
Detection of Tumor-Specific PTPmu in Gynecological Cancer and Patient Derived Xenografts


Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Ethics and Patient Information
2.2. Reagents
2.3. Biomarker Labeling of Human Gynecologic Tissue
3. Results
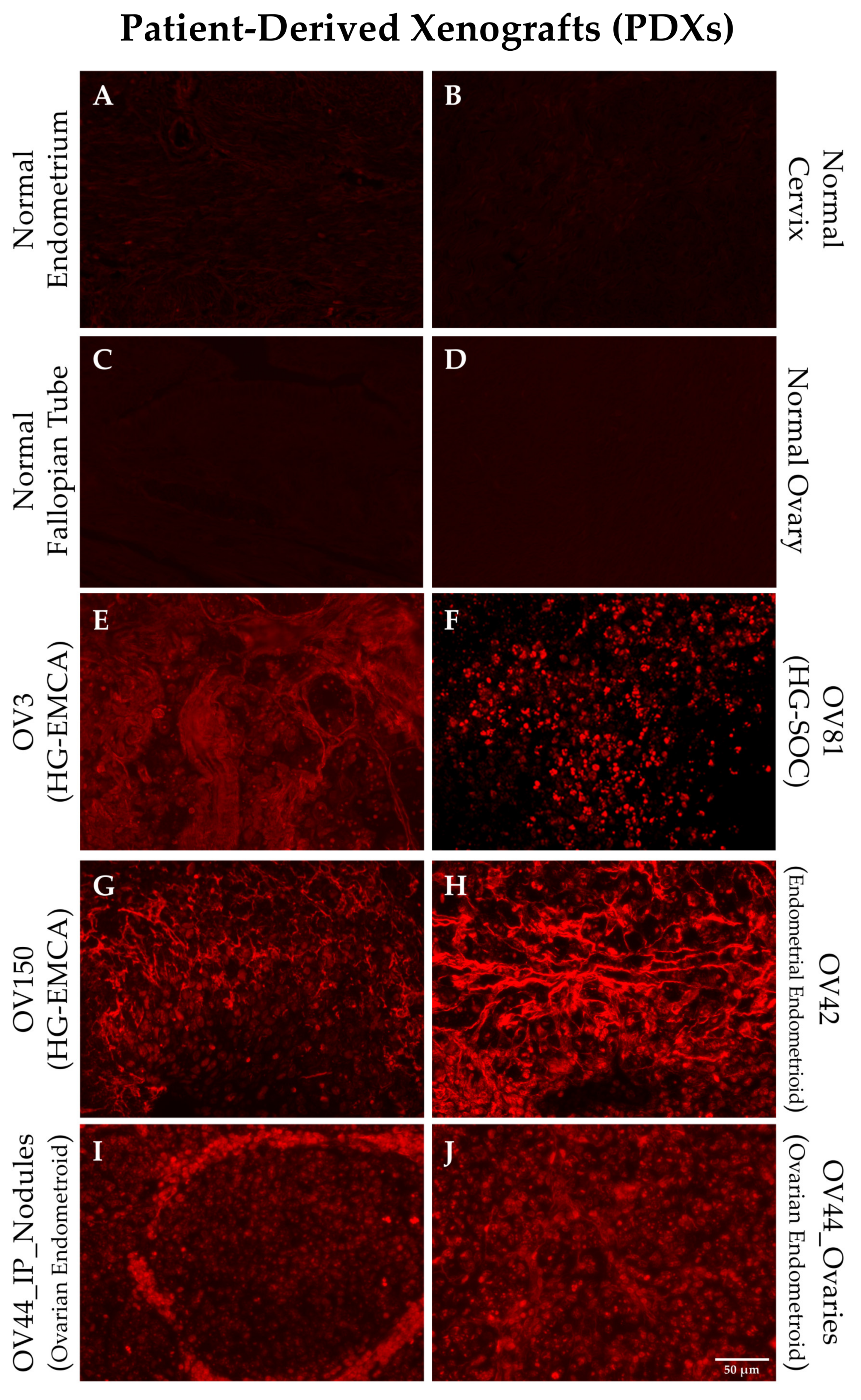
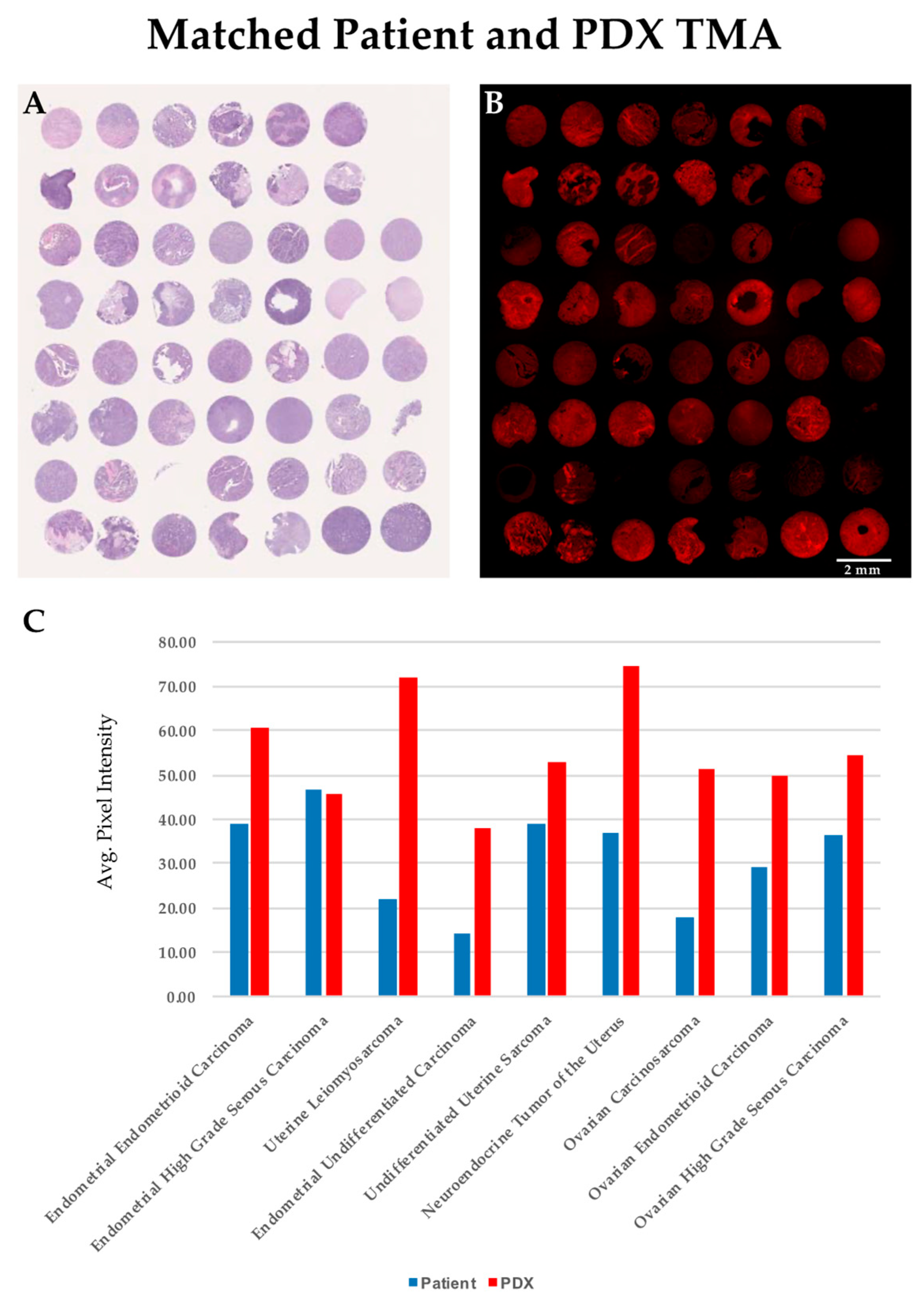
3.1. Patient Derived Xenografts and Their Matched Patient Tumor Tissue Label with SBK4-TR
3.2. Gynecological Cancer Tissue Staining for the PTPµ Biomarker
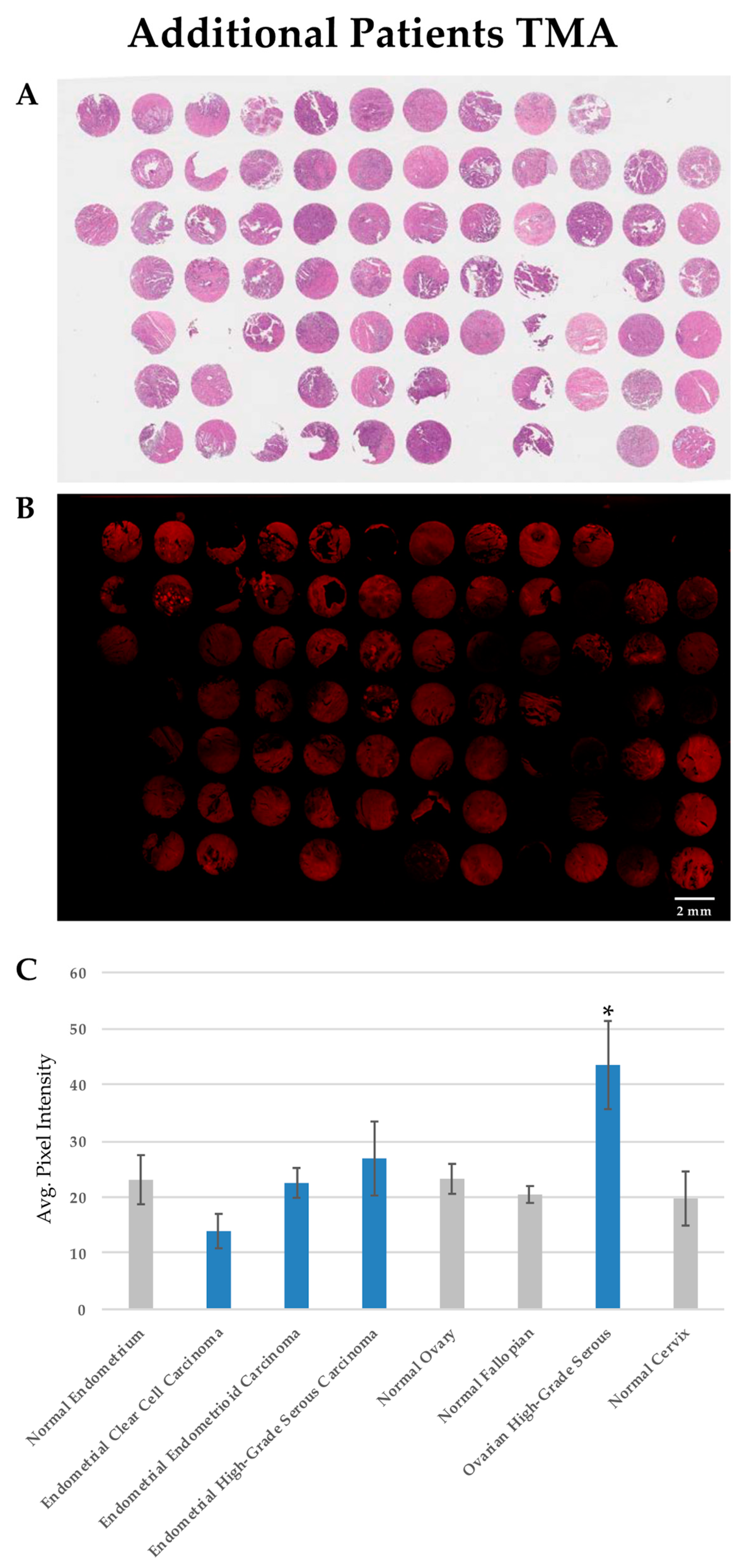
3.3. PTPµ Biomarker Staining is High in Patients with HG-SOC
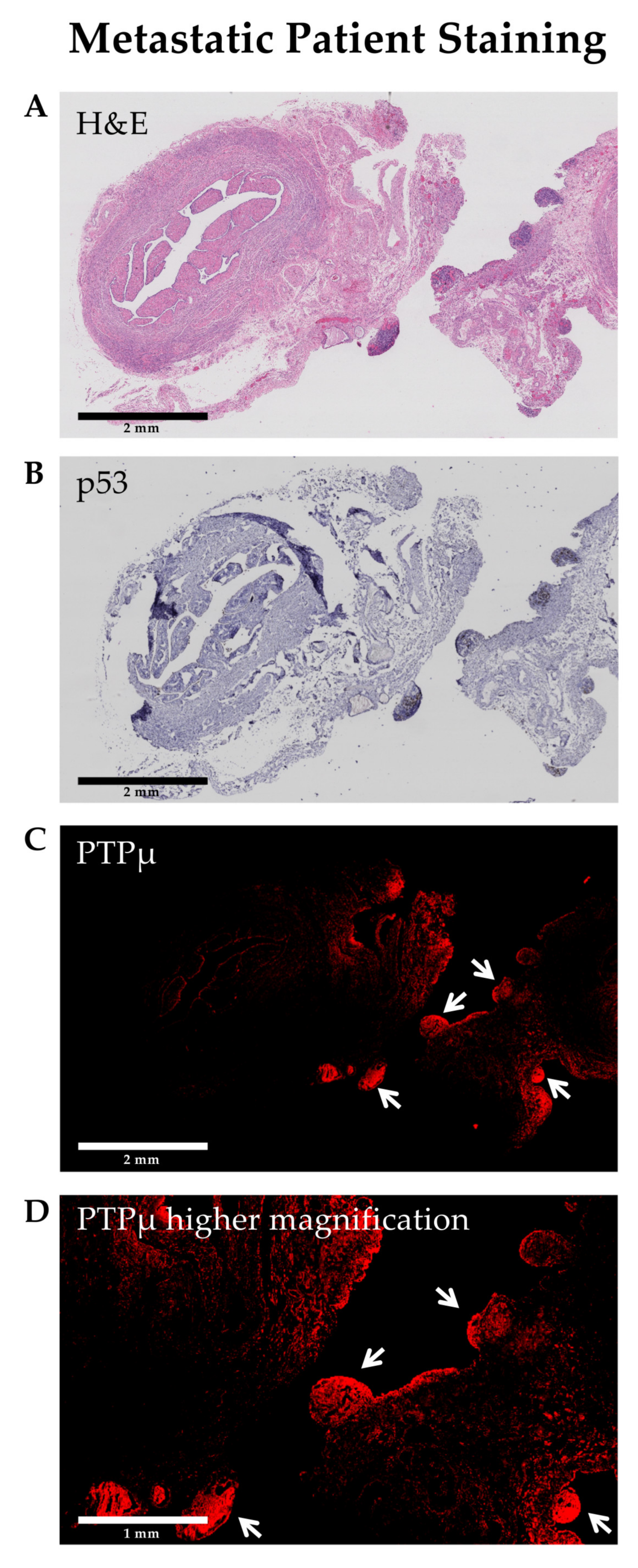
3.4. SBK4-TR Labels Metastatic Nodules in HG-SOC
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Lisio, M.-A.; Fu, L.; Goyeneche, A.A.; Gao, Z.-H.; Telleria, C.M. High-Grade Serous Ovarian Cancer: Basic Sciences, Clinical and Therapeutic Standpoints. Int. J. Mol. Sci. 2019, 20, 952. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- SEER Cancer Stat Facts: Ovarian Cancer. 2020. Available online: https://seer.cancer.gov/statfacts/html/ovary.html (accessed on 3 March 2020).
- SEER Cancer Stat Facts: Uterine Cancer. 2020. Available online: https://seer.cancer.gov/statfacts/html/corp.html (accessed on 3 March 2020).
- SEER Cancer Stat Facts: Cervical Cancer. 2020. Available online: https://seer.cancer.gov/statfacts/html/cervix.html (accessed on 3 March 2020).
- Nagaraj, A.B.; Joseph, P.; Kovalenko, O.; Singh, S.; Armstrong, A.; Redline, R.; Resnick, K.; Zanotti, K.; Waggoner, S.; DiFeo, A. Critical role of Wnt/beta-catenin signaling in driving epithelial ovarian cancer platinum resistance. Oncotarget 2015, 6, 23720–23734. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Craig, S.E.; Brady-Kalnay, S.M. Cancer Cells Cut Homophilic Cell Adhesion Molecules and Run. Cancer Res. 2010, 71, 303–309. [Google Scholar] [CrossRef] [Green Version]
- Phillips-Mason, P.J.; Craig, S.E.; Brady-Kalnay, S.M. Should I stay or should I go? Shedding of RPTPs in cancer cells switches signals from stabilizing cell-cell adhesion to driving cell migration. Cell Adhes. Migr. 2011, 5, 298–305. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Burgoyne, A.M.; Phillips-Mason, P.J.; Burden-Gulley, S.M.; Robinson, S.; Sloan, A.E.; Miller, R.H.; Brady-Kalnay, S.M. Proteolytic cleavage of protein tyrosine phosphatase mu regulates glioblastoma cell migration. Cancer Res. 2009, 69, 6960–6968. [Google Scholar] [CrossRef] [Green Version]
- Brady-Kalnay, S.M.; Flint, A.J.; Tonks, N.K. Homophilic binding of PTP mu, a receptor-type protein tyrosine phosphatase, can mediate cell-cell aggregation. J. Cell Biol. 1993, 122, 961–972. [Google Scholar] [CrossRef] [Green Version]
- Phillips-Mason, P.J.; Craig, S.E.; Brady-Kalnay, S.M. A protease storm cleaves a cell-cell adhesion molecule in cancer: Multiple proteases converge to regulate PTPmu in glioma cells. J. Cell. Biochem. 2014, 115, 1609–1623. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Burgoyne, A.M.; Palomo, J.M.; Phillips-Mason, P.J.; Burden-Gulley, S.M.; Major, D.L.; Zaremba, A.; Robinson, S.; Sloan, A.E.; Vogelbaum, M.A.; Miller, R.H.; et al. PTPmu suppresses glioma cell migration and dispersal. Neuro. Oncol. 2009, 11, 767–778. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Burden-Gulley, S.M.; Gates, T.J.; Burgoyne, A.M.; Cutter, J.L.; Lodowski, D.T.; Robinson, S.; Sloan, A.E.; Miller, R.H.; Basilion, J.P.; Brady-Kalnay, S.M. A novel molecular diagnostic of glioblastomas: Detection of an extracellular fragment of protein tyrosine phosphatase mu. Neoplasia 2010, 12, 305–316. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Burden-Gulley, S.M.; Qutaish, M.Q.; Sullivant, K.E.; Tan, M.; Craig, S.E.; Basilion, J.P.; Lu, Z.-R.; Wilson, D.L.; Brady-Kalnay, S.M. Single cell molecular recognition of migrating and invading tumor cells using a targeted fluorescent probe to receptor PTPmu. Int. J. Cancer 2012, 132, 1624–1632. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Burden-Gulley, S.M.; Zhou, Z.; Craig, S.E.L.; Lu, Z.; Brady-Kalnay, S.M. Molecular Magnetic Resonance Imaging of Tumors with a PTPmu Targeted Contrast Agent. Transl. Oncol. 2013, 6, 329–337. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Herrmann, K.; Johansen, M.L.; Craig, S.E.L.; Vincent, J.A.; Howell, M.D.; Gao, Y.; Lu, L.; Erokwu, B.; Agnes, R.S.; Lu, Z.-R.; et al. Molecular Imaging of Tumors Using a Quantitative T1 Mapping Technique via Magnetic Resonance Imaging. Diagnostics 2015, 5, 318–332. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Johansen, M.L.; Gao, Y.; Hutnick, M.A.; Craig, S.E.L.; Pokorski, J.K.; Flask, C.A.; Brady-Kalnay, S.M. Quantitative Molecular Imaging with a Single Gd-Based Contrast Agent Reveals Specific Tumor Binding and Retention in Vivo. Anal. Chem. 2017, 89, 5932–5939. [Google Scholar] [CrossRef] [PubMed]
- Johansen, M.L.; Vincent, J.A.; Gittleman, H.; Craig, S.E.L.; Couce, M.; Sloan, A.E.; Barnholtz-Sloan, J.S.; Brady-Kalnay, S.M. A PTPmu Biomarker is Associated with Increased Survival in Gliomas. Int. J. Mol. Sci. 2019, 20, 2372. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Vang, R.; Ie, M.S.; Kurman, R.J. Ovarian low-grade and high-grade serous carcinoma: Pathogenesis, clinicopathologic and molecular biologic features, and diagnostic problems. Adv. Anat. Pathol. 2009, 16, 267–282. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hatano, Y.; Hatano, K.; Tamada, M.; Morishige, K.-I.; Tomita, H.; Yanai, H.; Hara, A. A Comprehensive Review of Ovarian Serous Carcinoma. Adv. Anat. Pathol. 2019, 26, 329–339. [Google Scholar] [CrossRef] [PubMed]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Histology | Endometrial Endometrioid Carcinoma | HG-EMCA | Uterine Leiomyo-Sarcoma | Endometrial Undifferentiated Carcinoma | Undifferentiated Uterine Sarcoma | Neuro-Endocrine Tumor of the Uterus | Ovarian Carcino-Sarcoma | HG-SOC | Ovarian Endometroid Carcinoma |
|---|---|---|---|---|---|---|---|---|---|
| Number of Patients | 4 | 3 | 1 | 1 | 1 | 1 | 1 | 6 | 2 |
| Tumor Grade (%) | |||||||||
| FIGO grade 1 | 1 (25) | ||||||||
| FIGO grade 2 | 1 (25) | ||||||||
| FIGO grade 3 | 2 (50) | 1 (33.3) | 1 (100) | 1 (100) | 1 (100) | 1 (100) | 1 (100) | 5 (83.3) | 1 (50) |
| High grade | 2 (66.7) | 1 (16.7) | 1 (50) | ||||||
| Tumor Stage (%) | N/A | ||||||||
| I | 1 (25) | 1 (100) | 1 (50) | ||||||
| II | 1 (50) | ||||||||
| III | 2 (50) | 1 (100) | 3 (50) | ||||||
| IV | 1 (25) | 3 (100) | 1 (100) | 1 (100) | 3 (50) | ||||
| Number African American Patients (%) | 1 (25) | 3 (100) | 0 | 0 | 1 (100) | 0 | 0 | 1 (50) | |
| Number Caucasian Patients (%) | 3 (75) | 0 | 1 (100) | 1 (100) | 0 | 1 (100) | 6 (100) | 1 (50) | |
| Mean Age | 53.5 | 70.3 | 47 | 54 | 67 | 62 | 82 | 54.0 | 60 |
| Average SBK4 staining (SE) | 44.5 (5.6) | 41.1 (6.43) | 71.91 (N/A) | 37.7 (N/A) | 52.9 (6.0) | 74.8 (N/A) | 51.2 (N/A) | 54.51 (6.0) | 49.8 (5.2) |
| Histological Type | Endometrial Clear Cell Carcinoma | Endometrial Endometrioid Carcinoma | HG-EMCA | HG-SOC | Ovarian Endometroid Carcinoma |
|---|---|---|---|---|---|
| Number of Patients | 3 | 18 | 6 | 16 | 2 |
| Tumor Grade (%) | |||||
| FIGO grade 1 | 5 (27.8) | 0 | |||
| FIGO grade 2 | 5 (27.8) | 0 | |||
| FIGO grade 3 | 8 (44.4) | 2 (100) | |||
| High grade | 3 (100) | 6 (100) | 16 (100) | ||
| Tumor Stage (ratio) | |||||
| I | 2 (2/3) | 9 (9/17) | 2 (2/6) | 0 | 1 (1/2) |
| II | 0 | 1 (1/17) | 0 | 0 | 0 |
| III | 1 (1/3) | 4 (4/17) | 1 (1/6) | 12 (12/16) | 1 (1/2) |
| IV | 0 | 3 (3/17) | 3 (3/6) | 4 (4/16) | 0 |
| Number African American Patients (ratio) | 3 (3/3) | 7 (7/16) | 5 (5/6) | 0 (0/9) | 1 (1/2) |
| Number Caucasian Patients (ratio) | 0 (0/3) | 9 (9/16) | 1 (1/6) | 9 (9/9) | 1 (1/2) |
| Mean Age (SD) | 73.3 (13.1) | 57.4 (10.5) | 68.2 (9.6) | 56.9 (8.7) | 60 (2.82) |
| Average SBK4 staining (SE) | 13.9 (3.1) | 23.4 (2.3) | 26.9 (6.6) | 44.0 (8.05) | 29.0 (1.0) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Vincent, J.; Craig, S.E.L.; Johansen, M.L.; Narla, J.; Avril, S.; DiFeo, A.; Brady-Kalnay, S.M. Detection of Tumor-Specific PTPmu in Gynecological Cancer and Patient Derived Xenografts. Diagnostics 2021, 11, 181. https://0-doi-org.brum.beds.ac.uk/10.3390/diagnostics11020181
Vincent J, Craig SEL, Johansen ML, Narla J, Avril S, DiFeo A, Brady-Kalnay SM. Detection of Tumor-Specific PTPmu in Gynecological Cancer and Patient Derived Xenografts. Diagnostics. 2021; 11(2):181. https://0-doi-org.brum.beds.ac.uk/10.3390/diagnostics11020181
Chicago/Turabian StyleVincent, Jason, Sonya E. L. Craig, Mette L. Johansen, Jyosthna Narla, Stefanie Avril, Analisa DiFeo, and Susann M. Brady-Kalnay. 2021. "Detection of Tumor-Specific PTPmu in Gynecological Cancer and Patient Derived Xenografts" Diagnostics 11, no. 2: 181. https://0-doi-org.brum.beds.ac.uk/10.3390/diagnostics11020181