Gender Equality, Drinking Cultures and Second-Hand Harms from Alcohol in the 50 US States

 , and
, and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Survey Datasets
2.2. Measures
2.2.1. Outcome Variables
2.2.2. State-Level Predictors
2.2.3. Individual-Level Predictors
2.3. Analyses
3. Results
3.1. Main Effects Models
3.2. Moderation Models
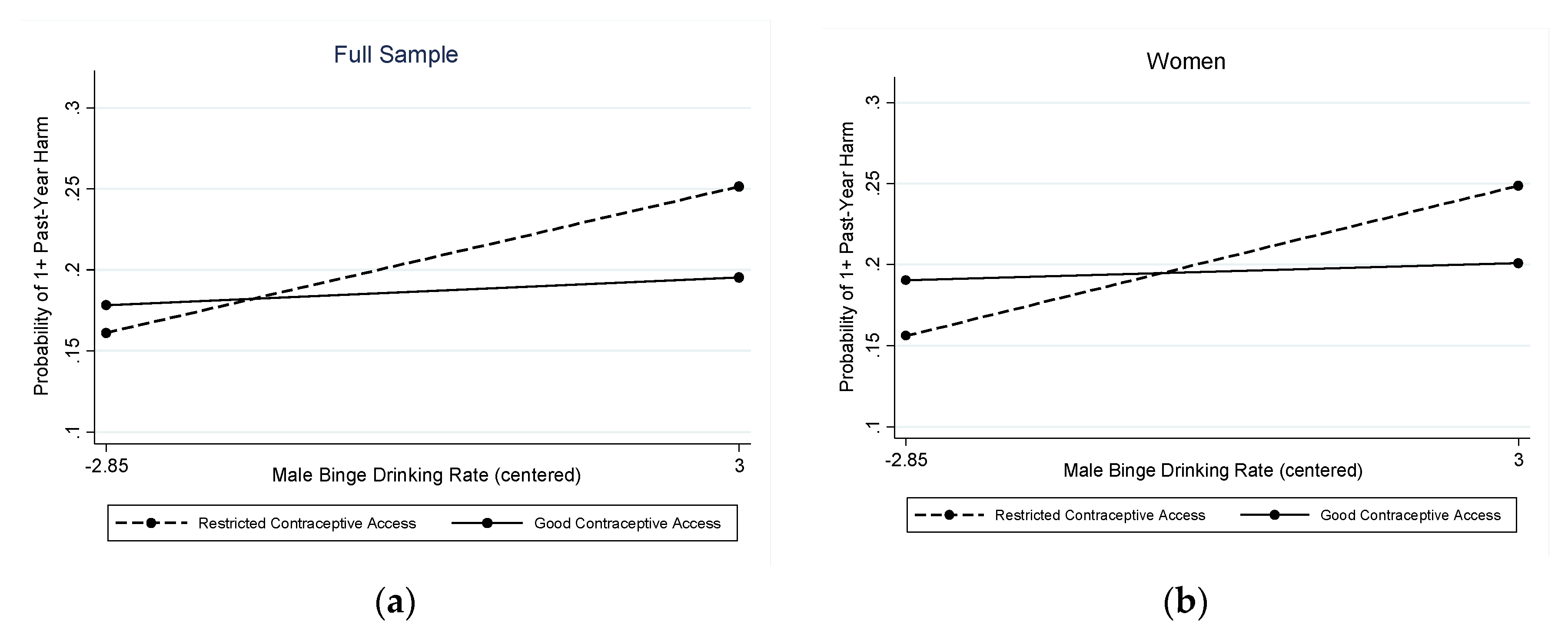
3.2.1. Any Past-Year Second-Hand Harm
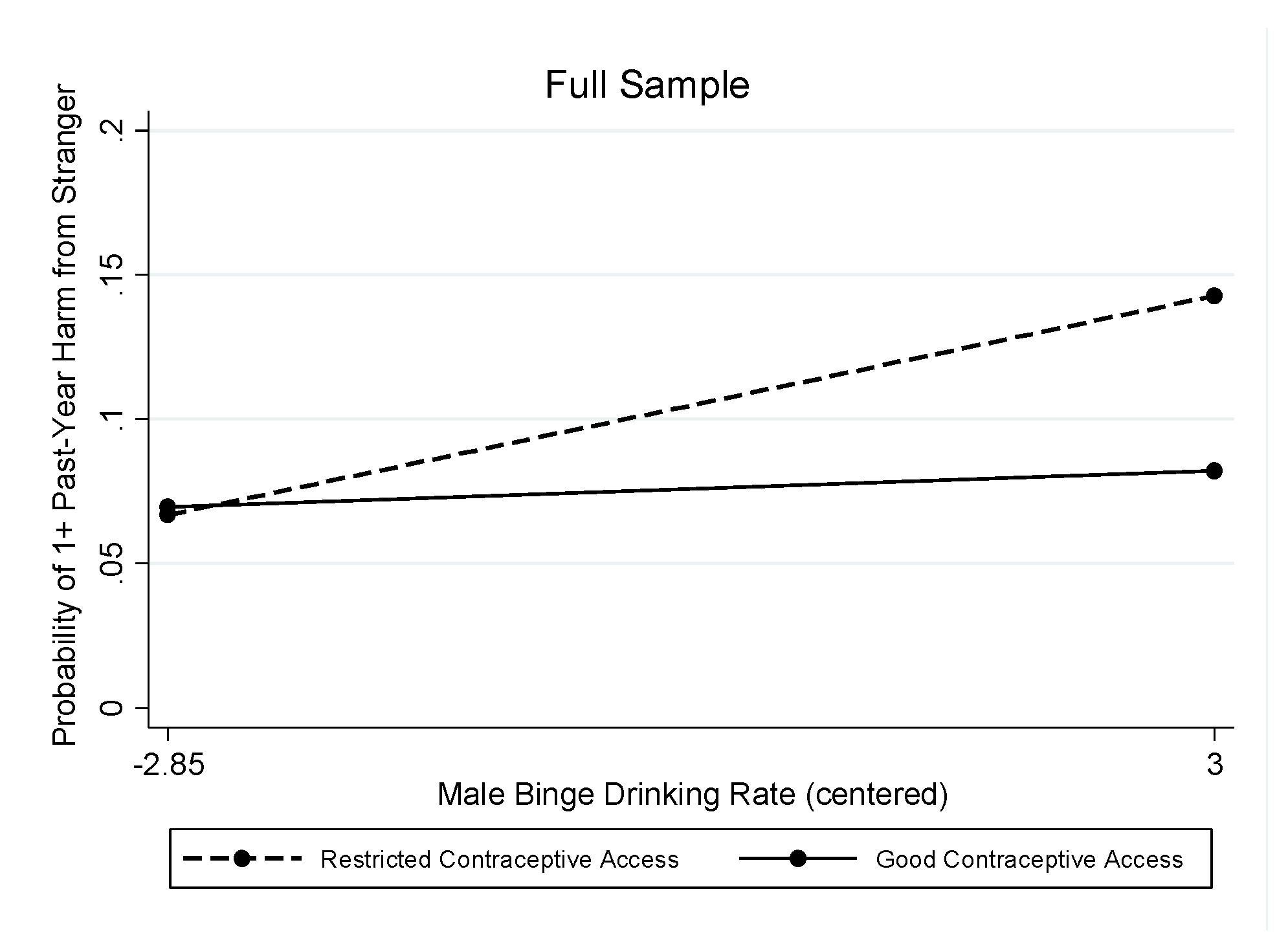
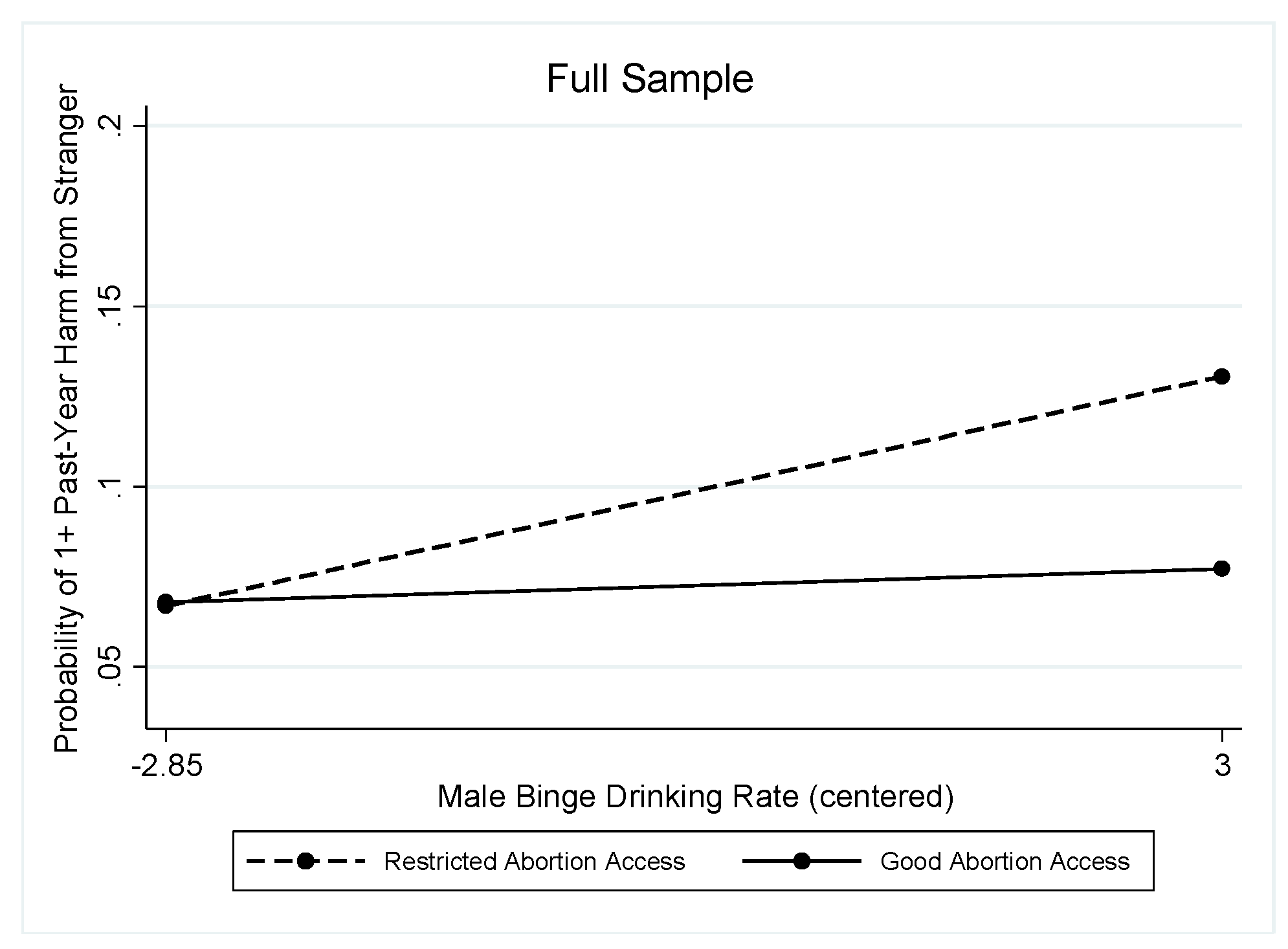
3.2.2. Past-Year Stranger-Perpetrated Harm
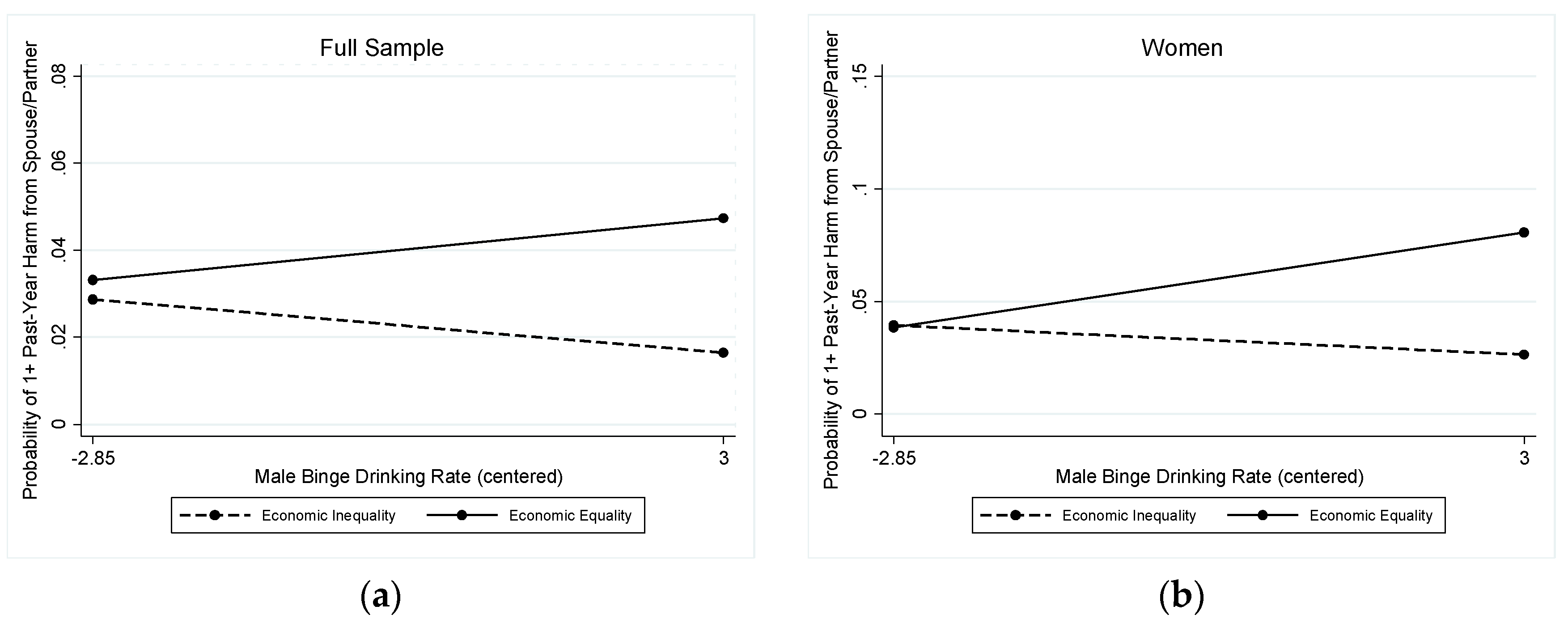
3.2.3. Past-Year Spouse- or Partner-Perpetrated Harm
4. Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Sen, G.; Ostlin, P. Gender inequity in health: Why it exists and how we can change it. Glob. Public Health 2008, 3 (Suppl. 1), 1–12. [Google Scholar] [CrossRef]
- King, T.L.; Kavanagh, A.M.; Scovelle, A.J.; Milner, A. Associations between gender equality and health: A systematic review. Health Promot. Int. 2018. [Google Scholar] [CrossRef] [PubMed]
- Borrell, C.; Palencia, L.; Muntaner, C.; Urquia, M.; Malmusi, D.; O’Campo, P. Influence of macrosocial policies on women’s health and gender inequalities in health. Epidemiol. Rev. 2014, 36, 31–48. [Google Scholar] [CrossRef] [PubMed]
- Kawachi, I.; Kennedy, B.P.; Gupta, V.; Prothrow-Stith, D. Women’s status and the health of women and men: A view from the States. Soc. Sci. Med. 1999, 48, 21–32. [Google Scholar] [CrossRef]
- Homan, P. Political gender inequality and infant mortality in the United States, 1990–2012. Soc. Sci. Med. 2017, 182, 127–135. [Google Scholar] [CrossRef] [PubMed]
- Koenen, K.C.; Lincoln, A.; Appleton, A. Women’s status and child well-being: A state-level analysis. Soc. Sci. Med. 2006, 63, 2999–3012. [Google Scholar] [CrossRef]
- Kavanagh, S.A.; Shelley, J.M.; Stevenson, C. Does gender inequity increase men’s mortality risk in the United States? A multilevel analysis of data from the National Longitudinal Mortality Study. SSM Popul. Health 2017, 3, 358–365. [Google Scholar] [CrossRef]
- Roberts, S.C.M. What can alcohol researchers learn from research about the relationship between macro-level gender equality and violence against women? Alcohol Alcohol. 2011, 46, 95–104. [Google Scholar] [CrossRef]
- Schwab, K.; Samans, R.; Zahidi, S.; Leopold, T.A.; Ratcheva, V.; Hausmann, R.; Tyson, L.D. The Global Gender Gap Report 2017; World Economic Forum: Geneva, Switzerland, 2017; p. 349. Available online: https://www.weforum.org/reports/the-global-gender-gap-report-2017 (accessed on 7 May 2018).
- United Nations Development Programme Gender Inequality Index. Available online: Http://hdr.undp.org/en/content/gender-inequality-index-gii (accessed on 5 July 2018).
- Institute for Women’s Policy Research. Status of Women in the States; Institute for Women’s Policy Research: Washington, DC, USA, 2018; p. 7. Available online: Https://iwpr.org/publications/status-of-women-fact-sheet-2018/ (accessed on 7 May 2018).
- Roberts, S.C.M. Macro-level gender equality and alcohol consumption: A multi-level analysis across U.S. states. Soc. Sci. Med. 2012, 75, 60–68. [Google Scholar] [CrossRef]
- Petticrew, M.; Shemilt, I.; Lorenc, T.; Marteau, T.M.; Melendez-Torres, G.J.; O’Mara-Eves, A.; Stautz, K.; Thomas, J. Alcohol advertising and public health: Systems perspectives versus narrow perspectives. J. Epidemiol. Community Health 2017, 71, 308–312. [Google Scholar] [CrossRef]
- Emslie, C.; Hunt, K.; Lyons, A. Transformation and time-out: The role of alcohol in identity construction among Scottish women in early midlife. Int. J. Drug Policy 2015, 26, 437–445. [Google Scholar] [CrossRef] [PubMed]
- Kuntsche, E.; Kuntsche, S.; Knibbe, R.; Simons-Morton, B.; Farhat, T.; Hublet, A.; Bendtsen, P.; Godeau, E.; Demetrovics, Z. Cultural and gender convergence in adolescent drunkenness: Evidence from 23 European and North American countries. Arch. Pediatr. Adolesc. Med. 2011, 165, 152–158. [Google Scholar] [CrossRef] [PubMed]
- Wilsnack, R.W.; Wilsnack, S.C.; Gmel, G.; Kantor, L.W. Gender differences in binge drinking: Prevalence, predictors, and consequences. Alcohol Res. 2018, 39, 1–20. [Google Scholar]
- Giesbrecht, N.; Cukier, S.; Steeves, D. (Eds.) Collateral damage from alcohol: Implications of ‘second-hand effects of drinking’ for populations and health priorities. Addiction 2010, 105, 1323–1325. [Google Scholar] [CrossRef]
- Room, R.; Ferris, J.; Laslett, A.-M.; Livingston, M.; Mugavin, J.; Wilkinson, C. The drinker’s effect on the social environment: A conceptual framework for studying alcohol’s harm to others. Int. J. Environ. Res. Public Health 2010, 7, 1855–1871. [Google Scholar] [CrossRef]
- Karriker-Jaffe, K.J.; Greenfield, T.K.; Kaplan, L.M. Distress and alcohol-related harms from intimates, friends and strangers. J. Subst. Use 2017, 22, 434–441. [Google Scholar] [CrossRef]
- Greenfield, T.K.; Ye, Y.; Kerr, W.; Bond, J.; Rehm, J.; Giesbrecht, N. Externalities from alcohol consumption in the 2005 US National Alcohol Survey: Implications for policy. Int. J. Environ. Res. Public Health 2009, 6, 3205–3224. [Google Scholar] [CrossRef]
- Laslett, A.-M.; Catalano, P.; Chikritzhs, T.; Dale, C.; Doran, C.; Ferris, J.; Jainullabudeen, T.; Livingston, M.; Matthews, S.; Mugavin, J.; et al. The Range and Magnitude of Alcohol’s Harm to Others; AER Centre for Alcohol Policy Research, Turning Point Alcohol and Drug Centre, Eastern Health: Fitzroy, Australia, 2010; p. 214. Available online: http://www.webcitation.org/5wB6fDhnQ (accessed on 1 February 2011).
- Wilsnack, R.W.; Kristjanson, A.F.; Wilsnack, S.C.; Bloomfield, K.; Grittner, U.; Crosby, R.D. The harms that drinkers cause: Regional variations within countries. Int. J. Alcohol Drug Res. 2018, 7, 30–36. [Google Scholar] [CrossRef]
- Room, R.; Callinan, S.; Greenfield, T.K.; Rekve, D.; Waleewong, O.; Stanesby, O.; Thamarangsi, T.; Benegal, V.; Casswell, S.; Florenzano, R.; et al. The social location of harm from others’ drinking in ten societies. Addiction 2019, 114, 425–433. [Google Scholar] [CrossRef]
- Karriker-Jaffe, K.J.; Greenfield, T.K. Gender differences in associations of neighbourhood disadvantage with alcohol’s harms to others: A cross-sectional study from the USA. Drug Alcohol Rev. 2014, 33, 296–303. [Google Scholar] [CrossRef]
- Nayak, M.B.; Patterson, D.; Wilsnack, S.C.; Karriker-Jaffe, K.J.; Greenfield, T.K. Alcohol’s secondhand harms in the United States.: New data on prevalence and risk factors. J. Stud. Alcohol Drugs 2019, 80, 273–281. [Google Scholar] [CrossRef] [PubMed]
- Ferris, J.A.; Laslett, A.-M.; Livingston, M.; Room, R.; Wilkinson, C. The impacts of others’ drinking on mental health. Med. J. Aust. 2011, 195 (Suppl. 3), 22–26. [Google Scholar] [CrossRef]
- Karriker-Jaffe, K.J.; Li, L.; Greenfield, T.K. Estimating mental health impacts of alcohol’s harms from other drinkers: Using propensity scoring methods with national cross-sectional data from the United States. Addiction 2018, 113, 1826–1839. [Google Scholar] [CrossRef] [PubMed]
- Casswell, S.; You, R.Q.; Huckle, T. Alcohol’s harm to others: Reduced wellbeing and health status for those with heavy drinkers in their lives. Addiction 2011, 106, 1087–1094. [Google Scholar] [CrossRef]
- Greenfield, T.K.; Karriker-Jaffe, K.J.; Kerr, W.C.; Ye, Y.; Kaplan, L.M. Those harmed by others’ drinking in the US population are more depressed and distressed. Drug Alcohol Rev. 2016, 35, 22–29. [Google Scholar] [CrossRef] [PubMed]
- Yllö, K. The status of women, marital equality and violence against wives: A contextual analysis. J. Fam. Issues 1984, 5, 307–320. [Google Scholar] [CrossRef]
- Lei, M.K.; Simons, R.L.; Simons, L.G.; Edmond, M.B. Gender equality and violent behavior: How neighborhood gender equality influences the gender gap in violence. Violence Vict. 2014, 29, 89–108. [Google Scholar] [CrossRef]
- Bond, J.C.; Roberts, S.C.M.; Greenfield, T.K.; Korcha, R.; Ye, Y.; Nayak, M.B. Gender differences in public and private drinking contexts: A multi-level GENACIS analysis. Int. J. Environ. Res. Public Health 2010, 7, 2136–2160. [Google Scholar] [CrossRef]
- Roberts, S.C.M.; Bond, J.; Korcha, R.; Greenfield, T.K. Genderedness of bar drinking culture and alcohol-related harms: A multi-country study. Int. J. Ment. Health Addict. 2013, 11, 50–63. [Google Scholar] [CrossRef]
- Room, R. Intoxication and bad behaviour: Understanding cultural differences in the link. Soc. Sci. Med. 2001, 53, 189–198. [Google Scholar] [CrossRef]
- Kerr, W.C. Categorizing US state drinking practices and consumption trends. Int. J. Environ. Res. Public Health 2010, 7, 269–283. [Google Scholar] [CrossRef] [PubMed]
- Naimi, T.S.; Brewer, R.D.; Mokdad, A.; Denny, C.; Serdula, M.K.; Marks, J.S. Binge drinking among U.S. adults. JAMA 2003, 289, 70–75. [Google Scholar] [CrossRef] [PubMed]
- Nelson, T.F.; Naimi, T.S.; Brewer, R.D.; Wechsler, H. The state sets the rate: The relationship among state-specific college binge drinking, state binge drinking rates, and selected state alcohol control policies. Am. J. Public Health 2005, 95, 441–446. [Google Scholar] [CrossRef] [PubMed]
- Wechsler, H.; Lee, J.E.; Hall, J.; Wagenaar, A.C.; Lee, H. Secondhand effects of student alcohol use reported by neighbors of colleges: The role of alcohol outlets. Soc. Sci. Med. 2002, 55, 425–435. [Google Scholar] [CrossRef] [Green Version]
- Stanesby, O.; Callinan, S.; Graham, K.; Wilson, I.M.; Greenfield, T.K.; Wilsnack, S.; Hettige, S.; Hanh, H.; Ibanga, A.; Siengsounthone, L.; et al. Harm from known others’ drinking by relationship proximity to the harmful drinker and gender: A meta-analysis across 10 countries. Alcohol. Clin. Exp. Res. 2018, 42, 1693–1703. [Google Scholar] [CrossRef] [PubMed]
- Kaplan, L.M.; Nayak, M.B.; Greenfield, T.K.; Karriker-Jaffe, K.J. Alcohol’s harm to children: Findings from the 2015 United States National Alcohol’s Harm to Others Survey. J. Pediatr. 2017, 184, 186–192. [Google Scholar] [CrossRef] [Green Version]
- Greenfield, T.K.; Karriker-Jaffe, K.J.; Giesbrecht, N.; Kerr, W.C.; Ye, Y.; Bond, J. Second-hand drinking may increase support for alcohol policies: New results from the 2010 National Alcohol Survey. Drug Alcohol Rev. 2014, 33, 259–267. [Google Scholar] [CrossRef]
- Eliany, M.; Giesbrecht, N.; Nelson, M.; Wellman, B.; Wortley, S. Alcohol and Other Drug Use by Canadians: A National Alcohol and Other Drugs Survey (1989) Technical Report; The Unit: Ottawa, ON, Canada, 1992; p. 450. [Google Scholar]
- World Health Organization. Harm to Others from Drinking: A WHO/Thai Health International Collaborative Research Project. Master Research Protocol; WHO: Geneva, Switzerland, 2012; p. 22. [Google Scholar]
- NARAL Pro-Choice America. Who Decides? The Status of Women’s Reproductive Rights in the United States; NARAL: Washington, DC, USA, 2015; Available online: Https://www.prochoiceamerica.org/wp-content/uploads/2017/04/2015-Who-Decides.pdf (accessed on 7 May 2018).
- Roberts, S.C.M.; Biggs, M.A.; Chibber, K.S.; Gould, H.; Rocca, C.H.; Foster, D.G. Risk of violence from the man involved in the pregnancy after receiving or being denied an abortion. BMC Med. 2014, 12, 144. [Google Scholar] [CrossRef] [Green Version]
- Institute for Women’s Policy Research Status of Women in the States: Download the Data. Available online: Https://statusofwomendata.org/explore-the-data/download-the-data/ (accessed on 21 June 2017).
- Centers for Disease Control and Prevention. Behavioral Risk Factor Surveillance System Survey Data and Documentation; Centers for Disease Control and Prevention: Atlanta, GA, USA, 2013. [Google Scholar]
- U.S. Census Bureau. 2011–2015 American Community Survey. Data Profiles; U.S. Census Bureau: Washington, DC, USA, 2015. Available online: http://www.webcitation.org/6tv0XSKlm (accessed on 2 October 2017).
- StataCorp. Stata Statistical Software: Release 15; StataCorp LLC: College Station, TX, USA, 2017. [Google Scholar]
- Rossow, I.; Hauge, R. Who pays for the drinking? Characteristics of the extent and distribution of social harms from others’ drinking. Addiction 2004, 99, 1094–1102. [Google Scholar] [CrossRef]
- Seid, A.K.; Grittner, U.; Greenfield, T.K.; Bloomfield, K. To cause harm and to be harmed by others: New perspectives on alcohol’s harms to others. Subst. Abuse 2015, 9 (Suppl. 2), 13–22. [Google Scholar] [CrossRef]
- Atkinson, A.M.; Kirton, A.W.; Sumnall, H.R. The gendering of alcohol in consumer magazines: An analysis of male and female targeted publications. J. Gend. Stud. 2012, 21, 365–386. [Google Scholar] [CrossRef]
- Peralta, R.L. Raced and gendered reactions to the deviance of drunkenness: A sociological analysis of race and gender disparities in alcohol use. Contemp. Drug Probl. 2010, 37, 381–415. [Google Scholar] [CrossRef] [Green Version]
- Keyes, K.M.; Jager, J.; Mal-Sarkar, T.; Patrick, M.E.; Rutherford, C.; Hasin, D. Is There a Recent Epidemic of Women’s Drinking? A Critical Review of National Studies. Alcohol. Clin. Exp. Res. 2019, 43, 1344–1359. [Google Scholar] [CrossRef] [PubMed]
- Kuntsche, S.; Knibbe, R.A.; Kuntsche, E.; Gmel, G. Housewife or working mum--Each to her own? The relevance of societal factors in the association between social roles and alcohol use among mothers in 16 industrialized countries. Addiction 2011, 106, 1925–1932. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Flood, M.; Pease, B. Factors influencing attitudes to violence against women. Trauma Violence Abuse 2009, 10, 125–142. [Google Scholar] [CrossRef] [Green Version]
- Reingold, R.B.; Gostin, L.O. State Abortion Restrictions and the New Supreme Court: Women’s Access to Reproductive Health Services. JAMA 2019, 322, 21–22. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variables | Full Sample | Men | Women | p |
|---|---|---|---|---|
| N = 7792 | n = 3156 | n = 4636 | ||
| Unmarried (%) | 42.3 | 40.1 | 44.3 | * |
| Race/Ethnicity (%) | *** | |||
| White | 66.4 | 67.2 | 65.8 | |
| Black | 11.9 | 10.7 | 13.0 | |
| Hispanic | 14.1 | 15.0 | 13.3 | |
| Other/Missing | 7.5 | 7.1 | 7.9 | |
| Less than College Degree | 70.2 | 69.1 | 71.2 | |
| Income (%) | *** | |||
| Up to $20,000 | 20.9 | 18.0 | 23.6 | |
| $20,000–$60,000 | 32.6 | 33.7 | 31.7 | |
| $60,001–$100,000 | 20.3 | 21.0 | 19.7 | |
| $100,001 or more | 14.9 | 18.0 | 12.1 | |
| Missing Income | 11.3 | 9.3 | 13.0 | |
| Age, M (SD) | 52.6 (17.7) | 51.3 (17.6) | 53.5 (17.6) | † |
| Drinking Status (%) | *** | |||
| Non-Drinker | 33.3 | 29.7 | 36.7 | |
| Drinker, Does not Exceed Guidelines a | 38.8 | 37.4 | 40.0 | |
| At-risk Drinker, Exceeds Guidelines | 28.0 | 32.9 | 23.3 | |
| State Median Income (by $10k), M (SD) | 5.4 (0.8) | 5.5 (0.8) | 5.5 (0.8) | |
| State Male Binge Drinking %, M (SD) | 23.1 (2.9) | 23.0 (2.9) | 23.0 (2.9) | |
| State Female Binge Drinking %, M (SD) | 11.1 (2.1) | 11.1 (2.1) | 11.0 (2.1) | |
| State Gender Equality Indicators (%) | ||||
| Contraceptive Access | 80.5 | 80.3 | 80.6 | |
| Reproductive Rights | 43.6 | 44.2 | 43.1 | |
| Economic Equality | 78.7 | 79.0 | 78.4 |
| Predictor Variables | Full Sample | Men | Women |
|---|---|---|---|
| (N = 7792) | (n = 3156) | (n = 4636) | |
| OR (95% CI) | OR (95% CI) | OR (95% CI) | |
| Male | 0.93 (0.80, 1.08) | - | - |
| Unmarried | 1.36 (1.06, 1.74) * | 1.71 (1.26, 2.31) *** | 1.13 (0.87, 1.48) |
| Race/Ethnicity 2 | |||
| Black | 1.06 (0.85, 1.31) | 1.06 (0.70, 1.59) | 1.03 (0.78, 1.37) |
| Hispanic | 0.87 (0.71, 1.05) | 0.96 (0.62, 1.49) | 0.74 (0.53, 1.03) † |
| Other/Missing | 1.40 (0.99, 2.00) † | 1.69 (1.06, 2.69) * | 1.21 (0.71, 2.07) |
| Less than College Degree | 1.08 (0.86, 1.36) | 1.20 (0.84, 1.69) | 1.02 (0.74, 1.39) |
| Income 3 | |||
| Up to $20,000 | 1.75 (1.26, 2.43) ** | 1.42 (0.90, 2.26) | 2.05 (1.37, 3.08) *** |
| $20,000–$60,000 | 1.41 (1.04, 1.93) * | 1.28 (0.76, 2.15) | 1.55 (1.06, 2.27) * |
| $60,001–$100,000 | 1.11 (0.81, 1.52) | 1.21 (0.75, 1.94) | 0.96 (0.62, 1.48) |
| Missing Income | 0.99 (0.74, 1.33) | 1.09 (0.62, 1.95) | 0.90 (0.57, 1.41) |
| Age | 0.98 (0.97, 0.98) *** | 0.98 (0.97, 0.99) *** | 0.97 (0.96, 0.98) *** |
| Drinking Status 4 | |||
| Drinker, Does not Exceed Guidelines | 1.14 (0.90, 1.45) | 0.96 (0.64, 1.44) | 1.26 (0.92, 1.74) |
| At-risk Drinker, Exceeds Guidelines | 2.32 (1.89, 2.84) *** | 2.14 (1.51, 3.03) | 2.53 (1.86, 3.44) *** |
| State Median Income | 1.06 (0.17, 6.65) | 0.92 (0.05, 16.82) | 1.97 (0.88, 1.17) |
| State Male Binge Drinking Rate | 1.11 (1.01, 1.23) * | 1.07 (0.93, 1.24) | 1.12 (1.02, 1.22) * |
| State Female Binge Drinking Rate | 1.02 (0.86, 1.22) | 1.00 (0.79, 1.25) | 1.01 (0.88, 1.17) |
| Contraceptive Access 5 | 0.90 (0.65, 1.24) | 0.84 (0.49, 1.43) | 0.99 (0.73, 1.32) |
| Male Binge * Contraceptive Access 6 | 0.92 (0.85, 0.99) * | - | 0.91 (0.85, 0.97) ** |
| Constant | 0.34 (0.12, 0.96) * | 0.23 (0.03, 1.60) | 0.29 (0.12, 0.69) ** |
| Predictor Variables | Full Sample | Men | Women |
|---|---|---|---|
| (N = 7792) | (n = 3156) | (n = 4636) | |
| OR (95% CI) | OR (95% CI) | OR (95% CI) | |
| Male | 1.37 (1.07, 1.74) * | - | - |
| Unmarried | 1.34 (1.03, 1.75) * | 1.52 (0.96, 2.40) † | 1.31 (0.92, 1.87) |
| Race/Ethnicity 1 | |||
| Black | 1.08 (0.74, 1.57) | 1.19 (0.67, 2.11) | 0.92 (0.57, 1.47) |
| Hispanic | 0.90 (0.66, 1.21) | 0.86 (0.51, 1.46) | 0.82 (0.44, 1.51) |
| Other/Missing | 1.64 (1.11, 2.42) * | 2.49 (1.43, 4.33) ** | 0.97 (0.48, 1.97) |
| Less than College Degree | 0.90 (0.64, 1.26) | 1.21 (0.74, 1.98) | 0.67 (0.43, 1.05) † |
| Income 2 | |||
| Up to $20,000 | 1.34 (0.85, 2.11) | 0.84 (0.43, 1.63) | 1.89 (0.91, 3.96) † |
| $20,000–$60,000 | 1.23 (0.75, 2.04) | 1.21 (0.60, 2.44) | 1.19 (0.65, 2.16) |
| $60,001–$100,000 | 0.97 (0.64, 1.48) | 1.04 (0.53, 2.04) | 0.82 (0.38, 1.77) |
| Missing Income | 1.01 (0.61, 1.67) | 1.08 (0.52, 2.22) | 0.88 (0.36, 2.14) |
| Age | 0.97 (0.97, 0.98) *** | 0.99 (0.97, 1.00) * | 0.96 (0.95, 0.97) *** |
| Drinking Status 3 | |||
| Drinker, Does not Exceed Guidelines | 0.95 (0.70, 1.29) | 0.89 (0.55, 1.43) | 0.92 (0.53, 1.61) |
| At-risk Drinker, Exceeds Guidelines | 1.85 (1.41, 2.44) *** | 1.80 (1.11, 2.93) * | 1.82 (1.06, 3.12) * |
| State Median Income | 1.02 (0.15, 7.11) | 0.48 (0.02, 12.16) | 1.72 (0.74, 1.18) |
| State Male Binge Drinking Rate | 1.17 (1.04, 1.31) * | 1.08 (0.94, 1.25) | 1.13 (0.95, 1.36) |
| State Female Binge Drinking Rate | 1.02 (0.85, 1.22) | 1.02 (0.80, 1.28) | 0.93 (0.74, 1.18) |
| Contraceptive Access 4 | 0.74 (0.48, 1.14) | 0.84 (0.38, 1.87) | 0.68 (0.35, 1.34) |
| Male Binge * Contraceptive Access 5 | 0.89 (0.81, 0.97) * | - | - |
| Constant | 1.73 (0.44, 0.67) * | 0.13 (0.01, 1.32) † | 0.32 (0.06, 1.76) |
| Predictor Variables | Full Sample | Men | Women |
|---|---|---|---|
| (N = 7792) | (n = 3156) | (n = 4636) | |
| OR (95% CI) | OR (95% CI) | OR (95% CI) | |
| Male | 1.36 (1.07, 1.74) * | - | - |
| Unmarried | 1.34 (1.03, 1.74) * | 1.52 (0.96, 2.41) † | 1.31 (0.92, 1.86) |
| Race/Ethnicity 1 | |||
| Black | 1.08 (0.74, 1.56) | 1.18 (0.67, 2.08) | 0.90 (0.56, 1.44) |
| Hispanic | 0.90 (0.66, 1.22) | 0.87 (0.51, 1.48) | 0.81 (0.44, 1.49) |
| Other/Missing | 1.63 (1.11, 2.41) * | 2.50 (1.44, 4.35) ** | 0.97 (0.47, 1.97) |
| Less than College Degree | 0.90 (0.64, 1.26) | 1.21 (0.74, 1.97) | 0.67 (0.43, 1.05) † |
| Income 2 | |||
| Up to $20,000 | 1.34 (0.85, 2.11) | 0.84 (0.43, 1.63) | 1.90 (0.90, 3.99) † |
| $20,000–$60,000 | 1.23 (0.75, 2.03) | 1.21 (0.60, 2.42) | 1.19 (0.65, 2.16) |
| $60,001–$100,000 | 0.97 (0.64, 1.48) | 1.04 (0.53, 2.03) | 0.81 (0.37, 1.76) |
| Missing Income | 1.01 (0.61, 1.67) | 1.08 (0.52, 2.22) | 0.89 (0.36, 2.16) |
| Age | 0.97 (0.97, 0.98) *** | 0.99 (0.97, 1.00) * | 0.96 (0.95, 0.97) *** |
| Drinking Status 3 | |||
| Drinker, Does not Exceed Guidelines | 0.95 (0.70, 1.29) | 0.89 (0.55, 1.42) | 0.91 (0.52, 1.59) |
| At-risk Drinker, Exceeds Guidelines | 1.85 (1.40, 2.43) *** | 1.80 (1.11, 2.92) * | 1.81 (1.05, 3.11) * |
| State Median Income | 1.68 (0.26, 11.02) | 1.63 (0.07, 37.35) | 2.87 (0.39, 20.94) |
| State Male Binge Drinking Rate | 1.14 (1.02, 1.29) * | 1.06 (0.92, 1.23) | 1.18 (0.95, 1.48) |
| State Female Binge Drinking Rate | 1.02 (0.85, 1.22) | 1.07 (0.83, 1.38) | 0.96 (0.74, 1.25) |
| Abortion Rights | 0.74 (0.49, 1.12) | 0.64 (0.30, 1.37) | 0.81 (0.46, 1.42) |
| Male Binge * Abortion Rights 4 | 0.90 (0.82, 0.98) * | - | 0.88 (0.76, 1.01) † |
| Constant | 0.12 (0.04, 0.40) *** | 0.07 (0.01, 0.51) ** | 0.21 (0.54, 0.84) * |
| Predictor Variables | Full Sample | Men | Women |
|---|---|---|---|
| (N = 7792) | (n = 3156) | (n = 4636) | |
| OR (95% CI) | OR (95% CI) | OR (95% CI) | |
| Male | 0.42 (0.26, 0.68) *** | - | - |
| Unmarried | 0.87 (0.56, 1.34) | 1.02 (0.38, 2.69) | 0.84 (0.50, 1.42) |
| Race/Ethnicity 1 | |||
| Black | 0.96 (0.52, 1.79) | 1.49 (0.57, 3.88) | 0.80 (0.39, 1.65) |
| Hispanic | 0.78 (0.45, 1.35) | 1.38 (0.44, 4.34) | 0.66 (0.34, 1.30) |
| Other/Missing | 1.71 (0.87, 3.39) | 3.02 (0.90, 10.15) † | 1.40 (0.61, 3.23) |
| Less than College Degree | 1.50 (0.98, 2.31) † | 1.29 (0.52, 3.20) | 1.53 (0.96, 2.44) † |
| Income 2 | |||
| Up to $20,000 | 1.81 (0.94, 3.45) † | 1.90 (0.71, 5.07) | 1.87 (0.76, 4.61) |
| $20,000–$60,000 | 1.20 (0.67, 2.17) | 0.66 (0.20, 2.24) | 1.60 (0.69, 3.68) |
| $60,001–$100,000 | 0.95 (0.49, 1.85) | 0.80 (0.38, 1.69) | 0.98 (0.41, 2.34) |
| Missing Income | 0.58 (0.25, 1.38) | 0.77 (1.17, 3.53) | 0.49 (0.18, 1.31) |
| Age | 0.98 (0.97, 0.99) *** | 1.00 (0.98, 1.01) | 0.97 (0.96, 0.98) *** |
| Drinking Status 3 | |||
| Drinker, Does not Exceed Guidelines | 1.51 (0.88, 2.58) | 1.64 (0.53, 5.06) | 1.39 (0.67, 2.88) |
| At-risk Drinker, Exceeds Guidelines | 2.23 (1.37, 3.65) ** | 2.68 (1.04, 6.88) * | 2.13 (1.06, 4.27) * |
| State Median Income | 2.96 (0.07, 117.38) | 7.06 (0.06, 781.29) | 5.16 (0.05, 540.02) |
| State Male Binge Drinking Rate | 0.90 (0.76, 1.07) | 0.90 (0.71, 1.14) | 0.93 (0.74, 1.16) |
| State Female Binge Drinking Rate | 0.90 (0.67, 1.20) | 1.02 (0.68, 1.50) | 0.85 (0.61, 1.19) |
| Economic Equality | 1.88 (0.97, 3.63) † | 1.39 (0.62, 3.12) | 1.83 (0.70, 4.80) |
| Male Binge * Economic Equality 4 | 1.18 (1.00, 1.39) * | - | 1.25 (1.02, 1.54) * |
| Constant | 0.02 (0.00, 0.12) *** | 0.00 (0.00, 0.03) *** | 0.01 (0.00, 0.16) ** |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Karriker-Jaffe, K.J.; Tam, C.C.; Cook, W.K.; Greenfield, T.K.; Roberts, S.C.M. Gender Equality, Drinking Cultures and Second-Hand Harms from Alcohol in the 50 US States. Int. J. Environ. Res. Public Health 2019, 16, 4619. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph16234619
Karriker-Jaffe KJ, Tam CC, Cook WK, Greenfield TK, Roberts SCM. Gender Equality, Drinking Cultures and Second-Hand Harms from Alcohol in the 50 US States. International Journal of Environmental Research and Public Health. 2019; 16(23):4619. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph16234619
Chicago/Turabian StyleKarriker-Jaffe, Katherine J., Christina C. Tam, Won Kim Cook, Thomas K. Greenfield, and Sarah C.M. Roberts. 2019. "Gender Equality, Drinking Cultures and Second-Hand Harms from Alcohol in the 50 US States" International Journal of Environmental Research and Public Health 16, no. 23: 4619. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph16234619