1. Introduction
High levels of physical inactivity and sedentary behaviour are a global concern. Self-reported data from 39 countries indicate that only 23% and 19% of 11 and 13 year olds achieve the recommended 60 min per day of moderate-to-vigorous physical activity (MVPA) [
1]. Objectively measured physical activity data show that among Canadian children aged 6- to 10-years, 14% of boys and 7% of girls achieve the recommendations, and they spend an average of 7.4 h per day being sedentary [
2]. Data from 27 countries point toward worldwide declines in the performance of children in the 20 m shuttle run test over the last few decades [
3].
In parallel with these trends, evidence suggests that the current generation of children play outside less frequently and for shorter durations than their parents’ generation did [
4,
5]. It has been suggested that children’s physical activity is moving away from unstructured and unsupervised outdoor play toward structured and supervised activities that primarily occur indoors [
6,
7]. Certain parenting practices common among the middle-class are partially responsible for this shift. The prioritization of academic achievement [
8,
9] and the tendency for middle-class parents to engage in “concerted cultivation”—Enrolling children in an abundance of extra-curricular enrichment activities, has left children with little unstructured time [
8,
10]. Heightened concerns for child safety (
i.e., injuries, strangers, gangs, and other hazards) [
5,
6,
11,
12,
13] may also be among the forces pushing children indoors. Although some children have said they prefer to play outside when given the choice [
14,
15,
16], others have reported that they are drawn indoors by interest in sedentary activities such as screen time (e.g., watching TV, playing video games, using the internet), listening to music, art, and reading [
17]. This is likely motivated, in part, by the changing nature of children’s social environments, which occurs decreasingly outside and increasingly on screens [
18].
Several researchers have proposed that increasing outdoor time could be an effective strategy for limiting sedentary behaviour and increasing physical activity and fitness in children e.g., [
19,
20]. However, researchers typically cite only a few cross-sectional studies, if any, as evidence of a relationship with outdoor time. Recently published reviews have identified outdoor time as one of several correlates of children’s physical activity behaviour [
21,
22,
23,
24]. However, none of these reviews goes beyond the identification of cross-sectional relationships, which typically provide insufficient evidence of a causal relationship between outdoor time and physical activity [
21,
22,
23,
24]. Relationships between outdoor time and children’s physical fitness and sedentary behaviour have not been examined systematically to our knowledge. Therefore, the purpose of the current study was to systematically review and evaluate the evidence on the relationship between outdoor time and: (1) physical activity, (2) cardiorespiratory fitness, (3) musculoskeletal fitness, (4) sedentary behavior; and (5) motor skill development in children aged 3–12 years. Our review aimed to include prospective and experimental studies in addition to cross-sectional studies.
2. Methods
This systematic review is registered with the international prospective register of systematic reviews PROSPERO network (registration No. CRD42014009307), and followed the PRISMA statement for reporting systematic reviews [
25].
2.1. Study Inclusion Criteria
We aimed to identify all studies that examined the relationship between outdoor time and physical activity, sedentary behaviour, fitness, or motor skill development in children. Study designs eligible for inclusion were randomized controlled trial (RCT) and non-randomized controlled study (NRS) designs (e.g., cross-sectional, retrospective cohorts, prospective cohorts, case-control). Longitudinal studies were only included if there was an assessment of outdoor time within our set age limits. Studies in languages other than English were included if we were able to translate results using Google Translate.
Study inclusion was dependent upon meeting the pre-determined population, intervention, comparator, and outcome (PICO) study criteria [
26].
Population: Apparently healthy children (
i.e., no clinical diagnosis) aged 3.00–12.99 years. If age was not reported but school year/grade was, the standard regional age range associated with that year/grade was used to determine eligibility for inclusion.
Intervention (exposure): Duration of outdoor time.
Comparator: Indoor time or various durations of outdoor time. Eligible contexts included outdoor settings in general and those that contrasted outdoor and indoor time under specific circumstances (e.g., an unstructured school recess held indoors compared to outdoors). Eligible measures of outdoor time and indoor time included objective measures (e.g., global positioning system), direct observation (e.g., momentary time sampling), and subjective assessments (e.g., proxy- and self-reported outdoor time).
Outcome: Five movement behaviours and aspects of physical fitness were chosen as outcome indicators by expert agreement. The five eligible indicators in this review were:
Physical activity (any intensity and all forms)
Cardiorespiratory fitness (submaximal exercise capacity, maximal aerobic power, heart functions, lung functions, blood pressure)
Musculoskeletal fitness (power, strength, endurance, bone density)
Sedentary behaviour (prolonged sitting, screen time such as watching television, playing video games, computer use, or motorized transportation)
Motor skill (agility, balance, coordination, speed of movement)
Physical activity and sedentary behaviour were categorized depending on whether they were assessed as acute or habitual outcome behaviours. To be categorized as acute (single bout), the outcome behaviour must have been reported separately during outdoor time and during indoor time, such that it was possible to compare the behaviour in outdoor and indoor settings. For example, a study could have compared the proportion of time spent sedentary when children were outdoors vs. when they were indoors. To be categorized as habitual (typical/usual), the assessment of indoor/outdoor time and the outcome needed to be reported in generalities, such that it was possible to conclude that children who typically spend a certain amount of time outdoors accumulate a certain overall level of the outcome behaviour. For example, the typical duration spent outside each day and weekly physical activity.
2.2. Search Strategy
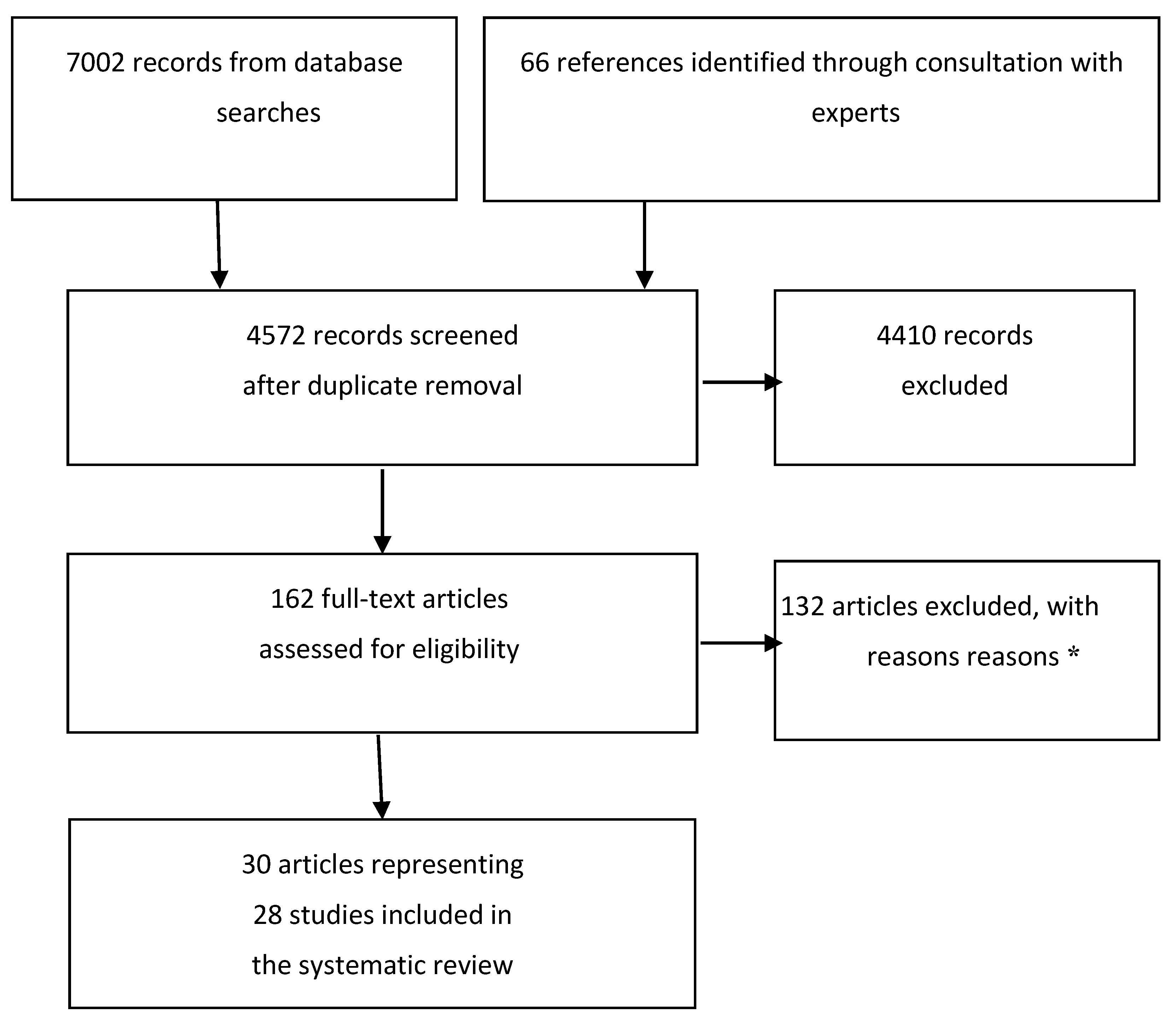
The electronic search strategy was created by M.S. The following databases were searched using the Ovid interface: MEDLINE including In-Process & Other Non-Indexed Citations (1946 to 31 March 2014), Embase (1980 to 2014 week 3), and PsycInfo (1806 to March week 4 2014). CINAHL and SportDiscus were searched using the EBSCOhost interface (database dates not given). No language or study design limits were applied. The search strategies are presented in
Supplementary File 1. All co-authors were asked to recommend potentially relevant studies to assist M.S. in the development of the search strategy. Key content experts (
n = 5) were asked to scan their personal libraries to identify the most influential papers on outdoor time, physical activity, sedentary behaviour, and physical fitness related outcomes in children. No new relevant articles were identified through key content experts, suggesting it is unlikely key articles were missed by the search.
References were imported into Reference Manager Software (Thompson Reuters, San Francisco, CA, USA) where duplicate references were removed. Two independent reviewers screened titles and abstracts of potentially relevant articles, and subsequently examined all potentially relevant full text articles (Rebecca Gibbons and Richard Larouche). Disagreements were resolved by discussion and consensus between the two reviewers or by a third reviewer (Casey Gray) if consensus could not be achieved.
4. Discussion
This review found that outdoor time is positively related to physical activity and negatively related to sedentary behaviour in children aged 3–12 years. Studies that examined habitual behaviours showed that children with higher amounts of outdoor time engaged in higher amounts of physical activity and lower amounts of sedentary behaviour than children who spend less time outdoors. Studies that examined acute behaviours showed that children were more physically active and less sedentary while they were outside than while they were inside.
All of the studies examined showed that physical activity was higher outdoors compared with indoors. The consistent positive relationship between outdoor time and physical activity held across sexes, age groups (preschoolers, school-aged children), and contexts (full day, leisure time, adult directed). Our finding that outdoor time is a positive correlate of physical activity is consistent with three previous systematic reviews and one review of reviews carried out with preschoolers, children and youth [
22,
23,
24,
59]. Between them, the four reviews captured a total of four studies in 6 papers [
28,
39,
40,
43,
44,
57], all of which were also captured by our search, increasing our confidence that our review was comprehensive. Of the studies included, all reported small sample sizes (N’s = 191–246) and relied on direct observation of outdoor time; three studies used direct observation to assess physical activity and one used pedometers. Furthermore, the previous reviews were designed to examine correlates of physical activity, and did not assess the risk of bias or overall quality of evidence. We found that all of the studies included in our review were also observational and assessed exposures and outcomes of interest simultaneously rather than prospectively, which may limit our ability to infer causal relationships between outdoor time and identified outcomes. The design of included studies also prevented us from assigning a high quality of evidence rating in accordance with GRADE framework. However, the use of objective measures of physical activity and sedentary behaviour (e.g., accelerometers) and outdoor location (
i.e., GPS) in some studies, and the consistency of the results pertaining to the relationships between outdoor time, physical activity and sedentary behaviour is reason not to rule out the possibility of causation.
Four studies examined sedentary behaviour in this review. Studies conducted in preschool settings showed that increased time outside at preschool was related to lower sedentary behaviour [
34,
48,
50,
51]. Interestingly, this contrasts with the findings of Dowda and colleagues [
60], who identified that preschool policies promoting outdoor time had no effect on preschoolers’ sedentary behaviour levels. Rather than concluding outdoor time did not influence sedentary behaviour, it may be that policies to increase outdoor time in early childcare centres were not implemented appropriately [
60], that outdoor play policies hindered movement, or that the outdoor play spaces were not challenging enough [
61].
To the best of our knowledge, this is the first attempt to systematically review the literature on the effects of outdoor time on cardiorespiratory fitness, musculoskeletal fitness, or motor skill development in children. Very few studies that examined indicators of cardiorespiratory fitness and motor skill development were identified in our review, and those that did reported no clear relationship with outdoor time. Schaefer and colleagues [
62] reported positive cross-sectional relationships between self-reported time spent outdoors after school and Leger shuttle run scores in 9–17 year olds (
x = 13.6 ± 1.4 years), with children who spend most or all of their afterschool time outdoors achieving higher cardiorespiratory fitness than children who spend none of their after school time outside. No differences were found for outdoor time and blood pressure [
62]. This study was ineligible for our review because the mean age of participants was outside of our target range; however, these results suggest that outdoor time may be associated with greater aerobic fitness in children and youth similarly across age ranges.
This review examined outdoor
versus indoor time in general. It did not assess outcomes in relation to the quality of the outdoor environment, which has been suggested to be an important correlate of physical activity [
63]. For example, it is plausible that greater benefits would be derived from more natural outdoor settings. Proximity to undeveloped green space (e.g., accessible wooded areas) was related to increased physical activity in a sample of 11–13 year old participants of the Canadian Health Behaviour in School-Aged Children survey [
64]. Positive relationships in increasingly natural settings may be particularly beneficial for blood pressure, as adult studies have shown that outdoor exercise lowers systolic blood pressure more than treadmill training [
57]. Other environmental characteristics have also been forwarded as promoting physical activity or reducing sedentary behaviour in outdoor environments. For instance, McKenzie [
42] observed that children more frequently prompt each other to be active outdoors than indoors, and prompt each other to be sedentary more often indoors than outdoors. Parents are also very likely to prompt children to be sedentary while indoors. Alternatively, increasingly natural environments may not improve the relationship between outdoor time and movement behaviours universally. For example, children who reside in neighbourhoods marked by high levels of physical disorder and those living in public housing played outdoors more often than other children [
65]. There is a need for future research to further elucidate the role of nature in the relationships between outdoor time and movement behaviours. A combination of accelerometers with GPS and geographic information systems can be used to provide greater insights into the characteristics of outdoor environments that promote or discourage physical activity [
66].
Increasing the amount of time children spend outdoors has been recommended as a promising strategy for increasing children’s physical activity levels [
19,
20]. Child reported preferences for outdoor play suggest interventions to increase outdoor time would be well-received by the targeted population [
14,
15]. However, some public health campaigns have collectively recommended keeping children indoors for almost the entire day. These include campaigns that recommend staying indoors during peak daylight hours (10:00 am–4:00 pm) to avoid sun exposure and melanoma risk (e.g.,
http://www.healthlinkbc.ca/healthfiles/pdf/hfile26.pdf) [
67], campaigns that recommend staying indoors in the rush-hour periods before and after school to avoid traffic related air pollution (e.g.,
http://www.peelregion.ca/health/cleanairpeel/smog-health.htm) [
68], and campaigns that recommend staying indoors in the evening hours (from dusk to dawn) to prevent mosquito carried illnesses (e.g.,
http://www.healthlinkbc.ca/healthfiles/pdf/hfile88.pdf) [
69]. By continuing to demonstrate that outdoor time is also related to positive health outcomes, researchers can contribute to informing a more balanced perspective to health promotion and chronic disease prevention.
Efforts to increase children’s outdoor time face another barrier—Parent concerns about child safety and prioritizing of academic achievement over physical health [
3,
4,
5,
6,
7]. Some have said that this is having a negative effect on children’s outdoor time [
6,
7,
12]. There is a clear need to convey the serious importance of increasing physical activity and decreasing sedentary behaviour on the present and future health of children and youth, and to understand children’s need to experience increasing levels of challenge such as wandering without adult supervision and other types of “risky play” [
70,
71].
Strengths and Limitations
There were several strengths associated with this systematic review. Our comprehensive search strategy was developed by a research librarian with specific expertise in the systematic reviews with guidance from a strong team of content area experts. Our inclusion and exclusion criteria and analysis plan were registered on PROSPERO
a-priori for improved transparency. We included objective and subjective measures of outdoor time, allowing us to comment on the duration of outdoor time, but also the specific context; four studies used GPS to determine indoor and outdoor location [
35,
45,
47,
52], while the remaining studies used direct observation [
28,
31,
39,
40,
42,
43,
48,
49,
50,
51,
56], proxy-report [
29,
30,
31,
32,
33,
34,
37,
41,
53,
54], and self-report [
36,
38,
46,
58]. Finally, we followed systematic processes for examining the risk of bias and quality of included studies [
27], which enabled the synthesized results to be interpreted within the context of the inherent limitations of each study. The observational nature of included studies automatically increases the risk of bias associated with studies in this review. However, there were few other factors of concern.
Limitations of this review included heterogeneity in the measurement of outdoor time and outcome variables across the included studies. As such, while it was possible to ascertain the direction of the detected relationships, it was not possible to quantify the overall effect size for each outcome. All of the included studies relied on observational designs, and nearly all (
i.e., 26 of 28 studies) used cross-sectional designs. There is a clear need for more evidence from studies using randomized research designs to examine whether increasing outdoor time leads to increased physical activity and decreased sedentary time. Without these experimental designs it was difficult to definitively state if there are cause-effect relationships between outdoor time and included outcomes. Finally, our systematic review predominantly included studies from developed nations, which was a limitation of the evidence base. The type and quantity of physical activity and sedentary behaviour differ between developing and developed nations (e.g., active transportation and subsistence chores are generally more common in rural Africa than in developed nations) [
72]. Nevertheless, there is no reason to expect the direction of the relationships between outdoor time and physical activity or sedentary behaviour to differ in developing countries.





{kind=link}