
MicroRNA Expression Profile Identifies High Grade, Non-Muscle-Invasive Bladder Tumors at Elevated Risk to Progress to an Invasive Phenotype

 ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Patient Tissue Samples
2.2. RNA Extraction
2.3. Microarray Analysis
2.4. Quantitative Real Time RT-PCR
2.5. Statistical Analysis
3. Results
3.1. Discovery Sample Set
3.2. Microarray Results for miRNAs Differentially Expressed in Non-Progressive Versus Progressive High-Grade Ta and T1 Lesions: Discovery Sample Set
3.3. Validation of Differential Expression of miRNAs Using qRT-PCR: Discovery Sample Set
3.4. miRNA Expression of an Expanded Sample Set Including Patients with CIS and/or Therapy
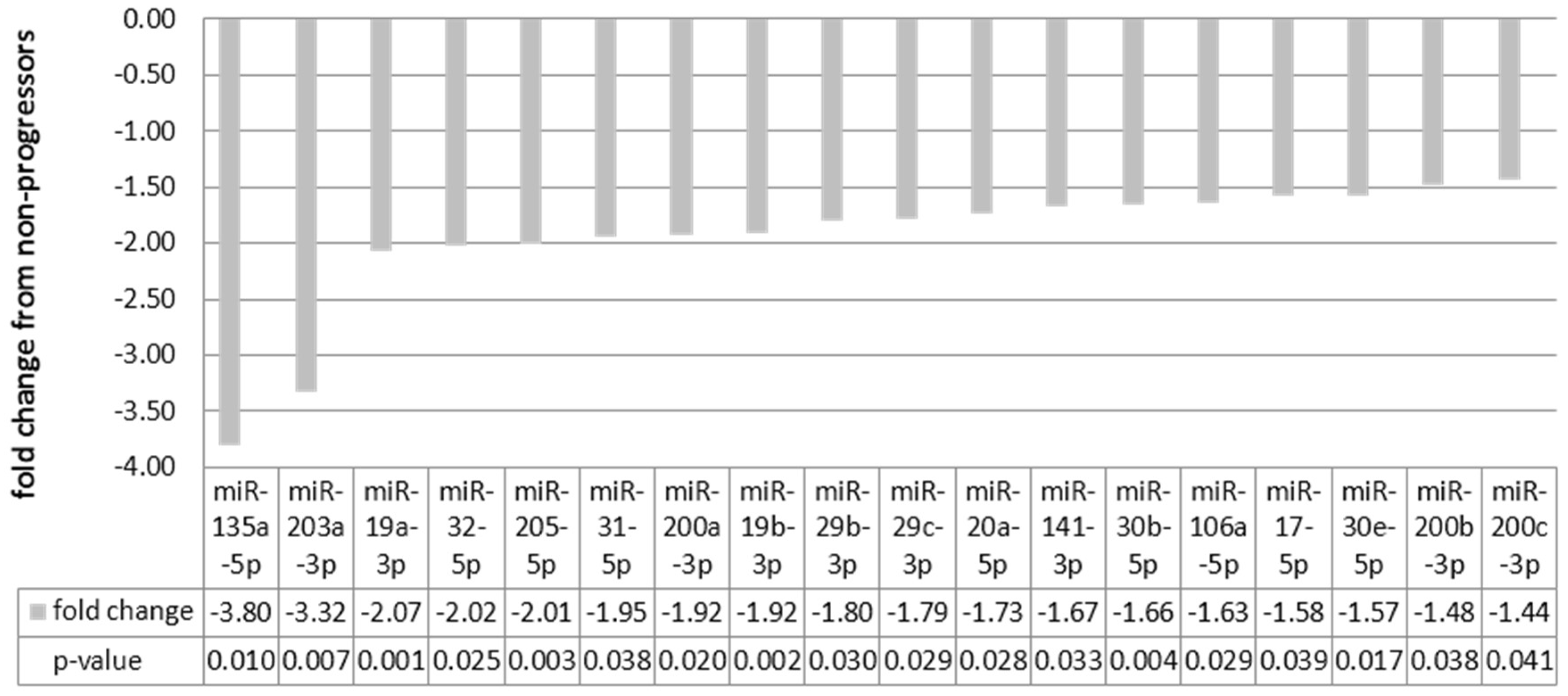
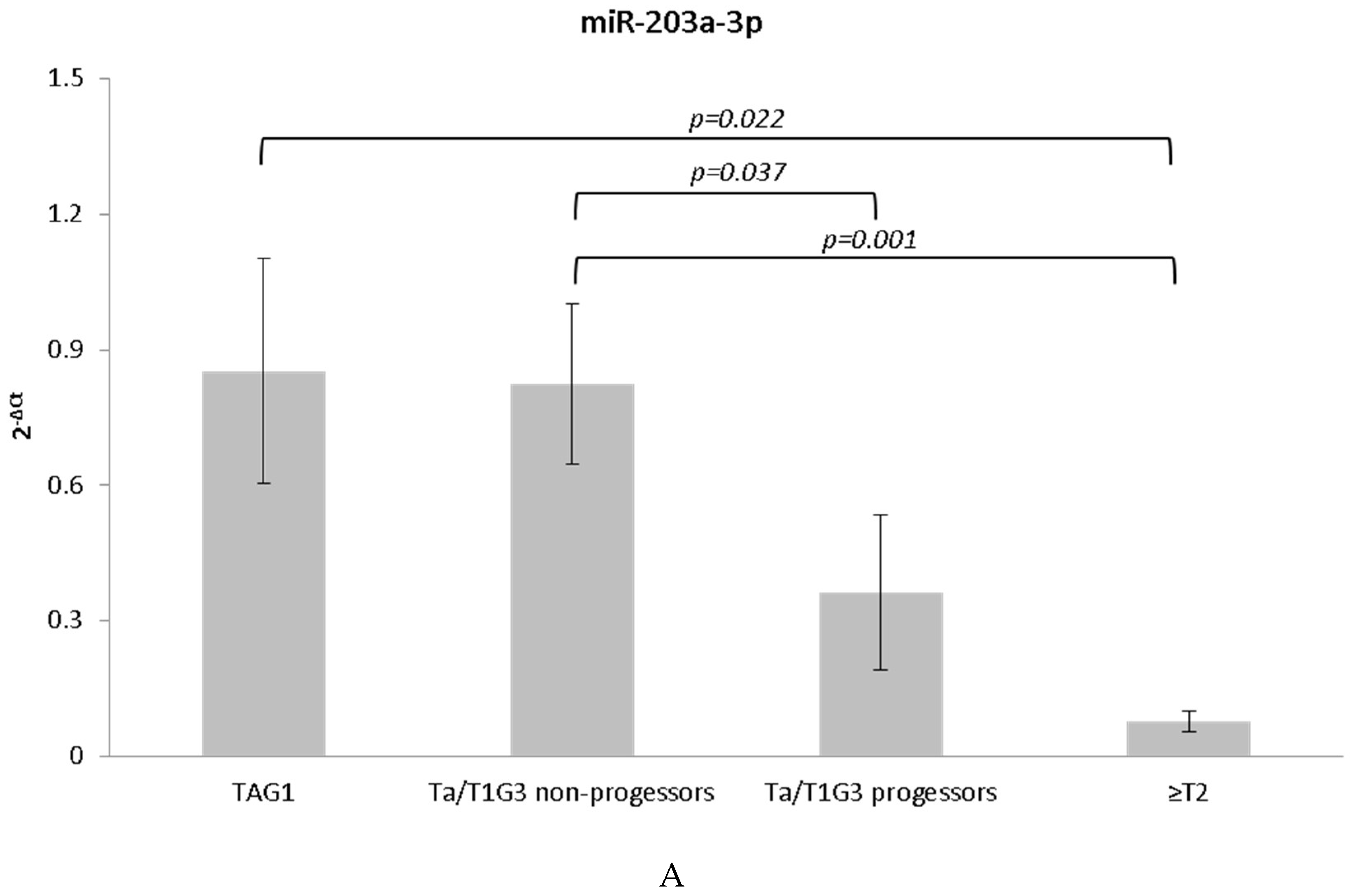
3.5. miRNAs Indicative of Progression
3.6. miRNAs Indicative of Mortality
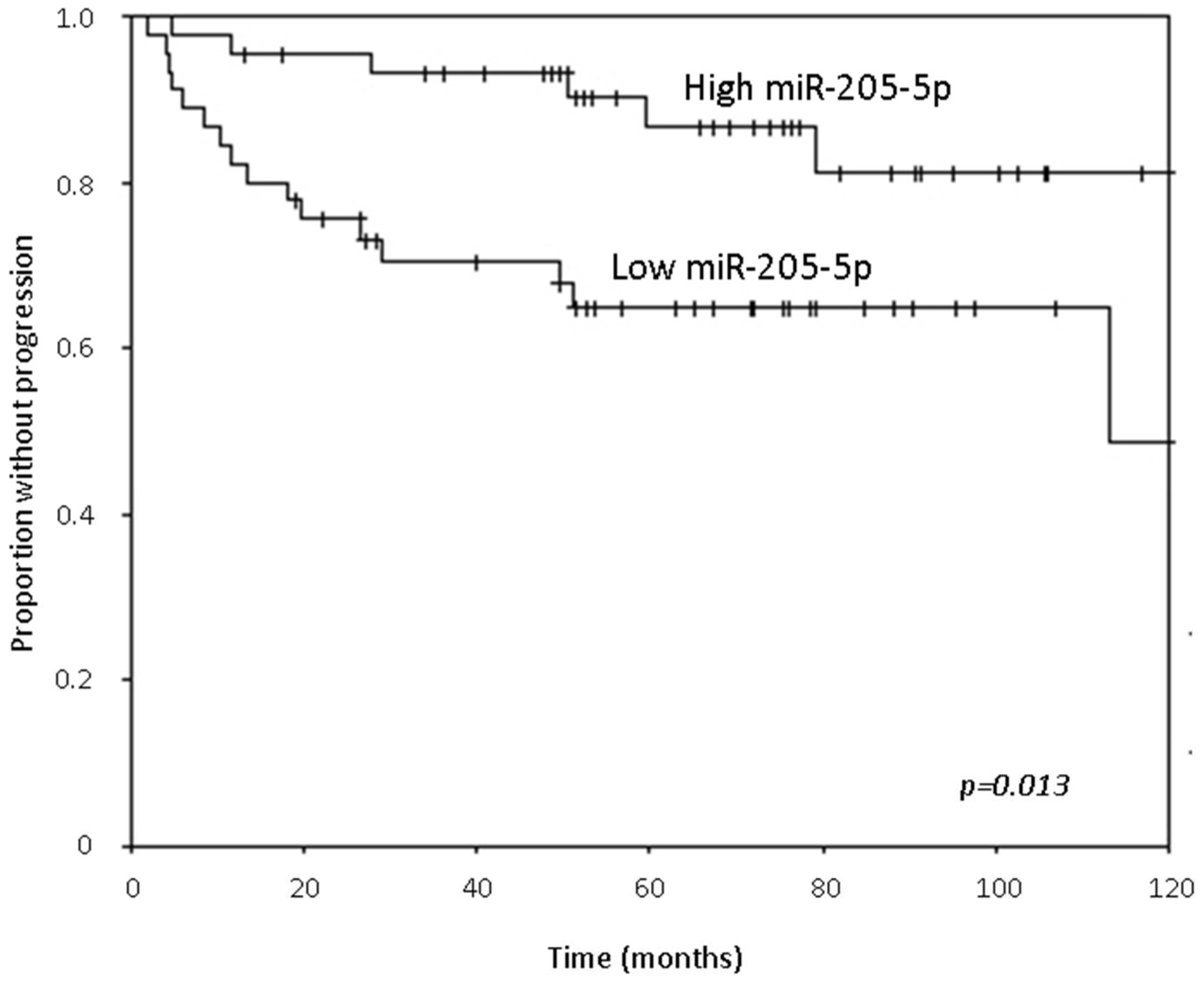
3.7. Time to Progression Analyses
3.8. Time to Death Analyses
4. Discussion
5. Conclusions
Supplementary Materials
Acknowledgments
Author Contributions
Conflicts of Interest
References
- National Cancer Institute. Available online: http://www.cancer.gov/cancertopics/types/bladder (accessed on 20 July 2016).
- Jung, I.; Messing, E. Molecular mechanisms and pathways in bladder cancer development and progression. Cancer Control 2000, 7, 325–334. [Google Scholar] [PubMed]
- Kamat, A.M.; Hahn, N.M.; Efstathiou, J.A.; Lerner, S.P.; Malmström, P.U.; Choi, W.; Guo, C.C.; Lotan, Y.; Kassouf, W. Bladder cancer. Lancet 2016. [Google Scholar] [CrossRef]
- Serretta, V.; Ruggirello, A.; Dispensa, N.; Allegro, R.; Aragona, F.; Melloni, D. Multiplicity and history have a detrimental effect on survival of patients with T1G3 bladder tumors selected for conservative treatment. J. Urol. 2008, 180, 886–891. [Google Scholar] [CrossRef] [PubMed]
- Van den Bosch, S.; Witjes, J.A. Long-term cancer-specific survival in patients with high-risk, non-muscle-invasive bladder cancer and tumour progression: A systematic review. Eur. Urol. 2011, 60, 493–500. [Google Scholar] [CrossRef] [PubMed]
- Chang, S.S.; Boorjian, S.A.; Chou, R.; Clark, P.E.; Daneshmand, S.; Konety, B.R.; Pruthi, R.; Quale, D.Z.; Ritch, C.R.; Seigne, J.D.; et al. Diagnosis and treatment of non-muscle invasive bladder cancer: AUA/SUO guideline. J. Urol. 2016, 196, 1021–1029. [Google Scholar] [CrossRef] [PubMed]
- Pasin, E.; Josephson, D.Y.; Mitra, A.P.; Cote, R.J.; Stein, J.P. Superficial bladder cancer: An update on etiology, molecular development, classification, and natural history. Rev. Urol. 2008, 10, 31–43. [Google Scholar] [PubMed]
- Bryan, R.T.; Wallace, D.M. “Superficial” bladder cancer—Time to uncouple pT1 tumours from pTa tumours. BJU Int. 2002, 90, 846–852. [Google Scholar] [CrossRef] [PubMed]
- Jimenez, R.E.; Gheiler, E.; Oskanian, P.; Tiguert, R.; Sakr, W.; Wood, D.P., Jr.; Pontes, J.E.; Grignon, D.J. Grading the invasive component of urothelial carcinoma of the bladder and its relationship with progression-free survival. Am. J. Surg. Pathol. 2000, 24, 980–987. [Google Scholar] [CrossRef] [PubMed]
- Herr, H.W. Tumor progression and survival of patients with high grade, noninvasive papillary (TaG3) bladder tumors: 15-year outcome. J. Urol. 2000, 163, 60–61. [Google Scholar] [CrossRef]
- Sylvester, R.J.; van der Meijden, A.; Witjes, J.A.; Jakse, G.; Nonomura, N.; Cheng, C.; Torres, A.; Watson, R.; Kurth, K.H. High-grade Ta urothelial carcinoma and carcinoma in situ of the bladder. Urology 2005, 66, 90–107. [Google Scholar] [CrossRef] [PubMed]
- Schwaibold, H.E.; Sivalingam, S.; May, F.; Hartung, R. The value of a second transurethral resection for T1 bladder cancer. BJU Int. 2006, 97, 1199–1201. [Google Scholar] [CrossRef] [PubMed]
- Dalbagni, G.; Vora, K.; Kaag, M.; Cronin, A.; Bochner, B.; Donat, S.M.; Herr, H.W. Clinical outcome in a contemporary series of restaged patients with clinical T1 bladder cancer. Eur. Urol. 2009, 56, 903–910. [Google Scholar] [CrossRef] [PubMed]
- The Cancer Genome Atlas Research Network. Comprehensive molecular characterization of urothelial bladder carcinoma. Nature 2014, 507, 315–322. [Google Scholar]
- Thykjaer, T.; Workman, C.; Kruhoffer, M.; Demtröder, K.; Wolf, H.; Andersen, L.D.; Frederiksen, C.M.; Knudsen, S.; Orntoft, T.F. Identification of gene expression patterns in superficial and invasive human bladder cancer. Cancer Res. 2001, 61, 2492–2499. [Google Scholar] [PubMed]
- Hedegaard, J.; Lamy, P.; Nordentoft, I.; Algaba, F.; Høyer, S.; Ulhøi, B.P.; Vang, S.; Reinert, T.; Hermann, G.G.; Mogensen, K.; et al. Comprehensive transcriptional analysis of early-stage urothelial carcinoma. Cancer Cell 2016, 30, 27–42. [Google Scholar] [CrossRef] [PubMed]
- Choi, W.; Porten, S.; Kim, S.; Willis, D.; Plimack, E.R.; Hoffman-Censits, J.; Roth, B.; Cheng, T.; Tran, M.; Lee, I.L.; et al. Identification of distinct basal and luminal subtypes of muscle-invasive bladder cancer with different sensitivities to frontline chemotherapy. Cancer Cell 2014, 25, 152–165. [Google Scholar] [CrossRef] [PubMed]
- Dyrskjot, L.; Thykjaer, T.; Kruhoffer, M.; Jensen, J.L.; Marcussen, N.; Hamilton-Dutoit, S.; Wolf, H.; Orntoft, T.F. Identifying distinct classes of bladder carcinoma using microarrays. Nat. Genet. 2003, 33, 90–96. [Google Scholar] [CrossRef] [PubMed]
- Knowles, M.A.; Hurst, C.D. Molecular biology of bladder cancer: New insights into pathogenesis and clinical diversity. Nat. Rev. Cancer 2015, 15, 25–41. [Google Scholar] [CrossRef] [PubMed]
- Smith, S.C.; Baras, A.S.; Dancik, G.; Ru, Y.; Ding, K.F.; Moskaluk, C.A.; Fradet, Y.; Lehmann, J.; Stöckle, M.; Hartmann, A.; et al. A 20-gene model for molecular nodal staging of bladder cancer: Development and prospective assessment. Lancet Oncol. 2011, 12, 137–143. [Google Scholar] [CrossRef]
- Liu, Y.; Noon, A.P.; Aguiar Cabeza, E.; Shen, J.; Kuk, C.; Ilczynski, C.; Ni, R.; Sukhu, B.; Chan, K.; Barbosa-Morais, N.L.; et al. Next-generation RNA sequencing of archival formalin-fixed paraffin-embedded urothelial bladder cancer. Eur. Urol. 2014, 66, 982–986. [Google Scholar] [CrossRef] [PubMed]
- Dyrskjot, L.; Zieger, K.; Kruhoffer, M.; Thykjaer, T.; Jensen, J.L.; Primdahl, H.; Aziz, N.; Marcussen, N.; Møller, K.; Orntoft, T.F. A molecular signature in superficial bladder carcinoma predicts clinical outcome. Clin. Cancer Res. 2005, 11, 4029–4036. [Google Scholar] [CrossRef]
- Mitra, A.P.; Pagliarulo, V.; Yang, D.; Waldman, F.M.; Datar, R.H.; Skinner, D.G.; Groshen, S.; Cote, R.J. Generation of a concise gene panel for outcome prediction in urinary bladder cancer. J. Clin. Oncol. 2009, 27, 3929–3937. [Google Scholar] [CrossRef] [PubMed]
- Mitra, A.P.; Lam, L.L.; Ghadessi, M.; Erho, N.; Vergara, I.A.; Alshalalfa, M.; Buerki, C.; Haddad, Z.; Sierocinski, T.; Triche, T.J.; et al. Discovery and validation of novel expression signature for postcystectomy recurrence in high-risk bladder cancer. J. Natl. Cancer Inst. 2014, 106. [Google Scholar] [CrossRef] [PubMed]
- Jeong, P.; Ha, Y.S.; Cho, I.C.; Yun, S.J.; Yoo, E.S.; Kim, I.Y.; Choi, Y.H.; Moon, S.K.; Kim, W.J. Three-gene signature predicts disease progression of non-muscle invasive bladder cancer. Oncol. Lett. 2011, 2, 679–684. [Google Scholar] [PubMed]
- Takata, R.; Katagiri, T.; Kanehira, M.; Tsunoda, T.; Shuin, T.; Miki, T.; Namiki, M.; Kohri, K.; Matsushita, Y.; Fujioka, T.; et al. Predicting response to methotrexate, vinblastine, doxorubicin, and cisplatin neoadjuvant chemotherapy for bladder cancers through genome-wide gene expression profiling. Clin. Cancer Res. 2005, 11, 2625–2636. [Google Scholar] [CrossRef] [PubMed]
- Bellmunt, J.; Pons, F.; Orsola, A. Molecular determinants of response to cisplatin-based neoadjuvant chemotherapy. Curr. Opin. Urol. 2013, 23, 466–471. [Google Scholar] [CrossRef] [PubMed]
- Gottardo, F.; Liu, C.G.; Ferracin, M.; Calin, G.A.; Fassan, M.; Bassi, P.; Sevignani, C.; Byrne, D.; Negrini, M.; Pagano, F.; et al. Micro-RNA profiling in kidney and bladder cancers. Urol. Oncol. 2007, 25, 387–392. [Google Scholar] [CrossRef] [PubMed]
- Veerla, S.; Lindgren, D.; Kvist, A.; Frigyesi, A.; Staaf, J.; Persson, H.; Liedberg, F.; Chebil, G.; Gudjonsson, S.; Borg, A.; et al. MiRNA expression in urothelial carcinomas: Important roles of miR-10a, miR-222, miR-125b-5p, miR-7 and miR-452 for tumor stage and metastasis, and frequent homozygous losses of miR-31–5p. Int. J. Cancer 2008, 124, 2236–2242. [Google Scholar] [CrossRef] [PubMed]
- Schaefer, A.; Jung, M.; Kristiansen, G.; Lein, M.; Schrader, M.; Miller, K.; Stephan, C.; Jung, K. MicroRNAs and cancer: Current state and future perspectives in urologic oncology. Urol. Oncol. 2008, 28, 413. [Google Scholar] [CrossRef] [PubMed]
- Catto, J.W.; Miah, S.; Owen, H.C.; Bryant, H.; Myers, K.; Dudziec, E.; Larré, S.; Milo, M.; Rehman, I.; Rosario, D.J.; et al. Distinct microRNA alterations characterize high- and low-grade bladder cancer. Cancer Res. 2009, 69, 8472–8481. [Google Scholar] [CrossRef] [PubMed]
- Lin, T.; Dong, W.; Huang, J.; Pan, Q.; Fan, X.; Zhang, C.; Huang, L. MicroRNA-143–3p as a tumor suppressor for bladder cancer. J. Urol. 2009, 181, 1372–1380. [Google Scholar] [CrossRef] [PubMed]
- Dyrskjot, L.; Ostenfeld, M.S.; Bramsen, J.B.; Silahtaroglu, A.N.; Lamy, P.; Ramanathan, R.; Fristrup, N.; Jensen, J.L.; Andersen, C.L.; Zieger, K.; et al. Genomic profiling of microRNAs in bladder cancer: MiR-129 is associated with poor outcome and promotes cell death in vitro. Cancer Res. 2009, 69, 4851–4860. [Google Scholar] [CrossRef] [PubMed]
- Baffa, R.; Fassan, M.; Volinia, S.; O’Hara, B.; Liu, C.G.; Palazzo, J.P.; Gardiman, M.; Rugge, M.; Gomella, L.G.; Croce, C.M.; et al. MicroRNA expression profiling of human metastatic cancers identifies cancer gene targets. J. Pathol. 2009, 219, 214–221. [Google Scholar] [CrossRef]
- Ratert, N.; Meyer, H.A.; Jung, M.; Lioudmer, P.; Mollenkopf, H.J.; Wagner, I.; Miller, K.; Kilic, E.; Erbersdobler, A.; Weikert, S.; et al. MiRNA profiling identifies candidate mirnas for bladder cancer diagnosis and clinical outcome. J. Mol. Diagn. 2013, 15, 695–705. [Google Scholar] [CrossRef] [PubMed]
- Dip, N.; Reis, S.T.; Timoszczuk, L.S.; Viana, N.I.; Piantino, C.B.; Morais, D.R.; Moura, C.M.; Abe, D.K.; Silva, I.A.; Srougi, M.; et al. Stage, grade and behavior of bladder urothelial carcinoma defined by the microRNA expression profile. J. Urol. 2012, 188, 1951–1956. [Google Scholar] [CrossRef] [PubMed]
- Rosenberg, E.; Baniel, J.; Spector, Y.; Faerman, A.; Meiri, E.; Aharonov, R.; Margel, D.; Goren, Y.; Nativ, O. Predicting progression of bladder urothelial carcinoma using microRNA expression. BJU Int. 2013, 112, 1027–1034. [Google Scholar] [CrossRef] [PubMed]
- Neely, L.A.; Rieger-Christ, K.M.; Silva Neto, B.S.; Eroshkin, A.; Garver, J.; Patel, S.; Phung, N.A.; McLaughlin, S.; Libertino, J.A.; Whitney, D.; et al. A microRNA expression ratio defining the invasive phenotype in bladder tumors. Urol. Oncol. 2008, 28, 39–48. [Google Scholar] [CrossRef] [PubMed]
- Wszoleck, M.; Rieger-Christ, K.M.; Kenney, P.A.; Gould, J.J.; Silva Neto, B.; LaVoie, A.K.; Logvinenko, T.; Libertino, J.A.; Summerhayes, I.C. MicroRNA expression profiles and biomarkers linked to the invasive bladder tumor phenotype. Urol. Oncol. 2011, 29, 794–801. [Google Scholar] [CrossRef] [PubMed]
- Gregory, P.A.; Bert, A.G.; Paterson, E.L.; Barry, S.C.; Tsykin, A.; Farshid, G.; Vadas, M.A.; Khew-Goodall, Y.; Goodall, G.J. The miR-200 family and miR-205-5p regulate epithelial to mesenchymal transition by targeting ZEB1 and SIP1. Nat. Cell Biol. 2008, 10, 593–601. [Google Scholar] [CrossRef] [PubMed]
- Korpal, M.; Lee, E.S.; Hu, G.; Kang, Y. The miR-200 family inhibits epithelial-mesenchymal transition and cancer cell migration by direct targeting of E-cadherin transcriptional repressors ZEB1 and ZEB2. J. Biol. Chem. 2008, 283, 14910–14914. [Google Scholar] [CrossRef] [PubMed]
- Park, S.M.; Gaur, A.B.; Lengye, E.; Peter, M.E. The miR-200 family determines the epithelial phenotype of cancer cells by targeting the E-cadherin repressors ZEB1 and ZEB2. Genes Dev. 2008, 22, 894–907. [Google Scholar] [CrossRef] [PubMed]
- Majid, S.; Dar, A.A.; Saini, S.; Deng, G.; Chang, I.; Greene, K.; Tanaka, Y.; Dahiya, R.; Yamamura, S. MicroRNA-23b functions as a tumor suppressor by regulating Zeb1 in bladder cancer. PLoS ONE 2013, 8, e67686. [Google Scholar] [CrossRef]
- Zaravinos, A.; Radojicic, J.; Lambrou, G.I.; Volanis, D.; Delakas, D.; Stathopoulos, E.N.; Spandidos, D.A. Expression of miRNAs involved in angiogenesis, tumor cell proliferation, tumor suppressor inhibition, epithelial-mesenchymal transition and activation of metastasis in bladder cancer. J. Urol. 2012, 188, 615–623. [Google Scholar] [CrossRef] [PubMed]
- Van der Heijden, A.G.; Witjes, J.A. Recurrence, progression, and follow-up in non–muscle-invasive bladder cancer. Eur. Urol. Sup. 2009, 8, 556–562. [Google Scholar] [CrossRef]
- Sonkoly, E.; Wei, T.; Janson, P.C.; Sääf, A.; Lundeberg, L.; Tengvall-Linder, M.; Norstedt, G.; Alenius, H.; Homey, B.; Scheynius, A.; et al. MicroRNAs: Novel regulators involved in the pathogenesis of psoriasis? PLoS ONE 2007, 2, e610. [Google Scholar] [CrossRef] [PubMed]
- Yi, R.; Poy, M.N.; Stoffel, M.; Fuchs, E. A skin microRNA promotes differentiation by repressing “stemness”. Nature 2008, 452, 225–229. [Google Scholar] [CrossRef] [PubMed]
- Bueno, M.J.; Pérez de Castro, I.; Gómez de Cedrón, M.; Santos, J.; Calin, G.A.; Cigudosa, J.C.; Croce, C.M.; Fernández-Piqueras, J.; Malumbres, M. Genetic and epigenetic silencing of microRNA-203 enhances ABL1 and BCR-ABL1 oncogene expression. Cancer Cell 2008, 13, 496–506. [Google Scholar] [CrossRef] [PubMed]
- Greene, S.B.; Gunaratne, P.H.; Hammond, S.M.; Rosen, J.M. A putative role for microRNA-205-5p in mammary epithelial cell progenitors. J. Cell Sci. 2010, 123, 606–618. [Google Scholar] [CrossRef] [PubMed]
- Iorio, M.V.; Casalini, P.; Piovan, C.; Di Leva, G.; Merlo, A.; Triulzi, T.; Ménard, S.; Croce, C.M.; Tagliabue, E. MicroRNA-205-5p regulates HER3 in human breast cancer. Cancer Res. 2009, 69, 2195–2200. [Google Scholar] [CrossRef] [PubMed]
- Yu, J.; Ryan, D.G.; Getsios, S.; Oliveira-Fernandes, M.; Fatima, A.; Lavker, R.M. MicroRNA-184 antagonizes microRNA-205-5p to maintain SHIP2 levels in epithelia. Proc. Natl. Acad. Sci. USA 2008, 105, 19300–19305. [Google Scholar] [CrossRef] [PubMed]
- Wu, H.; Zhu, S.; Mo, Y.Y. Suppression of cell growth and invasion by miR-205-5p in breast cancer. Cell Res. 2009, 19, 439–448. [Google Scholar] [CrossRef] [PubMed]
- Gandellini, P.; Folini, M.; Longoni, N.; Pennati, M.; Binda, M.; Colecchia, M.; Salvioni, R.; Supino, R.; Moretti, R.; Limonta, P.; et al. miR-205-5p Exerts tumor-suppressive functions in human prostate through down-regulation of protein kinase Cε. Cancer Res. 2009, 69, 2287–2295. [Google Scholar] [CrossRef] [PubMed]
- Ma, H.; Pan, J.S.; Jin, L.X.; Wu, J.; Ren, Y.D.; Chen, P.; Xiao, C.; Han, J. MicroRNA-17-5p~92 inhibits colorectal cancer progression by targeting angiogenesis. Cancer Lett. 2016, 376, 293–302. [Google Scholar] [CrossRef] [PubMed]
- Bo, J.; Yang, G.; Huo, K.; Jiang, H.; Zhang, L.; Liu, D.; Huang, Y. MicroRNA-203 suppresses bladder cancer development by repressing bcl-w expression. FEBS J. 2011, 278, 786–792. [Google Scholar] [CrossRef] [PubMed]
- Wiklund, E.D.; Bramsen, J.B.; Hulf, T.; Dyrskjøt, L.; Ramanathan, R.; Hansen, T.B.; Villadsen, S.B.; Gao, S.; Ostenfeld, M.S.; Borre, M.; et al. Coordinated epigenetic repression of the miR-200 family and miR-205-5p in invasive bladder cancer. Int. J. Cancer 2011, 128, 1327–1334. [Google Scholar] [CrossRef] [PubMed]
- Inamoto, T.; Taniguchi, K.; Takahara, K.; Iwatsuki, A.; Takai, T.; Komura, K.; Yoshikawa, Y.; Uchimoto, T.; Saito, K.; Tanda, N.; et al. Intravesical administration of exogenous microRNA-145-5p as a therapy for mouse orthotopic human bladder cancer xenograft. Oncotarget 2015, 6, 21628–21635. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Table 1A: Discovery Sample Set | Non-Progressor | Progressor |
| n | 10 | 7 |
| TaG3/T1G3 (n/n) | 5/5 | 4/3 |
| Male (%) | 70 | 86 |
| Age (mean years ± SD) | 71 ± 8 | 73 ± 7 |
| Time to progression (mean mo ± SD) | n/a | 34 ± 37 |
| Time to follow-up (mean mo ± SD) | 88 ± 29 | 55 ± 43 |
| Table 1B: Expanded Sample Set | Non-Progressor | Progressor |
| n | 67 | 22 |
| TaG3/T1G3 (n/n) | 37/30 | 7/15 |
| Male (%) | 78 | 86 |
| Age (mean yrs ± SD) | 69 ± 9 | 73 ± 7 |
| Time to progression (mean mo ± SD) | n/a | 25 ± 26 |
| Time to follow-up (mean mo ± SD) | 73 ± 32 | 49 ± 33 |
| Intravesical therapy (n, %) | 11, 16% | 5, 23% |
| Status (alive, %) | 49, 73% | 10, 45% |
| Site (Lahey/UW) | 53/14 | 18/4 |
| microRNA | Microarray Fold Change | qRT-PCR | |||||
|---|---|---|---|---|---|---|---|
| Fold Change | p-Value | Non-Progressors | Progressors | ||||
| Mean | Std. Dev. | Mean | Std. Dev. | ||||
| hsa-miR-125b-5p | 2.46 | 3.28 | 0.057 | 0.64 | 1.10 | 2.09 | 1.54 |
| hsa-miR-145-5p | 2.09 | 3.51 | 0.031 | 0.10 | 0.10 | 0.37 | 0.25 |
| hsa-miR-223-3p | 1.82 | 4.32 | 0.102 | 0.26 | 0.23 | 1.11 | 1.16 |
| hsa-miR-143-3p | 1.70 | 1.96 | 0.103 | 0.15 | 0.20 | 0.30 | 0.15 |
| hsa-miR-338-5p | 1.69 | 2.96 | 0.274 | 0.00 | 0.00 | 0.01 | 0.02 |
| hsa-miR-31-5p | −2.71 | −2.24 | 0.143 | 5.24 | 5.29 | 2.34 | 2.10 |
| hsa-miR-203a-3p | −2.59 | −4.75 | 0.025 | 0.54 | 0.49 | 0.11 | 0.13 |
| hsa-miR-141-3p | −2.44 | −3.04 | 0.008 | 2.18 | 1.25 | 0.72 | 0.71 |
| hsa-miR-200a-3p | −2.25 | −2.19 | 0.021 | 5.12 | 2.85 | 2.34 | 1.56 |
| hsa-miR-205-5p | −2.12 | −3.05 | 0.034 | 15.97 | 12.90 | 5.24 | 5.06 |
| hsa-miR-429 | −2.09 | −1.55 | 0.366 | 0.63 | 0.62 | 0.41 | 0.36 |
| hsa-miR-29c-3p | −1.92 | −1.61 | 0.339 | 1.02 | 1.08 | 0.63 | 0.50 |
| hsa-miR-20a-5p | −1.88 | −1.43 | 0.299 | 1.79 | 1.15 | 1.25 | 0.91 |
| hsa-miR-29b-3p | −1.86 | −1.87 | 0.064 | 0.36 | 0.23 | 0.19 | 0.10 |
| hsa-miR-19b-3p | −1.77 | −2.13 | 0.080 | 1.73 | 1.36 | 0.81 | 0.59 |
| hsa-miR-17-5p | −1.72 | −1.29 | 0.443 | 1.87 | 1.12 | 1.45 | 1.04 |
| hsa-miR-106a-5p | −1.71 | −1.29 | 0.446 | 1.67 | 0.99 | 1.30 | 0.97 |
| hsa-miR-200b-3p | −1.63 | −1.34 | 0.335 | 4.98 | 2.29 | 3.70 | 2.76 |
| hsa-miR-30e-5p | −1.58 | −1.23 | 0.547 | 0.88 | 0.77 | 0.72 | 0.29 |
| All Patients of the Expanded Sample Set (n = 88) | Without Therapy | With Therapy | ||||
| miRNA | fold change | p-value | mean | std. dev. | mean | std. dev. |
| hsa-miR-15a-5p | −3.00 | <0.001 | 0.37 | 0.32 | 0.12 | 0.05 |
| hsa-miR-20a-5p | −2.71 | <0.001 | 1.40 | 1.38 | 0.52 | 0.29 |
| hsa-miR-21-5p | −2.24 | 0.003 | 8.83 | 10.31 | 3.93 | 3.86 |
| hsa-miR-200a-3p | −3.58 | <0.001 | 3.65 | 5.25 | 1.02 | 1.06 |
| hsa-miR-1308 | −2.79 | <0.001 | 171.92 | 191.95 | 61.63 | 42.86 |
| Within Progressors Only (n = 21) | Without Therapy | With Therapy | ||||
| miRNA | fold change | p-value | mean | std. dev. | mean | std. dev. |
| hsa-miR-15a-5p | −2.32 | 0.004 | 0.33 | 0.15 | 0.14 | 0.06 |
| hsa-miR-32-5p | −3.13 | 0.010 | 0.01 | 0.01 | 0.00 | 0.00 |
| hsa-miR-141-3p | −3.02 | 0.011 | 0.88 | 0.77 | 0.29 | 0.19 |
| hsa-miR-200a-3p | −2.31 | 0.011 | 2.11 | 1.37 | 0.91 | 0.48 |
| hsa-miR-200c-3p | −2.05 | 0.014 | 10.51 | 6.26 | 5.12 | 2.33 |
| hsa-miR-429 | −2.17 | 0.034 | 0.32 | 0.28 | 0.15 | 0.07 |
| Within Non-Progressors Only (n = 67) | Without Therapy | With Therapy | ||||
| miRNA | fold change | p-value | mean | std. dev. | mean | std. dev. |
| hsa-miR-15a-5p | −3.33 | <0.001 | 0.38 | 0.36 | 0.11 | 0.05 |
| hsa-miR-17-5p | −2.56 | <0.001 | 1.82 | 1.62 | 0.71 | 0.46 |
| hsa-miR-19a-3p | −2.93 | <0.001 | 0.24 | 0.26 | 0.08 | 0.06 |
| hsa-miR-19b-3p | −2.20 | 0.004 | 1.58 | 1.73 | 0.72 | 0.57 |
| hsa-miR-20a-5p | −2.99 | <0.001 | 1.55 | 1.48 | 0.52 | 0.33 |
| hsa-miR-21-5p | −3.21 | <0.001 | 9.87 | 11.36 | 3.08 | 3.52 |
| hsa-miR-29b-3p | −2.37 | 0.008 | 0.42 | 0.63 | 0.18 | 0.09 |
| hsa-miR-30b-5p | −1.64 | 0.012 | 3.10 | 3.07 | 1.89 | 0.75 |
| hsa-miR-30e-5p | −1.90 | 0.005 | 1.36 | 1.31 | 0.71 | 0.28 |
| hsa-miR-32-5p | −2.23 | 0.018 | 0.01 | 0.02 | 0.01 | 0.00 |
| hsa-miR-106a-5p | −2.27 | 0.002 | 1.66 | 1.51 | 0.73 | 0.52 |
| hsa-miR-135a-5p | −6.99 | 0.003 | 0.08 | 0.14 | 0.01 | 0.01 |
| hsa-miR-141-3p | −2.42 | 0.005 | 1.41 | 1.48 | 0.59 | 0.64 |
| hsa-miR-200a-3p | −3.90 | <0.001 | 4.11 | 5.88 | 1.06 | 1.23 |
| hsa-miR-200b-3p | −2.27 | 0.003 | 4.68 | 4.24 | 2.07 | 1.95 |
| hsa-miR-203a-3p | −2.99 | 0.010 | 0.93 | 1.58 | 0.31 | 0.32 |
| hsa-miR-301a-3p | −5.56 | 0.012 | 0.09 | 0.20 | 0.02 | 0.01 |
| hsa-miR-429 | −3.72 | 0.002 | 0.56 | 0.86 | 0.15 | 0.18 |
| hsa-miR-1308 | −2.81 | 0.001 | 177.74 | 208.59 | 63.22 | 37.36 |
© 2017 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license ( http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lenherr, S.M.; Tsai, S.; Silva Neto, B.; Sullivan, T.B.; Cimmino, C.B.; Logvinenko, T.; Gee, J.; Huang, W.; Libertino, J.A.; Summerhayes, I.C.; et al. MicroRNA Expression Profile Identifies High Grade, Non-Muscle-Invasive Bladder Tumors at Elevated Risk to Progress to an Invasive Phenotype. Genes 2017, 8, 77. https://0-doi-org.brum.beds.ac.uk/10.3390/genes8020077
Lenherr SM, Tsai S, Silva Neto B, Sullivan TB, Cimmino CB, Logvinenko T, Gee J, Huang W, Libertino JA, Summerhayes IC, et al. MicroRNA Expression Profile Identifies High Grade, Non-Muscle-Invasive Bladder Tumors at Elevated Risk to Progress to an Invasive Phenotype. Genes. 2017; 8(2):77. https://0-doi-org.brum.beds.ac.uk/10.3390/genes8020077
Chicago/Turabian StyleLenherr, Sara M., Sheaumei Tsai, Brasil Silva Neto, Travis B. Sullivan, Cara B. Cimmino, Tanya Logvinenko, Jason Gee, Wei Huang, John A. Libertino, Ian C. Summerhayes, and et al. 2017. "MicroRNA Expression Profile Identifies High Grade, Non-Muscle-Invasive Bladder Tumors at Elevated Risk to Progress to an Invasive Phenotype" Genes 8, no. 2: 77. https://0-doi-org.brum.beds.ac.uk/10.3390/genes8020077