Lifestyle Interventions for People with, and at Risk of Type 2 Diabetes in Polynesian Communities: A Systematic Review and Meta-Analysis




Abstract
:1. Introduction
2. Research Design and Methods
2.1. Study Eligibility
2.2. Search Strategy
2.3. Data Extraction and Assessment of Risk of Bias
2.4. Data Synthesis and Statistical Analysis
3. Results
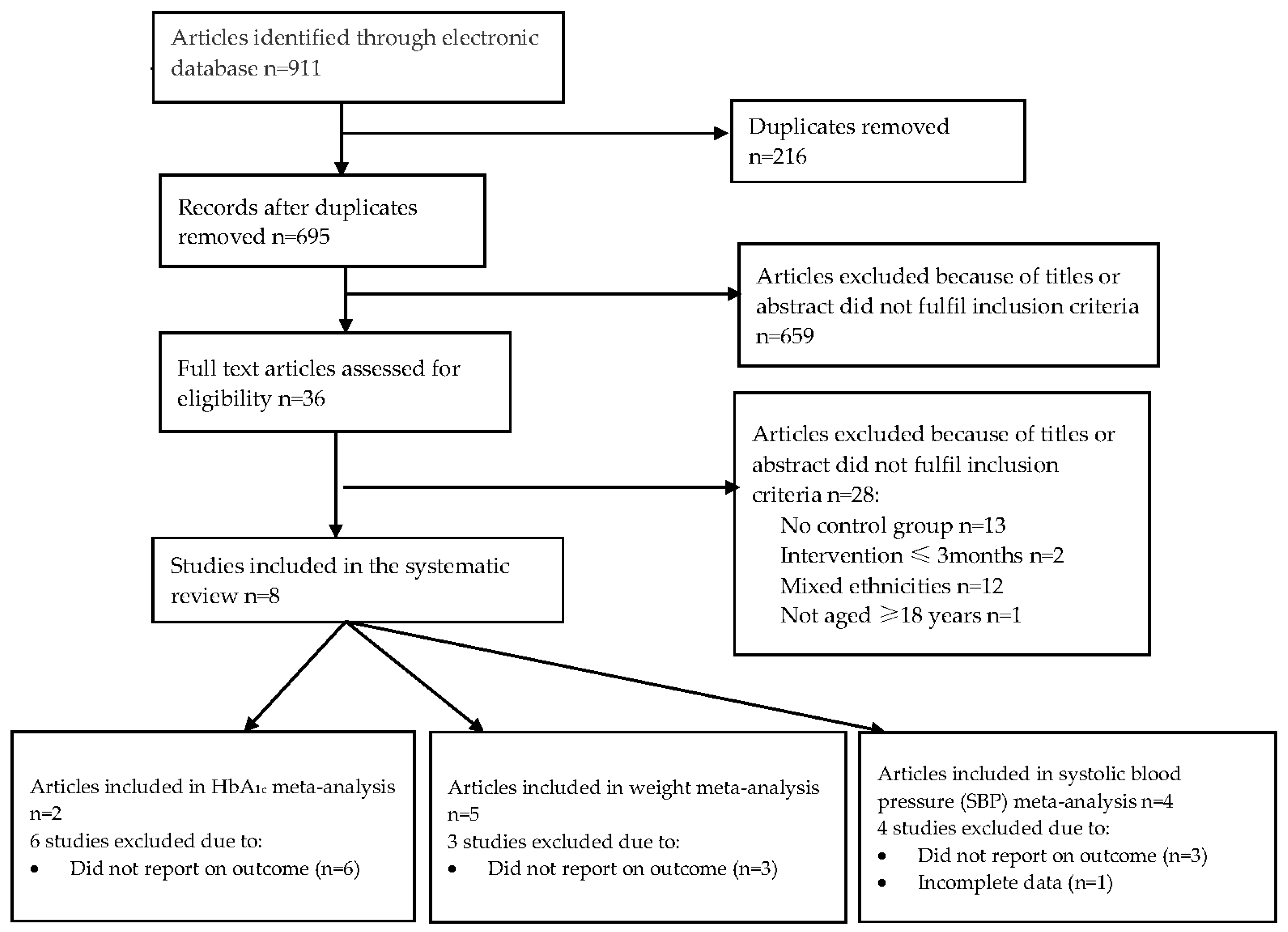
3.1. Identification of Studies
3.2. Participants and Study Characteristics
3.3. Risk of Bias of the Included Studies
3.4. Impacts of Interventions
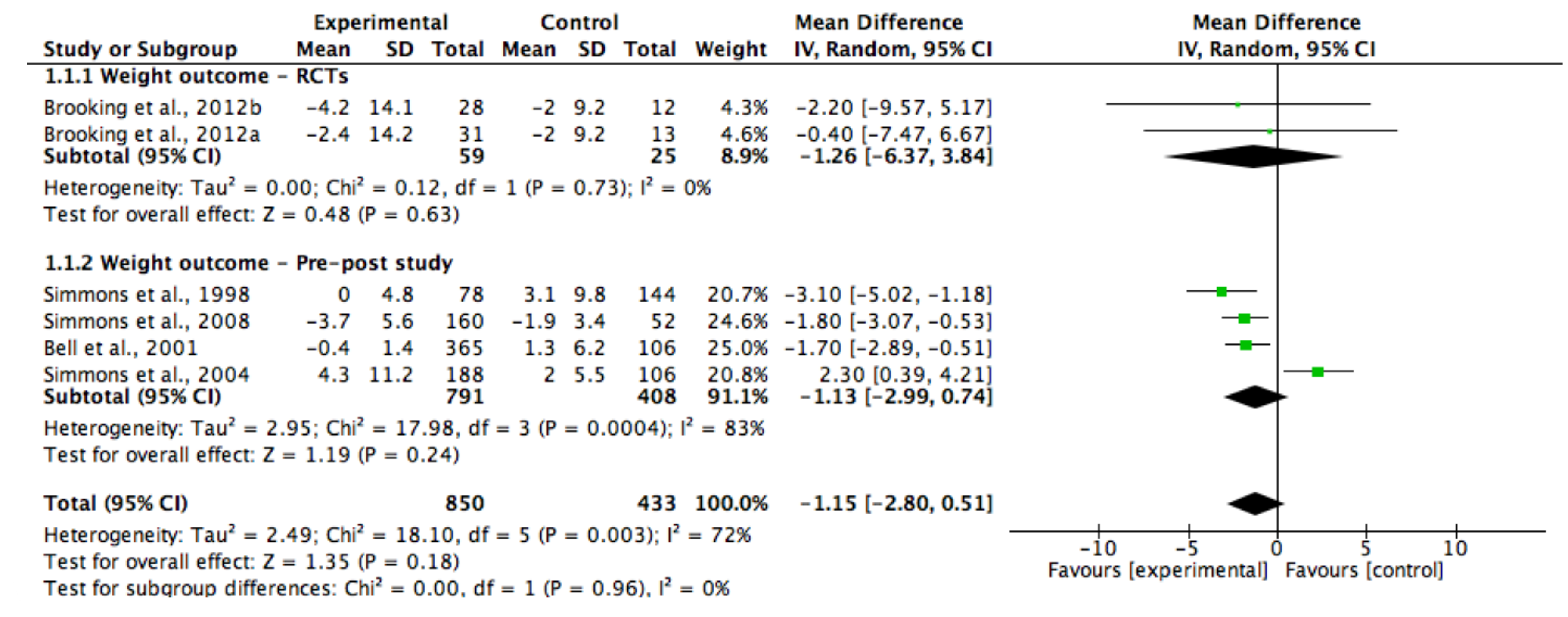
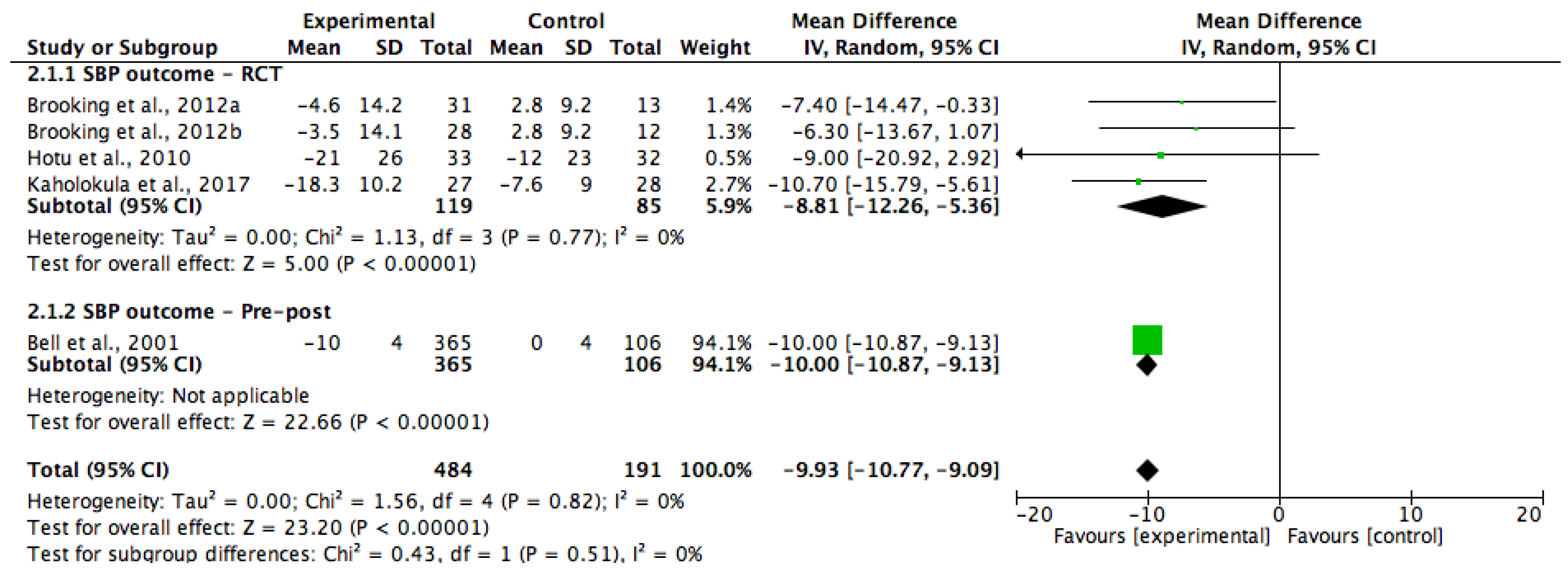
3.4.1. Meta-Analyses Findings
3.4.2. Narrative FindingsBody Mass Index (BMI)
Body Mass Index (BMI)
Waist Circumference
4. Discussion
Limitations and Recommendations for Future Practice
5. Conclusions
Supplementary Materials
Author Contributions
Acknowledgments
Conflicts of Interest
References
- Nanditha, A.; Ma, R.C.; Ramachandran, A.; Snehalatha, C.; Chan, J.N.; Chia, K.S.; Shaw, J.E. Diabetes in Asia and the Pacific: Implications for the global epidemic. Diabetes Care 2016, 39, 472–485. [Google Scholar] [CrossRef] [PubMed]
- Hawley, N.L.; McGarvey, S.T. Obesity and Diabetes in Pacific Islanders: The Current Burden and the Need for Urgent Action. Curr. Diabetes Rep. 2015, 15, 29. [Google Scholar] [CrossRef] [PubMed]
- Ing, C.T.; Zhang, G.; Dillard, A.; Yoshimura, S.R.; Hughes, C.; Palakiko, D.-M.; Kehauoha, BP.; Sinclair, K.A.; Kaholokula, J.K. Social Support Groups in the Maintenance of Glycemic Control after Community-Based Intervention. J. Diabetes Res. 2016. [Google Scholar] [CrossRef] [PubMed]
- Sinclair, K.A.; Makahi, E.K.; Shea-Solatorio, C.; Yoshimura, S.R.; Townsend, C.K.; Kaholokula, J.K. Outcomes from a Diabetes Self-management Intervention for Native Hawaiians and Pacific People: Partners in Care. Ann. Behav. Med. 2013, 45, 24–32. [Google Scholar] [CrossRef] [PubMed]
- Mau, M.K.; Kaholokula, J.K.; West, M.R.; Leake, A.; Efird, J.M.; Rose, C.; Palakiko, D.M.; Yoshimura, S.; Kekauoha, P.B.; Gomes, H. Translating diabetes prevention into native Hawaiian and Pacific Islander communities: The PILI ‘Ohana Pilot project. Prog. Community Health Partnersh. 2010, 4, 7–16. [Google Scholar] [CrossRef] [PubMed]
- Sukala, W.R.; Page, R.; Cheema, B.S. Targeting the type 2 diabetes epidemic in Polynesia: Historical perspective and rationale for exercise intervention trials. Ethn. Dis. 2012, 22, 123–128. [Google Scholar] [PubMed]
- Furubayashi, J.L.; Look, M.A. Type 2 diabetes in Native Hawaiians and Pacific Islanders in Hawaii. Pac. Health Surveill. Resp. 2005, 12, 103–110. [Google Scholar]
- McAuley, K.A.; Murphy, E.; McLay, R.T.; Chisholm, A.; Story, G.; Mann, J.I.; Thomson, R.; Bell, D.; Williams, S.M.; Goulding, A.; et al. Implementation of a successful lifestyle intervention programme for New Zealand Maori to reduce the risk of type 2 diabetes and cardio-vascular disease. Asia Pac. J. Clin. Nutr. 2003, 12, 423–436. [Google Scholar] [PubMed]
- Davis, J.; Busch, J.; Hammatt, Z.; Novotny, R.; Harrigan, R.; Grandinetti, A.; David, E. The relationship between ethnicity and obesity in Asian and Pacific Islander populations: A literature review. Ethn. Dis. 2004, 14, 111–118. [Google Scholar] [PubMed]
- Chan, J.C.; Cho, N.H.; Tajima, N.; Shaw, J. Diabetes in the Western Pacific Region-Past, Present and Future. Diabetes Res. Clin. Pract. 2014, 103, 244–255. [Google Scholar] [CrossRef] [PubMed]
- Williams, E.; Harris, N. Understanding the nutrition information needs of migrant communities: The needs of African and Pacific Islander communities of Logan, Queensland. Public Health Nutr. 2010, 14, 989–994. [Google Scholar] [CrossRef] [PubMed]
- Simmons, D.; Voyle, J.A.; Fout, F.; Feot, S.; Leakehet, L. Tale of two churches: Differential impact of a church-based diabetes control programme among Pacific Islands people in New Zealand. Diabet. Med. 2004, 21, 122–128. [Google Scholar] [CrossRef] [PubMed]
- Kaholokula, J.K.; Townsend, C.M.; Ige, A.; Sinclair, K.A.; Mau, M.K.; Leake, A.; Palakiko, D.-M.; Yoshimura, S.R.; Kekauoha, P.; Hughes, C. Socio-demographic, behavioral, and biological variables related to weight loss in native Hawaiins and other Pacific Islanders. Obesity 2012, 21, 196–203. [Google Scholar] [CrossRef] [PubMed]
- Rush, E.; Plank, L.; Chandu, V.; Laulu, M.; Simmons, D. Body size, body composition, and fat distribution: A comparison of young New Zealand men of European, Pacific Island, and Asian Indian ethnicities. N. Z. Med. J. 2004, 117, 1–9. [Google Scholar]
- Guariguata, L.; Whiting, D.; Hambleton, I.; Beagley, J.; Linnenkamp, U.; Shaw, J.E. Global estimates of diabetes prevalence for 2013 and projections for 2035. Diabetes Res. Clin. Pract. 2014, 103, 137–149. [Google Scholar] [CrossRef] [PubMed]
- Zimmet, P. The burden of type 2 diabetes: Are we doing enough? Diabetes Metab. 2003, 29, S9–S18. [Google Scholar] [CrossRef]
- Department of Health and Ageing. Australian National Diabetes Strategy 2016–2020; DOH Publ. No. 11229; Australian Government, 2015. Available online: http://www.health.gov.au/internet/main/publishing.nsf/content/3AF935DA210DA043CA257EFB000D0C03/$File/Australian%20National%20Diabetes%20Strategy%202016-2020.pdf (accessed on 11 June 2017).
- Lee, C.M.; Colagiuri, R.; Magliano, D.J.; Cameron, A.J.; Shaw, J.; Zimmet, P.; Colagiuri, S. The cost of diabetes in adults in Australia. Diabetes Res. Clin. Pract. 2013, 99, 385–390. [Google Scholar] [CrossRef] [PubMed]
- Dunkley, A.J.; Bodicoat, D.H.; Greaves, C.J.; Russell, C.; Yates, T.; Davies, M.J.; Khunti, K. Diabetes Prevention in the Real World: Effectiveness of pragmatic lifestyle interventions for the prevention of Type 2 Diabetes and the impact of adherence to guideline recommendations. A systematic review and meta-analysis. Diabetes Care 2014, 37, 922–933. [Google Scholar] [CrossRef] [PubMed]
- Liburd, L.C.; Vinicor, F. Rethinking diabetes prevention and control in racial and ethnic communities. J. Public Health Manag. Pract. 2003, 9, S74–S79. [Google Scholar] [CrossRef]
- Hall, D.L.; Lattie, E.G.; McCalla, J.R.; Saab, P.G. Translation of the Diabetes Prevention Program to Ethnic Communities in the United States. J. Immigr. Minor. Health 2016, 18, 479–489. [Google Scholar] [CrossRef] [PubMed]
- Hamman, R.F.; Wing, R.R.; Edelstein, S.L.; Lachin, J.M.; Bray, G.A.; Delahanty, M.S.; Hoskin, M.; Kriska, A.M.; Mayer-Davis, E.J.; Pi-Sunyer, X.; et al. Effect of weight loss with lifestyle intervention on risk of diabetes. Diabetes Care 2006, 29, 2102–2107. [Google Scholar] [CrossRef] [PubMed]
- Knowler, W.C.; Barrett-Connor, E.; Fowler, S.E.; Hamman, R.F.; Lachin, J.M.; Walker, E.A. Diabetes Prevention Program Research Group. Reduction in the incidence of type 2 diabetes with lifestyle interventions or metformin. N. Engl. J. Med. 2002, 346, 393–403. [Google Scholar] [CrossRef] [PubMed]
- Tuomilehto, J.; Lindsrtom, J.; Eriksson, J.G.; Valle, T.T.; Hamalainem, H.; IIanne-Parikka, P.; Keinanem-Kiukaanniemi, S.; Laakso, M.; Lourheranta, A.; Rastas, M.; et al. Prevention of type 2 diabetes mellitus by changes in lifestyle among subjects with impaired glucose tolerance. N. Engl. J. Med. 2001, 344, 1343–1350. [Google Scholar] [CrossRef] [PubMed]
- Sukala, W.R.; Page, R.A.; Rowlands, D.S.; Lys, I.; Krebs, J.D.; Leikis, M.J.; Cheema, B.S. Exercise intervention in New Zealand Polynesian peoples with type 2 diabetes: Cultural considerations and clinical trial recommendations. Australas. Med. J. 2012, 5, 429–435. [Google Scholar] [CrossRef] [PubMed]
- Petticrew, M.; Roberts, H. Systematic Reviews in the Social Sciences: A Practical Guide; Wiley-Blackwell: Oxford, UK, 2006; pp. 38–43. [Google Scholar]
- Higgins, J.P.; Green, S. Cochrane Handbook for Systematic Reviews of Interventions Version 5.1.0; The Cochrane Collaboration. 2011. Available online: http://handbook.cochrane.org (accessed on 21 May 2017).
- Sterne, J.A.; Higgins, J.P.; Barney, R.; Jelena, S. The Risk of Bias in Non-Randomised Studies-of Interventions (ROBINS-1) Assessment Tool. 2016. Available online: http://www.riskofbias.info (accessed on 21 May 2017).
- Kaholokula, J.K.; Look, M.; Mabellos, T.; Zhang, G.; de Silva, M.; Yoshimura, S.; Solatorio, C.; Wills, T.; Seto, T.B.; Sinclair, K.A. Cultural dance program improves hypertension management for native Hawaiians and Pacific Islanders: A pilot randomised trial. J. Racial Ethn. Health Dispar. 2017, 4, 35–46. [Google Scholar] [CrossRef] [PubMed]
- Bell, A.C.; Swinburn, B.A.; Amosa, H.; Amosa, H.; Scragg, R.K. A nutrition and exercise program for controlling weight in Samoan communities in New Zealand. Int. J. Obes. Relat. Metab. Disord. 2001, 25, 920–927. [Google Scholar] [CrossRef] [PubMed]
- Depue, J.D.; Dunsiger, S.; Seiden, A.D.; Blume, J.; Rosen, R.K.; Golstein, M.G.; Nu’usolia, O.; Tuitele, J.; McGarvey, S.T. Nurse-community health worker team improves diabetes care in American Samoa: Results of a randomized controlled trial. Diabetes Care 2013, 36, 1947–1953. [Google Scholar] [CrossRef] [PubMed]
- Simmons, D.; Rush, E.; Crook, N. Development and piloting of a community health worker-based intervention for the prevention of diabetes among New Zealand Maori in Te Wai o Rona: Diabetes Prevention Strategy. Public Health Nutr. 2008, 11, 1318–1325. [Google Scholar] [CrossRef] [PubMed]
- Simmons, D.; Fleming, C.; Voyle, J.; Fou, F.; Feo, S.; Gatland, B. A pilot urban church-based programme to reduce risk factors for diabetes among Western Samoans in New Zealand. Diabetic Med. 1998, 15, 136–142. [Google Scholar] [CrossRef]
- Hotu, C.; Bagg, W.; Collins, J.; Harwood, L.; Whalley, G.; Doughty, R.; Gamble, G.; Braatvedt, G. A community-based model of care improves blood pressure control and delays progression of proteinuria, left ventricular hypertrophy and diastolic dysfunction in Maori and Pacific patients with type 2 diabetes and chronic kidney disease: A randomized controlled trial. Nephrol. Dial. Transplant. 2010, 25, 3260–3266. [Google Scholar] [CrossRef] [PubMed]
- Brooking, L.A.; Williams, S.M.; Mann, J.I. Effects of macronutrient composition of the diet on body fat in indigenous people at high risk of type 2 diabetes. Diabetes Res. Clin. Pract. 2012, 96, 40–46. [Google Scholar] [CrossRef] [PubMed]
- Umpierre, D.; Ribeiro, P.A.; Kramer, C.K.; Leitao, C.B.; Zucatti, A.T.; Azevedo, M.J.; Gross, J.L.; Ribeiro, J.P.; Schaan, B.D. Physical activity advice only structured exercise training and association with HbA1c levels in Type 2 Diabetes. JAMA 2011, 305, 1790–1798. [Google Scholar] [CrossRef] [PubMed]
- Bennette, C.; Vickers, A. Against quantiles: Categorisation of continuous variables in epidemiologic research, and its discontents. Med. Res. Methodol. 2012, 12, 1–5. [Google Scholar] [CrossRef] [PubMed]
- Knowler, W.C.; Barrett-Connor, E.; Fowler, S.E.; Hamman, R.F.; Lachin, J.M.; Walker, E.A. The Diabetes Prevention Program (DPP) Research Group: Description of lifestyle intervention. Diabetes Care 2002, 25, 2165–2171. [Google Scholar] [CrossRef]
- Li, G.; Zhang, P.; Wang, J. The long-term effect of lifestyle interventions to prevent diabetes in the China Da Qing Diabetes Prevention Study: A 20-year follow-up study. Lancet 2008, 371, 1783–1789. [Google Scholar] [CrossRef]
- Dickinson, H.O.; Mason, J.M.; Nicolson, D.J.; Campbell, F.; Beyer, F.; Cook, J.V.; Williams, B.; Ford, G.A. Lifestyle interventions to reduce raised blood pressure: A systematic review of randomized controlled trials. J. Hypertens. 2006, 24, 215–233. [Google Scholar] [CrossRef] [PubMed]
- Wing, R.R.; Bahnson, J.L.; Bray, G.A.; Clark, J.M.; Coday, M.; Egan, C.; Espeland, M.A.; Foreyt, J.P.; Gregg, E.W.; Goldman, V.; et al. Long term effects of a lifestyle intervention on weight and cardiovascular risk factors in individuals with type 2 diabetes: Four year results of the Look AHEAD Trial. Arch. Intern. Med. 2010, 170, 1566–1575. [Google Scholar] [CrossRef] [PubMed]
- Svetkey, L.P.; Harsha, D.W.; Vollmer, W.M.; Stevens, V.J.; Obarzanek, W.; Elmer, P.J.; Lin, P.; Champagne, C.; Simons-Morton, D.G.; Aickin, M.; et al. Premier: A Clinical Trial of Comprehensive Lifestyle Modification for Blood Pressure Control: Rationale, Design and Baseline Characteristics. Ann. Epidemiol. 2003, 13, 462–471. [Google Scholar] [CrossRef]
- Handley, M.A.; Schillinger, D.; Shiboski, S. Quasi-Experimental designs in practice-based research settings: Design and implemention considerations. J. Am. Board Fam. Med. 2011, 24, 589–596. [Google Scholar] [CrossRef] [PubMed]
- Verheijden, M.W.; Kok, F.J. Public health impact of community-based nutrition and lifestyle interventions. Eur. J. Clin. Nutr. 2005, 59, S66–S76. [Google Scholar] [CrossRef] [PubMed]
- Mowbray, C.T.; Holter, M.C.; Teague, G.B.; Bybee, D. Fidelity criteria: Development, measurement and variation. Am. J. Eval. 2003, 24, 315–340. [Google Scholar] [CrossRef]
- Ali, M.K.; Echouffo-Tcheugui, J.B.; Williamson, D.F. How effective were lifestyle interventions in real-world settings that were modelled on the diabetes prevention program? Health Aff. 2012, 31, 67–75. [Google Scholar] [CrossRef] [PubMed]
- Tang, T.S.; Funnell, M.; Sinco, B.; Piatt, G.; Palmisano, G.; Spencer, M.S.; Kieffer, E.C.; Heisler, M. Comparative effectiveness of peer leaders and community helat workers in Diabetes self-management support: Results of a randomised controlled trial. Diabetes Care 2014, 37, 1525–1534. [Google Scholar] [CrossRef] [PubMed]
- Simmons, D. Peer support: Time to tap the (largely) untapped. Pract. Diabetes 2013, 30, 246–250. [Google Scholar] [CrossRef]
- Heisler, M.; Vijan, S.; Makki, F.; Piette, J.D. Diabetes control with reciprocal peer support versus nurse care management: A randomised trial. Ann. Intern. Med. 2010, 153, 507–515. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Studies on Diabetes Prevention | |||||||
|---|---|---|---|---|---|---|---|
| Author, (Year), Country | Aim | Study Design | Duration | Study Population | Study Population Age (M ± SD); Gender (%), n = Study Participants | Intervention and Control Groups | Outcome Measures |
| Brooking et al. (2012) New Zealand [35] | To determine the effects of a fibre rich carbohydrate, fat reduction, or a high protein diet on body fat in Maori that are at risk of diabetes. | RCT | 24 weeks | New Zealand Maori | Intervention (HCHF): 45.8 ± 12.75; Male (26%); n = 31. Intervention (HP): 38.9 ± 10.50; Male (29%); n = 28 Control: 35.9 ± 10.9; Male 36%; n = 25. | Intervention: Participants were randomised into two interventions groups (fibre rich carbohydrate and fat reduction [HCHF] group, and a high protein diet [HP] group). The participants received prescriptive dietary advice, such as meal options, and portion sizes specific to the allocated diet group, with cooking demonstrations and food shopping tours provided. The diet intervention was based on the recommendations of the European Association for the Study of Diabetes (EASD) and American Diabetes Association (ADA). Control group: continued with their usual diet and received dietary advice at end of the study. | Weight (kgs); waist circumference (cms); total fat mass (kg). |
| Kaholokula et al. (2017) USA (Hawaii) [29] | To assess the feasibility and efficacy of Hula, a traditional Hawaiian dance, in reducing blood pressure in the Native Hawaiians and Pacific Islanders (NHPI) community. | RCT | 12 weeks | Native Hawaiians and Pacific Islander | Intervention:55 ± 10; Female (93%); n = 27 Control: 55 ± 12; Female (79%); n = 28 | Intervention: participants received 3 h of hypertension education and two 60-min classes of hula instruction and training per week, over 12 weeks. Waitlist (control) group: participants did not receive any intervention materials and no contact was made during the time they were on the waitlist. | Blood pressure (mmHg); physical functioning (assessed by the 6-min walk test); health related quality of life (HRQL). |
| Bell et al. (2001) New Zealand (Auckland) [30] | To evaluate the impact of a 1-year nutrition and exercise intervention program in promoting weight loss in three Samoan church communities. | Quasi-experimental (pre-post) | 12 months | Samoans | Intervention: 43.9 ± 13.7; Female (60%); n = 365 Control: 39.1 ± 13.2; Female (60%); n = 106. | Intervention: participants received informal nutrition education sessions 1 h long (a total of 31 sessions held) and aerobic sessions were incorporated into regular church activities (total of 170 aerobic sessions were conducted) delivered initially by trained instructors from Pacific Islands Heartbeat (PIHB) program. Control: no details provided on the control group | Weight (kg); BMI (kg/m2); blood pressure (mmHg); diet and physical activity (questionnaire). |
| Simmons et al. (1998) New Zealand (South Auckland) [33] | To investigate the impact of a 2-year diabetes awareness/exercise lifestyle programme among a Samoan church congregation at risk of diabetes. | Pre-post | 2 years | Samoans | Intervention 37 ± 16; Female (66%); n = 67 Control: 35 ± 17; Female (61%); n = 115. | Intervention: The Samoan community’s diabetes educator presented four diabetes awareness sessions (video and flipcharts), which were later followed by exercise groups consisting of aerobics, walking, sports, and sitting exercises, which were delivered by a Samoan health worker that was trained as an aerobics instructor, which were held weekly for the first year and twice per week in the second year. The participants attended practical sessions on cooking demonstrations. Control: the usual care, received the intervention upon study completion. | Weight (kg).Waist circumference (cms); diabetes knowledge (validated questionnaire) |
| Simmons et al. (2004) New Zealand (South Auckland) [12] | To assess the impact of a 2-year diabetes risk reduction programme on weight and exercise in a Samoan and Tongan church congregation. | Pre-post | 2 years | Tongans | Intervention group: 33 ± 13; Female (52%); n = 167. Control: 34 ± 13; Female (49%); n = 86. | Intervention: The intervention church used leaflets and videos that were translated to Tongan. The messages that were delivered covered topics on diabetes and its symptoms and complications; nutrition, which included cooking demonstrations; and exercises sessions that were delivered by a trained aerobics instructor. Control: the usual care, received intervention on study completion. | weight (kg); waist circumference (cms). |
| Simmons et al. (2008) New Zealand [32] | To evaluate whether the intensive lifestyle interventions were effective in preventing or delaying type 2 diabetes among Maori community. | Pre-post | 6 months | New Zealand Maori | Intervention:47 ± 13; Male (34.4%); n = 160. Control: 50 (13); Male (40.4%); n = 52. | Intervention: participants received the intervention based upon 12 key diet and physical activity messages (adapted from the Maori diet and physical activity behaviours) and were delivered by a trained Maori Community Health Worker (MCHW). Control: the usual care, did not receive intervention on study completion. | Weight (kg). |
| Studies on Diabetes Management | |||||||
| Author, (Year), Country | Aim | Study Design | Duration | Study Population | Age (M ± SD) | Intervention and Control Groups | Outcome Measures |
| DePue et al. (2013) USA [31] | To evaluate the effectiveness of a primary care nurse and community health worker team in improving diabetes management among American Samoa. | RCT | 12 months | American Samoa | Intervention: 55 ± 12.5; Female (57%); n = 104. Control: 54 ± 12.9; Female (65%); n = 164. | Intervention: Participants were seen weekly, in a group meeting held by the nurse care manager and a CHW, if considered to be high risk participants, moderate risk and low risk participants were seen by a CHW monthly and every 3 months, respectively (the length of the meetings was not specified). The meetings were based on diabetes management covering eight topics of healthy eating, physical activity, medication use, healthy coping, monitoring and understanding of blood glucose, and blood pressure measurements. Blood sugar was measured on each encounter. Received a copy of “Four steps to control diabetes for life”. Usual care (control) group: To receive intervention after 12 months. Received one phone call at 6 months to promote study retention rates. Received a copy of “Four steps to control diabetes for life”, no further contact was made until the end of the intervention. | HbA1c (%); BMI (kg/m2); waist circumference (cms); blood pressure (mmHg). |
| Hotu et al. (2010) New Zealand (Auckland) [34] | To determine whether the community health-care assistants are more effective in achieving and maintaining BP targets in Maori and Pacific patients. | RCT | 12 months | Maori | Intervention:63 ± 6.6; Female (45%); n = 33. Control: 60 ± 7.1; Female (47%) n = 32. | Intervention: Ongoing monthly education on the importance of medication compliance, dietary modification, exercise, and smoking cessation. Participants were visited monthly by nurse/ health care assistant. Anti-hypertensives were adjusted regularly by a physician using a stepwise protocol. Received a diabetes education package at the start of the intervention Control: no alterations were made in their lifestyle or medication. | SBP (mmHg);HbA1c (%); 24-h urine protein excretion (g/day); total cholesterol (mmol/L). |
© 2018 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ndwiga, D.W.; MacMillan, F.; McBride, K.A.; Simmons, D. Lifestyle Interventions for People with, and at Risk of Type 2 Diabetes in Polynesian Communities: A Systematic Review and Meta-Analysis. Int. J. Environ. Res. Public Health 2018, 15, 882. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph15050882
Ndwiga DW, MacMillan F, McBride KA, Simmons D. Lifestyle Interventions for People with, and at Risk of Type 2 Diabetes in Polynesian Communities: A Systematic Review and Meta-Analysis. International Journal of Environmental Research and Public Health. 2018; 15(5):882. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph15050882
Chicago/Turabian StyleNdwiga, Dorothy W., Freya MacMillan, Kate A. McBride, and David Simmons. 2018. "Lifestyle Interventions for People with, and at Risk of Type 2 Diabetes in Polynesian Communities: A Systematic Review and Meta-Analysis" International Journal of Environmental Research and Public Health 15, no. 5: 882. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph15050882