Smoking and Mental Illness: Prevalence, Patterns and Correlates of Smoking and Smoking Cessation among Psychiatric Patients

 , , , , , , ,
, , , , , , ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Participants
2.2. Measures
2.2.1. Smoking Habits and Cessation
2.2.2. Health Status
2.2.3. Nicotine Dependence (ND)
2.3. Analysis
2.3.1. Sampling and Sample Size
2.3.2. Statistical Analysis
3. Results
3.1. Sociodemographics
3.2. Prevalence of Smoking and Smoking Habits Subsection
3.3. Nicotine Dependence
3.4. Factors Associated with Smoking
3.5. Smoking Cessation: Motivators and Help Seeking
3.5.1. Help Seeking in Smokers
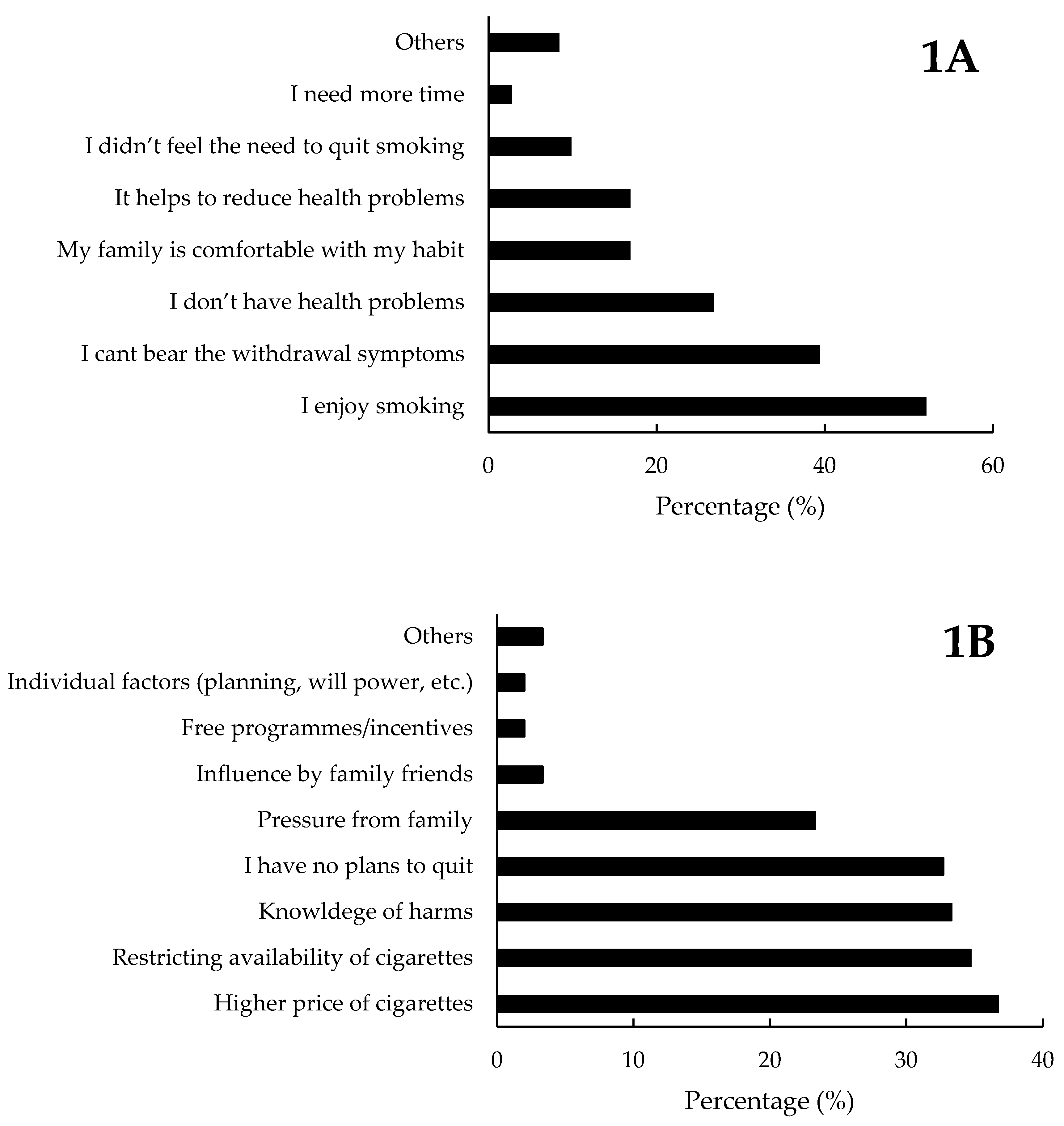
3.5.2. Motivation to Quit Smoking in Current Smokers
3.5.3. Help Seeking for Cessation in Past Smokers
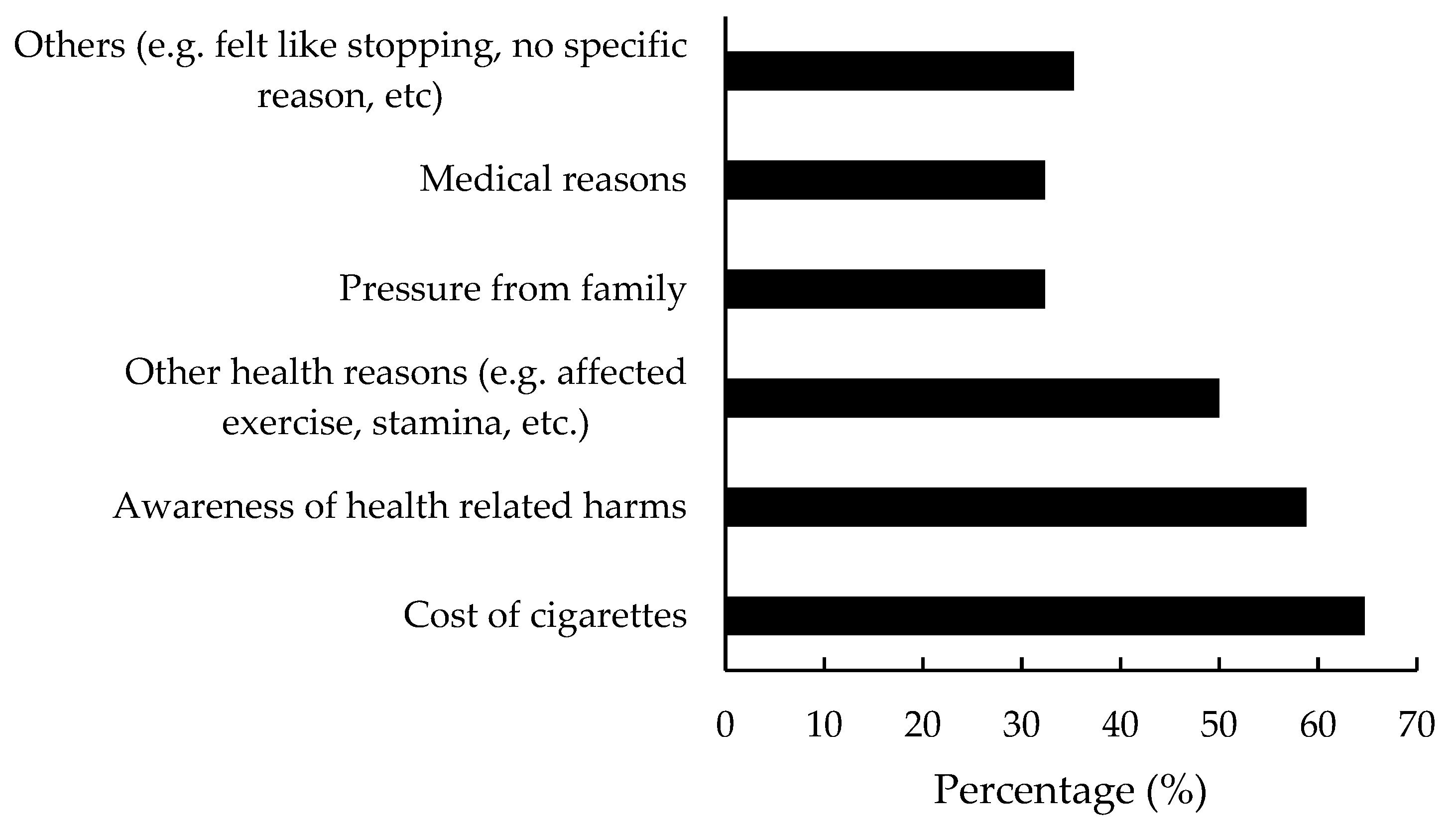
3.5.4. Motivators and Other Factors in Successful Smoking Cessation: Past Smokers
4. Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- World Health Organization (WHO). WHO Launches New Report on Global Tobacco Use Trends. 2019. Available online: https://www.who.int/news-room/detail/19-12-2019-who-launches-new-report-on-global-tobacco-use-trends (accessed on 12 February 2020).
- Banks, E.; Joshy, G.; Weber, M.F.; Liu, B.; Grenfell, R.; Egger, S.; Paige, E.; Lopez, A.D.; Sitas, F.; Beral, V. Tobacco smoking and all-cause mortality in a large Australian cohort study: Findings from a mature epidemic with current low smoking prevalence. BMC Med. 2015, 13, 38. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Shah, S.R.; Cole, J.W. Smoking and stroke: The more you smoke the more you stroke. Expert Rev. Cardiovasc. Ther. 2010, 8, 917–932. [Google Scholar] [CrossRef]
- Jethwa, A.R.; Khariwala, S.S. Tobacco-related carcinogenesis in head and neck cancer. Cancer Metastasis Rev. 2017, 36, 411–423. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization WHO. Framework Convention on Tobacco Control; World Health Organization: Geneva, Switzerland, 2005; Available online: https://www.who.int/fctc/text_download/en/ (accessed on 10 June 2020).
- Zheng, W.; McLerran, D.F.; Rolland, B.A.; Fu, Z.; Boffetta, P.; He, J.; Gupta, P.C.; Ramadas, K.; Tsugane, S.; Irie, F.; et al. Burden of Total and Cause-Specific Mortality Related to Tobacco Smoking among Adults Aged ≥45 Years in Asia: A Pooled Analysis of 21 Cohorts. PLoS Med. 2014, 11, e1001631. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Reitsma, M.B.; Fullman, N.; Ng, M.; Salama, J.S.; Abajobir, A.A.; Abate, K.H.; Abbafati, C.; Abera, S.F.; Abraham, B.; Abyu, G.Y.; et al. Smoking prevalence and attributable disease burden in 195 countries and territories, 1990–2015: A systematic analysis from the Global Burden of Disease Study 2015. Lancet 2017, 389, 1885–1906. [Google Scholar] [CrossRef] [Green Version]
- Katanoda, K.; Jiang, Y.; Park, S.; Lim, M.K.; Qiao, Y.-L.; Inoue, M. Tobacco control challenges in East Asia: Proposals for change in the world’s largest epidemic region. Tob. Control 2014, 23, 359. [Google Scholar] [CrossRef] [PubMed]
- Ministry of Health. National Health Survey. Available online: https://www.moh.gov.sg/content/dam/moh_web/Publications/Reports/2011/NHS2010%20-%20low%20res.pdf (accessed on 12 February 2020).
- National Population Health Survey. 2017. Available online: https://www.moh.gov.sg/docs/librariesprovider5/resources-statistics/reports/executive-summary-nphs-2016_17.pdf (accessed on 12 February 2020).
- Picco, L.; Subramaniam, S.; Abdin, E.; Vaignakar, J.A.; Chong, S.A. Smoking and nicotine dependence in Singapore: Finding from a Cross-Sectional Epidemiology study. Ann. Acad. Med. Singap. 2012, 41, 325–334. [Google Scholar]
- Shahwan, S.; Abdin, E.; Shafie, S.; Chang, S.; Sambasivam, R.; Zhang, Y.; Vaingankar, J.A.; Teo, Y.Y.; Heng, D.; Chong, S.A.; et al. Prevalence and correlates of smoking and nicotine dependence: Results of a nationwide cross-sectional survey among Singapore residents. BMJ Open 2019, 9, e032198. [Google Scholar] [CrossRef] [Green Version]
- National Registry of Disease Office. Publications, Annual Report. Available online: https://www.nrdo.gov.sg/publications (accessed on 9 June 2020).
- Dierker, L.C.; Ramirez, R.R.; Chavez, L.M.; Canino, G. Association between psychiatric disorders and smoking stages among Latino adolescents. Drug Alcohol Depend. 2005, 80, 361–368. [Google Scholar] [CrossRef]
- Wilens, T.; Biederman, J.; Adamson, J.; Henin, A.; Sgambati, S.; Gignac, M.; Sawtelle, R.; Santry, A.; Monuteaux, M.C. Further evidence of an association between adolescent bipolar disorder with smoking and substance use disorders: A controlled study. Drug Alcohol Depend. 2008, 95, 188–198. [Google Scholar] [CrossRef] [Green Version]
- Grant, B.F.; Hasin, D.S.; Chou, S.P.; Stinson, F.S.; Dawson, D.A. Nicotine dependence and psychiatric disorders in the United States: Results from the national epidemiologic survey on alcohol and related conditions. Arch. Gen. Psychiatry 2004, 61, 1107–1115. [Google Scholar] [CrossRef] [PubMed]
- Lasser, K.; Boyd, J.W.; Woolhandler, S.; Himmelstein, D.U.; McCormick, D.; Bor, D.H. Smoking and mental illness: A population-based prevalence study. J. Am. Med. Assoc. 2000, 284, 2606–2610. [Google Scholar] [CrossRef] [PubMed]
- Smith, P.H.; Mazure, C.M.; McKee, S.A. Smoking and mental illness in the US population. Tob. Control 2014, 23, e147–e153. [Google Scholar] [CrossRef] [PubMed]
- Li, X.-H.; An, F.-R.; Ungvari, G.S.; Ng, C.H.; Chiu, H.F.K.; Wu, P.-P.; Jin, X.; Ning, Y. Prevalence of smoking in patients with bipolar disorder, major depressive disorder and schizophrenia and their relationships with quality of life. Sci. Rep. 2017, 7, 8430. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wootton, R.E.; Richmond, R.C.; Stuijfzand, B.G.; Lawn, R.B.; Sallis, H.M.; Taylor, G.M.; Hemani, G.; Jones, H.J.; Zammit, S.; Smith, G.D.; et al. Evidence for causal effects of lifetime smoking on risk for depression and schizophrenia: A Mendelian randomisation study. Psychol. Med. 2019, 1–9. [Google Scholar] [CrossRef] [Green Version]
- Ziedonis, D.; Williams, J.M.; Smelson, D. Serious Mental Illness and Tobacco Addiction: A Model Program to Address This Common but Neglected Issue. Am. J. Med. Sci. 2003, 326, 223–230. [Google Scholar] [CrossRef]
- Winterer, G. Why do patients with schizophrenia smoke? Curr. Opin. Psychiatry 2010, 23, 112–119. [Google Scholar] [CrossRef]
- Kenny, P.J.; File, S.E.; Rattray, M. Acute nicotine decreases, and chronic nicotine increases the expression of brain-derived neuro- trophic factor mRNA in rat hippocampus. Brain Res. Mol. Brain Res. 2000, 85, 234–238. [Google Scholar] [CrossRef]
- Rizos, E.N.; Rontos, I.; Laskos, E.; Arsenis, G.; Michalopoulou, P.G.; Vasilopoulos, D.; Gournellis, R.; Lykouras, L. Investigation of serum BDNF levels in drug-naive patients with schizophre-nia. Prog. Neuropsychopharmacol. Biol. Psychiatry 2008, 32, 1308–1311. [Google Scholar] [CrossRef]
- Xiu, M.H.; Hui, L.; Dang, Y.F.; Hou, T.D.; Zhang, C.X.; Zheng, Y.L.; Chen, D.C.; Kosten, T.R.; Zhang, X.Y. Decreased serum BDNF levels in chronic institutionalized schizophrenia on long-term treatment with typical and atypical antipsychotics. Prog. Neuropsychopharmacol. Biol. Psychiatry 2009, 33, 1508–1512. [Google Scholar] [CrossRef]
- Zhang, X.Y.; Xiu, M.H.; De Yang, F.; Wu, G.Y.; Lu, L.; Kosten, T.A.; Kosten, T.R. Nicotine dependence and serum BDNF levels in male patients with schizophrenia. Psychopharmacology 2010, 212, 301–307. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. Premature Death among People with Severe Mental Disorders. 2017. Available online: https://www.who.int/mental_health/management/info_sheet.pdf (accessed on 13 May 2020).
- Bandiera, F.C.; Anteneh, B.; Le, T.; Delucchi, K.; Guydish, J. Tobacco-related mortality among persons with mental health and substance abuse problems. PLoS ONE 2015, 10, e0120581. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cheng, K.Y.; Chen, S.Y. Avoidable mortality among long-stay patients with schizophrenia under different smoking-restriction settings. Taiwan J. Psychiatry 2019, 33, 160–163. [Google Scholar] [CrossRef]
- McNally, L.; Oyefeso, A.; Annan, J.; Perryman, K.; Bloor, R.; Freeman, S.; Wain, B.; Andrews, H.; Grimmer, M.; Crisp, A.; et al. A survey of staff attitudes to smoking-related policy and intervention in psychiatric and general health care settings. J. Public Health 2006, 28, 192–196. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Taylor, G.; McNeill, A.; Girling, A.; Farley, A.; Lindson-Hawley, N.; Aveyard, P. Change in mental health after smoking cessation: Systematic review and meta-analysis. Bmj 2014, 348, g1151. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Stockings, E.; Bowman, J.; McElwaine, K.; Baker, A.; Terry, M.; Clancy, R.; Bartlem, K.; Wye, P.; Bridge, P.; Knight, J.; et al. Readiness to quit smoking and quit attempts among Australian mental health inpatients. Nicotine Tob. Res. 2013, 15, 942–949. [Google Scholar] [CrossRef] [Green Version]
- World Health Organization. Global Adult Tobacco Survey. 2015. Available online: https://www.who.int/tobacco/publications/surveillance/gatstlas/en/ (accessed on 13 May 2020).
- Centre for Disease Control, National Health Interview Survey. Available online: https://www.cdc.gov/nchs/nhis/tobacco/tobacco_glossary.htm (accessed on 10 June 2020).
- Fagerström, K.; Furberg, H. A comparison of the Fagerström Test for Nicotine Dependence and smoking prevalence across countries. Addiction 2008, 103, 841–845. [Google Scholar] [CrossRef]
- Fagerström, K.O.; Kunze, M.; Schoberberger, R.; Breslau, N.; Hughes, J.R.; Hurt, R.D.; Puska, P.; Ramstrom, L.; Zatonski, W. Nicotine dependence versus smoking prevalence: Comparisons among countries and categories of smokers. Tob. Control 1996, 5, 52–56. [Google Scholar] [CrossRef]
- De Leon, J.; Becoña, E.; Gurpegui, M.; Gonzalez-Pinto, A.; Diaz, F.J. The Association between High Nicotine Dependence and Severe Mental Illness May Be Consistent across Countries. J. Clin. Psychiatry 2002, 63, 812–816. [Google Scholar] [CrossRef]
- Hughes, J.R.; Hatsukami, D.K.; Mitchell, J.E.; Dahlgren, L.A. Prevalence of Smoking among Psychiatric Outpatients. Am. J. Psychiatry 1986, 143, 993–997. [Google Scholar]
- Siru, R.; Hulse, G.K.; Tait, R.J. Assessing Motivation to Quit Smoking in People with Mental Illness: A Review. Addiction 2009, 104, 719–733. [Google Scholar] [CrossRef] [PubMed]
- Caraballo, R.S.; Jamal, A.; Nguyen, K.H.; Kuiper, N.M.; Arrazola, R.A. Electronic Nicotine Delivery System Use among U.S. Adults, 2014. Am. J. Prev. Med. 2016, 50, 226–229. [Google Scholar] [CrossRef] [PubMed]
- Weaver, S.R.; Majeed, B.A.; Pechacek, T.F.; Nyman, A.L.; Gregory, K.R.; Eriksen, M.P. Use of Electronic Nicotine Delivery Systems and Other Tobacco Products among USA Adults, 2014: Results from a National Survey. Int. J. Public Health 2016, 61, 177–188. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Richardson, A.; Pearson, J.; Xiao, H.; Stalgaitis, C.; Vallone, D. Prevalence, Harm Perceptions, and Reasons for Using Noncombustible Tobacco Products among Current and Former Smokers. Am. J. Public Health 2014, 104, 1437–1444. [Google Scholar] [CrossRef]
- See, J.H.J.; Yong, T.H.; Poh, S.L.K.; Lum, Y.C. Smoker motivations and predictors of smoking cessation: Lessons from an inpatient smoking cessation programme. Singap. Med. J. 2019, 60, 583. [Google Scholar] [CrossRef]
- Siqueira, L.; Diab, M.; Bodian, C.; Rolnitzky, L. Adolescents Becoming Smokers: The Roles of Stress and Coping Methods. J. Adolesc. Health 2000, 27, 399–408. [Google Scholar] [CrossRef]
- Baker, T.B.; Piper, M.E.; McCarthy, D.E.; Majeskie, M.R.; Fiore, M.C. Addiction Motivation Reformulated: An Affective Processing Model of Negative Reinforcement. Psychol. Rev. 2004, 111, 33–51. [Google Scholar] [CrossRef] [Green Version]
- Rohde, P.; Lewinsohn, P.M.; Brown, R.A.; Gau, J.M.; Kahler, C.W. Psychiatric Disorders, Familial Factors and Cigarette Smoking: I. Associations with Smoking Initiation. Nicotine Tob. Res. 2003, 5, 85–98. [Google Scholar] [CrossRef]
- Gurpegui, M.; Martínez-Ortega, J.M.; Aguilar, M.C.; Diaz, F.J.; Quintana, H.M.; de Leon, J. Smoking Initiation and Schizophrenia: A Replication Study in a Spanish Sample. Schizophr. Res. 2005, 76, 113–118. [Google Scholar] [CrossRef]
- Schauer, G.L.; Malarcher, A.M.; Berg, C.J. Differences in Smoking and Cessation Characteristics among Adult Nondaily Smokers in the United States: Findings from the 2009–2010 National Adult Tobacco Survey. Nicotine Tob. Res. 2014, 16, 58–68. [Google Scholar] [CrossRef]
- Hu, L.; Sekine, M.; Gaina, A.; Nasermoaddeli, A.; Kagamimori, S. Association of Smoking Behavior and Socio-Demographic Factors, Work, Lifestyle and Mental Health of Japanese Civil Servants. J. Occup. Health 2007, 49, 443–452. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kick, S.D.; Cooley, D.D. Depressive, Not Anxiety, Symptoms Are Associated with Current Cigarette Smoking among University Internal Medical Patients. Psychosomatics 1997, 38, 132–139. [Google Scholar] [CrossRef]
- Escobedo, L.G.; Reddy, M.; Giovino, G.A. The Relationship between Depressive Symptoms and Cigarette Smoking in US Adolescents. Addiction 1998, 93, 433–440. [Google Scholar] [CrossRef] [PubMed]
- Haukkala, A.; Uutela, A.; Vartiainen, E.; McAlister, A.; Knekt, P. Depression and Smoking Cessation: The Role of Motivation and Self-Efficacy. Addict. Behav. 2000, 25, 311–316. [Google Scholar] [CrossRef]
- Hymowitz, N.; Cummings, K.M.; Hyland, A.; Lynn, W.R.; Pechacek, T.F.; Hartwell, T.D. Predictors of Smoking Cessation in a Cohort of Adult Smokers Followed for Five Years. Tob. Control 1997, 6, S57. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ferguson, S.G.; Shiffman, S.; Gitchell, J.G.; Sembower, M.A.; West, R. Unplanned Quit attempts—Results from a U.S. Sample of Smokers and Ex-Smokers. Nicotine Tob. Res. 2009, 11, 827–832. [Google Scholar] [CrossRef]
- Amul, G.G.H.; Pang, T. Progress in tobacco control in Singapore: Lessons and challenges in the implementation of the framework convention on tobacco control. Asia Pac. Policy Stud. 2018, 5, 102–121. [Google Scholar] [CrossRef] [Green Version]
- Low, L.T.; Ng, C.W.; Lee, C. Nicotine dependence treatment: Provision of a dedicated programme by the National Addictions Management Service. Singap. Med. J. 2019, 1–9. [Google Scholar] [CrossRef]
- Ministry of Health. Proposed Tobacco Contro Measures in Singapore-The Standardized Packaging Proposal. Outcome of the 2018 Public Consultation and the Government’s Final Assessment. 2018. Available online: https://www.moh.gov.sg/docs/librariesprovider5/default-document-library/outcome-of-the-2018-public-consultation-and-the-government-s-final-assese3bf46dd03e8495998d07cdf5cde7e9f.pdf (accessed on 16 July 2020).
- Cher, B.P.; Chen, C.; Yoong, J. Prevalence-based, disease-specific estimate of the social cost of smoking in Singapore. BMJ Open 2017, 7, e014377. [Google Scholar] [CrossRef] [Green Version]
- Callaghan, R.C.; Veldhuizen, S.; Jeysingh, T.; Orlan, C.; Graham, C.; Kakouris, G.; Remington, G.; Gatley, J. Patterns of tobacco-related mortality among individuals diagnosed with schizophrenia, bipolar disorder, or depression. J. Psychiatr. Res. 2014, 48, 102–110. [Google Scholar] [CrossRef]
- Prochaska, J.J.; Das, S.; Young-Wolff, K.C. Smoking, mental illness, and public health. Annu. Rev. Public Health 2017, 38, 165–185. [Google Scholar] [CrossRef] [PubMed] [Green Version]



{kind=link}
{kind=link}
| Socio-Demographic Factors | Smokers n (%) n = 150 | Past Smokers n (%) n = 34 | Non-Smokers n (%) n = 196 | Total | p-Value | |
|---|---|---|---|---|---|---|
| Age | 21–40 | 61(40.7) | 18(52.9) | 109 (55.6) | 188 (49.5) | 0.02 |
| 41–65 | 89 (59.3) | 16 (47.1) | 87(44.4) | 192 (50.5) | ||
| Gender | Male | 116 (77.3) | 23 (67.6) | 71(36.2) | 210 (55.3) | <0.001 |
| Female | 34 (22.7) | 11(32.4) | 125 (63.8) | 170 (44.7) | ||
| Ethnicity | Chinese | 92 (61.3) | 25 (73.5) | 162 (82.7) | 279 (73.4) | 0.002 |
| Malay | 32 (21.3) | 5 (14.7) | 18 (9.2) | 55 (14.5) | ||
| Indian | 21(14.0) | 4 (11.8) | 14 (7.1) | 39 (10.3) | ||
| Others | 5 (3.3) | 0 | 2 (1.0) | 7 (1.8) | ||
| Marital status | Married | 21(14.0) | 9 (26.5) | 32 (16.3) | 62 (16.3) | 0.001 |
| Single | 94 (62.7) | 22 (64.7) | 148 (75.5) | 264 (69.5) | ||
| Divorced/separated/widowed | 10 (18.7) | 0 | 14 (8.1) | 54 (13.2) | ||
| Nationality | Singaporean | 146 (97.3) | 32 (94.1) | 190 (96.9) | 368 (96.8) | 0.662 |
| Permanent Resident | 4 (2.7) | 2 (5.9) | 6(3.1) | 12 (3.2) | ||
| Education | Primary or lower | 34 (22.7) | 4 (11.8) | 13 (6.6) | 51(13.4) | <0.001 |
| Secondary | 47(31.3) | 9(26.5) | 46 (23.5) | 102 (26.8) | ||
| Pre-U/diploma | 28 (18.7) | 15 (44.1) | 69 (35.2) | 112 (29.5) | ||
| Vocational/ITE | 26 (17.3) | 2 (5.9) | 25 (12.8) | 53 (14) | ||
| Degree and above | 15 (10.0) | 4 (11.8) | 43 (21.9) | 62 (16.3) | ||
| Employment | Employed | 60 (40.0) | 21(61.8) | 98 (50.0) | 179 (47.1) | 0.064 |
| Unemployed | 78 (52) | 11(32.4) | 77(39.3) | 166 (43.7) | ||
| Economically inactive | 12 (8.0) | 2 (5.9) | 21(10.7) | 35 (10.7) | ||
| Income | Below 2000 | 131(87.3) | 23 (67.6) | 154 (78.6) | 308 (81.1) | 0.02 |
| 2000 to 3999 | 17(11.3) | 7 (20.6) | 30 (15.3) | 54 (14.2) | ||
| 4000 and above | 2 (1.3) | 4 (11.8) | 12 (6.1) | 18 (4.7) | ||
| Children | Yes | 39 (26.2) | 11(32.4) | 34 (17.3) | 84 (22.2) | 0.048 |
| No | 110 (73.8) | 23 (67.6) | 162 (82.7) | 295 (77.8) | ||
| Mean number of household members | 3.25 (±2.1) | 3.32 (±1.12) | 3.26 (±1.31) | 3.26 (±1.64) | 0.973 | |
| Diagnosis | Depressive disorder | 73 (48.7) | 22 (64.7) | 82 (41.8) | 177 (46.6) | 0.038 |
| Schizophrenia spectrum and other psychotic disorder | 77 (51.3) | 12 (35.3) | 114 (58.2) | 203 (53.4) | ||
| Dependence | Smokers n (%) | Past Smokers n (%) |
|---|---|---|
| Low (0–4) | 71(47.7) | 23 (69.7) |
| Moderate (5–7) | 56(37.6) | 8 (24.2) |
| High (8 and above) | 22 (14.8) | 2 (6.1) |
| Overall (5 and above) | 78 (52.3%) | 10 (30.3) |
| Variables | Odds Ratio | CI (95%) | p-Value | |
|---|---|---|---|---|
| Age | 21–40 | Ref. | ||
| 41–65 | 1.6 | 0.8–3.1 | 0.152 | |
| Gender | Male | Ref. | ||
| Female | 0.1 | 0.1–0.2 | 0.000 | |
| Ethnicity | Chinese | Ref. | ||
| Malay | 3.8 | 1.7–8.6 | 0.001 | |
| Indian | 3.0 | 1.2–7.4 | 0.016 | |
| Others | 16.4 | 1.2–233.6 | 0.039 | |
| Marital status | Married | Ref. | ||
| Single | 1.3 | 0.5–3.5 | 0.559 | |
| Divorced/separated/widowed | 2.4 | 0.8–7.4 | 0.134 | |
| Education | Degree and above | Ref. | ||
| Primary or lower | 6.1 | 1.8–21.1 | 0.004 | |
| Secondary | 2.4 | 0.9–6.1 | 0.069 | |
| Pre-U/diploma | 1.1 | 0.5–2.5 | 0.829 | |
| Vocational/ITE | 1.2 | 0.4–3.4 | 0.702 | |
| Employment | Employed | Ref. | ||
| Unemployed | 0.9 | 0.5–1.6 | 0.665 | |
| Economically inactive | 0.6 | 0.2–1.5 | 0.269 | |
| Income | Below 2000 | Ref. | ||
| 2000 to 3999 | 0.7 | 0.3–1.7 | 0.444 | |
| 4000 and above | 1.2 | 0.3-4.7 | 0.766 | |
| Children | No | Ref. | ||
| Yes | 0.7 | 0.2–1.7 | 0.395 | |
| Mean number of household members | 1.0 | 0.9–1.3 | 0.635 | |
| Diagnosis | Depressive disorder | Ref. | ||
| Schizophrenia spectrum and other psychotic disorders | 0.3 | 0.2–0.6 | 0.000 | |
| Risk perception | Yes | Ref. | ||
| No | 7.9 | 2.3–27.9 | 0.001 | |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Asharani, P.V.; Ling Seet, V.A.; Abdin, E.; Siva Kumar, F.D.; Wang, P.; Roystonn, K.; Lee, Y.Y.; Cetty, L.; Teh, W.L.; Verma, S.; et al. Smoking and Mental Illness: Prevalence, Patterns and Correlates of Smoking and Smoking Cessation among Psychiatric Patients. Int. J. Environ. Res. Public Health 2020, 17, 5571. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17155571
Asharani PV, Ling Seet VA, Abdin E, Siva Kumar FD, Wang P, Roystonn K, Lee YY, Cetty L, Teh WL, Verma S, et al. Smoking and Mental Illness: Prevalence, Patterns and Correlates of Smoking and Smoking Cessation among Psychiatric Patients. International Journal of Environmental Research and Public Health. 2020; 17(15):5571. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17155571
Chicago/Turabian StyleAsharani, P. V., Vanessa Ai Ling Seet, Edimansyah Abdin, Fiona Devi Siva Kumar, Peizhi Wang, Kumarasan Roystonn, Ying Ying Lee, Laxman Cetty, Wen Lin Teh, Swapna Verma, and et al. 2020. "Smoking and Mental Illness: Prevalence, Patterns and Correlates of Smoking and Smoking Cessation among Psychiatric Patients" International Journal of Environmental Research and Public Health 17, no. 15: 5571. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17155571