Hypertension in Obese Type 2 Diabetes Patients is Associated with Increases in Insulin Resistance and IL-6 Cytokine Levels: Potential Targets for an Efficient Preventive Intervention

Abstract
:1. Introduction
2. Methods
2.1. Subjects
2.2. Study Design
2.3. Evaluation of Insulin Sensitivity
2.4. Laboratory Measurements
2.5. Statistical Analysis
3. Results and Discussion
3.1. Results
3.1.1. Patients Characteristics

{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Group | ||||
|---|---|---|---|---|
| A T2D + HTA+ | B T2D + HTA− | C Control | p value (Group A vs. B) | |
| n (M/F) | 30 (16/14) | 30 (15/15) | 15 (7/8) | NS |
| Age (years) | 56.47 ± 3.91 | 57.67 ± 3.96 | 44.06 ± 4.51 | NS |
| Duration of diabetes (years) | 4.59 ± 1.53 | 4.44 ± 1.26 | - | NS |
| BMI (kg/m2) * | 31.20 ± 2.53 | 30.92 ± 2.34 | 22.77 ± 2.9 | NS |
| SBP (mmHg) * | 140.17 ± 12.25 | 141.66 ± 13.13 | 122.03 ± 6.97 | NS |
| DBP (mmHg) * | 86.67 ± 9.12 | 85.56 ± 8.81 | 78.67 ± 4.81 | NS |
| HbA1c (%) * | 6.51 ± 0.66 | 6.53 ± 0.60 | 4.71 ± 0.32 | NS |
| FPG (mmol/L) * | 7.36 ± 1.40 | 7.46 ± 1.51 | 4.06 ± 0.71 | NS |
| Total Ch (mmol/L) * | 6.16 ± 0.93 | 6.14 ± 0.82 | 5.6 ± 0.98 | NS |
| Triglycerides (mmol/L) * | 2.66 ± 1.15 | 2.37 ± 0.80 | 1.29 ± 0.59 | NS |
| HDL-Ch (mmol/L) * | 0.98 ± 0.11 | 1.12 ± 0.18 | 1.58 ± 0.47 | p < 0.05 |
| LDL-Ch (mmol/L) * | 3.85 ± 0.78 | 3.99 ± 0.75 | 3.53 ± 0.64 | NS |
| Smoking (n, %) | 10 (33.3) | 11 (36.3) | 5 (33.3) | NS |

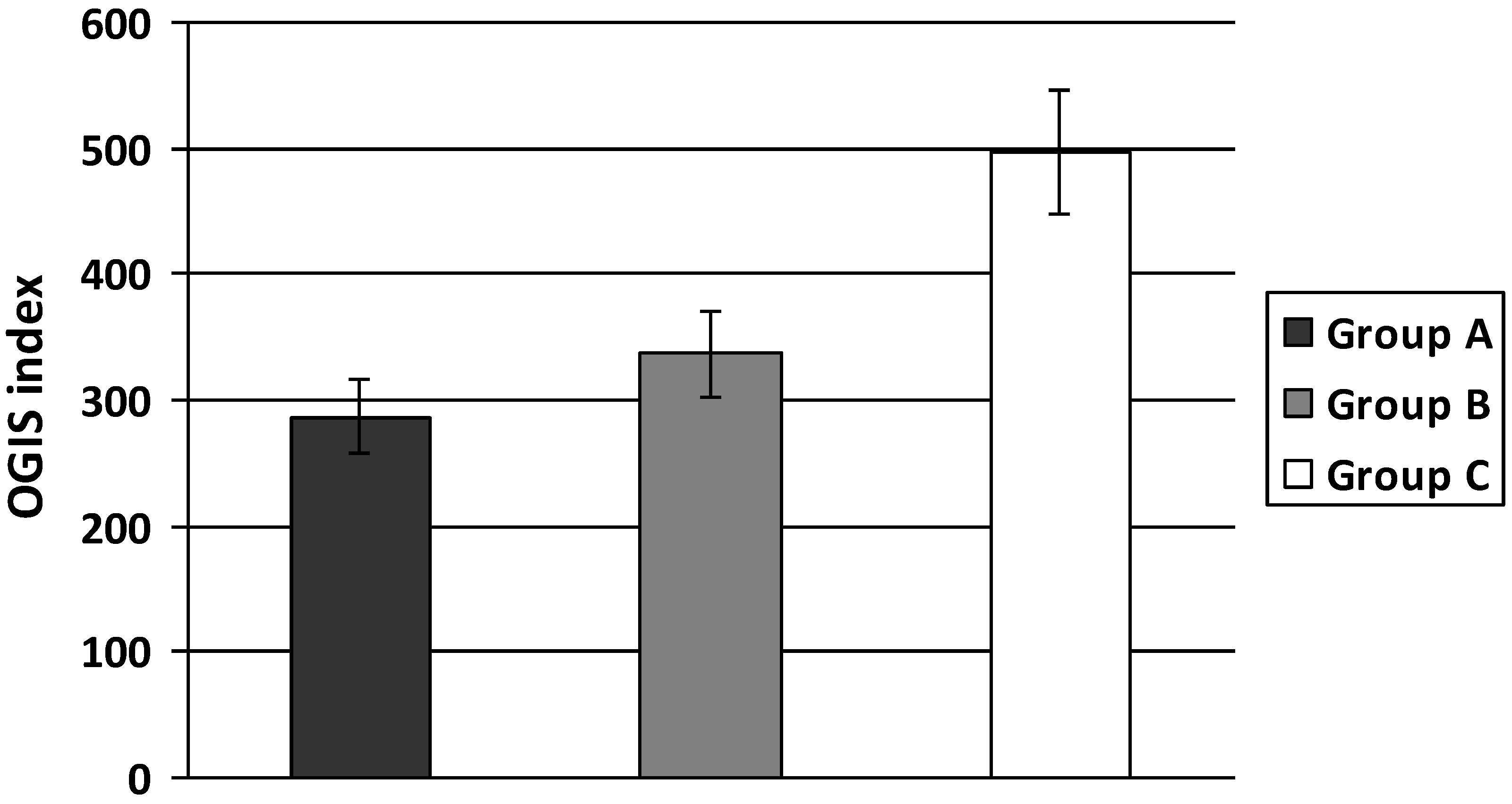
3.1.2. Insulin Sensitivity

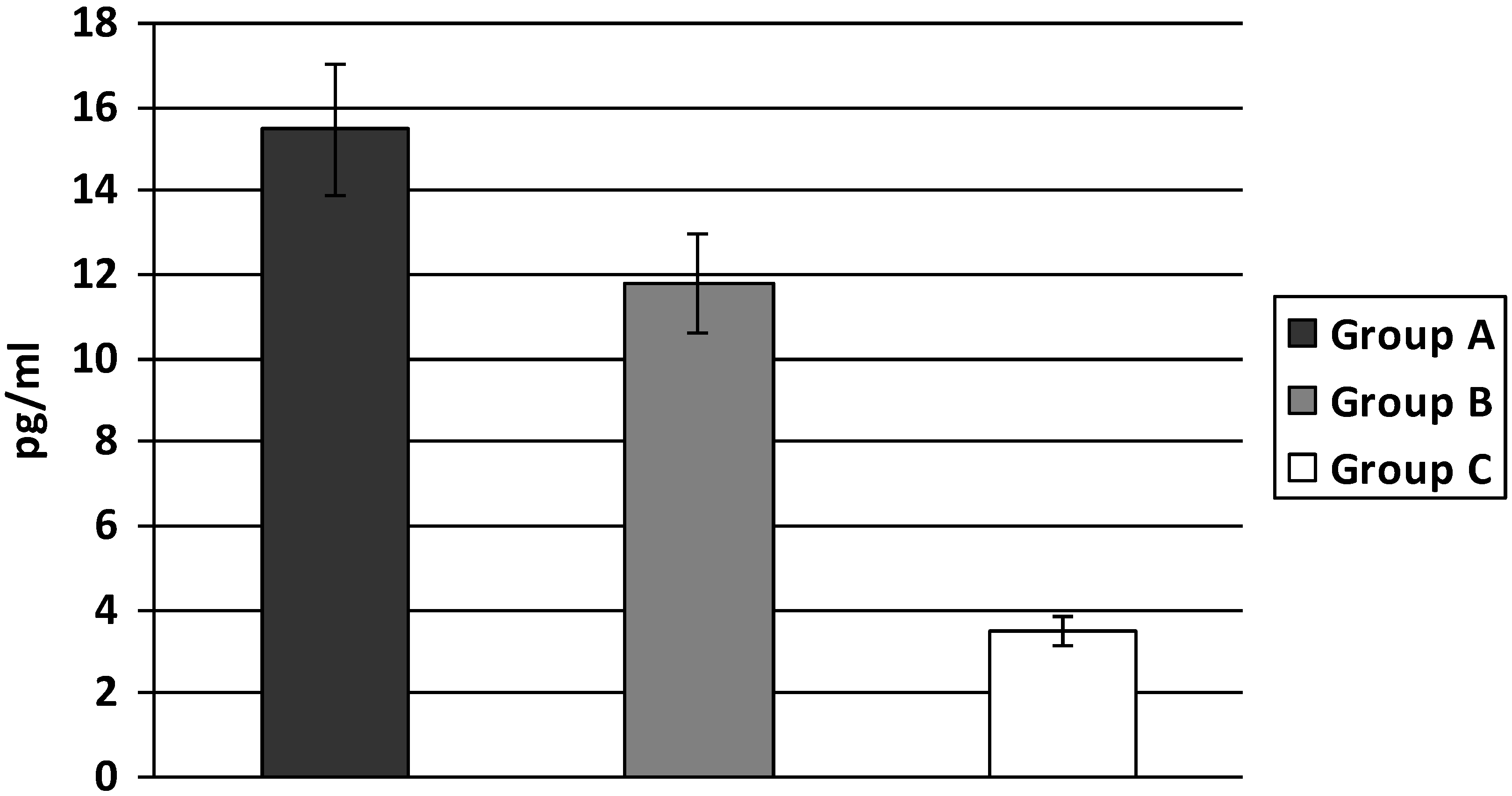
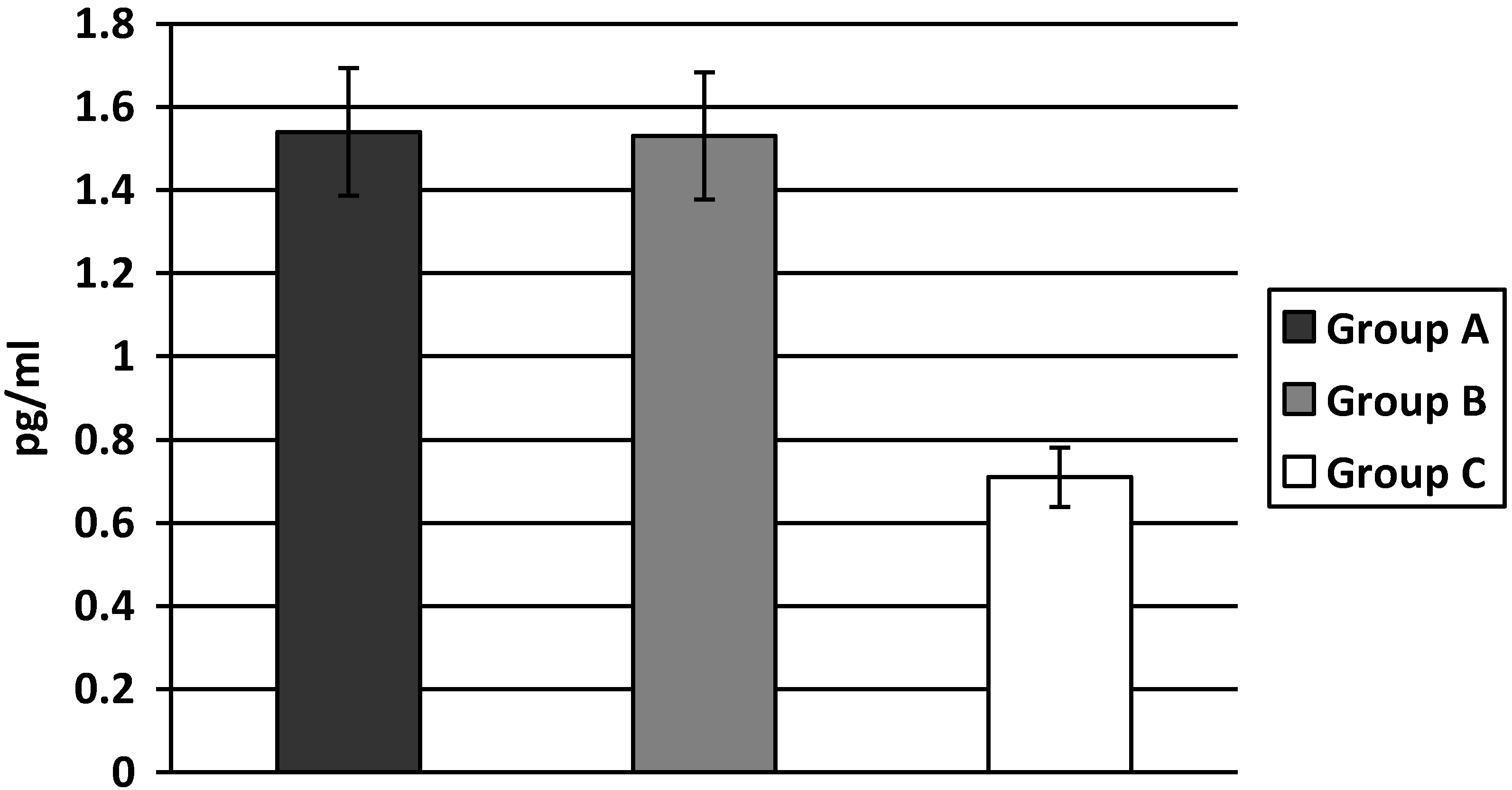
3.1.3. Pro-inflammatory Cytokines


3.2. Discussion
4. Conclusions
Abbreviations
| OGIS | Oral Glucose Insulin Sensitivity index |
| IL-6 | Interleukin-6 |
| TNF-α | Tumor Necrosis Factor-α |
| BMI | Body Mass Index |
Acknowledgments
Author Contributions
Conflicts of Interest
References
- Savoia, C.; Schiffrin, E. Vascular inflammation in hypertension and diabetes: Molecular mechanisms and therapeutic interventions. Clin. Sci. 2007, 112, 375–384. [Google Scholar] [CrossRef]
- Pearson, T.A.; Mensah, G.A.; Alexander, R.W.; Anderson, J.L.; Cannon, R.O.; Criqui, M.; Fadl, Y.Y.; Fortmann, S.P.; Hong, Y.; Myers, G.L.; et al. Markers of inflammation and cardiovascular disease application to clinical and public health practice: A statement for healthcare professionals from the centers for disease control and prevention and the American Heart Association. Circulation 2003, 107, 499–511. [Google Scholar] [CrossRef]
- Hotamisligil, G.S. The role of TNF alpha and TNF receptors in obesity and insulin resistance. J. Intern. Med. 1999, 245, 621–625. [Google Scholar] [CrossRef]
- Febbraio, M.A.; Pedersen, B.K. Muscle derived interleukin-6: Mechanisms for activation and possible biological roles. FASEB J. 2002, 16, 1335–1347. [Google Scholar] [CrossRef]
- Shoelson, S.E.; Lee, J.; Goldfine, A.B. Inflammation and insulin resistance. J. Clin. Invest. 2006, 116, 1793–1801. [Google Scholar] [CrossRef]
- Tataranni, P.A.; Ortega, E. A burning question: Does an adipokine-induced activation of the immune system mediate the effect of overnutrition on type 2 diabetes? Diabetes 2005, 54, 917–927. [Google Scholar] [CrossRef]
- Carley, A.L.; Bruce, C.R.; Sacchetti, M.; Anderson, M.J.; Olsen, D.B.; Saltin, B.; Hawley, J.A.; Febbraio, M.A. Interleukin-6 and tumor necrosis factor-alpha are not increased in patients with type 2 diabetes: Evidence that plasma interleukin-6 is related to fat mass not insulin responsiveness. Diabetologia 2004, 47, 1029–1037. [Google Scholar]
- Cartier, A.; Lemieux, I.; Almeras, N.; Tremblay, A.; Bergeron, J.; Despres, J.P. Visceral obesity and plasma glucoe-insulin homeostasis: Contributions of interleukin-6 and tumor necrosis factor-alpha in men. J. Clin. Endocrinol. Metab. 2008, 93, 1931–1938. [Google Scholar] [CrossRef]
- McLaughlin, T.; Abbasi, F.; Lamendola, C.; Liang, L.; Reaven, G.; Schaaf, P.; Reaven, P. Differentiation between obesity and insulin resistance in the association with C-reactive protein. Circulation 2002, 106, 2908–2912. [Google Scholar] [CrossRef]
- Preik, M.; Kelm, M.; Rosen, P.; Tschope, D.; Strauer, B. Additive effect of coexistent type 2 diabetes and arterial hypertension on endothelial dysfunction in resistance arteries of human forarm vasculature. Angiology 2000, 51, 545–554. [Google Scholar] [CrossRef]
- Natali, A.; Toschi, E.; Baldeweg, S.; Ciociaro, D.; Favilla, S.; Sacca, L.; Ferranninni, E. Clustering of insulin resistance with vascular dysfunction and low-grade inflammation in type 2 diabetes. Diabetes 2006, 55, 1133–1140. [Google Scholar] [CrossRef]
- Al-Shukaili, A.; AL-Ghafri, S.; Al-Marhoobi, S.; Al-Abri, S.; Al-Lawati, J.; Al-Maskari, M. Analysis of inflammatory mediators in type 2 diabetes patients. Int. J. Endocrinol. 2013, 2013. [Google Scholar] [CrossRef]
- Van Bussel, B.C.; Schouten, F.; Henry, R.M.; Schalkwijk, C.G.; de Boer, M.R.; Ferreira, I.; Smulders, Y.M.; Twisk, J.W.; Stehouwer, C.D. Endothelial dysfunction and low-grade inflammation are associated with greater arterial stiffness over a 6-year period. Hypertension 2011, 58, 588–595. [Google Scholar] [CrossRef]
- Garcia, C.; Feve, B.; Ferre, P.; Halimi, S.; Baizri, H.; Bordier, L.; Guiu, G.; Dupuy, O.; Bauduceau, B.; Mayaudon, H. Diabetes and inflammation: Fundamental aspects and clinical implications. Diabetes Metab. 2010, 36, 327–338. [Google Scholar] [CrossRef]
- Goldfine, A.B.; Fonseca, V.; Shoelson, S.E. Therapeutic approaches to target inflammation in type 2 diabetes. Clinical Chemistry 2011, 57, 162–167. [Google Scholar] [CrossRef]
- Definition and Diagnosis of Diabetes Mellitus and Intermediate Hyperglycemia: Report of A WHO/IDF Consultation; World Health Organization: Geneva, Switzerland, 2006.
- Chobanian, A.V.; Bakris, G.R.; Black, H.F.; Cushman, W.C.; Green, L.A.; Izzo, J.L.; Jones, D.W.; Materson, B.J.; Oparil, S.; Wright, J.T.; et al. National Heart, Lung and Blood Institute Joint National Committee on prevention, detection, evaluation, and treatment of high blood pressure; National High Blood Pressure Education Program Coordinating Committee: Seventh report of joint national committee on prevention, detection, evaluation and treatment of high blood pressure; the JNC 7 report. J. Amer. Med. Assoc. 2003, 289, 2560–2572. [Google Scholar] [CrossRef]
- Mari, A.; Pacini, G.; Murphy, E.; Ludvik, B.; Nolan, J.J. A model-based method for assessing insulin sensitivity from the oral glucose tolerance test. Diabetes Care 2001, 24, 539–548. [Google Scholar] [CrossRef]
- Messerli, F.H.; Williams, B.; Ritz, E. Essential hypertension. Lancet 2007, 370, 591–603. [Google Scholar] [CrossRef]
- Ferrannini, E.; Buzzigoli, G.; Bonadona, R. Insulin resistance in essential hypertension. N. Engl. J. Med. 1987, 317, 350–357. [Google Scholar] [CrossRef]
- Pollare, T; Lithell, H.; Berne, C. Insulin resistance is a characteristic feature of primary hypertension independent of obesity. Metabolism 1990, 39, 167–174. [Google Scholar] [CrossRef]
- Reaven, GM; Lithell, H; Lansberg, L. Hypertension and associated metabolic abnormalities—The role of insulin resistance and the sympathoadrenal system. N. Engl. J. Med. 1996, 334, 374–381. [Google Scholar] [CrossRef]
- Sironi, A.M.; Gastaldelli, A.; Mari, A.; Ciociaro, D.; Postano, V.; Buzzigoli, E.; Ghione, S.; Turchi, S.; Lombardi, M.; Ferrannini, E. Visceral fat in hypertension influence on insulin resistance and β-cell function. Hypertension 2004, 44, 127–133. [Google Scholar] [CrossRef]
- Sironi, A.M.; Pingitore, A.; Ghione, S.; De Marchi, D.; Scattini, B.; Positano, V.; Muscelli, E.; Ciociaro, D.; Lombardi, M.; Ferrannini, E.; et al. Early hypertension is associated with reduced regional cardiac function, insulin resistance, epicardial, and visceral fat. Hypertension 2008, 51, 282–288. [Google Scholar] [CrossRef]
- Mari, A.; Pacini, G.; Brazzale, A.R.; Ahren, B. Comparative evaluation of simple insulin sensitivity methods based on the oral glucose tolerance test. Diabetologia 2005, 48, 748–751. [Google Scholar] [CrossRef]
- Tran, T.T.; Gupta, N.; Goh, T.; Naigamwalla, D.; Chia, M.C.; Koohestani, N.; Mehrotra, S.; McKeown-Eyssen, G.; Giacca, A.; Bruce, W.R. Direct measure of insulin sensitivity with the hyperinsulinemic-euglycemic clamp and surrogate measures of insulin sensitivity with the oral glucose tolerance test correlations with aberrant crypt foci promotion in rats. Cancer Epidemiol. Biomark. Prev. 2003, 12, 47–56. [Google Scholar]
- Mari, A.; Tura, A.; Pacini, G.; Kautzky‐Willer, A.; Ferrannini, E. Relationships between insulin secretion after intravenous and oral glucose administration in subjects with glucose tolerance ranging from normal to overt diabetes. Diabet. Med. 2008, 25, 671–677. [Google Scholar] [CrossRef]
- Bastard, J.P.; Vandernotte, J.M.; Faraj, M.; Karelis, A.D.; Messier, L.; Malita, F.M.; Garrel, D.; Prud’homme, D.; Rabasa-Lhoretet, R. Relationship between the hyperinsulinemic-euglycaemic clamp and a new simple index assessing insulin sensitivity in overweight and obese postmenopausal women. Diabetes Metab. 2007, 33, 261–268. [Google Scholar] [CrossRef]
- Muniyappa, R.; Lee, S.; Chen, H.; Quon, M.J. Current approaches for assessing insulin sensitivity and resistance in vivo: Advantages, limitations, and appropriate usage. Am. J. Physiol. Endocrinol. Metab. 2008, 294, E15–E26. [Google Scholar] [CrossRef]
- Pickup, J.C.; Crook, M.A. Is type II diabetes mellitus a disease of the innate immune system? Diabetologia 1998, 41, 1241–1248. [Google Scholar] [CrossRef]
- Weisberg, S.P.; McCann, M.; Desai, M.; Rosenbaum, R.; Leibel, L.; Ferrante, A.W. Obesity is associated with macrophage accumulation in adipose tissue. J. Clin. Investig. 2003, 112, 1796–1808. [Google Scholar] [CrossRef]
- Kern, P.A.; Ranganathan, S.; Li, C.; Wood, L.; Ranganathan, G. Adipose tissue tumor necrosis factor and interleukin-6 expression in human obesity and insulin resistance. Am. J. Physiol. Endocrinol. Metab. 2001, 280, E745–E751. [Google Scholar]
- Stephens, J.W.; Hurel, S.J.; Cooper, J.A.; Acharya, J.; Miller, G.J.; Humphries, S.E. A common functional variant in the interleukin-6 gene is associated with increased body mass index in subjects with type 2 diabetes mellitus. Mol. Genet. Metab. 2004, 82, 180–186. [Google Scholar] [CrossRef]
- Olson, C.N.; Callas, W.P.; Hanley, A.J.; Festa, A.; Haffner, S.M.; Wagenknecht, L.E.; Tracy, R.P. Circulating levels of TNF are associated with impaired glucose tolerance, increased insulin reistance, and ethinicity: The insulin resistance atherosclerosis study. J. Clin. Endocrinol. Metab. 2012, 97, 1032–1040. [Google Scholar] [CrossRef]
- Zinman, B.; Hanley, A.J.; Harris, S.B.; Kwan, J.; Fantus, I.G. Circulating tumor necrosis factor-α concentrations in a native Canadian population with high rates of type 2 diabetes mellitus. J. Clin. Endocrinol. Metab. 1999, 84, 272–278. [Google Scholar]
- Miyazaki, Y.; Pipek, R.; Mandarino, L.J.; DeFronzo, R.A. Tumor necrosis factor α and insulin resistance in obese type 2 diabetic patients. Int. J. Obes. 2003, 27, 88–94. [Google Scholar] [CrossRef]
- Popko, E.; Gorska, A.; Stelmaszczyk-Emmel, A.; Plywaczewski, R.; Stoklosa, A.; Gorecka, D.; Pyrzak, B.; Demkow, U. Proinflammatory cytokines IL-6 and TNF-α and the development of inflammation in obese subjects. Eur. J. Med. Res. 2010, 15, 120–122. [Google Scholar]
- Hu, F.B.; Meigs, J.B.; Li, T.Y.; Manson, J.E. Inflammatory markers and risk of developing type 2 diabetes in women. Diabetes 2004, 53, 693–700. [Google Scholar] [CrossRef]
- Schmidt, M.I.; Duncan, B.B.; Sharrett, A.R. Markers of inflammation and prediction of diabetes mellitus in adults (atherosclerosis risk in communities study): A cohort study. The Lancet 1999, 353, 1649–1652. [Google Scholar] [CrossRef]
- Boos, C.J.; Lip, G.Y.H. Is hypertension an inflammatory process? Curr. Pharm. Des. 2006, 12, 1623–1635. [Google Scholar] [CrossRef]
- Pérez Pérez, A.; Ybarra Muñoz, J.; Blay Cortés, V; De Pablos Velasco, P. Obesity and cardiovascular disease. Public Health Nutr. 2007, 10, 1156–1163. [Google Scholar]
- De Jager, J.; Dekker, J.M.; Kooy, A.; Kostense, P.J.; Nijpels, G.; Heine, R.J.; Bouter, L.M.; Stehouwer, C.D.A. Endothelial dysfunction and low-grade inflammation explain much of the excess cardiovascular mortality in individuals with type 2 diabetes The Hoorn Study. Arterioscler. Thromb. Vasc. Boil. 2006, 26, 1086–1093. [Google Scholar] [CrossRef]
- Ganne, S.; Arora, S.K.; Dotsenko, O.; McFarlane, S.I.; Whaley-Connell, A. Hypertension in people with diabetes and the metabolic syndrome: Pathophysiologic insights and therapeutic update. Curr. Diabetes Rep. 2007, 7, 208–217. [Google Scholar]
- Pirro, M.; Schillaci, G.; Savarese, G.; Gemelli, F.; Mannarino, M.R.; Siepi, D.; Bagaglia, F.; Mannarino, E. Attenuation of inflammation with short-term dietary intervention is associated with a reduction of arterial stiffness in subjects with hypercholesterolaemia. Eur. J. Cardiovasc. Prev. Rehabil. 2004, 11, 497–502. [Google Scholar]
- Egan, B.M. Insulin resistance and sympathetic nervous system. Curr. Hypertens. Rep. 2003, 5, 247–254. [Google Scholar] [CrossRef]
- Frontoni, S.; Bracaglia, D.; Gigli, F. Relationship between autonomic dysfunction, insulin resistance and hypertension, in diabetes. Nutr. Metab. Cardiovasc. Dis. 2005, 15, 441–449. [Google Scholar] [CrossRef]
- Olson, T.P.; Dengel, D.R.; Leon, A.S.; Schmitz, K.H. Changes in inflammatory biomarkers following one-year of moderate resistance training in overweight women. Int. J. Obes. 2007, 31, 996–1003. [Google Scholar] [CrossRef]
- Badawi, A.; Klip, A.; Haddad, P.; Cole, D.E.C.; Bailo, B.G.; El-Sohemy, A.; Karmali, M. Type 2 diabetes mellitus and inflammation: Prospects for biomarkers of risk and nutritional intervention. Diabetes Metab. Syndr. Obes. 2010, 26, 173–186. [Google Scholar]
- Christiansen, T.; Paulsen, S.K.; Bruun, J.M.; Pedersen, S.B.; Richelsen, B. Exercise training versus diet-induced weight-loss on metabolic risk factors and inflammatory markers in obese subjects: A 12-week randomized intervention study. Am. J. Physiol. Endocrinol. Metab. 2010, 298, E824–E831. [Google Scholar] [CrossRef]
- Rosenzweig, J.L.; Ferrannini, E.; Grundy, S.M.; Haffner, S.M.; Heine, R.J.; Horton, E.S.; Kawamori, R. Primary prevention of cardiovascular disease and type 2 diabetes in patients at metabolic risk: an endocrine society clinical practice guideline. J. Clin. Endocrinol. Metab. 2008, 93, 3671–3689. [Google Scholar] [CrossRef]
- Lalic, N.M.; Zamaklar, M.; Pudar, G. Early Detection and Prevention of Type 2 Diabetes: National Program Serbia. In Diabetes Prevention in Practice; ISBN 978-3-00-030765-2; Schwarz, P., Reddy, P., Greaves, C., Dunbar, J., Schwarz, J., Eds.; TUMAINI Institute for Prevention Management: Dresden, Germany, 2010; pp. 117–124. [Google Scholar]
© 2014 by the authors; licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution license (http://creativecommons.org/licenses/by/3.0/).
Share and Cite
Lukic, L.; Lalic, N.M.; Rajkovic, N.; Jotic, A.; Lalic, K.; Milicic, T.; Seferovic, J.P.; Macesic, M.; Gajovic, J.S. Hypertension in Obese Type 2 Diabetes Patients is Associated with Increases in Insulin Resistance and IL-6 Cytokine Levels: Potential Targets for an Efficient Preventive Intervention. Int. J. Environ. Res. Public Health 2014, 11, 3586-3598. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph110403586
Lukic L, Lalic NM, Rajkovic N, Jotic A, Lalic K, Milicic T, Seferovic JP, Macesic M, Gajovic JS. Hypertension in Obese Type 2 Diabetes Patients is Associated with Increases in Insulin Resistance and IL-6 Cytokine Levels: Potential Targets for an Efficient Preventive Intervention. International Journal of Environmental Research and Public Health. 2014; 11(4):3586-3598. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph110403586
Chicago/Turabian StyleLukic, Ljiljana, Nebojsa M. Lalic, Natasa Rajkovic, Aleksandra Jotic, Katarina Lalic, Tanja Milicic, Jelena P. Seferovic, Marija Macesic, and Jelena Stanarcic Gajovic. 2014. "Hypertension in Obese Type 2 Diabetes Patients is Associated with Increases in Insulin Resistance and IL-6 Cytokine Levels: Potential Targets for an Efficient Preventive Intervention" International Journal of Environmental Research and Public Health 11, no. 4: 3586-3598. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph110403586