Assessing Spatial Accessibility to Medical Resources at the Community Level in Shenzhen, China

 ,
,
Abstract
:1. Introduction
2. Materials and Methods
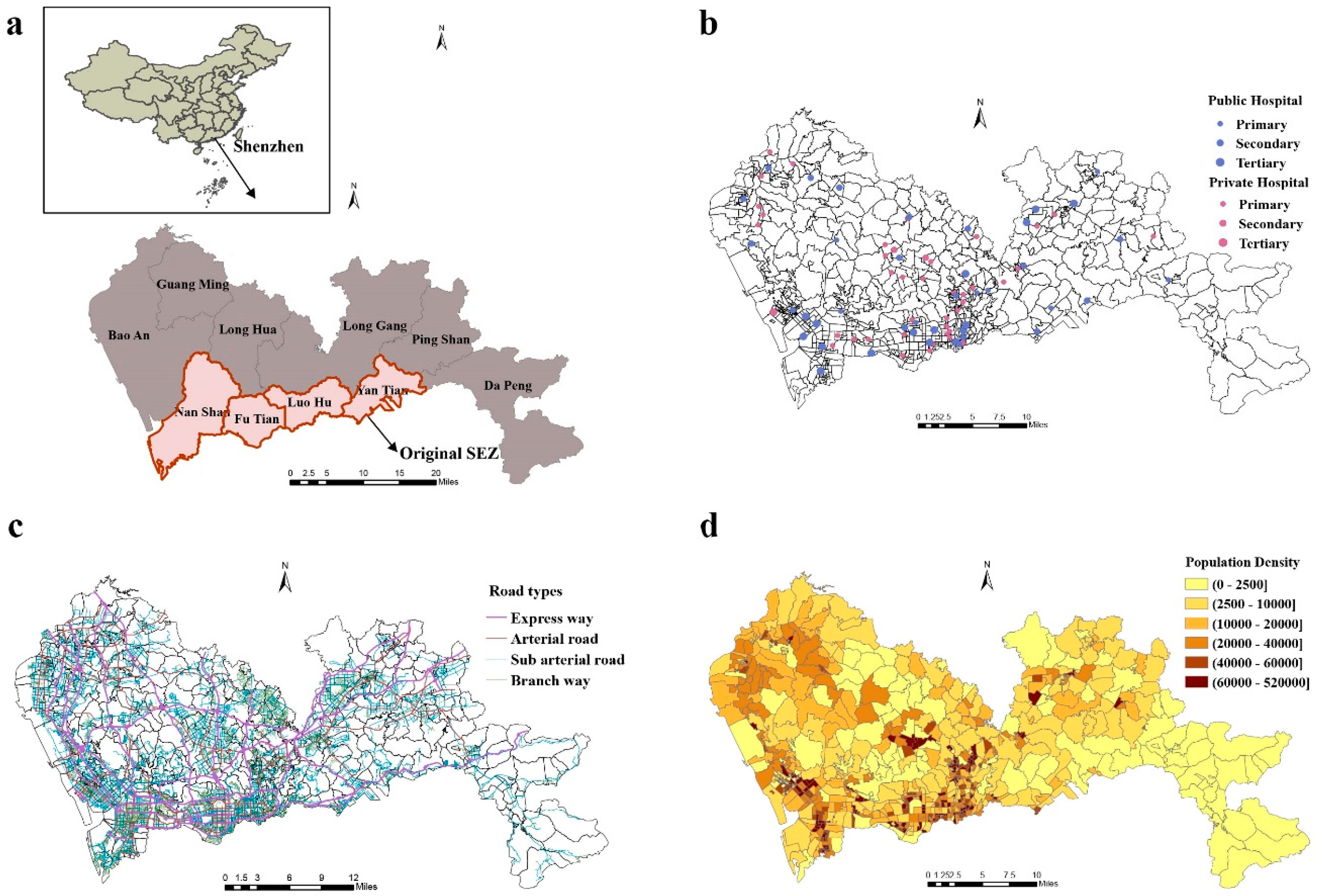
2.1. Study Area and Data Sources
2.2. Study Design
2.2.1. Measuring Travel Time Cost to General Hospitals
2.2.2. Measuring Inequality Using Gini Coefficients and Lorenz Curves
2.2.3. Assessing Spatial Accessibility Using the E2SFCA Method
3. Results
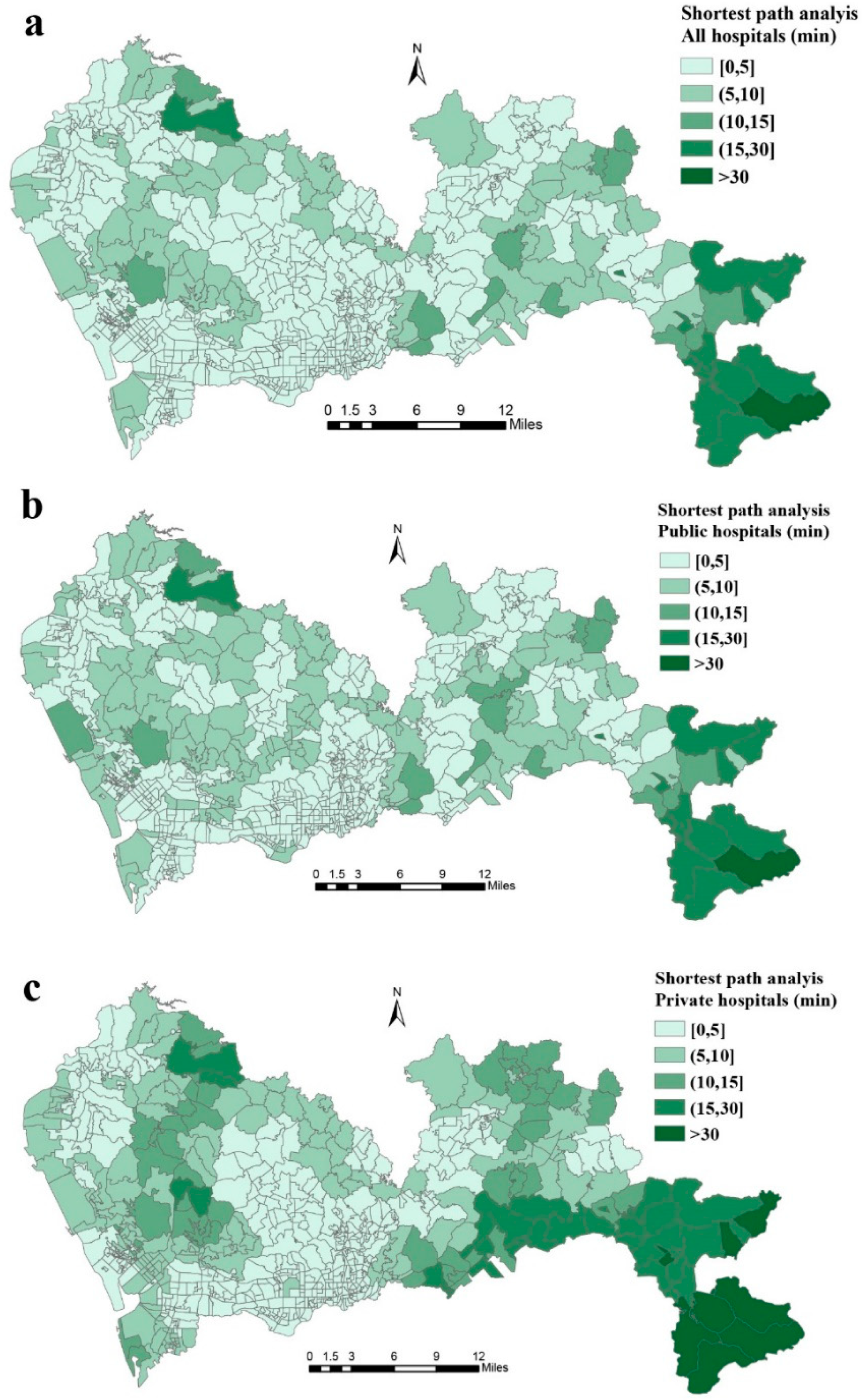
3.1. Shortest Path Analysis
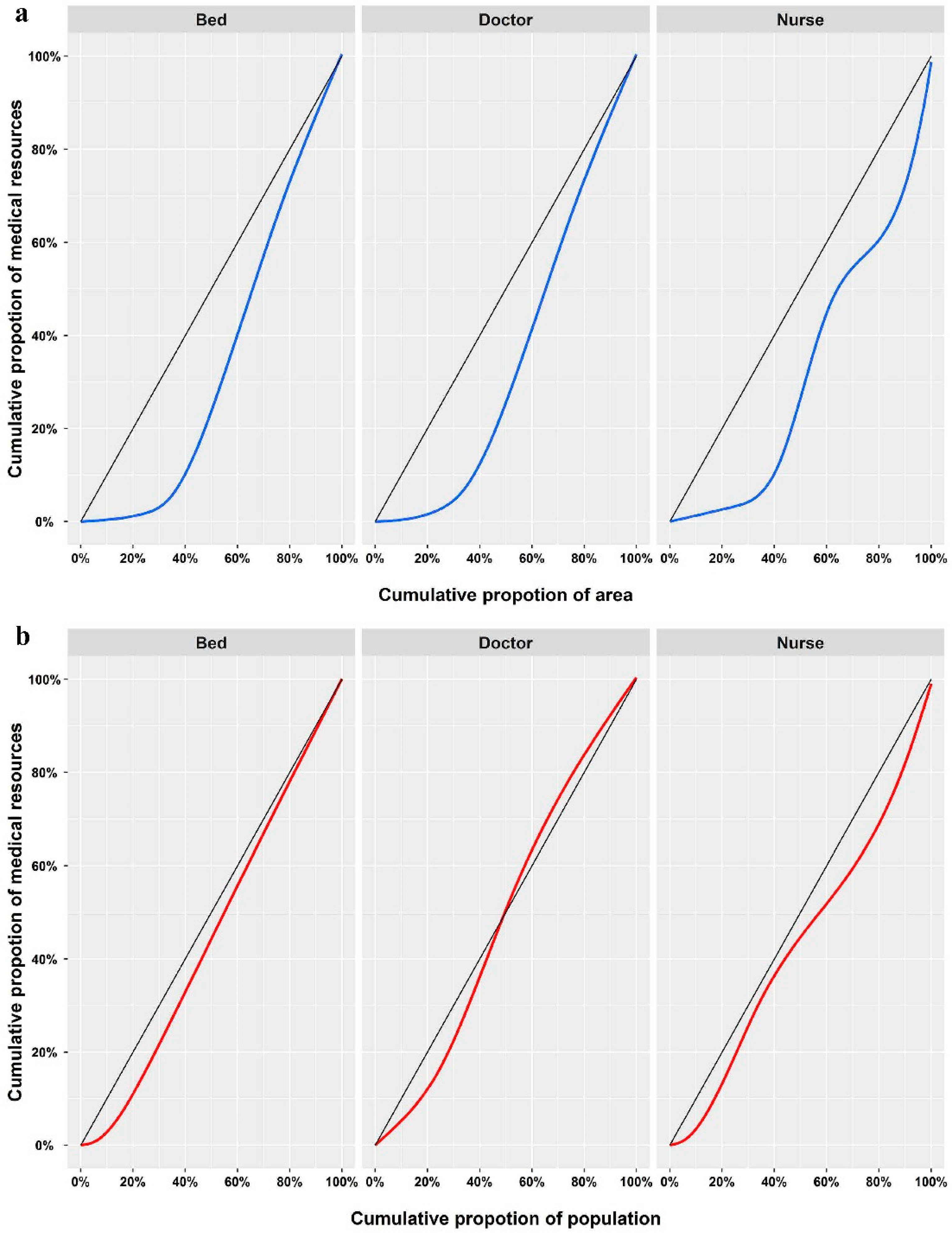
3.2. Gini Coefficients and Lorenz Curves
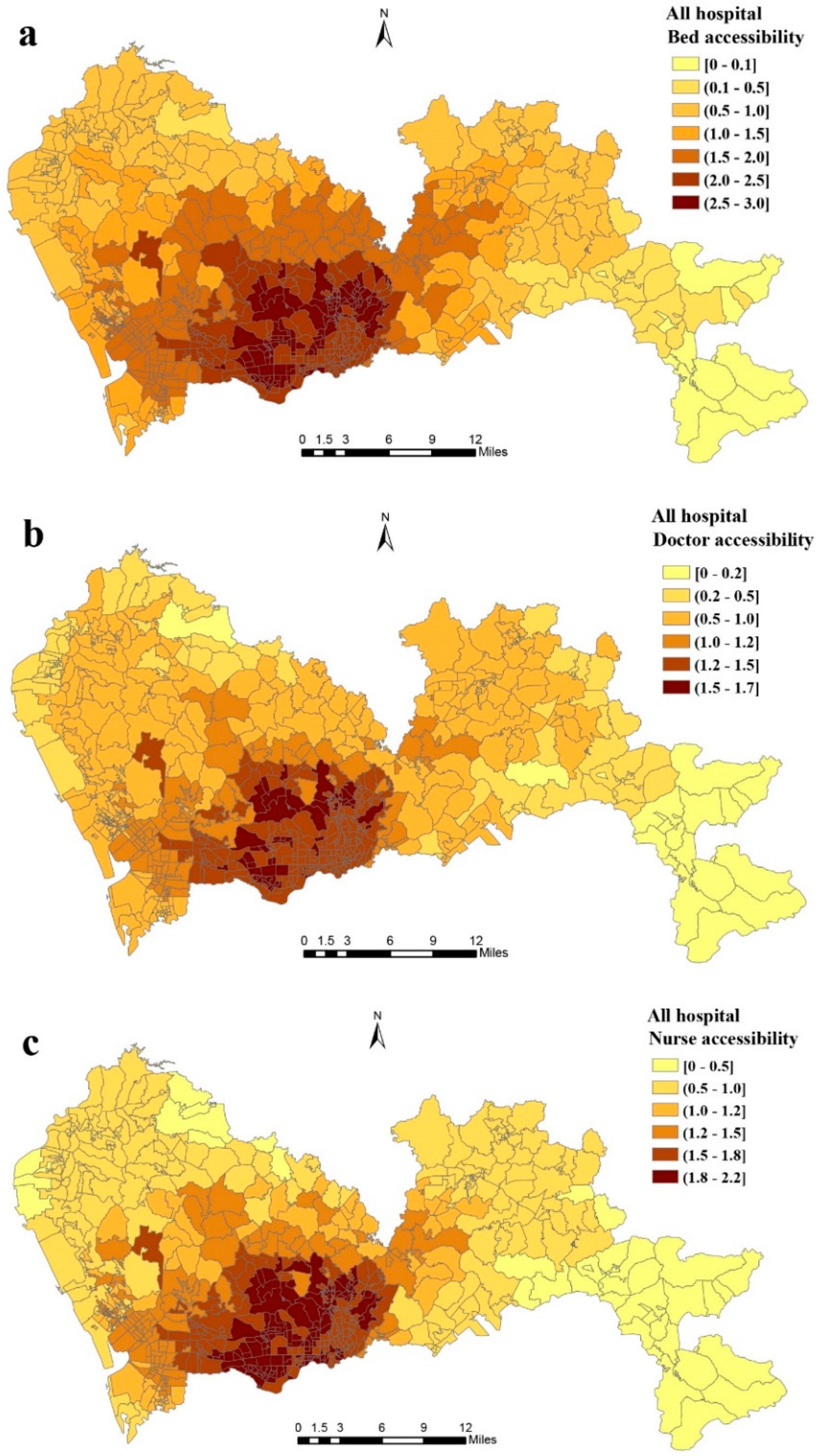
3.3. Spatial Accessibility of All General Hospitals by E2SFCA
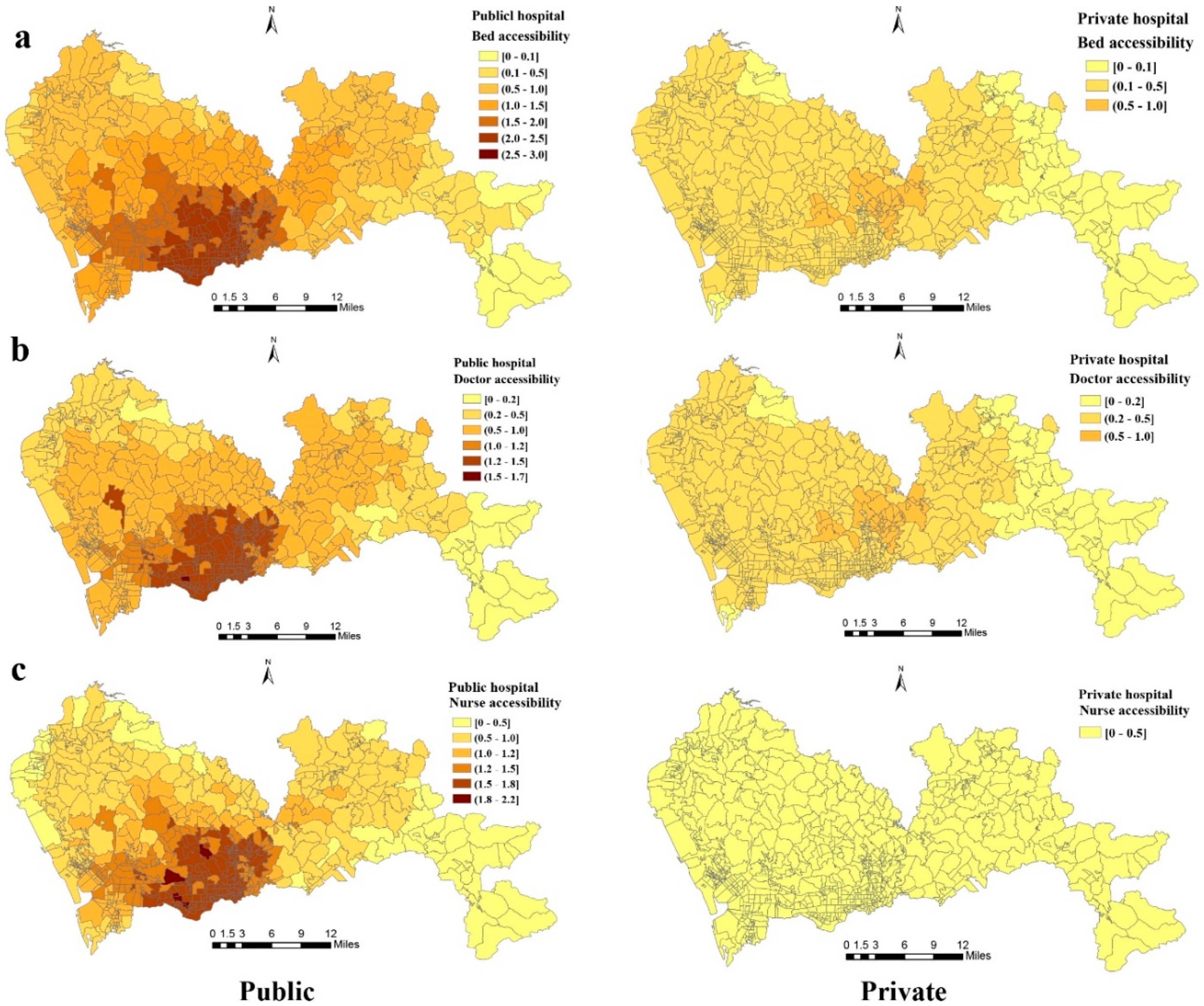
3.4. Spatial Accessibility of Public and Private Hospitals by E2SFCA
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Conflicts of Interest
References
- United Nations Transforming our world: The 2030 Agenda for Sustainable Development. Available online: https://sustainabledevelopment.un.org/post2015/transformingourworld/ (accessed on 25 September 2015).
- Tang, J.H.; Chiu, Y.H.; Chiang, P.H.; Su, M.D.; Chan, T.C. A flow-based statistical model integrating spatial and nonspatial dimensions to measure healthcare access. Health Place 2017, 47, 126–138. [Google Scholar] [CrossRef] [PubMed]
- Clarke, J.R.; Trooskin, S.Z.; Doshi, P.J.; Greenwald, L.; Mode, C.J. Time to laparotomy for intra-abdominal bleeding from trauma does affect survival for delays up to 90 minutes. J. Trauma Acute Care Surg. 2002, 52, 420–425. [Google Scholar] [CrossRef]
- Wang, F.; McLafferty, S.; Escamilla, V.; Luo, L. Late-Stage Breast Cancer Diagnosis and Health Care Access in Illinois. Prof. Geogr. J. Assoc. Am. Geogr. 2008, 60, 54–69. [Google Scholar] [CrossRef] [PubMed]
- Buchmueller, T.C.; Jacobson, M.; Wold, C. How far to the hospital? The effect of hospital closures on access to care. J. Health Econ. 2006, 25, 740–761. [Google Scholar] [CrossRef] [PubMed]
- Funk, L.M.; Weiser, T.G.; Berry, W.R.; Lipsitz, S.R.; Merry, A.F.; Enright, A.C.; Wilson, I.H.; Dziekan, G.; Gawande, A.A. Global operating theatre distribution and pulse oximetry supply: An estimation from reported data. Lancet 2010, 376, 1055–1061. [Google Scholar] [CrossRef]
- Hsia, R.Y.; Shen, Y.C. Rising closures of hospital trauma centers disproportionately burden vulnerable populations. Health Aff. 2011, 30, 1912–1920. [Google Scholar] [CrossRef] [PubMed]
- Alkire, B.C.; Raykar, N.P.; Shrime, M.G.; Weiser, T.G.; Bickler, S.W.; Rose, J.A.; Nutt, C.T.; Greenberg, S.L.M.; Kotagal, M.; Riesel, J.N.; et al. Global access to surgical care: A modelling study. Lancet Glob. Health 2015, 3, e316–e323. [Google Scholar] [CrossRef]
- Wu, H.C.; Tseng, M.H. Evaluating Disparities in Elderly Community Care Resources: Using a Geographic Accessibility and Inequality Index. Int. J. Environ. Res. Public Health 2018, 15, 1353. [Google Scholar] [CrossRef]
- Ding, J.; Hu, X.; Zhang, X.; Shang, L.; Yu, M.; Chen, H. Equity and efficiency of medical service systems at the provincial level of China’s mainland: A comparative study from 2009 to 2014. BMC Public Health 2018, 18, 214. [Google Scholar] [CrossRef]
- World Bank Group; World Health Organization; Ministry of Finance, P.R.C.; National Health Family Planning Commission, P.R.C.; Ministry of Human Resources and Social Security, P.R.C. Deepening Health Reform In China Building High-Quality And Value-Based Service Delivery; World Bank: Washington, DC, USA, 2016.
- Yang, G.; Wang, Y.; Zeng, Y.; Gao, G.F.; Liang, X.; Zhou, M.; Wan, X.; Yu, S.; Jiang, Y.; Naghavi, M.; et al. Rapid health transition in China, 1990-2010: Findings from the Global Burden of Disease Study 2010. Lancet 2013, 381, 1987–2015. [Google Scholar] [CrossRef]
- Tao, Z.; Yao, Z.; Kong, H.; Duan, F.; Li, G. Spatial accessibility to healthcare services in Shenzhen, China: Improving the multi-modal two-step floating catchment area method by estimating travel time via online map APIs. BMC Health Serv. Res. 2018, 18, 345. [Google Scholar] [CrossRef] [PubMed]
- Pan, J.; Zhao, H.; Wang, X.; Shi, X. Assessing spatial access to public and private hospitals in Sichuan, China: The influence of the private sector on the healthcare geography in China. Soc. Sci. Med. 2016, 170, 35–45. [Google Scholar] [CrossRef] [PubMed]
- Pan, J.; Liu, H.; Wang, X.; Xie, H.; Delamater, P.L. Assessing the spatial accessibility of hospital care in Sichuan Province, China. Geospat. Health 2015, 10, 384. [Google Scholar] [CrossRef] [PubMed]
- Song, P.; Zhu, Y.; Mao, X.; Li, Q.; An, L. Assessing spatial accessibility to maternity units in Shenzhen, China. PLoS ONE 2013, 8, e70227. [Google Scholar] [CrossRef]
- China State Council State Council Transmit the Opinions on Further Encourage and Introduce Social Capital to Build Health Care Institutions. Available online: www.gov.cn/xxgk/pub/govpublic/mrlm/201012/t20101203_63073.html (accessed on 26 November 2011).
- China State Council State Council General Office Notice to Issue Some Policy Measures about Promoting Social-do-medical Speed up Development. Available online: www.gov.cn/zhengce/content/2015-06/15/content_9845.htm (accessed on 15 June 2015).
- National Health Commission of the PRC Statistical Bulletin on the Development of China’s Health and Family Planning Undertakings in 2016. Available online: http://www.moh.gov.cn/guihuaxxs/s10748/201708/d82fa7141696407abb4ef764f3edf095.shtml?winzoom=1 (accessed on 18 August 2017).
- Ministry of Housing and Urban-Rural Development China Urban Construction Statistical Yearbook 2016. Available online: http://www.mohurd.gov.cn/xytj/tjzljsxytjgb/ (accessed on 5 January 2018).
- Shenzhen Statistics Bureau, NBS Survey Office in Shenzhen. Shenzhen Statistical Yearbook 2017. Available online: http://www.sztj.gov.cn/xxgk/zfxxgkml/tjsj/tjnj/201712/t20171219_10611980.htm (accessed on 19 December 2017).
- Department of Urban Surveys National Bureau of Statistics of China China City Statistical Yearbook 2017. Available online: http://www.stats.gov.cn/tjsj/tjcbw/201806/t20180612_1604098.html (accessed on 13 June 2018).
- General Office of Shenzhen Municipal People’s Government Notice on the Issuance of Trial Measures for Community Construction in Shenzhen. Available online: http://www.law-lib.com/law/law_view.asp?id=91830 (accessed on 22 February 2005).
- Karduni, A.; Kermanshah, A.; Derrible, S. A protocol to convert spatial polyline data to network formats and applications to world urban road networks. Sci. Data 2016, 3, 160046. [Google Scholar] [CrossRef] [PubMed]
- Ministry of Housing and Urban and Rural Construction Code for Design of Urban Road Engineering (2016 Revised Edition). Available online: http://www.mohurd.gov.cn/wjfb/201607/t20160712_228082.html (accessed on 28 June 2016).
- Stentzel, U.; Piegsa, J.; Fredrich, D.; Hoffmann, W.; van den Berg, N. Accessibility of general practitioners and selected specialist physicians by car and by public transport in a rural region of Germany. BMC Health Serv. Res. 2016, 16, 587. [Google Scholar] [CrossRef]
- Esquivel, M.M.; Uribe-Leitz, T.; Makasa, E.; Lishimpi, K.; Mwaba, P.; Bowman, K.; Weiser, T.G. Mapping Disparities in Access to Safe, Timely, and Essential Surgical Care in Zambia. JAMA Surg. 2016, 151, 1064–1069. [Google Scholar] [CrossRef]
- McGrail, M.R. Spatial accessibility of primary health care utilising the two step floating catchment area method: An assessment of recent improvements. Int. J. Health Geogr. 2012, 11, 50. [Google Scholar] [CrossRef]
- Clark, D.E.; Cowley, R.A. The “Golden Hour,” the “Momentary Pause,” and the “Third Space”. Am. Surg. 2017, 83, 1401–1406. [Google Scholar]
- Rolfe, M.I.; Donoghue, D.A.; Longman, J.M.; Pilcher, J.; Kildea, S.; Kruske, S.; Kornelsen, J.; Grzybowski, S.; Barclay, L.; Morgan, G.G. The distribution of maternity services across rural and remote Australia: Does it reflect population need? BMC Health Serv. Res. 2017, 17, 163. [Google Scholar] [CrossRef] [PubMed]
- Luo, W.; Qi, Y. An enhanced two-step floating catchment area (E2SFCA) method for measuring spatial accessibility to primary care physicians. Health Place 2009, 15, 1100–1107. [Google Scholar] [CrossRef] [PubMed]
- Wan, N.; Zhan, F.B.; Zou, B.; Chow, E. A relative spatial access assessment approach for analyzing potential spatial access to colorectal cancer services in Texas. Appl. Geogr. 2012, 32, 291–299. [Google Scholar] [CrossRef]
- CPC Central Committee, C.S.C. The Plan of Health China 2030. Available online: http://www.gov.cn/zhengce/2016-10/25/content_5124174.htm (accessed on 25 October 2016).
- Mauguen, A.; Begg, C.B. Using the Lorenz Curve to Characterize Risk Predictiveness and Etiologic Heterogeneity. Epidemiology 2016, 27, 531–537. [Google Scholar] [CrossRef] [PubMed]
- Horev, T.; Pesis-Katz, I.; Mukamel, D.B. Trends in geographic disparities in allocation of health care resources in the US. Health Policy 2004, 68, 223–232. [Google Scholar] [CrossRef]
- Wu, J. Measuring inequalities in the demographical and geographical distribution of physicians in China: Generalist versus specialist. Int. J. Health Plan. Manag. 2018. [Google Scholar] [CrossRef]
- Nakamura, T.; Nakamura, A.; Mukuda, K.; Harada, M.; Kotani, K. Potential accessibility scores for hospital care in a province of Japan: GIS-based ecological study of the two-step floating catchment area method and the number of neighborhood hospitals. BMC Health Serv. Res. 2017, 17, 438. [Google Scholar] [CrossRef]
- Gao, F.; Kihal, W.; Le Meur, N.; Souris, M.; Deguen, S. Assessment of the spatial accessibility to health professionals at French census block level. Int. J. Equity Health 2016, 15, 125. [Google Scholar] [CrossRef]
- Cromley, E.K.; Mclafferty, S.L. GIS and Public Health, 2nd ed.; Guilford Press: New York, NY, USA, 2012. [Google Scholar]
- Shenzhen Municipal Health Planning Commission Notice of the Municipal Health and Family Planning Commission on publishing the Shenzhen Regional Health Plan (2016–2020). Available online: http://www.szhfpc.gov.cn/wjtz/201706/t20170620_7174309.htm (accessed on 20 June 2017).
- Xiong, X.; Jin, C.; Chen, H.; Luo, L. Using the Fusion Proximal Area Method and Gravity Method to Identify Areas with Physician Shortages. PLoS ONE 2016, 11, e0163504. [Google Scholar] [CrossRef]
- Xiong, X.; Bai, G.; Jin, C.; Zhou, Y.; Chen, H.; Fu, C.; Wu, L.; Luo, L. A method of calculating and visualizing spatial accessibility to health services based on the nearest distance method. Chin. Health Resour. 2016, 19, 5. (In Chinese) [Google Scholar]
- Wang, X.; Pan, J. Assessing the disparity in spatial access to hospital care in ethnic minority region in Sichuan Province, China. BMC Health Serv. Res. 2016, 16, 399. [Google Scholar] [CrossRef]
- Luo, J.; Chen, G.; Li, C.; Xia, B.; Sun, X.; Chen, S. Use of an E2SFCA Method to Measure and Analyse Spatial Accessibility to Medical Services for Elderly People in Wuhan, China. Int. J. Environ. Res. Public Health 2018, 15, 1503. [Google Scholar] [CrossRef] [PubMed]
- Shi, X.; Wang, F. Applications of Geospatial Information Technologies in Public Health; Higher Education Press: Beijing, China, 2016. [Google Scholar]
- Cheng, Y.; Wang, J.; Rosenberg, M.W. Spatial access to residential care resources in Beijing, China. Int. J. Health Geogr. 2012, 11, 32. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zhi-kui, X.; Zhuo, L. Immigration Culture and Development of EmergingCities: Based on Shenzhen Experience. J. Shenzhen Univ. 2017, 34, 32–37. (In Chinese) [Google Scholar]
- Wang, F.; Luo, W. Assessing spatial and nonspatial factors for healthcare access: Towards an integrated approach to defining health professional shortage areas. Health Place 2005, 11, 131–146. [Google Scholar] [CrossRef] [PubMed]
- Cummings, J.R.; Allen, L.; Clennon, J.; Ji, X.; Druss, B.G. Geographic Access to Specialty Mental Health Care Across High- and Low-Income US Communities. JAMA Psychiatry 2017, 74, 476–484. [Google Scholar] [CrossRef] [PubMed]
- Hu, K.J.; Sun, Z.Z.; Rui, Y.J.; Mi, J.Y.; Ren, M.X. Shortage of paediatricians in China. Lancet 2014, 383, 954. [Google Scholar] [CrossRef]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Types of hospital | Hospital Number | Total Number of Beds | Total Number of Doctors | Total Number of Nurses |
|---|---|---|---|---|
| All general hospitals | 82 | 30,646 | 18,186 | 23,014 |
| Public hospital | 41 | 24,751 | 16,155 | 19,872 |
| Public primary hospital | 8 | 1354 | 1298 | 1591 |
| Public secondary hospital | 17 | 7943 | 6049 | 7122 |
| Public tertiary hospital | 16 | 15,454 | 8808 | 11,159 |
| Private hospital | 41 | 5895 | 2031 | 3142 |
| Private primary hospital | 36 | 4722 | 1657 | 2551 |
| Private secondary hospital | 3 | 503 | 142 | 218 |
| Private tertiary hospital | 1 | 600 | 194 | 294 |
| Unrated hospital | 1 | 70 | 38 | 79 |
| Spatial Accessibility | Max | Min | Median | Q1 a | Q3 | IQR | |
|---|---|---|---|---|---|---|---|
| Bed | All | 3.01 * | 0.01 | 1.74 | 1.05 | 2.43 | 1.37 |
| Public | 2.48 | 0.01 | 1.42 | 0.83 | 2.01 | 1.18 | |
| Private | 0.66 | 0.00 | 0.31 | 0.20 | 0.42 | 0.22 | |
| Doctor | All | 1.67 | 0.01 | 1.04 | 0.67 | 1.39 | 0.72 |
| Public | 1.50 | 0.01 | 0.92 | 0.60 | 1.23 | 0.63 | |
| Private | 0.20 | 0.00 | 0.12 | 0.07 | 0.16 | 0.09 | |
| Nurse | All | 2.11 | 0.01 | 1.31 | 0.82 | 1.77 | 0.95 |
| Public | 1.86 | 0.01 | 1.13 | 0.72 | 1.53 | 0.81 | |
| Private | 0.31 | 0.00 | 0.18 | 0.10 | 0.24 | 0.14 | |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Zhu, L.; Zhong, S.; Tu, W.; Zheng, J.; He, S.; Bao, J.; Huang, C. Assessing Spatial Accessibility to Medical Resources at the Community Level in Shenzhen, China. Int. J. Environ. Res. Public Health 2019, 16, 242. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph16020242
Zhu L, Zhong S, Tu W, Zheng J, He S, Bao J, Huang C. Assessing Spatial Accessibility to Medical Resources at the Community Level in Shenzhen, China. International Journal of Environmental Research and Public Health. 2019; 16(2):242. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph16020242
Chicago/Turabian StyleZhu, Lei, Shuang Zhong, Wei Tu, Jing Zheng, Shenjing He, Junzhe Bao, and Cunrui Huang. 2019. "Assessing Spatial Accessibility to Medical Resources at the Community Level in Shenzhen, China" International Journal of Environmental Research and Public Health 16, no. 2: 242. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph16020242