The Role of Movement Analysis in Diagnosing and Monitoring Neurodegenerative Conditions: Insights from Gait and Postural Control




 , ,
, ,
Abstract
:1. Introduction
2. Section I: Quantitative Movement Analysis: From Measurement Tools to Outcome Measures
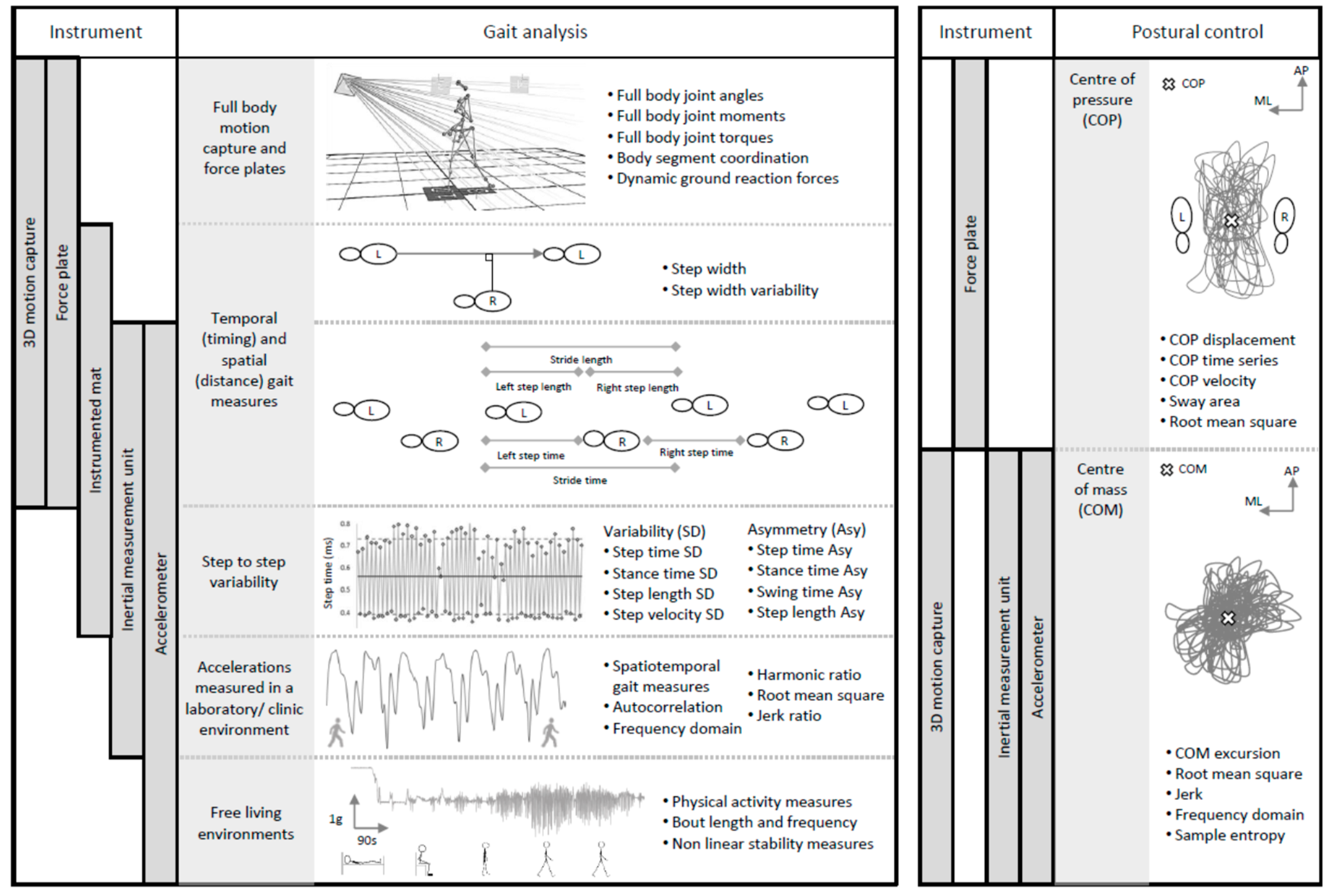
2.1. Quantifying Gait and Postural Control—Which Tools?
2.2. Outcome Measures and Data Collection Protocols
3. Section II: Distinguishing Features of Gait and Postural Control across Neurodegenerative Conditions
3.1. Parkinson’s Disease
3.2. Ataxia
3.3. Dementia
3.4. Summary
4. Section III: Emerging Techniques for Disease Classification and Risk Prediction—So-Called ‘Big Data’ Approaches
5. Section IV: Recommendations and Future Direction
Recommendations
- Quantitative, objective assessments of gait and postural control should supplement traditional disease-specific scales in clinical trials to aid diagnostic accuracy and patient monitoring.
- Education around the advantages and disadvantages of quantitative analysis should be available to allow the clinician and clinical academic to make an informed decision about the best tool, protocol, and outcomes.
- Continued efforts are needed to validate the optimal protocol and outcome measures to best inform clinical management and research, and this requires a discrete condition-based approach.
- Further research using machine/deep learning should be explored to advance opportunities for optimised diagnosis and disease monitoring.
- Development of normative values across a range of standardised outcomes will help interpret gait and postural control outcome measures, and embed their clinical use and a personalised approach to management.
- Further research is needed in order to validate gait and postural control as approved disease biomarkers and progression markers.
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Tinetti, M.E. Performance-oriented assessment of mobility problems in elderly patients. J. Am. Geriatr. Soc. 1986, 34, 119–126. [Google Scholar] [CrossRef]
- Anne, S.-C.; Marjorie, H. Motor Control: Theory and Practical Applications; Lippincott, Williams & Wilkins: Philadelphia, PA, USA, 2000. [Google Scholar]
- Berg, K.; Wood-Dauphine, S.; Williams, J.I.; Gayton, D. Measuring balance in the elderly: Preliminary development of an instrument. Physiother. Can. 1989, 41, 304–311. [Google Scholar] [CrossRef]
- Berg, K.O.; Maki, B.E.; Williams, J.I.; Holliday, P.J.; Wood-Dauphinee, S.L. Clinical and laboratory measures of postural balance in an elderly population. Arch. Phys. Med. Rehabil. 1992, 73, 1073–1080. [Google Scholar] [PubMed]
- Fritz, S.; Lusardi, M. Walking speed: The sixth vital sign. J. Geriatr. Phys. Ther. 2009, 32, 2–5. [Google Scholar] [CrossRef]
- Cimolin, V.; Galli, M. Summary measures for clinical gait analysis: A literature review. Gait Posture 2014, 39, 1005–1010. [Google Scholar] [CrossRef] [PubMed]
- Godinho, C.; Domingos, J.; Cunha, G.; Santos, A.T.; Fernandes, R.M.; Abreu, D.; Gonçalves, N.; Matthews, H.; Isaacs, T.; Duffen, J.; et al. A systematic review of the characteristics and validity of monitoring technologies to assess Parkinson’s disease. J. Neuroeng. Rehabil. 2016, 13, 24. [Google Scholar] [CrossRef]
- Ferrari, A.; Benedetti, M.G.; Pavan, E.; Frigo, C.; Bettinelli, D.; Rabuffetti, M.; Crenna, P.; Leardini, A. Quantitative comparison of five current protocols in gait analysis. Gait Posture 2008, 28, 207–216. [Google Scholar] [CrossRef]
- Menz, H.B.; Latt, M.D.; Tiedemann, A.; Kwan, M.M.S.; Lord, S.R. Reliability of the GAITRite walkway system for the quantification of temporo-spatial parameters of gait in young and older people. Gait Posture 2004, 20, 20–25. [Google Scholar] [CrossRef]
- Mcdonough, A.L.; Batavia, M.; Chen, F.C.; Kwon, S.; Ziai, J.; Al, A.M.; Batavia, M.; Fc, C. The Validity and Reliability of the GAITRite System’ s Measurements: A Preliminary Evaluation. Arch. Phys. Med. Rehabil. 2001, 82, 419–425. [Google Scholar] [CrossRef]
- Van Uden, C.J.T.; Besser, M.P. Test-retest reliability of temporal and spatial gait characteristics measured with an instrumented walkway system (GAITRite). BMC Musculoskelet. Disord. 2004, 5, 13. [Google Scholar] [CrossRef]
- Lord, S.; Galna, B.; Rochester, L. Moving forward on gait measurement: Toward a more refined approach. Mov. Disord. 2013, 28, 1534–1543. [Google Scholar] [CrossRef] [PubMed]
- Galna, B.; Lord, S.; Rochester, L. Is gait variability reliable in older adults and Parkinson’s disease? Towards an optimal testing protocol. Gait Posture 2013, 37, 580–585. [Google Scholar] [CrossRef] [PubMed]
- Muro-De-La-Herran, A.; Garcia-Zapirain, B.; Mendez-Zorrilla, A. Gait analysis methods: An overview of wearable and non-wearable systems, highlighting clinical applications. Sensors 2014, 14, 3362–3394. [Google Scholar] [CrossRef] [PubMed]
- Del Din, S.; Godfrey, A.; Mazza, C.; Lord, S.; Rochester, L. Free-Living Monitoring of Parkinson’ s Disease: Lessons from the Field. Mov. Disord. 2016, 31, 1293–1313. [Google Scholar] [CrossRef] [PubMed]
- Weiss, A.; Sharifi, S.; Plotnik, M.; van Vugt, J.P.P.; Giladi, N.; Hausdorff, J.M. Toward Automated, At-Home Assessment of Mobility among Patients with Parkinson Disease, Using a Body-Worn Accelerometer. Neurorehabil. Neural Repair 2011, 25, 810–818. [Google Scholar] [CrossRef] [PubMed]
- Weiss, A.; Brozgol, M.; Dorfman, M.; Herman, T.; Shema, S.; Giladi, N.; Hausdorff, J.M. Does the evaluation of gait quality during daily life provide insight into fall risk? A novel approach using 3-Day accelerometer recordings. Neurorehabil. Neural Repair 2013, 27, 742–752. [Google Scholar] [CrossRef]
- Weiss, A.; Herman, T.; Giladi, N.; Hausdorff, J.M. Objective assessment of fall risk in Parkinson’s disease using a body-fixed sensor worn for 3 days. PLoS ONE 2014, 9, e96675. [Google Scholar] [CrossRef]
- Croce, U. Della; Cereatti, A.; Mancini, M. Gait Parameters Estimated Using Inertial Measurement Units. In Handbook of Human Motion; Springer: Cham, Switzerland, 2017. [Google Scholar]
- Morris, R.; Hickey, A.; Del Din, S.; Godfrey, A.; Lord, S.; Rochester, L. A model of free-living gait: A factor analysis in Parkinson’s disease. Gait Posture 2017, 52, 68–71. [Google Scholar] [CrossRef]
- Lowe, S.A.; ÓLaighin, G. Monitoring human health behaviour in one’s living environment: A technological review. Med. Eng. Phys. 2014, 36, 147–168. [Google Scholar] [CrossRef]
- El-Gohary, M.; Pearson, S.; McNames, J.; Mancini, M.; Horak, F.; Mellone, S.; Chiari, L. Continuous monitoring of turning in patients with movement disability. Sensors 2014, 14, 356–369. [Google Scholar] [CrossRef]
- Awais, M.; Palmerini, L.; Bourke, A.; Ihlen, E.; Helbostad, J.; Chiari, L. Performance Evaluation of State of the Art Systems for Physical Activity Classification of Older Subjects Using Inertial Sensors in a Real Life Scenario: A Benchmark Study. Sensors 2016, 16, 2105. [Google Scholar] [CrossRef] [PubMed]
- Buckley, C.; Galna, B.; Rochester, L.; Mazzà, C. Upper body accelerations as a biomarker of gait impairment in the early stages of Parkinson’s disease. Gait Posture 2018. [Google Scholar] [CrossRef] [PubMed]
- Del Din, S.; Godfrey, A.; Rochester, L. Validation of an Accelerometer to Quantify a Comprehensive Battery of Gait Characteristics in Healthy Older Adults and Parkinson ’ s Disease: Toward Clinical and at Home Use. IEEE J. Biomed. Health Inform. 2016, 20, 838–847. [Google Scholar] [CrossRef] [PubMed]
- Hickey, A.; Gunn, E.; Alcock, L.; Del Din, S.; Godfrey, A.; Rochester, L.; Galna, B. Validity of a wearable accelerometer to quantify gait in spinocerebellar ataxia type 6. Physiol. Meas. 2016, 37, N105–N117. [Google Scholar] [CrossRef]
- Robles-García, V.; Corral-Bergantiños, Y.; Espinosa, N.; Jácome, M.A.; García-Sancho, C.; Cudeiro, J.; Arias, P. Spatiotemporal gait patterns during overt and covert evaluation in patients with Parkinson’s disease and healthy subjects: Is there a Hawthorne effect? J. Appl. Biomech. 2015, 31, 189–194. [Google Scholar] [CrossRef]
- Lord, S.; Galna, B.; Verghese, J.; Coleman, S.; Burn, D.; Rochester, L. Independent domains of gait in older adults and associated motor and nonmotor attributes: Validation of a factor analysis approach. J. Gerontol. A. Biol. Sci. Med. Sci. 2013, 68, 820–827. [Google Scholar] [CrossRef]
- Beauchet, O.; Allali, G.; Sekhon, H.; Verghese, J.; Guilain, S.; Steinmetz, J.-P.; Kressig, R.W.; Barden, J.M.; Szturm, T.; Launay, C.P. Guidelines for assessment of gait and reference values for spatiotemporal gait parameters in older adults: The biomathics and canadian gait consortiums initiative. Front. Hum. Neurosci. 2017, 11, 353. [Google Scholar] [CrossRef]
- Oh-Park, M.; Holtzer, R.; Xue, X.; Verghese, J. Conventional and robust quantitative gait norms in community-dwelling older adults. J. Am. Geriatr. Soc. 2010, 58, 1512–1518. [Google Scholar] [CrossRef]
- Verghese, J.; Robbins, M.; Holtzer, R.; Zimmerman, M.; Wang, C.; Xue, X.; Lipton, R.B. Gait dysfunction in mild cognitive impairment syndromes. J. Am. Geriatr. Soc. 2008, 56, 1244–1251. [Google Scholar] [CrossRef]
- Hollman, J.; McDade, E.; Petersen, R.C. Undefined Normative spatiotemporal gait parameters in older adults. Gait Posture 2011, 34, 111–118. [Google Scholar] [CrossRef]
- Hausdorff, J.M. Gait variability: Methods, modeling and meaning Example of Increased Stride Time Variability in Elderly Fallers Quantification of Stride-to-Stride Fluctuations. J. Neuroeng. Rehabil. 2005, 2, 19. [Google Scholar] [CrossRef] [PubMed]
- Hausdorff, J.M. Gait dynamics in Parkinson’s disease: Common and distinct behavior among stride length, gait variability, and fractal-like scaling. Chaos Interdiscip. J. Nonlinear Sci. 2009, 19, 026113. [Google Scholar] [CrossRef] [PubMed]
- Graham, J.E.; Ostir, G.V.; Fisher, S.R.; Ottenbacher, K.J. Assessing walking speed in clinical research: A systematic review. J. Eval. Clin. Pract. 2008, 14, 552–562. [Google Scholar] [CrossRef] [PubMed]
- Van Kan, G.A.; Rolland, Y.; Andrieu, S.; Bauer, J.; Beauchet, O.; Bonnefoy, M.; Cesari, M.; Donini, L.M.; Gillette-Guyonnet, S.; Inzitari, M. Gait speed at usual pace as a predictor of adverse outcomes in community-dwelling older people an International Academy on Nutrition and Aging (IANA) Task Force. J. Nutr. Health Aging 2009, 13, 881–889. [Google Scholar] [CrossRef]
- Lim, L.; Van Wegen, E.E.H.; De Goede, C.J.T.; Jones, D.; Rochester, L.; Hetherington, V.; Nieuwboer, A.; Willems, A.-M.; Kwakkel, G. Measuring gait and gait-related activities in Parkinson’s patients own home environment: A reliability, responsiveness and feasibility study. Parkinsonism Relat. Disord. 2005, 11, 19–24. [Google Scholar] [CrossRef]
- Steffen, T.; Seney, M. Test-retest reliability and minimal detectable change on balance and ambulation tests, the 36-item short-form health survey, and the unified Parkinson disease rating scale in people with parkinsonism. Phys. Ther. 2008, 88, 733–746. [Google Scholar] [CrossRef]
- Ries, J.D.; Echternach, J.L.; Nof, L.; Gagnon Blodgett, M. Test-retest reliability and minimal detectable change scores for the timed “up & go” test, the six-minute walk test, and gait speed in people with Alzheimer disease. Phys. Ther. 2009, 89, 569–579. [Google Scholar] [CrossRef]
- Tyson, S.; Connell, L. The psychometric properties and clinical utility of measures of walking and mobility in neurological conditions: A systematic review. Clin. Rehabil. 2009, 23, 1018–1033. [Google Scholar] [CrossRef]
- Hollman, J.H.; Childs, K.B.; McNeil, M.L.; Mueller, A.C.; Quilter, C.M.; Youdas, J.W. Number of strides required for reliable measurements of pace, rhythm and variability parameters of gait during normal and dual task walking in older individuals. Gait Posture 2010, 32, 23–28. [Google Scholar] [CrossRef]
- Riva, F.; Bisi, M.C.; Stagni, R. Gait variability and stability measures: Minimum number of strides and within-session reliability. Comput. Biol. Med. 2014, 50, 9–13. [Google Scholar] [CrossRef]
- Steffen, T.M.; Hacker, T.A.; Mollinger, L. Age-and gender-related test performance in community-dwelling elderly people: Six-Minute Walk Test, Berg Balance Scale, Timed Up & Go Test, and gait speeds. Phys. Ther. 2002, 82, 128–137. [Google Scholar] [PubMed]
- Snijders, A.H.; van de Warrenburg, B.P.; Giladi, N.; Bloem, B.R. Neurological gait disorders in elderly people: Clinical approach and classification. Lancet Neurol. 2007, 6, 63–74. [Google Scholar] [CrossRef]
- Mancini, M.; Salarian, A.; Carlson-Kuhta, P.; Zampieri, C.; King, L.; Chiari, L.; Horak, F.B. ISway: A sensitive, valid and reliable measure of postural control. J. Neuroeng. Rehabil. 2012, 9, 59. [Google Scholar] [CrossRef] [PubMed]
- Mancini, M.; Horak, F. Trunk accelerometry reveals postural instability in untreated Parkinson’s disease. Parkinsonism Relat. Disord. 2011, 17, 557–562. [Google Scholar] [CrossRef] [PubMed]
- Schoneburg, B.; Mancini, M. Framework for understanding balance dysfunction in Parkinson’s disease. Mov. Disord. 2013, 28, 1474–1482. [Google Scholar] [CrossRef] [PubMed]
- Baston, C.; Mancini, M.; Schoneburg, B.; Horak, F.; Rocchi, L. Postural strategies assessed with inertial sensors in healthy and parkinsonian subjects. Gait Posture 2014, 40, 70–75. [Google Scholar] [CrossRef] [PubMed]
- Kelly, V.E.; Johnson, C.O.; McGough, E.L.; Shumway-Cook, A.; Horak, F.B.; Chung, K.A.; Espay, A.J.; Revilla, F.J.; Devoto, J.; Wood-Siverio, C. Association of cognitive domains with postural instability/gait disturbance in Parkinson’s disease. Parkinsonism Relat. Disord. 2015, 21, 692–697. [Google Scholar] [CrossRef] [PubMed]
- Rocchi, L.; Chiari, L.; Horak, F.B. Effects of deep brain stimulation and levodopa on postural sway in Parkinson’s disease. J. Neurol. Neurosurg. Psychiatry 2002, 73, 267–274. [Google Scholar] [CrossRef]
- Palmerini, L.; Rocchi, L.; Mellone, S.; Valzania, F.; Chiari, L. Feature selection for accelerometer-based posture analysis in Parkinsons disease. IEEE Trans. Inf. Technol. Biomed. 2011, 15, 481–490. [Google Scholar] [CrossRef]
- Fukunaga, J.Y.; Quitschal, R.M.; Doná, F.; Ferraz, H.B.; Ganança, M.M.; Caovilla, H.H. Postural control in Parkinson’s disease. Braz. J. Otorhinolaryngol. 2014, 80, 508–514. [Google Scholar] [CrossRef]
- Pantall, A.; Del, S.; Rochester, L. Longitudinal changes over thirty-six months in postural control dynamics and cognitive function in people with Parkinson’s disease. Gait Posture 2018, 62, 468–474. [Google Scholar] [CrossRef] [PubMed]
- Ruhe, A.; Fejer, R.; Walker, B. The test-retest reliability of centre of pressure measures in bipedal static task conditions–a systematic review of the literature. Gait Posture 2010, 32, 436–445. [Google Scholar] [CrossRef]
- Mancini, M.; Horak, F.B. The relevance of clinical balance assessment tools to differentiate balance deficits. Eur. J. Phys. Rehabil. Med. 2010, 46, 239. [Google Scholar] [PubMed]
- Del Din, S.; Godfrey, A.; Coleman, S.; Galna, B.; Lord, S.; Rochester, L. Time-dependent changes in postural control in early Parkinson’s disease: What are we missing? Med. Biol. Eng. Comput. 2016, 54, 401–410. [Google Scholar] [CrossRef] [PubMed]
- Paillard, T.; Noé, F. Techniques and Methods for Testing the Postural Function in Healthy and Pathological Subjects. BioMed Res. Int. 2015, 981390. [Google Scholar] [CrossRef]
- Dorsey, E.R.; Bloem, B.R. The Parkinson pandemic—A call to action. JAMA Neurol. 2018, 75, 9–10. [Google Scholar] [CrossRef]
- Feigin, V.L.; Abajobir, A.A.; Abate, K.H.; Abd-Allah, F.; Abdulle, A.M.; Abera, S.F.; Abyu, G.Y.; Ahmed, M.B.; Aichour, A.N.; Aichour, I. Global, regional, and national burden of neurological disorders during 1990–2015: A systematic analysis for the Global Burden of Disease Study 2015. Lancet Neurol. 2017, 16, 877–897. [Google Scholar] [CrossRef]
- Emamzadeh, F.N.; Surguchov, A. Parkinson’s Disease: Biomarkers, Treatment, and Risk Factors. Front. Neurosci. 2018, 12, 612. [Google Scholar] [CrossRef]
- Marinus, J.; Zhu, K.; Marras, C.; Aarsland, D.; van Hilten, J.J. Risk factors for non-motor symptoms in Parkinson’s disease. Lancet Neurol. 2018, 17, 559–568. [Google Scholar] [CrossRef]
- Goetz, C.G.; Tilley, B.C.; Shaftman, S.R.; Stebbins, G.T.; Fahn, S.; Martinez-Martin, P.; Poewe, W.; Sampaio, C.; Stern, M.B.; Dodel, R. Movement Disorder Society-sponsored revision of the Unified Parkinson’s Disease Rating Scale (MDS-UPDRS): Scale presentation and clinimetric testing results. Mov. Disord. 2008, 23, 2129–2170. [Google Scholar] [CrossRef]
- Hoehn, M.M.; Yahr, M.D. Parkinsonism: Onset, progression, and mortality. Neurology 1967, 17, 427. [Google Scholar] [CrossRef] [PubMed]
- Rovini, E.; Maremmani, C.; Cavallo, F. How wearable sensors can support parkinson’s disease diagnosis and treatment: A systematic review. Front. Neurosci. 2017, 11, 555. [Google Scholar] [CrossRef] [PubMed]
- Galna, B.; Lord, S.; Burn, D.J.; Rochester, L. Progression of Gait Dysfunction in Incident Parkinson’s Disease: Impact of Medication and Phenotype. Mov. Disord. 2015, 30, 359–367. [Google Scholar] [CrossRef] [PubMed]
- Jankovic, J. Parkinson’s disease: Clinical features and diagnosis. J. Neurol. Neurosurg. Psychiatry 2008, 79, 368–376. [Google Scholar] [CrossRef]
- Schaafsma, J.D.; Giladi, N.; Balash, Y.; Bartels, A.L.; Gurevich, T.; Hausdorff, J.M. Gait dynamics in Parkinson’s disease: Relationship to Parkinsonian features, falls and response to levodopa. J. Neurol. Sci. 2003, 212, 47–53. [Google Scholar] [CrossRef]
- Hoskovcová, M.; Dusek, P.; Sieger, T.; Brozová, H.; Zárubová, K.; Bezdicek, O.; Sprdlik, O.; Jech, R.; Stochl, J.; Roth, J.; et al. Predicting falls in Parkinson disease: What is the value of instrumented testing in off medication state? PLoS ONE 2015, 10, e0139849. [Google Scholar] [CrossRef]
- Morris, R.; Lord, S.; Lawson, R.A.; Coleman, S.; Galna, B.; Duncan, G.W.; Khoo, T.K.; Yarnall, A.J.; Burn, D.J.; Rochester, L. Gait Rather Than Cognition Predicts Decline in Specific Cognitive Domains in Early Parkinson’s Disease. J. Gerontol. Ser. A 2017, 72, 1656–1662. [Google Scholar] [CrossRef]
- Coelho, M.; Ferreira, J.J. Late-stage Parkinson disease. Nat. Rev. Neurol. 2012, 8, 435. [Google Scholar] [CrossRef]
- Rochester, L.; Galna, B.; Lord, S.; Yarnall, A.J.; Morris, R.; Duncan, G.; Khoo, T.K.; Mollenhauer, B.; Burn, D.J. Decrease in Aβ42 predicts dopa-resistant gait progression in early Parkinson disease. Neurology 2017, 88, 1501–1511. [Google Scholar] [CrossRef]
- McDade, E.M.; Boot, B.P.; Christianson, T.J.H.; Pankratz, V.S.; Boeve, B.F.; Ferman, T.J.; Bieniek, K.; Hollman, J.H.; Roberts, R.O.; Mielke, M.M.; et al. Subtle gait changes in patients with REM sleep behavior disorder. Mov. Disord. 2013, 28, 1847–1853. [Google Scholar] [CrossRef]
- Lowry, K. a; Smiley-Oyen, A.L.; Carrel, A.J.; Kerr, J.P. Walking stability using harmonic ratios in Parkinson’s disease. Mov. Disord. 2009, 24, 261–267. [Google Scholar] [CrossRef] [PubMed]
- Latt, M.; Menz, H.; Fung, V.; Lord, S. Acceleration patterns of the head and pelvis during gait in older people with Parkinson’s disease: A comparison of fallers and nonfallers. J. Gerontol. 2009, 64, 700–706. [Google Scholar] [CrossRef]
- Latt, M.; Menz, H.; Fung, V.; Lord, S. Walking speed, cadence and step length are selected to optimize the stability of head and pelvis accelerations. Exp. Brain Res. 2008, 184, 201–209. [Google Scholar] [CrossRef]
- Sejdic, E.; Lowry, K.; Roche, J.; Redfern, M.; Brach, J. A comprehensive assessment of gait accelerometry signals in time, frequency and time-frequency domains. IEEE Trans. Neural Syst. Rehabil. Eng. 2013, 22, 603–612. [Google Scholar] [CrossRef] [PubMed]
- Mirelman, A.; Bernad-Elazari, H.; Thaler, A.; Giladi-Yacobi, E.; Gurevich, T.; Gana-Weisz, M.; Saunders-Pullman, R.; Raymond, D.; Doan, N.; Bressman, S.B. Arm swing as a potential new prodromal marker of Parkinson’s disease. Mov. Disord. 2016, 31, 1527–1534. [Google Scholar] [CrossRef]
- Rizzo, G.; Copetti, M.; Arcuti, S.; Martino, D.; Fontana, A.; Logroscino, G. Accuracy of clinical diagnosis of Parkinson disease A systematic review and meta-analysis. Neurology 2016, 86, 566–576. [Google Scholar] [CrossRef] [PubMed]
- Smulders, K.; Dale, M.L.; Carlson-Kuhta, P.; Nutt, J.G.; Horak, F.B. Pharmacological treatment in Parkinson’s disease: Effects on gait. Parkinsonism Relat. Disord. 2016, 31, 3–13. [Google Scholar] [CrossRef]
- Rochester, L.; Yarnall, A.J.; Baker, M.R.; David, R.V.; Lord, S.; Galna, B.; Burn, D.J. Cholinergic dysfunction contributes to gait disturbance in early Parkinson’s disease. Brain 2012, 135, 2779–2788. [Google Scholar] [CrossRef]
- Muller, M.; Bohnen, N.; Bhaumik, A.; Albin, R.; Frey, K.; Gilman, S. Striatal dopaminergic denervation and cardiac post-ganglionic sympathetic denervation correlate independently with gait velocity in Parkinson disease. In Neurology; Lippincott Williams & Wilkins: Philadelphia, PA, USA, 2011; Volume 76, p. A265. [Google Scholar]
- Bloem, B.; Hausdorff, J. Falls and freezing of gait in Parkinson’s disease: A review of two interconnected, episodic phenomena. Mov. Disord. 2004, 19, 871–884. [Google Scholar] [CrossRef]
- Shah, J.; Pillai, L.; Williams, D.K.; Doerhoff, S.M.; Larson-Prior, L.; Garcia-Rill, E.; Virmani, T. Increased foot strike variability in Parkinson’s disease patients with freezing of gait. Parkinsonism Relat. Disord. 2018, 53, 58–63. [Google Scholar] [CrossRef]
- Weiss, A.; Herman, T.; Giladi, N.; Hausdorff, J.M. New evidence for gait abnormalities among Parkinson’s disease patients who suffer from freezing of gait: Insights using a body-fixed sensor worn for 3 days. J. Neural Transm. 2015, 122, 403–410. [Google Scholar] [CrossRef] [PubMed]
- Hausdorff, J.M.; Schaafsma, J.D.; Balash, Y.; Bartels, A.L.; Gurevich, T.; Giladi, N. Impaired regulation of stride variability in Parkinson’s disease subjects with freezing of gait. Exp. Brain Res. 2003, 149, 187–194. [Google Scholar] [CrossRef]
- Moore, S.T.; Yungher, D.A.; Morris, T.R.; Dilda, V.; MacDougall, H.G.; Shine, J.M.; Naismith, S.L.; Lewis, S.J.G. Autonomous identification of freezing of gait in Parkinson’s disease from lower-body segmental accelerometry. J. Neuroeng. Rehabil. 2013, 10, 19. [Google Scholar] [CrossRef] [PubMed]
- Lipsmeier, F.; Taylor, K.I.; Kilchenmann, T.; Wolf, D.; Scotland, A.; Schjodt-Eriksen, J.; Cheng, W.-Y.; Fernandez-Garcia, I.; Siebourg-Polster, J.; Jin, L.; et al. Evaluation of smartphone-based testing to generate exploratory outcome measures in a phase 1 Parkinson’s disease clinical trial. Mov. Disord. 2018, 33, 1287–1297. [Google Scholar] [CrossRef]
- Rocchi, L.; Palmerini, L.; Weiss, A.; Herman, T.; Hausdorff, J. Balance Testing With Inertial Sensors in Patients With Parkinson’s Disease: Assessment of Motor Subtypes. IEEE Trans. Neural Syst. Rehabil. Eng. 2014, 22, 1064–1071. [Google Scholar] [CrossRef]
- Oyama-Higa, M.; Niwa, T.; Wang, W.; Kawanabe, Y. Identifying Characteristic Physiological Patterns of Parkinson’s Disease Sufferers using Sample Entropy of Pulse Waves. In Proceedings of the 11th International Joint Conference on Biomedical Engineering Systems and Technologies, Funchal, Portugal; 2018; pp. 189–196. [Google Scholar] [CrossRef]
- Ruano, L.; Melo, C.; Silva, M.C.; Coutinho, P. The global epidemiology of hereditary ataxia and spastic paraplegia: A systematic review of prevalence studies. Neuroepidemiology 2014, 42, 174–183. [Google Scholar] [CrossRef] [PubMed]
- Matsumura, R.; Futamura, N.; Fujimoto, Y.; Yanagimoto, S.; Horikawa, H.; Suzumura, A.; Takayanagi, T. Spinocerebellar ataxia type 6. Molecular and clinical features of 35 Japanese patients including one homozygous for the CAG repeat expansion. Neurology 1997, 49, 1238–1243. [Google Scholar] [CrossRef]
- Furtado, S.; Das, S.; Suchowersky, O. A review of the inherited ataxias: Recent advances in genetic, clinical and neuropathologic aspects. Park. Relat. Disord. 1998, 4, 161–169. [Google Scholar] [CrossRef]
- Takahashi, H.; Ishikawa, K.; Tsutsumi, T.; Fujigasaki, H.; Kawata, A.; Okiyama, R.; Fujita, T.; Yoshizawa, K.; Yamaguchi, S.; Tomiyasu, H. A clinical and genetic study in a large cohort of patients with spinocerebellar ataxia type 6. J. Hum. Genet. 2004, 49, 256. [Google Scholar] [CrossRef]
- Globas, C.; du Montcel, S.T.; Baliko, L.; Boesch, S.; Depondt, C.; DiDonato, S.; Durr, A.; Filla, A.; Klockgether, T.; Mariotti, C. Early symptoms in spinocerebellar ataxia type 1, 2, 3, and 6. Mov. Disord. 2008, 23, 2232–2238. [Google Scholar] [CrossRef] [PubMed]
- Rochester, L.; Galna, B.; Lord, S.; Mhiripiri, D.; Eglon, G.; Chinnery, P.F. Gait impairment precedes clinical symptoms in spinocerebellar ataxia type 6. Mov. Disord. 2014, 29, 252–255. [Google Scholar] [CrossRef] [PubMed]
- Sakakibara, R.; Terayama, K.; Ogawa, A.; Haruta, H.; Akiba, T.; Tateno, F.; Kishi, M.; Tsuyusaki, Y.; Aiba, Y.; Ogata, T. Wearable gait sensors to measure degenerative cerebellar ataxia. J. Neurol. Sci. 2017, 381, 56–57. [Google Scholar] [CrossRef]
- König, N.; Taylor, W.R.; Baumann, C.R.; Wenderoth, N.; Singh, N.B. Revealing the quality of movement: A meta-analysis review to quantify the thresholds to pathological variability during standing and walking. Neurosci. Biobehav. Rev. 2016, 68, 111–119. [Google Scholar] [CrossRef] [PubMed]
- Pradhan, C.; Wuehr, M.; Akrami, F.; Neuhaeusser, M.; Huth, S.; Brandt, T.; Jahn, K.; Schniepp, R. Automated classification of neurological disorders of gait using spatio-temporal gait parameters. J. Electromyogr. Kinesiol. 2015, 25, 413–422. [Google Scholar] [CrossRef] [PubMed]
- Chini, G.; Ranavolo, A.; Draicchio, F.; Casali, C.; Conte, C.; Martino, G.; Leonardi, L.; Padua, L.; Coppola, G.; Pierelli, F.; et al. Local Stability of the Trunk in Patients with Degenerative Cerebellar Ataxia During Walking. Cerebellum 2017, 16, 26–33. [Google Scholar] [CrossRef] [PubMed]
- Serrao, M.; Chini, G.; Bergantino, M.; Sarnari, D.; Casali, C.; Conte, C.; Ranavolo, A.; Marcotulli, C.; Rinaldi, M.; Coppola, G.; et al. Identification of specific gait patterns in patients with cerebellar ataxia, spastic paraplegia, and Parkinson’s disease: A non-hierarchical cluster analysis. Hum. Mov. Sci. 2018, 57, 267–279. [Google Scholar] [CrossRef]
- Buckley, E.; Mazzà, C.; McNeill, A. A systematic review of the gait characteristics associated with Cerebellar Ataxia. Gait Posture 2018, 60, 154–163. [Google Scholar] [CrossRef]
- Serrao, M.; Mari, S.; Conte, C.; Ranavolo, A.; Casali, C.; Draicchio, F.; Di Fabio, R.; Bartolo, M.; Monamì, S.; Padua, L.; et al. Strategies adopted by cerebellar ataxia patients to perform u-turns. Cerebellum 2013, 12, 460–468. [Google Scholar] [CrossRef]
- Serrao, M.; Chini, G.; Iosa, M.; Casali, C.; Morone, G.; Conte, C.; Bini, F.; Marinozzi, F.; Coppola, G.; Pierelli, F.; et al. Corrigendum to “Harmony as a convergence attractor that minimizes the energy expenditure and variability in physiological gait and the loss of harmony in cerebellar ataxia.”[Clin. Biomech. 48 (2017) 15-23]. Clin. Biomech. 2017, 50, 160. [Google Scholar] [CrossRef]
- Martino, G.; Ivanenko, Y.P.; Serrao, M.; Ranavolo, A.; d’Avella, A.; Draicchio, F.; Conte, C.; Casali, C.; Lacquaniti, F. Locomotor patterns in cerebellar ataxia. J. Neurophysiol. 2014, 112, 2810–2821. [Google Scholar] [CrossRef]
- Sharma, J.; Maclennan, W. Causes of Ataxia in patients attending a falls laboratory. Age Ageing 1988, 17, 94–102. [Google Scholar] [CrossRef]
- Schniepp, R.; Wuehr, M.; Neuhaeusser, M.; Kamenova, M.; Dimitriadis, K.; Klopstock, T.; Strupp, M.; Brandt, T.; Jahn, K. Locomotion speed determines gait variability in cerebellar ataxia and vestibular failure. Mov. Disord. 2012, 27, 125–131. [Google Scholar] [CrossRef] [PubMed]
- Milne, S.C.; Murphy, A.; Georgiou-Karistianis, N.; Yiu, E.M.; Delatycki, M.B.; Corben, L.A. Psychometric properties of outcome measures evaluating decline in gait in cerebellar ataxia: A systematic review. Gait Posture 2018, 61, 149–162. [Google Scholar] [CrossRef] [PubMed]
- Marquer, A.; Barbieri, G.; Pérennou, D. The assessment and treatment of postural disorders in cerebellar ataxia: A systematic review. Ann. Phys. Rehabil. Med. 2014, 57, 67–78. [Google Scholar] [CrossRef] [PubMed]
- Stolze, H.; Klebe, S.; Baecker, C.; Zechlin, C.; Friege, L.; Pohle, S.; Deuschl, G. Prevalence of Gait disorders in hospitalized neurological patients. Mov. Disord. 2005, 20, 89–94. [Google Scholar] [CrossRef]
- Jayadev, S.; Bird, T.D. Hereditary ataxias: Overview. Genet. Med. 2013, 15, 673–683. [Google Scholar] [CrossRef]
- Sandford, E.; Burmeister, M. Genes and genetic testing in hereditary ataxias. Genes 2014, 5, 586–603. [Google Scholar] [CrossRef]
- Schmitz-Hübsch, T.; Du Montcel, S.T.; Baliko, L.; Berciano, J.; Boesch, S.; Depondt, C.; Giunti, P.; Globas, C.; Infante, J.; Kang, J.-S. Scale for the assessment and rating of ataxia: Development of a new clinical scale. Neurology 2006, 66, 1717–1720. [Google Scholar] [CrossRef]
- Ilg, W.; Golla, H.; Thier, P.; Giese, M.A. Specific influences of cerebellar dysfunctions on gait. Brain 2007, 130, 786–798. [Google Scholar] [CrossRef] [PubMed]
- Comber, L.; Sosnoff, J.J.; Galvin, R.; Coote, S. Postural control deficits in people with Multiple Sclerosis: A systematic review and meta-analysis. Gait Posture 2018, 61, 445–452. [Google Scholar] [CrossRef] [PubMed]
- Bakker, M.; Allum, J.H.J.; Visser, J.E.; Grüneberg, C.; van de Warrenburg, B.P.; Kremer, B.H.P.; Bloem, B.R. Postural responses to multidirectional stance perturbations in cerebellar ataxia. Exp. Neurol. 2006, 202, 21–35. [Google Scholar] [CrossRef] [PubMed]
- Bunn, L.M.; Marsden, J.F.; Giunti, P.; Day, B.L. Stance instability in spinocerebellar ataxia type 6. Mov. Disord. 2013, 28, 510–516. [Google Scholar] [CrossRef] [PubMed]
- Fonteyn, E.M.R.; Schmitz-Hübsch, T.; Verstappen, C.C.; Baliko, L.; Bloem, B.R.; Boesch, S.; Bunn, L.; Charles, P.; Dürr, A.; Filla, A.; et al. Falls in spinocerebellar ataxias: Results of the EuroSCA fall study. Cerebellum 2010, 9, 232–239. [Google Scholar] [CrossRef] [PubMed]
- Paquette, C.; Franzén, E.; Horak, F.B. More falls in cerebellar ataxia when standing on a slow up- moving tilt of the support surface HHS Public Access. Cerebellum 2016, 15, 336–342. [Google Scholar] [CrossRef]
- Van de Warrenburg, B.P.C.; Bakker, M.; Kremer, B.P.H.; Bloem, B.R.; Allum, J.H.J. Trunk sway in patients with spinocerebellar ataxia. Mov. Disord. 2005, 20, 1006–1013. [Google Scholar] [CrossRef] [PubMed]
- Ramakers, R.; Koene, S.; Groothuis, J.T.; de Laat, P.; Janssen, M.C.H.; Smeitink, J. Quantification of gait in mitochondrial m. 3243A > G patients: A validation study. Orphanet J. Rare Dis. 2017, 12, 91. [Google Scholar] [CrossRef] [PubMed]
- Serrao, M.; Chini, G.; Bergantino, M.; Sarnari, D.; Casali, C.; Conte, C.; Ranavolo, A.; Marcotulli, C.; Rinaldi, M.; Coppola, G. Dataset on gait patterns in degenerative neurological diseases. Data Br. 2018, 16, 806–816. [Google Scholar] [CrossRef]
- Shirai, S.; Yabe, I.; Matsushima, M.; Ito, Y.M.; Yoneyama, M.; Sasaki, H. Quantitative evaluation of gait ataxia by accelerometers. J. Neurol. Sci. 2015, 358, 253–258. [Google Scholar] [CrossRef] [PubMed]
- Earhart, G.M.; Bastian, A.J. Selection and coordination of human locomotor forms following cerebellar damage. J. Neurophysiol. 2001, 85, 759–769. [Google Scholar] [CrossRef]
- Fonteyn, E.M.R.; Heeren, A.; Engels, J.J.C.; Den Boer, J.J.; van de Warrenburg, B.P.C.; Weerdesteyn, V. Gait adaptability training improves obstacle avoidance and dynamic stability in patients with cerebellar degeneration. Gait Posture 2014, 40, 247–251. [Google Scholar] [CrossRef]
- Morton, S.M.; Dordevic, G.S.; Bastian, A.J. Cerebellar damage produces context-dependent deficits in control of leg dynamics during obstacle avoidance. Exp. Brain Res. 2004, 156, 149–163. [Google Scholar] [CrossRef] [PubMed]
- Mari, S.; Serrao, M.; Casali, C.; Conte, C.; Ranavolo, A.; Padua, L.; Draicchio, F.; Iavicoli, S.; Monamì, S.; Sandrini, G.; et al. Turning strategies in patients with cerebellar ataxia. Exp. Brain Res. 2012, 222, 65–75. [Google Scholar] [CrossRef] [PubMed]
- Ilg, W.; Fleszar, Z.; Schatton, C.; Hengel, H.; Harmuth, F.; Bauer, P.; Timmann, D.; Giese, M.; Schöls, L.; Synofzik, M. I ndividual changes in preclinical spinocerebellar ataxia identified via increased motor complexity. Mov. Disord. 2016, 31, 1891–1900. [Google Scholar] [CrossRef] [PubMed]
- Alzheimer’s Association. 2017 Alzheimer’s disease facts and figures. Alzheimers Dement. 2017, 13, 325–373. [Google Scholar] [CrossRef]
- American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders (DSM-5®); American Psychiatric Pub: New York, NY, USA, 2013; ISBN 0890425574. [Google Scholar]
- Werner, P.; Savva, G.M.; Maidment, I.; Thyrian, J.R.; Fox, C. Dementia: Introduction, Epidemiology and Economic Impact. In Mental Health and Older People; Springer: Cham, Switzerland, 2016; pp. 197–209. [Google Scholar]
- Prince, M.; Wimo, A.; Guerchet, M.; Ali, G.; Wu, Y.; Prina, M. World Alzheimer Report 2015 The Global Impact of Dementia; King’s College: London, UK, 2015. [Google Scholar]
- Gauthier, S.; Reisberg, B.; Zaudig, M.; Petersen, R.C.; Ritchie, K.; Broich, K.; Belleville, S.; Brodaty, H.; Bennett, D.; Chertkow, H. Mild cognitive impairment. Lancet 2006, 367, 1262–1270. [Google Scholar] [CrossRef]
- Kane, J.P.M.; Surendranathan, A.; Bentley, A.; Barker, S.A.H.; Taylor, J.-P.; Thomas, A.J.; Allan, L.M.; McNally, R.J.; James, P.W.; McKeith, I.G.; et al. Clinical prevalence of Lewy body dementia. Alzheimers. Res. 2018, 10, 19. [Google Scholar] [CrossRef] [PubMed]
- Toledo, J.B.; Cairns, N.J.; Da, X.; Chen, K.; Carter, D.; Fleisher, A.; Householder, E.; Ayutyanont, N.; Roontiva, A.; Bauer, R.J.; et al. Clinical and multimodal biomarker correlates of ADNI neuropathological findings. Acta Neuropathol. Commun. 2013, 1, 65. [Google Scholar] [CrossRef] [PubMed]
- Tiraboschi, P.; Salmon, D.P.; Hansen, L.A.; Hofstetter, R.C.; Thal, L.J.; Corey-Bloom, J. What best differentiates Lewy body from Alzheimer’s disease in early-stage dementia? Brain 2006, 129, 729–735. [Google Scholar] [CrossRef] [PubMed]
- McKeith, I. Dementia with Lewy bodies. In Handbook of Clinical Neurology; Elsevier: Philadelphia, PA, USA, 2007; Volume 84, pp. 531–548. [Google Scholar]
- Morris, R.; Lord, S.; Bunce, J.; Burn, D.; Rochester, L. Gait and cognition: Mapping the global and discrete relationships in ageing and neurodegenerative disease. Neurosci. Biobehav. Rev. 2016, 64, 326–345. [Google Scholar] [CrossRef]
- Beauchet, O.; Annweiler, C.; Callisaya, M.L.; De Cock, A.-M.; Helbostad, J.L.; Kressig, R.W.; Srikanth, V.; Steinmetz, J.-P.; Blumen, H.M.; Verghese, J. Poor gait performance and prediction of dementia: Results from a meta-analysis. J. Am. Med. Dir. Assoc. 2016, 17, 482–490. [Google Scholar] [CrossRef]
- Bahureksa, L.; Najafi, B.; Saleh, A.; Sabbagh, M.; Coon, D.; Mohler, M.J.; Schwenk, M. The impact of mild cognitive impairment on gait and balance: A systematic review and meta-analysis of studies using instrumented assessment. Gerontology 2017, 63, 67–83. [Google Scholar] [CrossRef] [PubMed]
- Valkanova, V.; Ebmeier, K.P. What can gait tell us about dementia? Review of epidemiological and neuropsychological evidence. Gait Posture 2017, 53, 215–223. [Google Scholar] [CrossRef] [PubMed]
- van Iersel, M.B.; Hoefsloot, W.; Munneke, M.; Bloem, B.R.; Rikkert, M.G.M.O. Systematic review of quantitative clinical gait analysis in patients with dementia. Z. Gerontol. Geriatr. 2004, 37, 27–32. [Google Scholar] [CrossRef] [PubMed]
- Gillain, S.; Warzee, E.; Lekeu, F.; Wojtasik, V.; Maquet, D.; Croisier, J.L.; Salmon, E.; Petermans, J. The value of instrumental gait analysis in elderly healthy, MCI or Alzheimer’s disease subjects and a comparison with other clinical tests used in single and dual-task conditions. Ann. Phys. Rehabil. Med. 2009, 52, 453–474. [Google Scholar] [CrossRef] [PubMed]
- Coelho, F.G.; Stella, F.; de Andrade, L.P.; Barbieri, F.A.; Santos-Galduroz, R.F.; Gobbi, S.; Costa, J.L.; Gobbi, L.T. Gait and risk of falls associated with frontal cognitive functions at different stages of Alzheimer’s disease. Aging Neuropsychol. Cognit. 2012, 19, 644–656. [Google Scholar] [CrossRef] [PubMed]
- Muir, S.W.; Speechley, M.; Wells, J.; Borrie, M.; Gopaul, K.; Montero-Odasso, M. Gait assessment in mild cognitive impairment and Alzheimer’s disease: The effect of dual-task challenges across the cognitive spectrum. Gait Posture 2012, 35, 96–100. [Google Scholar] [CrossRef] [PubMed]
- Mc Ardle, R.; Morris, R.; Wilson, J.; Galna, B.; Thomas, A.J.; Rochester, L. What Can Quantitative Gait Analysis Tell Us about Dementia and Its Subtypes? A Structured Review. J. Alzheimers Dis. 2017, 60, 1295–1312. [Google Scholar] [CrossRef] [PubMed]
- Fritz, N.E.; Kegelmeyer, D.A.; Kloos, A.D.; Linder, S.; Park, A.; Kataki, M.; Adeli, A.; Agrawal, P.; Scharre, D.W.; Kostyk, S.K. Motor Performance Differentiates Individuals with Lewy Body Dementia, Parkinson’s and Alzheimer’s Disease. Gait Posture 2016, 50, 1–7. [Google Scholar] [CrossRef] [PubMed]
- Merory, J.R.; Wittwer, J.E.; Rowe, C.C.; Webster, K.E. Quantitative gait analysis in patients with dementia with Lewy bodies and Alzheimer’s disease. Gait Posture 2007, 26, 414–419. [Google Scholar] [CrossRef] [PubMed]
- Tanaka, A.; Okuzumi, H.; Kobayashi, I.; Murai, N.; Meguro, K.; Nakamura, T. Gait Disturbance of Patients with Vascular and Alzheimer-Type Dementias. Percept. Mot. Ski. 1995, 80, 735–738. [Google Scholar] [CrossRef] [PubMed]
- Nakamura, T.; Meguro, K.; Sasaki, H. Relationship between falls and stride length variability in senile dementia of the Alzheimer type. Gerontology 1996, 42, 108–113. [Google Scholar] [CrossRef] [PubMed]
- Webster, K.E.; Merory, J.R.; Wittwer, J.E. Gait Variability in Community Dwelling Adults With Alzheimer Disease. Alzheimer Dis. Assoc. Disord. 2006, 20, 37–40. [Google Scholar] [CrossRef] [PubMed]
- Maquet, D.; Lekeu, F.; Warzee, E.; Gillain, S.; Wojtasik, V.; Salmon, E.; Petermans, J.; Croisier, J.L. Gait analysis in elderly adult patients with mild cognitive impairment and patients with mild Alzheimer’s disease: Simple versus dual task: A preliminary report. Clin. Physiol. Funct. Imaging 2010, 30, 51–56. [Google Scholar] [CrossRef] [PubMed]
- Western Geriatric Research Institute. Alzheimer Disease and Associated Disorders; Lawrence, K., Ed.; Western Geriatric Research Institute: Philadelphia, PA, USA, 1987. [Google Scholar]
- Allali, G.; Annweiler, C.; Blumen, H.M.; Callisaya, M.L.; De Cock, A.-M.M.; Kressig, R.W.; Srikanth, V.; Steinmetz, J.-P.P.; Verghese, J.; Beauchet, O. Gait phenotype from mild cognitive impairment to moderate dementia: Results from the GOOD initiative. Eur. J. Neurol. 2016, 23, 527–541. [Google Scholar] [CrossRef] [PubMed]
- Rochester, L.; Lord, S.; Yarnall, A.J.; Burn, D.J. Falls in Patients with Dementia. In Movement Disorders in Dementias; Springer: London, UK, 2014; pp. 45–60. [Google Scholar]
- Stark, S.L.; Roe, C.M.; Grant, E.A.; Hollingsworth, H.; Benzinger, T.L.; Fagan, A.M.; Buckles, V.D.; Morris, J.C. Preclinical Alzheimer disease and risk of falls. Neurology 2013, 81, 437–443. [Google Scholar] [CrossRef] [PubMed]
- Mesbah, N.; Perry, M.; Hill, K.D.; Kaur, M.; Hale, L. Postural Stability in Older Adults With Alzheimer Disease. Phys. Ther. 2017, 97, 290–309. [Google Scholar] [CrossRef]
- Gietzelt, M.; Wolf, K.-H.; Kohlmann, M.; Marschollek, M.; Haux, R. Measurement of Accelerometry-based Gait Parameters in People with and without Dementia in the Field. Methods Inf. Med. 2013, 52, 319–325. [Google Scholar]
- Mc Ardle, R.; Morris, R.; Hickey, A.; Del Din, S.; Koychev, I.; Gunn, R.N.; Lawson, J.; Zamboni, G.; Ridha, B.; Sahakian, B.J.; et al. Gait in Mild Alzheimer’s Disease: Feasibility of Multi-Center Measurement in the Clinic and Home with Body-Worn Sensors: A Pilot Study. J. Alzheimers Dis. 2018, 63, 331–341. [Google Scholar] [CrossRef]
- Mirelman, A.; Gurevich, T.; Giladi, N.; Bar-Shira, A.; Orr-Urtreger, A.; Hausdorff, J.M. Gait alterations in healthy carriers of the LRRK2 G2019S mutation. Ann. Neurol. 2011, 69, 193–197. [Google Scholar] [CrossRef]
- Phinyomark, A.; Petri, G.; Ibáñez-Marcelo, E.; Osis, S.T.; Ferber, R. Analysis of big data in gait biomechanics: Current trends and future directions. J. Med. Biol. Eng. 2018, 38, 244–260. [Google Scholar] [CrossRef]
- Gao, C.; Sun, H.; Wang, T.; Tang, M.; Bohnen, N.I.; Müller, M.L.T.M.; Herman, T.; Giladi, N.; Kalinin, A.; Spino, C. Model-based and Model-free Machine Learning Techniques for Diagnostic Prediction and Classification of Clinical Outcomes in Parkinson’s Disease. Sci. Rep. 2018, 8, 7129. [Google Scholar] [CrossRef] [PubMed]
- Caramia, C.; Bernabucci, I.; D’Anna, C.; De Marchis, C.; Schmid, M. Gait parameters are differently affected by concurrent smartphone-based activities with scaled levels of cognitive effort. PLoS ONE 2017, 12, e0185825. [Google Scholar] [CrossRef] [PubMed]
- Raknim, P.; Lan, K.C. Gait Monitoring for Early Neurological Disorder Detection Using Sensors in a Smartphone: Validation and a Case Study of Parkinsonism. Telemed. E-Health 2016, 22, 75–81. [Google Scholar] [CrossRef] [PubMed]
- LeMoyne, R.; Heerinckx, F.; Aranca, T.; De Jager, R.; Zesiewicz, T.; Saal, H.J. Wearable body and wireless inertial sensors for machine learning classification of gait for people with Friedreich’s ataxia. In Proceedings of the 13th Annual Body Sensor Networks Conference, BSN 2016, San Francisco, CA, USA, 14–17 June 2016; Institute of Electrical and Electronics Engineers Inc.: Piscataway, NJ, USA, 2016; pp. 147–151. [Google Scholar]
- Costa, L.; Gago, M.F.; Yelshyna, D.; Ferreira, J.; Silva, H.D.; Rocha, L.; Sousa, N.; Bicho, E. Application of Machine Learning in Postural Control Kinematics for the Diagnosis of Alzheimer’s Disease. Comput. Intell. Neurosci. 2016, 3891253. [Google Scholar] [CrossRef] [PubMed]
- Duda, R.O.; Hart, P.E.; Stork, D.G. Pattern classification; John Wiley & Sons, 2012; ISBN 111858600X. [Google Scholar]
- Abdulhay, E.; Arunkumar, N.; Narasimhan, K.; Vellaiappan, E.; Venkatraman, V. Gait and tremor investigation using machine learning techniques for the diagnosis of Parkinson disease. Futur. Gener. Comput. Syst. 2018, 83, 366–373. [Google Scholar] [CrossRef]
- Aich, S.; Choi, K.; Park, J.; Kim, H.C.; Seoul National, U. Prediction of Parkinson disease using nonlinear classifiers with decision tree using gait dynamics. In Proceedings of the 4th International Conference on Biomedical and Bioinformatics Engineering, ICBBE 2017, Seoul, Korea, 12–14 November 2017; Association for Computing Machinery: New York, NY, USA, 2017; Volume Part F1338, pp. 52–57. [Google Scholar]
- Cuzzolin, F.; Sapienza, M.; Esser, P.; Saha, S.; Franssen, M.M.; Collett, J.; Dawes, H. Metric learning for Parkinsonian identification from IMU gait measurements. Gait Posture 2017, 54, 127–132. [Google Scholar] [CrossRef]
- Mannini, A.; Trojaniello, D.; Cereatti, A.; Sabatini, A.M. A machine learning framework for gait classification using inertial sensors: Application to elderly, post-stroke and huntington’s disease patients. Sensors 2016, 16, 134. [Google Scholar] [CrossRef]
- Papavasileiou, I.; Zhang, W.; Wang, X.; Bi, J.; Zhang, L.; Han, S. Classification of Neurological Gait Disorders Using Multi-task Feature Learning. In Proceedings of the 2nd IEEE International Conference on Connected Health: Applications, Systems and Engineering Technologies, CHASE 2017, Philadelphia, PA, USA, 17–19 July 2017; Institute of Electrical and Electronics Engineers Inc.: Piscataway, NJ, USA, 2017; pp. 195–204. [Google Scholar]
- Ceseracciu, E.; Sawacha, Z.; Cobelli, C. Comparison of markerless and marker-based motion capture technologies through simultaneous data collection during gait: Proof of concept. PLoS ONE 2014, 9, e87640. [Google Scholar] [CrossRef]
- Schmitz, A.; Ye, M.; Shapiro, R.; Yang, R.; Noehren, B. Accuracy and repeatability of joint angles measured using a single camera markerless motion capture system. J. Biomech. 2014, 47, 587–591. [Google Scholar] [CrossRef]
- Müller, B.; Ilg, W.; Giese, M.A.; Ludolph, N. Validation of enhanced kinect sensor based motion capturing for gait assessment. PLoS ONE 2017, 12, e0175813. [Google Scholar] [CrossRef]
- Dekhtyar, S.; Wang, H.-X.; Scott, K.; Goodman, A.; Koupil, I.; Herlitz, A. A life-course study of cognitive reserve in dementia—From childhood to old age. Am. J. Geriatr. Psychiatry 2015, 23, 885–896. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Device | Advantages | Disadvantages |
|---|---|---|
| 3D motion capture | - Considered the gold standard - Highly precise and accurate - Potential to measure a large variety of outcomes - Non-invasive - High-resolution data | - High cost - Requires experienced technical expertise - Requires a large purpose-built dedicated space usually limited to laboratory/research environments - Participant preparation can be time-consuming |
| Force plates | - Considered gold standard for measuring ground reaction forces and COP - Non-invasive - Minimal space required - Minimal participant preparation time - High-resolution data | - High cost - Requires experienced technical expertise - Requires a purpose-built dedicated space |
| Instrumented mats | - Minimal processing time - Non-invasive - Minimal participant preparation time - Portable | - Extractable features are limited by mat dimensions - Requires a large space to accommodate the mat dimensions - Limited to temporal spatial and foot pressure gait outcomes of the lower extremities |
| Inertial measurement units | - Capable of capturing continuous movements in laboratory and community environments - Non-invasive with minimal participant preparation time - Certain systems provide automated reports - Cheaper than the gold standard - Portable | - Often requires complex algorithms and special expertise to extract key features - Features are often indirect measures requiring additional participant measurements - Free-living measurements may be limited by recording time (if battery powered) or data storage (if data is stored internally on the device) |
| Accelerometer | - Low cost - Wearable, wireless technology capable of capturing continuous movements in lab and community environments for prolonged periods (>one week) - Non-invasive - Minimal participant preparation time - Portable | - Often requires complex algorithms and special expertise to extract key features post-data collection - Features are often indirect measures requiring additional participant measurements - Data collected in community living environments lack context |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Buckley, C.; Alcock, L.; McArdle, R.; Rehman, R.Z.U.; Del Din, S.; Mazzà, C.; Yarnall, A.J.; Rochester, L. The Role of Movement Analysis in Diagnosing and Monitoring Neurodegenerative Conditions: Insights from Gait and Postural Control. Brain Sci. 2019, 9, 34. https://0-doi-org.brum.beds.ac.uk/10.3390/brainsci9020034
Buckley C, Alcock L, McArdle R, Rehman RZU, Del Din S, Mazzà C, Yarnall AJ, Rochester L. The Role of Movement Analysis in Diagnosing and Monitoring Neurodegenerative Conditions: Insights from Gait and Postural Control. Brain Sciences. 2019; 9(2):34. https://0-doi-org.brum.beds.ac.uk/10.3390/brainsci9020034
Chicago/Turabian StyleBuckley, Christopher, Lisa Alcock, Ríona McArdle, Rana Zia Ur Rehman, Silvia Del Din, Claudia Mazzà, Alison J. Yarnall, and Lynn Rochester. 2019. "The Role of Movement Analysis in Diagnosing and Monitoring Neurodegenerative Conditions: Insights from Gait and Postural Control" Brain Sciences 9, no. 2: 34. https://0-doi-org.brum.beds.ac.uk/10.3390/brainsci9020034