
Relationship between Cerebrospinal Fluid Matrix Metalloproteinases Levels and Brain Amyloid Deposition in Mild Cognitive Impairment

Abstract
:1. Introduction
2. Materials and Methods
2.1. Subjects
2.2. Multiplex Assay
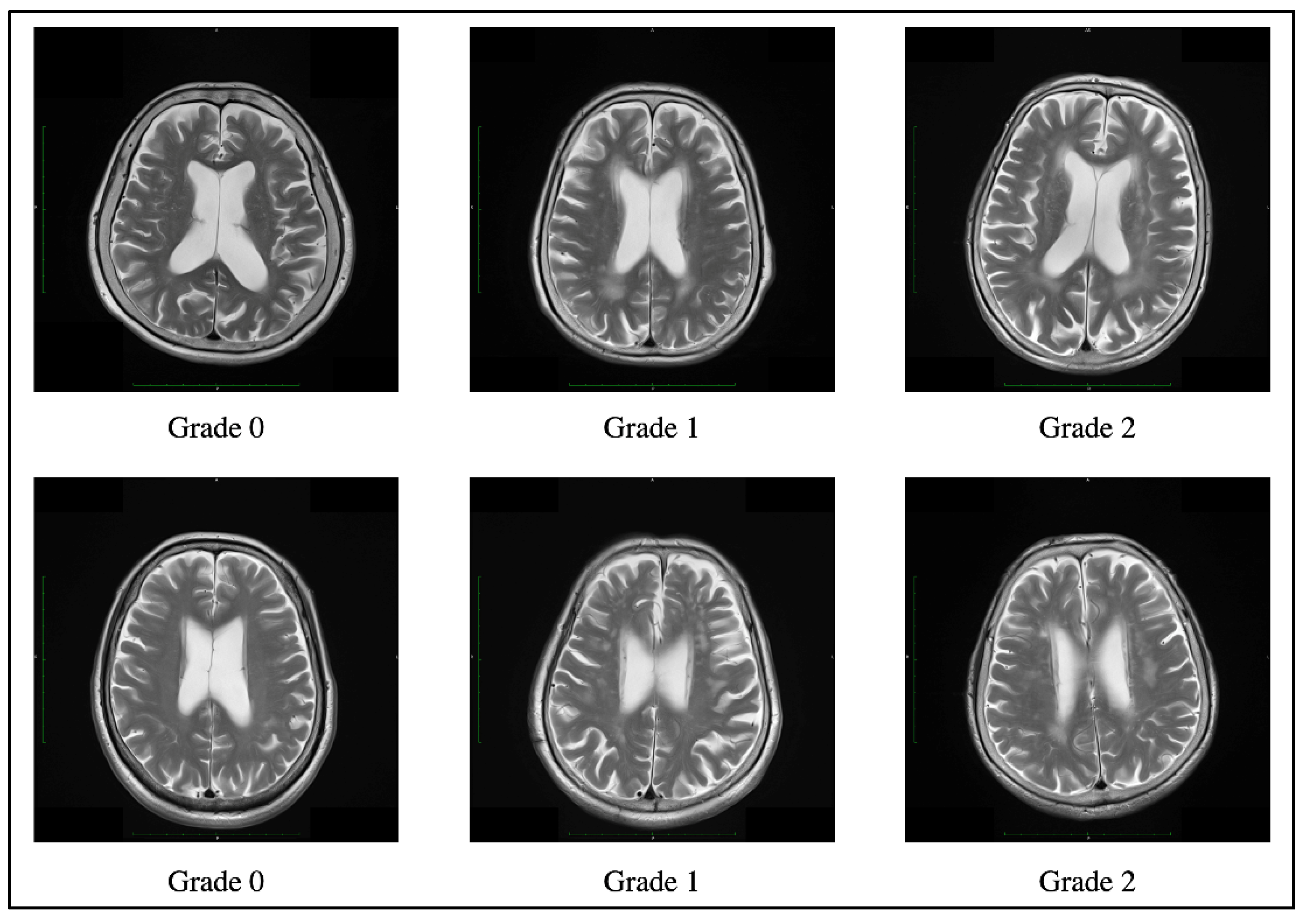
2.3. White Matter Lesion Assessment
2.4. Apolipoprotein E Phenotype
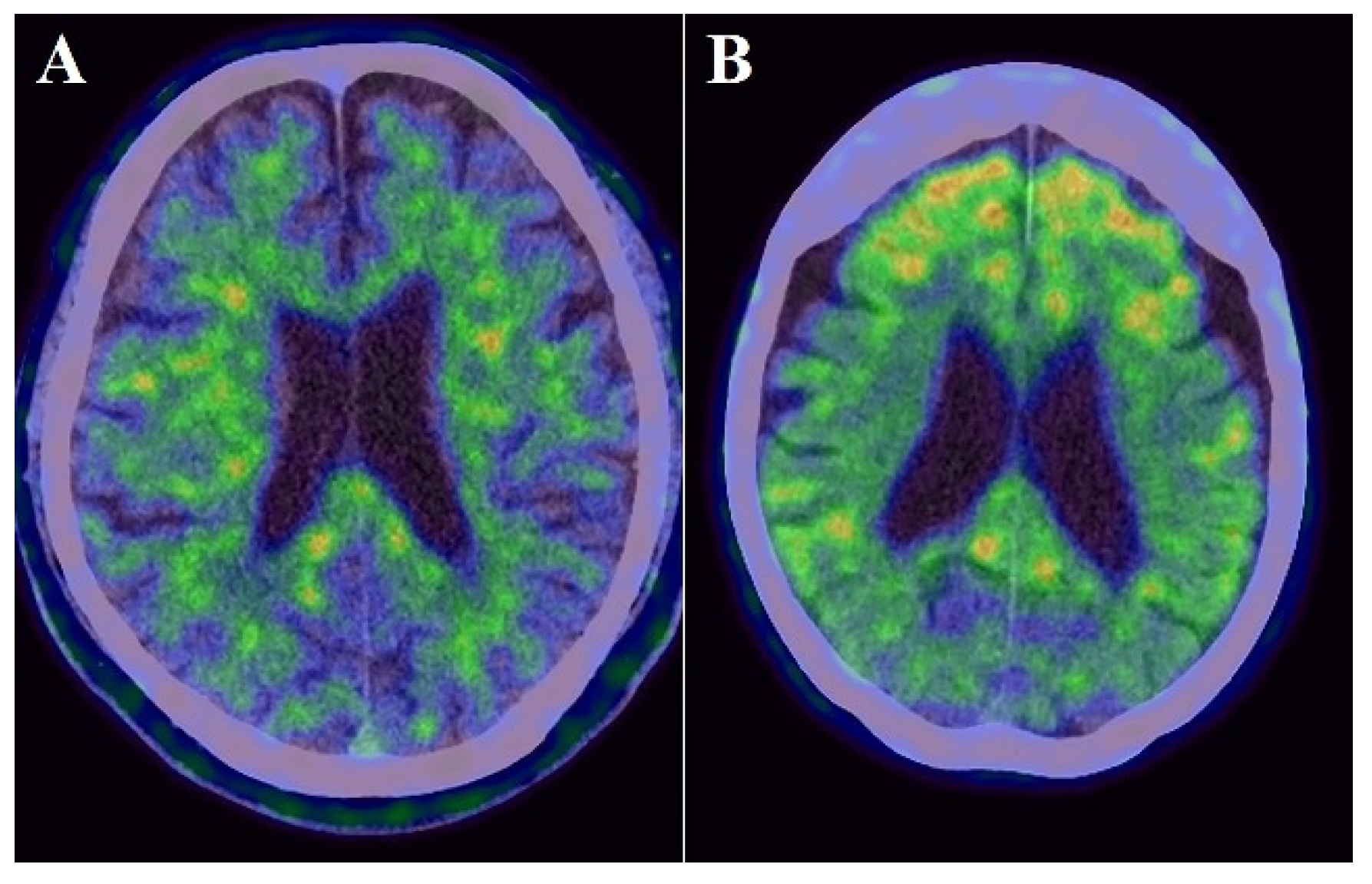
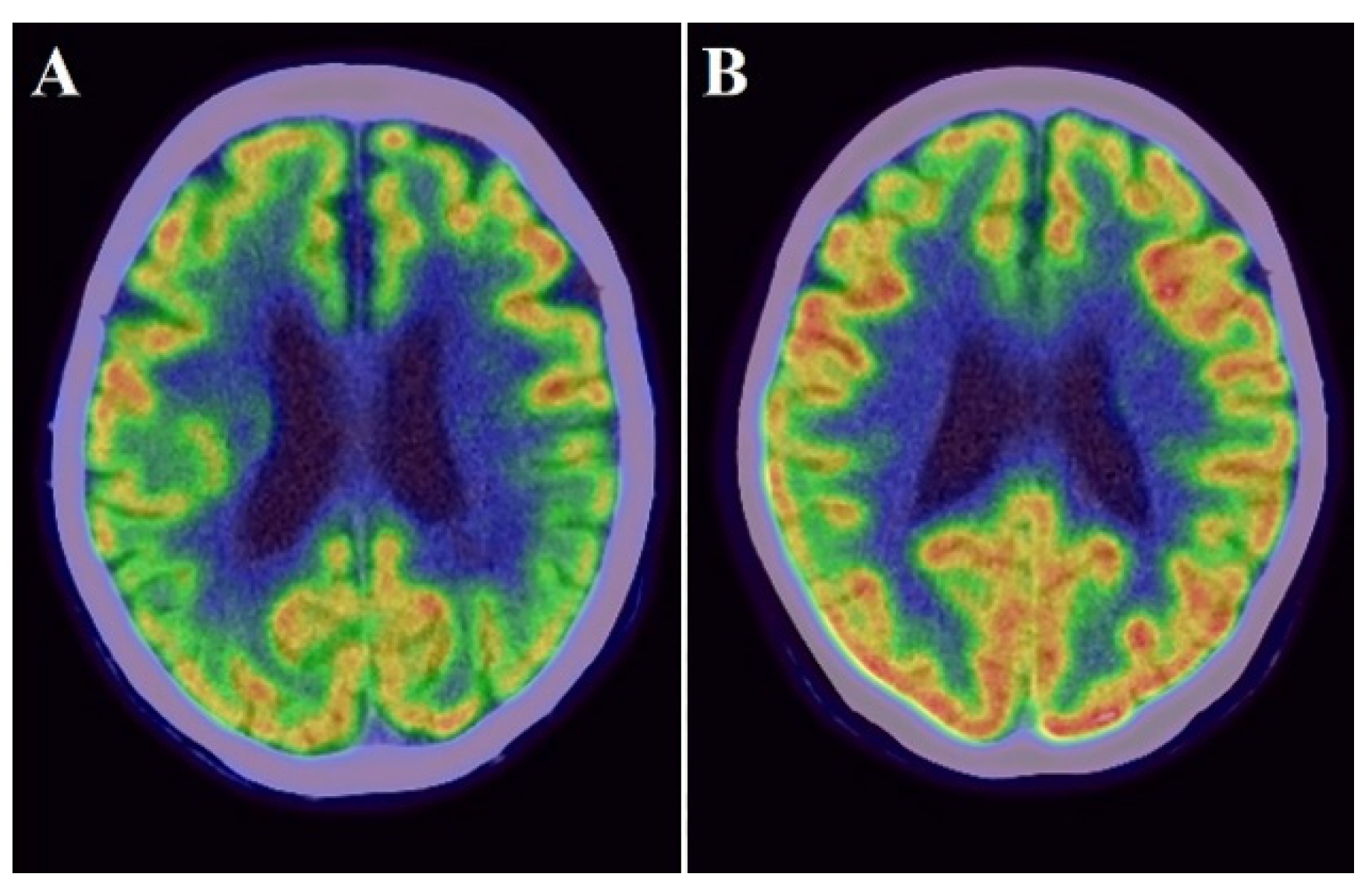
2.5. PET
2.6. Statistical Analysis
3. Results
3.1. Clinical and Demographic Characteristics
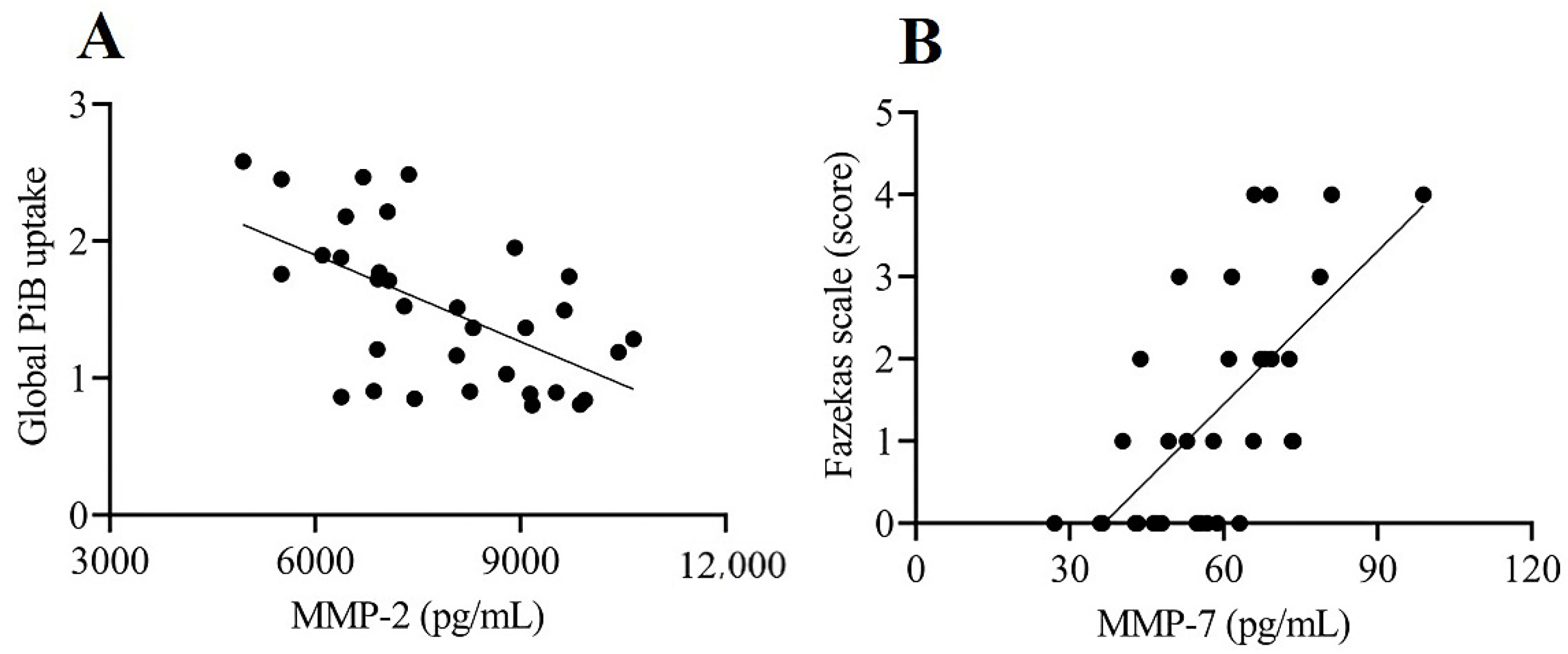
3.2. Relationship among CSF Levels of MMPs and TIMPs and PiB and FDG Uptake Values and Fazekas Scale Scores
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
| Aβ | amyloid β |
| AD | Alzheimer’s disease |
| APOE | apolipoprotein E |
| BBB | blood–brain barrier |
| CI | confidence interval |
| CSF | cerebrospinal fluid |
| CT | computed tomography |
| F | female |
| FDG | 18F-fluorodeoxyglucose |
| FL | frontal lobe |
| M | male |
| MCI | mild cognitive impairment |
| MMP | matrix metalloproteinase |
| MMSE | Mini-Mental State Examination |
| MRI | magnetic resonance imaging |
| PET | positron emission tomography |
| PiB | 11C-Pittsburgh Compound B |
| PL-TL | parietotemporal lobe |
| POSC | posterior cingulate gyrus |
| ROI | region of interest |
| SD | standard deviation |
| SUVR | standardized uptake value ratio |
| TIMP | tissue inhibitor of metalloproteinase |
| WML | white matter lesion |
References
- Yong, V.W.; Power, C.; Forsyth, P.; Edwards, D.R. Metalloproteinases in biology and pathology of the nervous system. Nat. Rev. Neurosci. 2001, 2, 502–511. [Google Scholar] [CrossRef] [PubMed]
- Massova, I.; Kotra, L.P.; Fridman, R.; Mobashery, S. Matrix metalloproteinases: Structures, evolution, and diversification. FASEB J. 1998, 12, 1075–1095. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rosenberg, G.A. Matrix metalloproteinases and their multiple roles in neurodegenerative diseases. Lancet Neurol. 2009, 8, 205–216. [Google Scholar] [CrossRef]
- Rivera, S.; García-González, L.; Khrestchatisky, M.; Baranger, K. Metalloproteinases and their tissue inhibitors in Alzheimer’s disease and other neurodegenerative disorders. Cell. Mol. Life Sci. 2019, 76, 3167–3191. [Google Scholar] [CrossRef]
- Bruno, M.A.; Mufson, E.J.; Wuu, J.; Cuello, A.C. Increased matrix metalloproteinase 9 activity in mild cognitive impairment. J. Neuropathol. Exp. Neurol. 2009, 68, 1309–1318. [Google Scholar] [CrossRef] [PubMed]
- Peress, N.; Perillo, E.; Zucker, S. Localization of tissue inhibitor of matrix metalloproteinases in Alzheimer’s disease and normal brain. J. Neuropathol. Exp. Neurol. 1995, 54, 16–22. [Google Scholar] [CrossRef] [PubMed]
- Yin, K.J.; Cirrito, J.R.; Yan, P.; Hu, X.; Xiao, Q.; Pan, X.; Bateman, R.; Song, H.; Hsu, F.F.; Turk, J.; et al. Matrix metalloproteinases expressed by astrocytes mediate extracellular amyloid-beta peptide catabolism. J. Neurosci. 2006, 26, 10939–10948. [Google Scholar] [CrossRef]
- Horstmann, S.; Budig, L.; Gardner, H.; Koziol, J.; Deuschle, M.; Schilling, C.; Wagner, S. Matrix metalloproteinases in peripheral blood and cerebrospinal fluid in patients with Alzheimer’s disease. Int. Psychogeriatr. 2010, 22, 966–972. [Google Scholar] [CrossRef]
- Zlokovic, B.V. Neurovascular pathways to neurodegeneration in Alzheimer’s disease and other disorders. Nat. Rev. Neurosci. 2011, 12, 723–738. [Google Scholar] [CrossRef]
- Zlokovic, B.V. The blood-brain barrier in health and chronic neurodegenerative disorders. Neuron 2008, 57, 178–201. [Google Scholar] [CrossRef] [Green Version]
- Feng, S.; Cen, J.; Huang, Y.; Shen, H.; Yao, L.; Wang, Y.; Chen, Z. Matrix metalloproteinase-2 and -9 secreted by leukemic cells increase the permeability of blood-brain barrier by disrupting tight junction proteins. PLoS ONE 2011, 6, e20599. [Google Scholar] [CrossRef]
- Rempe, R.G.; Hartz, A.M.S.; Bauer, B. Matrix metalloproteinases in the brain and blood-brain barrier: Versatile breakers and makers. J. Cereb. Blood Flow Metab. 2016, 36, 1481–1507. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Brkic, M.; Balusu, S.; Van Wonterghem, E.; Gorlé, N.; Benilova, I.; Kremer, A.; Van Hove, I.; Moons, L.; De Strooper, B.; Kanazir, S.; et al. Amyloid β oligomers disrupt Blood-CSF barrier integrity by activating matrix metalloproteinases. J. Neurosci. 2015, 35, 12766–12778. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wang, X.X.; Tan, M.S.; Yu, J.T.; Tan, L. Matrix metalloproteinases and their multiple roles in Alzheimer’s disease. BioMed Res. Int. 2014, 2014, 908636. [Google Scholar] [CrossRef]
- Kimura, N.; Aikawa, M.; Etou, K.; Aso, Y.; Matsubara, E. Association between matrix metalloproteinases, their tissue inhibitor and white matter lesions in mild cognitive impairment. Curr. Alzheimer Res. 2020, 17, 547–555. [Google Scholar] [CrossRef]
- Hanzel, C.E.; Iulita, M.F.; Eyjolfsdottir, H.; Hjorth, E.; Schultzberg, M.; Eriksdotter, M.; Cuello, A.C. Analysis of matrix metallo-proteases and the plasminogen system in mild cognitive impairment and Alzheimer’s disease cerebrospinal fluid. J. Alzheimers Dis. 2014, 40, 667–678. [Google Scholar] [CrossRef]
- Whelan, C.D.; Mattsson, N.; Nagle, M.W.; Vijayaraghavan, S.; Hyde, C.; Janelidze, S.; Stomrud, E.; Lee, J.; Fitz, L.; Samad, T.A.; et al. Multiplex proteomics identifies novel CSF and plasma biomarkers of early Alzheimer’s disease. Acta Neuropathol. Commun. 2019, 7, 169. [Google Scholar] [CrossRef]
- Duits, F.H.; Hernandez-Guillamon, M.; Montaner, J.; Goos, J.D.; Montañola, A.; Wattjes, M.P.; Barkhof, F.; Scheltens, P.; Teunissen, C.E.; van der Flier, W.M. Matrix metalloproteinases in Alzheimer’s disease and concurrent cerebral microbleeds. J. Alzheimers Dis. 2015, 48, 711–720. [Google Scholar] [CrossRef]
- Bjerke, M.; Zetterberg, H.; Edman, Å.; Blennow, K.; Wallin, A.; Andreasson, U. Cerebrospinal fluid matrix metalloproteinases and tissue inhibitor of metalloproteinases in combination with subcortical and cortical biomarkers in vascular dementia and Alzheimer’s disease. J. Alzheimers Dis. 2011, 27, 665–676. [Google Scholar] [CrossRef]
- Tuna, G.; Yener, G.G.; Oktay, G.; İşlekel, G.H.; Kİrkalİ, F.G. Evaluation of matrix metalloproteinase-2 (MMP-2) and -9. J. Alzheimers Dis. 2018, 66, 1265–1273. [Google Scholar] [CrossRef] [PubMed]
- Ma, Y.; Zhang, S.; Li, J.; Zheng, D.M.; Guo, Y.; Feng, J.; Ren, W.D. Predictive accuracy of amyloid imaging for progression from mild cognitive impairment to Alzheimer disease with different lengths of follow-up: A meta-analysis. Medicine 2014, 93, e150. [Google Scholar] [CrossRef]
- Jack, C.R., Jr.; Knopman, D.S.; Jagust, W.J.; Petersen, R.C.; Weiner, M.W.; Aisen, P.S.; Shaw, L.M.; Vemuri, P.; Wiste, H.J.; Weigand, S.D.; et al. Tracking pathophysiological processes in Alzheimer’s disease: An updated hypothetical model of dynamic biomarkers. Lancet Neurol. 2013, 12, 207–216. [Google Scholar] [CrossRef] [Green Version]
- Brun, A.; Englund, E. A white matter disorder in dementia of the Alzheimer type: A pathoanatomical study. Ann. Neurol. 1986, 19, 253–262. [Google Scholar] [CrossRef]
- Kimura, N.; Nakama, H.; Nakamura, K.; Aso, Y.; Kumamoto, T. Effect of white matter lesions on brain perfusion in Alzheimer’s disease. Dement. Geriatr. Cogn. Disord. 2012, 34, 256–261. [Google Scholar] [CrossRef]
- Wardlaw, J.M.; Smith, E.E.; Biessels, G.J.; Cordonnier, C.; Fazekas, F.; Frayne, R.; Lindley, R.I.; O’Brien, J.T.; Barkhof, F.; Benavente, O.R.; et al. Neuroimaging standards for research into small vessel disease and its contribution to ageing and neurodegeneration. Lancet Neurol. 2013, 12, 822–838. [Google Scholar] [CrossRef] [Green Version]
- Freeze, W.M.; Jacobs, H.I.L.; de Jong, J.J.; Verheggen, I.C.M.; Gronenschild, E.H.B.M.; Palm, W.M.; Hoff, E.I.; Wardlaw, J.M.; Jansen, J.F.A.; Verhey, F.R.; et al. White matter hyperintensities mediate the association between blood-brain barrier leakage and information processing speed. Neurobiol. Aging 2020, 85, 113–122. [Google Scholar] [CrossRef]
- Molgaard, C.A. Multivariate analysis of Hachinski’s Scale for discriminating senile dementia of the Alzheimer’s type from multiinfarct dementia. Neuroepidemiology 1987, 6, 153–160. [Google Scholar] [CrossRef] [PubMed]
- Fazekas, F.; Chawluk, J.B.; Alavi, A.; Hurtig, H.I.; Zimmerman, R.A. MR signal abnormalities at 1.5 T in Alzheimer’s dementia and normal aging. Am. J. Roentgenol. 1987, 149, 351–356. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gupta, V.B.; Laws, S.M.; Villemagne, V.L.; Ames, D.; Bush, A.I.; Ellis, K.A.; Lui, J.K.; Masters, C.; Rowe, C.C.; Szoeke, C.; et al. Plasma apolipoprotein E and Alzheimer disease risk: The AIBL study of aging. Neurology 2011, 76, 1091–1098. [Google Scholar] [CrossRef] [PubMed]
- Kimura, N.; Aso, Y.; Yabuuchi, K.; Ishibashi, M.; Hori, D.; Sasaki, Y.; Nakamichi, A.; Uesugi, S.; Jikumaru, M.; Sumi, K.; et al. Association of modifiable lifestyle factors with cortical amyloid burden and cerebral glucose metabolism in older adults with mild cognitive impairment. JAMA Netw. Open 2020, 3, e205719. [Google Scholar] [CrossRef] [PubMed]
- Herholz, K.; Salmon, E.; Perani, D.; Baron, J.C.; Holthoff, V.; Frölich, L.; Schönknecht, P.; Ito, K.; Mielke, R.; Kalbe, E.; et al. Discrimination between Alzheimer dementia and controls by automated analysis of multicenter FDG PET. Neuroimage 2002, 17, 302–316. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jack, C.R., Jr.; Lowe, V.J.; Senjem, M.L.; Weigand, S.D.; Kemp, B.J.; Shiung, M.M.; Knopman, D.S.; Boeve, B.F.; Klunk, W.E.; Mathis, C.A.; et al. 11C PiB and structural MRI provide complementary information in imaging of Alzheimer’s disease and amnestic mild cognitive impairment. Brain 2008, 131, 665–680. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jansen, W.J.; Ossenkoppele, R.; Knol, D.L.; Tijms, B.M.; Scheltens, P.; Verhey, F.R.; Visser, P.J.; Aalten, P.; Aarsland, D.; Alcolea, D.; et al. Prevalence of cerebral amyloid pathology in persons without dementia: A meta-analysis. JAMA 2015, 313, 1924–1938. [Google Scholar] [CrossRef] [PubMed]
- Targosz-Gajniak, M.; Siuda, J.; Ochudło, S.; Opala, G. Cerebral white matter lesions in patients with dementia—From MCI to severe Alzheimer’s disease. J. Neurol. Sci. 2009, 283, 79–82. [Google Scholar] [CrossRef] [PubMed]
- Heo, J.H.; Lee, S.T.; Kon, C.; Park, H.J.; Shim, J.Y.; Kim, M. White matter hyperintensities and cognitive dysfunction in Alzheimer disease. J. Geriatr. Psychiatr. Neurol. 2009, 22, 207–212. [Google Scholar] [CrossRef]
- Kao, Y.H.; Chou, M.C.; Chen, C.H.; Yang, Y.H. White Matter Changes in Patients with Alzheimer’s Disease and Associated Factors. J. Clin. Med. 2019, 8, 167. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Snoek-van Beurden, P.A.M.; Von den Hoff, J.W. Zymographic techniques for the analysis of matrix metalloproteinases and their inhibitors. BioTechniques 2005, 38, 73–83. [Google Scholar] [CrossRef] [Green Version]
- Backstrom, J.R.; Lim, G.P.; Cullen, M.J.; Tökés, Z.A. Matrix metalloproteinase-9 (MMP-9) is synthesized in neurons of the human hippocampus and is capable of degrading the amyloidbeta peptide. J. Neurosci. 1996, 16, 7910–7919. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yan, P.; Hu, X.; Song, H.; Yin, K.; Bateman, R.J.; Cirrito, J.R.; Xiao, Q.; Hsu, F.F.; Turk, J.W.; Xu, J.; et al. Matrix metalloproteinase-9 degrades amyloid-beta fibrils in vitro and compact plaques in situ. J. Biol. Chem. 2006, 281, 24566–24574. [Google Scholar] [CrossRef] [Green Version]
- Miners, J.S.; Baig, S.; Palmer, J.; Palmer, L.E.; Kehoe, P.G.; Love, S. Abeta-degrading enzymes in Alzheimer’s disease. Brain Pathol. 2008, 18, 240–252. [Google Scholar] [CrossRef] [PubMed]
- Mlekusch, R.; Humpel, C. Matrix metalloproteinases-2 and -3 are reduced in cerebrospinal fluid with low beta-amyloid1-42 levels. Neurosci. Lett. 2009, 466, 135–138. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Stomrud, E.; Björkqvist, M.; Janciauskiene, S.; Minthon, L.; Hansson, O. Alterations of matrix metalloproteinases in the healthy elderly with increased risk of prodromal Alzheimer’s disease. Alzheimers Res. Ther. 2010, 2, 20. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Omori, W.; Hattori, K.; Kajitani, N.; Tsuchioka, M.O.; Boku, S.; Kunugi, H.; Okamoto, Y.; Takebayashi, M. Increased matrix metalloproteinases in cerebrospinal fluids of patients with major depressive disorder and schizophrenia. Int. J. Neuropsychopharmacol. 2020, 23, 713–720. [Google Scholar] [CrossRef] [PubMed]
- Wilson, C.L.; Matrisian, L.M. Matrilysin: An epithelial matrix metalloproteinase with potentially novel functions. Int. J. Biochem. Cell Biol. 1996, 28, 123–136. [Google Scholar] [CrossRef]
- Conant, K.; McArthur, J.C.; Griffin, D.E.; Sjulson, L.; Wahl, L.M.; Irani, D.N. Cerebrospinal fluid levels of MMP-2, 7, and 9 are elevated in association with human immunodeficiency virus dementia. Ann. Neurol. 1999, 46, 391–398. [Google Scholar] [CrossRef]
- Castellazzi, M.; Ligi, D.; Contaldi, E.; Quartana, D.; Fonderico, M.; Borgatti, L.; Bellini, T.; Trentini, A.; Granieri, E.; Fainardi, E.; et al. Multiplex matrix metalloproteinases analysis in the cerebrospinal fluid reveals potential specific patterns in multiple sclerosis patients. Front Neurol. 2018, 9, 1080. [Google Scholar] [CrossRef]
- Ragin, A.B.; Wu, Y.; Ochs, R.; Du, H.; Epstein, L.G.; Conant, K.; McArthur, J.C. Marked relationship between matrix metalloproteinase 7 and brain atrophy in HIV infection. J. Neurovirol. 2011, 17, 153–158. [Google Scholar] [CrossRef] [Green Version]
- Taniguchi, M.; Matsuura, K.; Nakamura, R.; Kojima, A.; Konishi, M.; Akizawa, T. MMP-7 cleaves amyloid β fragment peptides and copper ion inhibits the degradation. Biometals 2017, 30, 797–807. [Google Scholar] [CrossRef]
- Ikonomovic, M.D.; Klunk, W.E.; Abrahamson, E.E.; Mathis, C.A.; Price, J.C.; Tsopelas, N.D.; Lopresti, B.J.; Ziolko, S.; Bi, W.; Paljug, W.R.; et al. Post-mortem correlates of in vivo PiB-PET amyloid imaging in a typical case of Alzheimer’s disease. Brain 2008, 131, 1630–1645. [Google Scholar] [CrossRef] [Green Version]
- Cummings, J.; Lee, G.; Ritter, A.; Sabbagh, M.; Zhong, K. Alzheimer’s disease drug development pipeline: 2020. Alzheimers Dement. 2020, 6, e12050. [Google Scholar] [CrossRef]
- Marasco, R.A. Current and evolving treatment strategies for the Alzheimer disease continuum. Am. J. Manag. Care 2020, 26, 167–176. [Google Scholar]
- Hwang, J.; Estick, C.M.; Ikonne, U.S.; Butler, D.; Pait, M.C.; Elliott, L.H.; Ruiz, S.; Smith, K.; Rentschler, K.M.; Mundell, C.; et al. The Role of Lysosomes in a Broad Disease-Modifying Approach Evaluated across Transgenic Mouse Models of Alzheimer’s Disease and Parkinson’s Disease and Models of Mild Cognitive Impairment. Int. J. Mol. Sci. 2019, 20, 4432. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Li, W.; Poteet, E.; Xie, L.; Liu, R.; Wen, Y.; Yang, S.-H. Regulation of matrix metalloproteinase 2 by oligomeric amyloid β protein. Brain Res. 2011, 1387, 141–148. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Boström, G.; Freyhult, E.; Virhammar, J.; Alcolea, D.; Tumani, H.; Otto, M.; Brundin, R.M.; Kilander, L.; Löwenmark, M.; Giedraitis, V.; et al. Different inflammatory signatures in Alzheimer’s disease and frontotemporal dementia cerebrospinal fluid. J. Alzheimers Dis. 2021, 81, 629–640. [Google Scholar] [CrossRef] [PubMed]
- Lorenzl, S.; Albers, D.S.; LeWitt, P.A.; Chirichigno, J.W.; Hilgenberg, S.L.; Cudkowicz, M.E.; Beal, M.F. Tissue inhibitors of matrix metalloproteinases are elevated in cerebrospinal fluid of neurodegenerative diseases. J. Neurol. Sci. 2003, 207, 71–76. [Google Scholar] [CrossRef]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Characteristic | Cohort (N = 33) |
|---|---|
| Age, mean (SD), years | 75.6 (5.4) |
| Sex (M/F) | 11:22 |
| Education level, mean (SD), years | 11.4 (1.9) |
| APOE4, no. (%) | 11 (33.3%) |
| Hypertension (%) | 20 (60.6%) |
| Diabetes (%) | 3 (9.1%) |
| Hypercholesterolemia (%) | 17 (51.5%) |
| MMSE, mean (SD), score | 24.8 (2.0) |
| FL PiB uptake, mean (SD) | 1.46 (0.55) |
| POSC PiB uptake, mean (SD) | 1.91 (0.81) |
| PL-TL PiB uptake, mean (SD) | 1.48 (0.53) |
| Global PiB uptake, mean (SD) | 1.51 (0.56) |
| Global FDG uptake, mean (SD) | 0.88 (0.08) |
| Fazekas scale, mean (SD) | 1.33 (1.41) |
| CSF Level | Global PiB Uptake | Global FDG Uptake | Fazekas Scale Score | |||
|---|---|---|---|---|---|---|
| β (95% CI) | p | β (95% CI) | p | β (95% CI) | p | |
| MMP-2 | −0.414 (−0.796, −0.032) | 0.035 1 | 0.174 (−0.247, 0.595) | 0.403 | 0.106 (−0.304, 0.517) | 0.598 |
| MMP-7 | −0.259 (−0.674, 0.156) | 0.209 | 0.105 (−0.329, 0.539) | 0.623 | 0.419 (0.036, 0.802) | 0.033 1 |
| MMP-12 | −0.139 (−0.531, 0.253) | 0.473 | −0.069 (−0.471, 0.333) | 0.724 | −0.04 (−0.43, 0.349) | 0.832 |
| TIMP-1 | −0.177 (−0.587, 0.233) | 0.382 | −0.126 (−0.547, 0.295) | 0.544 | 0.253 (−0.143, 0.649) | 0.20 |
| TIMP-2 | −0.103 (−0.519, 0.313) | 0.615 | −0.14 (−0.561, 0.282) | 0.50 | 0.166 (−0.239, 0.571) | 0.406 |
| CSF Level | FL | POSC | PL-TL | |||
|---|---|---|---|---|---|---|
| β (95% CI) | p | β (95% CI) | p | β (95% CI) | p | |
| MMP-2 | −0.376 (−0.76, 0.008) | 0.055 | −0.399 (−0.782, −0.017) | 0.041 1 | −0.476 (−0.856, −0.096) | 0.016 1 |
| MMP-7 | −0.226 (−0.64, 0.187) | 0.27 | −0.282 (−0.692, 0.128) | 0.169 | −0.303 (−0.723, 0.117) | 0.149 |
| MMP-12 | −0.147 (−0.534, 0.241) | 0.442 | −0.098 (−0.49, 0.294) | 0.611 | −0.131 (−0.532, 0.271) | 0.509 |
| TIMP-1 | −0.157 (−0.564, 0.251) | 0.435 | −0.221 (−0.626, 0.183) | 0.269 | −0.188 (−0.608, 0.231) | 0.363 |
| TIMP-2 | −0.108 (−0.52, 0.303) | 0.592 | −0.133 (−0.545, 0.28) | 0.513 | −0.068 (−0.495, 0.359) | 0.744 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Sasaki, Y.; Kimura, N.; Aso, Y.; Yabuuchi, K.; Aikawa, M.; Matsubara, E. Relationship between Cerebrospinal Fluid Matrix Metalloproteinases Levels and Brain Amyloid Deposition in Mild Cognitive Impairment. Biomolecules 2021, 11, 1496. https://0-doi-org.brum.beds.ac.uk/10.3390/biom11101496
Sasaki Y, Kimura N, Aso Y, Yabuuchi K, Aikawa M, Matsubara E. Relationship between Cerebrospinal Fluid Matrix Metalloproteinases Levels and Brain Amyloid Deposition in Mild Cognitive Impairment. Biomolecules. 2021; 11(10):1496. https://0-doi-org.brum.beds.ac.uk/10.3390/biom11101496
Chicago/Turabian StyleSasaki, Yuuki, Noriyuki Kimura, Yasuhiro Aso, Kenichi Yabuuchi, Miki Aikawa, and Etsuro Matsubara. 2021. "Relationship between Cerebrospinal Fluid Matrix Metalloproteinases Levels and Brain Amyloid Deposition in Mild Cognitive Impairment" Biomolecules 11, no. 10: 1496. https://0-doi-org.brum.beds.ac.uk/10.3390/biom11101496