Move-It: A Cluster-Randomised Digital Worksite Exercise Intervention in China: Outcome and Process Evaluation


Abstract
:1. Introduction
Aim
2. Methods
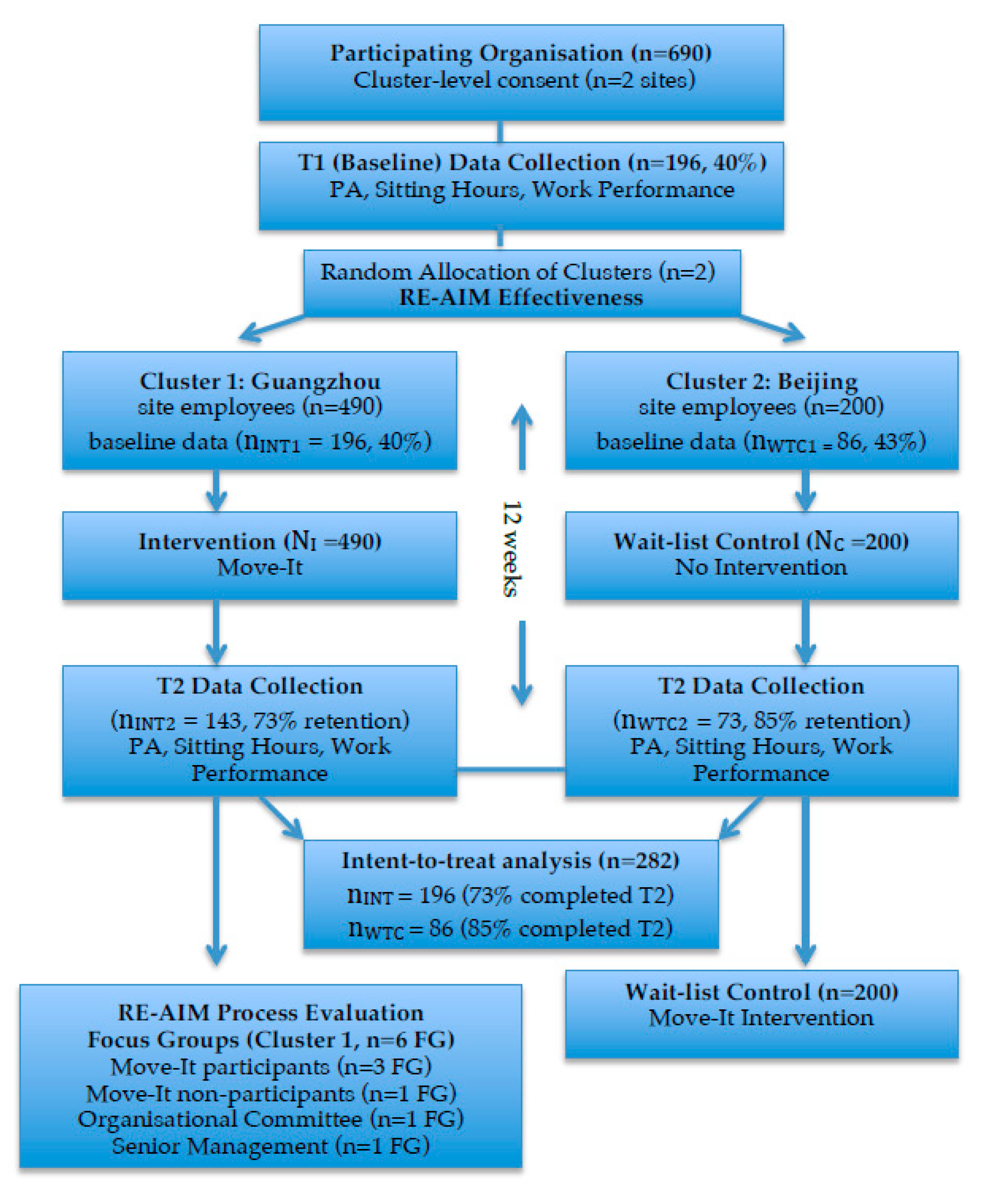
2.1. Design
2.2. Methods
2.2.1. Outcome Evaluation: Participants and Procedures
2.2.2. Process Evaluation: Participants and Procedures
Focus Groups with Employees
Focus Group with the Organisational Committee
Focus Group with Senior Management
2.3. The Move-It Intervention
2.4. Intervention Delivery
2.5. Measures
2.5.1. Physical Activity
2.5.2. Work Performance
2.5.3. Weekday Sitting Hours
2.5.4. Adherence and Adverse Events
2.6. Data Analysis
3. Results
3.1. Reach
“This programme definitely got 100% attention rate. Everyone from the top management to the junior staff knew about ‘Move-It’. And all levels of employees participated.”
“Even though some employees did not enrol on the programme for whatever reasons, they watched the videos and practised the exercises together.”
3.2. Effectiveness
“It helps with neck and muscle pain, which seems to be common among our colleagues.”;
“Exercise makes me feel good...more positive and energised.”
“It helped to build employees’ awareness of the importance of health at work.”;
“Staff would feel that we care for their well-being. It might help with stronger sense of belonging… staff retention perhaps.”
3.3. Adoption
“The mood was contagious. It was boring to do the exercises alone. For myself, when I saw the pop-up window and nobody nearby participated in the exercises, I didn’t do them.”
“Many enthusiastic employees participated in the project, including in the production of the promotional videos and with technical support to place the videos onto the company intranet.”
“They needed to be prompted, whether by machine or in person. They needed to be prompted to stop their current work and take an exercise break.”
3.4. Implementation
“The majority of participants practised the full version of exercise movements in the first two weeks.”
“Many behaved in the same way...the whole team practised together.”
“We could practise the exercise at the workstations and not much space was required.”
3.5. Maintenance
“We should persist with the programme maintenance and reinforce employees’ interests in this initiative. Mind-set training is crucial.”
“We should take an exercise break regularly…develop it as a habit and be aware of its importance for health.”
4. Discussion
Supplementary Materials
Author Contributions
Funding
Conflicts of Interest
References
- Wu, S.; Luo, Y.; Qiu, X.; Bao, M. Building a healthy China by enhancing physical activity: Priorities, challenges and strategies. J. Sport Health Sci. 2017, 6, 125–126. [Google Scholar] [CrossRef] [PubMed]
- Muntner, P.; Gu, D.; Wildman, R.; Chen, J.; Qan, W.; Whelton, P.; He, J. Prevalence of physical activity among chinese adults: Results from the international collaborative study of cardiovascular disease in Asia. Am. J. Pub. Health 2005, 95, 1631–1636. [Google Scholar] [CrossRef] [PubMed]
- Li, Y.; Zeng, X.; Liu, J.; Liu, Y.; Liu, S.; Yin, P.; Qi, J.; Zhao, Z.; Yu, S.; Hu, Y.; et al. Can China achieve a one-third reduction in premature mortality from non-communicable diseases by 2030? BMC Med. 2017, 15, 132. [Google Scholar] [CrossRef] [PubMed]
- Hu, L.; Huang, X.; You, C.; Li, J.; Hong, K.; Li, P.; Wu, Y.; Wu, Q.; Wang, Z.; Gao, R.; et al. Prevalence of overweight, obesity, abdominal obesity and obesity-related risk factors in southern China. PLoS ONE 2017, 12, e0183934. [Google Scholar] [CrossRef] [PubMed]
- Zhou, Y.; Wu, J.; Zhang, S.; Yan, S.; He, L.; Mkandawire, N.; Song, X.; Gan, Y.; Li, W.; Yang, T.; et al. Prevalence and risk factors of physical inactivity among middle-aged and older Chinese in Shenzhen: A cross-sectional study. BMJ Open 2018, 8, e019775. [Google Scholar] [CrossRef] [PubMed]
- Arena, R.; Sagner, M.; Byrne, N.; Williams, A.; McNeil, A.; Street, S.; Hills, A. Novel approaches for the promotion of physical activity and exercise for prevention and management of type 2 diabetes. Eur. J. Clin. Nutr. 2017, 71, 858–864. [Google Scholar] [CrossRef] [PubMed]
- Wang, Z.; Chen, Z.; Zhang, L.; Wang, X.; Hao, G.; Zhang, Z.; Shao, L.; Tian, Y.; Dony, Y.; Zheng, C.; et al. Status of hypertension in China: Results from the China hypertension survey, 2012–2015. Circulation 2018, 137, 2344–2356. [Google Scholar] [CrossRef] [PubMed]
- Yu, X.; Baade, P. Combating diabetes in China: A long-term perspective is needed. Lancet Pub. Health 2018, 3, 154–155. [Google Scholar] [CrossRef]
- González, H.; Fuentes, J.; Márquez, J. Physical inactivity, sedentary behavior and chronic diseases. Korean J. Fam. Med. 2017, 38, 111–115. [Google Scholar] [CrossRef]
- Ryan, C.; Dall, P.; Granat, M.; Grant, P. Sitting patterns at work: Objective measurement of adherence to current recommendations. Ergonomics 2011, 54, 531–538. [Google Scholar] [CrossRef]
- Tremblay, M.; Colley, R.; Saunders, T.; Healy, G.; Owen, N. Physiological and health implications of a sedentary lifestyle. Appl. Physiol. Nutr. Metab. 2010, 35, 725–740. [Google Scholar] [CrossRef] [PubMed]
- Koyanagi, A.; Stubbs, B.; Vancampfort, D. Correlates of sedentary behavior in the general population: A cross-sectional study using nationally representative data from six low- and middle-income countries. PLoS ONE 2018, 13, e0202222. [Google Scholar] [CrossRef] [PubMed]
- Fu, F.; Fung, L. The cardiovascular health of residents in selected metropolitan cities in China. Prev. Med. 2004, 38, 458–467. [Google Scholar] [CrossRef] [PubMed]
- Bell, A.; Ge, K.; Popkin, B. Weight gain and its predictors in Chinese adults. Int. J. Obes. 2001, 25, 1079–1086. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hu, G.; Pekkarinen, H.; Hänninen, O.; Yu, Z.; Tian, H.; Guo, Z.; Nissinen, A. Physical activity during leisure and commuting in Tianjin, China. Bull. World Health Organ. 2002, 80, 933–938. [Google Scholar] [PubMed]
- International Labour Organization, ILOSTAT Database. Employment to Population Ratio, 15+, Total (%) (Modeled ILO Estimate). Data Retrieved in April, 2019. Available online: https://data.worldbank.org/indicator/SL.EMP.TOTL.SP.ZS?view=chart (accessed on 31 August 2019).
- Wildau, G. China Migration: At the Turning Point. Financial Times. 4 May 2015. Available online: https://www.ft.com/content/767495a0-e99b-11e4-b863-00144feab7de (accessed on 11 July 2019).
- Abdin, S.; Welch, R.; Byron-Daniel, J.; Meyrick, J. The effectiveness of physical activity interventions in improving well-being across office-based workplace settings: A systematic review. Pub. Health 2018, 160, 70–76. [Google Scholar] [CrossRef] [PubMed]
- Oakman, J.; Neupane, S.; Proper, K.; Kinsman, N.; Nygård, C. Workplace interventions to improve work ability: A systematic review and meta-analysis of their effectiveness. Scand. J. Work Environ. Health 2018, 44, 134–146. [Google Scholar] [CrossRef] [PubMed]
- Commissaris, D.; Huysmans, M.; Mathiassen, S.; Srinivasan, D.; Koppes, L.; Hendriksen, I. Interventions to reduce sedentary behaviour and increase physical activity during productive work: A systematic review. Scand. J. Work Environ. Health 2016, 42, 181–191. [Google Scholar] [PubMed]
- Sjøgaard, G.; Christensen, J.; Justesen, J.; Murray, M.; Dalager, T.; Fredlund, G.; Søgaard, K. Exercise is more than medicine: The working age population’s well-being and productivity. J. Sport Health Sci. 2016, 5, 159–165. [Google Scholar] [CrossRef] [PubMed]
- Zhu, W.; Gutierrez, M.; Toledo, M.; Mullane, S.; Stella, A.; Diemar, R.; Buman, K.; Buman, M. Long-term effects of sit-stand workstations on workplace sitting: A natural experiment. J. Sci. Med. Sport 2018, 21, 811–816. [Google Scholar] [CrossRef] [PubMed]
- Lin, Y.; Hong, O.; Lin, C.C.; Lu, S.H.; Chen, M.M.; Lee, K.C. A “Sit Less, Walk More” workplace intervention for office workers: Long-term efficacy of a quasi-experimental study. J. Occup. Environ. Med. 2018, 60, e290–e299. [Google Scholar] [CrossRef] [PubMed]
- Lin, Y.; Lin, C.; Chen, M.M.; Lee, K.C. Short-term efficacy of a “Sit Less, Walk More” workplace intervention on improving cardiometabolic health and work productivity in office workers. J. Occup. Environ. Med. 2017, 59, 327–334. [Google Scholar] [CrossRef] [PubMed]
- Chen, M.M.; Tsai, A.C.; Wang, J.Y. The effectiveness and barriers of implementing a workplace health promotion program to improve metabolic disorders in older workers in Taiwan. Glob. Health Promot. 2016, 23, 6–14. [Google Scholar] [CrossRef] [PubMed]
- Yancey, A.K.; Sallis, R.E.; Bastani, R. Changing physical activity participation for the medical profession. JAMA 2013, 309, 141–142. [Google Scholar] [CrossRef] [PubMed]
- Barr-Anderson, D.J.; AuYoung, M.; Whitt-Glover, M.C.; Glenn, B.A.; Yancey, A.K. Integration of short bouts of physical activity into organisaitonal routine: A systematic review of the literature. Am. J. Prev. Med. 2010, 40, 76–93. [Google Scholar] [CrossRef] [PubMed]
- Huang, Y.; Benford, S.; Blake, H. Digital interventions to reduce sedentary behaviours of office workers: A scoping review. J. Med. Internet Res. 2019, 21, e11079. [Google Scholar] [CrossRef] [PubMed]
- Howarth, A.; Quesada, J.; Silva, J.; Judycki, S.; Mills, P.R. The impact of digital health interventions on health-related outcomes in the workplace: A systematic review. Digit. Health 2018, 4, 2055207618770861. [Google Scholar] [CrossRef] [PubMed]
- Hong, Y.A.; Zhou, Z. A profile of ehealth behaviors in China: Results from a national survey show a low of usage and significant digital divide. Front. Pub. Health 2018, 6, 274. [Google Scholar] [CrossRef]
- Klein, P.J.; Baumgarden, J.; Schneider, R. Qigong and Tai Chi as therapeutic exercise: Survey of systematic reviews and meta-analyses addressing physical health conditions. Altern. Ther. Health Med. 2019, AT5817, in press. [Google Scholar]
- Jahnke, R.; Larkey, L.; Rogers, C.; Etnier, J.; Lin, F. A comprehensive review of health benefits of Qigong and Tai Chi. Am. J. Health Promot. 2010, 24, e1–e25. [Google Scholar] [CrossRef]
- Chang, M.Y.; Chen, H.Y. Body composition outcomes of a qigong intervention among community dwelling ageing adults. West. J. Nurs. Res. 2016, 38, 1574–1594. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. Mental Health at Work: Impact, Issues and Good Practices. 2010. Available online: https://www.who.int/mental_health/media/en/712.pdf (accessed on 31 August 2019).
- Kachan, D.; Olano, H.; Tannenbaum, S.L.; Annane, D.W.; Mehta, A.; Arheart, K.L.; Fleming, L.E.; Yang, X.; McClure, L.A.; Lee, D.J. Prevalence of mindfulness practices in the US workforce: National health interview survey. Prev. Chronic Dis. 2017, 14, E01. [Google Scholar] [CrossRef] [PubMed]
- Montagni, I.; Dehman, A.; Jing’an, Y.Z.; Martinez, M.J.; Banner, S.; Rimbert, S.; Hayez, S.; Foster, C.; Fontvieille, A.M. Effectiveness of a blended web-based intervention to raise sleep awareness at workplace: The WarmUapp™ pilot study. J. Occup. Environ. Med. 2019, 61, e253–e259. [Google Scholar] [CrossRef] [PubMed]
- Pereira, J.P.; Coombes, B.K.; Comans, A.C.; Johnston, V. The impact of onsite workplace health-enhancing physical activity interventions on worker productivity: A systematic review. Occup. Environ. Med. 2015, 72, 401–402. [Google Scholar] [CrossRef] [PubMed]
- Glasgow, R.E.; Vogt, T.M.; Boles, S.M. Evaluating the public health impact of health promotion interventions: The RE-AIM framework. Am. J. Pub. Health 1999, 89, 1322–1327. [Google Scholar] [CrossRef] [PubMed]
- MacDonald, B.; Janssen, X.; Kirk, A.; Patience, M.; Gibson, A.M. An Integrative, Systematic Review Exploring the Research, Effectiveness, Adoption, Implementation, and Maintenance of Interventions to Reduce Sedentary Behaviour in Office Workers. Int. J. Environ. Res. Pub. Health 2018, 15, 2876. [Google Scholar] [CrossRef] [PubMed]
- Chang, P.S.; Chao, A.M.; Jang, M.; Lu, Y. Intervention fidelity in Qigong randomized controlled trials: A method review. Geriatr. Nurs. 2019, 40, 84–90. [Google Scholar] [CrossRef] [PubMed]
- Tucker, S.J.; Lanningham-Foster, L.M.; Murphy, J.N.; Thompson, W.G.; Weymiller, A.J.; Lohse, C.; Levine, J.A. Effects of a worksite physical activity intervention for hospital nurses who are working mothers. AAOHN J. 2011, 59, 377–386. [Google Scholar] [CrossRef]
- Renton, S.J.; Lightfoot, N.E.; Maar, M.A. Physical activity promotion in call centres: Employers’ perspectives. Health Educ. Res. 2011, 25, 1050–1059. [Google Scholar] [CrossRef] [PubMed]
- Asbury, L.D.; Wong, F.L.; Price, S.M.; Nolin, M.J. The VERB campaign: Applying a branding strategy in public health. Am. J. Prev. Med. 2008, 36, S183–S187. [Google Scholar] [CrossRef] [PubMed]
- Gardner, B.; Lally, P.; Wardle, J. Making health habitual: The psychology of ‘habit-formation’ and general practice. Br. J. Gen. Pract. 2012, 62, 664–666. [Google Scholar] [CrossRef] [PubMed]
- Michie, S.; Atkins, L.; West, R. The Behaviour Change Wheel: A Guide to Designing Interventions; Silverback Publishing: London, UK, 2014. [Google Scholar]
- Michie, S.; Richardson, M.; Johnston, M.; Abraham, C.; Francis, J.; Hardeman, W.; Eccles, M.P.; Cane, J.; Wood, C.E. The behavior change technique taxonomy (v1) of 93 hierarchically clustered techniques: Building an international consensus for the reporting of behavior change interventions. Ann. Behav. Med. 2013, 46, 81–95. [Google Scholar] [CrossRef] [PubMed]
- Hoffmann, T.C.; Glasziou, P.P.; Boutron, I.; Milne, R.; Perera, R.; Moher, D.; Altman, D.G.; Barbour, V.; Macdonald, H.; Johnston, M.; et al. Better reporting of interventions: Template for intervention description and replication (TIDieR) checklist and guide. BMJ 2014, 348, g1687. [Google Scholar] [CrossRef] [PubMed]
- Bale, J.M.; Gazmararian, J.A.; Elon, L. Effect of the work environment on using time at work to exercise. Am. J. Health Promot. 2015, 29, 345–352. [Google Scholar] [CrossRef] [PubMed]
- IPAQ Research Committee. Guidelines for the Data Processing and Analysis of the International Physical Activity Questionnaire. 2005. Available online: https://sites.google.com/site/theipaq (accessed on 11 July 2019).
- Kessler, R.C.; Ames, M.; Hymel, P.A.; Loeppke, R.; McKenas, D.K.; Richling, D.E.; Stang, P.E.; Ustun, T.B. Using the world health organization Health and Work Performance Questionnaire HPQ to evaluate the indirect workplace costs of illness. J. Occup. Environ. Med. 2004, 46, S23–S37. [Google Scholar] [CrossRef] [PubMed]
- Liu, T.J.; Zhang, W.C. Traditional Chinese Medicine Qigong; China Press of Traditional Chinese Medicine: Beijng, China, 2016. [Google Scholar]
- StataCorp. Stata Statistical Software: Release 16; StataCorp LLC: College Station, TX, USA, 2019. [Google Scholar]
- Anderson, D.; Villagra, V.G.; Coman, E.; Ahmed, T.; Porto, A.; Jepeal, N.; Maci, G.; Teevan, B. Reduced cost of specialty care using electronic consultations for medicaid patients. Health Aff. 2018, 37, 2031–2036. [Google Scholar] [CrossRef] [PubMed]
- Coman, E.N.; Picho, K.; McArdle, J.J.; Villagra, V.; Dierker, L.; Iordache, E. The paired t-test as a simple latent change score model. Front. Psychol. 2013, 4, 738. [Google Scholar] [CrossRef] [Green Version]
- Braun, V.; Clarke, V. Successful Qualitative Research: A Practical Guide for Beginners; Sage Publications Ltd.: London, UK, 2013. [Google Scholar]
- Belza, B.; Toobert, D.J.; Glasgow, R.E. RE-AIM for Program Planning: Overview and Applications. 2006. Available online: http://www.re-aim.org/2007-re-aim-for-program-planning-and-evaluation-overview-and-applications/ (accessed on 11 July 2019).
- Alley, S.; Jennings, C.; Plotnikoff, R.C.; Vandelanotte, C. Web-based video-coaching to assist an automated computer-tailored physical activity intervention for inactive adults: A randomized controlled trial. J. Med. Internet Res. 2016, 18, e223. [Google Scholar] [CrossRef] [PubMed]
- Handley, M.A.; Lyles, C.R.; McCullock, C.; Cattamanchi, A. Selecting and improving quasi-experimental designs in effectiveness and implementation research. Ann. Rev. Pub. Health 2018, 39, 5–25. [Google Scholar] [CrossRef]
- Conn, V.S.; Hafdahl, A.R.; Cooper, P.S.; Brown, L.M.; Lusk, S.L. Meta-analysis of workplace physical activity interventions. Am. J. Prev. Med. 2009, 37, 330–339. [Google Scholar] [CrossRef] [PubMed]
- Ilmarinen, J. The work ability index. Occup. Med. 2007, 57, 160. [Google Scholar] [CrossRef]
- Torp, S.; Grismsmo, A.; Hagen, S.; Duran, A.; Gudbergsson, S.B. Work engagement: A practical measure for workplace health promotion? Health Promot. Int. 2013, 28, 387–396. [Google Scholar] [CrossRef] [PubMed]
- Huang, Y.; Benford, S.; Hendrickx, H.; Treloar, R.; Blake, H. Office workers’ perceived barriers and facilitators to taking regular micro-breaks at work: A diary-probed interview study. In International Conference on Persuasive Technology; Springer: Cham, Switzerland, 2017. [Google Scholar]
- Krane, L.; Johnsen, R.; Fleten, N.; Nielsen, C.V.; Stapelfeldt, C.M.; Jensen, C.; Braaten, T. Sickness absence patterns and trends in the health care sector: 5-year monitoring of female municipal employees in the health and care sectors in Norway and Denmark. Hum. Resour. Health 2014, 12, 37. [Google Scholar] [CrossRef] [PubMed]
- Robroek, S.J.; van Lenthe, F.J.; van Empelen, P.; Burdorf, A. Determinants of participation in worksite health promotion programmes: A systematic review. Int. J. Behav. Nutr. Phys. Act. 2009, 20, 26. [Google Scholar] [CrossRef] [PubMed]
- Ryde, G.C.; Gilson, N.D.; Burton, N.W.; Brown, W.J. Recruitment rates in workplace physical activity interventions: Characteristics for success. Am. J. Health Promot. 2013, 27, E101–E112. [Google Scholar] [CrossRef]
- Parry, S.; Straker, L.; Gilson, N.D.; Smith, A.J. Participatory workplace interventions can reduce sedentary time for office workers—A randomised controlled trial. PLoS ONE 2013, 8, e78957. [Google Scholar] [CrossRef] [PubMed]
- Fry, J.P.; Neff, R.A. Periodic prompts and reminders in health promotion and health behavior interventions: Systematic review. J. Med. Internet Res. 2009, 11, e16. [Google Scholar] [CrossRef]
- Cooley, D.; Pedersen, S. A pilot study of increasing nonpurposeful movement breaks at work as a means of reducing prolonged sitting. J. Environ. Pub. Health 2013. [Google Scholar] [CrossRef]
- Bardus, M.; Blake, H.; Lloyd, S.; Suggs, L.S. Reasons for participating and not participating in a e-health workplace physical activity intervention: A qualitative analysis. Int. J. Workplace Health Manag. 2014, 7, 229–246. [Google Scholar] [CrossRef]
- Cui, Y.; Meng, J.; Lu, C. Recent developments in China’s labor market: Labour shortage, rising wages and their implications. Rev. Dev. Econ. 2018, 22, 1217–1238. [Google Scholar] [CrossRef]
- Dunbar, J.A.; Hernan, A.L.; Janus, E.D.; Vartialnen, E.; Laatikainen, T.; Versace, V.L.; Reynolds, J.; Best, J.D.; Skinner, T.C.; O’Reilly, S.L.; et al. Challenges of diabetes prevention in the real world—Results and lessons from the Melbourne Diabetes Prevention Study. BMJ Open Diabetes Res. Care 2015, 3, e000131. [Google Scholar] [CrossRef] [PubMed]
- Taylor, W.C. Transforming work breaks to promote health. Am. J. Prev. Med. 2005, 29, 461–465. [Google Scholar] [CrossRef] [PubMed]
- Glasgow, R.E.; Lichtenstein, E.; Marcus, A.C. Why don’t we see more translation of health promotion research into practice? Rethinking the efficacy-to-effectiveness transition. Am. J. Pub. Health 2003, 93, 1261–1267. [Google Scholar] [CrossRef] [PubMed]
- Moreira, R.F.C.; Foltran, F.A.; Albuquerque-Sendin, F.; Mancini, M.C.; Coury, H.J.C.G. Comparison of randomized and non-randomized trials evidence regarding the effectiveness of workplace exercise on musculoskeletal pain control. Work 2012, 41, 4782–4789. [Google Scholar] [PubMed]
- Pal, S.; Cheng, C.; Egger, G.; Binns, C.; Donovan, R. Using pedometers to increase physical activity in overweight and obese women: A pilot study. BMC Pub. Health 2009, 9, 309. [Google Scholar] [CrossRef] [PubMed]
- Justesen, J.B.; Søgaard, K.; Dalager, T.; Christensen, J.R.; Sjøgaard, G. The effect of intelligent physical exercise training on sickness presenteeism and absenteeism among office workers. J. Occup. Environ. Med. 2017, 59, 942–948. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Education | Persuasion | Training | Environmental Restructuring | Modelling | Enablement | |
|---|---|---|---|---|---|---|
| COM-B | ||||||
| C-Ph | X | X | ||||
| C-Ps | X | X | X | X | ||
| M-Re | X | X | ||||
| M-Au | X | X | X | X | ||
| O-Ph | X | |||||
| O-Soc | X | X | X | |||
| Policy | ||||||
| Communication and Marketing | X | X | X | |||
| Guidelines | X | X | X | |||
| Regulation | X | X | ||||
| Service Provision | X | X |
| Sample Characteristic (n = 282) | Intervention Group | Control Group |
|---|---|---|
| n (%) | n (%) | |
| All participants (baseline) | 196 (69.5) | 86 (30.5) |
| Gender | ||
| Female | 97 (49.5) | 37 (43.0) |
| Male | 96 (49.0) | 46 (53.5) |
| Not specified | 3 (1.5) | 3 (3.5) |
| Education | ||
| High school | 5 (2.6) | 0 (0) |
| College | 20 (10.2) | 1 (1.2) |
| University | 168 (85.7) | 82 (95.3) |
| Not specified | 3 (1.5) | 3 (3.5) |
| Marital status | ||
| Single | 58 (29.6) | 19 (22.1) |
| Married | 118 (60.2) | 62 (72.1) |
| Neither single nor married | 17 (8.7) | 2 (2.3) |
| Not specified | 3 (1.5) | 3 (3.5) |
| Tenure | ||
| <1 year | 24 (12.2) | 9 (10.5) |
| 1–3 years | 72 (36.7) | 41 (47.7) |
| 4–5 years | 26 (13.3) | 5 (5.8) |
| 5–10 years | 54 (27.6) | 17 (19.8) |
| >10 years | 17 (8.7) | 11 (12.8) |
| Not specified | 3 (1.5) | 3 (3.5) |
| T1 (Means) | (SD) | T2 (Means) | (SD) | Changes (InterceptsINT) | (SE) | p | Difference I-C 95% CI (Lower; Upper) | SE | d | p | |
|---|---|---|---|---|---|---|---|---|---|---|---|
| Physical activity (hours) | |||||||||||
| Control | 18.75 | (19.75) | 27.20 | (30.84) | 7.41 | 3.64 | 0.04 | −1.61 (−9.76; 6.53) | 4.16 | 0.05 | 0.70 |
| Intervention | 22.87 | (21.84) | 27.75 | (25.98) | 5.80 | 2.00 | 0.00 | ||||
| Work performanceALT | |||||||||||
| Control | 7.63 | (1.40) | 7.50 | (1.75) | 0.69 | 0.24 | 0.01 | −0.72 (−1.25; −0.19) | 0.27 | 0.36 | 0.01 |
| Intervention | 6.89 | (1.41) | 6.96 | (1.52) | −0.03 | 0.12 | 0.78 | ||||
| Sitting hours | |||||||||||
| Control | 9.20 | (2.20) | 9.41 | (2.01) | 10.34 | 1.04 | 0.00 | −4.66 (−7.25; −2.08) | 1.32 | 0.44 | <0.01 |
| Intervention | 9.51 | (2.69) | 9.64 | (2.55) | 5.68 | 0.82 | 0.00 |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Blake, H.; Lai, B.; Coman, E.; Houdmont, J.; Griffiths, A. Move-It: A Cluster-Randomised Digital Worksite Exercise Intervention in China: Outcome and Process Evaluation. Int. J. Environ. Res. Public Health 2019, 16, 3451. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph16183451
Blake H, Lai B, Coman E, Houdmont J, Griffiths A. Move-It: A Cluster-Randomised Digital Worksite Exercise Intervention in China: Outcome and Process Evaluation. International Journal of Environmental Research and Public Health. 2019; 16(18):3451. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph16183451
Chicago/Turabian StyleBlake, Holly, Betsy Lai, Emil Coman, Jonathan Houdmont, and Amanda Griffiths. 2019. "Move-It: A Cluster-Randomised Digital Worksite Exercise Intervention in China: Outcome and Process Evaluation" International Journal of Environmental Research and Public Health 16, no. 18: 3451. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph16183451