Associations of Sensor-Derived Physical Behavior with Metabolic Health: A Compositional Analysis in the Record Multisensor Study

 , ,
, , 
Abstract
:1. Introduction
2. Material and Methods
2.1. Study Subjects
2.2. Anthropological and Biological Data
2.3. Physical Activities and Postures
2.4. Other Data
2.5. Data Processing
2.6. Statistical Analysis
- Iso-temporal substitution models: they estimate the change in the health outcome variable associated with time reallocation (in proportion) from a behavior to another, while all other behavior time volumes remain constant. Thus, the models preserve the compositional structure of the data.
- Compositional models: they are identical to the familiar linear regression models, but before including them as regressors in the models, the compositions are transformed from coordinates in the Aitchison simplex for composition to the coordinates in the real space (here, we chose the isometric log ratio (ilr) transformation [35]). Once the coefficients for the compositions are estimated by the models, they are back-transformed to the Aitchison simplex. The independent variable (here, the health variable) is fitted in the same way as in a traditional linear model, but using the Aitchison geometry for compositions [22] (i.e., by taking the Aitchison inner product of the compositional vector and the corresponding coefficient vector, see Appendix A). Thus, we can estimate our health response variable for any composition, or the change in the response variable following any change in a composition, while operating in the appropriate mathematical framework for these data. To illustrate the change in a health outcome associated with a change in a time budget, we created four hypothetical profiles, which represent archetypes of physical activity patterns, and compared the predicted health outcomes for these profiles against the average profile. The four profiles are ‘couch potato’—a time budget with a strong component of lying/reclining postures (lie = 30%, sit = 50%, stand = 10%, LPA = 5%, MVPA = 5%); ‘office worker’—strong component of sitting (lie = 5%, sit = 70%, stand = 10%, LPA = 5%, MVPA = 10%); ‘doorman’—strong component of standing (lie = 5%, sit = 15%, stand = 70%, LPA = 5%, MVPA = 5%); active—strong component of MVPA (lie = 5%, sit = 40%, stand = 30%, LPA = 5%, MVPA = 20%). We implemented the models using the R-package compositions [36] and the handbook by van den Boogaart and Tolosana-Delgado [23].
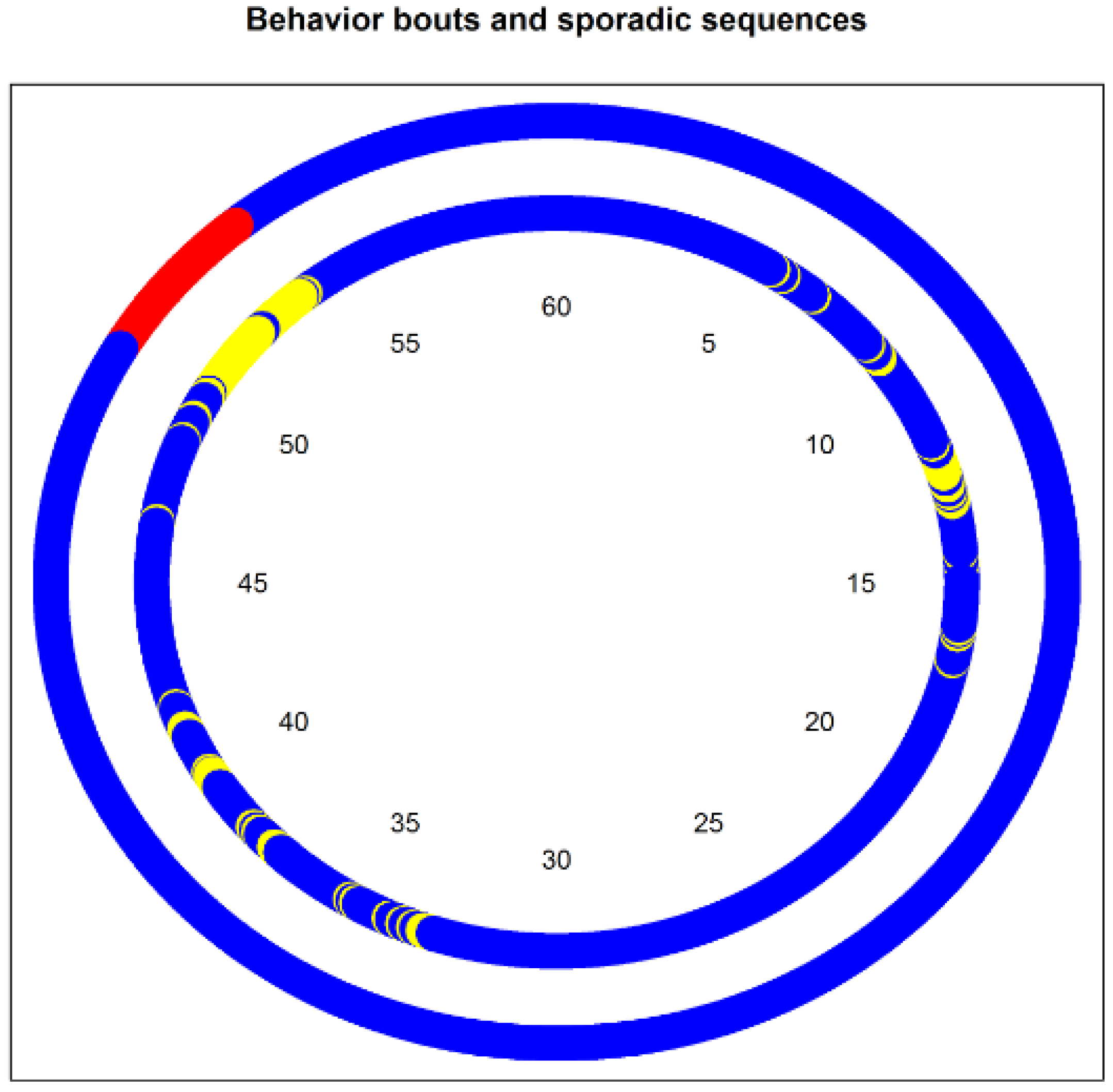
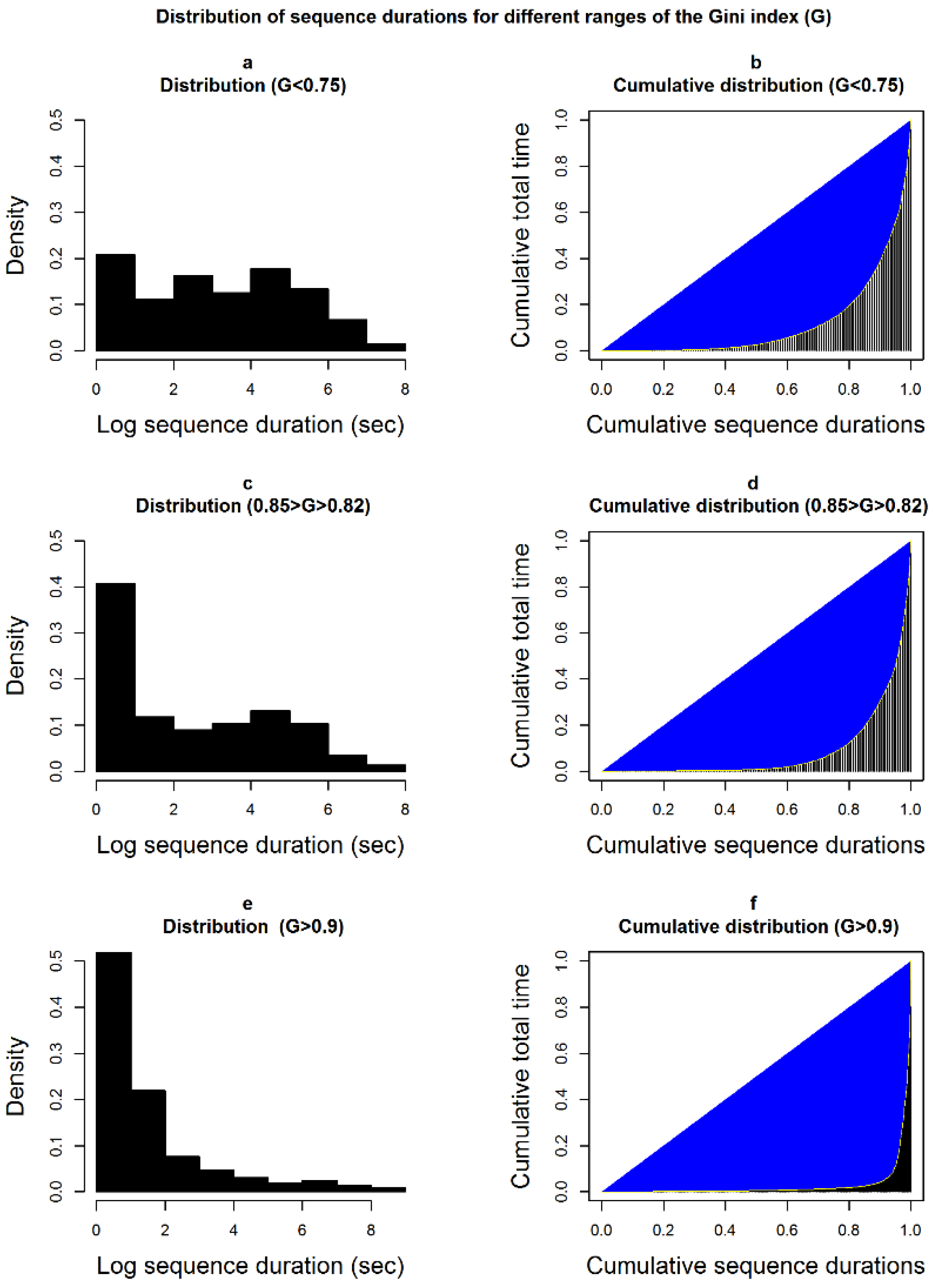
- Linear models for behavior partitioning: these are traditional linear models, which estimate the change in the health outcome associated with the change in a partitioning index. We did not calculate the indices for each behavior, but rather for three broader categories of behaviors (SB, non-SB, and MVPA). To make sure that the association of behavior partitioning with health is independent of the behavior time volumes, we added the behavior time budget (expressed as ilr) to the model as control variable. As partitioning indices, we use the median length of the behaviors bouts, the ratio of the behavior time in bouts to the total behavior time (spent in bouts or not, see Figure 1), and the Gini index of the total time distribution of sequences of different durations (see Figure 2).
3. Results
3.1. Anthropological, Demographics and Biological Characteristics of the Participants
3.2. Daily Pattern of Physical Activity and Sedentary Behaviors
3.3. Associations between Behaviors and Health Outcomes
3.3.1. Blood Glucose Concentration
3.3.2. Low-Density Lipoprotein (LDL), High-Density Lipoprotein (HDL), and Triglycerides
3.3.3. Body Mass Index and Waist Circumference
4. Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
Appendix A
- Colsure C:
- Perturbation :where D is the length of the vector.
- Aitchison’s inner product :
Appendix B

{kind=link}
{kind=link}
| Behavior | Lie | Sit | Stand | LPA | MVPA |
|---|---|---|---|---|---|
| Lie | 1.3334 | −0.3297 | −0.3355 | −0.3016 | −0.3666 |
| Sit | −0.3297 | 0.2170 | 0.0380 | 0.0208 | 0.0539 |
| Stand | −0.3355 | 0.0380 | 0.1636 | 0.0865 | 0.0475 |
| LPA | −0.3016 | 0.0208 | 0.0865 | 0.1265 | 0.0678 |
| MVPA | −0.3666 | 0.0539 | 0.0475 | 0.0678 | 0.1974 |
Appendix C
| Name of Variable | Type of Variable | Value |
|---|---|---|
| Education | Continuous | 0 = No diploma 1 = Certificat d’études primaire (completion primary school) 2 = Brevet élémentaire ou équivalent (completion of four first year of secondary education) 3 = Certificat d’aptitude professionnelle/Brevet d’études professionnelles (completion of 6 years of secondary vocational education) 4 = Baccalauréat professionnel (completion of vocational secondary cycle) 5 = Baccalauréat general (completion of general secondary cycle) 6 = Bac + 2 (completion of two years of higher education) 7 = Bac + 3 or Bac + 4 (Bachelor’s degree) 8 = Bac + 5 or doctorat (Master’s degree or higher) |
| Income (Total net revenues of household) | Continuous | 0 ≤ 500 € 1 = 500–1000 € 2 = 1000–1500 € 3 = 1500–2000 € 4 = 2000–3000 € 5 = 3000–4000 € 6 = 4000–5000 € 7 = 5000–6000 € 8 = 6000–7000 € 9 ≥ 7000 € |
| Nutritional habits | The first two dimensions of a principal component analysis including all variables were used as continuous variables. | Intake of olive oil, vegetables, fruits, juice, meat, dairy products, desserts, sodas, wine, legume, fish, pizza, lean meat, nuts, commercial desserts; preference of olive oil over other oils; whether usually eats between meals |
References
- Warburton, D.E.R.; Nicol, C.W.; Bredin, S.S.D. Health benefits of physical activity: The evidence. CMAJ 2006, 174, 801–809. [Google Scholar] [CrossRef] [PubMed]
- Kohl, H.W., 3rd; Craig, C.L.; Lambert, E.V.; Inoue, S.; Alkandari, J.R.; Leetongin, G.; Kahlmeier, S.; Lancet Physical Activity Series Working Group. The pandemic of physical inactivity: Global action for public health. Lancet 2012, 380, 294–305. [Google Scholar] [CrossRef]
- Lee, I.M.; Shiroma, E.J.; Lobelo, F.; Puska, P.; Blair, S.N.; Katzmarzyk, P.T.; Lancet Physical Activity Series Working Group. Effect of physical inactivity on major non-communicable diseases worldwide: An analysis of burden of disease and life expectancy. Lancet 2012, 380, 219–229. [Google Scholar] [CrossRef]
- Healy, G.N.; Wijndaele, K.; Dunstan, D.W.; Shaw, J.E.; Salmon, J.; Zimmet, P.Z.; Owen, N. Objectively measured sedentary time, physical activity, and metabolic risk: The Australian Diabetes, Obesity and Lifestyle Study (AusDiab). Diabetes Care 2008, 31, 369–371. [Google Scholar] [CrossRef] [PubMed]
- Thorp, A.A.; Owen, N.; Neuhaus, M.; Dunstan, D.W. Sedentary behaviors and subsequent health outcomes in adults a systematic review of longitudinal studies, 1996–2011. Am. J. Prev. Med. 2011, 41, 207–215. [Google Scholar] [CrossRef] [PubMed]
- Wilmot, E.G.; Edwardson, C.L.; Achana, F.A.; Davies, M.J.; Gorely, T.; Gray, L.J.; Khunti, K.; Yates, T.; Biddle, S.J. Sedentary time in adults and the association with diabetes, cardiovascular disease and death: Systematic review and meta-analysis. Diabetologia 2012, 55, 2895–2905. [Google Scholar] [CrossRef] [PubMed]
- Andersen, E.; Ekelund, U.; Anderssen, S.A. Effects of Reducing Sedentary Time on Glucose Metabolism in Immigrant Pakistani Men. Med. Sci. Sports Exerc. 2015, 47, 775–781. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Howard, R.A.; Freedman, D.M.; Park, Y.; Hollenbeck, A.; Schatzkin, A.; Leitzmann, M.F. Physical activity, sedentary behavior, and the risk of colon and rectal cancer in the NIH-AARP Diet and Health Study. Cancer Causes Control 2008, 19, 939–953. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gierach, G.L.; Chang, S.C.; Brinton, L.A.; Lacey, J.V., Jr.; Hollenbeck, A.R.; Schatzkin, A.; Leitzmann, M.F. Physical Activity, Sedentary Behavior, and Endometrial Cancer Risk in the NIH-AARP Diet and Health Study. Int. J. Cancer 2009, 124, 2139–2147. [Google Scholar] [CrossRef] [PubMed]
- Hamilton, M.T.; Hamilton, D.G.; Zderic, T.W. Exercise physiology versus inactivity physiology: An essential concept for understanding lipoprotein lipase regulation. Exerc. Sport Sci. Rev. 2004, 32, 161–166. [Google Scholar] [CrossRef] [PubMed]
- Owen, N.; Healy, G.N.; Matthews, C.E.; Dunstan, D.W. Too Much Sitting: The Population-Health Science of Sedentary Behavior. Exerc. Sport Sci. Rev. 2010, 38, 105–113. [Google Scholar] [CrossRef] [PubMed]
- Sedentary Behaviour Research Network. Letter to the editor: Standardized use of the terms “sedentary” and “sedentary behaviours”. Appl. Physiol. Nutr. Metab. 2012, 37, 540–542. [Google Scholar] [CrossRef] [PubMed]
- Tremblay, M.S.; Aubert, S.; Barnes, J.D.; Saunders, T.J.; Carson, V.; Latimer-Cheung, A.E.; Chastin, S.F.; Altenburg, T.M.; Chinapaw, M.J. Sedentary Behavior Research Network (SBRN)—Terminology Consensus Project process and outcome. Int. J. Behav. Nutr. Phys. Act. 2017, 14, 75. [Google Scholar] [CrossRef] [PubMed]
- Gibbs, B.B.; Hergenroeder, A.L.; Katzmarzyk, P.T.; Lee, I.-M.; Jakicic, J.M. Definition, Measurement, and Health Risks Associated with Sedentary Behavior. Med. Sci. Sports Exerc. 2015, 47, 1295–1300. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Alkhajah, T.A.; Reeves, M.M.; Eakin, E.G.; Winkler, E.A.H.; Owen, N.; Healy, G.N. Sit-stand workstations: A pilot intervention to reduce office sitting time. Am. J. Prev. Med. 2012, 43, 298–303. [Google Scholar] [CrossRef] [PubMed]
- Pulsford, R.M.; Blackwell, J.; Hillsdon, M.; Kos, K. Intermittent walking, but not standing, improves postprandial insulin and glucose relative to sustained sitting: A randomised cross-over study in inactive middle-aged men. J. Sci. Med. Sport 2017, 20, 278–283. [Google Scholar] [CrossRef] [PubMed]
- Bellettiere, J.; Winkler, E.A.; Chastin, S.F.; Kerr, J.; Owen, N.; Dunstan, D.W.; Healy, G.N. Associations of sitting accumulation patterns with cardio-metabolic risk biomarkers in Australian adults. PLoS ONE 2017, 12, e0180119. [Google Scholar] [CrossRef] [PubMed]
- Biddle, G.; Edwardson, C.; Henson, J.; Davies, M.; Khunti, K.; Rowlands, A.; Yates, T. Associations of Physical Behaviours and Behavioural Reallocations with Markers of Metabolic Health: A Compositional Data Analysis. Int. J. Environ. Res. Public Health 2018, 15, 2280. [Google Scholar] [CrossRef] [PubMed]
- Chastin, S.F.M.; Granat, M.H. Methods for objective measure, quantification and analysis of sedentary behaviour and inactivity. Gait Posture 2010, 31, 82–86. [Google Scholar] [CrossRef] [PubMed]
- Healy, G.N.; Matthews, C.E.; Dunstan, D.W.; Winkler, E.A.H.; Owen, N. Sedentary time and cardio-metabolic biomarkers in US adults: NHANES 2003–06. Eur. Heart J. 2011, 32, 590–597. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dunstan, D.W.; Kingwell, B.A.; Larsen, R.; Healy, G.N.; Cerin, E.; Hamilton, M.T.; Shaw, J.E.; Bertovic, D.A.; Zimmet, P.Z.; Salmon, J.; et al. Breaking Up Prolonged Sitting Reduces Postprandial Glucose and Insulin Responses. Diabetes Care 2012, 35, 976–983. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Aitchison, J. The statistical Analysis of Compositional Data; Blackburn Press: Caldwell, NJ, USA, 2003. [Google Scholar]
- Van den Boogaart, G.; Tolosana-Delgado, R. Analyzing Compositional Data with R; Springer: Berlin, Germany, 2013. [Google Scholar]
- Pedišić, Ž.; Dumuid, D.; Olds, T.S. Integrating sleep, sedentary behaviour, and physical activity research in the emerging field of time-use epidemiology: Definitions, concepts, statistical methods, theoretical framework, and future directions. Kinesiology 2017, 49, 252–269. [Google Scholar]
- Mekary, R.A.; Willett, W.C.; Hu, F.B.; Ding, E.L. Isotemporal substitution paradigm for physical activity epidemiology and weight change. Am. J. Epidemiol. 2009, 170, 519–527. [Google Scholar] [CrossRef] [PubMed]
- Healy, G.N.; Winkler, E.A.H.; Owen, N.; Anuradha, S.; Dunstan, D.W. Replacing sitting time with standing or stepping: Associations with cardio-metabolic risk biomarkers. Eur. Heart J. 2015, 36, 2643–2649. [Google Scholar] [CrossRef] [PubMed]
- Fairclough, S.J.; Dumuid, D.; Taylor, S.; Curry, W.; McGrane, B.; Stratton, G.; Maher, C.; Olds, T. Fitness, fatness and the reallocation of time between children’s daily movement behaviours: An analysis of compositional data. Int. J. Behav. Nutr. Phys. Act. 2017, 14, 64. [Google Scholar] [CrossRef] [PubMed]
- Talarico, R.; Janssen, I. Compositional associations of time spent in sleep, sedentary behavior and physical activity with obesity measures in children. Int. J. Obes. 2018, 42, 1508–1514. [Google Scholar] [CrossRef] [PubMed]
- El Aarbaoui, T.; Méline, J.; Brondeel, R.; Chaix, B. Short-term association between personal exposure to noise and heart rate variability: The RECORD MultiSensor Study. Environ. Pollut. 2017, 231 Pt 1, 703–711. [Google Scholar] [CrossRef] [PubMed]
- Chaix, B.; Jouven, X.; Thomas, F.; Leal, C.; Billaudeau, N.; Bean, K.; Kestens, Y.; Jëgo, B.; Pannier, B.; Danchin, N. Why socially deprived populations have a faster resting heart rate: Impact of behaviour, life course anthropometry, and biology—The RECORD Cohort Study. Soc. Sci. Med. 2011, 73, 1543–1550. [Google Scholar] [CrossRef] [PubMed]
- Troiano, R.P.; Berrigan, D.; Dodd, K.W.; MâSse, L.C.; Tilert, T.; Mcdowell, M. Physical Activity in the United States Measured by Accelerometer. Med. Sci. Sports Exerc. 2008, 40, 181–188. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lyden, K. ActivpalProcessing: Process activPAL Events Files. 2016. Available online: https://CRAN.R-project.org/package=activpalProcessing (accessed on 17 October 2018).
- Bowman, S.A. Television-viewing characteristics of adults: Correlations to eating practices and overweight and health status. Prev. Chronic Dis. 2006, 3, A38. [Google Scholar] [PubMed]
- Chaix, B.; Kestens, Y.; Bean, K.; Leal, C.; Karusisi, N.; Meghiref, K.; Burban, J.; Fon Sing, M.; Perchoux, C.; Thomas, F.; et al. Cohort profile: Residential and non-residential environments, individual activity spaces and cardiovascular risk factors and diseases—The RECORD Cohort Study. Int. J. Epidemiol. 2012, 41, 1283–1292. [Google Scholar] [CrossRef] [PubMed]
- Egozcue, J.J.; Pawlowsky-Glahn, V.; Mateu-Figueras, G.; Barceló-Vidal, C. Isometric Logratio Transformations for Compositional Data Analysis. Math. Geol. 2003, 35, 279–300. [Google Scholar] [CrossRef]
- Van den Boogaart, K.G.; Tolosana-Delgado, R.; Bren, M. Compositions: Compositional Data Analysis. 2018. Available online: https://CRAN.R-project.org/package=compositions (accessed on 19 October 2018).
- R Core Team. R: A Language and Environment for Statistical Computing; R Foundation for Statistical Computing: Vienna, Austria, 2018; Available online: https://www.R-project.org/ (accessed on 19 October 2018).
- IDF Consensus Worldwide Definition of the Metabolic Syndrome. Available online: https://www.idf.org/our-activities/advocacy-awareness/resources-and-tools/60:idfconsensus-worldwide-definitionof-the-metabolic-syndrome.html (accessed on 31 January 2019).
- Chaix, B.; Billaudeau, N.; Thomas, F.; Havard, S.; Evans, D.; Kestens, Y.; Bean, K. Neighborhood effects on health: Correcting bias from neighborhood effects on participation. Epidemiology 2011, 22, 18–26. [Google Scholar] [CrossRef] [PubMed]
- Mann, S.; Beedie, C.; Jimenez, A. Differential Effects of Aerobic Exercise, Resistance Training and Combined Exercise Modalities on Cholesterol and the Lipid Profile: Review, Synthesis and Recommendations. Sports Med. 2014, 44, 211–221. [Google Scholar] [CrossRef] [PubMed]
- Miles-Chan, J.L.; Dulloo, A.G. Posture Allocation Revisited: Breaking the Sedentary Threshold of Energy Expenditure for Obesity Management. Front. Physiol. 2017, 8. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tikkanen, O.; Haakana, P.; Pesola, A.J.; Häkkinen, K.; Rantalainen, T.; Havu, M.; Pullinen, T.; Finni, T. Muscle Activity and Inactivity Periods during Normal Daily Life. PLoS ONE 2013, 8, e52228. [Google Scholar] [CrossRef] [PubMed]
- Richter, E.A.; Hargreaves, M. Exercise, GLUT4, and skeletal muscle glucose uptake. Physiol. Rev. 2013, 93, 993–1017. [Google Scholar] [CrossRef] [PubMed]
- Carson, V.; Wong, S.L.; Winkler, E.; Healy, G.N.; Colley, R.C.; Tremblay, M.S. Patterns of sedentary time and cardiometabolic risk among Canadian adults. Prev. Med. 2014, 65, 23–27. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jefferis, B.J.; Parsons, T.J.; Sartini, C.; Ash, S.; Lennon, L.T.; Wannamethee, S.G.; Lee, I.M.; Whincup, P.H. Does duration of physical activity bouts matter for adiposity and metabolic syndrome? A cross-sectional study of older British men. Int. J. Behav. Nutr. Phys. Act. 2016, 13, 36. [Google Scholar] [CrossRef] [PubMed]
- Scientific Report—2018 Physical Activity Guidelines—Health.gov. Available online: https://health.gov/paguidelines/second-edition/report/ (accessed on 10 December 2018).
- Ekelund, U.; Brage, S.; Besson, H.; Sharp, S.; Wareham, N.J. Time spent being sedentary and weight gain in healthy adults: Reverse or bidirectional causality? Am. J. Clin. Nutr. 2008, 88, 612–617. [Google Scholar] [CrossRef] [PubMed]


| Descriptive Statistics of Physical Activity and Postures | Mean | SD | Min | Max |
|---|---|---|---|---|
| PHYSCIAL ACTIVTIES & POSTURES (time proportions) | ||||
| Lying | 0.0968 | 0.0960 | 0.0002 | 0.5363 |
| Sitting | 0.5157 | 0.1208 | 0.2275 | 0.7544 |
| Standing | 0.2713 | 0.0961 | 0.0925 | 0.6570 |
| LPA | 0.0358 | 0.0140 | 0.0109 | 0.0950 |
| MVPA | 0.0804 | 0.0330 | 0.0168 | 0.1798 |
| PARTITIONING INDICES (sedentary) | ||||
| Median length (minutes) | 6.58 | 2.72 | 1.73 | 15.43 |
| Gini | 0.7990 | 0.0608 | 0.6703 | 0.9368 |
| Ratio (bouts/total) | 0.9770 | 0.0196 | 0.8574 | 0.9958 |
| PARTITIONING INDICES (non-sedentary) | ||||
| Median length (minutes) | 4.37 | 1.59 | 1.52 | 10.90 |
| Gini | 0.8367 | 0.0502 | 0.7224 | 0.9365 |
| Ratio (bouts/total) | 0.9613 | 0.0336 | 0.7788 | 0.9964 |
| PARTITIONING INDICES (MVPA) | ||||
| Median length (minutes) | 1.80 | 0.66 | 1.00 | 5.18 |
| Gini index | 0.5954 | 0.0948 | 0.3301 | 0.8159 |
| Ratio (bouts/total) | 0.5280 | 0.1541 | 0.0797 | 0.8828 |
| Descriptive Statistics of Health and Control Variables | Mean | SD | Min | Max |
|---|---|---|---|---|
| Glucose (mg/dL) | 96 | 9 | 75 | 123 |
| LDL (mg/dL) | 160 | 38 | 82 | 252 |
| HDL (mg/dL) | 53 | 13 | 25 | 98 |
| Triglycerides (mg/dL) | 109 | 54 | 40 | 306 |
| BMI (kg/m2) | 25.77 | 3.89 | 16.03 | 37.56 |
| Waist Circumference (cm) | 87.34 | 12.17 | 57.00 | 116.00 |
| Sex (0 = female) | 0.64 | |||
| Age (years) | 50.55 | 9.57 | 34.00 | 83.00 |
| Education (categorical) | 5.66 | 2.16 | 0.00 | 9.00 |
| Income (categorical) | 6.66 | 2.71 | 0.00 | 9.00 |
| Nutritional index 1 | 0.00 | 1.55 | −3.94 | 3.08 |
| Nutritional index 2 | 0.00 | 1.37 | −3.19 | 4.62 |
| Results of iso-Temporal Substitution Models (Coefficients and 95% Confidence Intervals) | |||||
|---|---|---|---|---|---|
| Health Outcome | Behavior | Lie | Sit | Stand | LPA |
| GLUCOSE (mg/dL) | sit | −1.67 [−19.71; 16.37] | |||
| stand | −9.76 [−33.16; 13.63] | −8.09 [−27.34; 11.15] | |||
| LPA | 61.27 [−81.08; 203.62] | 62.94 [−78.69; 204.57] | 71.03 [−80.05; 222.12] | ||
| MVPA | −18.55 [−74.84; 37.74] | −16.88 [−73.26; 39.5] | −8.79 [−66.32; 48.74] | −79.82 [−254.1; 94.45] | |
| LDL (mg/dL) | sit | −60.66 [−134.8; 13.48] | |||
| stand | −41.59 [−138.16; 54.98] | 19.07 [−60.75; 98.89] | |||
| LPA | 136.35 [−453.69; 726.4] | 197.02 [−390.29; 784.32] | 177.95 [−448.61; 804.5] | ||
| MVPA | −251.97 * [−484.86; −19.08] | −191.31 [−425.06; 42.45] | −210.38 † [−448.89; 28.14] | −388.32 [−1111.13; 334.48] | |
| HDL (mg/dL) | sit | −5.07 [−27.36; 17.22] | |||
| stand | 18.87 [−10.17; 47.9] | 23.93 * [−0.07; 47.94] | |||
| LPA | −83.91 [−261.32; 93.5] | −78.84 [−255.43; 97.75] | −102.77 [−291.17; 85.62] | ||
| MVPA | 32.1 [−37.92; 102.13] | 37.17 [−33.11; 107.46] | 13.24 [−58.48; 84.95] | 116.01 [−101.32; 333.34] | |
| log TRIGLYCERIDES (mg/dL) | sit | −0.58 [−1.35; 0.19] | |||
| stand | −1.33 ** [−2.33; −0.32] | −0.74 † [−1.58; 0.09] | |||
| LPA | 3 [−3.14; 9.15] | 3.59 [−2.53; 9.7] | 4.33 [−2.2; 10.86] | ||
| MVPA | −4 *** [−6.43; −1.57] | −3.42 ** [−5.85; −0.98] | −2.67 * [−5.16; −0.19] | −7 † [−14.53; 0.53] | |
| log BMI (kg/m2) | sit | −0.45 *** [−0.7; −0.2] | |||
| stand | −0.33 † [−0.67; 0.01] | 0.13 [−0.16; 0.41] | |||
| LPA | −1.04 [−3.13; 1.05] | −0.59 [−2.68; 1.5] | −0.71 [−2.94; 1.51] | ||
| MVPA | −0.32 [−1.15; 0.51] | 0.13 [−0.7; 0.97] | 0.01 [−0.84; 0.86] | 0.72 [−1.85; 3.3] | |
| WAIST CIRCUMFERENCE (cm) | sit | −33.53 *** [−49.18; −17.87] | |||
| stand | −34.28 *** [−55.5; −13.06] | −0.75 [−18.39; 16.88] | |||
| LPA | −6 [−136.1; 124.11] | 27.53 [−102.5; 157.56] | 28.28 [−110.33; 166.89] | ||
| MVPA | −55.69 * [−107.27; −4.1] | −22.16 [−74.12; 29.79] | −21.41 [−74.38; 31.56] | −49.69 [−209.93; 110.54] | |
| Results of Compositional Models | ||||||
|---|---|---|---|---|---|---|
| COEFFICIENT VECTORS | ||||||
| Glucose | LDL | HDL | Log Trigl. | Log BMI | Waist Circum. | |
| lie | 0.3547 | 0.0198 | 0.0094 | 0.209 | 0.2053 | 0.748 |
| sit | 0.2318 | 0.0001 | 0.0008 | 0.23 | 0.1948 | 0.0563 |
| stand | 0.0361 | 0.0051 | 0.7822 | 0.1814 | 0.2002 | 0.0305 |
| LPA | 0.3041 | 0.975 | 0.0075 | 0.2188 | 0.1968 | 0.14 |
| MVPA | 0.0732 | <0.0001 | 0.2001 | 0.1608 | 0.203 | 0.0253 |
| p-value of the model | 0.5326 | 0.2033 | 0.1858 | 0.0097 | 0.0208 | 0.0006 |
| NORMALIZED COEFFICIENT VECTORS | ||||||
| lie | 0.2854 | 0.2347 | 0.1521 | 0.2183 | 0.3327 | 0.3924 |
| sit | 0.2305 | 0.1721 | 0.0975 | 0.3025 | 0.0987 | 0.1542 |
| stand | 0.0906 | 0.2167 | 0.3394 | 0.1347 | 0.1855 | 0.1236 |
| LPA | 0.2642 | 0.296 | 0.1461 | 0.2551 | 0.1253 | 0.2143 |
| MVPA | 0.1293 | 0.0805 | 0.265 | 0.0895 | 0.2578 | 0.1155 |
| Vector norm | 1.99 | 16.82 | 5.51 | 0.29 | 0.04 | 2.77 |
| PREDICTED VALUES compared to mean composition | ||||||
| Composition (%) [lie, sit, stand, LPA, MVPA] | Diff. | Diff. | Diff. | Ratio | Ratio | Diff. |
| [30,50,10,5,5]: ‘couch potato’ | 3.21 | 13.81 | −6.25 | 1.35 | 1.03 | 5.46 |
| [5,70,10,5,10]: ‘office worker’ | 1.36 | −3.67 | −4.22 | 1.12 | 0.99 | 0.58 |
| [5,15,70,5,5]: ‘doorman’ | −1.35 | 12.38 | 6.35 | 0.86 | 1.02 | 0.07 |
| [5,40,30,5,20]: ‘active’ | −0.82 | −9.79 | 2.96 | 0.8 | 1.01 | −1.16 |
| Results of Partitioning Models (Coefficients and 95% Confidence Intervals) | ||||||
|---|---|---|---|---|---|---|
| Index | Glucose | LDL | HDL | log Triglycerides | log BMI | Waist Circumf. |
| SEDENTARY BEHAVIORS | ||||||
| Median (min.) | −0.41 [−1.1; 0.28] | −0.98 [−3.88; 1.92] | −0.51 [−1.37; 0.36] | 0 [−0.03; 0.03] | 0 [−0.01; 0.01] | −0.12 [−0.77; 0.53] |
| Gini | −29.8 * [−56.73; −2.87] | 52.19 [−61.82; 166.21] | −6.82 [−40.93; 27.3] | 0.13 [−1.07; 1.34] | −0.16 [−0.57; 0.25] | −11.2 [−36.87; 14.46] |
| Ratio | −3944.26 * [−7423.65; −464.88] | 24.26 [−424.35; 472.86] | 28.55 [−105.22; 162.33] | 0.79 [−3.94; 5.53] | 1.45 † [−0.12; 3.03] | 26.26 [−72.96; 125.49] |
| Ratio2 | 2047.4 * [195.41; 3899.39] | |||||
| NON-SEDENTARY BEHAVIORS | ||||||
| Median (min.) | −4.75 * [−9.31; −0.19] | 2.31 [−3.07; 7.68] | −1.61 * [−3.19; −0.02] | 0.02 [−0.04; 0.08] | 0.02 ** [0.01; 0.04] | 0.83 [−0.34; 1.99] |
| Median2 (min.) | 0.39 * [0.01; 0.77] | |||||
| Gini | 13.31 [−20.3; 46.93] | 123.44 † [−15.92; 262.81] | 8.68 [−33.42; 50.77] | 1.13 [−0.34; 2.61] | 0.67 *** [0.21; 1.14] | 25.05 † [−4.61; 54.7] |
| Ratio | −46.65 [−107.6; 14.3] | −33.56 [−291.17; 224.06] | −63.7 † [−139.72; 12.31] | 0.61 [−2.11; 3.32] | 0.28 [−0.64; 1.21] | −2.76 [−60.41; 54.9] |
| MVPA | ||||||
| Median (min.) | −0.03 [−2.52; 2.46] | 2.29 [−8.12; 12.69] | −0.14 [−3.25; 2.97] | −0.03 [−0.14; 0.08] | −0.01 [−0.05; 0.02] | −1.79 [−4.09; 0.52] |
| Gini | −1 [−21.87; 19.86] | 18.45 [−68.83; 105.73] | 9.6 [−16.41; 35.6] | −0.38 [−1.3; 0.54] | −0.12 [−0.44; 0.19] | −8.47 [−27.91; 10.96] |
| Ratio | −1.09 [−13.77; 11.6] | 13.5 [−39.56; 66.57] | 3.82 [−12.02; 19.65] | −0.2 [−0.76; 0.35] | −0.05 [−0.24; 0.14] | −2.35 [−14.22; 9.52] |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Debache, I.; Bergouignan, A.; Chaix, B.; Sneekes, E.M.; Thomas, F.; Sueur, C. Associations of Sensor-Derived Physical Behavior with Metabolic Health: A Compositional Analysis in the Record Multisensor Study. Int. J. Environ. Res. Public Health 2019, 16, 741. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph16050741
Debache I, Bergouignan A, Chaix B, Sneekes EM, Thomas F, Sueur C. Associations of Sensor-Derived Physical Behavior with Metabolic Health: A Compositional Analysis in the Record Multisensor Study. International Journal of Environmental Research and Public Health. 2019; 16(5):741. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph16050741
Chicago/Turabian StyleDebache, Isaac, Audrey Bergouignan, Basile Chaix, Emiel M Sneekes, Frédérique Thomas, and Cédric Sueur. 2019. "Associations of Sensor-Derived Physical Behavior with Metabolic Health: A Compositional Analysis in the Record Multisensor Study" International Journal of Environmental Research and Public Health 16, no. 5: 741. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph16050741