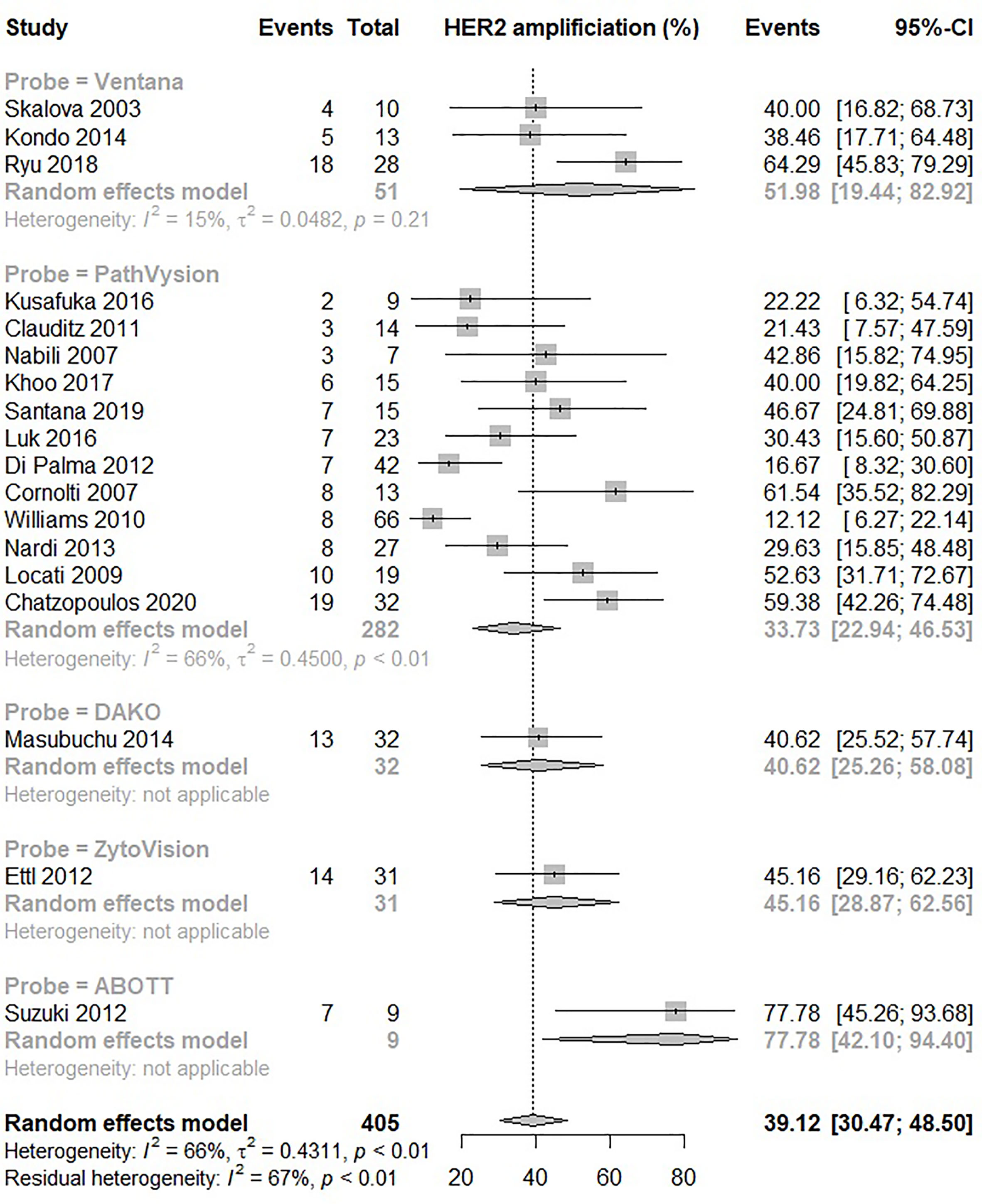
Figure 3 Forrest plot of HER2 gene amplification rate in SDC assessed by in situ hybridization.
Salivary Duct Carcinoma: HER2 Positivity
Thirty-seven studies with a total of 1,105 patients were included in the random effects model. The model predicted a prevalence of HER2 positivity in SDC patients to be 43% (95% CI: 36% – 51%) depicted in Figure 4. The heterogeneity between the studies was significant p<0.01, and substantial, I2 = 80%. There was significant difference between assays p=0.0017, although the differences seemed to level off for the most commonly used assays: Prevalence of 46% (95% CI: 32%- 62%) and 44% (95% CI: 36%- 53%) were estimated for 19 and 11 studies using DAKO and Ventana assays, respectively. Prevalence of less commonly used assays are shown in Supplemental S5.
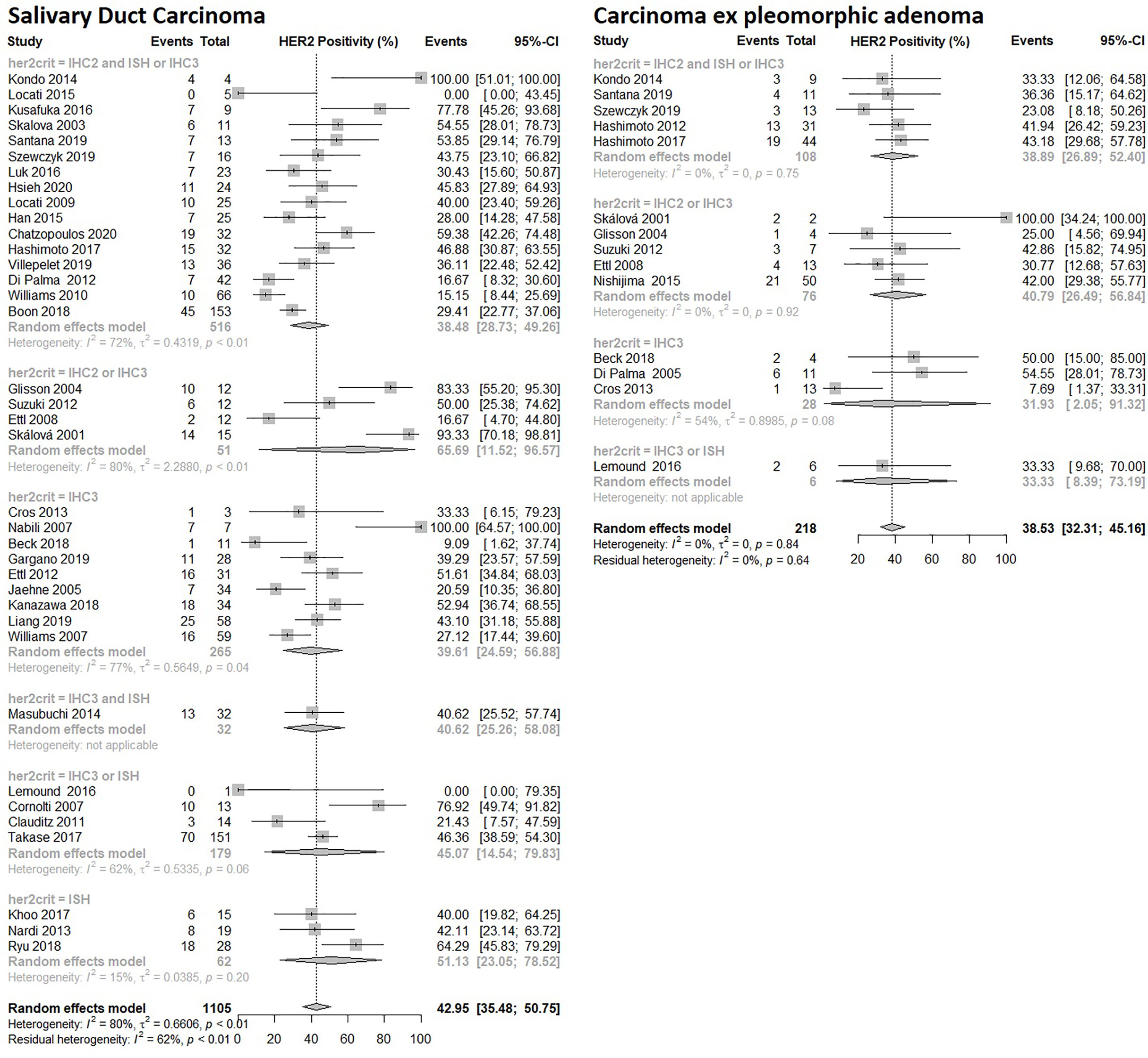
Figure 4 Forrest plot of HER2 Prevalence among SGC subtypes: Salivary Duct Carcinoma and Carcinoma ex pleomorphic adenoma.
There were no differences in the prevalence between studies using varying criteria for HER2 positivity (p=0.61) or conducted in different geographical regions (p=0.16).
Carcinoma Ex Pleomorphic Adenoma (CEP): HER2 Positivity
Fourteen studies were included in the random effects model with a total of 218 patients. The model predicted a prevalence of HER2 positivity in CEP patients to be 39% (95% CI: 32% – 45%) depicted in Figure 4. The heterogeneity between studies was not significant. There were no statistical differences based on the applied criteria for HER2 positivity (p=0.95), used assays (p=0.46) or the geographical regions (p=0.48).
Adenocarcinoma NOS (ADC NOS): HER2 Positivity
Fifteen studies were included in the random effects model with a total of 275 patients. The model predicted a prevalence of HER2 positivity in ADC NOS tumors of 13% (95% CI: 7.6% – 21%) as shown in Figure 5. The heterogeneity between studies was not significant. The prevalence were significantly different when comparing studies using different criteria for HER2 positivity (p=0.0052). However, the estimated prevalence was higher in those studies using the narrowest criteria for HER2 positivity. Neither geographical region (p=0.47) nor assay (p=0.30) used was associated with differences in prevalence.
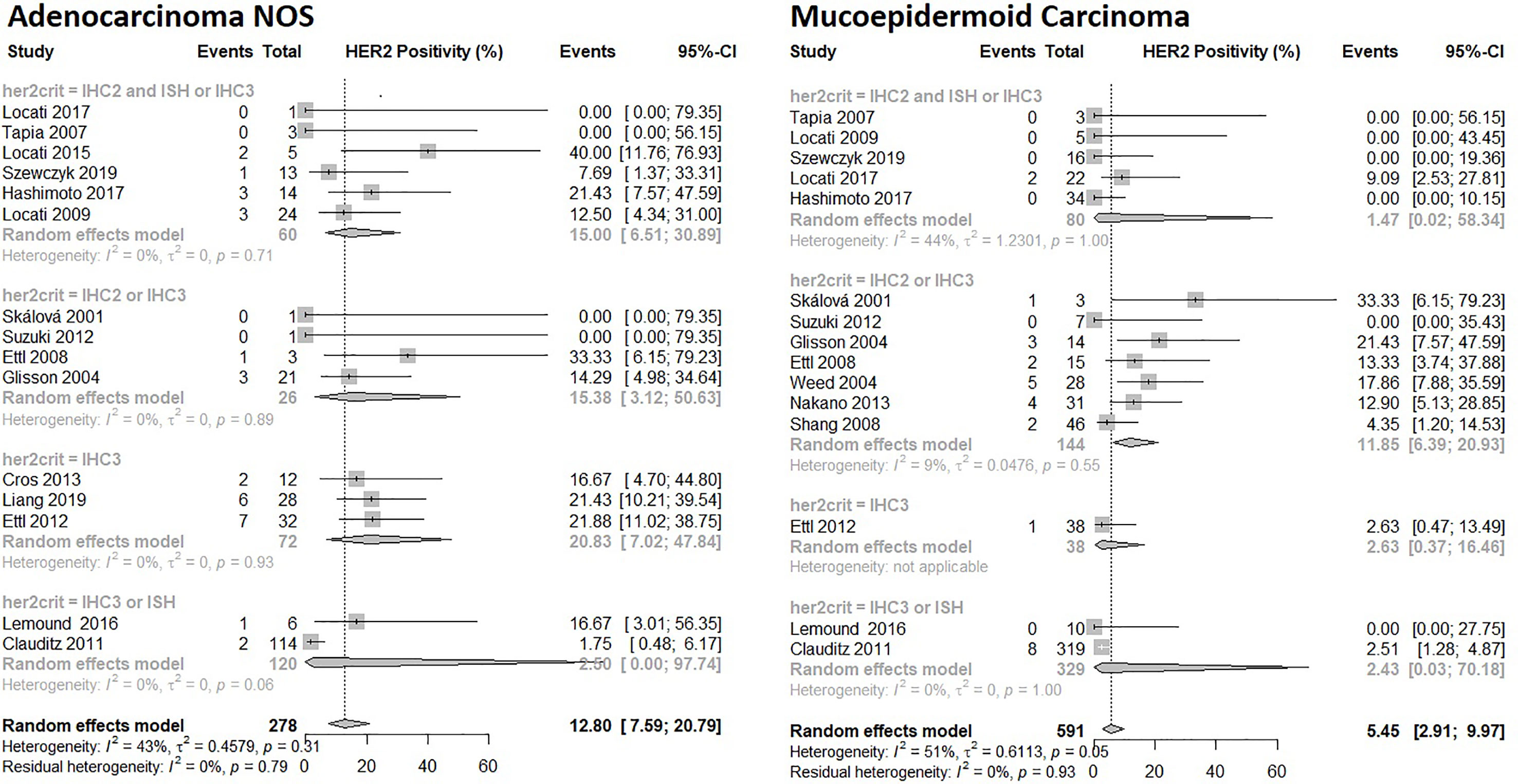
Figure 5 Forrest plot of HER2 Prevalence among SGC subtypes: Adenocarcinoma NOS and Mucoepidermoid Carcinoma.
Mucoepidermoid Carcinoma: HER2 Positivity
Fifteen studies with a total of 591 patients were included in the random effects model. The model predicted a prevalence of HER2 positivity in mucoepidermoid carcinoma patients to be 5.5% (95% CI: 2.9% – 9.6%) as seen in Figure 5. The heterogeneity between studies was moderate I2 = 51% and statistically significant p=0.050. There were significant differences in the prevalence between subgroups based on criteria for HER2 positivity (p=0.0014) and geographical region (p=0.0002). The broadest criteria defining HER2 positivity as IHC2+ and IHC3+ reached prevalence estimates of 12% (95% CI: 6.4% -21%). Two American studies resulted in prevalence estimates by the random effect model of 19% (95% CI: 0.16% – 97%), four Asian studies in prevalence estimates of 4.1 (95% CI: 0.41%-30%) and nine studies from Europe in prevalence estimates of 3.3% (95% CI: 1.8% - 5.9). There was no significant difference between assays used (p=0.56).
Myoepithelial Carcinoma: HER2 Positivity
Nine studies were included in the random effects model with a total of 70 patients. The model predicted a prevalence of HER2 positivity in myoepithelial carcinoma patients to be 4.3% (95% CI: 1.4% – 13%) depicted in Figure 6. The heterogeneity between studies was not statistically significant.
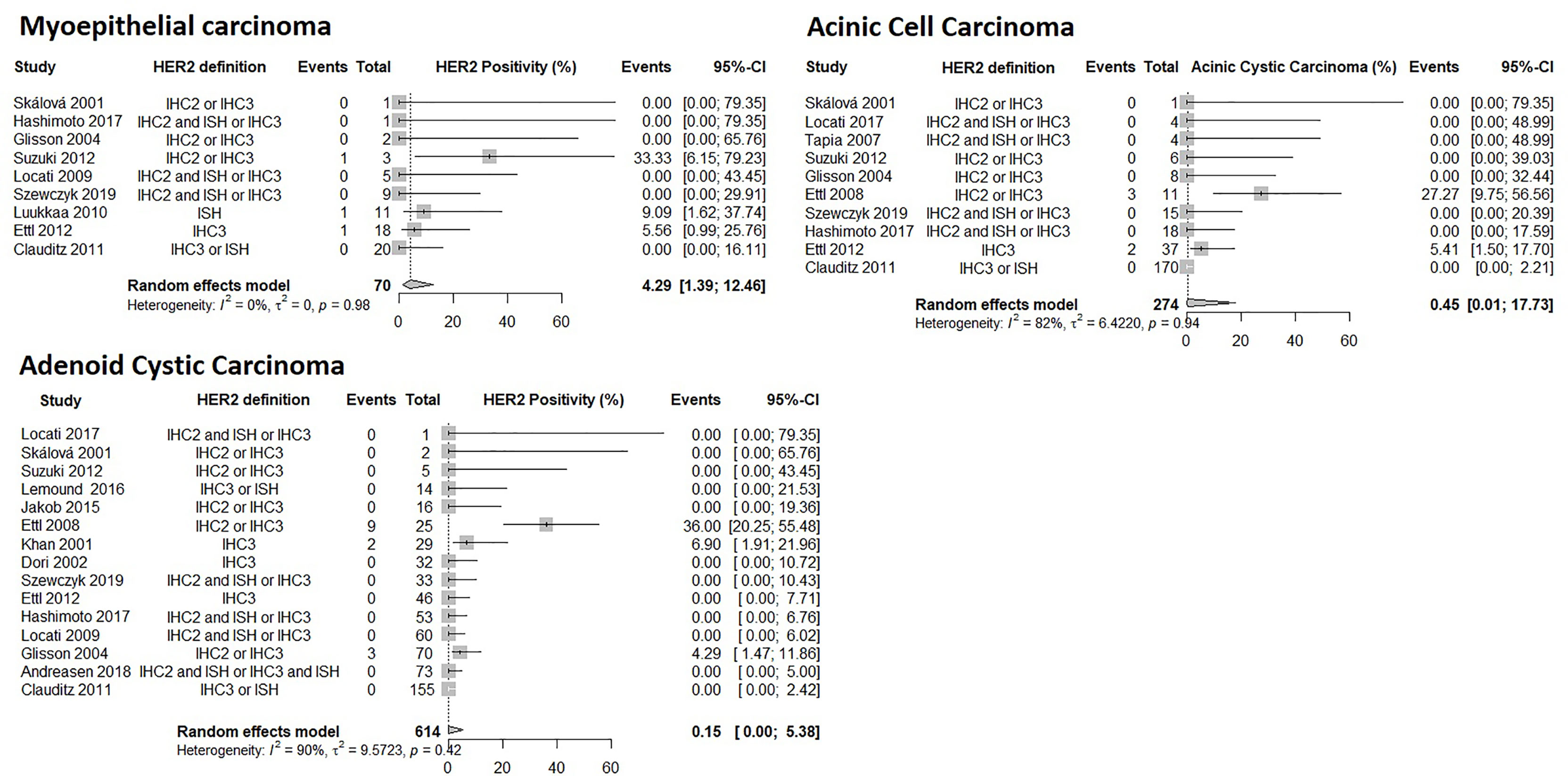
Figure 6 Forrest plot of HER2 Prevalence among SGC subtypes: Myoepithelial carcinoma, Acinic Cell Carcinoma, Adenoid Cystic Carcinoma.
Acinic Cell Carcinoma: HER2 Positivity
Ten studies with 274 patients were included in the random effects model. The model predicted a prevalence of HER2 positivity in acinic cell carcinoma patients to be 0.45% (95% CI: 0.0097% – 18%) depicted in Figure 6. The heterogeneity between studies was not statistically significant but two studies reported prevalence in the range of 5.4% to 27% while 8 studies reported a prevalence of 0%.
Adenoid Cystic Carcinoma: HER2 Positivity
Fifteen studies were included in the random effects model with a total of 614 patients. The model predicted the prevalence of HER2 positivity in adenoid cystic carcinoma patients to be 0.15% (95% CI: 0.037% – 5.4%) depicted in Figure 6. The heterogeneity between studies was not statistically significant but three studies reported prevalence of 4.3%, 6.9% and 36% while 12 studies reported a prevalence of 0%.
HER2 Positivity of Other Histological Subtypes
The low number of patients precluded the conduction of meaningful meta-analysis for the following histological subtypes (Full details of studies in Supplemental S5): For epithelial-myoepithelial carcinoma, 56 patients were included in two studies reporting a single HER2 positive tumor corresponding to a prevalence of 1.8% (95% CI: 0.04%-9.6%).
Seven out of 39 patients with squamous cell carcinoma in five studies had HER2 positive tumor corresponding to a prevalence of 17% (95% CI: 7.5%-33%). For poorly differentiated carcinoma, 15 patients were included in four studies with one HER2 positive tumor corresponding to 6.7% (95% CI: 0.17%-32%).
One study reported on nine patients with intraductal carcinoma with one HER2 positive case corresponding to 11% (95% CI: 0.28% – 48%).
Three studies included 50 patients with polymorphous adenocarcinoma, five studies included 33 patients with basal cell carcinoma, and three studies included 14 patients with oncocytic carcinoma. In all three tumor types, no HER2 positive cases were identified. Two studies reported a total of five patients with lymphoepithelial carcinoma of which zero were HER2 positive.
One study reported one patient with clear cell carcinoma which was not HER2 positive.
Discussion
The present work is the first comprehensive meta-analysis providing reliable estimates of the prevalence of HER2 positivity in salivary gland carcinomas including its histological subtypes. The results are summarized in Tables 2 and 3. Our results show that salivary gland tumors are very heterogeneous with respect to HER2 positivity ranging from 0% up to 43% with the highest prevalence in SDC which both genomically and morphologically resembles invasive ductal carcinoma of the breast (15). Interestingly, similar frequency measures were seen in histologically related tumors, since both SDC and CEP, as well as epithelial-myoepithelial and myoepithelial carcinoma have comparable estimates. Furthermore, a tendency was noted towards increasing frequency of HER2 positivity in tumor types derived from salivary gland ducts compared to tumors with origin from cells with exocrine function. Accordingly, SDC and SCC displayed high prevalence compared to acinic cell carcinomas and adenoid cystic carcinomas with virtually no HER2 expression. Caution should be advised when evaluating the prevalence estimates of rare histological subtypes with small number of patients and no identified HER2 positive cases.
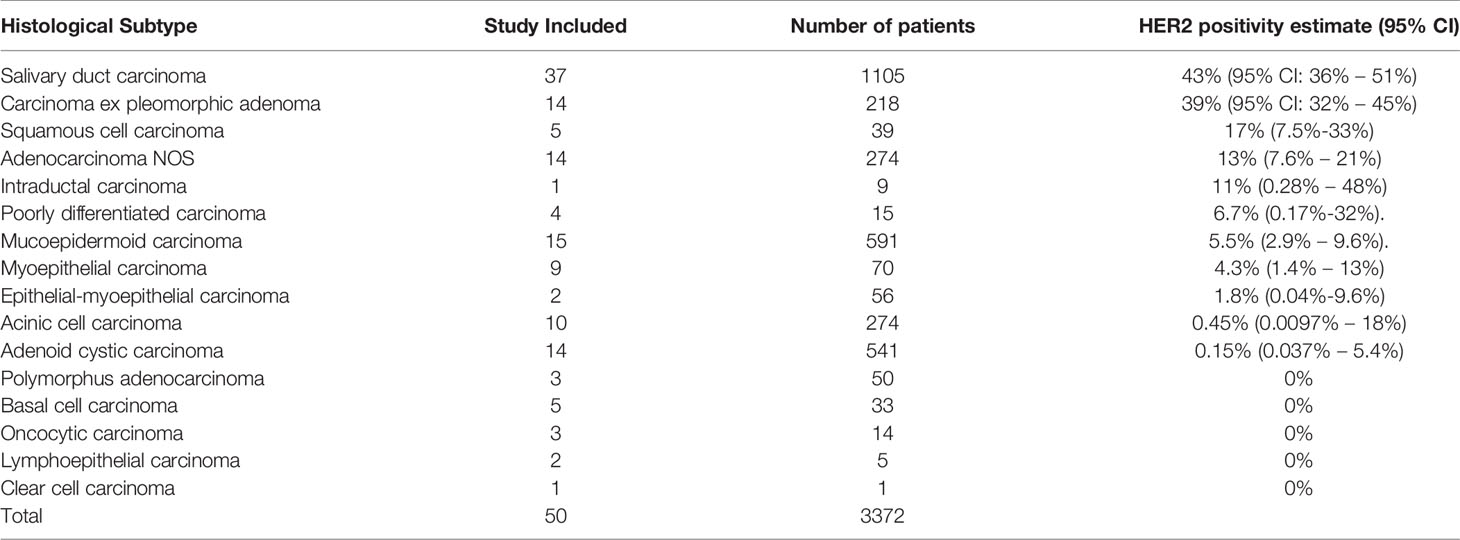
Table 2 Summary of results.

Table 3 Summary of HER2 protein expression assessed by IHC and HER2 amplification assessed by ISH among SDC patients in the meta-analysis.
There was sufficient data in four histological subtypes, SDC, CEP, ADC NOS and mucoepidermoid carcinoma to conduct subgroup analyses of the IHC assay used and its correlation with HER2 prevalence. In three of the subgroup analyses: CEP, ADC NOS and mucoepidermoid carcinoma there was no significant difference between the IHC assays used. However, in SDC there was a significant difference based on the IHC assay used, but no difference between probes used in ISH analysis of HER2 amplification (Figures 2, 3). The difference based on IHC assay used may in part be due to inter-observer variability which is thought to be higher when scoring IHC, compared to ISH scoring which is more objective and quantitative (66). Of note, differences disappeared when comparison was restricted to the two most commonly used IHC assays, DAKO and Ventana. There was similarity in frequency measures in IHC and ISH derived estimates of HER2 positivity and amplification of 43% (95% CI: 36% – 51%) and 39% (95% CI: 31-49) respectively.
The criteria used to define HER2 positivity varied among studies with seven different definitions being employed. Subgroup differences between criteria applied to define HER2 positivity were also analyzed (Figures 4, 5). A significant difference depending on the criteria used was observed in ADC NOS and mucoepidermoid carcinoma, in the latter the broadest definition of HER2 positivity of IHC2+ and IHC3+ also yielded the highest prevalence estimate, but this pattern was not as clear in the ADC NOS subgroup analysis. In subtypes with higher prevalence i.e. SDC and CEP subgroup analyses, use of varying criteria did not seem to result in differences in estimated prevalence. Our estimates are limited by these varying criteria for HER2 positivity used in the included studies.
In recent years, it has become common to use IHC2+ confirmed by ISH or IHC3+ as the definition of HER2 positivity as a threshold for using HER2 targeted therapies. In SGC HER2 is often evaluated by use of a HER2 scoring system developed in breast cancer with the use of a threshold chosen based upon clinical response in patients with breast cancer (67).
Another quite unique application of HER2 testing in SGC is its use in the diagnosis of SDC, since this subtype has a higher prevalence of HER2 overexpression and gene amplification than other subtypes.
There is no generally accepted standard treatment of metastatic SGC, and the role of HER2 targeted therapy in this setting is still unclear. Currently there is not sufficient data on newer HER2 targeted drugs in SGC to further define which patient population benefits from the treatment. As such, defining the specific cut-off value to decide which patients should be regarded as “HER2 positive” to receive HER2 targeted therapy remains to be answered. One step in this direction may be the HER2 scoring criteria for SGC proposed by Chatzopoulos et al. (14).
While HER2 treatment results in survival benefits in breast, gastric and esophageal ADC, only limited data are available in SGC. Single agent HER2 directed therapy antitumor effect in patients with HER2 positive SGC is at best modest (7, 8). Several resistance mechanisms have been proposed for HER2 targeted therapy including HER2 receptors lacking extracellular trastuzumab binding domain, upregulation of other tyrosine kinase receptors or alteration of downstream components resulting in aberrant PI3K/Akt/mTOR pathways (68).
But an exact reason to why response with these drugs seem lower in SGC compared to breast cancer and gastric and esophageal ADC has yet to be found. However, HER2 still remains an important potential target for therapies. Thus, promising strategies have emerged applying dual HER2 blockage with trastuzumab and pertuzumab or combining with chemotherapy (trastuzuamb/docetaxel) or as a drug-antibody-conjugate (ado-trastuzumab-emtasine) (9–11).
In summary, the expression of HER2 in SGC is very heterogeneous between and within histological subtypes. The prevalence of HER2 positivity ranged from 0% to 43% in 3,372 patients with sixteen subtypes of SGC. HER2 positivity was most prevalent in SDC and in some tumor subtypes derived from exocrine cells virtually no HER2 expression was reported. Prospective clinical trials are needed to further evaluate novel HER2 directed therapy and to establish the optimal definition of HER2 positivity based on treatment response in SGC with high prevalence of HER2 positivity.
Data Availability Statement
The original contributions presented in the study are included in the article/Supplementary Material. Further inquiries can be directed to the corresponding author.
Author Contributions
KE and MM-S conceived the project idea. KE and CH reviewed the literature and included studies. KE undertook data analysis. All authors assisted in writing the manuscript and interpreting results. NW, CK, and MM-S provided advice and guidance. All authors contributed to the article and approved the submitted version.
Conflict of Interest
CK has served in advisory boards for MSD, Bristol-Myers Squibb, and Merck Serono. MM-S has served in advisory boards for Roche, Genmab, Bayer, and Karyopharm Therapeutics and received research grants from Karyopharm Therapeutic, Puma Biotechnologies and MSD.
The remaining authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Supplementary Material
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fonc.2021.693394/full#supplementary-material
References
1. Bray F, Ferlay J, Soerjomataram I, Siegel RL, Torre LA, Jemal A. Global Cancer Statistics 2018: GLOBOCAN Estimates of Incidence and Mortality Worldwide for 36 Cancers in 185 Countries. CA: A Cancer J Clin (2018) 68(6):394–424. doi: 10.3322/caac.21492
2. El-Naggar Chan JKC, Grandis JR, Takata T, Slootweg PJ. Who Classification of Head and Neck Tumours, 4th ed, Vol. Vol 9. IARC Publications (2017).
3. Dimas K, Ulukaya E, Sakellaridis N. Salivary Gland Tumors☆. In: Reference Module in Biomedical Sciences. Elsevier (2015). doi: 10.1016/B978-0-12-801238-3.99478-9
4. Son E, Panwar A, Mosher CH, Lydiatt D. Cancers of the Major Salivary Gland. J Oncol Pract (2018) 14(2):99–108. doi: 10.1200/JOP.2017.026856
5. Nakaguro M, Tada Y, Faquin WC, Sadow PM, Wirth LJ, Nagao T. Salivary Duct Carcinoma: Updates in Histology, Cytology, Molecular Biology, and Treatment. Cancer Cytopathol (2020) 128(10):693–703. doi: 10.1002/cncy.22288
6. Wang X, Luo Y, Li M, Yan H, Sun M, Fan T. Management of Salivary Gland Carcinomas - A Review. Oncotarget (2017) 8(3):3946–56. doi: 10.18632/oncotarget.13952
7. Haddad R, Colevas AD, Krane JF, Cooper D, Glisson B, Amrein PC, et al. Herceptin in Patients With Advanced or Metastatic Salivary Gland Carcinomas. A Phase II Study. Oral Oncol (2003) 39(7):724–7. doi: 10.1016/S1368-8375(03)00097-6
8. Agulnik M, Cohen EWE, Cohen RB, Chen EX, Vokes EE, Hotte SJ, et al. Phase II Study of Lapatinib in Recurrent or Metastatic Epidermal Growth Factor Receptor and/or erbB2 Expressing Adenoid Cystic Carcinoma and Non-Adenoid Cystic Carcinoma Malignant Tumors of the Salivary Glands. J Clin Oncol (2007) 25(25):3978–84. doi: 10.1200/JCO.2007.11.8612
9. Takahashi H, Tada Y, Saotome T, Akazawa K, Ojiri H, Fushimi C, et al. Phase II Trial of Trastuzumab and Docetaxel in Patients With Human Epidermal Growth Factor Receptor 2-Positive Salivary Duct Carcinoma. J Clin Oncol (2019) 37(2):125–34. doi: 10.1200/JCO.18.00545
10. Li BT, Shen R, Offin M, Buonocore DJ, Myers ML, Venkatesh A, et al. Ado-Trastuzumab Emtansine in Patients With HER2 Amplified Salivary Gland Cancers (SGCS): Results From a Phase II Basket Trial. J Clin Oncol (2019) 37(15_suppl):6001–1. doi: 10.1200/jco.2019.37.15_suppl.6001
11. Kurzrock R, Bowles DW, Kang H, Meric-Bernstam F, Hainsworth J, Spigel DR, et al. Targeted Therapy for Advanced Salivary Gland Carcinoma Based on Molecular Profiling: Results From MyPathway, a Phase IIa Multiple Basket Study. Ann Oncol (2020) 31:412–21. doi: 10.1016/j.annonc.2019.11.018
12. Wolff AC, Hammond MEH, Allison KH, Harvey BE, McShane LM, Dowsett M. HER2 Testing in Breast Cancer: American Society of Clinical Oncology/College of American Pathologists Clinical Practice Guideline Focused Update Summary. J Oncol Pract (2018) 14(7):437–41. doi: 10.1200/JOP.18.00206
13. Bartley AN, Washington MK, Colasacco C, Ventura CB, Ismaila N, Benson AB, et al. Her2 Testing and Clinical Decision Making in Gastroesophageal Adenocarcinoma: Guideline From the College of American Pathologists, American Society for Clinical Pathology, and the American Society of Clinical Oncology. J Clin Oncol (2017) 35(4):446–64. doi: 10.1200/JCO.2016.69.4836
14. Chatzopoulos K, Collins AR, Sotiriou S, Keeney MG, Visscher DW, Rivera M, et al. Increased ERBB2 Gene Copy Numbers Reveal a Subset of Salivary Duct Carcinomas With High Densities of Tumor Infiltrating Lymphocytes and PD-L1 Expression. Head Neck Pathol (2020) 14.4:1–15. doi: 10.1007/s12105-020-01163-x
15. Dalin MG, Desrichard A, Katabi N, Makarov V, Walsh LA, Lee KW, et al. Comprehensive Molecular Characterization of Salivary Duct Carcinoma Reveals Actionable Targets and Similarity to Apocrine Breast Cancer. Clin Cancer Res (2016) 22(18):4623–33. doi: 10.1158/1078-0432.CCR-16-0637
16. Dekkers OM, Vandenbroucke JP, Cevallos M, Renehan AG, Altman DG, Egger M. Cosmos-E: Guidance on Conducting Systematic Reviews and Meta-Analyses of Observational Studies of Etiology. PloS Med (2019) 16(2):e1002742. doi: 10.1371/journal.pmed.1002742
17. Glisson B, Colevas AD, Haddad R, Krane J, El-Naggar A, Kies M, et al. Her2 Expression in Salivary Gland Carcinomas: Dependence on Histological Subtype. Clin Cancer Res (2004) 10(3):944–6. doi: 10.1158/1078-0432.CCR-03-0253
18. Villepelet A, Lefèvre M, Verillaud B, Janot F, Garrel R, Vergez S, et al. Salivary Duct Carcinoma: A Prospective Multicenter Study of 61 Cases of the Réseau D’expertise Français Des Cancers Orl Rares. Head Neck (2018) 41(3):584–91. doi: 10.1002/hed.25194
19. Khan AJ, Digiovanna MP, Ross DA, Sasaki CT, Carter D, Son YH, et al. Adenoid Cystic Carcinoma: A Retrospective Clinical Review. Int J Cancer (2001) 96(3):149–58. doi: 10.1002/ijc.1013
20. Skálová A, Stárek I, Kuerová V, Szépe P, Plank L. Salivary Duct Carcinoma - a Highly Aggressive Salivary Gland Tumor With HER-2/neu Oncoprotein Overexpression. Pathol Res Pract (2001) 197(9):621–6. doi: 10.1078/0344-0338-00136
21. Dori S, Vered M, David R, Buchner A. HER2/Neu Expression in Adenoid Cystic Carcinoma of Salivary Gland Origin: An Immunohistochemical Study. J Oral Pathol Med (2002) 31(8):463–7. doi: 10.1034/j.1600-0714.2002.00017.x
22. Skálová A, Stárek I, Vanecek T, Kucerová V, Plank L, Szépe P, et al. Expression of HER-2/neu Gene and Protein in Salivary Duct Carcinomas of Parotid Gland as Revealed by Fluorescence in-Situ Hybridization and Immunohistochemistry. Histopathology (2003) 42(4):348–56. doi: 10.1046/j.1365-2559.2003.01600.x
23. Weed DT, Gomez-Fernandez C, Pacheco J, Ruiz J, Hamilton-Nelson K, Arnold DJ, et al. MUC4 and ERBB2 Expression in Major and Minor Salivary Gland Mucoepidermoid Carcinoma. Head Neck (2004) 26(4):353–64. doi: 10.1002/hed.10387
24. Di Palma S, Skálová A, Vanìèek T, Simpson RHW, Stárek I, Leivo I. Non-Invasive (Intracapsular) Carcinoma Ex Pleomorphic Adenoma: Recognition of Focal Carcinoma by HER-2/neu and MIB1 Immunohistochemistry. Histopathology (2005) 46(2):144–52. doi: 10.1111/j.1365-2559.2005.02058.x
25. Jaehne M, Roeser K, Jaekel T, David Schepers J, Albert N, Löning T. Clinical and Immunohistologic Typing of Salivary Duct Carcinoma: A Report of 50 Cases. Cancer (2005) 103(12):2526–33. doi: 10.1002/cncr.21116
26. Cornolti G, Ungari M, Morassi ML, Facchetti F, Rossi E, Lombardi D, et al. Amplification and Overexpression of Her2/neu Gene and HER2/neu Protein in Salivary Duct Carcinoma of the Parotid Gland. Arch Otolaryngol - Head Neck Surg (2007) 133(10):1031–6. doi: 10.1001/archotol.133.10.1031
27. Nabili V, Tan JW, Bhuta S, Sercarz JA, Head CS. Salivary Duct Carcinoma: A Clinical and Histologic Review With Implications for Trastuzumab Therapy. Head Neck (2007) 29(10):907–12. doi: 10.1002/hed.20614
28. Tapia C, Glatz K, Novotny H, Lugli A, Horcic M, Seemayer CA, et al. Close Association Between HER-2 Amplification and Overexpression in Human Tumors of Non-Breast Origin. Mod Pathol (2007) 20(2):192–8. doi: 10.1038/modpathol.3800729
29. Williams MD, Roberts D, Blumenschein GR, Temam S, Kies MS, Rosenthal DI, et al. Differential Expression of Hormonal and Growth Factor Receptors in Salivary Duct Carcinomas: Biologic Significance and Potential Role in Therapeutic Stratification of Patients. Am J Surg Pathol (2007) 31(11):1645–52. doi: 10.1097/PAS.0b013e3180caa099
30. Ettl T, Schwarz S, Kleinsasser N, Hartmann A, Reichert TE, Driemel O. Overexpression of EGFR and Absence of C-KIT Expression Correlate With Poor Prognosis in Salivary Gland Carcinomas. Histopathology (2008) 53(5):567–77. doi: 10.1111/j.1365-2559.2008.03159.x
31. Shang J, Shui Y, Sheng L, Wang K, Hu Q, Wei Q. Epidermal Growth Factor Receptor and Human Epidermal Growth Receptor 2 Expression in Parotid Mucoepidermoid Carcinoma: Possible Implications for Targeted Therapy. Oncol Rep (2008) 19(2):435–40. doi: 10.3892/or.19.2.435
32. Locati LD, Perrone F, Losa M, Mela M, Casieri P, Orsenigo M, et al. Treatment Relevant Target Immunophenotyping of 139 Salivary Gland Carcinomas (Sgcs). Oral Oncol (2009) 45(11):986–90. doi: 10.1016/j.oraloncology.2009.05.635
33. Luukkaa H, Klemi P, Leivo I, Mäkitie AA, Irish J, Gilbert R, et al. Expression of Matrix metalloproteinase-1, -7, -9, -13, Ki-67, and HER-2 in Epithelial-Myoepithelial Salivary Gland Cancer. Head Neck (2010) 32(8):1019–27. doi: 10.1002/hed.21277
34. Williams MD, Roberts DB, Kies MS, Mao L, Weber RS, El-Naggar AK. Genetic and Expression Analysis of HER-2 and EGFR Genes in Salivary Duct Carcinoma: Empirical and Therapeutic Significance. Clin Cancer Res (2010) 16(8):2266–74. doi: 10.1158/1078-0432.CCR-09-0238
35. Clauditz TS, Reiff M, Gravert L, Gnoss A, Tsourlakis MC, Münscher A, et al. Human Epidermal Growth Factor Receptor 2 (HER2) in Salivary Gland Carcinomas. Pathology (2011) 43(5):459–64. doi: 10.1097/PAT.0b013e3283484a60
36. Di Palma S, Simpson RHW, Marchió C, Skálová A, Ungari M, Sandison A, et al. Salivary Duct Carcinomas Can Be Classified Into Luminal Androgen Receptor-Positive, HER2 and Basal-Like Phenotypes. Histopathology (2012) 61(4):629–43. doi: 10.1111/j.1365-2559.2012.04252.x
37. Ettl T, Stiegler C, Zeitler K, Agaimy A, Zenk J, Reichert TE, et al. Egfr, HER2, Survivin, and Loss of pSTAT3 Characterize High-Grade Malignancy in Salivary Gland Cancer With Impact on Prognosis. Hum Pathol (2012) 43(6):921–31. doi: 10.1016/j.humpath.2011.08.006
38. Hashimoto K, Yamamoto H, Shiratsuchi H, Nakashima T, Tamiya S, Nishiyama KI, et al. Her-2/neu Gene Amplification in Carcinoma Ex Pleomorphic Adenoma in Relation to Progression and Prognosis: A Chromogenic In-Situ Hybridization Study. Histopathology (2012) 60(6 B):E131–42. doi: 10.1111/j.1365-2559.2012.04201.x
39. Suzuki S, Dobashi Y, Minato H, Tajiri R, Yoshizaki T, Ooi A. EGFR and HER2-Akt-mTOR Signaling Pathways Are Activated in Subgroups of Salivary Gland Carcinomas. Virchows Arch (2012) 461(3):271–82. doi: 10.1007/s00428-012-1282-3
40. Cros J, Sbidian E, Hans S, Roussel H, Scotte F, Tartour E, et al. Expression and Mutational Status of Treatment-Relevant Targets and Key Oncogenes in 123 Malignant Salivary Gland Tumours. Ann Oncol (2013) 24(10):2624–9. doi: 10.1093/annonc/mdt338
41. Nakano T, Yamamoto H, Hashimoto K, Tamiya S, Shiratsuchi H, Nakashima T, et al. HER2 and EGFR Gene Copy Number Alterations are Predominant in High-Grade Salivary Mucoepidermoid Carcinoma Irrespective of MAML2 Fusion Status. Histopathology (2013) 63(3):378–92. doi: 10.1111/his.12183
42. Nardi V, Sadow PM, Juric D, Zhao D, Cosper AK, Bergethon K, et al. Detection of Novel Actionable Genetic Changes in Salivary Duct Carcinoma Helps Direct Patient Treatment. Clin Cancer Res (2013) 19(2):480–90. doi: 10.1158/1078-0432.CCR-12-1842
43. Kondo Y, Kikuchi T, Esteban JC, Kumaki N, Ogura G, Inomoto C, et al. Intratumoral Heterogeneity of HER2 Protein and Amplification of HER2 Gene in Salivary Duct Carcinoma. Pathol Int (2014) 64(9):453–9. doi: 10.1111/pin.12195
44. Masubuchi T, Tada Y, Maruya Si, Osamura Y, Kamata Se, Miura K, et al. Clinicopathological Significance of Androgen Receptor, HER2, Ki-67 and EGFR Expressions in Salivary Duct Carcinoma. Int J Clin Oncol (2015) 20(1):35–44. doi: 10.1007/s10147-014-0674-6
45. Han MW, Roh JL, Choi SH, Nam SY, Lee HJ, Cho KJ, et al. Prognostic Factors and Outcome Analysis of Salivary Duct Carcinoma. Auris Nasus Larynx (2015) 42(6):472–7. doi: 10.1016/j.anl.2015.04.005
46. Jakob JA, Kies MS, Glisson BS, Kupferman ME, Liu DD, Lee JJ, et al. Phase II Study of Gefitinib in Patients With Advanced Salivary Gland Cancers. Head Neck (2015) 37(5):644–9. doi: 10.1002/hed.23647
47. Nishijima T, Yamamoto H, Nakano T, Nakashima T, Taguchi KI, Masuda M, et al. Dual Gain of HER2 and EGFR Gene Copy Numbers Impacts the Prognosis of Carcinoma Ex Pleomorphic Adenoma. Hum Pathol (2015) 46(11):1730–43. doi: 10.1016/j.humpath.2015.07.014
48. Kusafuka K, Kawasaki T, Maeda M, Yamanegi K, Baba S, Ito Y, et al. Salivary Duct Carcinoma With Rhabdoid Features: A Salivary Counterpart of Pleomorphic Lobular Carcinoma of the Breast. Histopathology (2017) 70(2):164–73. doi: 10.1111/his.12987
49. Locati LD, Perrone F, Cortelazzi B, Lo Vullo S, Bossi P, Dagrada G, et al. Clinical Activity of Androgen Deprivation Therapy in Patients With Metastatic/Relapsed Androgen Receptor-Positive Salivary Gland Cancers. Head Neck (2016) 38(5):724–31. doi: 10.1002/hed.23940
50. Lemound J, Schenk M, Keller G, Stucki-Koch A, Witting S, Kreipe H, et al. Cytogenetic and Immunohistochemical Biomarker Profiling of Therapy-Relevant Factors in Salivary Gland Carcinomas. J Oral Pathol Med (2016) 45(9):655–63. doi: 10.1111/jop.12429
51. Luk PP, Weston JD, Yu B, Selinger CI, Ekmejian R, Eviston TJ, et al. Salivary Duct Carcinoma: Clinicopathologic Features, Morphologic Spectrum, and Somatic Mutations. Head Neck (2016) 38:E1838–47. doi: 10.1002/hed.24332
52. Hashimoto K, Hayashi R, Mukaigawa T, Yamazaki M, Fujii S. Concomitant Expression of Ezrin and HER2 Predicts Distant Metastasis and Poor Prognosis of Patients With Salivary Gland Carcinomas. Hum Pathol (2017) 63:110–9. doi: 10.1016/j.humpath.2017.02.017
53. Khoo TK, Yu B, Smith JA, Clarke AJ, Luk PP, Selinger CI, et al. Somatic Mutations in Salivary Duct Carcinoma and Potential Therapeutic Targets. Oncotarget (2017) 8(44):75893–903. doi: 10.18632/oncotarget.18173
54. Locati LD, Collini P, Imbimbo M, Barisella M, Testi A, Licitra LF, et al. Immunohistochemical and Molecular Profile of Salivary Gland Cancer in Children. Pediatr Blood Cancer (2017) 64(9). doi: 10.1002/pbc.26468
55. Takase S, Kano S, Tada Y, Kawakita D, Shimura T, Hirai H, et al. Biomarker Immunoprofile in Salivary Duct Carcinomas: Clinicopathological and Prognostic Implications With Evaluation of the Revised Classification. Oncotarget (2017) 8(35):59023–35. doi: 10.18632/oncotarget.19812
56. Andreasen S, Tan Q, Agander TK, Steiner P, Bjørndal K, Høgdall E, et al. Adenoid Cystic Carcinomas of the Salivary Gland, Lacrimal Gland, and Breast are Morphologically and Genetically Similar But Have Distinct microRNA Expression Profiles. Mod Pathol (2018) 31(8):1211–25. doi: 10.1038/s41379-018-0005-y
57. Beck AJCC, Lohuis PJFM, Al-Mamgani A, Smit LA, Klop WMC. Salivary Duct Carcinoma: Evaluation of Treatment and Outcome in a Tertiary Referral Institute. Eur Arch Oto-Rhino-Laryngol (2018) 275(7):1885–92. doi: 10.1007/s00405-018-5000-x
58. Boon E, Bel M, van Boxtel W, van der Graaf WTA, van Es RJJ, Eerenstein SEJ, et al. A Clinicopathological Study and Prognostic Factor Analysis of 177 Salivary Duct Carcinoma Patients From The Netherlands. Int J Cancer (2018) 143(4):758–66. doi: 10.1002/ijc.31353
59. Kanazawa T, Misawa K, Fukushima H, Misawa Y, Sato Y, Maruta M, et al. Epigenetic Inactivation of Galanin Receptors in Salivary Duct Carcinoma of the Parotid Gland: Potential Utility as Biomarkers for Prognosis. Oncol Lett (2018) 15(6):9043–50. doi: 10.3892/ol.2018.8525
60. Ryu HJ, Koh YW, Yoon SO. The Implications of TrkA and MET Aberrations in Novo Salivary Duct Carcinoma. Hum Pathol (2018) 81:18–25. doi: 10.1016/j.humpath.2018.04.027
61. Gargano SM, Senarathne W, Feldman R, Florento E, Stafford P, Swensen J, et al. Novel Therapeutic Targets in Salivary Duct Carcinoma Uncovered by Comprehensive Molecular Profiling. Cancer Med (2019) 8(17):7322–9. doi: 10.1002/cam4.2602
62. Liang L, Williams MD, Bell D. Expression of PTEN, Androgen Receptor, HER2/Neu, Cytokeratin 5/6, Estrogen Receptor-Beta, HMGA2, and PLAG1 in Salivary Duct Carcinoma. Head Neck Pathol (2019) 13(4):529–34. doi: 10.1007/s12105-018-0984-5
63. Santana T, Pavel A, Martinek P, Steiner P, Grossmann P, Baněčková M, et al. Biomarker Immunoprofile and Molecular Characteristics in Salivary Duct Carcinoma: Clinicopathological and Prognostic Implications. Hum Pathol (2019) 93:37–47. doi: 10.1016/j.humpath.2019.08.009
64. Szewczyk M, Marszałek A, Sygut J, Golusiński P, Golusiński W. Prognostic Markers in Salivary Gland Cancer and Their Impact on Survival. Head Neck (2019) 41(9):3338–47. doi: 10.1002/hed.25857
65. Hsieh MS, Lee YH, Jin YT, Kuo YJ. Clinicopathological Study of Intraductal Carcinoma of the Salivary Gland, With Emphasis on the Apocrine Type. Virchows Arch (2020) 477(4):581–92. doi: 10.1007/s00428-020-02823-7
66. Perez EA, Cortés J, Gonzalez-Angulo AM, Bartlett JMS. HER2 Testing: Current Status and Future Directions. Cancer Treat Rev (2014) 40(2):276–84. doi: 10.1016/j.ctrv.2013.09.001
67. Rakha EA, Pinder SE, Bartlett JMS, Ibrahim M, Starczynski J, Carder PJ, et al. Updated UK Recommendations for HER2 Assessment in Breast Cancer. J Clin Pathol (2015) 68(2):93–9. doi: 10.1136/jclinpath-2014-202571
Keywords: HER2, salivary gland (S.G) tumors, ERBB2, salivary duct carcinoma, prevalence
Citation: Egebjerg K, Harwood CD, Woller NC, Kristensen CA and Mau-Sørensen M (2021) HER2 Positivity in Histological Subtypes of Salivary Gland Carcinoma: A Systematic Review and Meta-Analysis. Front. Oncol. 11:693394. doi: 10.3389/fonc.2021.693394
Received: 10 April 2021; Accepted: 19 May 2021;
Published: 24 June 2021.
Edited by:
Vincent Vander Poorten, KU Leuven, BelgiumReviewed by:
Laura Deborah Locati, Istituto Nazionale dei Tumori (IRCCS), ItalyAlena Skalova, Charles University, Czechia
Copyright © 2021 Egebjerg, Harwood, Woller, Kristensen and Mau-Sørensen. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Kristian Egebjerg, kristian.egebjerg@gmail.com