
The Influence of Family Bonding, Support, Engagement in Healthcare, on PrEP Stigma among Young Black and Latino Men Who Have Sex with Men: A Path Analysis

 , , , and
, , , and
Abstract
:1. Introduction
Ecodevelopmental Theory
2. Methods
2.1. Procedures
2.2. Measures
2.3. Statistical Analysis Plan
2.4. Sample Characteristics
2.5. Bivariate Correlations
2.6. Path Analysis
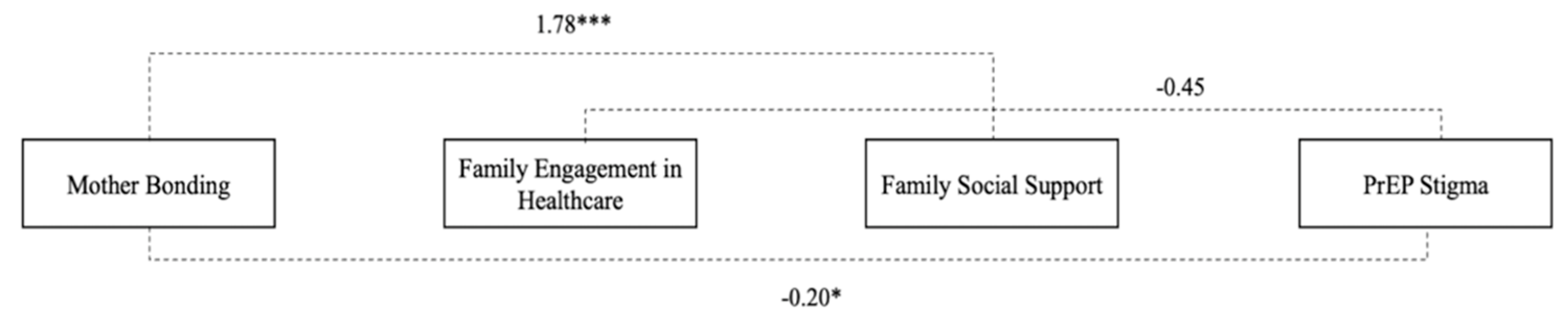
2.6.1. Mother Bonding
2.6.2. Father Bonding
3. Discussion
4. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Khurana, N.; Yaylali, E.; Farnham, P.G.; Hicks, K.A.; Allaire, B.T.; Jacobson, E.; Sansom, S.L. Impact of improved HIV care and treatment on PrEP effectiveness in the United States, 2016–2020. JAIDS J. Acquir. Immune Defic. Syndr. 2018, 78, 399–405. [Google Scholar] [CrossRef] [Green Version]
- Fonner, V.A.; Dalglish, S.L.; Kennedy, C.E.; Baggaley, R.; O’reilly, K.R.; Koechlin, F.M.; Grant, R.M. Effectiveness, and safety of oral HIV preexposure prophylaxis for all populations. AIDS 2016, 30, 1973–1983. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Elopre, L.; Kudroff, K.; Westfall, A.O.; Overton, E.T.; Mugavero, M.J. The right people, right places, and right practices: Disparities in PrEP access among African American men, women and MSM in the Deep South. JAIDS J. Acquir. Immune Defic. Syndr. 2017, 74, 56–59. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Goedel, W.C.; King, M.R.; Lurie, M.N.; Nunn, A.S.; Chan, P.A.; Marshall, B.D. Effect of racial inequities in preexposure prophylaxis use on racial disparities in HIV incidence among men who have sex with men: A modeling study. JAIDS J. Acquir. Immune Defic. Syndr. 2018, 79, 323–329. [Google Scholar] [CrossRef] [PubMed]
- Lelutiu-Weinberger, C.; Golub, S.A. Enhancing PrEP access for Black and Latino men who have sex with men. JAIDS J. Acquir. Immune Defic. Syndr. 2016, 73, 547–555. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nieto, O.; Brooks, R.A.; Landrian, A.; Cabral, A.; Fehrenbacher, A.E. PrEP discontinuation among Latino/a and Black MSM and transgender women: A need for PrEP support services. PLoS ONE 2020, 15, e0241340. [Google Scholar] [CrossRef] [PubMed]
- Centers for Disease Control and Prevention. Monitoring Selected National HIV Prevention and Care Objectives by Using HIV Surveillance Data—United States and 6 Dependent Areas, 2019. HIV Surveillance Supplemental Report. 2019; p. 26. Available online: http://www.cdc.gov/hiv/library/reports/hiv-surveillance.html (accessed on 1 October 2021).
- Centers for Disease Control and Prevention. Diagnoses of HIV Infection in the United States and Dependent Areas, 2019; HIV Surveillance Report 2021; Centers for Disease Control and Prevention: Atlanta, GA, USA, 2019; p. 32. [Google Scholar]
- Lindsey, M.A.; Sheftall, A.H.; Xiao, Y.; Joe, S. Trends of suicidal behaviors among high school students in the United States: 1991–2017. Pediatrics 2019, 144, e20191187. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Calabrese, S.K. Understanding, contextualizing, and addressing PrEP stigma to enhance PrEP implementation. Curr. HIV/AIDS Rep. 2020, 17, 579–588. [Google Scholar] [CrossRef]
- Eaton, L.A.; Kalichman, S.C.; Price, D.; Finneran, S.; Allen, A.; Maksut, J. Stigma and conspiracy beliefs related to Preexposure Prophylaxis (PrEP) and interest in using PrEP among Black and White men and transgender women who have sex with men. AIDS Behav. 2017, 21, 1236–1246. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Golub, S.A. PrEP stigma: Implicit and explicit drivers of disparity. Curr. HIV/AIDS Rep. 2018, 15, 190–197. [Google Scholar] [CrossRef] [PubMed]
- Flores, D.D.; Meanley, S.P.; Wood, S.M.; Bauermeister, J.A. Family characteristics in sex communication and social support: Implications for emerging adult men who have sex with men’s PrEP engagement. Arch. Sex. Behav. 2020, 49, 2145–2153. [Google Scholar] [CrossRef] [PubMed]
- Moskowitz, D.A.; Macapagal, K.; Mongrella, M.; Pérez-Cardona, L.; Newcomb, M.E.; Mustanski, B. What if my dad finds out?: Assessing adolescent men who have sex with men’s perceptions about parents as barriers to PrEP uptake. AIDS Behav. 2020, 24, 2703–2719. [Google Scholar] [PubMed]
- Boyd, D.T.; Quinn, C.R.; Aquino, G.A. The inescapable effects of parent support on black males and HIV testing. J. Racial Ethn. Health Disparities 2020, 7, 563–570. [Google Scholar] [CrossRef]
- Boyd, D.T.; Threats, M.; Winifred, O.; Nelson, L.E. The association between African American father–child relationships and HIV testing. Am. J. Men’s Health 2020, 14, 1557988320982702. [Google Scholar] [CrossRef] [PubMed]
- Boyd, D.T.; Quinn, C.R.; Jones, K.V.; Beer, O.W. Suicidal ideations and attempts within the family context: The role of parent support, bonding, and peer experiences with suicidal behaviors. J. Racial Ethn. Health Disparities 2021, 1–10. [Google Scholar] [CrossRef]
- Hadley, W.; Brown, L.K.; Lescano, C.M.; Kell, H.; Spalding, K.; DiClemente, R.; Donenberg, G. Parent–adolescent sexual communication: Associations of condom use with condom discussions. AIDS Behav. 2009, 13, 997–1004. [Google Scholar] [CrossRef] [Green Version]
- Coleman, C.L. A qualitative analysis of family support among older seropositive African American MSM. J. Cult. Divers. 2018, 25, 82–86. [Google Scholar]
- Bronfenbrenner, U. The Ecology of Human Development: Experiments By Nature and Design; Harvard University Press: Cambridge, MA, USA, 1979. [Google Scholar]
- Szapocznik, J.; Coatsworth, J.D. An Ecodevelopmental Framework for Organizing the Influences on Drug Abuse: A Developmental Model of Risk and Protection. In Drug abuse: Origins & Interventions; American Psychological Association: Washington, DC, USA, 1999; pp. 331–366. [Google Scholar]
- Nathanson, M.; Baird, A.; Jemail, J. Family functioning and the adolescent mother: A systems approach. Adolescence 1986, 21, 827–841. Available online: https://pubmed.ncbi.nlm.nih.gov/3825665 (accessed on 30 September 2021). [PubMed]
- Quinn, K.G. Applying an intersectional framework to understand syndemic conditions among young Black gay, bisexual, and other men who have sex with men. Soc. Sci. Med. 2019, 112779. [Google Scholar] [CrossRef]
- Kipke, M.D.; Kubicek, K.; Akinyemi, I.C.; Hawkins, W.; Belzer, M.; Bhandari, S.; Bray, B. The healthy young men’s cohort: Health, stress, and risk profile of Black and Latino young men who have sex with men (YMSM). J. Urban Health 2020, 97, 653–667. [Google Scholar] [CrossRef] [PubMed]
- Mustanski, B.; Ryan, D.T.; Hayford, C.; Phillips, G.; Newcomb, M.E.; Smith, J.D. Geographic and individual associations with PrEP stigma: Results from the RADAR cohort of diverse young men who have sex with men and transgender women. AIDS Behav. 2018, 22, 3044–3056. [Google Scholar] [CrossRef] [PubMed]
- Córdova, D.; Heinze, J.E.; Mistry, R.; Salas-Wright, C.P.; Zimmerman, M.A. Ecodevelopmental trajectories of family functioning: Links with HIV/STI risk behaviors and STI among Black adolescents. Dev. Psychol. 2016, 52, 1115–1127. [Google Scholar] [CrossRef] [PubMed]
- Marrs, J.; Cossar, J.; Wroblewska, A. Keeping the family together and bonding: A father’s role in a perinatal mental health unit. J. Reprod. Infant Psychol. 2014, 32, 340–354. [Google Scholar] [CrossRef] [Green Version]
- Brooks, R.A.; Nieto, O.; Landrian, A.; Donohoe, T.J. Persistent stigmatizing and negative perceptions of preexposure prophylaxis (PrEP) users: Implications for PrEP adoption among Latino men who have sex with men. AIDS Care 2019, 31, 427–435. [Google Scholar] [CrossRef]
- Cené, C.W.; Johnson, B.H.; Wells, N.; Baker, B.; Davis, R.; Turchi, R. A narrative review of patient and family engagement: The “foundation” of the medical home. Med. Care 2016, 54, 697–705. [Google Scholar] [CrossRef] [PubMed] [Green Version]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variable | Frequency (%) |
|---|---|
| Age, in years (mean, (SD)) | 22 (2.01) |
| Race | |
| Latino | 250 (59%) |
| Black | 174 (41%) |
| Education | |
| College graduate and above | 282 (22%) |
| Some college/AA | 631 (50%) |
| High school/AA | 239 (19%) |
| 9th–12th | 36 (3%) |
| Employment | |
| I am not working at this time | 43 (10%) |
| Yes, part-time | 172 (38%) |
| Yes, full-time | 123 (27%) |
| Not working at this time and NOT looking | 20 (4%) |
| Not working at this time but looking for work | 84 (19%) |
| Sexual Orientation | |
| Homosexual (gay or bisexual) | 334 (76%) |
| Heterosexual (straight) | 1 (0.22) |
| Bisexual | 74 (17%) |
| Other same sex (e.g., MSM) | 20 (4%) |
| Pansexual | 11 (2%) |
| Unsure/questioning | 4 (0.89%) |
| Other—please specify | 2 (0.45) |
| Do not know | 2 (0.45) |
| In the last 30 days, how often did you use a condom during ANAL receptive sex? | |
| 0–25% of the time | 98 (36%) |
| 26–50% of the time | 30 (11%) |
| 51–75% of the time | 33 (12%) |
| 76–99% of the time | 39 (14%) |
| 100% of the time | 70 (26%) |
| In the last 30 days, how often did you use a condom during ANAL insertive sex? | |
| 0–25% of the time | 113 (39%) |
| 26–50% of the time | 35 (12%) |
| 51–75% of the time | 20 (7%) |
| 76–99% of the time | 42 (14%) |
| 100% of the time | 82 (28%) |
| PrEP Use | |
| Yes | 56 (14%) |
| No | 343 (86%) |
| PrEP Stigma | 1 | |||||
| PrEP attitudes | −0.41 *** | 1 | ||||
| Family social support | −0.15 *** | 0.07 | 1 | |||
| Family engagement in healthcare | −0.04 * | 0.03 * | 0.21 *** | 1 | ||
| History of mother bonding | 0.01 | 0.01 | 0.34 *** | 0.13 * | 1 | |
| History of father bonding | −0.02 | 0.06 | 0.40 *** | 0.04 | 0.50 *** | 1 |
| Mean | 4 | 3.62 | 5 | 7.01 | 0.81 | 0.66 |
| SD | 1.1 | 0.69 | 1.49 | 2.2 | 0.29 | 0.36 |
| Range | 2.0–8.0 | 2.0–5 | 1.0–7.0 | 2.0–11.0 | 0.0–1.0 | 0.0–1.0 |
| Observed | B | 95% CI | SE | β |
|---|---|---|---|---|
| Direct Effects | ||||
| Family engagement in healthcare | ||||
| Mother bonding | 0.44 | 0.02, 0.85 | 0.21 | 0.11 ** |
| Family social support | ||||
| Family engagement in healthcare | 4.05 | 0.29, 7.80 | 1.91 | 3.27 ** |
| PrEP stigma | ||||
| Family social support | −0.11 | −0.18, −0.04 | −0.04 | −0.15 ** |
| Indirect Effects | ||||
| Family social support | ||||
| Mother bonding | 1.78 *** | 1.29, 2.26 | 0.24 | |
| PrEP stigma | ||||
| Family engagement in healthcare | −0.45 | −0.96, 0.06 | 0.26 | |
| Mother bonding | −0.20 * | −0.33, −0.05 | 0.07 | |
| Observed | B | 95% CI | SE | β |
|---|---|---|---|---|
| Direct Effects | ||||
| Family engagement in healthcare | ||||
| Father bonding | 0.35 | 10.01, 0.71 | 0.18 | 0.09 |
| Family social support | ||||
| Family engagement in healthcare | 5.27 | 0.08, 10.47 | 2.64 | 4.25 ** |
| PrEP stigma | ||||
| Family social support | −0.11 | −0.18, −0.04 | 0.04 | −0.15 ** |
| Indirect Effects | ||||
| Family social support | ||||
| Father bonding | 1.86 *** | 1.37, 2.34 | 0.25 | |
| PrEP stigma | ||||
| Family engagement in healthcare | −0.58 | −1.27, 0.10 | 0.35 | |
| Father bonding | −0.20 * | −0.35, −0.06 | 0.07 | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Boyd, D.T.; Abubakari, G.M.; Turner, D.; Ramos, S.R.; Hill, M.J.; Nelson, L.E. The Influence of Family Bonding, Support, Engagement in Healthcare, on PrEP Stigma among Young Black and Latino Men Who Have Sex with Men: A Path Analysis. Children 2022, 9, 330. https://0-doi-org.brum.beds.ac.uk/10.3390/children9030330
Boyd DT, Abubakari GM, Turner D, Ramos SR, Hill MJ, Nelson LE. The Influence of Family Bonding, Support, Engagement in Healthcare, on PrEP Stigma among Young Black and Latino Men Who Have Sex with Men: A Path Analysis. Children. 2022; 9(3):330. https://0-doi-org.brum.beds.ac.uk/10.3390/children9030330
Chicago/Turabian StyleBoyd, Donte T., Gamji M’Rabiu Abubakari, DeAnne Turner, S. Raquel Ramos, Mandy J. Hill, and LaRon E. Nelson. 2022. "The Influence of Family Bonding, Support, Engagement in Healthcare, on PrEP Stigma among Young Black and Latino Men Who Have Sex with Men: A Path Analysis" Children 9, no. 3: 330. https://0-doi-org.brum.beds.ac.uk/10.3390/children9030330