Residents’ Awareness of Family Doctor Contract Services, Status of Contract with a Family Doctor, and Contract Service Needs in Zhejiang Province, China: A Cross-Sectional Study

 ,
,
Abstract
:1. Introduction
2. Materials and Methods
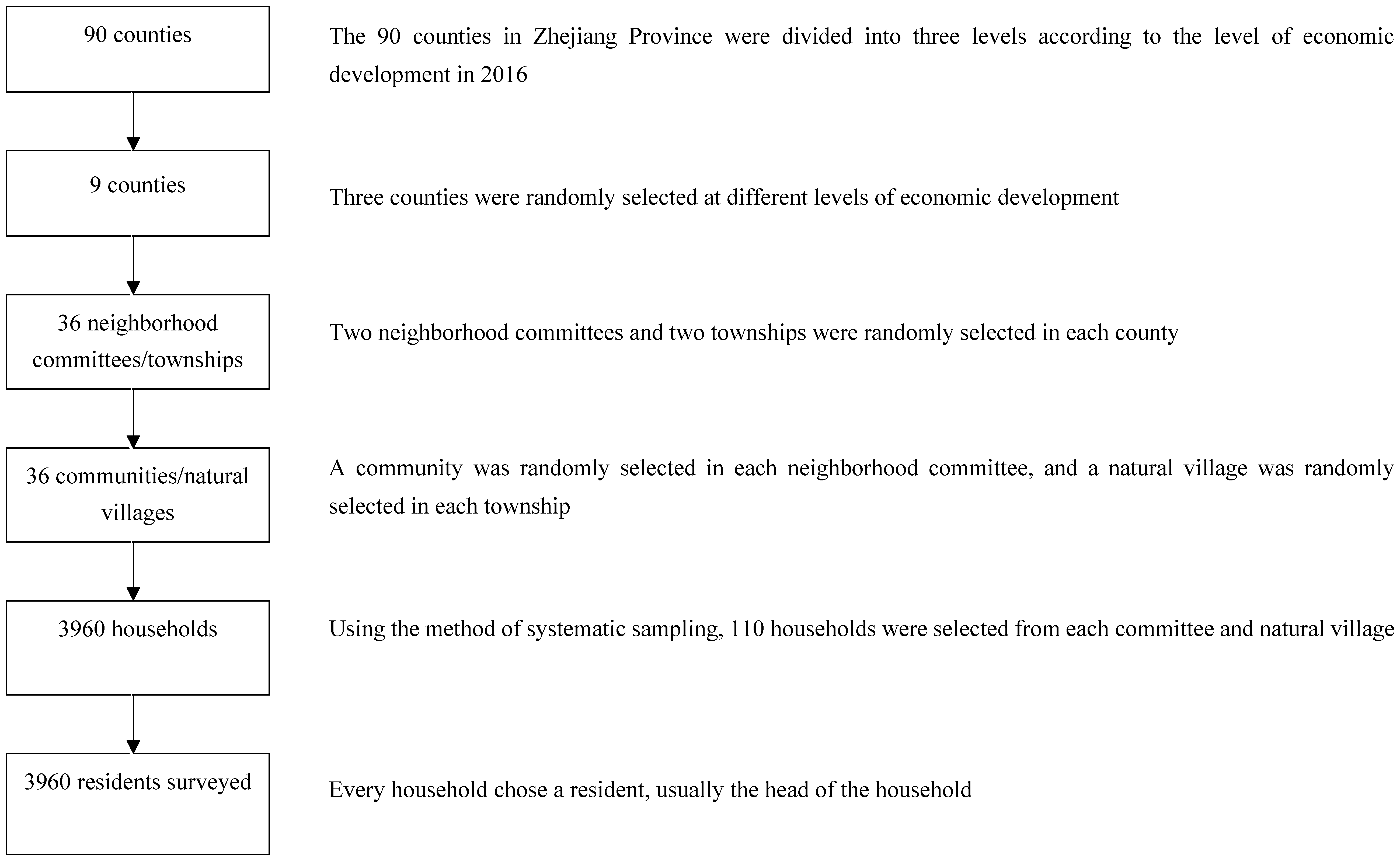
2.1. Research Participants
2.2. Methods and Data Collection
2.3. Statistical Analysis
2.4. Ethical Considerations
3. Results
3.1. Sociodemographic Information of Participants
3.2. Residents’ Awareness of FDCS and Influencing Factors
3.3. Residents Who Had a Contract with FDs and Influencing Factors
3.4. Residents’ Need for the 10 Items of FDCS
4. Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Liu, L.Q. Promoting contracted services of family doctors to strengthen the construction of hierarchical medical system. Chin. Gen. Pract. 2018, 21, 1–4. [Google Scholar]
- Huang, J.L.; Liu, S.S.; He, R.R.; Fang, S.; Lu, W.; Wu, J.; Liang, H.; Zhang, Y.M. Factors associated with residents’ contract behavior with family doctors in community health service centers: A longitudinal survey from China. PLoS ONE 2018, 13, e0208200. [Google Scholar] [CrossRef] [PubMed]
- Zhao, Y.R.; Lin, J.F.; Qiu, Y.W.; Yang, Q.; Wang, X.Y.; Shang, X.P.; Xu, X.P. Demand and Signing of General Practitioner Contract Service among the Urban Elderly: A Population-Based Analysis in Zhejiang Province, China. Int. J. Environ. Res. Public Health 2017, 14, 356. [Google Scholar] [CrossRef] [PubMed]
- The Central People’s Government of the People’s Republic of China. Opinions on Deepening the Reform of the Medical and Health System. 2009. Available online: http://www.gov.cn/jrzg/2009-04/06/content_1278721.htm (accessed on 23 July 2019). (In Chinese)
- Chen, Z. Launch of the health-care reform plan in China. Lancet 2009, 373, 1322–1324. [Google Scholar] [CrossRef]
- The Central People’s Government of the People’s Republic of China. Guiding Opinions on Establishing a General Practitioner System. 2011. Available online: http://www.gov.cn/zhengce/content/2011-07/06/content_6123.htm (accessed on 23 July 2019). (In Chinese)
- National Medical Reform Office. Notice on Promoting Guidance for Family Doctor Contract Services. 2016. Available online: http://www.mohrss.gov.cn/SYrlzyhshbzb/shehuibaozhang/zcwj/yiliao/201606/t20160615_241854.html. (accessed on 23 July 2019). (In Chinese)
- Jiang, X.X.; Hu, L.; Wu, Y.P. The practice and thinking for the general practitioners’ contracted service in Zhejiang Province. Chin. J. Health Policy 2015, 8, 52–55. [Google Scholar]
- The People’s Government of Zhejiang Province. Guiding Opinions on the Promotion of Contract Services for Responsible Doctors. 2015. Available online: http://www.zj.gov.cn/art/2015/6/15/art_1582412_27548.html (accessed on 23 July 2019). (In Chinese)
- Health Commission of Zhejiang Province. Notice on Further Implementation and Details of the Family Doctor Contract Service. Available online: http://www.zjwjw.gov.cn/art/2018/4/30/art_1267707_461.html (accessed on 23 July 2019). (In Chinese)
- Fang, J.Q. Medical Statistics and Computer Experiments, 2nd ed.; World Scientific Publishing: Singapore, 2014. [Google Scholar]
- Weiss, N.S.; Koepsell, T.D. Epidemiologic Methods, 2nd ed.; Oxford University Press: New York, NY, USA, 2014. [Google Scholar]
- Li, X.; Lu, J.P.; Hu, S.; Cheng, K.K.; Maeseneer, J.D.; Meng, Q.Y.; Mossialos, E.; Xu, D.R.; Yip, W.; Zhang, H.Z.; et al. The primary health-care system in China. Lancet 2017, 390, 2584–2594. [Google Scholar] [CrossRef]
- Zhao, M.; Zhu, Z.F.; Sun, H.M.; Sun, G.N. Survey on awareness and utilization of community family doctors’ service on residents in Beijing and influential factors. Chin. J. Hosp. Admin. 2016, 32, 382–384. [Google Scholar]
- Niu, Y.J.; Yu, M.W.; Qiu, Y.; Cai, J.; He, Z.H.; Huang, X.J.; Ding, C.F.; Miao, J.Q.; Lin, Y.Y.; Li, L. Status and influencing factors of contracting and renewing on family doctor service in pilot areas in Guangzhou. Chin. J. Hosp. Admin. 2017, 33, 939–943. [Google Scholar]
- Wang, J.Y.; Wu, Y.; Wang, X.; Xu, H.L.; Guo, Q.; Su, H.L. Perception of the contract responsibility system for family doctors in Shanghai’s Minhang district: Patient and physician perspectives. Chin. Gen. Pract. 2018, 21, 3385–3388. [Google Scholar]
- Wang, L.C.; Ge, M.; Jiang, P.; Zhu, M.J.; Zhao, X.P.; Liang, H.; Huang, J.L.; Liu, S.S.; Zhang, Y.M. Community residents’ awareness and willingness towards contractual services from family doctors. Chin. Gen. Pract. 2018, 21, 401–406. [Google Scholar]
- Li, L.; Fu, H.Q. China’s health care system reform: Progress and prospects. Int. J. Health Plann. Mgmt. 2017, 32, 240–253. [Google Scholar] [CrossRef] [PubMed]
- Huang, J.; Liang, H.; Zhang, W.; Zhang, J.; Wang, C.; Chen, X.; Liu, S.; He, R.; Zhang, Y. Influencing factor analysis of signing a contract with a family doctor among residents in Hongkou district. Chin. Gen. Pract. 2019, 22, 687–691. [Google Scholar]
- Yuan, L.; Zhou, C.; Jiang, P.; Xu, L.; Zhao, Q.; Xu, B. Community residents’ demand for family physician service in Changning Districe, Shanghai. Chin. Gen. Pract. 2014, 17, 3860–3864. [Google Scholar]
- Mo, H.; Wang, J. Study on the Status of Family Doctor Signing Service in Different Areas of Guangdong Province and It’s Countermeasure Proposal; Guangzhou Medical University: Guangzhou, China, 2017; p. 5. [Google Scholar]
- Jing, L.; Shu, Z.; Sun, X.; Chiu, J.F.; Lou, J.; Xie, C. Factors influencing patients’ contract choice with general practitioners in Shanghai: A preliminary study. Asia Pac. J. Public Health 2015, 27 (Suppl. 2), 77S–85S. [Google Scholar] [CrossRef] [PubMed]
- Kuang, L.; Liang, Y.; Mei, J.; Zhao, J.; Wang, Y.; Liang, H. Family practice and the quality of primary care: A study of Chinese patients in Guangdong Province. Fam. Pract. 2015, 32, 557–563. [Google Scholar] [CrossRef] [PubMed]
- Huang, J.L.; Lu, W.; Wang, L.; Zhang, T.; Liu, C.J.; Liu, S.S.; Liang, H.; Zhang, Y.M.; Guo, D.F. A preliminary effect analysis of family doctor and medical insurance payment coordination reform in Changning District of Shanghai, China. BMC Fam. Pract. 2019, 20, 60. [Google Scholar] [CrossRef]
- Cheng, J.M.; Yuan, Y.X.; Lu, W.; Yang, L. Primary health care in China: Is China’s health reform reform forthe whole nation? Prim. Health Care Res. Dev. 2017, 18, 398–403. [Google Scholar] [CrossRef] [PubMed]
- Liang, H. The key to advancing the hierarchical diagnosis and treatment system is to establish and improve the Family doctor system. Chin. J. Health Policy 2016, 9, 1–2. [Google Scholar]
- Liu, G.G.; Vortherms, S.A.; Hong, X.Z. China’s Health Reform Update. Annu. Rev. Public Health 2017, 38, 431–448. [Google Scholar] [CrossRef]
- Ge, G.; Tang, N.; Chen, Z.; Wang, J. Residents’ awareness and satisfaction of family doctor services and two-way referral in two pilot towns of Shaanxi Province. Chin. Gen. Pract. 2017, 20, 3493–3497. [Google Scholar]
- Liu, W.; Hou, Y.; Feng, J.; Wang, H.; Hu, B. Implementation status and residents’ need analysis of contracted family doctor service in Chongqing City. Chin. Gen. Pract. 2019, 22, 777–782. [Google Scholar]
- Shi, Y.; Li, N.; Zhao, J.; Wang, M. Community residents’ demands for family physician service in Xicheng District fo Beijing. Chin. J. Soc. Med. 2017, 34, 372–375. [Google Scholar]
- Tang, Q.; Song, P.P.; Xu, L.Z. The role of family physicians contracted healthcare in China: A “Cardiotonic” or a “Band-Aid” for healthcare reform? Biosci. Trends 2016, 10, 325–326. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Variables | Cases N (%) | Awareness | χ2 | p-Value | Signed | χ2 | p-Value | ||
|---|---|---|---|---|---|---|---|---|---|
| Yes, N (%) | No, N (%) | Yes, N (%) | No, N (%) | ||||||
| Total | 3871 | 2771 (71.58) | 1100 (28.42) | 1952 (50.43) | 1919 (49.57) | ||||
| Gender | 1.278 | 0.261 | 0.014 | 0.906 | |||||
| Male | 1571 (40.58) | 1109 (70.59) | 462 (29.41) | 794 (50.54) | 777 (49.46) | ||||
| Female | 2300 (59.42) | 1662 (72.26) | 638 (27.74) | 1158 (50.35) | 1142 (49.65) | ||||
| Age | 89.543 | <0.001 | 422.768 | <0.001 | |||||
| 16–34 | 830 (21.44) | 529 (63.73) | 301 (36.27) | 253 (30.48) | 577 (69.52) | ||||
| 35–49 | 1040 (26.87) | 693 (66.63) | 347 (33.37) | 401 (38.56) | 639 (61.44) | ||||
| 50–64 | 761 (19.66) | 547 (71.88) | 214 (28.12) | 406 (53.35) | 355 (46.65) | ||||
| ≥65 | 1240 (32.03) | 1002 (80.81) | 238 (19.19) | 892 (71.94) | 348 (28.06) | ||||
| Education Level | 32.837 | <0.001 | 155.201 | <0.001 | |||||
| Elementary school or lower | 1487 (38.41) | 1092 (73.44) | 395 (26.56) | 932 (62.68) | 555 (37.32) | ||||
| Junior middle school | 1033 (26.69) | 698 (67.57) | 335 (32.43) | 475 (45.98) | 558 (54.02) | ||||
| High school | 592 (15.29) | 395 (66.72) | 197 (33.28) | 253 (42.74) | 339 (57.26) | ||||
| Junior college | 327 (8.45) | 241 (73.70) | 86 (26.30) | 130 (39.76) | 197 (60.24) | ||||
| Bachelor’s degree or higher | 432 (11.16) | 345 (79.86) | 87 (20.14) | 162 (37.50) | 270 (62.50) | ||||
| Marital Status | 4.693 | 0.096 | 53.767 | <0.001 | |||||
| Single | 348 (8.99) | 234 (67.24) | 114 (32.76) | 126 (36.21) | 222 (63.79) | ||||
| Married | 3249 (83.93) | 2332 (71.78) | 917 (28.22) | 1646 (50.66) | 1603 (49.34) | ||||
| Divorced or widowed | 274 (7.08) | 205 (74.82) | 69 (25.18) | 180 (65.69) | 94 (34.31) | ||||
| Household registration | 3.343 | 0.067 | 8.499 | 0.004 | |||||
| Local | 3785 (97.78) | 2717 (71.78) | 1068 (28.22) | 1922 (50.78) | 1863 (49.22) | ||||
| Non-local | 86 (2.22) | 54 (62.79) | 32 (37.21) | 30 (34.88) | 56 (65.12) | ||||
| Personal Income (per month) | 11.347 | 0.010 | 79.661 | <0.001 | |||||
| ≤2000 | 1642 (42.42) | 1193 (72.66) | 449 (27.34) | 958 (58.34) | 684 (41.66) | ||||
| 2001–5000 | 1645 (42.49) | 1136 (69.06) | 509 (30.94) | 711 (43.22) | 934 (56.78) | ||||
| 5001–8000 | 427 (11.03) | 320 (74.94) | 107 (25.06) | 197 (46.14) | 230 (53.86) | ||||
| ≥8001 | 157 (4.06) | 122 (77.71) | 35 (22.29) | 86 (54.78) | 71 (45.22) | ||||
| Chronic disease history | 187.98 | <0.001 | 514.872 | <0.001 | |||||
| Yes | 1516 (39.16) | 1273 (83.97) | 243 (16.03) | 1109 (73.15) | 407 (26.85) | ||||
| No | 2355 (60.84) | 1498 (63.61) | 857 (36.39) | 843 (35.80) | 1512 (64.20) | ||||
| Variables | B | SE | Wald Chi-Square Value | p-Value | OR (95% CI) |
|---|---|---|---|---|---|
| Constant | −0.381 | 0.131 | |||
| Age 16–34 (Ref.) | |||||
| 35–49 | 0.455 | 0.113 | 16.109 | <0.001 | 1.576 (1.262, 1.969) |
| 50–64 | 0.66 | 0.136 | 23.418 | <0.001 | 1.935 (1.481, 2.528) |
| ≥65 | 1.023 | 0.144 | 50.501 | <0.001 | 2.781 (2.098, 3.688) |
| Education Level Elementary school or lower (Ref.) | |||||
| Junior middle school | 0.264 | 0.102 | 6.716 | 0.010 | 1.302 (1.066, 1.590) |
| High school | 0.479 | 0.127 | 14.295 | <0.001 | 1.614 (1.259, 2.069) |
| Junior college | 1.107 | 0.167 | 43.961 | <0.001 | 3.025 (2.181, 4.196) |
| Bachelor’s degree or higher | 1.531 | 0.165 | 86.327 | <0.001 | 4.623 (3.347, 6.386) |
| Chronic Disease History No (Ref.) | |||||
| Yes | 1.058 | 0.095 | 123.197 | <0.001 | 2.880 (2.390, 3.472) |
| Variables | B | SE | Wald Chi-Square Value | p-Value | OR (95% CI) |
|---|---|---|---|---|---|
| Constant | −2.916 | 0.176 | |||
| Age 16–34 (Ref.) | |||||
| 35–49 | 0.096 | 0.126 | 0.583 | 0.445 | 1.101 (0.860, 1.408) |
| 50–64 | 0.388 | 0.151 | 6.569 | 0.01 | 1.474 (1.096, 1.982) |
| ≥65 | 0.977 | 0.155 | 39.584 | <0.001 | 2.656 (1.959, 3.601) |
| Education Level Elementary school or lower (Ref.) | |||||
| Junior middle school | −0.165 | 0.118 | 1.944 | 0.163 | 0.848 (0.673, 1.069) |
| High school | −0.172 | 0.143 | 1.448 | 0.229 | 0.842 (0.636, 1.115) |
| Junior college | −0.286 | 0.181 | 2.506 | 0.113 | 0.751 (0.527, 1.071) |
| Bachelor’s degree or higher | −0.534 | 0.174 | 9.377 | 0.002 | 0.586 (0.417, 0.825) |
| Personal Income (per month) ≤2000 (Ref.) | |||||
| 2001–5000 | −0.303 | 0.097 | 9.679 | 0.002 | 0.739 (0.610, 0.894) |
| 5001–8000 | −0.017 | 0.147 | 0.013 | 0.91 | 0.984 (0.737, 1.312) |
| ≥8001 | 0.604 | 0.216 | 7.836 | 0.005 | 1.829 (1.198, 2.791) |
| Chronic Disease History No (Ref.) | |||||
| Yes | 0.967 | 0.098 | 97.21 | <0.001 | 2.629 (2.170, 3.186) |
| Awareness of FDCS No (Ref.) | |||||
| Yes | 3.125 | 0.123 | 642.608 | <0.001 | 22.753 (17.870, 28.971) |
| Variables | Health Consultation | Follow-Up of Chronic Patients | Long-Term Prescriptions of Chronic Patients | Rehabilitation Guidance | Appointment Referral | Regular Physical Examination | Increasing the Proportion of MI Reimbursements | TCM Health Care | Family Bed Service | Free Door-to-Door Service |
|---|---|---|---|---|---|---|---|---|---|---|
| Total | 3276 (84.63) | 2550 (65.87) | 2173 (56.14) | 2512 (64.89) | 2424 (62.62) | 3163 (81.71) | 3099 (80.06) | 2291 (59.18) | 1522 (39.32) | 2253 (58.20) |
| Sex | ||||||||||
| Male | 1314 (83.64) | 1004 (63.91) | 889 (56.59) | 1031 (65.63) | 992 (63.14) | 1253 (79.76) | 1241 (78.99) | 920 (58.56) | 628 (39.97) | 892 (56.78) |
| Female | 1962 (85.30) | 1546 (67.22) | 1284 (55.83) | 1481 (64.39) | 1432 (62.26) | 1910 (83.04) | 1858 (80.78) | 1371 (59.61) | 894 (38.87) | 1361 (59.17) |
| χ2 | 1.985 | 4.547 | 0.220 | 0.626 | 0.311 | 6.742 | 1.870 | 0.424 | 0.478 | 2.201 |
| p-Value | 0.159 | 0.033 | 0.639 | 0.429 | 0.577 | 0.009 | 0.172 | 0.515 | 0.489 | 0.138 |
| Age | ||||||||||
| 16–34 | 682 (82.17) | 455 (54.82) | 408 (49.16) | 520 (62.65) | 557 (67.11) | 620 (74.70) | 653 (78.67) | 489 (58.92) | 340 (40.96) | 478 (57.59) |
| 35–49 | 885 (85.10) | 627 (60.29) | 541 (52.02) | 658 (63.27) | 679 (65.29) | 851 (81.83) | 860 (82.69) | 621 (59.71) | 394 (37.88) | 581 (55.87) |
| 50–64 | 627 (82.39) | 506 (66.49) | 427 (56.11) | 469 (61.63) | 441 (57.95) | 634 (83.31) | 583 (76.61) | 434 (57.03) | 259 (30.04) | 409 (53.75) |
| ≥65 | 1082 (87.26) | 962 (77.58) | 797 (64.27) | 865 (69.76) | 747 (60.24) | 1058 (85.32) | 1003 (80.89) | 747 (60.24) | 529 (42.66) | 785 (63.31) |
| χ2 | 13.554 | 135.278 | 56.930 | 19.476 | 20.393 | 39.445 | 11.717 | 2.180 | 16.552 | 21.956 |
| p-Value | 0.004 | <0.001 | <0.001 | <0.001 | <0.001 | <0.001 | 0.008 | 0.536 | 0.001 | <0.001 |
| Education Level | ||||||||||
| Elementary school or lower | 1254 (84.33) | 1082 (72.76) | 856 (57.57) | 958 (64.43) | 824 (55.41) | 1277 (85.88) | 1195 (80.36) | 813 (54.67) | 556 (37.39) | 887 (59.65) |
| Junior middle school | 869 (84.12) | 647 (62.63) | 568 (54.99) | 657 (63.60) | 655 (63.41) | 861 (83.35) | 821 (79.48) | 606 (58.66) | 373 (36.11) | 574 (55.57) |
| High school | 506 (85.47) | 366 (61.82) | 335 (56.59) | 383 (64.70) | 415 (70.10) | 469 (79.22) | 482 (81.42) | 380 (64.19) | 245 (41.39) | 341 (57.60) |
| Junior college | 277 (84.71) | 201 (61.47) | 168 (51.38) | 220 (67.28) | 227 (69.42) | 251 (76.76) | 257 (78.59) | 213 (65.14) | 148 (45.26) | 193 (59.02) |
| Bachelor’s degree or higher | 370 (85.65) | 254 (58.80) | 246 (56.94) | 294 (68.06) | 303 (70.14) | 305 (70.60) | 344 (79.63) | 279 (64.58) | 200 (46.30) | 258 (59.72) |
| χ2 | 0.975 | 52.997 | 4.962 | 3.623 | 64.312 | 62.623 | 1.481 | 28.788 | 21.492 | 4.820 |
| p-Value | 0.914 | <0.001 | 0.291 | 0.459 | <0.001 | <0.001 | 0.830 | <0.001 | <0.001 | 0.306 |
| Marital Status | ||||||||||
| Single | 272 (78.16) | 187 (53.74) | 166 (47.70) | 209 (60.06) | 215 (61.78) | 244 (70.11) | 253 (72.70) | 191 (54.89) | 142 (40.80) | 197 (56.61) |
| Married | 2766 (85.13) | 2161 (66.51) | 1831 (56.36) | 2117 (65.16) | 2053 (63.19) | 2689 (82.76) | 2617 (80.55) | 1944 (59.83) | 1275 (39.24) | 1894 (58.29) |
| Divorced or widowed | 238 (86.86) | 202 (73.72) | 176 (64.23) | 186 (67.88) | 156 (56.93) | 230 (83.94) | 229 (83.58) | 156 (56.93) | 105 (38.32) | 162 (59.12) |
| χ2 | 12.879 | 30.907 | 17.415 | 4.748 | 4.337 | 34.635 | 14.410 | 3.804 | 0.444 | 0.470 |
| p-Value | 0.002 | <0.001 | <0.001 | 0.093 | 0.114 | <0.001 | 0.001 | 0.149 | 0.809 | 0.790 |
| Household Registration | ||||||||||
| Local | 3198 (84.49) | 2504 (66.16) | 2133 (56.35) | 2460 (64.99) | 2372 (62.67) | 3095 (81.77) | 3030 (80.05) | 2245 (59.31) | 1488 (39.31) | 2202 (58.17) |
| Non-local | 78 (90.70) | 46 (53.49) | 40 (46.51) | 52 (60.47) | 52 (60.47) | 68 (79.07) | 69 (80.23) | 46 (53.49) | 34 (39.53) | 51 (59.30) |
| χ2 | 2.490 | 6.002 | 3.308 | 0.757 | 0.174 | 0.410 | 0.002 | 1.181 | 0.002 | 0.044 |
| p-Value | 0.115 | 0.014 | 0.069 | 0.384 | 0.676 | 0.522 | 0.967 | 0.277 | 0.967 | 0.834 |
| Personal Monthly Income | ||||||||||
| ≤2000 | 1396 (85.02) | 1156 (70.40) | 920 (56.03) | 1037 (63.15) | 955 (58.16) | 1396 (85.02) | 1317 (80.21) | 912 (55.54) | 611 (37.21) | 984 (59.92) |
| 2001–5000 | 1381 (83.95) | 1033 (62.80) | 915 (55.62) | 1092 (66.38) | 1064 (67.68) | 1343 (81.64) | 1329 (80.79) | 1020 (62.01) | 666 (40.49) | 945 (57.45) |
| 5001–8000 | 367 (85.95) | 257 (60.19) | 250 (58.55) | 279 (65.34) | 295 (69.09) | 317 (74.24) | 344 (80.56) | 264 (61.83) | 177 (41.45) | 235 (55.04) |
| ≥8001 | 132 (84.08) | 104 (66.24) | 88 (56.05) | 104 (66.24) | 110 (70.06) | 107 (68.15) | 109 (69.43) | 95 (60.51) | 68 (43.31) | 89 (56.69) |
| χ2 | 1.380 | 28.059 | 1.193 | 3.944 | 28.278 | 47.287 | 11.757 | 15.788 | 5.862 | 4.302 |
| p-Value | 0.710 | <0.001 | 0.755 | 0.268 | <0.001 | <0.001 | 0.008 | 0.001 | 0.119 | 0.231 |
| Chronic Disease History | ||||||||||
| No | 1930 (81.95) | 1289 (54.73) | 1123 (47.69) | 1424 (60.47) | 1476 (62.68) | 1863 (79.11) | 1868 (79.32) | 1369 (58.13) | 914 (38.81) | 1315 (55.84) |
| Yes | 1346 (88.79) | 1261 (83.18) | 1050 (69.26) | 1088 (71.77) | 948 (62.53) | 1300 (85.75) | 1231 (81.20) | 922 (60.82) | 608 (40.11) | 938 (61.87) |
| χ2 | 33.103 | 331.953 | 174.355 | 51.699 | 0.008 | 27.240 | 2.042 | 2.755 | 0.648 | 13.807 |
| p-Value | <0.001 | <0.001 | <0.001 | <0.001 | 0.929 | <0.001 | 0.153 | 0.097 | 0.421 | <0.001 |
| Contract with Family Doctor | ||||||||||
| No | 1525 (79.47) | 1088 (56.70) | 959 (49.97) | 1163 (60.60) | 1131 (58.94) | 1469 (76.55) | 1491 (77.70) | 1073 (55.91) | 723 (37.68) | 1073 (55.91) |
| Yes | 1751 (89.70) | 1462 (74.90) | 1214 (62.19) | 1349 (69.11) | 1293 (66.24) | 1694 (86.78) | 1608 (82.38) | 1218 (62.40) | 799 (40.93) | 1180 (60.45) |
| χ2 | 77.919 | 142.607 | 58.672 | 30.718 | 22.047 | 67.797 | 13.277 | 16.836 | 4.301 | 8.185 |
| p-Value | <0.001 | <0.001 | <0.001 | <0.001 | <0.001 | <0.001 | <0.001 | <0.001 | 0.038 | 0.004 |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Shang, X.; Huang, Y.; Li, B.; Yang, Q.; Zhao, Y.; Wang, W.; Liu, Y.; Lin, J.; Hu, C.; Qiu, Y. Residents’ Awareness of Family Doctor Contract Services, Status of Contract with a Family Doctor, and Contract Service Needs in Zhejiang Province, China: A Cross-Sectional Study. Int. J. Environ. Res. Public Health 2019, 16, 3312. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph16183312
Shang X, Huang Y, Li B, Yang Q, Zhao Y, Wang W, Liu Y, Lin J, Hu C, Qiu Y. Residents’ Awareness of Family Doctor Contract Services, Status of Contract with a Family Doctor, and Contract Service Needs in Zhejiang Province, China: A Cross-Sectional Study. International Journal of Environmental Research and Public Health. 2019; 16(18):3312. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph16183312
Chicago/Turabian StyleShang, Xiaopeng, Yangmei Huang, Bi’e Li, Qing Yang, Yanrong Zhao, Wei Wang, Yang Liu, Junfen Lin, Chonggao Hu, and Yinwei Qiu. 2019. "Residents’ Awareness of Family Doctor Contract Services, Status of Contract with a Family Doctor, and Contract Service Needs in Zhejiang Province, China: A Cross-Sectional Study" International Journal of Environmental Research and Public Health 16, no. 18: 3312. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph16183312