
Knowledge, Attitudes, and Perception towards COVID-19 among Medical Students in Yemen: A Cross-Sectional Survey
 , , , , , , , ,
, , , , , , , , 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design and Population Selection
2.2. Data Collection
- Sociodemographic characteristics of the participants, including age, gender, residence area, educational level, and specialty.
- Knowledge of COVID-19, including sources of COVID-19 information, COVID-19 mode of transmission, COVID-19 symptoms, and preventive measures adopted to avoid contracting COVID-19 (21 questions).
- Attitudes and behaviors that may be associated with the prevention of the spread of the virus (15 questions).
- Perception about the virus and the disease including the dangers of the disease, possibility that another family member is infected with the virus, the infection is associated with stigma, the media coverage of the disease, and the virus is initially designed as a biological weapon (5 questions).
2.3. Validation and Trialling of the Study
2.4. Sampling
2.5. Ethical Considerations
2.6. Statistical Analysis
3. Results
3.1. Baseline Characteristics of the Participants
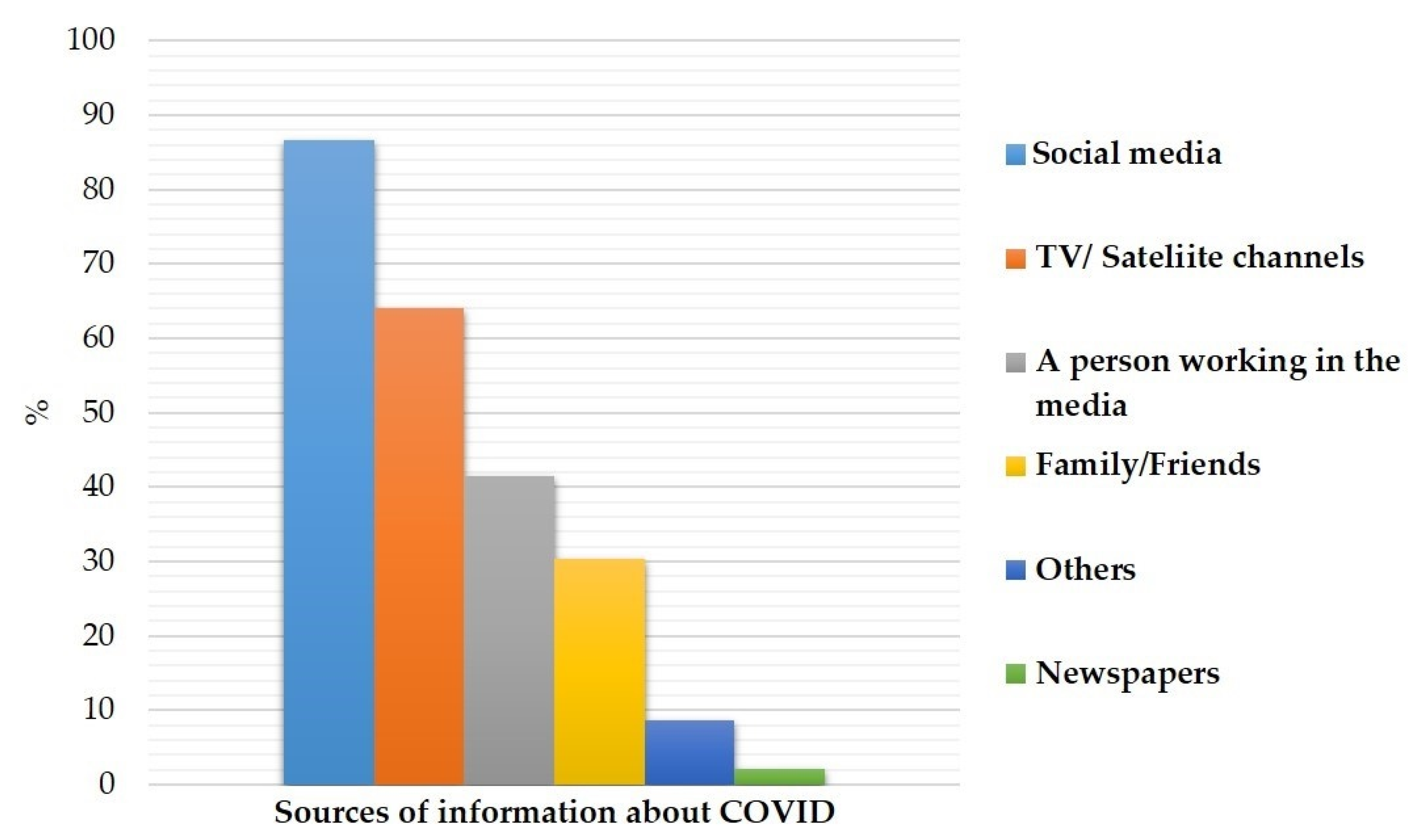
3.2. Sources of Information about COVID-19
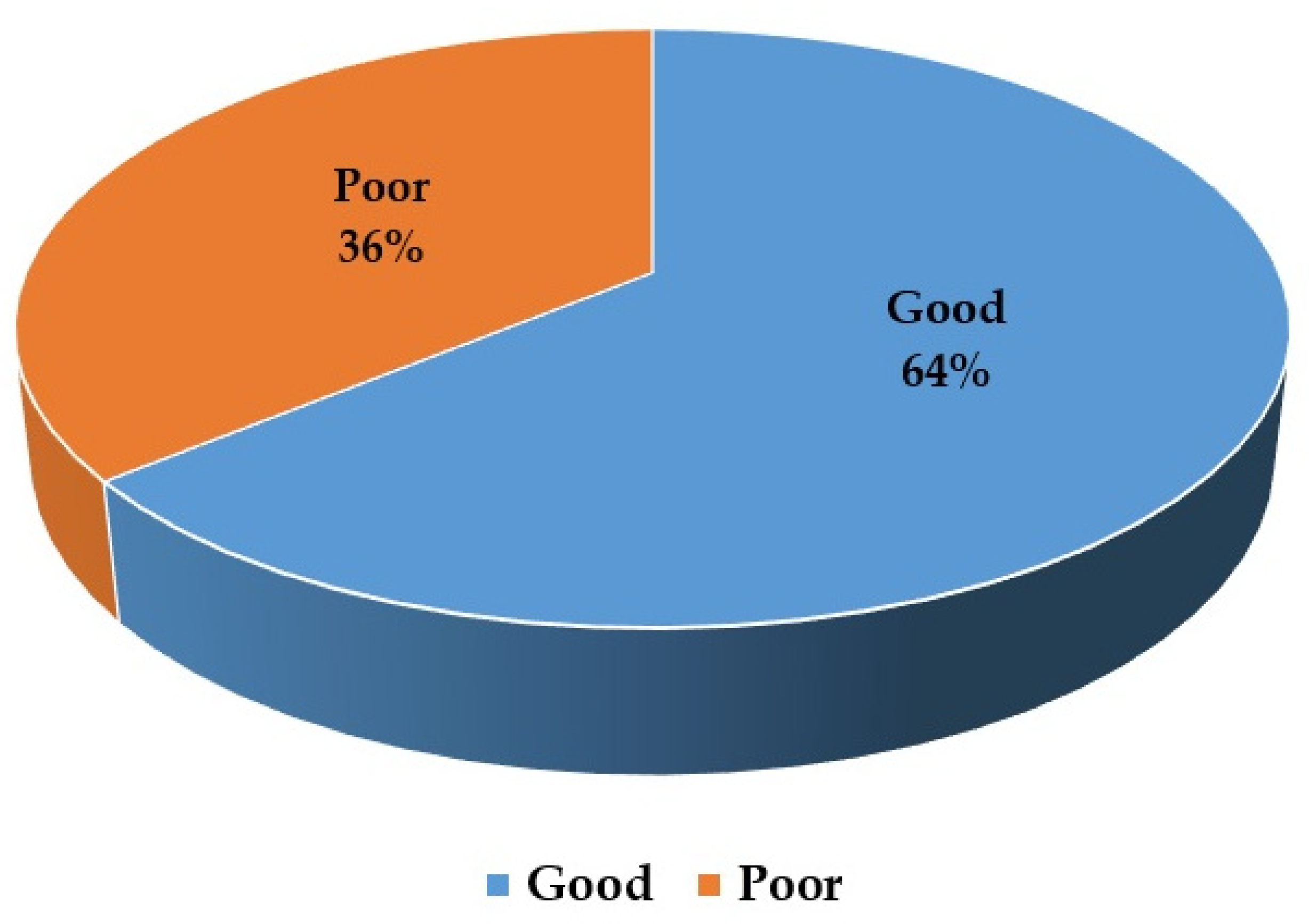
3.3. Knowledge of the Participants about Spread, Symptoms and Prevention of COVID-19
3.4. Attitudes of the Participants Preventive Measures against COVID-19
3.5. Perception of the Participants about the Virus and the Disease
3.6. Relationship between Sociodemographic of the Participants and Mean Knowledge Score about COVID-19
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Spagnuolo, G.; De Vito, D.; Rengo, S.; Tatullo, M. COVID-19 Outbreak: An Overview on Dentistry. Int. J. Environ. Res. Public Health 2020, 17, 2094. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- She, J.; Jiang, J.; Ye, L.; Hu, L.; Bai, C.; Song, Y. 2020 2019 novel coronavirus of pneumonia in Wuhan, China: Emerging attack and management strategies. Clin. Transl. Med. 2019, 9, 19. [Google Scholar]
- WHO. WHO Director-General’s Opening Remarks at the Media Briefing on COVID-19—11 March 2020; WHO: Geneva, Switzerland, 2020. Available online: https://www.who.int/director-general/speeches/detail/who-director-general-s-opening-remarks-at-the-media-briefing-on-covid-19---11-march-2020 (accessed on 20 June 2021).
- Baud, D.; Qi, X.; Nielsen-Saines, K.; Musso, D.; Pomar, L.; Favre, G. Real estimates of mortality following COVID-19 infection. Lancet Infect. Dis. 2020, 20, 773. [Google Scholar] [CrossRef] [Green Version]
- Pal, M.; Berhanu, G.; Desalegn, C.; Kandi, V. Severe Acute Respiratory Syndrome Coronavirus-2 (SARS-CoV-2): An Update. Cureus 2020, 12, e7423. [Google Scholar] [CrossRef] [Green Version]
- CDC. Centers for Disease Control. Atlanta, USA. People Who Are at Increased Risk for Severe Illness. Available online: https://www.cdc.gov/coronavirus/2019-ncov/need-extra-precautions/people-at-increased-risk.html (accessed on 18 June 2021).
- CDC. Coronavirus Disease 2019 (COVID-19). Centers for Disease Control. Atlanta, USA. 2020. Available online: https://www.cdc.gov/coronavirus/2019-ncov/about/%20transmission (accessed on 8 June 2021).
- Jin, Y.H.; Cai, L.; Cheng, Z.S.; Cheng, H.; Deng, T.; Fan, Y.P.; Huang, D.; Huang, L.Q.; Huang, Q.; Han, Y. A rapid advice guideline for the diagnosis and treatment of 2019 novel coronavirus (2019-nCoV) infected pneumonia (standard version). Mil. Med. Res. 2020, 7, 4. [Google Scholar] [CrossRef] [Green Version]
- Kandel, N.; Chungong, S.; Omaar, A.; Xing, J. Health security capacities in the context of COVID-19 outbreak: An analysis of International Health Regulations annual report data from 182 countries. Lancet 2020, 395, 1047–1053. [Google Scholar] [CrossRef]
- Ministry of Health: The Tests Carried out on Those in Contact with the Affected Case in Hadramout are Negative. 2020. Available online: http://sahel.had-health.info/view/4162.aspx (accessed on 6 June 2020).
- Yemen Covid-19 Tracker. 2020. Available online: https://yemen-corona.com/ (accessed on 15 June 2020).
- Yemeni Gravediggers Overwhelmed Amid Spike in Virus Deaths. 2020. Available online: https://apnews.com/4ff7155b074703c629600dc5bfca968f (accessed on 6 June 2020).
- Hundreds Die in Yemen of Suspected Coronavirus Outbreak. 2020. Available online: https://apnews.com/0fa08ac04778a3d8a37579fb97a63572 (accessed on 6 June 2020).
- Yemen ‘Faces Nightmare’ as First Coronavirus Case Confirmed. 2020. Available online: https://www.bbc.com/news/world-middle-east-52249624 (accessed on 18 June 2020).
- Cao, W.; Fang, Z.; Hou, G.; Han, M.; Xu, X.; Dong, J.; Zheng, J. The psychological impact of the COVID-19 epidemic on college students in China. Psychiatry Res. 2020, 287, 112934. [Google Scholar] [CrossRef]
- Ferdous, M.Z.; Islam, M.S.; Sikder, M.T.; Mosaddek, A.S.M.; Zegarra-Valdivia, J.A.; Gozal, D. Knowledge, attitude, and practice regarding COVID-19 outbreak in Bangladesh: An online-based cross-sectional study. PLoS ONE 2020, 15, e0239254. [Google Scholar] [CrossRef]
- Abdelhafiz, A.S.; Mohammed, Z.; Ibrahim, M.E.; Ziady, H.H.; Alorabi, M.; Ayyad, M.; Sultan, E.A. Knowledge, Perceptions, and Attitude of Egyptians Towards the Novel Coronavirus Disease (COVID-19). J. Community Health 2020, 5, 881–890. [Google Scholar] [CrossRef]
- Lemeshow, S.; Hosmer, D.W.; Klar, J.; Lwanga, S.K.; World Health Organization. Adequacy of Sample Size in Health Studies. 1990. Available online: https://apps.who.int/iris/handle/10665/41607 (accessed on 16 December 2021).
- Soltan, E.M.; El-Zoghby, S.M.; Salama, H.M. Knowledge, Risk Perception, and Preventive Behaviors Related to COVID-19 Pandemic Among Undergraduate Medical Students in Egypt. SN Compr. Clin. Med. 2020, 2, 2568–2575. [Google Scholar] [CrossRef]
- Alzoubi, H.; Alnawaiseh, N.; Al-Mnayyis, A.; Abu Lubad, M.; Aqel, A.; Al-Shagahin, H. COVID-19—Knowledge, Attitude and Practice among Medical and Non-Medical University Students in Jordan. J. Pure Appl. Microbiol. 2020, 14, 17–24. [Google Scholar] [CrossRef]
- Yakar, B.; Kaygusuz, T.Ö.; Pirincci, E.; Önalan, E.; Ertekin, Y.H. Knowledge, attitude and anxiety of medical students about the current COVID-19 outbreak in Turkey. Fam. Pract. Palliat. Care 2020, 5, 36–44. [Google Scholar] [CrossRef]
- Modi, P.D.; Nair, G.; Uppe, A.; Modi, J.; Tuppekar, B.; Gharpure, A.S.; Langade, D. COVID-19 awareness among healthcare students and professionals in Mumbai metropolitan region: A questionnaire-based survey. Cureus 2020, 12, e7514. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Abd El Fatah, S.A.M.; Salem, M.R.; Abdel Hakim, A.S.; El Desouky, E.D. Knowl-edge, attitude, and behavior of Egyptian medical students toward the novelcoronavirus disease-19: A cross-sectional study. Open Access Maced. J. Med. Sci. 2020, 8, 443–450. [Google Scholar] [CrossRef]
- Singh, J.P.; Sewda, A.; Gupta, S.D. Assessing the knowledge, attitude andpractices of students regarding the COVID-19 pandemic. J. Health Manag. 2020, 22, 281–290. [Google Scholar] [CrossRef]
- Olum, R.; Kajjimu, J.; Kanyike, A.M.; Chekwech, G.; Wekha, G.; Nassozi, D.R.; Kemigisa, J.; Mulyamboga, P.; Muhoozi, O.K.; Nsenga, L.; et al. Perspective of medical students on the COVID-19 pandemic: Survey of nine medical schools in Uganda. JMIR Public Health Surveill. 2020, 6, e19847. [Google Scholar] [CrossRef]
- Ahmed, N.; Khan, A.; Naveed, H.A.; Moizuddin, S.M.; Khan, J. Concerns of undergraduate medical students towards an outbreak of Covid-19. Int. J. CurrMed. Pharm. Res. 2020, 6, 5055–5062. [Google Scholar]
- World Health Organisation Website. Available online: https://www.who.int/dg/speeches/detail/who-director-general-s-opening-remarks-at-the-media-briefing-on-covid-19 (accessed on 23 March 2020).
- Huang, C.; Wang, Y.; Li, X.; Ren, L.; Zhao, J.; Hu, Y.; Zhang, L.; Fan, G.; Xu, J.; Gu, X.; et al. Clinical features of patients infected with 2019 novel coronavirus in Wuhan. China. Lancet 2020, 395, 497–506. [Google Scholar] [CrossRef] [Green Version]
- Srichan, P.; Apidechkul, T.; Tamornpark, R.; Yeemard, F.; Khunthason, S.; Kitchanapaiboon, S.; Wongnuch, P.; Wongphaet, A.; Upala, P. Knowledge, Attitude and Preparedness to Respond to the 2019 Novel Coronavirus (COVID-19) Among the Bordered Pop-ulation of Northern Thailand in the Early Period of the Outbreak: A Cross-Sectional Study. SSRN Electron. J. 2020. Available online: https://papers.ssrn.com/sol3/papers.cfm?abstract_id=3546046 (accessed on 23 March 2020).
- Zhong, B.-L.; Luo, W.; Li, H.-M.; Zhang, Q.-Q.; Liu, X.-G.; Li, W.-T.; Li, Y. Knowledge, attitudes, and practices towards COVID-19 among Chinese residents during the rapid rise period of the COVID-19 outbreak: A quick online cross-sectional survey. Int. J. Biol. Sci. 2020, 16, 1745–1752. [Google Scholar] [CrossRef] [Green Version]
- Saqlain, M.; Munir, M.M.; Rehman, S.U.; Gulzar, A.; Naz, S.; Ahmed, Z.; Tahir, A.H.; Mashhood, M. Knowledge, attitude, practice and perceived barriers among healthcare professionals regarding COVID-19: A Cross-sectional survey from Pakistan. medRxiv 2020, 105, 419–423. [Google Scholar] [CrossRef] [Green Version]
- Adhikari, S.P.; Meng, S.; Wu, Y.-J.; Mao, Y.-P.; Ye, R.-X.; Wang, Q.-Z.; Sun, C.; Sylvia, S.; Rozelle, S.; Raat, H.; et al. Epidemiology, causes, clinical manifestation and diagnosis, prevention and control of coronavirus disease (COVID-19) during the early outbreak period: A scoping review. Infect. Dis. Poverty 2020, 9, 29. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Recommendation Regarding the Use of Cloth Face Coverings, Especially in Areas of Significant Community-Based Transmission. 2020. Available online: https://www.cdc.gov/coronavirus/2019-ncov/prevent-gettng-sick/cloth-face-cover.html (accessed on 4 April 2020).
- Coronavirus Disease (COVID-19) Advice for the Public: When and How to Use Masks. 2020. Available online: https://www.who.int/emergencies/diseases/novel-coronavirus-2019/advice-for-public/when-and-how-to-use-masks (accessed on 4 April 2020).
- Kabbash, I.A.; Ali, E.A.A.; Elgendy, M.M.; Abdrabo, M.M.; Salem, H.M.; Gouda, M.R.; Elbasiony, Y.S.; Elboshy, N.; Hamed, M. HIV/AIDS-related stigma and discrimination among health care workers at Tanta University Hospitals Egypt. Environ. Sci. Pollut. Res. Int. 2018, 25, 30755–30762. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Participants No. (389) | No. | % |
|---|---|---|
| Sex: | ||
| Male Female | 133 256 | 34.2 65.8 |
| Age group (years): | ||
| ≤18 19–24 25–30 30> | 6 345 37 1 | 1.5 88.7 9.5 0.3 |
| Area of residence: | ||
| Rural area Urban urea | 75 314 | 19.3 80.7 |
| Specialty: | ||
| Medicine Pharmacy Medical laboratory Nursing | 229 59 45 56 | 58.9 15.2 11.6 14.4 |
| Academic level: | 79 | 20.3 |
| First level Second level Third level Fourth level Fifth level Sixth level | 107 80 61 40 22 | 27.5 20.6 15.7 10.3 5.7 |
| Data are presented as frequencies (n) and percentage (%). | ||
| Knowledge Items | Yes | No | Not Sure | |||
|---|---|---|---|---|---|---|
| No. | % | No. | % | No. | % | |
| COVID-19 spreads by: | ||||||
| 382 | 98.2 | 3 | 0.8 | 4 | 1.0 |
| 360 | 92.5 | 3 | 0.8 | 21 | 5.4 |
| 277 | 71.2 | 32 | 8.2 | 80 | 20.6 |
| 74 | 19 | 177 | 45.5 | 138 | 35.5 |
| 59 | 15.2 | 207 | 53.2 | 123 | 31.6 |
| 277 | 71.2 | 68 | 17.5 | 44 | 11.3 |
| Symptoms of the disease: | ||||||
| 386 | 99.2 | 0 | 0 | 3 | 0.8 |
| 381 | 97.9 | 3 | 0.8 | 5 | 1.3 |
| 279 | 71.7 | 34 | 8.7 | 76 | 19.5 |
| 179 | 46.0 | 102 | 26.2 | 108 | 27.8 |
| 136 | 35.0 | 143 | 36.8 | 110 | 28.3 |
| 231 | 59.4 | 71 | 18.3 | 87 | 22.4 |
| 387 | 99.5 | 1.0 | 0.3 | 1.0 | 0.3 |
| Measures to prevent the viral spreading: | ||||||
| 388 | 99.7 | 0 | 0 | 1 | 0.3 |
| 386 | 99.2 | 1 | 0.3 | 2 | 0.5 |
| 384 | 98.7 | 3 | 0.8 | 2 | 0.5 |
| 379 | 97.4 | 3 | 0.8 | 7 | 1.8 |
| 36 | 9.3 | 286 | 73.5 | 67 | 17.2 |
| 35 | 9.0 | 279 | 71.7 | 75 | 19.3 |
| 6 | 1.5 | 331 | 85.1 | 52 | 13.4 |
| Mean knowledge score: 16.17 ± 2.33 | ||||||
| Data are presented as frequencies (n) and percentage (%). | ||||||
| Attitude Items | Strongly Agree | Agree | Not Sure | Don’t Agree | Do Strongly Agree | |||||
|---|---|---|---|---|---|---|---|---|---|---|
| No. | % | No. | % | No. | % | No. | % | No. | % | |
| 48 | 12.3 | 67 | 17.2 | 17 | 4.4 | 119 | 30.6 | 138 | 35.5 |
| 11 | 2.8 | 25 | 6.4 | 12 | 3.1 | 87 | 22.4 | 254 | 65.3 |
| 250 | 64.3 | 26 | 6.7 | 4.1 | 16 | 53 | 13.6 | 44 | 11.3 |
| 110 | 28.3 | 76 | 19.5 | 29 | 7.5 | 113 | 29.0 | 61 | 15.7 |
| 168 | 43.2 | 80 | 20.6 | 54 | 13.9 | 46 | 11.8 | 41 | 10.5 |
| 179 | 46.0 | 76 | 19.5 | 40 | 10.3 | 40 | 10.3 | 54 | 13.9 |
| 271 | 69.7 | 46 | 11.8 | 24 | 6.2 | 4 | 1.0 | 44 | 11.3 |
| 163 | 41.9 | 68 | 17.5 | 41 | 10.5 | 47 | 12.1 | 70 | 18.0 |
| 224 | 57.6 | 76 | 19.5 | 31 | 8.0 | 19 | 4.9 | 39 | 10.0 |
| 203 | 52.2 | 78 | 20.1 | 40 | 10.3 | 23 | 5.9 | 45 | 11.6 |
| 198 | 50.9 | 63 | 16.2 | 31 | 8.0 | 57 | 14.7 | 40 | 10.3 |
| 132 | 33.9 | 88 | 22.6 | 43 | 11.1 | 85 | 21.9 | 41 | 10.5 |
| 127 | 32.6 | 70 | 18.0 | 45 | 11.6 | 79 | 20.3 | 68 | 17.5 |
| 204 | 52.4 | 89 | 22.9 | 40 | 10.3 | 22 | 5.7 | 34 | 8.7 |
| 261 | 67.1 | 55 | 14.1 | 22 | 5.7 | 7 | 1.8 | 44 | 11.3 |
| Data are presented as frequencies (n) and percentage (%). | ||||||||||
| Perceptions Items | Yes | No | Not Sure | |||
|---|---|---|---|---|---|---|
| No. | % | No. | % | No. | % | |
| 232 | 59.6 | 136 | 35 | 21 | 5.4 |
| 283 | 72.8 | 91 | 23.4 | 15 | 3.9 |
| 58 | 14.9 | 315 | 81 | 16 | 4.1 |
| 251 | 64.5 | 112 | 28.8 | 26 | 6.7 |
| 133 | 34.2 | 96 | 24.6 | 160 | 41.1 |
| Data are presented as frequencies (n) and percentage (%) | ||||||
| Sociodemographic Data | Mean Knowledge Score | p-Value | |
|---|---|---|---|
| Min-Max | Mean ± SD | ||
| Sex Male Female | 5–22 10–22 | 16.52 ± 2.50 15.98 ± 2.21 | 0.029 |
| Residence area Urban Rural | 5–20 10–22 | 16.27 ± 2.24 15.75 ± 2.64 | 0.080 |
| Specialty Medicine Pharmacy Medical laboratory Nursing | 5–22 11–19 10–19 10–21 | 16.58 ± 2.34 16.00 ± 2.10 14.89 ± 2.25 *,† 15.67 ± 2.08 * | <0.001 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Al-Ghazali, R.H.; Barhoom, E.S.; Dahdah, K.A.; Basalem, K.S.; Mugibel, T.A.; Sumaily, K.M.; Sabi, E.M.; Mujamammi, A.H.; Ben Salman, S.M.; Bin Dahman, L.S. Knowledge, Attitudes, and Perception towards COVID-19 among Medical Students in Yemen: A Cross-Sectional Survey. Infect. Dis. Rep. 2022, 14, 841-854. https://0-doi-org.brum.beds.ac.uk/10.3390/idr14060086
Al-Ghazali RH, Barhoom ES, Dahdah KA, Basalem KS, Mugibel TA, Sumaily KM, Sabi EM, Mujamammi AH, Ben Salman SM, Bin Dahman LS. Knowledge, Attitudes, and Perception towards COVID-19 among Medical Students in Yemen: A Cross-Sectional Survey. Infectious Disease Reports. 2022; 14(6):841-854. https://0-doi-org.brum.beds.ac.uk/10.3390/idr14060086
Chicago/Turabian StyleAl-Ghazali, Ruqaiah H., Eman S. Barhoom, Khawla A. Dahdah, Khulood S. Basalem, Tayba A. Mugibel, Khalid M. Sumaily, Essa M. Sabi, Ahmed H. Mujamammi, Saleh M. Ben Salman, and Lotfi S. Bin Dahman. 2022. "Knowledge, Attitudes, and Perception towards COVID-19 among Medical Students in Yemen: A Cross-Sectional Survey" Infectious Disease Reports 14, no. 6: 841-854. https://0-doi-org.brum.beds.ac.uk/10.3390/idr14060086