Trimester-Specific Assessment of Diet Quality in a Sample of Canadian Pregnant Women

 ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Population
2.2. Nutritional Sata Collection
2.3. Healthy Eating Index
2.4. Supplement Use
2.5. Nutrition Knowledge
2.6. Nausea, Vomiting and Food Preferences During Pregnancy
2.7. Other Variables
2.8. Statistical Analyses
3. Results
3.1. Participants’ Characteristics
3.2. Supplement Use
3.3. Adherence to Canada’s Food Guide
3.4. Diet Quality throughout Pregnancy
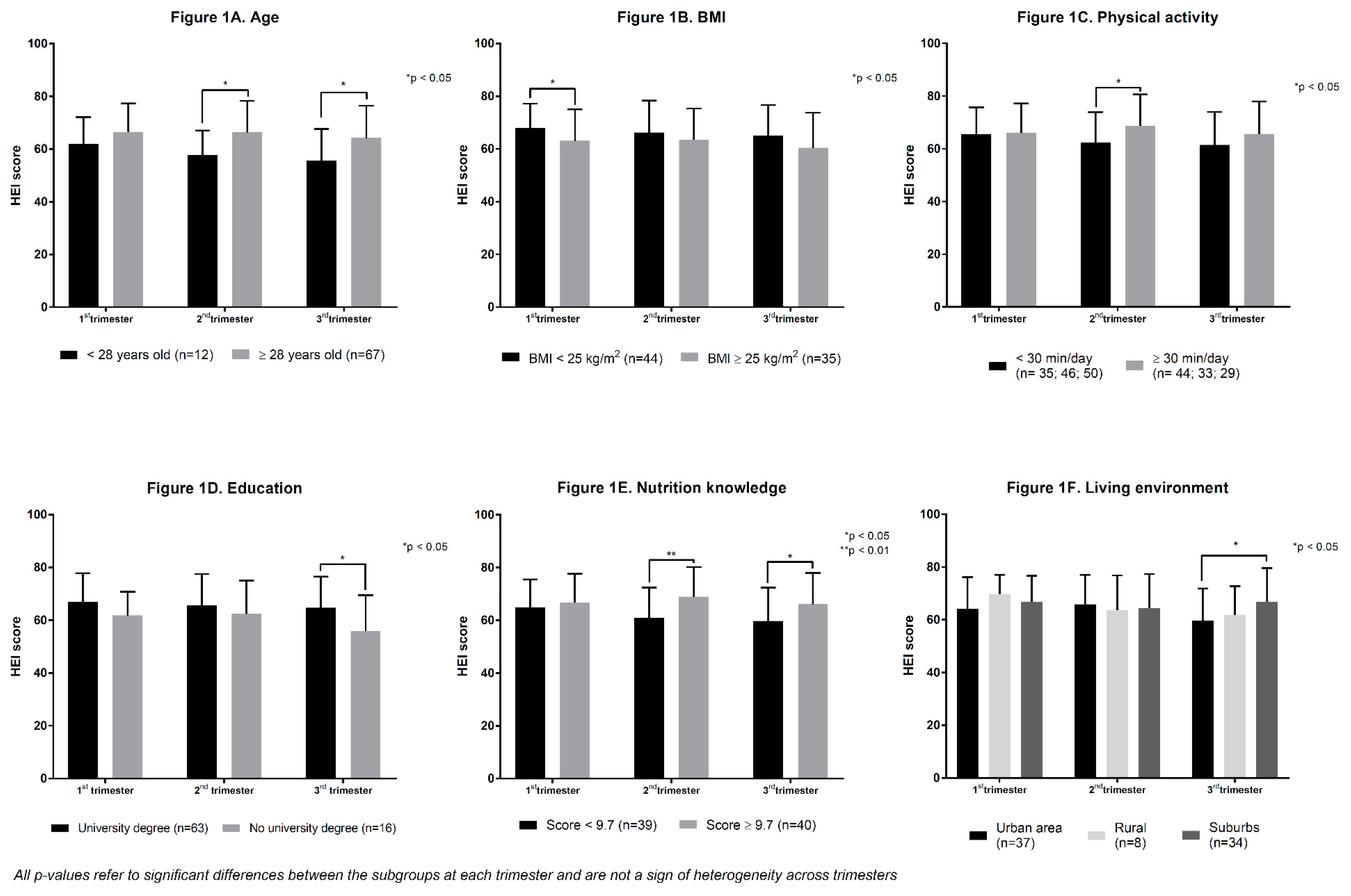
3.5. Trimester-Specific Diet Quality
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Kaiser, L.; Allen, L.H. Position of the American Dietetic Association: Nutrition and lifestyle for a healthy pregnancy outcome. J. Am. Diet. Assoc. 2008, 108, 553–561. [Google Scholar] [PubMed]
- Symonds, M.E.; Ramsay, M.M. Maternal-Fetal Nutrition during Pregnancy and Lactation; Cambridge University Press: Cambridge, UK, 2010. [Google Scholar]
- Whitney, E.N.; Cataldo, C.B.; Rolfes, S.R. Understanding Normal and Clinical Nutrition; Wadsworth Publishing Company, Inc.: Belmont, CA, USA, 2002. [Google Scholar]
- Barker, D.J. The fetal and infant origins of disease. Eur. J. Clin. Investig. 1995, 25, 457–463. [Google Scholar] [CrossRef] [Green Version]
- Black, R.E.; Victora, C.G.; Walker, S.P.; Bhutta, Z.A.; Christian, P.; de Onis, M.; Ezzati, M.; Grantham-McGregor, S.; Katz, J.; Martorell, R.; et al. Maternal and child undernutrition and overweight in low-income and middle-income countries. Lancet 2013, 382, 427–451. [Google Scholar] [CrossRef]
- Grieger, J.A.; Clifton, V.L. A review of the impact of dietary intakes in human pregnancy on infant birthweight. Nutrients 2014, 7, 153–178. [Google Scholar] [CrossRef] [PubMed]
- Ladipo, O.A. Nutrition in pregnancy: Mineral and vitamin supplements. Am. J. Clin. Nutr. 2000, 72, 280S–290S. [Google Scholar] [CrossRef] [PubMed]
- Ramakrishnan, U. Nutrition and low birth weight: From research to practice. Am. J. Clin. Nutr. 2004, 79, 17–21. [Google Scholar] [CrossRef] [PubMed]
- Martin, J.C.; Zhou, S.J.; Flynn, A.C.; Malek, L.; Greco, R.; Moran, L. The Assessment of Diet Quality and Its Effects on Health Outcomes Pre-pregnancy and during Pregnancy. Semin. Reprod. Med. 2016, 34, 83–92. [Google Scholar] [CrossRef] [PubMed]
- Hu, F.B.; Rimm, E.; Smith-Warner, S.A.; Feskanich, D.; Stampfer, M.J.; Ascherio, A.; Sampson, L.; Willett, W.C. Reproducibility and validity of dietary patterns assessed with a food-frequency questionnaire. Am. J. Clin. Nutr. 1999, 69, 243–249. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kennedy, E.T.; Ohls, J.; Carlson, S.; Fleming, K. The Healthy Eating Index: Design and applications. J. Am. Diet. Assoc. 1995, 95, 1103–1108. [Google Scholar] [CrossRef]
- Slattery, M.L. Defining dietary consumption: Is the sum greater than its parts? Am. J. Clin. Nutr. 2008, 88, 14–15. [Google Scholar] [CrossRef]
- Emond, J.A.; Karagas, M.R.; Baker, E.R.; Gilbert-Diamond, D. Better Diet Quality during Pregnancy Is Associated with a Reduced Likelihood of an Infant Born Small for Gestational Age: An Analysis of the Prospective New Hampshire Birth Cohort Study. J. Nutr. 2018, 148, 22–30. [Google Scholar] [CrossRef] [Green Version]
- Schoenaker, D.A.; Mishra, G.D.; Callaway, L.K.; Soedamah-Muthu, S.S. The Role of Energy, Nutrients, Foods, and Dietary Patterns in the Development of Gestational Diabetes Mellitus: A Systematic Review of Observational Studies. Diabetes Care 2016, 39, 16–23. [Google Scholar] [CrossRef] [PubMed]
- Grandy, M.; Snowden, J.M.; Boone-Heinonen, J.; Purnell, J.Q.; Thornburg, K.L.; Marshall, N.E. Poorer maternal diet quality and increased birth weight. J. Matern. Fetal. Neonatal. Med. 2018, 31, 1613–1619. [Google Scholar] [CrossRef] [PubMed]
- Institute of Medicine. Nutrition During Pregnancy; Institute of Medicine: Washington, DC, USA, 1990. [Google Scholar] [CrossRef]
- Wu, G.; Imhoff-Kunsch, B.; Girard, A.W. Biological mechanisms for nutritional regulation of maternal health and fetal development. Paediatr. Perinat. Epidemiol. 2012, 26 (Suppl. 1), 4–26. [Google Scholar] [CrossRef]
- Wu, G.; Bazer, F.W.; Cudd, T.A.; Meininger, C.J.; Spencer, T.E. Maternal nutrition and fetal development. J. Nutr. 2004, 134, 2169–2172. [Google Scholar] [CrossRef] [PubMed]
- Green, N.S. Folic acid supplementation and prevention of birth defects. J. Nutr. 2002, 132, 2356S–2360S. [Google Scholar] [CrossRef]
- Wang, S.; Ge, X.; Zhu, B.; Xuan, Y.; Huang, K.; Rutayisire, E.; Mao, L.; Huang, S.; Yan, S.; Tao, F. Maternal Continuing Folic Acid Supplementation after the First Trimester of Pregnancy Increased the Risk of Large-for-Gestational-Age Birth: A Population-Based Birth Cohort Study. Nutrients 2016, 8, 493. [Google Scholar] [CrossRef]
- Health Canada. Prenatal Nutrition Guidelines for Health Professionals. Background on Canada’s Food Guide; Health Canada: Ottawa, ON, Canada, 2009.
- Butte, N.F.; King, J.C. Energy requirements during pregnancy and lactation. Public Health Nutr. 2005, 8, 1010–1027. [Google Scholar] [CrossRef]
- Savard, C.; Lemieux, S.; Weisnagel, S.J.; Fontaine-Bisson, B.; Gagnon, C.; Robitaille, J.; Morisset, A.S. Trimester-Specific Dietary Intakes in a Sample of French-Canadian Pregnant Women in Comparison with National Nutritional Guidelines. Nutrients 2018, 10, 768. [Google Scholar] [CrossRef]
- Abeysekera, M.V.; Morris, J.A.; Davis, G.K.; O’Sullivan, A.J. Alterations in energy homeostasis to favour adipose tissue gain: A longitudinal study in healthy pregnant women. Aust. N. Z. J. Obstet. Gynaecol. 2016, 56, 42–48. [Google Scholar] [CrossRef]
- Dubois, L.; Diasparra, M.; Bedard, B.; Colapinto, C.K.; Fontaine-Bisson, B.; Morisset, A.S.; Tremblay, R.E.; Fraser, W.D. Adequacy of nutritional intake from food and supplements in a cohort of pregnant women in Quebec, Canada: The 3D Cohort Study (Design, Develop, Discover). Am. J. Clin. Nutr. 2017, 106, 541–548. [Google Scholar] [CrossRef] [PubMed]
- Kubota, K.; Itoh, H.; Tasaka, M.; Naito, H.; Fukuoka, Y.; Muramatsu Kato, K.; Kohmura, Y.K.; Sugihara, K.; Kanayama, N.; Hamamatsu Birth Cohort (HBC) Study Team. Changes of maternal dietary intake, bodyweight and fetal growth throughout pregnancy in pregnant Japanese women. J. Obstet. Gynaecol. Res. 2013, 39, 1383–1390. [Google Scholar] [CrossRef] [PubMed]
- Talai Rad, N.; Ritterath, C.; Siegmund, T.; Wascher, C.; Siebert, G.; Henrich, W.; Buhling, K.J. Longitudinal analysis of changes in energy intake and macronutrient composition during pregnancy and 6 weeks post-partum. Arch. Gynecol. Obstet. 2011, 283, 185–190. [Google Scholar] [CrossRef] [PubMed]
- Nash, D.M.; Gilliland, J.A.; Evers, S.E.; Wilk, P.; Campbell, M.K. Determinants of diet quality in pregnancy: Sociodemographic, pregnancy-specific, and food environment influences. J. Nutr. Educ. Behav. 2013, 45, 627–634. [Google Scholar] [CrossRef]
- Savard, C.; Lemieux, S.; Lafreniere, J.; Laramee, C.; Robitaille, J.; Morisset, A.S. Validation of a self-administered web-based 24-hour dietary recall among pregnant women. BMC Pregnancy Childbirth 2018, 18, 112. [Google Scholar] [CrossRef] [PubMed]
- Jacques, S.; Lemieux, S.; Lamarche, B.; Laramee, C.; Corneau, L.; Lapointe, A.; Tessier-Grenier, M.; Robitaille, J. Development of a Web-Based 24-h Dietary Recall for a French-Canadian Population. Nutrients 2016, 8, 724. [Google Scholar] [CrossRef] [PubMed]
- Lafreniere, J.; Laramee, C.; Robitaille, J.; Lamarche, B.; Lemieux, S. Assessing the relative validity of a new, web-based, self-administered 24 h dietary recall in a French-Canadian population. Public Health Nutr. 2018, 1–9. [Google Scholar] [CrossRef]
- Moshfegh, A.J.; Rhodes, D.G.; Baer, D.J.; Murayi, T.; Clemens, J.C.; Rumpler, W.V.; Paul, D.R.; Sebastian, R.S.; Kuczynski, K.J.; Ingwersen, L.A.; et al. The US Department of Agriculture Automated Multiple-Pass Method reduces bias in the collection of energy intakes. Am. J. Clin. Nutr. 2008, 88, 324–332. [Google Scholar] [CrossRef] [Green Version]
- Canadian Nutrient File (CNF). Available online: https://food-nutrition.canada.ca/cnf-fce/index-eng.jsp (accessed on 26 March 2018).
- Eating Well with Canada’s Food Guide; Health Canada: Ottawa, ON, Canada, 2007.
- Garriguet, D. Diet quality in Canada. Health Rep. 2009, 20, 41–52. [Google Scholar]
- Moran, L.J.; Sui, Z.; Cramp, C.S.; Dodd, J.M. A decrease in diet quality occurs during pregnancy in overweight and obese women which is maintained post-partum. Int. J. Obes. 2013, 37, 704–711. [Google Scholar] [CrossRef]
- Shin, D.; Bianchi, L.; Chung, H.; Weatherspoon, L.; Song, W.O. Is gestational weight gain associated with diet quality during pregnancy? Matern. Child Health J. 2014, 18, 1433–1443. [Google Scholar] [CrossRef] [PubMed]
- Tsigga, M.; Filis, V.; Hatzopoulou, K.; Kotzamanidis, C.; Grammatikopoulou, M.G. Healthy Eating Index during pregnancy according to pre-gravid and gravid weight status. Public Health Nutr. 2011, 14, 290–296. [Google Scholar] [CrossRef] [PubMed]
- National Nutrient Database for Standard Reference. Available online: https://www.ars.usda.gov/northeast-area/beltsville-md/beltsville-human-nutrition-research-center/nutrient-data-laboratory/docs/usda-national-nutrient-database-for-standard-reference-dataset-for-what-we-eat-in-america-nhanes-survey-sr/ (accessed on 26 March 2018).
- Bradette-Laplante, M.; Carbonneau, E.; Provencher, V.; Begin, C.; Robitaille, J.; Desroches, S.; Vohl, M.C.; Corneau, L.; Lemieux, S. Development and validation of a nutrition knowledge questionnaire for a Canadian population. Public Health Nutr. 2017, 20, 1184–1192. [Google Scholar] [CrossRef] [PubMed]
- Chandonnet, N.; Saey, D.; Almeras, N.; Marc, I. French Pregnancy Physical Activity Questionnaire compared with an accelerometer cut point to classify physical activity among pregnant obese women. PLoS ONE 2012, 7, e38818. [Google Scholar] [CrossRef] [PubMed]
- Chasan-Taber, L.; Schmidt, M.D.; Roberts, D.E.; Hosmer, D.; Markenson, G.; Freedson, P.S. Development and validation of a Pregnancy Physical Activity Questionnaire. Med. Sci. Sports Exerc. 2004, 36, 1750–1760. [Google Scholar] [CrossRef] [PubMed]
- Statistics Canada. Fertility: Fewer Children, Older Moms. 2014. Available online: https://www150.statcan.gc.ca/n1/pub/11-630-x/11-630-x2014002-eng.htm (accessed on 29 June 2018).
- Rifas-Shiman, S.L.; Rich-Edwards, J.W.; Willett, W.C.; Kleinman, K.P.; Oken, E.; Gillman, M.W. Changes in dietary intake from the first to the second trimester of pregnancy. Paediatr. Perinat. Epidemiol. 2006, 20, 35–42. [Google Scholar] [CrossRef] [Green Version]
- Lindqvist, M.; Lindkvist, M.; Eurenius, E.; Persson, M.; Mogren, I. Change of lifestyle habits—Motivation and ability reported by pregnant women in northern Sweden. Sex. Reprod. Healthc. 2017, 13, 83–90. [Google Scholar] [CrossRef]
- Thangaratinam, S.; Rogozinska, E.; Jolly, K.; Glinkowski, S.; Roseboom, T.; Tomlinson, J.W.; Kunz, R.; Mol, B.W.; Coomarasamy, A.; Khan, K.S. Effects of interventions in pregnancy on maternal weight and obstetric outcomes: Meta-analysis of randomised evidence. BMJ 2012, 344, e2088. [Google Scholar] [CrossRef]
- Skreden, M.; Bere, E.; Sagedal, L.R.; Vistad, I.; Overby, N.C. Changes in fruit and vegetable consumption habits from pre-pregnancy to early pregnancy among Norwegian women. BMC Pregnancy Childbirth 2017, 17, 107. [Google Scholar] [CrossRef] [PubMed]
- Shin, D.; Lee, K.W.; Song, W.O. Pre-Pregnancy Weight Status Is Associated with Diet Quality and Nutritional Biomarkers during Pregnancy. Nutrients 2016, 8, 162. [Google Scholar] [CrossRef] [PubMed]
- Li, N.; Liu, E.; Guo, J.; Pan, L.; Li, B.; Wang, P.; Liu, J.; Wang, Y.; Liu, G.; Baccarelli, A.A.; et al. Maternal prepregnancy body mass index and gestational weight gain on pregnancy outcomes. PLoS ONE 2013, 8, e82310. [Google Scholar] [CrossRef]
- Schummers, L.; Hutcheon, J.A.; Bodnar, L.M.; Lieberman, E.; Himes, K.P. Risk of adverse pregnancy outcomes by prepregnancy body mass index: A population-based study to inform prepregnancy weight loss counseling. Obstet. Gynecol. 2015, 125, 133–143. [Google Scholar] [CrossRef] [PubMed]
- Zhang, C.H.; Liu, X.Y.; Zhan, Y.W.; Zhang, L.; Huang, Y.J.; Zhou, H. Effects of Prepregnancy Body Mass Index and Gestational Weight Gain on Pregnancy Outcomes. Asia Pac. J. Public Health 2015, 27, 620–630. [Google Scholar] [CrossRef] [PubMed]
- Rifas-Shiman, S.L.; Rich-Edwards, J.W.; Kleinman, K.P.; Oken, E.; Gillman, M.W. Dietary quality during pregnancy varies by maternal characteristics in Project Viva: A US cohort. J. Am. Diet. Assoc. 2009, 109, 1004–1011. [Google Scholar] [CrossRef] [PubMed]
- Laraia, B.A.; Siega-Riz, A.M.; Kaufman, J.S.; Jones, S.J. Proximity of supermarkets is positively associated with diet quality index for pregnancy. Prev. Med. 2004, 39, 869–875. [Google Scholar] [CrossRef] [PubMed]
- Doyle, I.M.; Borrmann, B.; Grosser, A.; Razum, O.; Spallek, J. Determinants of dietary patterns and diet quality during pregnancy: A systematic review with narrative synthesis. Public Health Nutr. 2017, 20, 1009–1028. [Google Scholar] [CrossRef] [PubMed]
- Lindsay, K.L.; Buss, C.; Wadhwa, P.D.; Entringer, S. The Interplay between Maternal Nutrition and Stress during Pregnancy: Issues and Considerations. Ann. Nutr. Metab. 2017, 70, 191–200. [Google Scholar] [CrossRef] [Green Version]
- Hurley, K.M.; Caulfield, L.E.; Sacco, L.M.; Costigan, K.A.; Dipietro, J.A. Psychosocial influences in dietary patterns during pregnancy. J. Am. Diet. Assoc. 2005, 105, 963–966. [Google Scholar] [CrossRef]


{kind=link}
| Variables | Mean ± SD or N (%) | ||
|---|---|---|---|
| Baseline (1st Trimester) | 2nd Trimester | 3rd Trimester | |
| Age (years) | 32.1 ± 3.7 | - | - |
| Weeks of gestation at baseline (weeks) | 9.3 ± 0.7 | - | - |
| Primiparous | 28 (35.4) | - | - |
| BMI (kg/m2) | 25.7 ± 5.8 | - | - |
| Underweight | 2 (2.5) | - | - |
| Normal weight | 43 (54.4) | - | - |
| Overweight | 19 (24.1) | - | - |
| Obese | 15 (19.0) | - | - |
| Ethnicity-Caucasian 1 | 77 (97.5) | - | - |
| Education | |||
| High school | 4 (5.0) | - | - |
| College | 13 (16.5) | - | - |
| University | 62 (78.5) | - | - |
| Household income | |||
| <60,000 $ | 15 (19.0) | - | - |
| 60,000–79,999 $ | 13 (16.5) | - | - |
| 80,000–99,999 $ | 17 (21.5) | - | - |
| >100,000 $ | 33 (41.8) | - | - |
| Income missing | 1 (1.2) | - | - |
| Living environment | |||
| Urban | 37 (46.8) | - | - |
| Rural | 8 (10.1) | - | - |
| Suburbs | 34 (43.0) | - | - |
| General nutrition knowledge (total score) 2 | 9.6 ± 1.6 | - | - |
| Physical activity level (min/day) 3 | 60.5 ± 59.6 | 45.9 ± 51.1 | 35.2 ± 41.5 |
| Reported nausea (yes) | 70 (88.6) | 26 (32.9) | 16 (20.3) |
| Reported vomiting (yes) | 25 (31.7) | 15 (19.0) | 2 (2.5) |
| Food cravings (yes) | 44 (55.7) | 33 (41.8) | 25 (31.7) |
| Food aversions (yes) | 50 (63.3) | 28 (35.4) | 17 (21.5) |
| Food Groups | Number of Servings/Day (or Other) 1 | p-Value * | |||||
|---|---|---|---|---|---|---|---|
| 1st Trimester | 2nd Trimester | 3rd Trimester | |||||
| Recommended Range 2 | Mean ± SD | Recommended Range 3 | Mean ± SD | Recommended Range 4 | Mean ± SD | ||
| Fruits and vegetables | 7–8 | 6.4 ± 2.2 | 7–10 | 6.1 ± 2.6 | 7–11 | 5.8 ± 2.4 | 0.094 |
| Whole fruits | - | 2.0 ± 1.1 | - | 2.0 ± 1.3 | - | 2.0 ± 1.2 | 0.875 |
| Green and orange vegetables | 2 | 1.3 ± 0.8 | 2–4 | 1.2 ± 0.9 | 2–5 | 1.1 ± 0.8 | 0.321 |
| Grain products | 6–7 | 6.1 ± 1.8 | 6–9 | 5.9 ± 1.8 | 6–10 | 5.7 ± 2.0 | 0.206 |
| Whole grain products | 3 | 1.5 ± 1.3 | 3–5 | 1.5 ± 1.3 | 3–6 | 1.6 ± 1.4 | 0.868 |
| Milk and alternatives | 2 | 2.5 ± 1.1 | 2–4 | 2.7 ± 1.4 | 2–5 | 3.0 ± 1.4 | 0.002 |
| Meat and alternatives | 2 | 2.2 ± 0.9 | 2–4 | 2.2 ± 0.8 | 2–5 | 2.1 ± 0.8 | 0.740 |
| Saturated fats (% daily EI) | - | 12.8 ± 2.1 22.2 ± 9.6 | - | 13.2 ± 2.9 | - | 13.5 ± 2.5 | 0.047 |
| Other foods (% daily EI) | - | - | 22.0 ± 9.5 | - | 22.1 ± 10.3 | 0.969 | |
| HEI | 1st Trimester | 2nd Trimester | 3rd Trimester | p-Value * |
|---|---|---|---|---|
| Total | 65.8 ± 10.8 | 65.0 ± 12.0 | 62.9 ± 12.6 | 0.075 |
| Adequacy † | 47.2 ± 7.4 | 46.4 ± 7.7 | 44.7 ± 8.2 | 0.016 |
| Total vegetables and fruits | 8.3 ± 2.0 | 7.7 ± 2.1 | 7.7 ± 2.2 | 0.018 |
| Whole fruits | 4.3 ± 1.5 | 4.1 ± 1.4 | 4.3 ± 1.4 | 0.778 |
| Dark green and orange vegetables | 3.5 ± 1.6 | 3.4 ± 1.6 | 3.0 ± 1.6 | 0.056 |
| Total grain products | 4.5 ± 0.7 | 4.4 ± 0.8 | 4.2 ± 0.9 | 0.123 |
| Whole grains | 2.4 ± 1.8 | 2.3 ± 1.7 | 2.4 ± 1.9 | 0.893 |
| Milk and alternatives | 8.9 ± 2.0 | 8.9 ± 2.1 | 9.1 ± 1.9 | 0.685 |
| Meat and alternatives | 8.7 ± 2.0 | 8.9 ± 1.9 | 8.6 ± 2.2 | 0.566 |
| Unsaturated fats | 6.6 ± 3.0 | 6.6 ± 3.4 | 5.4 ± 3.4 | 0.008 |
| Moderation ‡ | 18.6 ± 7.2 | 18.6 ± 7.9 | 18.2 ± 8.1 | 0.894 |
| Saturated fats | 4.0 ± 2.7 | 3.6 ± 3.1 | 3.1 ± 2.8 | 0.039 |
| Sodium | 4.4 ± 2.6 | 4.7 ± 2.8 | 5.0 ± 2.7 | 0.173 |
| Other foods | 10.2 ± 5.1 | 10.3 ± 5.2 | 10.2 ± 5.7 | 0.970 |
| Maternal Characteristics | 1st Trimester | 2nd Trimester | 3rd Trimester | ||||||
|---|---|---|---|---|---|---|---|---|---|
| r2 × 100 | B b | p-Value | r2 × 100 | β | p-Value | r2 × 100 | β | p-Value | |
| Vomiting (yes/no) | 10.0 | 0.34 | 0.003 | 1.9 | −0.14 | NS | - | - | - |
| Multivitamin use (yes/no) | 4.5 | 0.23 | 0.042 | - | - | - | - | - | - |
| Pre-pregnancy BMI (kg/m2) | 4.2 | −0.22 | 0.047 | - | - | - | 4.5 | −0.20 | NS |
| Nutrition knowledge (score) | 3.5 | 0.21 | NS | 3.5 | 0.19 | NS | 6.8 | 0.26 | 0.017 |
| Living environment c | 3.3 | 0.32 | NS | - | - | - | 6.7 | 0.16 | NS |
| University degree (yes/no) | 1.7 | 0.14 | NS | - | - | - | 2.6 | 0.16 | NS |
| Physical activity (minutes/day) | - | - | - | 7.4 | 0.28 | 0.012 | - | - | - |
| Food cravings (yes/no) | - | - | - | 1.6 | −0.13 | NS | - | - | - |
| Total | 27.3 | 14.4 | 20.6 | ||||||
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Savard, C.; Lemieux, S.; Carbonneau, É.; Provencher, V.; Gagnon, C.; Robitaille, J.; Morisset, A.-S. Trimester-Specific Assessment of Diet Quality in a Sample of Canadian Pregnant Women. Int. J. Environ. Res. Public Health 2019, 16, 311. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph16030311
Savard C, Lemieux S, Carbonneau É, Provencher V, Gagnon C, Robitaille J, Morisset A-S. Trimester-Specific Assessment of Diet Quality in a Sample of Canadian Pregnant Women. International Journal of Environmental Research and Public Health. 2019; 16(3):311. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph16030311
Chicago/Turabian StyleSavard, Claudia, Simone Lemieux, Élise Carbonneau, Véronique Provencher, Claudia Gagnon, Julie Robitaille, and Anne-Sophie Morisset. 2019. "Trimester-Specific Assessment of Diet Quality in a Sample of Canadian Pregnant Women" International Journal of Environmental Research and Public Health 16, no. 3: 311. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph16030311