Geographic Distribution and Temporal Trends of HIV-1 Subtypes through Heterosexual Transmission in China: A Systematic Review and Meta-Analysis

Abstract
:1. Introduction
2. Methods
2.1. Literature Search Strategy
2.2. Inclusion and Exclusion Criteria
2.3. Data Extraction
2.4. Statistical Analysis
3. Results
3.1. Study Identification and Selection
3.2. General Characteristic of the Included Studies
3.3. The Overall Proportion of HIV-1 Subtypes
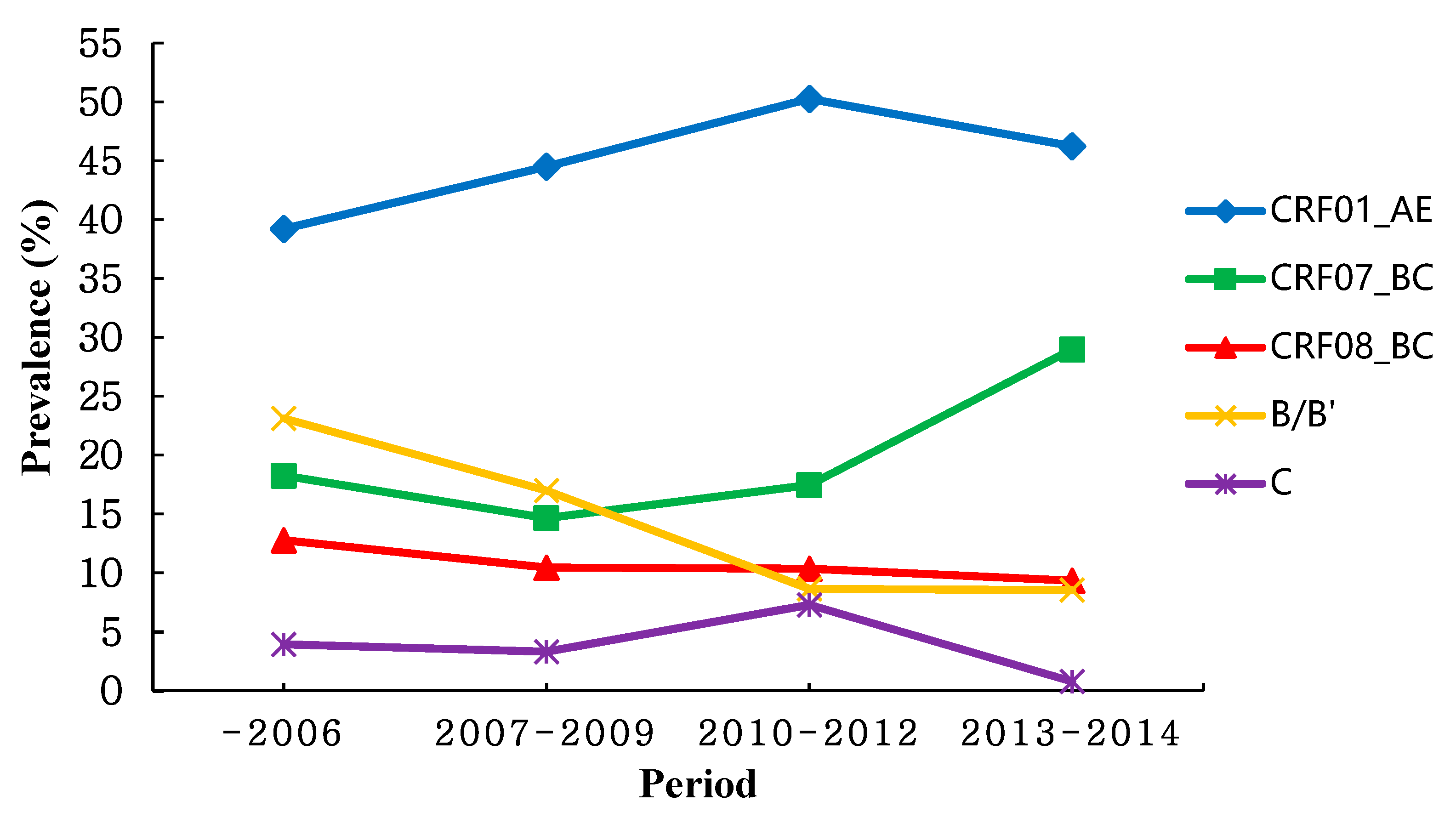
3.4. Temporal Trend of HIV-1 Subtypes
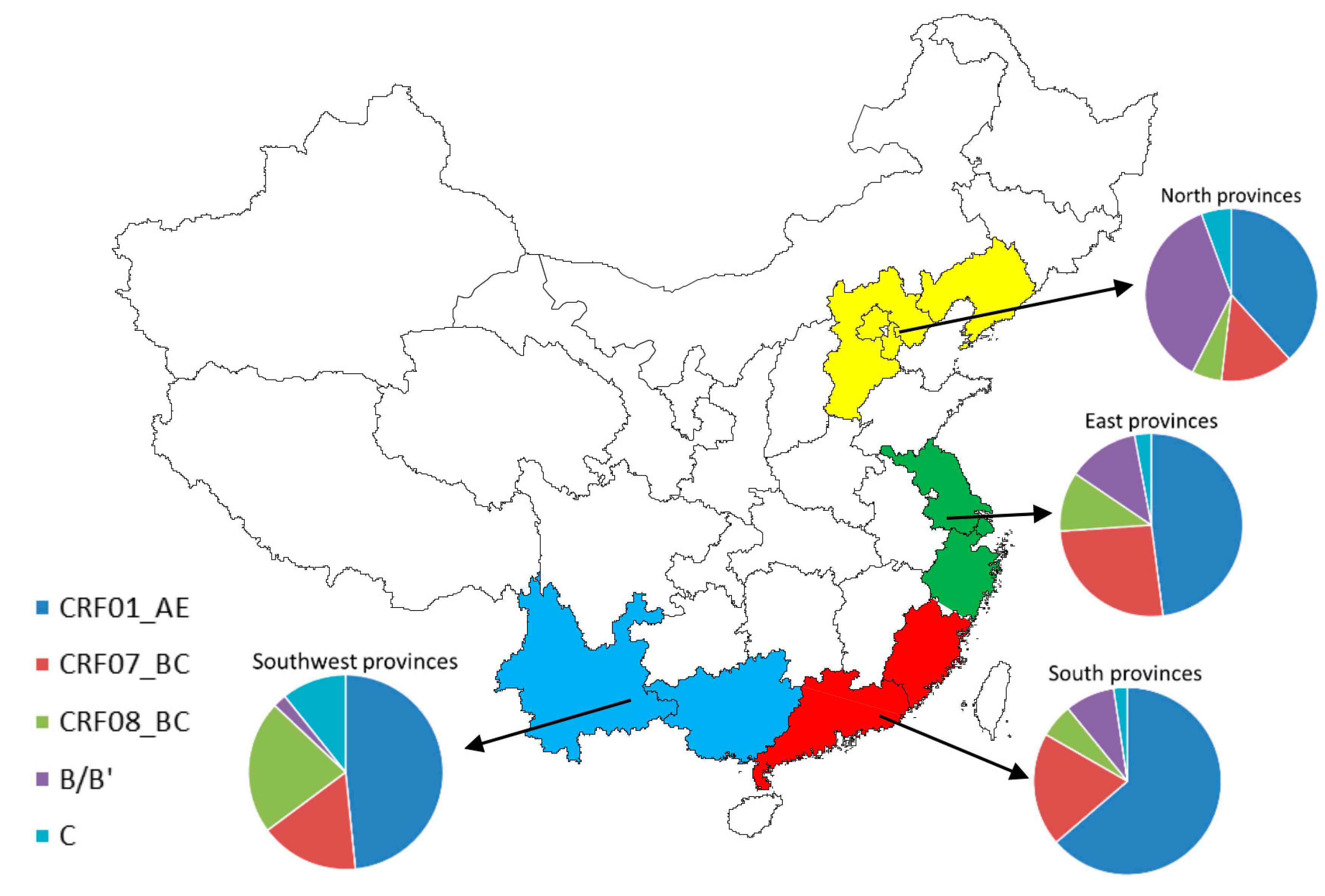
3.5. Geographic Distribution of HIV-1 Subtypes
3.6. Amplification of HIV-1 Gene Region
3.7. Sensitivity Analysis
4. Discussion
5. Conclusions
Supplementary Materials
Acknowledgments
Author Contributions
Conflicts of Interest
References
- Zeng, Y.; Fan, J.; Zhang, Q.; Wang, P.C.; Tang, D.J.; Zhon, S.C.; Zheng, X.W.; Liu, D.P. Detection of antibody to LAV/HTLV-III in sera from hemophiliacs in China. AIDS Res. 1986, 2, S147–S149. [Google Scholar] [PubMed]
- Xiao, Y.; Kristensen, S.; Sun, J.; Lu, L.; Vermund, S.H. Expansion of HIV/AIDS in China: Lessons from Yunnan province. Soc. Sci. Med. 2007, 64, 665–675. [Google Scholar] [CrossRef] [PubMed]
- Jia, Y.; Lu, F.; Sun, X.; Vermund, S.H. Sources of data for improved surveillance of HIV/AIDS in China. Southeast Asian J. Trop. Med. Public Health 2007, 38, 1041–1052. [Google Scholar] [PubMed]
- Wang, N.; Wang, L.; Wu, Z.; Guo, W.; Sun, X.; Poundstone, K.; Wang, Y. Estimating the number of people living with HIV/AIDS in China: 2003-09. Int. J. Epidemiol. 2010, 39, ii21–ii28. [Google Scholar] [CrossRef] [PubMed]
- National Center for AIDS/STD Control and Prevention, China CDC. Update on the AIDS/STD epidemic in China and main response in control and prevention in December, 2016. Chin. J. AIDS STD 2017, 23, 93. (In Chinese) [Google Scholar]
- Wang, L.; Ding, Z.; Qin, Q.; Cai, C.; Guo, W.; Cui, Y. Characteristics of HIV transmission through heterosexual contact in China, 2008–2014. Zhonghua Liuxingbingxue Zazhi 2015, 36, 1332–1336. [Google Scholar] [PubMed]
- Roberts, J.D.; Bebenek, K.; Kunkel, T.A. The accuracy of reverse transcriptase from HIV-1. Science 1988, 242, 1171–1173. [Google Scholar] [CrossRef] [PubMed]
- Lemey, P.; Pybus, O.G.; Wang, B.; Saksena, N.K.; Salemi, M.; Vandamme, A.M. Tracing the origin and history of the HIV-2 epidemic. Proc. Natl. Acad. Sci. USA 2003, 100, 6588–6592. [Google Scholar] [CrossRef] [PubMed]
- Sharp, P.M.; Hahn, B.H. Origins of HIV and the AIDS pandemic. Cold Spring Harb. Perspect. Med. 2011, 1, a006841. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Vidal, N.; Peeters, M.; Mulanga-Kabeya, C.; Nzilambi, N.; Robertson, D.; Ilunga, W.; Sema, H.; Tshimanga, K.; Bongo, B.; Delaporte, E. Unprecedented degree of human immunodeficiency virus type 1 (HIV-1) group M genetic diversity in the Democratic Republic of Congo suggests that the HIV-1 pandemic originated in Central Africa. J. Virol. 2000, 74, 10498–10507. [Google Scholar] [CrossRef] [PubMed]
- Sharp, P.M.; Hahn, B.H. The evolution of HIV-1 and the origin of AIDS. Philos. Trans. R. Soc. Lond. Ser. B Biol. Sci. 2010, 365, 2487–2494. [Google Scholar] [CrossRef] [PubMed]
- Hemelaar, J.; Gouws, E.; Ghys, P.D.; Osmanov, S. Global trends in molecular epidemiology of HIV-1 during 2000–2007. AIDS 2011, 25, 679–689. [Google Scholar] [CrossRef] [PubMed]
- Hemelaar, J. The origin and diversity of the HIV-1 pandemic. Trends. Mol. Med. 2012, 18, 182–192. [Google Scholar] [CrossRef] [PubMed]
- He, X.; Xing, H.; Ruan, Y.; Hong, K.; Cheng, C.; Hu, Y.; Xin, R.; Wei, J.; Feng, Y.; Hsi, J.H.; et al. A comprehensive mapping of HIV-1 genotypes in various risk groups and regions across China based on a nationwide molecular epidemiologic survey. PLoS ONE 2012, 7, e47289. [Google Scholar] [CrossRef] [PubMed]
- Li, Y.; Han, Y.; Xie, J.; Gu, L.; Li, W.; Wang, H.; Lv, W.; Song, X.; Li, Y.; Routy, J.P.; et al. CRF01_AE subtype is associated with X4 tropism and fast HIV progression in Chinese patients infected through sexual transmission. AIDS 2014, 28, 521–530. [Google Scholar] [CrossRef] [PubMed]
- Li, Y.; Gu, L.; Han, Y.; Xie, J.; Wang, H.; Lv, W.; Song, X.; Li, Y.; Iwamoto, A.; Ishida, T.; et al. HIV-1 subtype B/B’ and baseline drug resistance mutation are associated with virologic failure: A multicenter cohort study in China. J. Acquir. Immune Defic. Syndr. 2015, 68, 289–297. [Google Scholar] [CrossRef] [PubMed]
- Sui, H.; Gui, T.; Jia, L.; Guo, W.; Han, J.; Liu, Y.; Bao, Z.; Li, H.; Li, J.; Li, L. Different frequencies of drug resistance mutations among HIV-1 subtypes circulating in China: A comprehensive study. PLoS ONE 2014, 9, e91803. [Google Scholar] [CrossRef] [PubMed]
- Liberati, A.; Altman, D.G.; Tetzlaff, J.; Mulrow, C.; Gotzsche, P.C.; Ioannidis, J.P.; Clarke, M.; Devereaux, P.J.; Kleijnen, J.; Moher, D. The PRISMA statement for reporting systematic reviews and meta-analyses of studies that evaluate health care interventions: Explanation and elaboration. J. Clin. Epidemiol. 2009, 62, e1–e34. [Google Scholar] [CrossRef] [PubMed]
- Miller, J.J. The inverse of the Freeman-Tukey double arcsine transformation. Am. Stat. 1978, 32, 138. [Google Scholar] [CrossRef]
- Cassone, A. Prevalence of tuberculosis, hepatitis C virus, and HIV in homeless people: A systematic review and meta-analysis. Pathog. Glob. Health 2012, 106, 377. [Google Scholar] [CrossRef] [PubMed]
- Zhang, L.; Wang, Y.J.; Wang, B.X.; Yan, J.W.; Wan, Y.N.; Wang, J. Prevalence of HIV-1 subtypes among men who have sex with men in China: A systematic review. Int. J. STD AIDS 2015, 26, 291–305. [Google Scholar] [CrossRef] [PubMed]
- Higgins, J.P.; Thompson, S.G.; Deeks, J.J.; Altman, D.G. Measuring inconsistency in meta-analyses. BMJ 2003, 327, 557–560. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Higgins, J.P.; Thompson, S.G. Quantifying heterogeneity in a meta-analysis. Stat. Med. 2002, 21, 1539–1558. [Google Scholar] [CrossRef] [PubMed]
- Ye, J.R.; Li, Y.; Bai, L.S. Sequence and subtype analysis of gag gene of isolates confirmed by HIV-1 infections in Beijing in 2007. Virology 2009, 25, 420–423. (In Chinese) [Google Scholar]
- He, H.L.; Xu, F.l.; Cai, W.P.; Chen, X.J.; He, J.Y.; Jia, W.D. Molecular epidemiology of HIV-1 in Guangdong province. Guangdong Med. 2012, 33, 3471–3474. (In Chinese) [Google Scholar]
- Wu, X.F.; Cha, Y.F.; Ji, L.; Jing, M.H. Gene subtype analysis of HIV-1 strains isolated from different population groups in Huzhou. Chin. J. Health Lab. Technol. 2015, 25, 538–540. (In Chinese) [Google Scholar]
- Fan, W.; Yan, L.Q.; Huan, X.P. Study of spreading mode and molecular epidemiological characteristcs of heterosexual transmitted HIV in Huaian. Jiangsu J. Prev. Med. 2015, 26, 22–24. (In Chinese) [Google Scholar]
- Yan, L.Q.; Yang, P.F.; Guo, H.X. Epidemiological features and molecualr evolution of HIV-1 through heterosexual contact in Huaian. Pathog. Biol. 2016, 11, 55–59. (In Chinese) [Google Scholar]
- Yang, H.T.; Xu, X.Q.; Qiu, T.; Huan, X.P.; Hu, H.Y.; Guo, H.X. Molecular epidemiology of the human immunodeficiency virus-1 isolated from patients confirmed lately in Jiangsu province. ACTA Univ. Med. Nanjing 2009, 29, 976–980. (In Chinese) [Google Scholar]
- Li, X.J.; Xia, X.S.; Cao, C.M. Molecular epidemiology of HIV-1 transmission among heterosexuals in Kunming. Chin. J. Derm. Vener. 2009, 23, 294–295. (In Chinese) [Google Scholar]
- Wu, J.; Wang, X.Q.; Zhou, Y.Q.; Yu, X.L.; Gai, J.; Yuan, J.L.; Zheng, M.; Tao, J. Molecular epidemiological characteristics of HIV-1 in Shanghai, 2007–2013. Chin. J. AIDS STD 2016, 22, 5–9. (In Chinese) [Google Scholar]
- Tao, J.; Yu, X.L.; Zhang, J. Molecular epidemiological survey on HIV-1 subtypes in people with heterosexual transmission in Shanghai. J. Diagn. Concepts Pract. 2016, 15, 180–184. (In Chinese) [Google Scholar]
- Zhang, X.C.; Lin, Q.; Wang, X.G.; Fan, Y. Molecular epidemiological study of HIV-1 in Minghang District of Shanghai. Chin. Prev. Med. 2015, 16, 217–221. (In Chinese) [Google Scholar]
- Zhao, G.L.; Yu, W.; Zhang, J.J.; Chen, L.; Feng, T.J.; Wang, F. Study on the molecular-epidemiological characteristics of HIV-1 in Shenzhen, 1992–2008. Zhonghua Liuxingbingxue Zazhi 2012, 33, 82–87. [Google Scholar] [PubMed]
- Kong, D.F.; Wang, X.H.; Qin, Y.M. Molecular epidemiological characteristics of 528 HIV-1 infected cases in Shenzhen. Chin. Trop. Med. 2015, 15, 562–564. (In Chinese) [Google Scholar]
- Shi, X.D.; Chen, L.; Yang, Z.R.; Wang, X.H.; Zhao, J.; Wang, F. Molecular epidemiology of HIV-1 subtypes in Shenzhen of 2010. Chin. Trop. Med. 2012, 12, 192–194. (In Chinese) [Google Scholar]
- Wang, X.; Zheng, M.N.; Guo, Y. The genetic subtype of HIV-1 in different groups of HIV-1 infected person in Tianjin. Chin. J. Dis. Control Prev. 2012, 16, 509–512. (In Chinese) [Google Scholar]
- Zhao, C.Y.; Li, Q.M.; Zhao, H.R.; Lu, X.L. Study on subtypes distribution and characteristics for HIV-1 infection among MSM and heterosexuals. Chin. J. Dis. Control Prev. 2011, 15, 1035–1037. (In Chinese) [Google Scholar]
- Li, J.J.; Li, H.Q.; Li, J.Y.; Yang, S.M. Characteristics and distribution of HIV-1 subtypes in Yunnan province. Chin. J. AIDS STD 2016, 22, 145–149. (In Chinese) [Google Scholar]
- Chen, M.; Yao, S.T.; Ma, Y.L.; He, X.; Wang, J.B. Distribution of HIV-1 subtypes among different populations in Dehong prefecture, Yunnan province in 2011. Zhonghua Liuxingbingxue Zazhi 2012, 33, 883–887. [Google Scholar] [PubMed]
- Wang, H.; Liang, B.Y.; Zhou, B.; Jiang, J.J. Distribution of subtypes of pol gene in HIV-1 epidemic strains in Guangxi Zhuang Autonomous Region, 2010–2012. Chin. J. Prev. Med. 2016, 50, 79–84. (In Chinese) [Google Scholar]
- Zheng, M.; Wu, J.; Ni, Y.Q.; Zhou, Y.Q. Molecular epidemiology of HIV-1 in Shanghai in 2013. Chin. J. Infect. Dis. 2015, 33, 758–761. (In Chinese) [Google Scholar]
- Wu, J.; Xue, Y.L.; Kang, L.Y. Molecular epidemiology and drug resistance: Survey on HIV-1 in Luwan District of Shanghai. J. Diag. Concepts Pract. 2012, 11, 278–282. (In Chinese) [Google Scholar]
- Bao, Y.; Wang, X.H.; Chen, L.; He, T.P. Analysis on HIV-1 in homosexual and heterosexual transmission in molecular epidemiology in Shenzhen. Chin. J. Prev. Med. 2010, 44, 1055–1057. (In Chinese) [Google Scholar]
- Bao, Y.; Wang, X.H. The relationship between distribution of different subtypes of HIV-1 and the transmission routes in Shenzhen. Chin. J. Infect. Dis. 2012, 30, 532–537. (In Chinese) [Google Scholar]
- Pan, X.H.; Yao, Y.P.; Xia, S.C.; Yang, J.Z.; Guo, Z.H. Molecular epidemiology of HIV infection cases in 2003–2005 in Zhejiang province. Chin. J. AIDS STD 2007, 13, 308–310. (In Chinese) [Google Scholar]
- Qiu, D.H.; Wen, J.; Shen, W.W.; Chen, X.K. Molecular epidemiology among newly-diagonsed HIV-1 infections in Taizhou, Zhejiang province, 2011. Dis. Surveil. 2013, 28, 984–987. (In Chinese) [Google Scholar]
- Ye, J.R.; Su, X.L.; Yu, S.Q. Molecular epidemiological characteristics of HIV-1 strains isolated from newly diagnosed MSM subjects (2006–2010) in Beijing, China. Zhonghua Liuxingbingxue Zazhi 2013, 34, 49–52. [Google Scholar] [PubMed]
- Jin, M.H.; Wu, X.F.; Yang, Z.R. Analysis of subtypes of HIV-1 gag gene through sexually transmission in Huzhou. Chin. J. AIDS STD 2014, 20. (In Chinese) [Google Scholar]
- Zhang, S.; Zhang, J.F.; Gao, H.; Jiao, S.L. Molecualr epidemiology on HIV in Ningbo in 2009. Chin. J. HLT 2010, 20, 2889–2891. (In Chinese) [Google Scholar]
- Shen, P.; Su, Q.J.; Huang, Y.Y.; Jiang, L.P.; Zhang, D.Y.; Guo, J.C.; Wei, J.L.; Xu, H.Z. Modecular epidemiological study of HIV-1 in Qinann district of Qinzhou. Chin. J. RHSA 2015, 35, 1174–1177. (In Chinese) [Google Scholar]
- Cheng, H.; Yuan, R.; Xie, Y.; Ji, Y.Y.; Xiu, F.F.; Wang, B. A molecular epidemiological study on the human immunodeficiency virus infection in Wuxi city. Chin. J. Dis. Control Prev. 2015, 19, 1195–1199. (In Chinese) [Google Scholar]
- Han, X.; Dai, D.; Zhao, B.; Liu, J.; Ding, H.; Zhang, M.; Hu, Q.; Lu, C.; Goldin, M.; Takebe, Y.; et al. Genetic and epidemiologic characterization of HIV-1 infection in Liaoning province, China. J. Acquir. Immune Defic. Synd. 2010, 53, S27–S33. [Google Scholar] [CrossRef] [PubMed]
- Chen, S.; Cai, W.; He, J.; Vidal, N.; Lai, C.; Guo, W.; He, H.; Chen, X.; Fu, L.; Peeters, M.; et al. Molecular epidemiology of human immunodeficiency virus type 1 in Guangdong province of Southern China. PLoS ONE 2012, 7, e48747. [Google Scholar] [CrossRef] [PubMed]
- Bao, L.; Vidal, N.; Fang, H.; Deng, W.; Chen, S.; Guo, W.; Qin, C.; Peeters, M.; Delaporte, E.; Andrieu, J.M.; et al. Molecular tracing of sexual HIV type 1 transmission in the Southwest border of China. AIDS Res. Hum. Retrovir. 2008, 24, 733–742. [Google Scholar] [CrossRef] [PubMed]
- Li, L.; Chen, L.; Liang, S.; Liu, W.; Li, T.; Liu, Y.; Li, H.; Bao, Z.; Wang, X.; Li, J. Subtype CRF01_AE dominate the sexually transmitted human immunodeficiency virus type 1 epidemic in Guangxi, China. J. Med. Virol. 2013, 85, 388–395. [Google Scholar] [CrossRef] [PubMed]
- Deng, Y.; Zhang, C.; Yan, Y.; Yan, P.; Wu, S. Genetic subtype and epidemiological feature of HIV-1 circulating strains among recently infected patients in Fujian province. Zhonghua Liuxingbingxue Zazhi 2014, 35, 714–719. [Google Scholar] [PubMed]
- Yang, S.M.; Li, H.Q.; Chen, L.L.; Li, L.; Liu, Y.J.; Zhong, M.; Li, J.J.; Yang, B.H.; Gao, L.; Fan, Y.S.; et al. HIV-1 subtype and the distribution in Yunnan province. Zhonghua Liuxingbingxue Zazhi 2012, 33, 836–840. [Google Scholar] [PubMed]
- Zhang, J.F.; Pan, X.H.; Ding, X.B.; Chen, L.; Guo, Z.H.; Xu, Y.; Huang, J.J. Molecular epidemiological study on HIV/AIDS under the follow-up program in Zhejiang province in 2009. Zhonghua Liuxingbingxue Zazhi 2013, 34, 44–48. [Google Scholar] [PubMed]
- Pan, X.H.; Zhang, J.F.; Yao, Y.P.; Xu, Y.; Yang, J.Z.; Guo, Z.H. Subtype and transmission of HIV strain in both HIV infected spouses in Zhejiang province. Zhonghua Liuxingbingxue Zazhi 2010, 31, 638–641. [Google Scholar] [PubMed]
- Chen, Y.; Chen, S.; Kang, J.; Fang, H.; Dao, H.; Guo, W.; Lai, C.; Lai, M.; Fan, J.; Fu, L.; et al. Evolving molecular epidemiological profile of human immunodeficiency virus 1 in the Southwest border of China. PLoS ONE 2014, 9, e107578. [Google Scholar] [CrossRef] [PubMed]
- Li, Y.; Takebe, Y.; Yang, J.; Zhang, W.; Yang, R. High prevalence of HIV type 1 subtype B’ among heterosexuals in Western Hubei, Central China: Bridging the epidemic into the general population. AIDS Res. Hum. Retrovir. 2011, 27, 1025–1028. [Google Scholar] [CrossRef] [PubMed]
- Qin, C.; Zhang, P.; Zhu, W.; Hao, F.; Gu, A.; Fen, P.; Zhu, X.; Du, H. HIV-1 diversity in infected individuals in Suzhou and Suqian, China. SpringerPlus 2016, 5, 886. [Google Scholar] [CrossRef] [PubMed]
- Gui, T.; Lu, X.; Li, H.; Li, T.; Liu, Y.; Bao, Z.; Li, L.; Li, J. HIV-1 is spreading out of former high-risk population through heterosexual transmission in Hebei, China. Curr. HIV Res. 2016, 14, 148–153. [Google Scholar] [CrossRef] [PubMed]
- Zhong, P.; Kang, L.; Pan, Q.; Konings, F.; Burda, S.; Ma, L.; Xue, Y.; Zheng, X.; Jin, Z.; Nyambi, P. Identification and distribution of HIV type 1 genetic diversity and protease inhibitor resistance-associated mutations in Shanghai, P. R. China. J. Acquir. Immune Defic. Syndr. 2003, 34, 91–101. [Google Scholar] [CrossRef] [PubMed]
- Yao, X.; Wang, H.; Yan, P.; Lu, Y.; Lin, H.; Chen, L.; Ng, J.; Lau, E.; Liu, L.; Wu, J.; et al. Rising epidemic of HIV-1 infections among general populations in Fujian, China. J. Acquir. Immune Defic. Syndr. 2012, 60, 328–335. [Google Scholar] [CrossRef] [PubMed]
- Su, Y.; Liu, H.; Wu, J.; Zhu, L.; Wang, N. Distribution of HIV-1 genotypes in China: A systematic review. Zhonghua Liuxingbingxue Zazhi 2014, 35, 1164–1168. [Google Scholar] [PubMed]
- Li, X.; Li, W.; Zhong, P.; Fang, K.; Zhu, K.; Musa, T.H.; Song, Y.; Du, G.; Gao, R.; Guo, Y.; et al. Nationwide trends in molecular epidemiology of HIV-1 in China. AIDS Res. Hum. Retrovir. 2016, 32, 851–859. [Google Scholar] [CrossRef] [PubMed]
- Lin, H.; Ding, Y.; Liu, X.; Wu, Q.; Shen, W.; He, N. High prevalence of HIV infection and bisexual networks among a sample of men who have sex with men in Eastern China. PLoS ONE 2015, 10, e0129300. [Google Scholar] [CrossRef] [PubMed]
- Yun, K.; Xu, J.J.; Reilly, K.H.; Zhang, J.; Jiang, Y.J.; Wang, N.; Shang, H. Prevalence of bisexual behaviour among bridge population of men who have sex with men in China: A meta-analysis of observational studies. Sex. Transm. Infect. 2011, 87, 563–570. [Google Scholar] [CrossRef] [PubMed]
- Wei, H.; Xing, H.; Hsi, J.H.; Jia, M.; Feng, Y.; Duan, S.; He, C.; Yao, S.; Ruan, Y.; He, X.; et al. The sexually driven epidemic in youths in China’s Southwestern border region was caused by dynamic emerging multiple recombinant HIV-1 strains. Sci. Rep. 2015, 5, 11323. [Google Scholar] [CrossRef] [PubMed]
- Lim, R.B.; Wong, M.L.; Tan, P.H.; Govender, M. Heterosexual men who patronise entertainment establishments versus brothels in an asian urban setting—which group practises riskier sexual behaviours? BMC Public Health 2015, 15, 777. [Google Scholar] [CrossRef] [PubMed]
- Hittner, J.B. Meta-analysis of the association between methamphetamine use and high-risk sexual behavior among heterosexuals. Psychol. Addict. Behav. J. Soc. Psychol. Addict. Behav. 2016, 30, 147–157. [Google Scholar] [CrossRef] [PubMed]
- Tao, Y.L.; Zhao, X.T.; Tang, Y.F.; He, N. A systematic review of temporal and geographical distributions of HIV genotypes in China during 2000–2012. Chin. J. Dis. Control Prev. 2013, 17, 1073–1082. (In Chinese) [Google Scholar]
- Li, L.; Lu, X.; Li, H.; Chen, L.; Wang, Z.; Liu, Y.; Bao, Z.; Li, T.; Tian, C.; Liu, H.; et al. High genetic diversity of HIV-1 was found in men who have sex with men in Shijiazhuang, China. Infect. Genet. Evol. J. Mol. Epidemiol. Evol. Genet. Infect. Dis. 2011, 11, 1487–1492. [Google Scholar] [CrossRef] [PubMed]
- Zhang, Y.; Lu, L.; Ba, L.; Liu, L.; Yang, L.; Jia, M.; Wang, H.; Fang, Q.; Shi, Y.; Yan, W.; et al. Dominance of HIV-1 subtype CRF01_AE in sexually acquired cases leads to a new epidemic in Yunnan province of China. PLoS Med. 2006, 3, e443. [Google Scholar] [CrossRef] [PubMed]
- Wang, N.; Zhong, P. Molecular epidemiology of HIV in China: 1985–2015. Zhonghua Liuxingbingxue Zazhi 2015, 36, 541–546. [Google Scholar] [PubMed]
- Yu, X.F.; Chen, J.; Shao, Y.; Beyrer, C.; Lai, S. Two subtypes of HIV-1 among injection-drug users in Southern China. Lancet 1998, 351, 1250. [Google Scholar] [CrossRef]
- Feng, Y.; Takebe, Y.; Wei, H.; He, X.; Hsi, J.H.; Li, Z.; Xing, H.; Ruan, Y.; Yang, Y.; Li, F.; et al. Geographic origin and evolutionary history of China's two predominant HIV-1 circulating recombinant forms, CRF07_BC and CRF08_BC. Sci. Rep. 2016, 6, 19279. [Google Scholar] [CrossRef] [PubMed]
- Parczewski, M.; Leszczyszyn-Pynka, M.; Witak-Jedra, M.; Maciejewska, K.; Myslinska, S.; Urbanska, A. The temporal increase in HIV-1 non-R5 tropism frequency among newly diagnosed patients from northern poland is associated with clustered transmissions. J. Int. AIDS Soc. 2015, 18, 19993. [Google Scholar] [CrossRef] [PubMed]
- To, S.W.; Chen, J.H.; Wong, K.H.; Chan, K.C.; Chen, Z.; Yam, W.C. Determination of the high prevalence of dual/mixed- or X4-tropism among HIV type 1 CRF01_AE in Hong Kong by genotyping and phenotyping methods. AIDS Res. Hum. Retrovir. 2013, 29, 1123–1128. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hedskog, C.; Mild, M.; Albert, J. Transmission of the X4 phenotype of HIV-1: Is there evidence against the “random transmission” hypothesis? J. Infect. Dis. 2012, 205, 163–165. [Google Scholar] [CrossRef] [PubMed]
- Li, X.; Xue, Y.; Cheng, H.; Lin, Y.; Zhou, L.; Ning, Z.; Wang, X.; Yu, X.; Zhang, W.; Shen, F.; et al. HIV-1 genetic diversity and its impact on baseline CD4+T cells and viral loads among recently infected men who have sex with men in Shanghai, China. PLoS ONE 2015, 10, e0129559. [Google Scholar] [CrossRef] [PubMed]
- Li, X.; Xue, Y.; Zhou, L.; Lin, Y.; Yu, X.; Wang, X.; Zhen, X.; Zhang, W.; Ning, Z.; Yue, Q.; et al. Evidence that HIV-1 CRF01_AE is associated with low CD4+T cell count and CXCR4 co-receptor usage in recently infected young men who have sex with men (MSM) in Shanghai, China. PLoS ONE 2014, 9, e89462. [Google Scholar] [CrossRef] [PubMed]
- Huang, S.W.; Wang, S.F.; Lin, Y.T.; Yen, C.H.; Lee, C.H.; Wong, W.W.; Tsai, H.C.; Yang, C.J.; Hu, B.S.; Lin, Y.H.; et al. Patients infected with CRF07_BC have significantly lower viral loads than patients with HIV-1 subtype B: Mechanism and impact on disease progression. PLoS ONE 2014, 9, e114441. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Guo, H.; Hu, H.; Zhou, Y.; Huan, X.; Qiu, T.; Fu, G.; Lu, J.; Wang, X. The identification of a novel HIV-1 CRF01_AE/B recombinant using the near full length genome in Jiangsu province, China. AIDS Res. Hum. Retrovir. 2014, 30, 1239–1242. [Google Scholar] [CrossRef] [PubMed]
- Li, T.; Sun, G.; Jia, D.; Sun, C.; Wang, Z.; Liu, S.; Liu, Y.; Li, H.; Wang, X.; Li, J.; et al. Near full-length genome sequences of two novel HIV-1 recombinant forms detected in Henan province, China. AIDS Res. Hum. Retrovir. 2016, 32, 722–727. [Google Scholar] [CrossRef] [PubMed]
- Graf, M.; Shao, Y.; Zhao, Q.; Seidl, T.; Kostler, J.; Wolf, H.; Wagner, R. Cloning and characterization of a virtually full-length HIV type 1 genome from a subtype B’-Thai strain representing the most prevalent B-clade isolate in China. AIDS Res. Hum. Retrovir. 1998, 14, 285288. [Google Scholar] [CrossRef] [PubMed]
- Li, Z.; He, X.; Wang, Z.; Xing, H.; Li, F.; Yang, Y.; Wang, Q.; Takebe, Y.; Shao, Y. Tracing the origin and history of HIV-1 subtype B' epidemic by near full-length genome analyses. AIDS 2012, 26, 877–884. [Google Scholar] [CrossRef] [PubMed]
- Ng, O.T.; Eyzaguirre, L.M.; Carr, J.K.; Chew, K.K.; Lin, L.; Chua, A.; Leo, Y.S.; Redd, A.D.; Quinn, T.C.; Laeyendecker, O. Identification of new CRF51_01B in singapore using full genome analysis of three HIV type 1 isolates. AIDS Res. Hum. Retrovir. 2012, 28, 527–530. [Google Scholar] [CrossRef] [PubMed]
- Wei, H.; Liu, Y.; Feng, Y.; Hsi, J.; Xing, H.; He, X.; Liao, L.; Yutaka, T.; Li, J.; Shao, Y. Genome sequence of a novel HIV-1 circulating recombinant form (CRF57_BC) identified from Yunnan, China. AIDS Res. Hum. Retrovir. 2014, 30, 384–388. [Google Scholar] [CrossRef] [PubMed]
- Feng, Y.; Wei, H.; Hsi, J.; Xing, H.; He, X.; Liao, L.; Ma, Y.; Ning, C.; Wang, N.; Takebe, Y.; et al. Identification of a novel HIV type 1 circulating recombinant form (CRF65_cpx) composed of CRF01_AE and subtypes B and C in Western Yunnan, China. AIDS Res. Hum. Retrovir. 2014, 30, 598–602. [Google Scholar] [CrossRef] [PubMed]
- Zwahlen, M.; Renehan, A.; Egger, M. Meta-analysis in medical research: Potentials and limitations. Urol. Oncol. 2008, 26, 320–329. [Google Scholar] [CrossRef] [PubMed]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| First Author, Publication Year [Reference] | Study Period (Mid-Year) * | Location | Gene Amplification Region | Sample Sizes | The Frequency and Proportion of Different HIV-1 Subtypes | |||||
|---|---|---|---|---|---|---|---|---|---|---|
| CRF01_AE | CRF07_BC | CRF08_BC | B/B‘ | C | Other Subtypes | |||||
| Ye, J.R., 2009 [24] | 2007 | Beijing | gag | 36 | 9 (25.00%) | 14 (38.89%) | 2 (5.56%) | 10 (27.78%) | - | 1 (2.78%) |
| He, H.L., 2012 [25] | 2009 | Guangdong | env, pol | 104 | 68 (65.38%) | 16 (15.38%) | 4 (3.85%) | 6 (5.77%) | - | 10 (9.62%) |
| Wu, X.F., 2015 [26] | 2013 | Zhejiang | gag | 78 | 18 (23.08%) | 39 (50.00%) | 12 (15.38%) | 9 (11.54%) | - | - |
| Fan, W., 2015 [27] | 2006–2014 (2010) | Jiangsu | env, gag | 103 | 54 (52.43%) | 21 (20.39%) | 12 (11.65%) | 14 (13.59%) | - | 2 (1.94%) |
| Yan, Q.L., 2016 [28] | 2014 | Jiangsu | env | 136 | 73 (53.68%) | 25 (18.38%) | 12 (8.82%) | 20 (14.71%) | - | 6 (4.41%) |
| Yang, H.T., 2009 [29] | 2006 | Jiangsu | env, gag | 43 | 9 (20.93%) | 14 (32.56%) | 5 (11.63%) | 10 (23.26%) | 5 (11.63%) | - |
| Li, X.J., 2009 [30] | 1994–2002 (1998) | Yunnan | pol, gag | 15 | 1 (6.67%) | 4 (26.67%) | 6 (40.00%) | 4 (26.67%) | - | - |
| Wu, J., 2016 [31] | 2007–2013 (2010) | Shanghai | pol | 420 | 233 (55.48%) | 89 (21.19%) | 28 (6.67%) | 45 (10.71%) | 8 (1.90%) | 17 (4.05%) |
| Tao, J., 2016 [32] | 2013 | Shanghai | pol | 289 | 157 (54.33%) | 83 (28.72%) | 10 (3.46%) | 21 (7.27%) | 1 (0.35%) | 17 (5.88%) |
| Zhang, X.C., 2015 [33] | 2013 | Shanghai | pol | 31 | 18 (58.06%) | 8 (25.81%) | 2 (6.45%) | 2 (6.45%) | 1 (32.26%) | - |
| Zhao, G.L., 2012 [34] | 1992–2008 (2000) | Guangdong | env | 198 | 137 (69.19%) | 14 (7.07%) | 8 (4.04%) | 34 (17.17%) | 2 (1.01%) | 3 (1.52%) |
| Kong, D.F., 2105 [35] | 2007–2010 (2008–2009) | Guangdong | env, gag | 199 | 118 (59.30%) | 41 (20.60%) | 15 (7.54%) | 17 (8.54%) | 7 (3.52%) | 1 (0.50%) |
| Shi, X.D., 2012 [36] | 2010 | Guangdong | env, gag | 57 | 37 (64.91%) | 7 (12.28%) | 6 (10.53%) | 6 (10.53%) | 1 (1.75%) | - |
| Wang, X., 2012 [37] | 2010 | Tianjin | gag | 30 | 23 (76.67%) | 1 (3.33%) | - | 6 (20.00%) | - | - |
| Zhao, C.Y., 2011 [38] | 2009 | Hebei | env, gag | 60 | 18 (30.00%) | 9 (15.00%) | 4 (6.67%) | 26 (43.33%) | 1 (1.67%) | 2 (3.33%) |
| Li, J.J., 2016 [39] | 2012–2014 (2013) | Yunnan | env | 167 | 32 (19.16%) | 100 (59.88%) | 15 (8.98%) | 6 (35.93%) | 3 (1.80%) | 11 (6.59%) |
| Chen, M., 2012 [40] | 2011 | Yunnan | env, gag | 172 | 43 (25.00%) | 3 (1.74%) | 8 (4.65%) | 5 (2.91%) | 70 (40.70%) | 43 (25.00%) |
| Wang, H., 2016 [41] | 2010–2012 (2011) | Guangxi | pol | 86 | 58 (67.44%) | 18 (20.93%) | 7 (8.14%) | 2 (2.33%) | - | 1 (1.16%) |
| Zheng, M., 2015 [42] | 2013 | Shanghai | pol | 184 | 98 (53.26%) | 59 (32.07%) | 13 (7.07%) | 12 (6.52%) | - | 2 (1.08%) |
| Wu, J., 2012 [43] | 2010 | Shanghai | pol | 14 | 10 (71.43%) | 3 (21.43%) | - | - | 1 (7.14%) | - |
| Bao, Y., 2010 [44] | 2009 | Guangdong | env, gag | 123 | 76 (61.79%) | 35 (28.46%) | 5 (4.07%) | 5 (4.07%) | 2 (1.63%) | - |
| Bao, Y., 2012 [45] | 2010 | Guangdong | env, gag | 142 | 81 (57.04%) | 34 (23.94%) | 9 (6.34%) | 11 (7.75%) | 6 (4.23%) | 1 (0.70%) |
| Pan, X.H., 2007 [46] | 2003–2005 (2004) | Zhejiang | gag | 59 | 23 (38.98%) | 18 (30.51%) | 7 (11.86%) | 10 (16.95%) | - | 1 (1.69%) |
| Qiu, D.H., 2013 [47] | 2011 | Zhejiang | pol | 87 | 45 (51.72%) | 16 (18.39%) | 18 (20.69%) | 7 (8.05%) | 1 (1.15%) | - |
| Ye, J.R., 2013 [48] | 2006–2010 (2008) | Beijing | gag | 62 | 13 (20.97%) | 9 (14.52%) | 4 (6.45%) | 19 (30.65%) | 7 (11.29%) | 10 (16.13%) |
| Jin, M.H., 2014 [49] | 2008–2012 (2010) | Zhejiang | gag | 30 | 6 (20.00%) | 17 (56.67%) | 3 (10.00%) | 4 (13.33%) | - | - |
| Zhang, S., 2010 [50] | 2009 | Zhejiang | pol | 21 | 7 (33.33%) | 5 (23.81%) | 2 (9.52%) | 3 (14.29%) | 4 (19.05%) | - |
| Shen, P., 2015 [51] | 2014 | Guangxi | gag | 62 | 47 (75.81%) | 6 (9.68%) | 8 (12.90%) | - | - | 1 (1.61%) |
| Cheng, H., 2015 [52] | 2012–2013 (2012–2013) | Jiangsu | env | 87 | 38 (43.68%) | 19 (21.84%) | 14 (16.09%) | - | 2 (2.30%) | 14 (16.10%) |
| Han, X.X., 2010 [53] | 2000–2008 (2004) | Liaoning | gag | 70 | 26 (37.14%) | 5 (7.14%) | 3 (4.29%) | 26 (37.14%) | 1 (1.43%) | 9 (12.86%) |
| Chen, S., 2012 [54] | 2009 | Guangdong | pol, env | 85 | 56 (65.88%) | 14 (16.47%) | 4 (4.71%) | 6 (7.06%) | - | 5 (5.88%) |
| Bao, L.L., 2008 [55] | 1996–2005 (2000–2001) | Yunnan | Pol, env | 44 | 27 (61.36%) | - | 15 (34.09%) | - | - | 2 (4.54%) |
| Li, L., 2013 [56] | 2009 | Guangxi | gag, pol | 236 | 189 (80.08%) | 15 (6.36%) | 24 (10.17%) | 4 (1.69%) | - | 4 (1.69%) |
| Deng, Y.Y., 2014 [57] | 2011–2012 (2011–2012) | Fujian | env, gag, pol | 61 | 28 (45.90%) | 21 (34.43%) | 6 (9.84%) | 4 (6.56%) | - | 2 (3.28%) |
| Yang, S.M., 2012 [58] | 2008–2009 (2008–2009) | Yunnan | env, gag, pol | 402 | 117 (29.10%) | 27 (6.72%) | 212 (52.74%) | 7 (1.74%) | 7 (1.74%) | 32 (7.96%) |
| Zhang, J.F., 2013 [59] | 2009 | Zhejiang | gag | 146 | 87 (59.59%) | 22 (15.07%) | 15 (10.27%) | 20 (13.70%) | 1 (0.68%) | 1 (0.68%) |
| Pan, H.X., 2010 [60] | 2008 | Zhejiang | gag | 66 | 26 (39.39%) | 4 (6.06%) | 14 (21.21%) | 16 (24.24%) | 4 (6.06%) | 2 (3.03%) |
| Chen, Y.Y., 2014 [61] | 2009–2011 (2010) | Yunnan | pol | 238 | 94 (39.50%) | 32 (13.44%) | 88 (36.97%) | 3 (12.61%) | - | 21 (8.82%) |
| Li, Y., 2011 [62] | 2007–2008 (2007–2008) | Hubei | gag | 31 | 2 (6.45%) | 1 (3.23%) | - | 28 (90.32%) | - | - |
| Qin, C.H., 2016 [63] | 2011–2013 (2012) | Jiangsu | env, pol | 17 | 10 (58.82%) | 4 (23.53%) | 1 (5.88%) | - | - | 2 (11.76%) |
| Gui, T., 2016 [64] | 2012 | Hebei | gag, pol | 33 | 10 (30.30%) | 2 (6.06%) | 1 (3.03%) | 14 (42.42%) | 4 (12.12%) | 2 (6.06%) |
| Zhong, P., 2003 [65] | 1999–2001 (2000) | Shanghai | env, gag | 16 | 6 (37.50%) | - | 1 (6.25%) | 4 (25.00%) | 2 (12.50%) | 3 (18.75%) |
| Subgroups | CRF01_AE | CRF07_BC | CRF08_BC | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| N | Proportion, % (95% CI) | p #, I2 | p * | N | Proportion, % (95% CI) | p #, I2 | p * | N | Proportion, % (95% CI) | p #, I2 | p * | |
| Study region | <0.01 | <0.01 | <0.01 | |||||||||
| East provinces | 18 | 46.05 (40.44–51.70) | <0.01, 79.9% | 17 | 24.93 (20.06–30.11) | <0.01, 80.1% | 17 | 10.10 (7.44–13.08) | <0.01, 66.8% | |||
| South provinces | 8 | 61.75 (57.18–66.21) | 0.04, 50.5% | 8 | 18.97 (12.95–25.80) | <0.01, 84.2% | 8 | 5.64 (4.21–7.24) | 0.39, 4.3% | |||
| North provinces | 6 | 35.73 (22.50–50.12) | <0.01, 83.4% | 6 | 12.67 (5.58–21.85) | <0.01, 75.5% | 5 | 5.22 (2.64–8.48) | 0.95, 0.0% | |||
| Southwest provinces | 9 | 44.80 (28.17–62.03) | <0.01, 97.5% | 8 | 15.19 (5.13–29.02) | <0.01, 97.2% | 9 | 20.53 (8.51–35.87) | <0.01, 97.4% | |||
| Time period | <0.01 | <0.01 | 0.24 | |||||||||
| –2006 | 7 | 39.18 (22.58–57.09) | <0.01, 91.5% | 5 | 18.25 (7.16–32.65) | <0.01, 88.0% | 7 | 12.77 (4.92–23.17) | <0.01, 84.4% | |||
| 2007–2009 | 13 | 44.48 (32.00–57.31) | <0.01, 95.9% | 13 | 14.64 (9.98–19.98) | <0.01, 85.3% | 12 | 10.43 (3.03–21.16) | <0.01, 96.8% | |||
| 2010–2012 | 13 | 50.23 (41.35–59.10) | <0.01, 89.0% | 13 | 17.45 (11.09–24.81) | <0.01, 89.1% | 11 | 10.34 (4.71–17.63) | <0.01, 92.1% | |||
| 2013–2014 | 9 | 47.55 (36.16–59.07) | <0.01, 93.1% | 9 | 28.96 (19.37–39.75) | <0.01, 92.7% | 9 | 9.32 (6.29–12.82) | <0.01, 68.6% | |||
| Amplified gene region | 0.08 | <0.01 | 0.55 | |||||||||
| Only one | 24 | 45.16 (38.14–52.28) | <0.01, 91.2% | 24 | 21.14 (15.58–27.26) | <0.01, 91.8% | 21 | 10.39 (6.94–14.40) | <0.01, 88.2% | |||
| Two or more | 18 | 47.78 (37.70–57.96) | <0.01, 94.5% | 16 | 16.23 (10.97–22.24) | <0.01, 89.5% | 18 | 10.95 (4.63-19.25) | <0.01, 95.7% | |||
| Subgroups | B/B’ | C | ||||||||||
| N | Proportion, % (95% CI) | p # , I2 | p * | N | Proportion, % (95% CI) | p # , I2 | p * | |||||
| Study region | <0.01 | <0.01 | ||||||||||
| East provinces | 15 | 12.09 (9.47–14.96) | <0.01, 57.2% | 11 | 2.83 (0.86–5.59) | <0.01, 71.4% | ||||||
| South provinces | 8 | 8.28 (5.50–11.52) | <0.01, 62.7% | 5 | 2.28 (1.23–3.58) | 0.32, 13.7% | ||||||
| North provinces | 6 | 34.48 (29.02–40.14) | 0.21, 29.0% | 4 | 5.26 (0.87–12.27) | 0.02, 69.4% | ||||||
| Southwest provinces | 7 | 2.07 (0.85–3.69) | 0.03, 56.2% | 3 | 9.95 (0.00–38.04) | <0.01, 98.8% | ||||||
| Time period | <0.01 | <0.01 | ||||||||||
| –2006 | 6 | 23.10 (15.85–31.18) | 0.03, 58.8% | 4 | 3.92 (0.08–11.24) | <0.01, 75.9% | ||||||
| 2007–2009 | 13 | 16.98 (8.56–27.39) | <0.01, 95.6% | 8 | 3.29 (1.27–6.02) | <0.01, 70.6% | ||||||
| 2010–2012 | 11 | 8.62 (4.58–13.65) | <0.01, 86.1% | 7 | 7.27 (0.28–20.34) | <0.01, 96.3% | ||||||
| 2013–2014 | 7 | 8.52 (5.55–12.03) | <0.01, 65.7% | 4 | 0.75 (0.09–1.82) | 0.16, 41.1% | ||||||
| Amplified gene region | <0.01 | <0.01 | ||||||||||
| Only one | 21 | 15.19 (10.15–20.99) | <0.01, 92.1% | 13 | 2.05 (0.77–3.75) | <0.01, 65.1% | ||||||
| Two or more | 16 | 10.75 (6.24–16.19) | <0.01, 90.2% | 10 | 6.83 (1.42–15.20) | <0.01, 94.8% | ||||||
© 2017 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Xiao, P.; Li, J.; Fu, G.; Zhou, Y.; Huan, X.; Yang, H. Geographic Distribution and Temporal Trends of HIV-1 Subtypes through Heterosexual Transmission in China: A Systematic Review and Meta-Analysis. Int. J. Environ. Res. Public Health 2017, 14, 830. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph14070830
Xiao P, Li J, Fu G, Zhou Y, Huan X, Yang H. Geographic Distribution and Temporal Trends of HIV-1 Subtypes through Heterosexual Transmission in China: A Systematic Review and Meta-Analysis. International Journal of Environmental Research and Public Health. 2017; 14(7):830. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph14070830
Chicago/Turabian StyleXiao, Peipei, Jianjun Li, Gengfeng Fu, Ying Zhou, Xiping Huan, and Haitao Yang. 2017. "Geographic Distribution and Temporal Trends of HIV-1 Subtypes through Heterosexual Transmission in China: A Systematic Review and Meta-Analysis" International Journal of Environmental Research and Public Health 14, no. 7: 830. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph14070830