Years of Life Lost Due to Cervical Cancer in Poland in 2000 to 2015


Abstract
:1. Introduction
2. Materials and Methods
3. Results
4. Discussion
5. Limitations
6. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Bray, F.; Ferlay, J.; Soerjomataram, I.; Siegel, R.L.; Torre, L.A.; Jemal, A. Global Cancer Statistics 2018: GLOBOCAN Estimates of Incidence and Mortality Worldwide for 36 Cancers in 185 Countries. CA Cancer J. Clin. 2018, 68, 394–424. [Google Scholar] [CrossRef]
- WHO/ICO Information Center of HPV and Cervical Cancer (HPV Information Center). Human Papillomavirus and Related Diseases Report. Summary Report 2017. Available online: http://www.hpvcentre.net/statistics/reports/XWX.pdf (accessed on 24 June 2018).
- Fitzmaurice, C.; Allen, C.; Barber, R.M.; Barregard, L.; Bhutta, Z.A.; Brenner, H.; Fleming, T. Global, regional, and national cancer incidence, mortality, years of life lost, years lived with disability, and disability-adjusted life-years for 32 cancer groups, 1990 to 2015: A systematic analysis for the global burden of disease study. JAMA Oncol. 2017, 3, 524–548. [Google Scholar] [CrossRef]
- Fitzmaurice, C.; Dicker, D.; Pain, A.; Hamavid, H.; Moradi-Lakeh, M.; Maclntyre, M.F.; Hamadeh, R.R. The Global Burden of Cancer 2013. Global Burden of Disease Cancer Collaboration. JAMA Oncol. 2015, 1, 505–527. [Google Scholar] [CrossRef] [PubMed]
- Arbyn, M.; Raifu, A.O.; Weiderpass, E.; Bray, F.; Anttila, A. Trends of cervical cancer mortality in the member states of the European Union. Eur. J. Cancer 2009, 45, 2640–2648. [Google Scholar] [CrossRef]
- Wojciechowska, U.; Didkowska, J. Changes in five-year relative survival rates in Poland in patients diagnosed in the years 1999–2010. Nowotw. J. Oncol. 2017, 67, 349–358. [Google Scholar] [CrossRef]
- Sant, M.; Lopez, M.; Agresti, R.; Sánchez Pérez, M.J.; Holleczek, B.; Bielska-Lasota, M.; Dimitrova, N.; Innos, K.; Katalinic, A.; Langseth, H.; et al. Survival of women with cancers of breast and genital organs in Europe 1999–2007: Results of the EUROCARE-5 study. Eur. J. Cancer 2015, 51, 2191–2205. [Google Scholar] [CrossRef] [PubMed]
- Torre, L.A.; Islami, F.; Siegel, R.L.; Ward, E.M.; Jemal, A. Global Cancer in Women: Burden and Trends. Cancer Epidemiol. Biomark. Prev. 2017, 26, 444–457. [Google Scholar] [CrossRef]
- Campos, N.G.; Sharma, M.; Clarc, A.; Lee, K.; Geng, F.; Regan, C.; Kim, J.; Resch, S. The health and economic impact of scaling cervical cancer prevention in 50 low- and lower-middle-income countries. Int. J. Gynecol. Obstet. 2017, 138, 47–56. [Google Scholar] [CrossRef] [Green Version]
- Penner, D.; Pinheiro, P.; Krämer, A. Measuring the burden of disease due to premature mortality using standard expected years of life lost (SEYLL) in North Rhine-Westphalia, a federal state of Germany, in 2005. J. Public Health 2010, 18, 319–325. [Google Scholar] [CrossRef]
- Genova-Maleras, R.; Catala-Lopez, F.; de Larrea-Baz, N.; Alvarez-Martin, E.; Morant-Ginestar, C. The burden of premature mortality in Spain using standard expected years of life lost: A population-based study. BMC Public Health 2011, 11, 787. [Google Scholar] [CrossRef]
- Plass, D.; Kwan Chau, Y.; Thach, T.Q.; Jahn, H.J.; Lai, P.C.; Wong, C.M.; Kraemer, A. Quantifying the burden of disease due to premature mortality in Hong Kong using standard expected years of life lost. BMC Public Health 2013, 13, 863. [Google Scholar] [CrossRef]
- Castillo-Rodríguez, L.; Díaz-Jiménez, D.; Castañeda-Orjuela, C.; De la Hoz-Restrepo, F. Years of Life Lost (YLL) in Colombia 1998–2011: Overall and avoidable causes of death analysis. PLoS ONE 2015, 10, e0125456. [Google Scholar] [CrossRef]
- Pikala, M.; Maniecka-Bryła, I. Fifteen-year mortality trends in Poland analysed with the use of standard expected years of life lost, 2000–2014. Sci. Rep. 2017, 7, 8730. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pikala, M.; Bryla, M.; Bryla, P.; Maniecka-Bryla, I. Years of life lost due to external causes of death in the Lodz province, Poland. PLoS ONE 2014, 9, e96830. [Google Scholar] [CrossRef] [PubMed]
- Revision of the European Standard Population. Available online: https://ec.europa.eu/eurostat/documents/3859598/5926869/KS-RA-13-028-EN.PDF/e713fa79-1add-44e8-b23d-5e8fa09b3f8f (accessed on 2 June 2018).
- Murray, C.J.; Lopez, A.D. Global Burden of Diseases; University Medical Publishing House Vesalius: Warsaw, Poland, 2000; ISBN 83-85688-63-3. [Google Scholar]
- WHO Methods and Data Sources for Global Burden of Disease Estimates 2000–2011. Available online: https://www.who.int/healthinfo/statistics/GlobalDALYmethods_2000_2011 (accessed on 16 June 2018).
- Marshall, R.J. Standard Expected Years of Life Lost as a measure of disease burden: An investigation of its presentation, meaning and interpretation. In Handbook of Disease Burdens and Quality of Life Measures; Preedy, V.R., Watson, R.R., Eds.; Springer: New York, NY, USA, 2010; pp. 401–413. ISBN 978-0-387-78664-3. [Google Scholar]
- Kim, H.; Fay, M.P.; Feuer, E.J.; Midthune, D.N. Permutation tests for joinpoint regression with applications to cancer rates. Stat. Med. 2000, 19, 335–351. [Google Scholar] [CrossRef]
- Mackenbach, J.P.; Kunst, A.E. Measuring the magnitude of socio-economic inequalities in health: An overview of available measures illustrated with two examples from Europe. Soc. Sci. Med. 1997, 44, 757–771. [Google Scholar] [CrossRef]
- Goodman, A. HPV testing as a screen for cervical cancer. BMJ Br. Med. J. 2015, 350, h2372. [Google Scholar] [CrossRef]
- Chelimo, C.; Wouldes, T.A.; Cameron, L.D.; Elwood, J.M. Risk factors for and prevention of human papillomaviruses (HPV), genital warts and cervical cancer. J. Infect. 2013, 66, 207–217. [Google Scholar] [CrossRef]
- Roura, E.; Castellsagué, X.; Pawlita, M.; Travier, N.; Waterboer, T.; Margall, N.; Bosch, F.X.; de Sanjosé, S.; Dillner, J.; Gram, I.T.; et al. Smoking as a major risk factor for cervical cancer and pre-cancer: Results from the EPIC cohort. Int. J. Cancer 2014, 135, 453–466. [Google Scholar] [CrossRef] [Green Version]
- Lam, J.U.; Rebolj, M.; Dugué, P.A.; Bonde, J.; von Euler-Chelpin, M.; Lynge, E. Condom use in prevention of Human Papillomavirus infections and cervical neoplasia: Systematic review of longitudinal studies. J. Med. Screen. 2014, 21, 38–50. [Google Scholar] [CrossRef]
- Nowakowski, A.; Wojciechowska, U.; Wieszczy, P.; Cybulski, M.; Kamiński, M.; Didkowska, J. Trends in cervical cancer incidence and mortality in Poland: Is there an impact of the introduction of the organised screening? Eur. J. Epidemiol. 2017, 32, 529–532. [Google Scholar] [CrossRef]
- Maniecka-Bryła, I.; Bryła, M.; Bryła, P.; Pikala, M. The burden of premature mortality in Poland analysed with the use of standard expected years of life lost. BMC Public Health 2015, 15, 101. [Google Scholar] [CrossRef]
- Ponti, A.; Anttila, A.; Ronco, G.; Senore, C. Cancer Screening in the European Union; International Agency for Research on Cancer: Lyon, France, 2017. [Google Scholar]
- Pikala, M.; Burzynska, M.; Pikala, R.; Bryła, M.; Maniecka-Bryła, I. Educational inequalities in premature mortality in Poland, 2002–2011: A population-based cross-sectional study. BMJ Open 2016, 6, e011501. [Google Scholar] [CrossRef]
- Singh, G.K.; Azuine, R.E.; Siahpush, M. Global Inequalities in Cervical Cancer Incidence and Mortality are Linked to Deprivation, Low Socioeconomic Status, and Human Development. Int. J. MCH AIDS 2012, 1, 17–30. [Google Scholar] [CrossRef]
- Franceschi, S.; Plummer, M.; Clifford, G.; de Sanjose, S.; Bosch, X.; Herrero, R.; Muñoz, N.; Vaccarella, S. Differences in the risk of cervical cancer and human papillomavirus infection by education level. Br. J. Cancer 2009, 101, 865–870. [Google Scholar] [CrossRef] [Green Version]
- Siegel, R.; Ward, E.; Brawley, O.; Jemal, A. Cancer statistics, 2011: The impact of eliminating socioeconomic and racial disparities on premature cancer deaths. CA Cancer J. Clin. 2011, 61, 212–236. [Google Scholar] [CrossRef]
- Pikala, M.; Maniecka-Bryła, I. Years of life lost due to malignant neoplasms characterized by the highest mortality rate. Arch. Med. Sci. 2014, 10, 999–1006. [Google Scholar] [CrossRef] [Green Version]
- World Health Organization. Human papillomavirus vaccines: WHO position paper, May 2017-recommendations. Vaccine 2017, 35, 5753–5755. [Google Scholar] [CrossRef]
- Cierniak, M. Na co Umarł Pacjent—czyli, co Jest Wpisywane na Kartach Zgonów? Available online: http://stat.gov.pl/download/gfx/portalinformacyjny/pl/defaultaktualnosci/5746/1/1/2/l_na_co_umarl_pacjent.pdf (accessed on 19 March 2019).




{kind=link}
{kind=link}
{kind=link}
| Year | Number of Deaths | CDR (per 100,000) | SDR (per 100,000) | SEYLL | SEYLLp (per 100,000) | SEYLLd (per Deaths) |
|---|---|---|---|---|---|---|
| 2000 | 1987 | 10.1 | 12.0 | 55,730 | 394.3 | 28.1 |
| 2001 | 1826 | 9.3 | 10.8 | 51,128 | 360.0 | 28.0 |
| 2002 | 1855 | 9.4 | 10.9 | 51,721 | 315.5 | 27.9 |
| 2003 | 1825 | 9.3 | 10.6 | 50,228 | 304.5 | 27.5 |
| 2004 | 1819 | 9.3 | 10.3 | 50,501 | 304.3 | 27.8 |
| 2005 | 1796 | 9.1 | 10.0 | 49,219 | 295.0 | 27.4 |
| 2006 | 1824 | 9.3 | 10.1 | 48,671 | 290.3 | 26.7 |
| 2007 | 1907 | 9.7 | 10.5 | 50,294 | 298.9 | 26.4 |
| 2008 | 1745 | 8.8 | 9.5 | 45,622 | 270.3 | 26.1 |
| 2009 | 1748 | 8.9 | 9.4 | 45,993 | 271.8 | 26.3 |
| 2010 | 1735 | 8.7 | 9.1 | 45,310 | 266.2 | 26.1 |
| 2011 | 1656 | 8.3 | 8.7 | 42,743 | 250.7 | 25.8 |
| 2012 | 1669 | 8.4 | 8.6 | 42,891 | 251.4 | 25.7 |
| 2013 | 1669 | 8.4 | 8.5 | 41,455 | 243.1 | 24.8 |
| 2014 | 1628 | 8.2 | 8.2 | 39,518 | 231.7 | 24.3 |
| 2015 | 1585 | 8.0 | 7.9 | 37,634 | 220.9 | 23.7 |
| Coefficients | Number of Joinpoints | Years | APC (95% CI) | AAPC (95% CI) |
|---|---|---|---|---|
| CDR | 0 | 2000–2015 | −1.2 * (−8.4; −0.9) | |
| SDR | 0 | 2000–2015 | −2.4 * (−2.7; −2.1) | |
| SEYLLp | 1 | 2000–2002 | −9.9 * (−16.7; −2.6) | −3.6 * (−4.5; −2.6) |
| 2002–2015 | −2.6 * (−3.0; −2.2) | |||
| SEYLLd | 1 | 2000–2002 | −0.8 * (−1.0; −0,7) | −1.2 * (−1.4; −0.9) |
| 2002–2015 | −2.6 * (−3.9; −1.2) | |||
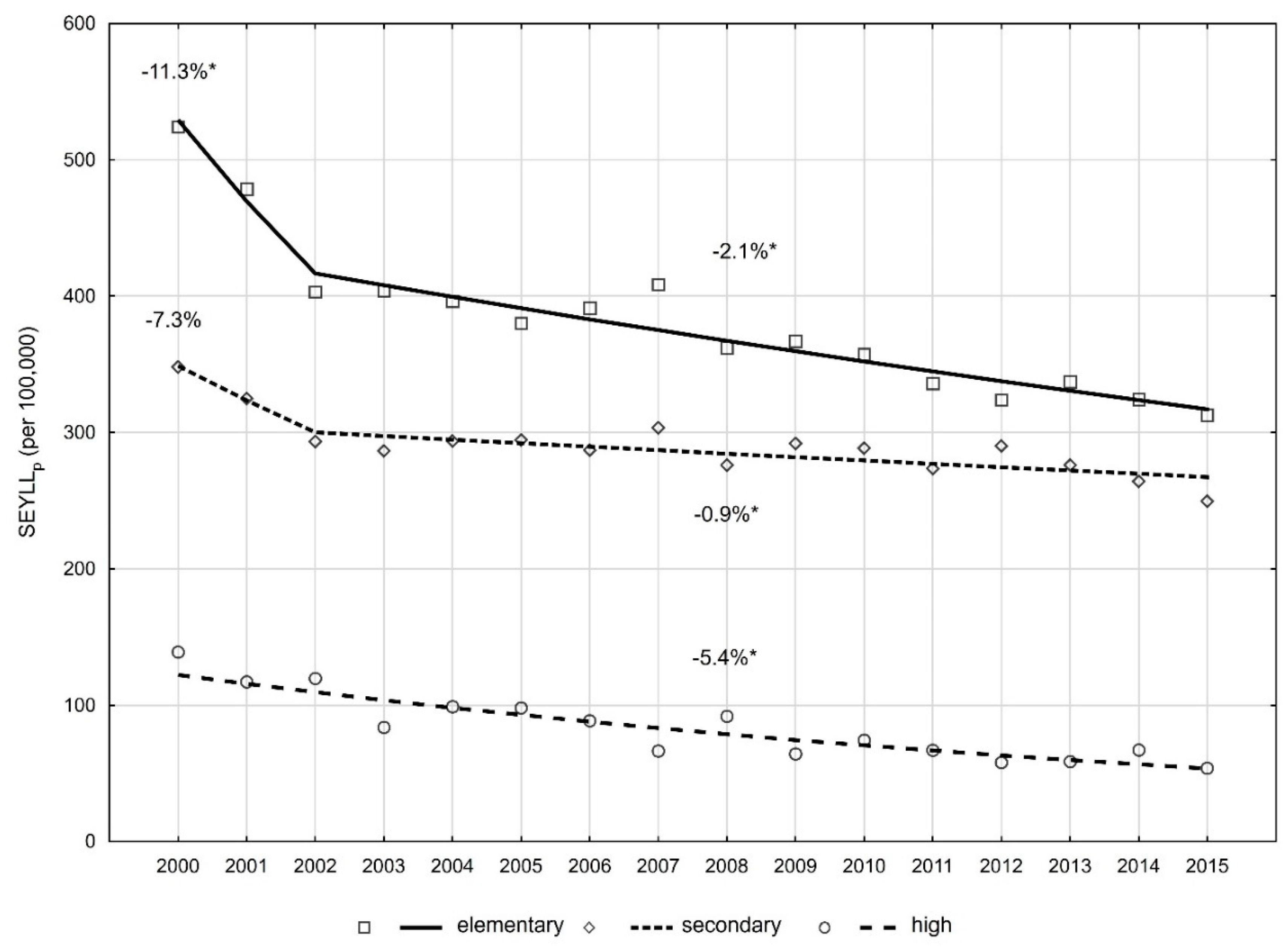
| SEYLLp according to level of education | ||||
| high | 0 | 2000–2015 | −5.4 * (−6.7; −4.0) | |
| secondary | 1 | 2000–2002 | −7.3 (−17.7; 4.5) | −1.8 * (−3.2; −0.3) |
| 2002–2015 | −0.9 * (−1.5; −0.3) | |||
| elementary | 1 | 2000–2002 | −11.3 * (−20.1; −1.5) | −3.4 * (−4.6; −2.1) |
| 2002–2015 | −2.1 * (−2.6; −1.5) | |||
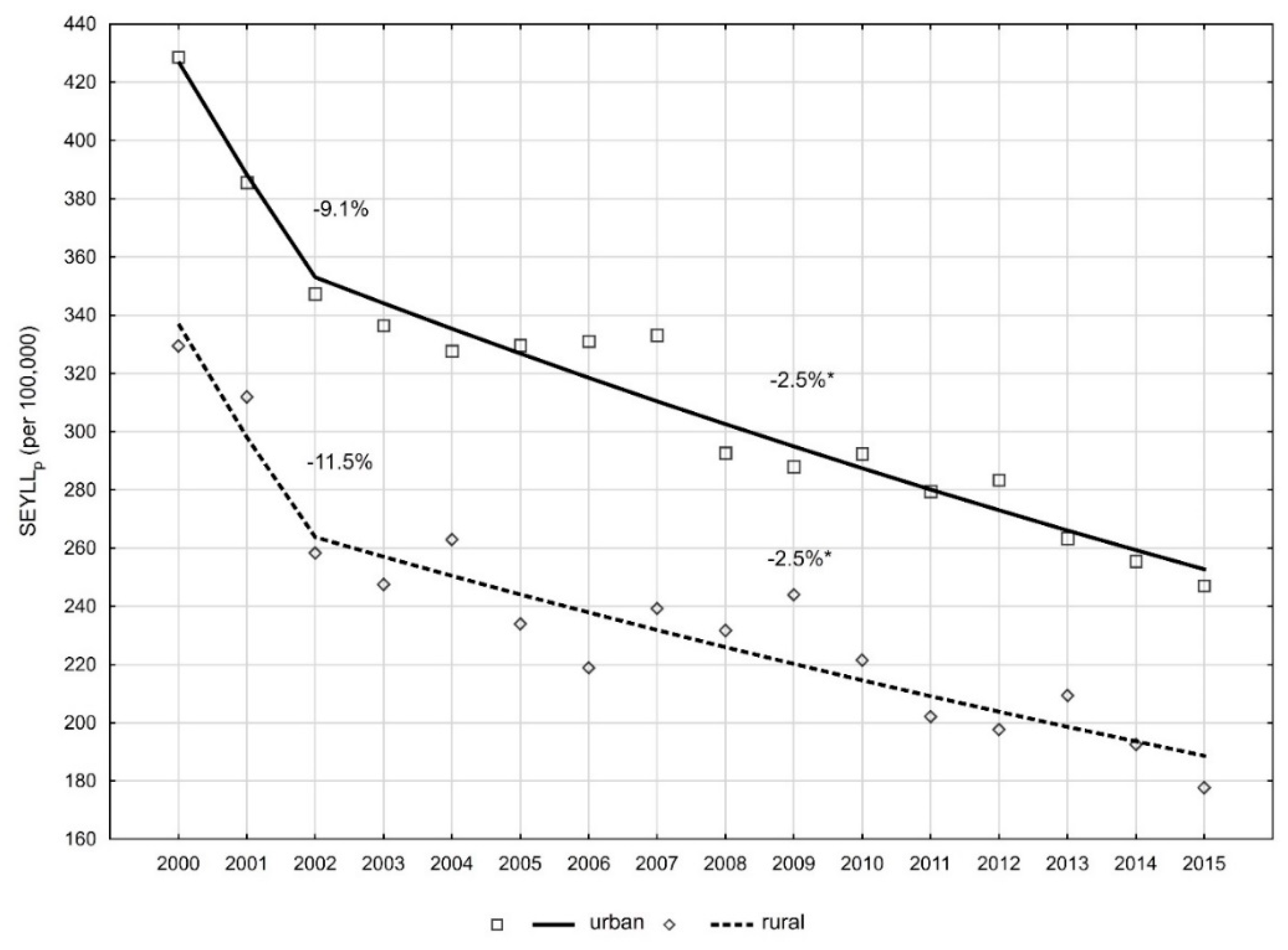
| SEYLLp according to place of residence | ||||
| urban | 1 | 2000–2002 | −9.1 (−17.9; 0.6) | −3.4 * (−4.7; −2.2) |
| 2002–2015 | −2.5 * (−3.1; −2.0) | |||
| rural | 1 | 2000–2002 | −11.5 (−25.6; 5.2) | −3.8 * (−5.9; −1.7) |
| 2002–2015 | −2.5 * (−3.4; −1.7) | |||
| Risk Factors | SEYLLp | SR (95% CI) | ||
|---|---|---|---|---|
| 2000 | 2015 | 2000 | 2015 | |
| Educational level | ||||
| high (ref) | 139.0 | 53.7 | 1.0 | 1.0 |
| secondary | 348.1 | 249.6 | 2.5 (2.4; 2.6) | 4.6 (4.4; 4.8) |
| elementary | 524.2 | 312.8 | 3.8 (3.6; 4.0) | 5.8 (5.5; 6.1) |
| Place of residence | ||||
| rural (ref) | 329.5 | 177.7 | 1.0 | 1.0 |
| urban | 428.6 | 247.1 | 1.3 (1.2; 1.3) | 1.4. (1.3; 1.4) |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Pikala, M.; Burzyńska, M.; Maniecka-Bryła, I. Years of Life Lost Due to Cervical Cancer in Poland in 2000 to 2015. Int. J. Environ. Res. Public Health 2019, 16, 1545. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph16091545
Pikala M, Burzyńska M, Maniecka-Bryła I. Years of Life Lost Due to Cervical Cancer in Poland in 2000 to 2015. International Journal of Environmental Research and Public Health. 2019; 16(9):1545. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph16091545
Chicago/Turabian StylePikala, Małgorzata, Monika Burzyńska, and Irena Maniecka-Bryła. 2019. "Years of Life Lost Due to Cervical Cancer in Poland in 2000 to 2015" International Journal of Environmental Research and Public Health 16, no. 9: 1545. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph16091545