The Global Contribution of Outdoor Air Pollution to the Incidence, Prevalence, Mortality and Hospital Admission for Chronic Obstructive Pulmonary Disease: A Systematic Review and Meta-Analysis

Abstract
:1. Introduction
2. Experimental Section
2.1. Data Sources
2.2. Search Terms and Strategy to Select Articles
- (1)
- Ambient air pollution
- (2)
- Urban air pollution
- (3)
- Outdoor air pollution
- (4)
- COPD
- (5)
- Chronic obstructive pulmonary disease
- (6)
- Chronic bronchitis
- (7)
- Emphysema
2.3. Study Selection
2.4. Data Extraction and Quality Assessment
2.5. Data Synthesis
3. Results
3.1. Outdoor Air Pollution to COPD Incidence
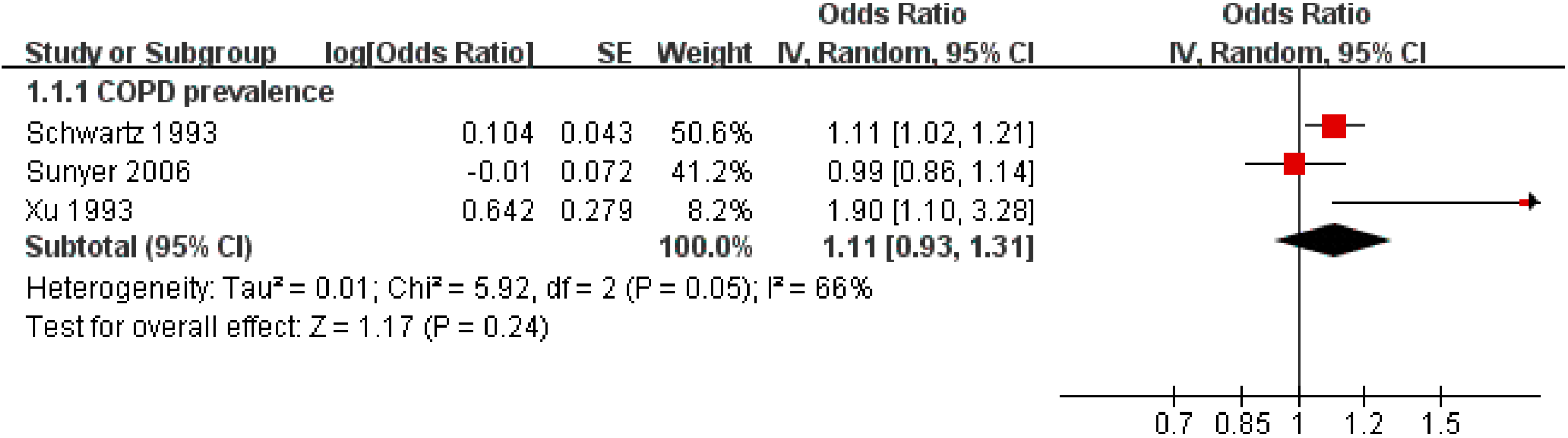
3.2. Outdoor Air Pollution to COPD Prevalence

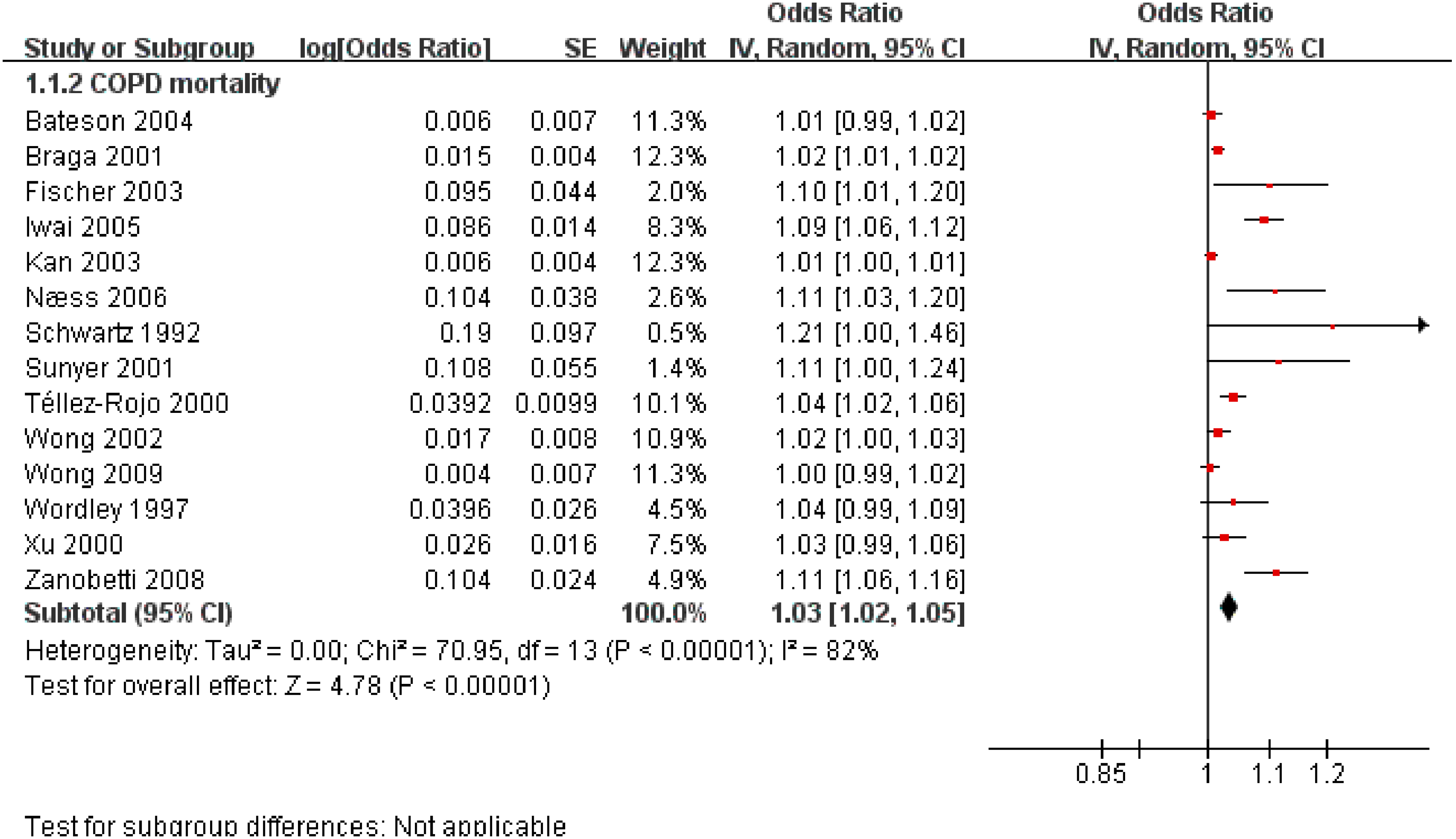
3.3. Outdoor Air Pollution to COPD Mortality


{kind=link}
{kind=link}
{kind=link}
| Category | Study Characteristics (Number of Studies) | Summary Estimate | Summary Estimate | I2 |
|---|---|---|---|---|
| Study design | Cohort (2) | 1.11 | 1.07~1.15 | 0%# |
| Case crossover (3) | 1.01 | 1.00~1.01 | 42%# | |
| Ecological study (8) | 1.02 | 1.01~1.03 | 57% | |
| Cross sectional (1) | 1.09 | 1.06~1.12 | NA | |
| Research field | EU (4) | 1.07 | 1.04~1.11 | 0%# |
| US (4) | 1.03 | 1.00~1.06 | 84% | |
| China (4) | 1.01 | 1.00~1.01 | 3%# | |
| others (2) | 1.06 | 1.02~1.11 | 87% | |
| PM size | PM10 (11) | 1.02 | 1.01~1.04 | 76% |
| TSP (3) | 1.07 | 1.01~1.13 | 79% | |
| PM increment | PM10 10 ug/m3 increment (8) | 1.02 | 1.01~1.03 | 76% |
| Others (6) | 1.08 | 1.04~1.12 | 58% | |
| The effect of 10 ug/m3 PM10 increment in different areas | China (3) | 1.01 | 1.00~1.01 | 0%# |
| US (3) | 1.03 | 1.00~1.06 | 87% | |
| EU (1) | 1.04 | 0.99~1.06 | NA | |
| Others (1) | 1.04 | 1.02~1.06 | NA | |
| Effect duration | Chronic effect (3) | 1.10 | 1.07~1.12 | 0%# |
| Acute effect (11) | 1.02 | 1.01~1.03 | 59% | |
| Acute effects in different areas | China (4) | 1.01 | 1.00~1.01 | 3%# |
| EU (3) | 1.06 | 1.02~1.11 | 0%# | |
| US (3) | 1.01 | 1.01~1.02 | 56%# |
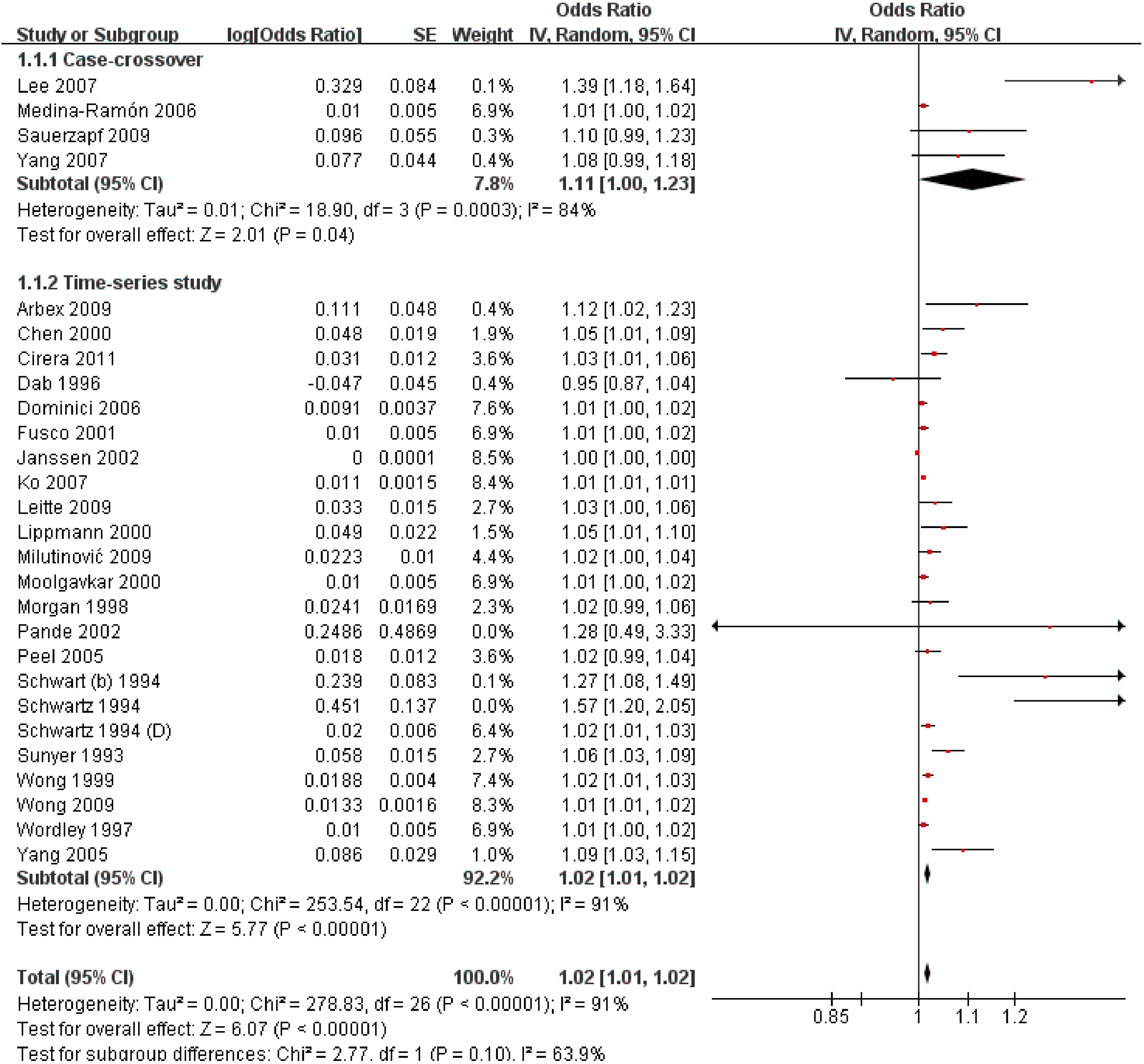
3.4. Outdoor Air Pollution and Hospital Admission for COPD

3.5. Publication Bias
| Category | Study Characteristics (Number of Studies) | Summary Estimate | Summary Estimate | I2 |
|---|---|---|---|---|
| Study Design | Case-crossover (4) | 1.11 | 1.00 ~ 1.23 | 84% |
| Ecological study (23) | 1.02 | 1.01 ~ 1.02 | 64% | |
| Research Field | US (10) | 1.02 | 1.01 ~ 1.03 | 71% |
| EU (8) | 1.02 | 1.01 ~ 1.04 | 61% | |
| China (5) | 1.01 | 1.01 ~ 1.02 | 80% | |
| Others (4) | 1.05 | 1.02 ~ 1.08 | 46% # | |
| PM size | PM10 (19) | 1.02 | 1.01 ~ 1.02 | 72% |
| Others (8) | 1.02 | 1.01 ~ 1.03 | 60% | |
| PM increment | PM10 10 ug/m3 increment (9) | 1.01 | 1.01 ~ 1.01 | 16% # |
| Others (18) | 1.03 | 1.02 ~ 1.05 | 75% | |
| The effect of 10 ug/m3 PM10 increment in different areas | china (3) | 1.01 | 1.01 ~ 1.01 | 46% # |
| US (4) | 1.02 | 1.01 ~ 1.03 | 0% # | |
| EU (2) | 1.01 | 1.00 ~ 1.02 | 59% # |
4. Discussion
5. Conclusions
Supplementary Files
Supplementary File 1Strengths
Limitations
Acknowledgements
Author Contributions
Conflicts of interest
References
- World Health Organization. The Global Burden Of Disease: 2004 Update; World Health Organization: Geneva, Switzerland, 2008. [Google Scholar]
- Lim, S.S.; Vos, T.; Flaxman, A.D.; Danaei, G.; Shibuya, K.; Adair-Rohani, H.; Amann, M.; Anderson, H.R.; Andrews, K.G.; Aryee, M.; et al. A comparative risk assessment of burden of disease and injury attributable to 67 risk factors and risk factor clusters in 21 regions, 1990–2010: A systematic analysis for the Global Burden of Disease Study 2010. Lancet 2012, 380, 2224–2260. [Google Scholar] [PubMed]
- Lozano, R.; Naghavi, M.; Foreman, K.; Lim, S.; Shibuya, K.; Aboyans, V.; Abraham, J.; Adair, T.; Aggarwal, R.; Ahn, S.Y.; et al. Global and regional mortality from 235 causes of death for 20 age groups in 1990 and 2010: A systematic analysis for the Global Burden of Disease Study 2010. Lancet 2012, 380, 2095–2128. [Google Scholar] [PubMed]
- World Health Organization. Chronic Obstructive Pulmonary Disease (COPD). Available online: www.who.int/respiratory/copd/en/ (accessed on 31 July 2014).
- Eisner, M.D.; Anthonisen, N.; Coultas, D.; Kuenzli, N.; Perez-Padilla, R.; Postma, D.; Romieu, I.; Silverman, E.K.; Balmes, J.R.; Committee on Nonsmoking COPD. An official American Thoracic Society public policy statement: Novel risk factors and the global burden of chronic obstructive pulmonary disease. Am. J. Respir. Crit. Care Med. 2010, 182, 693–718. [Google Scholar] [CrossRef] [PubMed]
- Schikowski, T.; Mills, I.C.; Anderson, H.R.; Cohen, A.; Hansell, A.; Kauffmann, F.; Kramer, U.; Marcon, A.; Perez, L.; Sunyer, J.; et al. Ambient air pollution:A cause for COPD? Eur. Respir.J. 2013, 43, 253–263. [Google Scholar]
- Ezzati, M.; Lopez, A.D. Smoking and oral tobacco use. In Comparative Quantification of Health Risks Global and Regional Burden of Disease Attribution to Selected Major Risk Factors; World Health Organization: Geneva, Switzerland, 2004; Volume 1, p. 883. [Google Scholar]
- Smith, K.R.; Mehta, S.; Maeusezahl-Feuz, M. Indoor air pollution from household use of solid fuels. In Comparative Quantification of Health Risks:Global and Regional Burden of Disease Attribution to Selected Major Risk Factors; World Health Organization: Geneva, Switzerland, 2004; Volume 2, p. 1435. [Google Scholar]
- Kurmi, O.P.; Semple, S.; Simkhada, P.; Smith, W.C.S.; Ayres, J.G. COPD and chronic bronchitis risk of indoor air pollution from solid fuel: A systematic review and meta-analysis. Thorax. 2010, 65, 221–228. [Google Scholar] [PubMed]
- Van de Meer, R.M.; Wagena, E.J.; Ostelo, R.W.; Jacobs, J.E.; Van Schayck, C.P. Smoking cessation for chronic obstructive pulmonary disease. Cochrane Database Syst. Rev. 2001, 1. [Google Scholar] [CrossRef]
- PubMed. Available online: www.ncbi.nlm.nih.gov/pubmed/ (accessed on 31 July 2014).
- Harvard University. EMBASE. Available online: www.embase.com.ezp-prod1.hul.harvard.edu/home (accessed on 31 July 2014).
- Cohen, A.J.; Anderson, H.R.; Ostro, B.; Pandey, K.D.; Krzyzanowski, M.; Künzli, N.; Gutschmidt, K.; Pope, C.A., III; Romieu, I.; Samet, J.M. Urban air pollution. In Comparative Quantification of Health Risks Global and Regional Burden of Disease Attributable to Selected Major Risk Factors; World Health Organization: Geneva, Switzerland, 2004; Volume 2, p. 1353. [Google Scholar]
- Higgins, J.P.; Green, S. Cochrane Handbook for Systematic Reviews of Interventions Version 5.0.2 [updated September 2009]. The Cochrane Collaboration, 2009. Available online: www.cochrane-handbook.org (accessed on 29 September 2009).
- Lin, H.H.; Ezzati, M.; Murray, M. Tobacco Smoke, Indoor Air Pollution and Tuberculosis: A Systematic Review and Meta-Analysis. PLOS Med. 2007, 4. [Google Scholar] [CrossRef]
- Tao, F.; Gonzalez-Flecha, B.; Kobzik, L. Reactive oxygen species in pulmonary inflammation by ambient particulates. Free Radic. Biol. Med. 2003, 35, 327–340. [Google Scholar] [CrossRef] [PubMed]
- Goldsmith, C.A.; Frevert, C.; Imrich, A.; Sioutas, C.; Kobzik, L. Alveolar macrophage interaction with air pollution particulates. Environ. Health Perspect. 1997, 105, 1191–1195. [Google Scholar] [CrossRef] [PubMed]
- Shi, M.M.; Chong, I.W.; Godleski, J.J.; Paulauskis, J.D. Regulation of macrophage inflammatory protein-2 gene expression by oxidative stress in rat alveolar macrophages. Immunology 1999, 97, 309–315. [Google Scholar] [CrossRef] [PubMed]
- Becker, S.; Soukup, J.M.; Gilmour, M.I.; Devlin, R.B. Stimulation of human and rat alveolar macrophages by urban air particulates: Effects on oxidant radical generation and cytokine production. Toxicol. Appl. Pharmacol. 1996, 141, 637–648. [Google Scholar] [CrossRef] [PubMed]
- Prahalad, A.K.; Soukup, J.M.; Inmon, J.; Willis, R.; Ghio, A.J.; Becker, S.; Gallagher, J.E. Ambient air particles: Effects on cellular oxidant radical generation in relation to particulate elemental chemistry. Toxicol. Appl. Pharmacol. 1999, 158, 81–91. [Google Scholar] [CrossRef] [PubMed]
- Ghio, A.J.; Stonehuerner, J.; Dailey, L.A.; Carter, J.D. Metals associated with both the water-soluble and insoluble fractions of an ambient air pollution particle catalyze an oxidative stress. Inhal. Toxicol. 1999, 11, 37–49. [Google Scholar] [CrossRef] [PubMed]
- Abbey, D.E.; Mills, P.K.; Petersen, F.F.; Beeson, W.L. Long-Term ambient concentrations of total suspended particulates and oxidants as related to incidence of chronic disease in california seventh-day adventists. Environ. Health Perspect. 1991, 94, 43–50. [Google Scholar] [CrossRef] [PubMed]
- Karakatsani, A.; Andreadaki, S.; Katsouyanni, K.; Dimitroulis, I.; Trichopoulos, D.; Benetou, V.; Trichopoulou, A. Air pollution in relation to manifestations of chronic pulmonary disease: A nested case-control study in Athens, Greece. Eur. J. Epidemiol. 2003, 18, 45–53. [Google Scholar] [CrossRef] [PubMed]
- Sunyer, J.; Jarvis, D.; Gotschi, T.; Garcia-Esteban, R.; Jacquemin, B.; Aguilera, I.; Ackerman, U.; de Marco, R.; Forsberg, B.; Gislason, T.; et al. Chronic bronchitis and urban air pollution in an international study. Occup. Environ. Med. 2006, 63, 836–843. [Google Scholar] [CrossRef] [PubMed]
- Schwartz, J. Particulate air pollution and chronic respiratory disease. Environ. Res. 1993, 62, 7–13. [Google Scholar] [CrossRef] [PubMed]
- World Health Organisation; Global Health Obervotary. Public Health and Environment (PHE): AmbientAir Pollution. Exposure to Particulate Matter Less Than 10 µm in Diameter in Uban Areas, 2008–2013. Available online: gamapserver.who.int/gho/interactive_charts/phe/oap_exposure/atlas.html. (access on 31 October 2013).
- Zanobetti, A.; Bind, M.-A.C.; Schwartz, J. Particulate air pollution and survival in a COPD cohort. Environ. Health 2008, 7. [Google Scholar] [CrossRef]
- Næss, Ø.; Nafstad, P.; Aamodt, G.; Claussen, B.; Rosland, P. Relation between concentration of air pollution and cause-specific mortality: Four-year exposures to nitrogen dioxide and particulate matter pollutants in 470 neighborhoods in Oslo, Norway. Am. J. Epidemiol. 2007, 165, 435–443. [Google Scholar]
© 2014 by the authors; licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Song, Q.; Christiani, D.C.; XiaorongWang; Ren, J. The Global Contribution of Outdoor Air Pollution to the Incidence, Prevalence, Mortality and Hospital Admission for Chronic Obstructive Pulmonary Disease: A Systematic Review and Meta-Analysis. Int. J. Environ. Res. Public Health 2014, 11, 11822-11832. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph111111822
Song Q, Christiani DC, XiaorongWang, Ren J. The Global Contribution of Outdoor Air Pollution to the Incidence, Prevalence, Mortality and Hospital Admission for Chronic Obstructive Pulmonary Disease: A Systematic Review and Meta-Analysis. International Journal of Environmental Research and Public Health. 2014; 11(11):11822-11832. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph111111822
Chicago/Turabian StyleSong, Qingkun, David C. Christiani, XiaorongWang, and Jun Ren. 2014. "The Global Contribution of Outdoor Air Pollution to the Incidence, Prevalence, Mortality and Hospital Admission for Chronic Obstructive Pulmonary Disease: A Systematic Review and Meta-Analysis" International Journal of Environmental Research and Public Health 11, no. 11: 11822-11832. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph111111822