 Sabrina Köchli
Sabrina Köchli Katharina Endes
Katharina Endes Julia Grenacher
Julia Grenacher Lukas Streese
Lukas Streese Giulia Lona
Giulia Lona Christoph Hauser
Christoph Hauser Arne DeiserothLukas Zahner
Arne DeiserothLukas Zahner Henner Hanssen*
Henner Hanssen*- Department of Sport, Exercise and Health, Medical Faculty, University of Basel, Basel, Switzerland
Background/Aims: Socioeconomic barriers and lifestyle conditions affect development of cardiovascular disease in adults, but little is known about the association of parental lifestyle and education with childhood health. We aimed to investigate the association of socioeconomic status (SES), migration background, parental physical activity (PA) and smoking status with micro-and macrovascular health in children.
Methods: In 2016/2017, 833 school children (aged 7.2 ± 0.4 years) in Basel (Switzerland) were screened for retinal arteriolar-to-venular ratio (AVR), pulse wave velocity (PWV), SES, migration background and parental PA as well as smoking status.
Results: High parental PA levels were associated with a favorable higher AVR (p = 0.020) and lower PWV (p = 0.035), but not independent of parental smoking status. Children with parents who smoked had a higher PWV [4.39 (4.35–4.42) m/s] compared to children with non-smoking parents [4.32 (4.29–4.34) m/s, p = 0.001]. Children of parents with a low household income had a higher PWV [4.36 (4.32–4.41) m/s] compared to children of parents with a high household income [4.30 (4.26–4.34) m/s, p = 0.033]. Low parental educational level was associated with a lower AVR [0.86 (0.85–0.88)] compared to children with highly educated parents [AVR:0.88 (0.87–0.88), p = 0.007; PWV: 4.33 (4.30–4.35) m/s, p = 0.041]. Children with a European background showed a higher AVR [0.88 (0.87–0.88)] compared to non-European children [AVR: (0.86 (0.85–0.87), p = 0.034].
Conclusion: Parental PA is associated with better macro- and microvascular childhood health. However, the positive association is lost when parental smoking is considered in the analysis. Socioeconomic factors seem to associate with subclinical vascular alterations in children. Primary prevention programs should focus on including parental lifestyle interventions and educational programs to reduce the burden of lifestyle-associated barriers in order to improve cardiovascular health during lifespan.
Clinical Trial Registration: ClinicalTrials.gov Exercise and Arterial Modulation in Youth, https://clinicaltrials.gov/ct2/show/NCT02853747, NCT02853747.
Introduction
In high-income western countries such as Switzerland, cardiovascular (CV) disease is the leading cause of death. CV disease has its origin early in life due to genetic predisposition, environmental influence as well as socioeconomic and lifestyle-associated status. Over the last decades, the assessment of retinal vessel diameters and arterial stiffness by aortic pulse wave velocity (PWV) have become well-established and recommended vascular biomarkers as a surrogate end point for CV risk assessment (1–4). We recently demonstrated that childhood obesity, high blood pressure (BP) and low physical fitness are associated with retinal micro- and macrovascular alterations in young children (5). Children with obesity and elevated BP had higher arterial stiffness and narrower retinal arteriolar diameters. Cardiorespiratory fitness was associated with a favorable higher retinal arteriolar-to-venular ratio (AVR) as well as lower arterial stiffness (5). Environmental conditions such as socioeconomic status (SES), migration background and parental lifestyle seem to play a major role in the development of CV risk factors in children and adolescence. Evidence suggests that the prevalence of CV risk factors is higher in children with low SES. For example, an inverse correlation has previously been described between household income and childhood overweight and obesity (6, 7). The International Study of Childhood Obesity, Lifestyle and the Environment in 12 countries around the world found that parental educational level is also inversely associated with childhood overweight and obesity (8). Parental educational level seems to be contributed to a higher prevalence of childhood obesity (9), elevated BP (10, 11) and sedentary behavior (7, 12). Passive smoking seems to affect development of childhood obesity (13) and vascular health (14, 15). Migration background has also been associated with higher prevalence of children with obesity and physical inactivity (7, 9, 12). Nonetheless, evidence for associations between socioeconomic status, parental smoking and physical activity (PA) behavior with childhood macro- and microvascular health are scarce. This study, for the first time, aimed to investigate the association of SES, migration background and parental lifestyle with large artery stiffness and retinal microvascular health in young school children.
Method
Study Design and Participants
This study is part of the large-scale, cross-sectional EXAMIN YOUTH study (16). Children were included if they were between 6 and 8 years old and had an informed consent from their parents to participate. Briefly, children with written informed consent were screened for large artery stiffness and retinal vessel diameters to assess macro-and microvascular health. Anthropometric parameters and blood pressure were determined according to standardized procedures for children. In addition, physical fitness was assessed on a separate day. The medical screening was performed in the morning on-site the regular school setting and children had to remain fastened before anthropometric and CV assessments. Parents were requested to complete a questionnaire on lifestyle behavior, level of education and SES (16). The questionnaires were handed out and re-collected by the teachers. If the questionnaire was not returned to the teachers by the parents, an additional reminder was sent to the parents asking them to return the completed questionnaire. Approval from the Ethics Committee of the University of Basel (EKBB, Basel, No. 258/12) was conferred. The study was designed according to the Guidelines for Good Clinical Practice of the Declaration of Helsinki (17) and the manuscript conforms to The Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) Guidelines (18).
Measurements
Retinal Microcirculation
Retinal vessels were assessed using a fundus camera (Topcon) and an advanced image processing unit (Visualis 3.1, Imedos Systems, Jena, Germany). This technique allows a non-invasive and semi-automated measurement of retinal vessel diameters. The method has been described elsewhere (16). Briefly, two valid images from the retina of the left and the right eye were taken at an angle of 45° with the optic disc in the center. Retinal vessel diameters were estimated to central retinal arteriolar (CRAE) and central retinal venular diameter equivalents (CRVE) applying the Parr-Hubbard formula (19). The AVR was calculated from CRAE and CRVE. CRAE and CRVE were presented in μm. One measuring unit assigns one μm in the Gullstrand‘s normal eye. Reproducibility for retinal vessel analysis is high with an interclass coefficient for CRAE of r = 0.94 and a coefficient of variation of about 2% in young children (20).
Large Artery Stiffness
PWV serves as a well-established and validated indicator of arterial stiffness (21). The assessment of PWV was performed using the non-invasive and validated oscillometric Mobil-O-Graph Monitor (I.E.M. GmbH, Germany) with integrated ARCSolver software (22–24). PWV was achieved in a sitting position and appropriate small-sized cuffs were settled on the left upper arm. After a resting period of 5 min, a blood pressure measurement was performed, which ensured a calibration with systolic BP. Two measurements of pulse wave analysis followed. After checking every measurement for erroneous values, the mean of two valid measurements was used for further analysis. Data on the validity for use of the Mobil-O-Graph in children has previously been published (5, 25).
Anthropometric Parameters and Physical Fitness
Anthropometric measurements and physical fitness assessments have been explained in detail elsewhere (16). Briefly, body height and weight (InBody 170 Biospace device; InBody Co., Seoul, Korea) were measured in light sport clothes without wearing shoes, and BMI was calculated. The InBody device has been validated in school-aged children and correlates strongly with the measurement of dual-energy X-ray absorptiometry (26). BP was assessed five times using an automated oscillograph (Oscillomate, CAS Medical Systems, Branford, CT, USA) after 5 min of rest and based on the recommendations of the American Heart Association. Physical fitness was objectively measured by the validated 20-m shuttle run test (27, 28).
Questionnaire
Parents were asked to fill in a questionnaire regarding their SES, migration background and parental lifestyle. Questionnaire items were included from our previous study (7) and translated into the seven most spoken languages in Switzerland.
Socioeconomic Status
SES included household income and parental educational level. Household income was determined as low (under CHF 5000/month), medium (CHF 5000-9000/month) and high (over CHF 9000/month) income. Parental educational level referred to the highest school level completed by at least one parent. A low educational level was defined as both parents having/ not having completed compulsory school education, whereas neither of them absolved a vocational training. A medium educational level was determined as at least one parent having completed compulsory school education and vocational training. A high educational level was defined as at least one parent having completed high-school education with or without tertiary education.
Migration Background
Children were categorized into children with two-sided non-European migration background (two non-European parents), migrants with one-sided European migration background (only one non-European parent) or without migration background (both parents are European).
Parental Lifestyle
Parental lifestyle consisted of parental PA level and smoking status. Parental PA was categorized into three groups. Low PA was determined as both parents never being physically active or no more than once a week. Medium PA was defined as at least one parent being physically active twice a week. High PA was defined as at least one parent being physically active several times per week or on a daily basis. Additionally, parents were asked if they were smoker, or non-smoker.
Statistical Analysis
Univariate analysis of covariate (ANCOVA) was used to analyse the association of household income, educational level, parental PA level and smoking status. Different models were fitted to adjust for age and sex as well as household income, educational level and parental lifestyle. Bonferroni post hoc testing was conducted to reveal the direction of the results. Additionally, we applied sensitivity analysis to adjust for further potential confounders. For quantitative analysis of parental PA categories and smoking status, bivariate analysis was performed. To indicate the amount of uncertainty the measurement of effect presents 95% confidence intervals (CI) and a two-sided level of significance of p = 0.05 denotes statistical significance. All analyses were performed using an up-to-date version of Stata 15 (StataCorp LP, College Station, TX, USA). The sample size of the study was given by the expected large number of children and parents giving their consent and was based on calculations of our previous smaller scale study (7, 20). In this study conducted by Imhof et al., we assumed a moderate effect size for the influence of a physical fitness performance on retinal vessel diameters in children. The sample size calculated with the software G-Power using F-tests (f = 0.25, power = 0.90% and 5% level of significance) was estimated to be ~290 children in total.
Results
Population characteristics are presented in Table 1. In our cohort, 3,068 children received an invitation and informed consent to participate. From 1,690 children with written consent from their parents, 221 children were ill at the day of examination. As can be seen from the flow diagram Figure 1, 833 children eventually had complete data from the medical screening and the returned questionnaires. Age, body weight and height, body fat, BMI and physical fitness data of the 636 excluded children are presented in Supplementary Table 1. Excluded children had lower fitness levels compared to children included in the study.
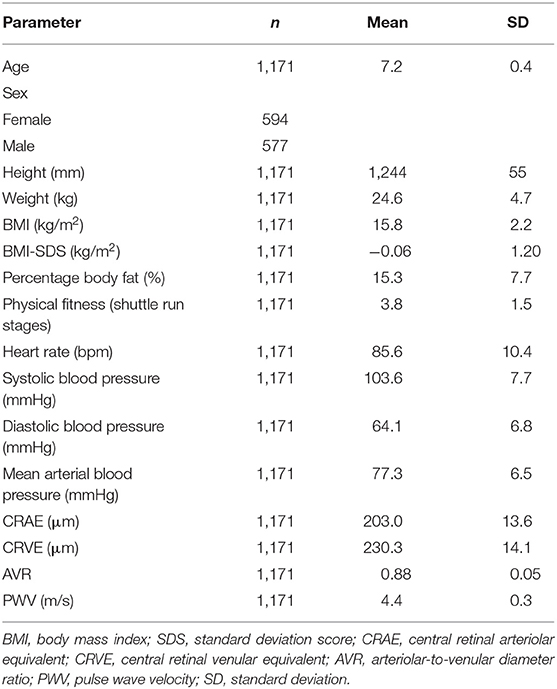
Table 1. Population characteristics.
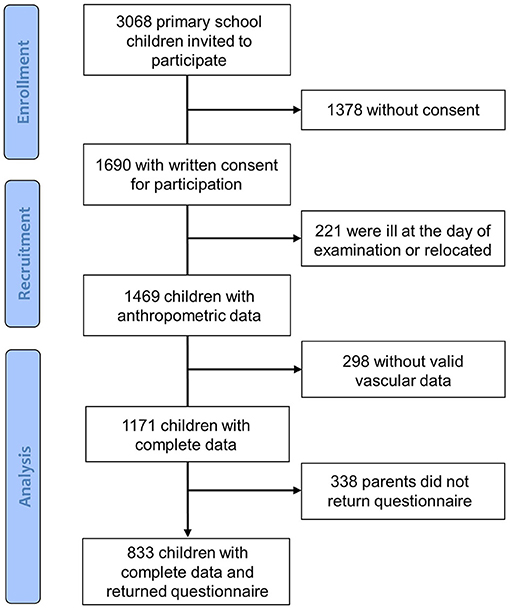
Figure 1. Flow diagram.
Analysis of Covariance
The results for differences in group-categories are shown in Table 2.
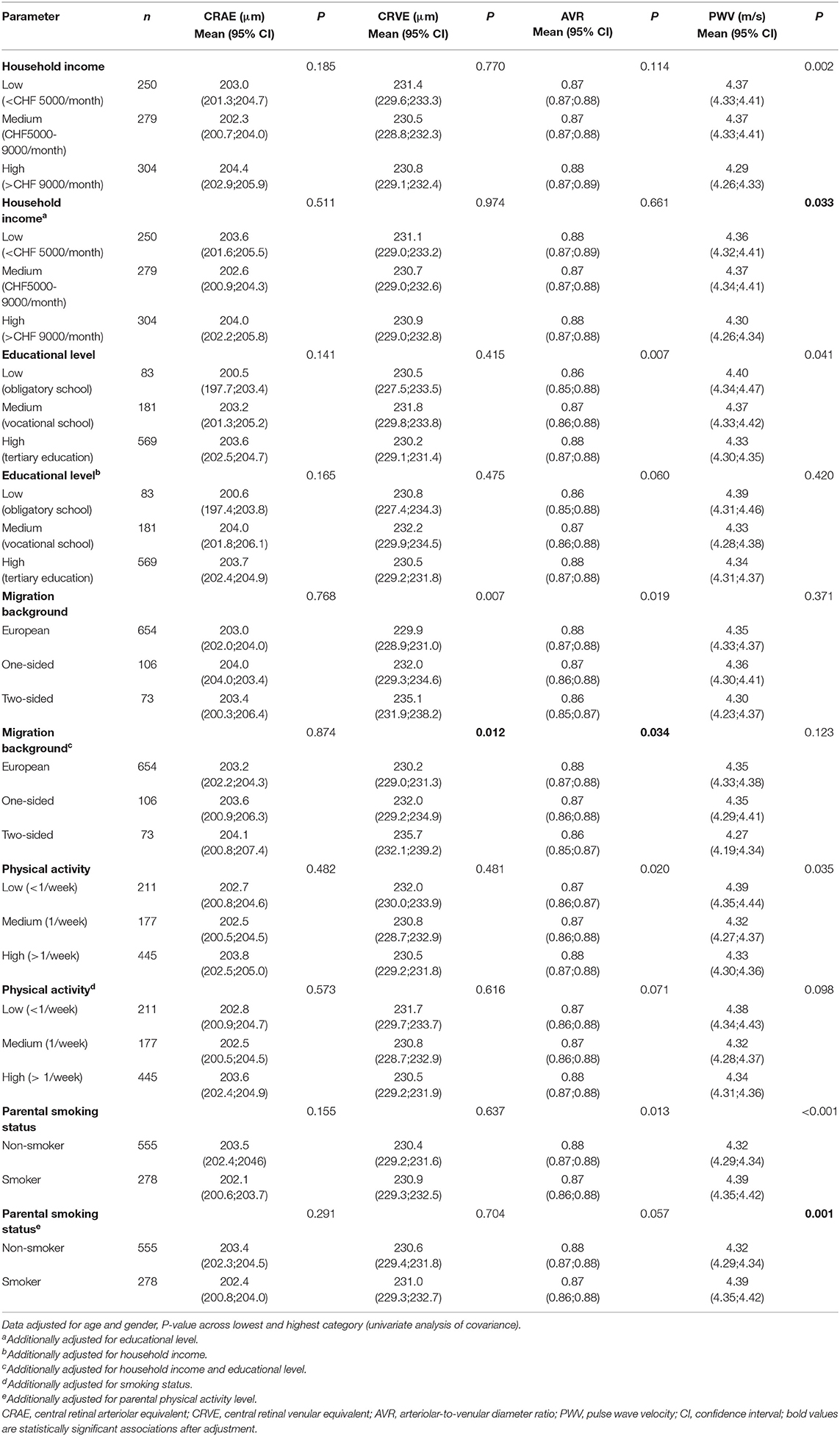
Table 2. Retinal vessel diameters and pulse wave velocity in relation to categories of household income, education level, migration background, parental smoking and physical activity behavior.
Socioeconomic Status
Thirty percentage (n = 250) of children were in the group with low, 33% (n = 279) with medium, and 37% (n = 304) with high household income. Eleven percentage (n = 83) were children with low, 22% (n = 181) with medium, and 67% (n = 569) with highly educated parents. Children with low household income parents had a higher PWV compared to children with high household income parents, also after adjustment for educational level (p = 0.033). Retinal vessel diameters were not associated with household income. Lower parental educational level was associated with a lower AVR (p = 0.007) and higher PWV (p = 0.041), but not independent of household income.
Migration Background
In our cohort, 9% (n = 73) of children had two-sided non-European parents, 13% (n = 106) had one-sided non-European parents and in 78% (n = 399) of children both parents were European.
Children with a European background showed narrower CRVE (p = 0.012) and higher AVR (p = 0.034) compared to non-European children, independent of household income and parental education. European migration background was not associated with arterial stiffness.
Parental Lifestyle
Based on parental PA level, 25% (n = 211) were classified as parents with a low PA level, 21% (n = 177) as medium and 54% (n = 445) as parents with a high PA level. Based on parental smoking status, 67% (n = 555) were non-smoking parents.
Higher parental PA level was related to higher AVR (p = 0.020) and lower PWV (p = 0.035), but not after adjustment for parental smoking status. Parental smoking status was associated with a lower AVR (p = 0.013), but not independent of parental PA level. Children with smoking parents had a higher PWV compared to children with non-smoking parents (p = 0.001), also after adjustment for potential confounders. Bivariate analysis illustrated that microvascular AVR increased according to increasing parental PA level and a non-smoking status (p < 0.001) (Figure 2).
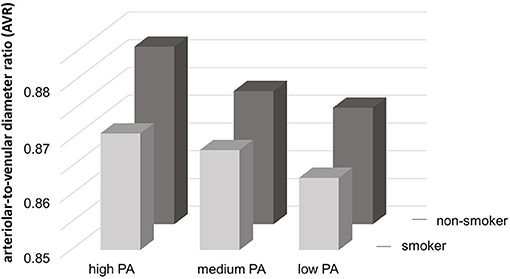
Figure 2. Interrelation between AVR and parental physical activity categories and smoking status. PA, physical activity.
Association With Parental Gender
Mother's and Father's educational level, migration background, smoking and PA behavior are shown separately in Supplementary Table 2. As a main result, children with a mother of high education had a higher AVR (p = 0.001) due to wider arterioles, independent of household income. The educational level of the father was not associated with childhood vascular health. Children with a European mother had a higher AVR (<0.001) due to narrower venules (p = 0.001) compared to children with a two- or one-sided non-European mother independent of household income and educational level. The migration background of the father was not independently associated with childhood vascular health. In children with high physically active mothers, retinal microvascular AVR was higher (p = 0.020) independent of parental smoking status. The PA level of the father was not associated with childhood vascular health. However, smoking status of the father was associated with an unfavorable lower AVR (p = 0.044) and a higher PWV (p = 0.001) independent of parental PA levels.
Discussion
Our study demonstrated several detrimental associations of socioeconomic and migration status as well as parental lifestyle with macro- and microvascular health in young children.
The influence of parental lifestyle on vascular phenotype was evident examining parental PA and smoking status with both, retinal vessel diameters and PWV. Children with smoking parents had higher arterial stiffness, independent of parental PA level. The analyses of the interrelation between parental PA categories and smoking status with microvascular AVR demonstrate the additive deleterious effects of parental physical inactivity and smoking on the microvascular phenotype of the children (Figure 2). Children with smoking and low physically active parents showed the lowest AVR in retinal microcirculation.
Parental PA levels and smoking status affect the vascular phenotype in young children. It has previously been shown that parental PA and perceptions of competence are associated with parental support for children's PA and therefore, for children's PA at home (29, 30). This could be one explanation for the association of parental PA level with vascular health in our study. In addition, there is evidence that childhood exposure of environmental tobacco smoke is associated with vascular functional impairments in adulthood (14, 15). In line with our results, a previous study demonstrated that passive smoking is associated to attenuated endothelial dysfunction in 11-year old children (31). Vascular alterations are related to impaired arterial vasodilatation. Arterial dilatation is mediated in large part by the release and bioavailability of nitric oxide. Our findings suggest that the lower AVR and higher arterial stiffness in smoking-exposed children may be due to the interaction of smoke particles with the nitric oxide pathway.
In our cohort of young children, higher household income was independently associated with lower arterial stiffness. The Young Finns study previously reported that childhood SES, defined as annual household income and years of parental education, is inversely associated with PWV in adulthood (32). Previous studies have shown that parental educational level seems to contribute to a higher prevalence of childhood obesity (9), elevated BP (10, 11) and sedentary behavior (7, 12). Lower maternal education has been associated with higher blood pressure in 6 year old children (11). However, no relationship between maternal education and arterial stiffness was found (11). In line with previous findings, parental education was not independently associated with PWV in our cohort. Our results show that high maternal education is related to favorable microvascular health (wider CRAE and higher AVR). Interestingly, maternal SES and lifestyle behavior was primarily associated with vascular health of children. An exception was seen for smoking status of the father which was independently association with micro- and macrovascular alterations of children. In adults, it has been shown that narrower CRAE and wider CRVE as well as higher arterial stiffness are predictors for increased risk of CV disease (1, 33). Therefore, disadvantaged SES may be an important influencing factor for the development of CV disease later in life.
With respect to migration background, European children had narrower CRVE and a higher AVR compared to non-European children. Similar results were found in a previous smaller-sized study on migration status and retinal microcirculation (7). In our cohort, no association of migration background and PWV was observed. There is evidence that migration background is associated with CV risk factors such as childhood obesity and sedentary behavior (7, 9, 12). We recently showed that childhood obesity and elevated blood pressure are related to retinal vessel alterations and arterial stiffness in this cohort of children (5). Based on our findings, we assumed that both micro- and macrovascular beds give separate clinically relevant information on health disadvantaged of children with migration background.
Some limitations have to be discussed. Our cross-sectional study is associative in nature and thus no differentiation in terms of causality can be made. Causal associations of vascular alterations with the development of CV disease in adulthood have to be verified by a longer-term follow up study. Our study was designed in a school setting and 45% of parents did not give consent for participation. Oftentimes parents find it difficult to follow instructions and to fully comprehend the content of the questionnaire and may therefore have decided not to participate (34). The low participation rates in questionnaire-based surveys are common limitations (34, 35). We were not able to compare participants with non-participants with respect to parental lifestyle and SES. However, children who did not participate in the medical screening and did not have a completed questionnaire had a similar BMI, but a lower physical fitness compared to those participating. The risk of a selection bias was therefore considered to be moderate. The oscillometric measurement with the Mobil-O-Graph device to estimate PWV is based on a calibration with systolic blood pressure. The assessment is thus associated with level of current systolic blood pressure. The assessment of PWV in large cohort of school children has been shown to be a validated approach (5). We refrained from additionally adjusting for systolic blood pressure in our statistical models to avoid over-adjustment. Our findings are related to a predominant Caucasian population with a small percentage of other ethnical groups. We have therefore chosen to characterize our population by looking at non-European migration background. Future studies have to investigate the association of SES, migration background and parental lifestyle with vascular health in other ethnic groups and populations from different countries. One strength of our study is the large sample size and the limited age range of young children. During childhood, mirco- and macrovascular function and structure continuously develop, and especially during puberty, age adaptations occur rapidly. Investigating different vascular beds in a large sample of children at the same age therefore reduces a developmental impact of our findings. Future studies may still investigate the association of SES, migration background and parental lifestyle with vascular health in a wider age range from infancy to adolescence to account for the dynamic pattern of small and large vessel development during childhood.
Conclusion
Parental PA has been found to be associated with better micro- and macrovascular health but not independent of parental smoking status. It appears that parental smoking may mitigate the positive association of parental PA on childhood vascular health. Parental smoking was itself independently associated with impaired large artery stiffness in children. Cessation of parental smoking therefore seems key to improve childhood vascular health. Prospective follow-up studies will have to prove if cessation of parental smoking can improve CV outcome in offspring long-term. SES and migration background also affect micro-and macrovascular impairments early in life. Primary treatment strategies will have to address reduction of socioeconomic barriers. Family-based interventions targeting cessation of parental smoking, increase of parental PA, and reduction of socioeconomic barriers may be effective means to counteract the development of CV risk and disease in offspring and during lifespan.
Data Availability Statement
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
Ethics Statement
The studies involving human participants were reviewed and approved by Ethics Committee of the University of Basel (EKBB, Basel, No. 258/12). Written informed consent to participate in this study was provided by the participants' legal guardian/next of kin.
Author Contributions
SK planned and conducted the study, collected data, performed the statistical analysis, prepared and revised the manuscript. KE designed the study and revised the manuscript. JG collected data and revised the manuscript. LS, GL, and CH interpreted data and revised the manuscript. LZ designed the study and revised the manuscript. HH conceptualized and designed the study, discussed the statistical analysis, prepared and critically reviewed the manuscript. All authors approved the final manuscript as submitted and agreed to be accountable for all aspects of the work.
Conflict of Interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Acknowledgments
The authors of this manuscript thank the children, as well as their parents and teachers, and the heads of schools, who participated in this study. We also would like to acknowledge the support and cooperation of the Cantonal Office of Sport of Basel-Stadt and the Department of Education of Basel-Stadt.
Supplementary Material
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fpubh.2021.610268/full#supplementary-material
References
1. Mitchell GF, Hwang S-J, Vasan RS, Larson MG, Pencina MJ, Hamburg NM, et al. Arterial stiffness and cardiovascular events: the Framingham Heart Study. Circulation. (2010) 121:505–11. doi: 10.1161/CIRCULATIONAHA.109.886655
2. Vlachopoulos C, Aznaouridis K, Stefanadis C. Prediction of cardiovascular events and all-cause mortality with arterial stiffness: a systematic review and meta-analysis. J Am Coll Cardiol. (2010) 55:1318–27. doi: 10.1016/j.jacc.2009.10.061
3. Ikram MK, de Jong FJ, Bos MJ, Vingerling JR, Hofman A, Koudstaal PJ, et al. Retinal vessel diameters and risk of stroke: the Rotterdam Study. Neurology. (2006) 66:1339–43. doi: 10.1212/01.wnl.0000210533.24338.ea
4. Wang JJ, Rochtchina E, Liew G, Tan AG, Wong TY, Leeder SR, et al. The long-term relation among retinal arteriolar narrowing, blood pressure, and incident severe hypertension. Am J Epidemiol. (2008) 168:80–8. doi: 10.1093/aje/kwn100
5. Köchli S, Endes K, Steiner R, Engler L, Infanger D, Schmidt-Trucksäss A, et al. Obesity, high blood pressure, and physical activity determine vascular phenotype in young children. Hypertens Dallas Tex. (2019) 73:153–61. doi: 10.1161/HYPERTENSIONAHA.118.11872
6. Drenowatz C, Eisenmann JC, Pfeiffer KA, Welk G, Heelan K, Gentile D, et al. Influence of socio-economic status on habitual physical activity and sedentary behavior in 8- to 11-year old children. BMC Public Health. (2010) 10:214. doi: 10.1186/1471-2458-10-214
7. Imhof K, Faude O, Donath L, Bean-Eisenhut S, Hanssen H, Zahner L. The association of socio-economic factors with physical fitness and activity behaviours, spinal posture and retinal vessel parameters in first graders in urban Switzerland. J Sports Sci. (2016) 34:1271–80. doi: 10.1080/02640414.2015.1109703
8. Muthuri SK, Onywera VO, Tremblay MS, Broyles ST, Chaput J-P, Fogelholm M, et al. Relationships between parental education and overweight with childhood overweight and physical activity in 9–11 year old children: results from a 12-country study. PLoS ONE. (2016) 11:e0147746. doi: 10.1371/journal.pone.0147746
9. Murer SB, Saarsalu S, Zimmermann J, Herter-Aeberli I. Risk factors for overweight and obesity in Swiss primary school children: results from a representative national survey. Eur J Nutr. (2016) 55:621–9. doi: 10.1007/s00394-015-0882-5
10. van den Berg G, van Eijsden M, Galindo-Garre F, Vrijkotte TGM, Gemke RJBJ. Explaining socioeconomic inequalities in childhood blood pressure and prehypertension: the ABCD study. Hypertension. (2013) 61:35–41. doi: 10.1161/HYPERTENSIONAHA.111.00106
11. Bouthoorn SH, Van Lenthe FJ, De Jonge LL, Hofman A, Van Osch-Gevers L, Jaddoe VWV, et al. Maternal educational level and blood pressure, aortic stiffness, cardiovascular structure and functioning in childhood: the generation R study. Am J Hypertens. (2014) 27:89–98. doi: 10.1093/ajh/hpt180
12. Ebenegger V, Marques-Vidal P-M, Nydegger A, Laimbacher J, Niederer I, Bürgi F, et al. Independent contribution of parental migrant status and educational level to adiposity and eating habits in preschool children. Eur J Clin Nutr. (2011) 65:210–8. doi: 10.1038/ejcn.2010.248
13. Leary SD, Smith GD, Rogers IS, Reilly JJ, Wells JC, Ness AR. Smoking during pregnancy and offspring fat and lean mass in childhood. Obes Silver Spring Md. (2006) 14:2284–93. doi: 10.1038/oby.2006.268
14. Juonala M, Magnussen CG, Raitakari OT. Parental smoking produces long-term damage to vascular function in their children. Curr Opin Cardiol. (2013) 28:569–74. doi: 10.1097/HCO.0b013e3283642882
15. Nagel G, Arnold FJ, Wilhelm M, Link B, Zoellner I, Koenig W. Environmental tobacco smoke and cardiometabolic risk in young children: results from a survey in south-west Germany. Eur Heart J. (2009) 30:1885–93. doi: 10.1093/eurheartj/ehp180
16. Endes K, Köchli S, Zahner L, Hanssen H. Exercise and arterial modulation in children: the EXAMIN YOUTH study. Front Physiol. (2019) 10:43. doi: 10.3389/fphys.2019.00043
17. World Medical Association. World Medical Association Declaration of Helsinki: ethical principles for medical research involving human subjects. JAMA. (2013) 310:2191–4. doi: 10.1001/jama.2013.281053
18. von Elm E, Altman DG, Egger M, Pocock SJ, Gøtzsche PC, Vandenbroucke JP, et al. The Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) statement: guidelines for reporting observational studies. Lancet Lond Engl. (2007) 370:1453–7. doi: 10.1016/S0140-6736(07)61602-X
19. Hubbard LD, Brothers RJ, King WN, Clegg LX, Klein R, Cooper LS, et al. Methods for evaluation of retinal microvascular abnormalities associated with hypertension/sclerosis in the Atherosclerosis Risk in Communities Study. Ophthalmology. (1999) 106:2269–80. doi: 10.1016/S0161-6420(99)90525-0
20. Imhof K, Zahner L, Schmidt-Trucksäss A, Faude O, Hanssen H. Influence of physical fitness and activity behavior on retinal vessel diameters in primary schoolchildren. Scand J Med Sci Sports. (2016) 26:731–8. doi: 10.1111/sms.12499
21. Wilkinson IB, Fuchs SA, Jansen IM, Spratt JC, Murray GD, Cockcroft JR, et al. Reproducibility of pulse wave velocity and augmentation index measured by pulse wave analysis. J Hypertens. (1998) 16:2079–84. doi: 10.1097/00004872-199816121-00033
22. Wassertheurer S, Kropf J, Weber T, van der Giet M, Baulmann J, Ammer M, et al. A new oscillometric method for pulse wave analysis: comparison with a common tonometric method. J Hum Hypertens. (2010) 24:498–504. doi: 10.1038/jhh.2010.27
23. Weiss W, Gohlisch C, Harsch-Gladisch C, Tölle M, Zidek W, van der Giet M. Oscillometric estimation of central blood pressure: validation of the Mobil-O-Graph in comparison with the SphygmoCor device. Blood Press Monit. (2012) 17:128–31. doi: 10.1097/MBP.0b013e328353ff63
24. Franssen PML, Imholz BPM. Evaluation of the Mobil-O-Graph new generation ABPM device using the ESH criteria. Blood Press Monit. (2010) 15:229–31. doi: 10.1097/MBP.0b013e328339be38
25. Elmenhorst J, Hulpke-Wette M, Barta C, Dalla Pozza R, Springer S, Oberhoffer R. Percentiles for central blood pressure and pulse wave velocity in children and adolescents recorded with an oscillometric device. Atherosclerosis. (2015) 238:9–16. doi: 10.1016/j.atherosclerosis.2014.11.005
26. Lee L-W, Liao Y-S, Lu H-K, Hsiao P-L, Chen Y-Y, Chi C-C, et al. Validation of two portable bioelectrical impedance analyses for the assessment of body composition in school age children. PLoS ONE. (2017) 12:e0171568. doi: 10.1371/journal.pone.0171568
27. Bös K, Wohlmann R. Allgemeiner Sportmotorischer Test <AST 6-11> zur Diagnose der konditionellen und koordinativen Leistungsfaehigket. Sportunterricht. (1987) 36:S. 145–56.
28. van Mechelen W, Hlobil H, Kemper HC. Validation of two running tests as estimates of maximal aerobic power in children. Eur J Appl Physiol. (1986) 55:503–6. doi: 10.1007/BF00421645
29. Loprinzi PD, Trost SG. Parental influences on physical activity behavior in preschool children. Prev Med. (2010) 50:129–33. doi: 10.1016/j.ypmed.2009.11.010
30. Mutz M, Albrecht P. Parents' social status and children's daily physical activity: the role of familial socialization and support. J Child Fam Stud. (2017) 26:3026–35. doi: 10.1007/s10826-017-0808-3
31. Kallio K, Jokinen E, Raitakari OT, Hämäläinen M, Siltala M, Volanen I, et al. Tobacco smoke exposure is associated with attenuated endothelial function in 11-year-old healthy children. Circulation. (2007) 115:3205–12. doi: 10.1161/CIRCULATIONAHA.106.674804
32. Puolakka E, Pahkala K, Laitinen TT, Magnussen CG, Hutri-Kähönen N, Kähönen M, et al. Childhood socioeconomic status and arterial stiffness in adulthood: the cardiovascular risk in young Finns study. Hypertens Dallas Tex. (2017) 70:729–35. doi: 10.1161/HYPERTENSIONAHA.117.09718
33. Wang JJ, Liew G, Klein R, Rochtchina E, Knudtson MD, Klein BEK, et al. Retinal vessel diameter and cardiovascular mortality: pooled data analysis from two older populations. Eur Heart J. (2007) 28:1984–92. doi: 10.1093/eurheartj/ehm221
34. Coyne I. Research with children and young people: the issue of parental (proxy) consent. Child Soc. (2010) 24:227–37. doi: 10.1111/j.1099-0860.2009.00216.x
Keywords: parental lifestyle, socioeconomic status, migration background, arterial stiffness, retinal microcirculation
Citation: Köchli S, Endes K, Grenacher J, Streese L, Lona G, Hauser C, Deiseroth A, Zahner L and Hanssen H (2021) Socioeconomic Status and Parental Lifestyle Are Associated With Vascular Phenotype in Children. Front. Public Health 9:610268. doi: 10.3389/fpubh.2021.610268
Received: 25 September 2020; Accepted: 03 March 2021;
Published: 26 March 2021.
Edited by:
Dora Il'yasova, Georgia State University, United StatesReviewed by:
Cihad Dundar, Ondokuz Mayis University, TurkeyTelmo Pereira, Instituto Politécnico de Coimbra, Portugal
Copyright © 2021 Köchli, Endes, Grenacher, Streese, Lona, Hauser, Deiseroth, Zahner and Hanssen. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Henner Hanssen, henner.hanssen@unibas.ch