 Susan Hua1,2*
Susan Hua1,2*- 1Therapeutic Targeting Research Group, School of Biomedical Sciences and Pharmacy, University of Newcastle, Callaghan, NSW, Australia
- 2Hunter Medical Research Institute, New Lambton Heights, NSW, Australia
The sublingual and buccal routes of administration have significant advantages for both local and systemic drug delivery. They have shown to be an effective alternative to the traditional oral route, especially when fast onset of action is required. Drugs can be rapidly and directly absorbed into the systemic circulation via venous drainage to the superior vena cava. Therefore, they are useful for drugs that undergo high hepatic clearance or degradation in the gastrointestinal tract, and for patients that have swallowing difficulties. Drugs administered via the sublingual and buccal routes are traditionally formulated as solid dosage forms (e.g., tablets, wafers, films, and patches), liquid dosage forms (e.g., sprays and drops), and semi-solid dosage forms (e.g., gels). Conventional dosage forms are commonly affected by physiological factors, which can reduce the contact of the formulation with the mucosa and lead to unpredictable drug absorption. There have been a number of advances in formulation development to improve the retention and absorption of drugs in the buccal and sublingual regions. This review will focus on the physiological aspects that influence buccal and sublingual drug delivery and the advances in nanoparticulate drug delivery approaches for sublingual and buccal administration. The clinical development pipeline with formulations approved and in clinical trials will also be addressed.
Introduction
Drugs are generally administered in the oral cavity to either treat local conditions (e.g., infections and ulcers) or for the systemic absorption of drugs. In particular, the sublingual and buccal mucosal regions are highly vascularized and, therefore, are useful for systemic drug delivery. Sublingual administration involves placing a drug under the tongue and buccal administration involves placing a drug between the gums and cheek. The sublingual and buccal routes are considered promising alternatives to the traditional oral route for drug delivery.
Figure 1 shows a schematic diagram of the sublingual and buccal regions in the oral cavity. The oral cavity has a relatively neutral pH of approximately 6.2–7.4 and has limited enzymatic activity. The surface area of the oral mucosa is relatively small (100–200 cm2), with the sublingual and buccal regions having an estimated surface area of 26.5 ± 4.2 cm2 and 50.2 ± 2.9 cm2, respectively (Czerkinsky and Holmgren, 2012; Kraan et al., 2014). These regions in the oral cavity are lined by non-keratinized, stratified squamous epithelium that is 100–200 µm and 8–12 cells thick in the sublingual region, and 500–800 µm and 40–50 cells thick in the buccal region (Czerkinsky and Holmgren, 2012; Kraan et al., 2014). Components from the saliva also binds to the surface of the buccal and sublingual epithelium to create a mucus layer with an average thickness of 70–100 µm (Teubl et al., 2013). Underneath the epithelium is the lamina propria and submucosa that consists of connective tissue with a network of blood vessels, lymphatic vessels and smooth muscles. Drugs can be rapidly and directly absorbed into the systemic circulation via venous drainage to the superior vena cava.
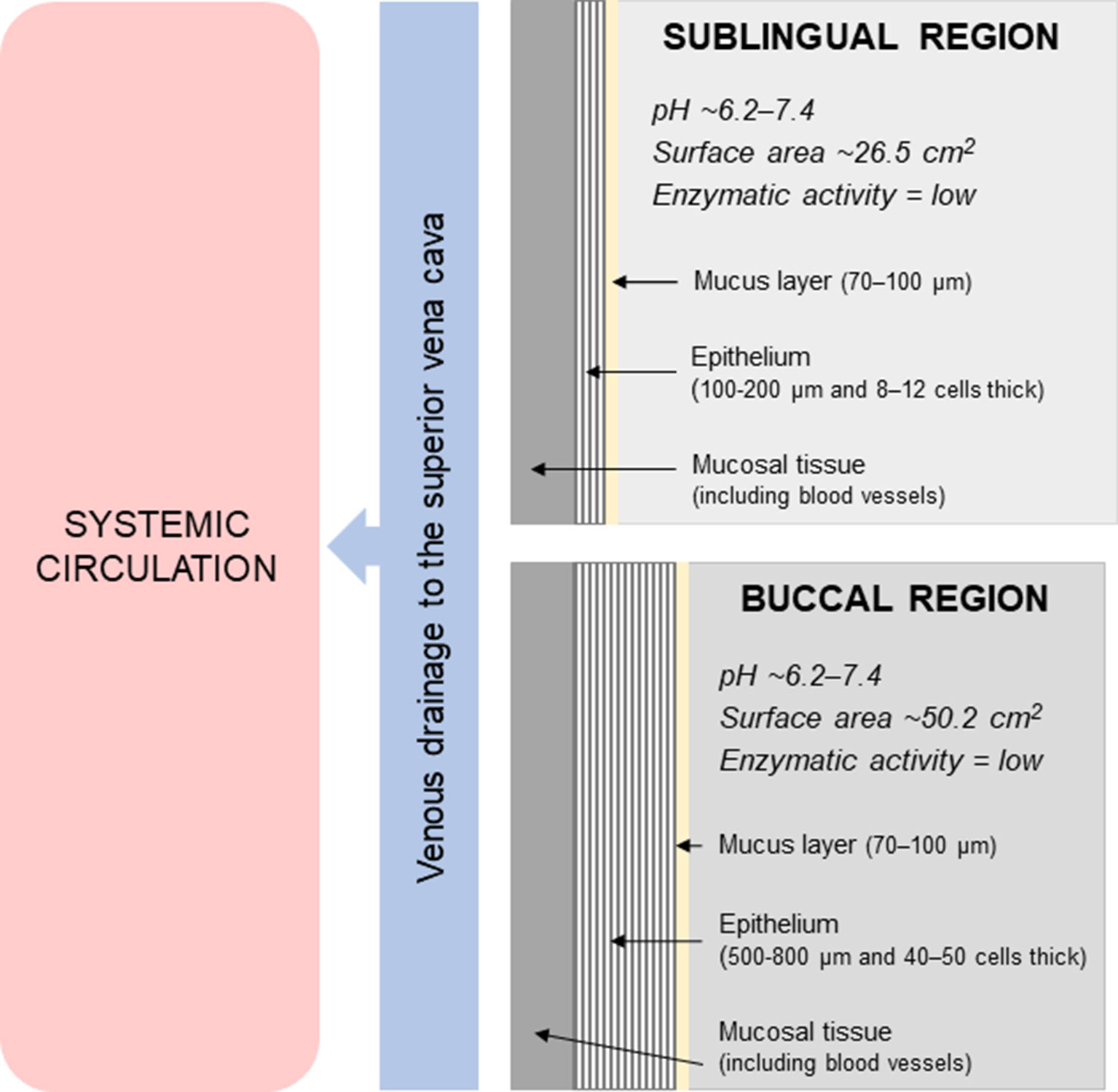
Figure 1 Schematic diagram of the sublingual and buccal regions in the oral cavity.
A number of advances in drug formulation have been made in the area of sublingual and buccal drug delivery. This review will focus on the physiological aspects that influence buccal and sublingual drug delivery and the advances in nanoparticulate drug delivery approaches for sublingual and buccal administration. The clinical development pipeline with formulations approved and in clinical trials will also be addressed.
Advantages and Disadvantages of the Sublingual and Buccal Routes for Drug Delivery
The sublingual and buccal routes of administration have a number of advantages (De Boer et al., 1984; Allen et al., 2011; Teubl et al., 2013), especially for systemic drug delivery. In general, they produce faster onset of action compared to orally ingested drug formulations. Drug absorption is relatively faster across the sublingual mucosa compared to the buccal mucosa due to the thinner epithelium. In addition to rapid absorption, the portion of drug that is absorbed through the blood vessels directly enters the systemic circulation and bypasses hepatic first-pass metabolic processes. Therefore, this route is particularly useful for highly soluble drugs that undergo high hepatic clearance or decomposition in the gastrointestinal tract. The non-adherent saliva in the buccal and sublingual regions also contains less mucin and limited enzymes (e.g., salivary amylase). Drugs may also be more stable owing to the pH in the mouth being relatively neutral compared to other parts of the gastrointestinal tract. Patients can easily self-administer doses and in most cases the effect of the drug can be quickly terminated, for example, by spitting out or swallowing the tablet. It is also beneficial for patients who suffer from swallowing difficulties.
In terms of disadvantages (De Boer et al., 1984; Allen et al., 2011; Teubl et al., 2013), the sublingual and buccal routes can be inconvenient for patients as it can involve some technical procedures to maintain the drug in the sublingual or buccal area for absorption without swallowing the drug. Not all drugs can be delivered via this route and generally only small doses can be administered. Drugs may also be unpalatable, bitter, or cause irritation to the oral mucosa, which may lead to voluntary expulsion or swallowing. Although the risk is low, there is a chance of accidental aspiration of the medication. Therefore, patients are recommended to be in an upright position when administering a dose. For similar reasons, sublingual or buccal medication should be avoided when a patient is unconscious or uncooperative. Furthermore, the buccal and sublingual routes are generally not suited or preferred for sustained drug release or for prolonged administration due to discomfort or inconvenience, especially when eating or drinking.
Physiological Factors Influencing Sublingual and Buccal Drug Delivery
For effective drug delivery via the sublingual or buccal route of administration, several physiological factors should be considered in drug formulation design and development. These factors may influence drug bioavailability, stability, efficacy, and safety.
● Residence time of the formulation: Absorption is highly dependent on the residence time of the drug in the sublingual and buccal area. This may vary considerably depending on the formulation and the patient. Sublingual and buccal drugs are generally formulated as tablets, films, wafers, or sprays. The formulations differ in terms of need for disintegration and dissolution prior to drug absorption. In addition, patients should avoid eating, drinking, chewing, or swallowing until the medication has been absorbed (De Boer et al., 1984; Allen et al., 2011). Swallowing the medication will decrease the drug’s effectiveness. This can be particularly difficult for some patients, such as younger children.
● Drug absorption: For effective absorption to occur, the drug needs to have a balance between hydrophilic and lipophilic properties (De Boer et al., 1984; Allen et al., 2011; Brunton et al., 2018). That is, the drug needs to be soluble in aqueous buccal fluids and should also have high lipid solubility to be able to cross the epithelial membrane in these regions, which is usually by passive diffusion. This route is also more suitable for low to medium molecular weight drugs (De Boer et al., 1984; Allen et al., 2011; Brunton et al., 2018)— refer to examples in Table 1. In addition, drug absorption can be affected if the gums or mucosal membranes have open sores or areas of inflammation. This may lead to enhanced or irregular drug absorption and, therefore, should be avoided or used with caution. Conversely, smoking can decrease the sublingual or buccal absorption of medications due to vasoconstriction of the blood vessels.
● pH of the saliva: The pH of the saliva can affect drug absorption by affecting the ionization state of drugs. Drug molecules predominantly undergo passive absorption pathways via transcellular diffusion (through the cell) or paracellular diffusion (between cells), depending on their physicochemical characteristics (De Boer et al., 1984; Allen et al., 2011; Brunton et al., 2018). Transcellular diffusion is the most common mechanism and is usually proportional to the lipid solubility of the drug. Therefore, absorption is favored when the drug molecule is in the non-ionized form, which is much more lipophilic than the ionized form. For sublingual and buccal administration, this means that drugs with a high pKa value are preferred due to the relatively neutral pH of the saliva. Conversely, the paracellular pathway is favored for more hydrophilic or ionized molecules. It should be noted that the pH of the saliva can be temporarily altered by environmental (e.g., foods and drinks) or personal factors [e.g., oral disease (Baliga et al., 2013)], which can affect the sublingual and buccal absorption of drugs.
● Flow of saliva: Saliva flow can influence buccal and sublingual drug delivery by altering the rate of disintegration of the formulation and dissolution of the drug. For example, if the mouth is dry, this can negatively affect drug absorption. Conversely, if saliva flow is considerable, this can lead to the drug being swallowed before absorption. Saliva flow can be affected by age, medications (e.g., anticholinergic drugs), and medical conditions (e.g., Sjögren’s syndrome, cheilosis, glossodynia, dehydration, dysphagia, and problems with mastication) (Dawes, 1987; von Bultzingslowen et al., 2007).
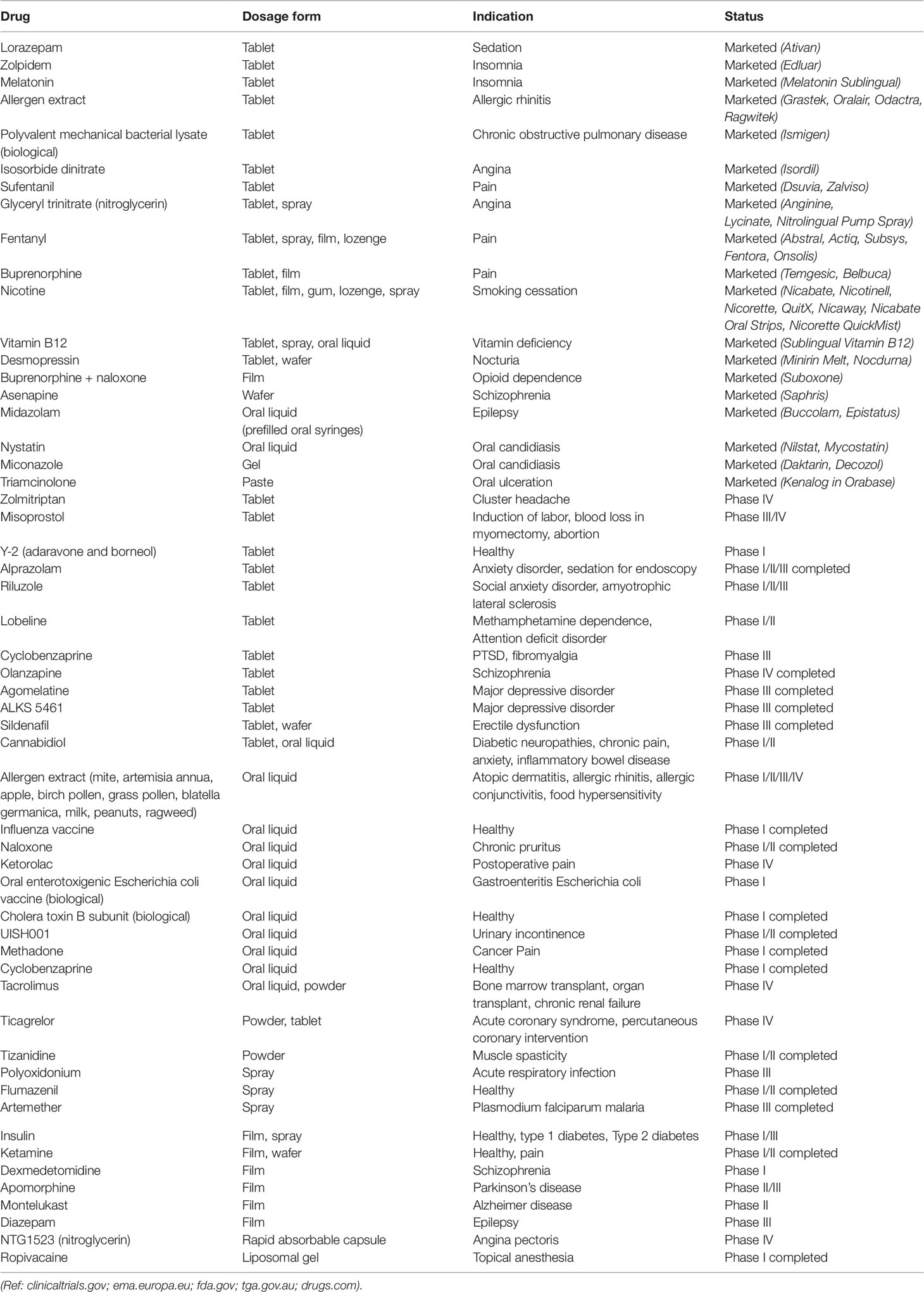
Table 1 Sublingual and buccal formulations marketed and in clinical trials
Nanoparticulate Drug Delivery Approaches
Nanoparticulate systems have previously been shown to improve the accumulation, uptake, and absorption of drugs across a variety of biological barriers, including the skin (Hua, 2015) and gastrointestinal tract (Hua et al., 2015). Therefore, it was inevitable for nanoparticles to be investigated for sublingual and buccally drug delivery. Nanoparticulate dosage forms differ from conventional dosage forms by loading the drug or active compound into nanoparticles prior to dispersion in a formulation base. They have been incorporated into various dosage forms for sublingual and buccal drug delivery, including gels (Marques et al., 2017), sprays (Baltzley et al., 2018), tablets (Gavin et al., 2015; El-Nahas et al., 2017), films (Giovino et al., 2013; Mortazavian et al., 2014; Al-Dhubiab et al., 2016; Masek et al., 2017; Castro et al., 2018a; Mahdizadeh Barzoki et al., 2018; Al-Nemrawi et al., 2019), and patches (Mahdizadeh Barzoki et al., 2016). These nanoparticulate formulations have been shown to: (i) improve drug permeability across the epithelium; (ii) modify drug release kinetics (e.g., controlled release or sustained release); (iii) provide solubilization (i.e., to deliver compounds which have physicochemical properties that strongly limit their aqueous solubility); and/or (iv) protect compounds that are sensitive to degradation (e.g., peptides) (Morales and Brayden, 2017; Hua et al., 2018). These factors all aim to promote higher sublingual or buccal bioavailability of drugs for subsequent systemic absorption.
For nanoparticulate dosage forms to be effective for sublingual or buccal drug delivery, two main factors should be considered. Firstly, the physicochemical properties of the nanoparticles themselves (e.g., size, charge, composition, and surface properties) for optimal interaction with the sublingual or buccal mucosa. A number of different nanoparticulate systems have been evaluated for sublingual and buccal drug delivery, with polymer-based and lipid-based compositions being the most common (He et al., 2009; Roblegg et al., 2012; Teubl et al., 2013; Teubl et al., 2015; Mouftah et al., 2016; Patil and Devarajan, 2016; Chaves et al., 2017; Xu et al., 2018). The composition and structure of nanoparticles can be designed to confer a number of different properties, including mucoadhesion, bioadhesion, mucus-penetration, controlled release, and deformability (Hua et al., 2015). For example, inclusion of a hydrophilic polyethylene glycol (PEG) coating to the surface of nanoparticles has been shown to reduce its interaction with the mucus constituents, increase particle translocation through the mucus and mucosa, and enhance its delivery into lymph nodes (Wang et al., 2008; Hua et al., 2015; Masek et al., 2017).
In terms of optimal nanoparticle size for sublingual or buccal administration, most of the studies in this area have used nanoparticles between approximately 100 to 300 nm in size. Very few studies have comprehensively evaluated a range of particle sizes for optimal interaction with the buccal or sublingual mucosa. For example, Teubl et al. (2013) demonstrated in ex vivo studies using porcine buccal mucosa that neutral polystyrene nanoparticles (25, 50, and 200 nm) dispersed in an aqueous base were able to penetrate into the mucosal tissue intact, with the 200-nm sized nanoparticles penetrating more rapidly and into deeper regions of the mucosa. It was suggested that the smaller nanoparticles were readily entrapped and immobilized in the mucus network. This is also supported by Holpuch et al. (Holpuch et al., 2010) which showed that 200-nm nanoparticles (FluoSpheres® polystyrene nanoparticles) were able to penetrate through the epithelium and basement membrane into the underlying connective tissue of intact normal human oral mucosal tissues that were obtained from patients undergoing surgical procedures. It should be noted that both studies used polystyrene nanoparticles, which are unable to be metabolized and can interfere with cell metabolism pathways (Holpuch et al., 2010). Therefore, further studies would be useful to evaluate the effect of more clinically translatable nanoparticulate compositions over a range of particle sizes for mucosal permeability and drug absorption for sublingual and buccal drug delivery.
There are conflicting results regarding the influence of surface charge on nanoparticle interaction with the oral mucosa. Roblegg et al. (2012) showed that 20 nm anionic (negatively charged) and 200 nm cationic (positively charged) nanoparticles were both able to permeate the mucus layer of porcine buccal mucosa. The cationic nanoparticles (200 nm) penetrated deeper into the buccal mucosal tissue compared to the 20 nm anionic nanoparticles, which remained in the top third region of the epithelium. The study reported that 200 nm anionic nanoparticles were entrapped within the mucus, formed agglomerates, and were unable to penetrate the epithelium. Similar differences in the interaction of the mucosa with nanoparticles of opposite charges were observed by Chaves et al. (2017). However, other studies have reported that cationic nanoparticles interacted more with the mucus and exhibited lower mucosal permeability in comparison to anionic nanoparticles (Chen et al., 2010; Yuan et al., 2011; Mouftah et al., 2016; Patil and Devarajan, 2016; Xu et al., 2018). This is also supported by studies in the lower gastrointestinal tract, whereby electrostatic interaction between cationic nanoparticles and the negatively charged mucins impeded the transport of the nanoparticles through the mucus layer (Hua et al., 2015). Anionic nanoparticles were able to interdiffuse among the mucus network due to less electrostatic interaction with the mucus (Hua et al., 2015).
The second main factor that should be considered for effective sublingual or buccal drug delivery is the interaction of the nanoparticles with the formulation base. The nanoparticles should be stable when incorporated into the pharmaceutical base, especially during manufacturing and storage. In addition, the formulation base should increase the residence time of the formulation in the sublingual or buccal region to optimize drug permeability and systemic absorption. There are inconsistent results as to the actual interaction of the nanoparticle-embedded formulations with the mucosal tissue. The majority of the studies have demonstrated sustained drug release from the nanoparticles embedded in the dosage form, with the drug then being diffused into the formulation base and absorbed into the adhered mucosa. These include nanoparticles incorporated into gels (Marques et al., 2017), sprays (Baltzley et al., 2018), tablets (Gavin et al., 2015; El-Nahas et al., 2017), films (Giovino et al., 2013; Mazzarino et al., 2014; Mortazavian et al., 2014; Al-Dhubiab et al., 2016; Masek et al., 2017; Castro et al., 2018a; Mahdizadeh Barzoki et al., 2018; Al-Nemrawi et al., 2019), and patches (Mahdizadeh Barzoki et al., 2016). Very few studies have demonstrated release of nanoparticles from the formulation base and mucosal penetration of intact nanoparticles for drug delivery (Mortazavian et al., 2014; Masek et al., 2017). For example, Masek et al. (2017) developed nanofiber-based mucoadhesive films consisting of an electrospun nanofibrous reservoir layer (with nanoparticles reversibly adsorbed to the surface of the nanofibers or deposited in the pores between the nanofibers), a mucoadhesive film layer, and a protective backing layer. The results from both ex vivo and in vivo studies in pigs demonstrated that the nanofibrous mucoadhesive films were able to avoid rapid clearance of nanoparticles from the site of application, maintain a long-term concentration gradient of nanoparticles at the mucosal surface, and ensure unidirectional diffusion of nanoparticles towards mucosal surfaces. Histological samples excised 2 h after in vivo administration showed penetration of intact nanoparticles into the mucosa as well as regional lymph nodes.
The reasons for the discrepancy in the mechanism of action of nanoparticles when administered in a liquid base (e.g., water or buffered solution) or embedded into a formulation base (e.g., films, gels, and tablets) for sublingual or buccal drug delivery are still incompletely understood. Further studies are needed to determine whether it is more beneficial for nanoparticles to be used as a scaffold to promote stability and control drug release kinetics from within the formulation base or following mucosal penetration as intact particles. The former mechanism would place more importance on the retention of the formulation base to the mucosa and the stability of the nanoparticles in the formulation base for drug release, whereas the latter mechanism would place more importance on the physicochemical characteristics of the nanoparticles themselves for mucosal penetration. Most of the studies have only been conducted in in vitro and/or ex vivo models, with very limited in vivo studies available. In vivo studies provide better insights into the real-time performance of the formulation, as drug absorption is affected by a number of physiological factors as discussed earlier. In addition, there are significant anatomical differences in the sublingual and buccal mucosa among species. Porcine mucosa is the most similar to human mucosa and is widely used in ex vivo studies, however it is more common to use rodents in in vivo studies which have keratinized mucosa (Masek et al., 2017). Keratinization of the mucosa acts as an additional barrier for the penetration of drugs and nanoparticles, which should be taken into account when evaluating the results. Although the results to date support the use of nanoparticulate drug delivery approaches for sublingual and buccal administration, further comprehensive mechanistic and preclinical studies are required to ensure reproducibility of efficacy and safety outcomes.
Sublingual and Buccal Formulations Approved and in Clinical Trials
A number of sublingual and buccal formulations are on the market with more in clinical development. Table 1 shows examples of the sublingual and buccal formulations that are approved or in clinical trials. Those approved for clinical use have varied indications that also benefit from faster onset of action, including sedation, insomnia, angina, pain, and smoking cessation. The drugs incorporated vary in their therapeutic index as well as their duration of use, which indicate the prospect of using drugs with a narrow therapeutic index and for long-term therapy. Biologics have also made its way into the market with the delivery of allergen extracts and polyvalent mechanical bacterial lysate for use in allergic rhinitis and chronic obstructive pulmonary disease (COPD), respectively. Sublingual and buccal formulations approved for clinical use generally incorporate drugs in conventional dosage forms such as solid dosage forms (e.g., tablets, wafers, lozenges, and films), liquid dosage forms (e.g., sprays and oral liquid drops), and semi-solid dosage forms (e.g., gels and paste) (Allen et al., 2011). Solid dosage forms are typically manufactured to disintegrate or dissolve rapidly in a small quantity of saliva to allow fast drug absorption through the mucosa, without the need for water. In contrast, liquid dosage forms for sublingual and buccal use contain the drug dissolved (solution) or dispersed (suspension) in a vehicle. This is then administered as oral liquid drops or sprays, with the latter typically having a metered valve to control the dose of the drug delivered.
The majority of the formulations in clinical trials (Table 1) incorporate already approved drugs or novel compounds into conventional sublingual and buccal dosage forms—in particular, tablets, films, and oral liquids. It should be noted that drugs evaluated in the early phases of clinical investigation are commonly administered as a powder or oral liquid. Powders are typically formulated by opening clinically available capsules or crushing tablets, whereas oral liquids are attained by dispersing the powder into a liquid base or using the parenteral formulations of the drug. These studies are mainly focused on evaluating the pharmacokinetics and efficacy of the drug following sublingual or buccal administration, rather than assessing the performance of novel formulations.
Very few innovative dosage forms for sublingual and buccal drug delivery have reached the clinical development phase. The main strategies have been the incorporation of permeation enhancers or mucoadhesive constituents to conventional dosage forms. Conventional dosage forms are commonly affected by physiological factors (e.g., saliva and swallowing), which can reduce the contact of the formulation with the mucosa and lead to unpredictable drug absorption. In addition, the multicellular thickness and stratified nature of the sublingual and buccal epithelium can contribute to reduced drug absorption across these regions. These strategies have been shown to improve mucosal retention and/or permeability of conventional dosage forms. For example, permeation enhancers (e.g., surfactants, bile salts, fatty acids, cyclodextrins, and chelators) have been shown to improve the mucosal permeability and absorption of various compounds (Tsutsumi et al., 1998; Shojaei et al., 1999; Bird et al., 2001; Burgalassi et al., 2006; Sohi et al., 2010; Tian et al., 2012; Prasanth et al., 2014; Patil and Devarajan, 2014; Ojewole et al., 2014; Marxen et al., 2018) by: (i) changing mucus rheology; (ii) increasing the fluidity of the lipid bilayer membrane; (iii) acting on the components at tight junctions; (iv) inhibiting mucosal enzymes; and (v) increasing the thermodynamic activity of drugs (Chinna Reddy and Chaitanya, 2011). In addition, the incorporation of mucoadhesive constituents has been demonstrated to enhance formulation retention time with the sublingual or buccal mucosa (Das and Das, 2004; Razafindratsita et al., 2007; Perioli and Pagano, 2013; Ikram et al., 2015; Yildiz Pekoz et al., 2016; El-Nabarawi et al., 2016; Ammar et al., 2017; Parodi et al., 2017; Celik, 2017; Salehi and Boddohi, 2017; Vasseur et al., 2017; Khan and Boateng, 2018; Razzaq et al., 2018; Sharma et al., 2018). This has been done primarily for solid dosage forms and semi-solid dosage forms. In particular, mucoadhesive polymers are commonly used in these formulations, including synthetic polymers (e.g., cellulose derivatives and poly(acrylic acid)-based polymers) and those from natural sources (e.g., chitosan, hyaluronic acid, agarose, and various gums). An impermeable backing layer may be incorporated in solid dosage forms (e.g., films, patches, and tablets) to allow unidirectional drug delivery (Guo and Cooklock, 1996; Benes et al., 1997; Shojaei et al., 1998; El-Nabarawi et al., 2016).
It is expected that more innovative dosage forms will eventually reach clinical trials following comprehensive preclinical assessment and optimization. This includes nanoparticulate formulations, especially for the systemic delivery of drugs. Ropivacaine liposomal gel is the only nanoparticulate formulation that has reached clinical studies for sublingual and buccal drug delivery. It has been evaluated for local drug delivery as a topical anesthetic in Phase I clinical studies. Furthermore, slow-disintegrating and non-disintegrating dosage forms, particularly for buccal drug delivery, have been extensively investigated in the literature to extend or control the release of active substances over a prolonged period (Scholz et al., 2008; Bahri-Najafi et al., 2014; Kaur et al., 2014; Jaipal et al., 2016; Celik, 2017; Lindert and Breitkreutz, 2017; Celik et al., 2017; Farag et al., 2018; Castro et al., 2018b). For example, multilayered films have been developed for controlled drug delivery and are generally designed to remain in their form and slowly release drug over a specified time (Lindert and Breitkreutz, 2017). It should be noted that formulations that have prolonged contact with the mucosa may cause irritation and/or discomfort for the patient, especially with concurrent eating or drinking. There is also a possibility for the dosage form to detach from the mucosa and be swallowed, which can lead to subsequent adherence to other parts of the gastrointestinal tract (e.g., esophagus). The results from clinical studies will determine the feasible of these dosage forms in clinical practice.
Conclusion
The sublingual and buccal routes of administration have significant advantages for systemic drug delivery. They have shown to be an effective alternative to the traditional oral route, especially when fast onset of action is required. In addition, they are useful for drugs that undergo high hepatic clearance or degradation in the gastrointestinal tract, and for patients that have swallowing difficulties. Although significant advances in drug formulation have been reported in the literature, particularly to improve retention and absorption in the buccal and sublingual regions, very few of them have translated to the clinical phase. For clinical translation to be justified, there needs to be a clear benefit of efficacy and/or safety with any new drug formulation compared to clinically available dosage forms (Hua et al., 2018). In addition, comprehensive evaluations of the pharmacokinetics, stability, efficacy, and safety of the formulations are required in appropriate animal models as well as in clinical studies, based on regulatory standards and protocols. For innovative platforms, such as nanoparticles, mechanism of action and safety of the different carriers following mucosal interaction and/or uptake need to be explored further (Bergin and Witzmann, 2013; Talkar et al., 2018; Vita et al., 2019). Complexity in drug formulation is also a key factor that can be a barrier to clinical translation, irrespective of its therapeutic efficacy (Hua et al., 2018). Therefore, simplification in formulation design is required to allow efficient and reproducible large-scale manufacturing. The availability of standardized testing methods can also be a limitation to reliably assess the quality of more complex or innovative formulations for regulatory standards.
Author Contributions
SH was involved in conception of the idea for the review, drafted the manuscript, and approved the final version of the manuscript.
Conflict of Interest
The author declares that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Acknowledgments
The author wishes to thank the University of Newcastle, Pharmacy Research Trust of New South Wales, Rebecca L. Cooper Medical Research Foundation, Gladys M Brawn Fellowship, and AusEE Research Foundation for providing financial support for this work.
References
Al-Dhubiab, B. E., Nair, A. B., Kumria, R., Attimarad, M., Harsha, S. (2016). Development and evaluation of buccal films impregnated with selegiline-loaded nanospheres. Drug Deliv. 23 (7), 2154–2162. doi: 10.3109/10717544.2014.948644
Allen, L. V., Popovich, N. G., Ansel, H. C. (2011). Ansel’s pharmaceutical dosage forms and drug delivery systems. Philadelphia: Lippincott Williams & Wilkins;.
Al-Nemrawi, N. K., Alsharif, S. S. M., Alzoubi, K. H., Alkhatib, R. Q. (2019). Preparation and characterization of insulin chitosan-nanoparticles loaded in buccal films. Pharm. Dev. Technol. 24 (8), 967–974. doi: 10.1080/10837450.2019.1619183
Ammar, H. O., Ghorab, M. M., Mahmoud, A. A., Shahin, H. I. (2017). Design and in vitro/in vivo evaluation of ultra-thin mucoadhesive buccal film containing fluticasone propionate. AAPS PharmSciTech 18 (1), 93–103. doi: 10.1208/s12249-016-0496-0
Bahri-Najafi, R., Tavakoli, N., Senemar, M., Peikanpour, M. (2014). Preparation and pharmaceutical evaluation of glibenclamide slow release mucoadhesive buccal film. Res. Pharmaceut. Sci. 9 (3), 213–223.
Baliga, S., Muglikar, S., Kale, R. (2013). Salivary pH: a diagnostic biomarker. J. Indian Soc. Periodontol. 17 (4), 461–465. doi: 10.4103/0972-124X.118317
Baltzley, S., Malkawi, A. A., Alsmadi, M., Al-Ghananeem, A. M. (2018). Sublingual spray drug delivery of ketorolac-loaded chitosan nanoparticles. Drug Dev. Ind. Pharm. 44 (9), 1467–1472. doi: 10.1080/03639045.2018.1460378
Benes, L., Claustrat, B., Horriere, F., Geoffriau, M., Konsil, J., Parrott, K. A., et al. (1997). Transmucosal, oral controlled-release, and transdermal drug administration in human subjects: A crossover study with melatonin. J. Pharm. Sci-Us. 86 (10), 1115–1119. doi: 10.1021/js970011z
Bergin, I. L., Witzmann, F. A. (2013). Nanoparticle toxicity by the gastrointestinal route: evidence and knowledge gaps. Int. J. BioMed. Nanosci. Nanotechnol 3 (1–2), 1–44. doi: 10.1504/IJBNN.2013.054515.
Bird, A. P., Faltinek, J. R., Shojaei, A. H. (2001). Transbuccal peptide delivery: stability and in vitro permeation studies on endomorphin-1. J. Control Release 73 (1), 31–36. doi: 10.1016/S0168-3659(01)00246-2
Brunton, L. L., Knollmann, B. C., Hilal-Dandan, R., (2018). Goodman & Gilman’s: The Pharmacological Basis of Therapeutics 13th edition. New York: McGraw-Hill Education;.
Burgalassi, S., Chetoni, P., Dini, L., Najarro, M., Monti, D., Morelli, P., et al. (2006). Effect of permeation enhancers on buccal absorption. Arzneimittel-Forschung 56 (7), 561–567. doi: 10.1055/s-0031-1296752
Castro, P. M., Baptista, P., Madureira, A. R., Sarmento, B., Pintado, M. E. (2018a). Combination of PLGA nanoparticles with mucoadhesive guar-gum films for buccal delivery of antihypertensive peptide. Int. J. Pharm. 547 (1-2), 593–601. doi: 10.1016/j.ijpharm.2018.05.051
Castro, P. M., Sousa, F., Magalhaes, R., Ruiz-Henestrosa, V. M. P., Pilosof, A. M. R., Madureira, A. R., et al. (2018b). Incorporation of beads into oral films for buccal and oral delivery of bioactive molecules. Carbohydr. Polymers 194, 411–421. doi: 10.1016/j.carbpol.2018.04.032
Celik, B. (2017). Risperidone mucoadhesive buccal tablets: formulation design, optimization and evaluation. Drug Des. Devel. Ther. 11, 3355–3365. doi: 10.2147/DDDT.S150774
Celik, B., Ozdemir, S., Barla Demirkoz, A., Uner, M. (2017). Optimization of piribedil mucoadhesive tablets for efficient therapy of Parkinson’s disease: physical characterization and ex vivo drug permeation through buccal mucosa. Drug Dev. Ind. Pharm. 43 (11), 1836–1845. doi: 10.1080/03639045.2017.1349785
Chaves, P. D., Ourique, A. F., Frank, L. A., Pohlmann, A. R., Guterres, S. S., Beck, R. C. (2017). Carvedilol-loaded nanocapsules: Mucoadhesive properties and permeability across the sublingual mucosa. Eur. J. Pharm. Biopharm. 114, 88–95. doi: 10.1016/j.ejpb.2017.01.007
Chen, E. Y., Wang, Y. C., Chen, C. S., Chin, W. C. (2010). Functionalized positive nanoparticles reduce mucin swelling and dispersion. PloS One 5 (11), e15434. doi: 10.1371/journal.pone.0015434
Chinna Reddy, P., Chaitanya, K. S., Madhusudan Rao, Y. (2011). A review on bioadhesive buccal drug delivery systems: current status of formulation and evaluation methods. Daru 19 (6), 385–403.
Czerkinsky, C., Holmgren, J. (2012). Mucosal delivery routes for optimal immunization: targeting immunity to the right tissues. Curr. Topics Microbiol. Immunol. 354, 1–18. doi: 10.1007/82_2010_112
Das, N. G., Das, S. K. (2004). Development of mucoadhesive dosage forms of buprenorphine for sublingual drug delivery. Drug Deliv. 11 (2), 89–95. doi: 10.1080/10717540490280688
Dawes, C. (1987). Physiological factors affecting salivary flow rate, oral sugar clearance, and the sensation of dry mouth in man. J. Dental Res. 66, 648–653. doi: 10.1177/00220345870660S107
De Boer, A. G., De Leede, L. G., Breimer, D. D. (1984). Drug absorption by sublingual and rectal routes. Br. J. Anaesthesia 56 (1), 69–82. doi: 10.1093/bja/56.1.69
El-Nabarawi, M. A., Ali, A. A., Aboud, H. M., Hassan, A. H., Godah, A. H. (2016). Transbuccal delivery of betahistine dihydrochloride from mucoadhesive tablets with a unidirectional drug flow: in vitro, ex vivo and in vivo evaluation. Drug Des. Devel. Ther. 10, 4031–4045. doi: 10.2147/DDDT.S120613
El-Nahas, A. E., Allam, A. N., El-Kamel, A. H. (2017). Mucoadhesive buccal tablets containing silymarin Eudragit-loaded nanoparticles: formulation, characterisation and ex vivo permeation. J. Microencapsul. 34 (5), 463–474. doi: 10.1080/02652048.2017.1345996
Farag, M. M., El Malak, N. S., Yehia, S. A. (2018). Zaleplon loaded bi-layered chronopatch: a novel buccal chronodelivery approach to overcome circadian rhythm related sleep disorder. Int. J. Pharm. 542 (1-2), 117–124. doi: 10.1016/j.ijpharm.2018.03.014
Gavin, A., Pham, J. T., Wang, D., Brownlow, B., Elbayoumi, T. A. (2015). Layered nanoemulsions as mucoadhesive buccal systems for controlled delivery of oral cancer therapeutics. Int. J. Nanomed. 10, 1569–1584. doi: 10.2147/IJN.S75474
Giovino, C., Ayensu, I., Tetteh, J., Boateng, J. S. (2013). An integrated buccal delivery system combining chitosan films impregnated with peptide loaded PEG-b-PLA nanoparticles. Colloids Surf B Biointerfaces 112, 9–15. doi: 10.1016/j.colsurfb.2013.07.019
Guo, J. H., Cooklock, K. M. (1996). The effects of backing materials and multilayered systems on the characteristics of bioadhesive buccal patches. J. Pharm. Pharmacol. 48 (3), 255–257. doi: 10.1111/j.2042-7158.1996.tb05912.x
He, C., Cui, F., Yin, L., Qian, F., Tang, C., Yin, C. (2009). A polymeric composite carrier for oral delivery of peptide drugs: Bilaminated hydrogel film loaded with nanoparticles. Eur. Polym. J. 45, 368–376. doi: 10.1016/j.eurpolymj.2008.11.004
Holpuch, A. S., Hummel, G. J., Tong, M., Seghi, G. A., Pei, P., Ma, P., et al. (2010). Nanoparticles for local drug delivery to the oral mucosa: proof of principle studies. Pharmaceut. Res. 27 (7), 1224–1236. doi: 10.1007/s11095-010-0121-y
Hua, S. (2015). Lipid-based nano-delivery systems for skin delivery of drugs and bioactives. Front. Pharmacol. 6, 219. doi: 10.3389/fphar.2015.00219
Hua, S., Marks, E., Schneider, J. J., Keely, S. (2015). Advances in oral nano-delivery systems for colon targeted drug delivery in inflammatory bowel disease: selective targeting to diseased versus healthy tissue. Nanomedicine. 11 (5), 1117–1132. doi: 10.1016/j.nano.2015.02.018
Hua, S., de Matos, M. B. C., Metselaar, J. M., Storm, G. (2018). Current Trends and Challenges in the Clinical Translation of Nanoparticulate Nanomedicines: Pathways for Translational Development and Commercialization. Front. Pharmacol. 9, 790. doi: 10.3389/fphar.2018.00790
Ikram, M., Gilhotra, N., Gilhotra, R. M. (2015). Formulation and optimization of mucoadhesive buccal patches of losartan potassium by using response surface methodology. Advanced Biomed. Res. 4, 239. doi: 10.4103/2277-9175.168606
Jaipal, A., Pandey, M. M., Charde, S. Y., Sadhu, N., Srinivas, A., Prasad, R. G. (2016). Controlled release effervescent buccal discs of buspirone hydrochloride: in vitro and in vivo evaluation studies. Drug Deliv. 23 (2), 452–458. doi: 10.3109/10717544.2014.917388
Kaur, G., Singh, D., Brar, V. (2014). Bioadhesive okra polymer based buccal patches as platform for controlled drug delivery. Int. J. Biol. Macromol. 70, 408–419. doi: 10.1016/j.ijbiomac.2014.07.015
Khan, S., Boateng, J. (2018). Effects of cyclodextrins (beta and gamma) and l-Arginine on stability and functional properties of mucoadhesive buccal films loaded with omeprazole for pediatric patients. Polymers 10 (2), 157. doi: 10.3390/polym10020157.
Kraan, H., Vrieling, H., Czerkinsky, C., Jiskoot, W., Kersten, G., Amorij, J. P. (2014). Buccal and sublingual vaccine delivery. J. Control Release 190, 580–592. doi: 10.1016/j.jconrel.2014.05.060
Lindert, S., Breitkreutz, J. (2017). Oromucosal multilayer films for tailor-made, controlled drug delivery. Expert Opin. Drug Deliv. 14 (11), 1265–1279. doi: 10.1080/17425247.2017.1276899
Mahdizadeh Barzoki, Z., Emam-Djomeh, Z., Mortazavian, E., Akbar Moosavi-Movahedi, A., Rafiee Tehrani, M. (2016). Formulation, in vitro evaluation and kinetic analysis of chitosan-gelatin bilayer muco-adhesive buccal patches of insulin nanoparticles. J. Microencapsul. 33 (7), 613–624. doi: 10.1080/02652048.2016.1234513
Mahdizadeh Barzoki, Z., Emam-Djomeh, Z., Mortazavian, E., Rafiee-Tehrani, N., Behmadi, H., Rafiee-Tehrani, M., et al. (2018). Determination of diffusion coefficient for released nanoparticles from developed gelatin/chitosan bilayered buccal films. Int. J. Biol. Macromol. 112, 1005–1013. doi: 10.1016/j.ijbiomac.2018.01.215
Marques, A. C., Rocha, A. I., Leal, P., Estanqueiro, M., Lobo, J. M. S. (2017). Development and characterization of mucoadhesive buccal gels containing lipid nanoparticles of ibuprofen. Int. J. Pharm. 533 (2), 455–462. doi: 10.1016/j.ijpharm.2017.04.025
Marxen, E., Jin, L., Jacobsen, J., Janfelt, C., Hyrup, B., Nicolazzo, J. A. (2018). Effect of permeation enhancers on the Buccal permeability of nicotine: ex vivo transport studies complemented by MALDI MS Imaging. Pharmaceut. Res. 35 (3), 70. doi: 10.1007/s11095-017-2332-y
Masek, J., Lubasova, D., Lukac, R., Turanek-Knotigova, P., Kulich, P., Plockova, J., et al. (2017). Multi-layered nanofibrous mucoadhesive films for buccal and sublingual administration of drug-delivery and vaccination nanoparticles - important step towards effective mucosal vaccines. J. Control Release 249, 183–195. doi: 10.1016/j.jconrel.2016.07.036
Mazzarino, L., Borsali, R., Lemos-Senna, E. (2014). Mucoadhesive films containing chitosan-coated nanoparticles: a new strategy for buccal curcumin release. J. Pharm. Sci. 103 (11), 3764–3771. doi: 10.1002/jps.24142
Morales, J. O., Brayden, D. J. (2017). Buccal delivery of small molecules and biologics: of mucoadhesive polymers, films, and nanoparticles. Curr. Opin. Pharmacol. 36, 22–28. doi: 10.1016/j.coph.2017.07.011
Mortazavian, E., Dorkoosh, F. A., Rafiee-Tehrani, M. (2014). Design, characterization and ex vivo evaluation of chitosan film integrating of insulin nanoparticles composed of thiolated chitosan derivative for buccal delivery of insulin. Drug Dev. Ind. Pharm. 40 (5), 691–698. doi: 10.3109/03639045.2014.886590
Mouftah, S., Abdel-Mottaleb, M. M. A., Lamprecht, A. (2016). Buccal delivery of low molecular weight heparin by cationic polymethacrylate nanoparticles. Int. J. Pharm. 515 (1-2), 565–574. doi: 10.1016/j.ijpharm.2016.10.039
Ojewole, E., Kalhapure, R., Akamanchi, K., Govender, T. (2014). Novel oleic acid derivatives enhance buccal permeation of didanosine. Drug Dev. Ind. Pharm. 40 (5), 657–668. doi: 10.3109/03639045.2014.892958
Parodi, B., Russo, E., Baldassari, S., Zuccari, G., Pastorino, S., Yan, M., et al. (2017). Development and characterization of a mucoadhesive sublingual formulation for pain control: extemporaneous oxycodone films in personalized therapy. Drug Dev. Ind. Pharm. 43 (6), 917–924. doi: 10.1080/03639045.2017.1281290
Patil, N. H., Devarajan, P. V. (2014). Enhanced insulin absorption from sublingual microemulsions: effect of permeation enhancers. Drug Deliv. Trans. Res. 4 (5-6), 429–438. doi: 10.1007/s13346-014-0205-z
Patil, N. H., Devarajan, P. V. (2016). Insulin-loaded alginic acid nanoparticles for sublingual delivery. Drug Deliv. 23 (2), 429–436. doi: 10.3109/10717544.2014.916769
Perioli, L., Pagano, C. (2013). Preformulation studies of mucoadhesive tablets for carbamazepine sublingual administration. Colloids Surf B Biointerfaces 102, 915–922. doi: 10.1016/j.colsurfb.2012.10.001
Prasanth, V. V., Puratchikody, A., Mathew, S. T., Ashok, K. B. (2014). Effect of permeation enhancers in the mucoadhesive buccal patches of salbutamol sulphate for unidirectional buccal drug delivery. Res. Pharmaceut. Sci. 9 (4), 259–268.
Razafindratsita, A., Saint-Lu, N., Mascarell, L., Berjont, N., Bardon, T., Betbeder, D., et al (2007). Improvement of sublingual immunotherapy efficacy with a mucoadhesive allergen formulation. J. Allergy Clin. Immunol. 120 (2), 278–285. doi: 10.1016/j.jaci.2007.04.009
Razzaq, S., Hanif, S., Syed, M. A., Iqbal, J., Hassan, S. S., Raza, S. A., et al (2018). Development and evaluation of mucoadhesive buccal tablet containing metronidazole for the treatment of periodontitis and gingivitis. Pakistan J. Pharmaceut. Sci. 31 (5), 1903–1910.
Roblegg, E., Frohlich, E., Meindl, C., Teubl, B., Zaversky, M., Zimmer, A. (2012). Evaluation of a physiological in vitro system to study the transport of nanoparticles through the buccal mucosa. Nanotoxicology. 6 (4), 399–413. doi: 10.3109/17435390.2011.580863
Salehi, S., Boddohi, S. (2017). New formulation and approach for mucoadhesive buccal film of rizatriptan benzoate. Prog. Biomater. 6 (4), 175–187. doi: 10.1007/s40204-017-0077-7
Scholz, O. A., Wolff, A., Schumacher, A., Giannola, L. I., Campisi, G., Ciach, T., et al. (2008). Drug delivery from the oral cavity: focus on a novel mechatronic delivery device. Drug Discovery Today 13 (5-6), 247–253. doi: 10.1016/j.drudis.2007.10.018
Sharma, D., Sharma, A., Garg, R. (2018). Design, development and in vitro/ex vivo evaluation of mucoadhesive buccal film of benzydamine hydrochloride for the effective treatment of aphthous stomatitis. Recent Pat. Drug Delivery Formul. 12 (4), 277–294. doi: 10.2174/1872211313666190128151038
Shojaei, A. H., Zhuo, S. L., Li, X. (1998). Transbuccal delivery of acyclovir (II): feasibility, system design, and in vitro permeation studies. J. Pharm. Pharm. Sci. 1 (2), 66–73.
Shojaei, A. H., Khan, M., Lim, G., Khosravan, R. (1999). Transbuccal permeation of a nucleoside analog, dideoxycytidine: effects of menthol as a permeation enhancer. Int. J. Pharm. 192 (2), 139–146. doi: 10.1016/S0378-5173(99)00301-4
Sohi, H., Ahuja, A., Ahmad, F. J., Khar, R. K. (2010). Critical evaluation of permeation enhancers for oral mucosal drug delivery. Drug Dev. Ind. Pharm. 36 (3), 254–282. doi: 10.3109/03639040903117348
Talkar, S., Dhoble, S., Majumdar, A., Patravale, V. (2018). Transmucosal Nanoparticles: Toxicological Overview. Adv. Exp. Med. Biol. 1048, 37–57. doi: 10.1007/978-3-319-72041-8_3
Teubl, B. J., Meindl, C., Eitzlmayr, A., Zimmer, A., Frohlich, E., Roblegg, E. (2013). In-vitro permeability of neutral polystyrene particles via buccal mucosa. Small. 9 (3), 457–466. doi: 10.1002/smll.201201789
Teubl, B. J., Leitinger, G., Schneider, M., Lehr, C. M., Frohlich, E., Zimmer, A., et al. (2015). The buccal mucosa as a route for TiO2 nanoparticle uptake. Nanotoxicology. 9 (2), 253–261. doi: 10.3109/17435390.2014.921343
Tian, W., Hu, Q., Xu, Y., Xu, Y. (2012). Effect of soybean-lecithin as an enhancer of buccal mucosa absorption of insulin. Biomed. Materials Eng. 22 (1-3), 171–178. doi: 10.3233/BME-2012-0704
Tsutsumi, K., Obata, Y., Takayama, K., Loftsson, T., Nagai, T. (1998). Effect of cod-liver oil extract on the buccal permeation of ergotamine tartrate. Drug Dev. Ind. Pharm. 24 (8), 757–762. doi: 10.3109/03639049809082723
Vasseur, B., Dufour, A., Houdas, L., Goodwin, H., Harries, K., Emul, N. Y., et al. (2017). Comparison of the systemic and local pharmacokinetics of clonidine mucoadhesive buccal tablets with reference clonidine oral tablets in healthy volunteers: an open-label randomised cross-over trial. Adv. Ther. 34 (8), 2022–2032. doi: 10.1007/s12325-017-0585-9
Vita, A. A., Royse, E. A., Pullen, N. A. (2019). Nanoparticles and danger signals: oral delivery vehicles as potential disruptors of intestinal barrier homeostasis. J. Leukocyte Biol. 106 (1), 95–103. doi: 10.1002/JLB.3MIR1118-414RR
von Bultzingslowen, I., Sollecito, T. P., Fox, P. C., Daniels, T., Jonsson, R., Lockhart, P. B., et al. (2007). Salivary dysfunction associated with systemic diseases: systematic review and clinical management recommendations. Surg. Med. Pathol. Radiol. Endodontics 103 Suppl, S57 e1–S57 15. doi: 10.1016/j.tripleo.2006.11.010
Wang, Y. Y., Lai, S. K., Suk, J. S., Pace, A., Cone, R., Hanes, J. (2008). Addressing the PEG mucoadhesivity paradox to engineer nanoparticles that “slip” through the human mucus barrier. Angew Chem. Int. Ed. Engl. 47 (50), 9726–9729. doi: 10.1002/anie.200803526
Xu, Y., Zhang, X., Zhang, Y., Ye, J., Wang, H. L., Xia, X., et al. (2018). Mechanisms of deformable nanovesicles based on insulin-phospholipid complex for enhancing buccal delivery of insulin. Int. J. Nanomed. 13, 7319–7331. doi: 10.2147/IJN.S175425
Yildiz Pekoz, A., Sedef Erdal, M., Okyar, A., Ocak, M., Tekeli, F., Kaptan, E., et al. (2016). Preparation and in-vivo evaluation of dimenhydrinate buccal mucoadhesive films with enhanced bioavailability. Drug Dev. Ind. Pharm. 42 (6), 916–925. doi: 10.3109/03639045.2015.1091470
Keywords: buccal, sublingual, drug delivery, mucosal, formulation, nanoparticles, physiological factors, translation
Citation: Hua S (2019) Advances in Nanoparticulate Drug Delivery Approaches for Sublingual and Buccal Administration. Front. Pharmacol. 10:1328. doi: 10.3389/fphar.2019.01328
Received: 14 August 2019; Accepted: 15 October 2019;
Published: 05 November 2019.
Edited by:
Paul Chi-Lui Ho, National University of Singapore, SingaporeReviewed by:
Joshua Boateng, University of Greenwich, United KingdomNadeem Irfan Bukhari, University of the Punjab, Pakistan
Copyright © 2019 Hua. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Susan Hua, Susan.Hua@newcastle.edu.au