Low Myostatin Serum Levels Are Associated with Poor Outcome in Critically Ill Patients

 , , ,
, , ,  ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design and Patients’ Characteristics
2.2. Myostatin Measurements
2.3. Statistical Analysis
3. Results
3.1. Patients’ Characteristics
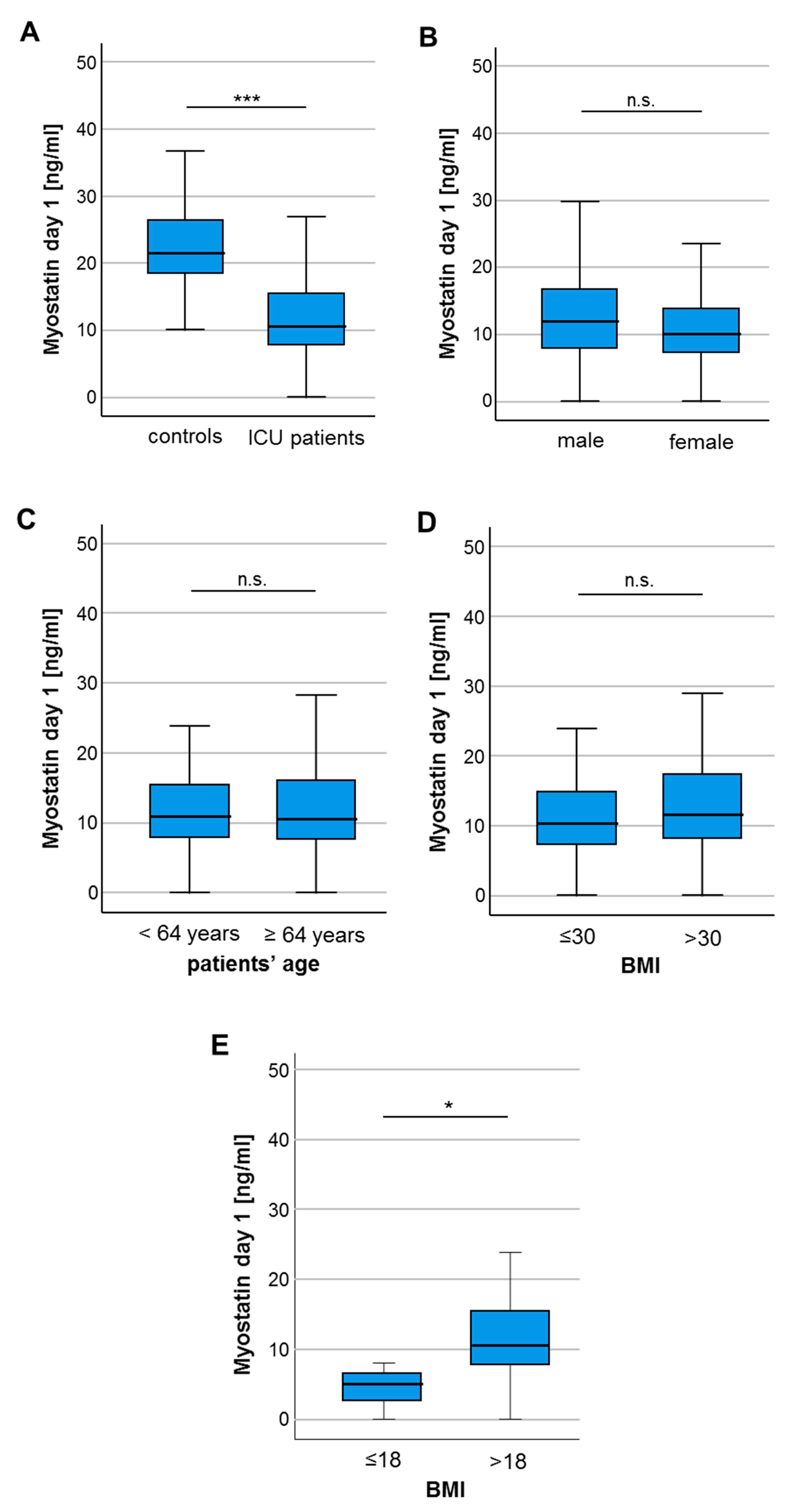
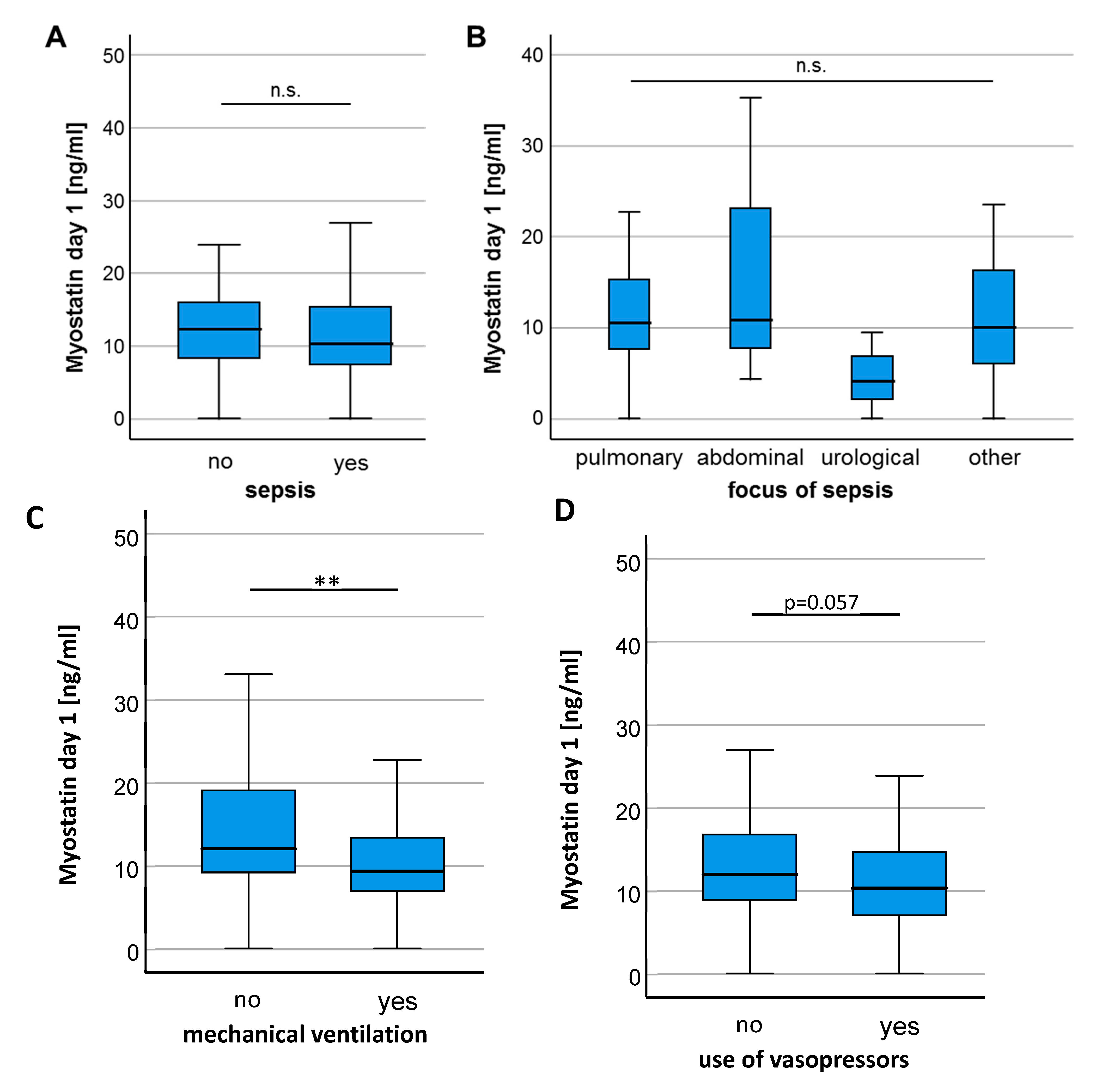
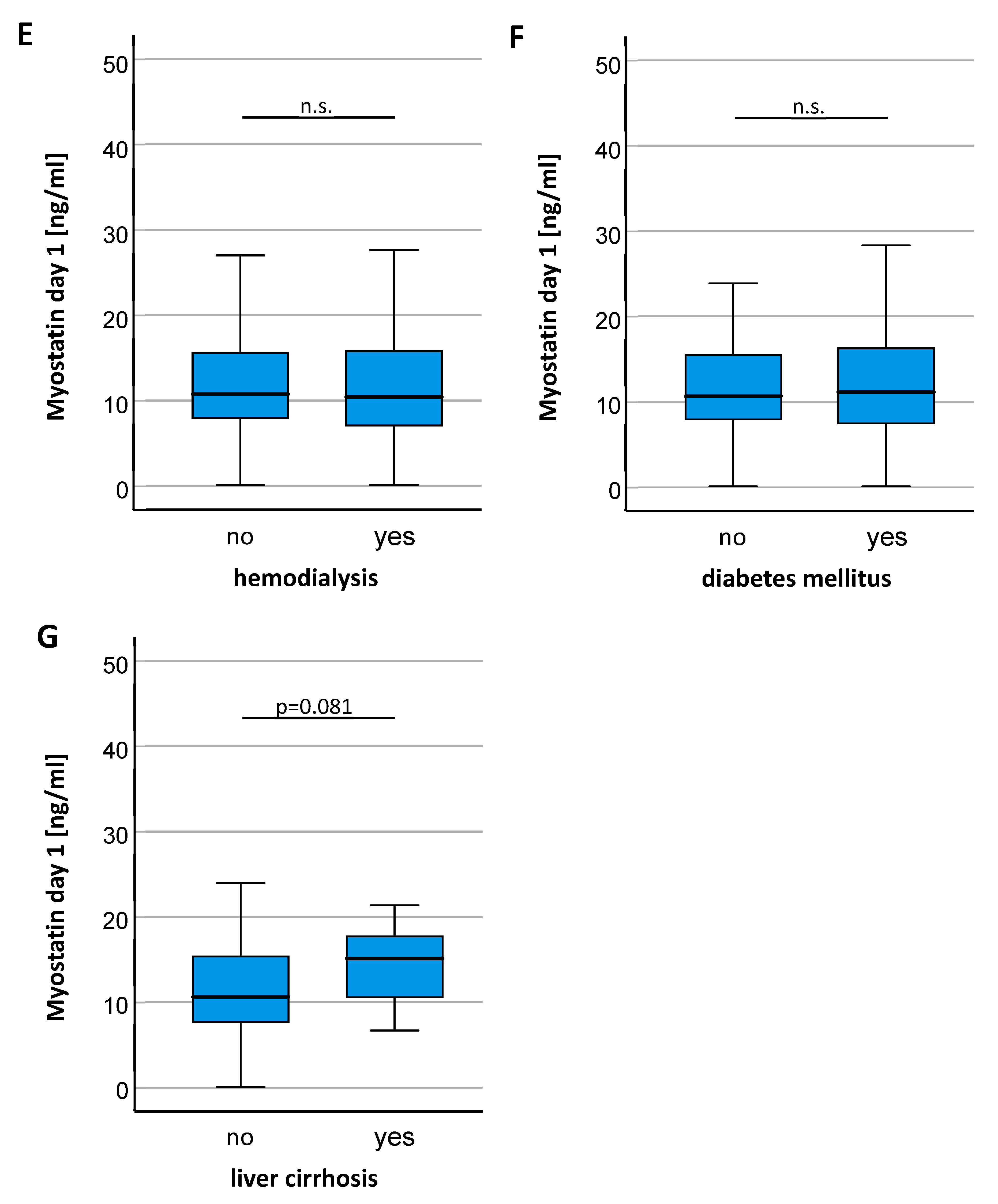
3.2. Myostatin Serum Concentrations Are Decreased in Critically Ill Patients
3.3. Myostatin Serum Levels in ICU Patients Negatively Correlate with Markers of Systemic Inflammation
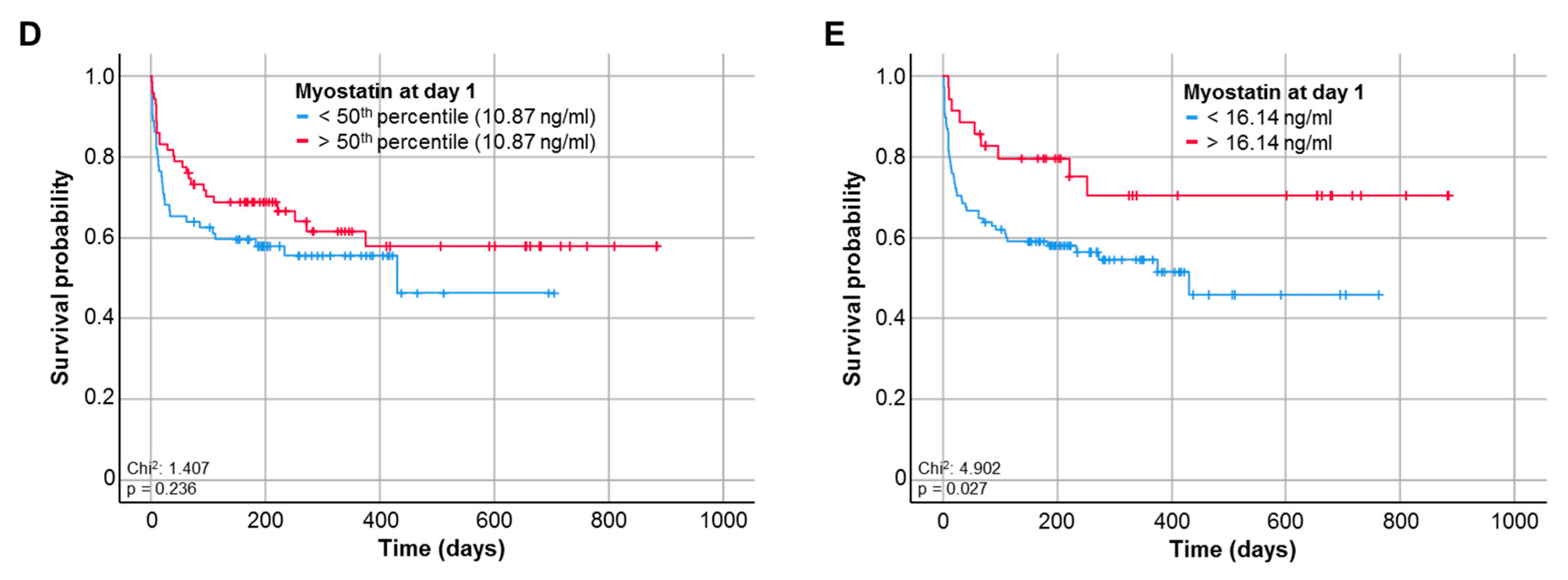
3.4. Baseline Myostatin Serum Levels Predict Overall Survival in ICU Patients
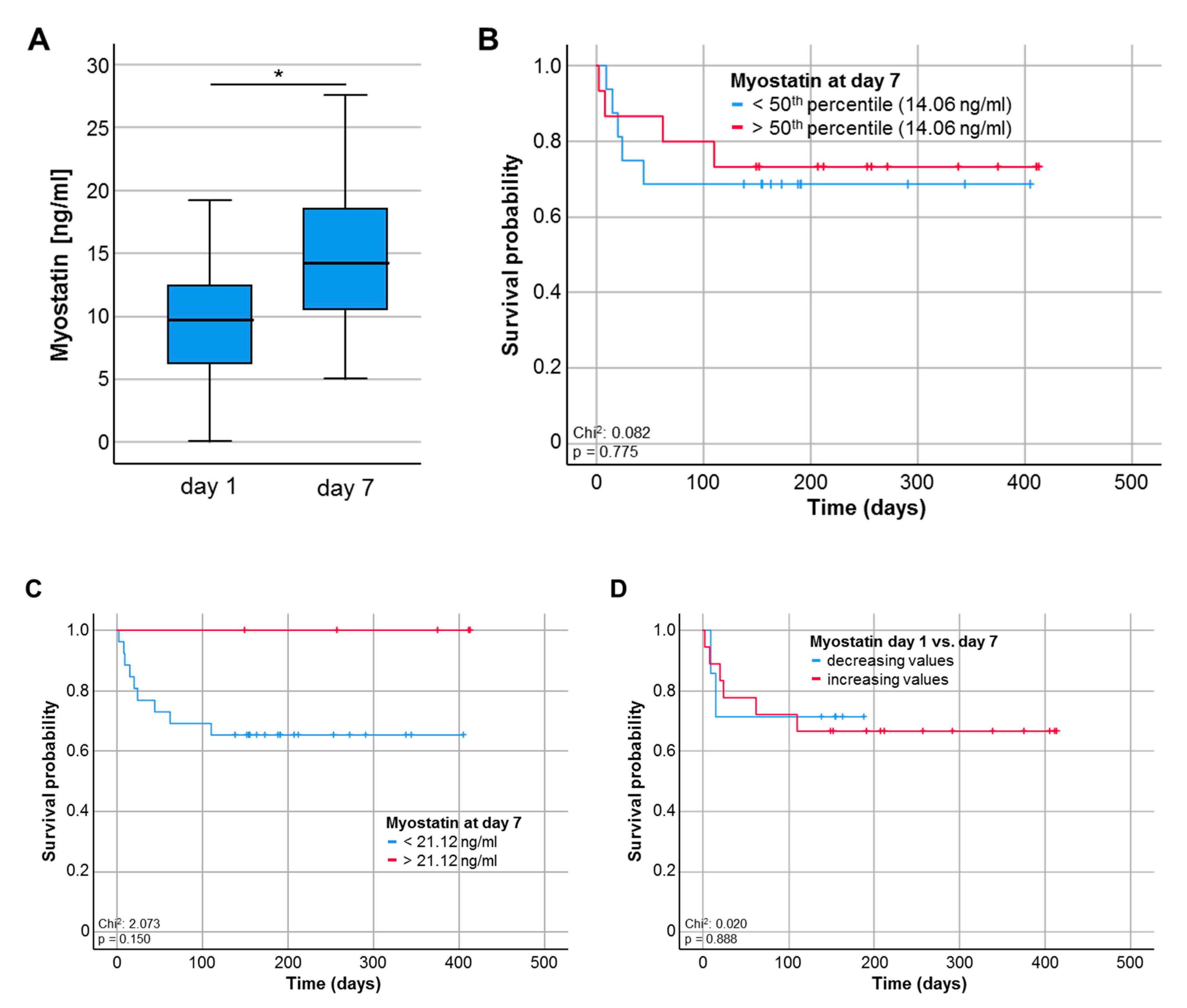
3.5. Myostatin Serum Levels during the Course of Critical Illness
4. Discussion
Author Contributions
Funding
Conflicts of Interest
Abbreviations
| ICU | medical intensive care unit |
| APACHE | acute physiology and chronic health evaluation score |
| SOFA | sequential organ failure assessment score |
| SAPS2 | simplified acute physiology score |
| BMI | body mass index |
| CRP | C-reactive protein |
| IL-6 | interleukin 6 |
| γGT | gamma-glutamyl transpeptidase |
| AST | aspartate aminotransferase |
| BNP | brain natriuretic peptide |
| GFR | glomerular filtration rate |
| LDH | lactate dehydrogenase |
| SIRS | systemic inflammatory distress syndrome |
| OS | overall survival |
References
- Verzola, D.; Barisione, C.; Picciotto, D.; Garibotto, G.; Koppe, L. Emerging role of myostatin and its inhibition in the setting of chronic kidney disease. Kidney Int. 2019, 95, 506–517. [Google Scholar] [CrossRef] [PubMed]
- McPherron, A.C.; Lawler, A.M.; Lee, S.-J. Regulation of skeletal muscle mass in mice by a new TGF-p superfamily member. Nature 1997, 387, 83–90. [Google Scholar] [CrossRef] [PubMed]
- Mosher, D.S.; Quignon, P.; Bustamante, C.D.; Sutter, N.B.; Mellersh, C.S.; Parker, H.G.; Ostrander, E.A. A mutation in the myostatin gene increases muscle mass and enhances racing performance in heterozygote dogs. PLoS Genet. 2007, 3, e79. [Google Scholar] [CrossRef] [PubMed]
- Schuelke, M.; Wagner, K.R.; Stolz, L.E.; Hübner, C.; Riebel, T.; Kömen, W.; Braun, T.; Tobin, J.F.; Lee, S.-J. Myostatin mutation associated with gross muscle hypertrophy in a child. N. Engl. J. Med. 2004, 350, 2682–2688. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Verzola, D.; Procopio, V.; Sofia, A.; Villaggio, B.; Tarroni, A.; Bonanni, A.; Mannucci, I.; De Cian, F.; Gianetta, E.; Saffioti, S.; et al. Apoptosis and myostatin mRNA are upregulated in the skeletal muscle of patients with chronic kidney disease. Kidney Int. 2011, 79, 773–782. [Google Scholar] [CrossRef] [Green Version]
- Zhang, L.; Pan, J.; Dong, Y.; Tweardy, D.J.; Dong, Y.; Garibotto, G.; Mitch, W.E. Stat 3 activation links a C/EBPdelta to myostatin pathway to stimulate loss of muscle mass. Cell. Metab. 2013, 18, 368–379. [Google Scholar] [CrossRef] [Green Version]
- Pirruccello, M.; Jackson, J.; Wawersik, S.; Webster, M.T.; Salta, L.; Long, K.; Mcconaughy, W.; Capili, A.; Boston, C.; Carven, G.J.; et al. Blocking extracellular activation of myostatin as a strategy for treating muscle wasting. Sci. Rep. 2018, 8, 2292. [Google Scholar] [CrossRef]
- Latres, E.; Pangilinan, J.; Miloscio, L.; Bauerlein, R.; Na, E.; Potocky, T.B.; Huang, Y.; Eckersdorff, M.; Rafique, A.; Mastaitis, J.; et al. Myostatin blockade with a fully human monoclonal antibody induces muscle hypertrophy and reverses muscle atrophy in young and aged mice. Skelet. Muscle 2015, 5, 34. [Google Scholar] [CrossRef] [Green Version]
- Smith, R.C.; Cramer, M.S.; Mitchell, P.J.; Capen, A.; Huber, L.; Wang, R.; Myers, L.; Jones, B.E.; Eastwood, B.J.; Ballard, D.; et al. Myostatin Neutralization Results in Preservation of Muscle Mass and Strength in Preclinical Models of Tumor-Induced Muscle Wasting. Mol. Cancer Ther. 2015, 14, 1661–1670. [Google Scholar] [CrossRef] [Green Version]
- Fearon, K.; Strasser, F.; Anker, S.D.; Bosaeus, I.; Bruera, E.; Fainsinger, R.L.; Jatoi, A.; Loprinzi, C.; Macdonald, N.; Mantovani, G.; et al. Definition and classification of cancer cachexia: An international consensus. Lancet Oncol. 2011, 12, 489–495. [Google Scholar] [CrossRef]
- Karmali, R.; Alrifai, T.; Fughhi, I.A.M.; Ng, R.; Chukkapalli, V.; Shah, P.; Basu, S.; Nathan, S.; Szymanski-Grant, K.; Gordon, L.I.; et al. Impact of cachexia on outcomes in aggressive lymphomas. Ann. Hematol. 2017, 96, 951–956. [Google Scholar] [CrossRef] [PubMed]
- Schols, A.M.W.J.; Slangen, J.; Volovics, L.; Wouters, E.F.M. Weight loss is a reversible factor in the prognosis of chronic obstructive pulmonary disease. Am. J. Respir. Crit. Care Med. 1998, 157, 1791–1797. [Google Scholar] [CrossRef] [PubMed]
- Grinspoon, S.K.; Mulligan, K. Weight Loss and Wasting in Patients Infected with Human Immunodeficiency Virus. Clin. Infect. Dis. 2003, 36, S69–S78. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Parry, S.M.; El-Ansary, D.; Cartwright, M.S.; Sarwal, A.; Berney, S.; Koopman, R.; Annoni, R.; A Puthucheary, Z.; Gordon, I.R.; Morris, P.E.; et al. Ultrasonography in the intensive care setting can be used to detect changes in the quality and quantity of muscle and is related to muscle strength and function. J. Crit. Care 2015, 30, 1151.e9–1151.e14. [Google Scholar] [CrossRef]
- Puthucheary, Z.A.; Rawal, J.; McPhail, M.; Connolly, B.; Ratnayake, G.; Chan, P.; Hopkinson, N.S.; Padhke, R.; Dew, T.; Sidhu, P.S.; et al. Acute skeletal muscle wasting in critical illness. JAMA 2013, 310, 1591–1600. [Google Scholar] [CrossRef] [Green Version]
- Singer, M.; Deutschman, C.S.; Seymour, C.W.; Shankar-Hari, M.; Annane, D.; Bauer, M.; Bellomo, R.; Bernard, G.R.; Chiche, J.-D.; Coopersmith, C.M.; et al. The Third International Consensus Definitions for Sepsis and Septic Shock (Sepsis-3). JAMA 2016, 315, 801–810. [Google Scholar] [CrossRef]
- Budczies, J.; Klauschen, F.; Sinn, B.V.; Győrffy, B.; Schmitt, W.D.; Darb-Esfahani, S.; Denkert, C. Cutoff Finder: A comprehensive and straightforward web application enabling rapid biomarker cutoff optimization. PLoS ONE 2012, 7, e51862. [Google Scholar] [CrossRef] [Green Version]
- Åkerfeldt, T.; Helmersson-Karlqvist, J.; Gunningberg, L.; Swenne, C.L.; Larsson, A. Postsurgical Acute Phase Reaction is Associated with Decreased Levels of Circulating Myostatin. Inflammation 2015, 38, 1727–1730. [Google Scholar] [CrossRef]
- Smith, I.J.; Aversa, Z.; Alamdari, N.; Petkova, V.; Hasselgren, P.-O. Sepsis downregulates myostatin mRNA levels without altering myostatin protein levels in skeletal muscle. J. Cell. Biochem. 2010, 111, 1059–1073. [Google Scholar] [CrossRef]
- Garcia, P.S.; Cabbabe, A.; Kambadur, R.; Nicholas, G.; Csete, M. Brief-reports: Elevated myostatin levels in patients with liver disease: A potential contributor to skeletal muscle wasting. Anesth. Analg. 2010, 111, 707–709. [Google Scholar] [CrossRef]
- Nishikawa, H.; Enomoto, H.; Ishii, A.; Iwata, Y.; Miyamoto, Y.; Ishii, N.; Yuri, Y.; Hasegawa, K.; Nakano, C.; Nishimura, T.; et al. Elevated serum myostatin level is associated with worse survival in patients with liver cirrhosis. J. Cachex Sarcopenia Muscle 2017, 8, 915–925. [Google Scholar] [CrossRef] [PubMed]
- Milan, G.; Nora, E.D.; Pilon, C.; Pagano, C.; Granzotto, M.; Manco, M.; Mingrone, G.; Vettor, R. Changes in muscle myostatin expression in obese subjects after weight loss. J. Clin. Endocrinol. Metab. 2004, 89, 2724–2727. [Google Scholar] [CrossRef]
- Wen, X.; Liu, P.; Wu, H.; Zhou, X. Relation between serum myostatin with BMI and PaO₂/PaCO₂ in patients with chronic obstructive pulmonary disease. Zhong Nan Da Xue Xue Bao. Yi Xue Ban J. Cent. South Univ. Med. Sci. 2014, 39, 807–810. [Google Scholar]
- McPherron, A.C.; Lee, S.J. Suppression of body fat accumulation in myostatin-deficient mice. J. Clin. Invest. 2002, 109, 595–601. [Google Scholar] [CrossRef] [PubMed]
- Deng, B.; Zhang, F.; Wen, J.; Ye, S.; Wang, L.; Yang, Y.; Gong, P.; Jiang, S.W. The function of myostatin in the regulation of fat mass in mammals. Nutr. Metab. 2017, 14, 29. [Google Scholar] [CrossRef] [Green Version]
- Manfredi, L.; Paula-Gomes, S.; Zanon, N.; Kettelhut, I. Myostatin promotes distinct responses on protein metabolism of skeletal and cardiac muscle fibers of rodents. Braz. J. Med. Boil. Res. 2017, 50, e6733. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hedayati, M.; Nozhat, Z.; Hannani, M. Can the Serum Level of Myostatin be Considered as an Informative Factor for Cachexia Prevention in Patients with Medullary Thyroid Cancer? Asian Pac. J. Cancer Prev. 2016, 17, 119–123. [Google Scholar] [CrossRef] [Green Version]
- Kim, S.H.; Kim, J.W.; Hwang, I.G.; Jang, J.S.; Hong, S.; Kim, T.-Y.; Baek, J.Y.; Shin, S.H.; Sun, D.S.; Hong, D.-S.; et al. Serum biomarkers for predicting overall survival and early mortality in older patients with metastatic solid tumors. J. Geriatr. Oncol. 2019, 10, 749–756. [Google Scholar] [CrossRef]
- Siriett, V.; Salerno, M.S.; Berry, C.; Nicholas, G.; Bower, R.; Kambadur, R.; Sharma, M. Antagonism of myostatin enhances muscle regeneration during sarcopenia. Mol. Ther. 2007, 15, 1463–1470. [Google Scholar] [CrossRef]
- Wagner, K.R.; McPherron, A.C.; Winik, N.; Lee, S.-J. Loss of myostatin attenuates severity of muscular dystrophy inmdx mice. Ann. Neurol. 2002, 52, 832–836. [Google Scholar] [CrossRef]
- Smith, R.C.; Lin, B.K. Myostatin inhibitors as therapies for muscle wasting associated with cancer and other disorders. Curr. Opin. Support. Palliat. Care 2013, 7, 352–360. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lach-Trifilieff, E.; Minetti, G.C.; Sheppard, K.; Ibebunjo, C.; Feige, J.N.; Hartmann, S.; Brachat, S.; Rivet, H.; Koelbing, C.; Morvan, F.; et al. An antibody blocking activin type II receptors induces strong skeletal muscle hypertrophy and protects from atrophy. Mol. Cell. Boil. 2013, 34, 606–618. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hatakeyama, S.; Summermatter, S.; Jourdain, M.; Melly, S.; Minetti, G.C.; Lach-Trifilieff, E. ActRII blockade protects mice from cancer cachexia and prolongs survival in the presence of anti-cancer treatments. Skelet. Muscle 2016, 6, 26. [Google Scholar] [CrossRef] [PubMed] [Green Version]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Parameter | Patients |
|---|---|
| Number | 165 |
| Gender | |
| Female, % | 57.6 |
| Male, % | 42.4 |
| Age, median, range (years) | 64 (18–90) |
| BMI, median, range (years) | 25.9 (15.9–86.5) |
| Diabetes mellitus type 2, % | 29.7 |
| Coronary artery disease, % | 22.8 |
| COPD, % | 31.7 |
| Main diagnosis/reason for admission, % (N) | |
| Sepsis | 64.2 (106) |
| focus of sepsis, % (N) | |
| Pulmonary | 54.7 (58) |
| Abdominal | 19.8 (21) |
| Urinary tract | 2.8 (3) |
| Other | 22.6 (24) |
| Liver cirrhosis | 4.2 (8) |
| Cardiopulmonary disease | 14.5 (23) |
| Acute liver failure | 1.2 (2) |
| Acute pancreatitis | 5.5 (9) |
| Gastrointestinal bleeding | 2.4 (4) |
| Other | 7.9 (13) |
| APACHE-II score at day 1 (points, median and range) | 18 (3–48) |
| <18, % (N) | 51.4 (75) |
| >18, % (N) | 48.6 (71) |
| SOFA score at day 1 (points, median and range) | 9 (0–17) |
| <9, % (N) | 56.7 (51) |
| >9, % (N) | 43.3 (39) |
| Mechanical ventilation demand at day 1, % (N) | 45.5 (75) |
| Vasopressor demand at day 1, % (N) | 62.4 (103) |
| Death on ICU, % (N) | 18.9 (30) |
| 30d mortality, % (N) | 24.3 (37) |
| 60d mortality, % (N) | 28.5 (44) |
| Overall mortality, % (N) | 36.4 (59) |
| Myostatin (ng/mL) | |
| Day 1 | 10.68 (0.1–44.46) |
| Week 1 | 14.23 (0.1–27.59) |
| r | p | |
|---|---|---|
| Baseline characteristics | ||
| Weight | 0.127 | 0.120 |
| BMI | 0.78 | 0.341 |
| Markers of inflammation | ||
| Leukocytes | 0.051 | 0.529 |
| CRP | −0.258 | 0.001 ** |
| Procalcitonin | −0.240 | 0.009 * |
| IL-6 | −0.342 | <0.001 *** |
| Laboratory markers | ||
| Sodium | −0.004 | 0.959 |
| Kalium | −0.072 | 0.373 |
| Magnesium | 0.241 | 0.012 * |
| Calcium | 0.202 | 0.012 * |
| Creatinine | 0.059 | 0.460 |
| Urea | 0.095 | 0.238 |
| GFR | −0.014 | 0.887 |
| Bilirubin total | 0.024 | 0.764 |
| AST | −0.129 | 0.118 |
| γGT | −0.145 | 0.072 |
| Lipase | −0.233 | 0.007 * |
| Prothrombin time | −0.173 | 0.033 * |
| Protein | 0.137 | 0.108 |
| Albumin | 0.296 | 0.007 * |
| CK | −0.144 | 0.075 |
| Lactate | −0.014 | 0.866 |
| LDH | −0.014 | 0.864 |
| NT-proBNP | −0,055 | 0.591 |
| Fibrinogen | −0.426 | <0.001 *** |
| Lipid and glucose metabolism | ||
| Glucose | −0.120 | 0.136 |
| Insulin | 0.229 | 0.087 |
| C-Peptide | 0.139 | 0.304 |
| HbA1c | −0.095 | 0.469 |
| Cholesterol | 0.151 | 0.084 |
| LDL | 0.302 | 0.023 * |
| HDL | 0.310 | 0.019 * |
| Triglycerides | 0.025 | 0.778 |
| Clinical Scores | ||
| APACHE II | −0.046 | 0.594 |
| SOFA | 0.002 | 0.988 |
| Parameter | Univariate Cox Regression | Multivariate Cox Regression | ||
|---|---|---|---|---|
| p-Value | Hazard-Ratio (95% CI) | p-Value | Hazard-Ratio (95% CI) | |
| Myostatin >16.14 ng/mL | 0.032 * | 0.458 (0.224–0.934) | 0.023 * | 0.433 (0.211–0.889) |
| Age | 0.001 ** | 1.036 (1.015–1.05) | 0.004 ** | 1.031 (1.010–1.053) |
| Sex | 0.928 | 1.024 (0.605–1.735) | ||
| BMI | 0.283 | 0.982 (0.950–1.015) | ||
| Sodium | 0.344 | 1.020 (0.979–1.062) | ||
| Potassium | 0.790 | 0.950 (0.654–1.382) | ||
| Leukocytes | 0.061 | 1.018 (0.999–1.036) | 0.486 | 1.008 (0.986–1.029) |
| Hemoglobin | 0.043 * | 0.988 (0.977–1.000) | 0.103 | 0.988 (0.975–1.002) |
| Platelets | 0.078 | 1.001 (1.000–1.003) | 0.572 | 1.001 (0.999–1.002) |
| AST | 0.261 | 0.999 (0.997–1.001) | ||
| ALT | 0.185 | 0.998 (0.995-1.001) | 0.170 | 0.998 (0.996–1.001) |
| LDH | 0.329 | 1.000 (0.999–1.000) | ||
| Bilirubin | 0.964 | 0.997 (0.887–1.122) | ||
| PCT | 0.658 | 1.002 (0.994–1.009) | ||
| CRP | 0.048 * | 1.003 (1.000–1.006) | 0.464 | 1.001 (0.998–1.004) |
| Creatinine | 0.754 | 1.016 (0.919–1.124) | ||
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Wirtz, T.H.; Loosen, S.H.; Buendgens, L.; Kurt, B.; Abu Jhaisha, S.; Hohlstein, P.; Brozat, J.F.; Weiskirchen, R.; Luedde, T.; Tacke, F.; et al. Low Myostatin Serum Levels Are Associated with Poor Outcome in Critically Ill Patients. Diagnostics 2020, 10, 574. https://0-doi-org.brum.beds.ac.uk/10.3390/diagnostics10080574
Wirtz TH, Loosen SH, Buendgens L, Kurt B, Abu Jhaisha S, Hohlstein P, Brozat JF, Weiskirchen R, Luedde T, Tacke F, et al. Low Myostatin Serum Levels Are Associated with Poor Outcome in Critically Ill Patients. Diagnostics. 2020; 10(8):574. https://0-doi-org.brum.beds.ac.uk/10.3390/diagnostics10080574
Chicago/Turabian StyleWirtz, Theresa H., Sven H. Loosen, Lukas Buendgens, Berkan Kurt, Samira Abu Jhaisha, Philipp Hohlstein, Jonathan F. Brozat, Ralf Weiskirchen, Tom Luedde, Frank Tacke, and et al. 2020. "Low Myostatin Serum Levels Are Associated with Poor Outcome in Critically Ill Patients" Diagnostics 10, no. 8: 574. https://0-doi-org.brum.beds.ac.uk/10.3390/diagnostics10080574