Does Severity of Hair Loss Matter? Factors Associated with Mental Health Outcomes in Women Irradiated for Tinea Capitis in Childhood


Abstract
:1. Introduction
2. Methods
Statistical Analysis
3. Results
3.1. Background Measures
3.2. Mental Health Conditions
3.3. Family and Social Problems
3.4. Predictors of Mental Health Outcomes
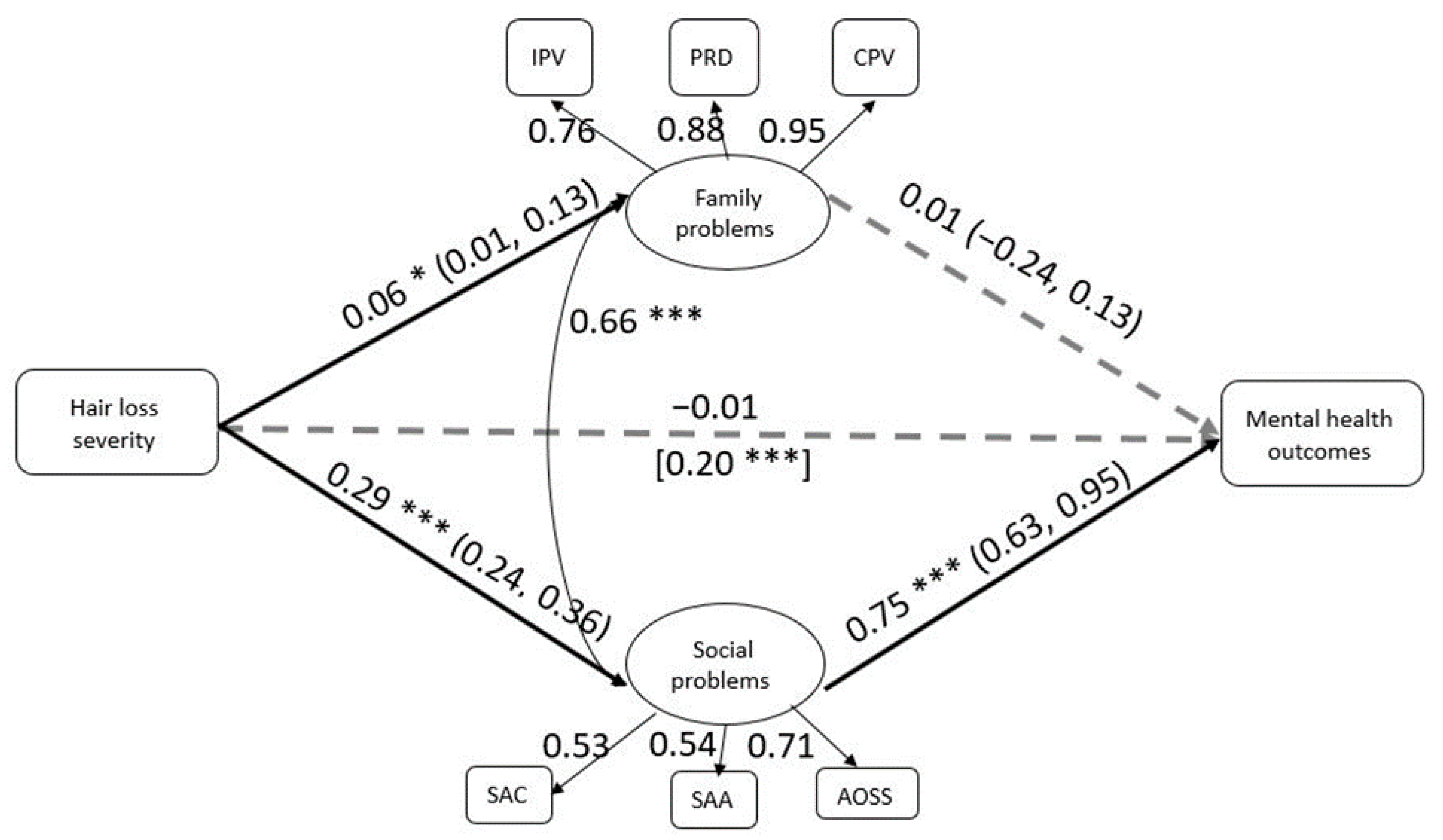
3.5. Test of Mediation
3.6. Physical Health Conditions
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Conflicts of Interest
References
- Lacarrubba, F.; Verzì, A.E.; Micali, G. Newly described features resulting from high-magnification dermoscopy of tinea capitis. JAMA Dermatol. 2015, 151, 308–310. [Google Scholar] [CrossRef] [PubMed]
- Nguyen, C.V.; Collier, S.; Merten, A.H.; Maguiness, S.M.; Hook, K.P. Tinea capitis: A single-institution retrospective review from 2010 to 2015. Pediatr. Dermatol. 2020, 37, 305–310. [Google Scholar] [CrossRef] [PubMed]
- Ali, S.; Graham, T.A.; Forgie, S.E. The assessment and management of tinea capitis in children. Pediatr. Emerg. Care 2007, 23, 662–668. [Google Scholar] [CrossRef] [PubMed]
- Ginter-Hanselmayer, G.; Weger, W.; Ilkit, M.; Smolle, J. Epidemiology of tinea capitis in Europe: Current state and changing patterns. Mycoses 2007, 5, 6–13. [Google Scholar] [CrossRef]
- Hay, R.J. Tinea capitis: Current status. Mycopathologia 2017, 182, 87–93. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Omran, A.R.; Shore, R.E.; Markoff, R.A.; Friedhoff, A.; Albert, R.E.; Barr, H.; Dahlstrom, W.G.; Pasternack, B.S. Follow-up study of patients treated by x-ray epilation for tinea capitis. II. Results of clinical and laboratory examinations. Arch. Environ. Health 1968, 17, 919–934. [Google Scholar] [CrossRef]
- Homei, A.; Worboys, M. Mycoses and Modernity, Science, Technology and Medicine in Modern History. In Fungal Disease in Britain and the United States 1850–2000: Mycoses and Modernity; Springer Nature: London, UK, 2013; pp. 17–42. [Google Scholar]
- Shvarts, S.; Sevo, G.; Tasic, M.; Shani, M.; Sadetzki, S. The tinea capitis campaign in Serbia in the 1950s. Lancet Infect. Dis. 2010, 10, 571–576. [Google Scholar] [CrossRef]
- Boaventura, P.; Bastos, J.; Pereira, D.; Soares, P.; Teixeira-Gomes, J.M. Alopecia in women submitted to childhood X-ray epilation for tinea capitis treatment. Br. J. Dermatol. 2010, 163, 643–644. [Google Scholar] [CrossRef] [PubMed]
- Little, M.P.; Wakeford, R.; Borrego, D.; French, B.; Zablotska, L.B.; Adams, M.J.; Allodji, R.; de Vathaire, F.; Lee, C.; Brenner, A.V.; et al. Leukaemia and myeloid malignancy among people exposed to low doses (<100 mSv) of ionising radiation during childhood: A pooled analysis of nine historical cohort studies. Lancet Haematol. 2018, 5, e346–e358. [Google Scholar] [CrossRef]
- Modan, B.; Alfandary, E.; Shapiro, D.; Lusky, A.; Chetrit, A.; Shewach-Millet, M.; Movshovitz, M. Factors affecting the development of skin cancer after scalp irradiation. Radiat. Res. 1993, 135, 125–128. [Google Scholar] [CrossRef]
- Ron, E.; Lubin, J.H.; Shore, R.E.; Mabuchi, K.; Modan, B.; Pottern, L.M.; Schneider, A.B.; Tucker, M.A.; Boice, J.D., Jr. Thyroid cancer after exposure to external radiation: A pooled analysis of seven studies. Radiat. Res. 1995, 141, 259–277. [Google Scholar] [CrossRef] [PubMed]
- Sadetzki, S.; Chetrit, A.; Freedman, L.; Stovall, M.; Modan, B.; Novikov, I. Long-term follow-up for brain tumor development after childhood exposure to ionizing radiation for tinea capitis. Radiat. Res. 2005, 163, 424–432. [Google Scholar] [CrossRef] [PubMed]
- Shore, R.E.; Albert, R.E.; Pasternack, B.S. Follow-up study of patients treated by X-ray epilation for Tinea capitis; resurvey of post-treatment illness and mortality experience. Arch. Environ. Health 1976, 31, 21–28. [Google Scholar] [CrossRef] [PubMed]
- Omran, A.R.; Shore, R.E.; Markoff, R.A.; Friedhoff, A.; Albert, R.E.; Barr, H.; Dahlstrom, W.G.; Pasternack, B.S. Follow-up study of patients treated by X-ray epilation for tinea capitis: Psychiatric and psychometric evaluation. Am. J. Public Health 1978, 68, 561–567. [Google Scholar] [CrossRef]
- Öberg, P.; Tornstam, L. Body images among men and women of different ages. Ageing Soc. 1999, 19, 629–644. [Google Scholar] [CrossRef] [Green Version]
- Quittkat, H.L.; Hartmann, A.S.; Düsing, R.; Buhlmann, U.; Vocks, S. body dissatisfaction, importance of appearance, and body appreciation in men and women over the lifespan. Front. Psychiatry 2019, 10. [Google Scholar] [CrossRef]
- Fink, B.; Hufschmidt, C.; Hirn, T.; Will, S.; McKelvey, G.; Lankhof, J. Age, health and attractiveness perception of virtual (rendered) human hair. Front. Psychol. 2016, 7, 1893. [Google Scholar] [CrossRef] [Green Version]
- Montgomery, K.; White, C.; Thompson, A. A mixed methods survey of social anxiety, anxiety, depression and wig use in alopecia. BMJ Open 2017, 7. [Google Scholar] [CrossRef]
- Hunt, N.; McHale, S. The psychological impact of alopecia. BMJ 2005, 331, 951–953. [Google Scholar] [CrossRef] [Green Version]
- Dinh, Q.Q.; Sinclair, R. Female pattern hair loss: Current treatment concepts. Clin. Interv. Aging 2007, 2, 189–199. [Google Scholar]
- Bereczkei, T.; Meskó, N. Hair length, facial attractiveness, personality attribution: A multiple fitness model of hairdressing. Rev. Psychol. 2006, 13, 35–42. [Google Scholar]
- Hinsz, V.B.; Matz, D.C.; Patience, R.A. Does women’s hair signal reproductive potential? J. Exp. Soc. Psychol. 2001, 37, 166–172. [Google Scholar] [CrossRef]
- Tallon, B.; Blanchard, E.; Goldberg, L.J. Permanent chemotherapy-induced alopecia: Case report and review of the literature. J. Am. Acad. Dermatol. 2010, 63, 333–336. [Google Scholar] [CrossRef] [PubMed]
- Watanabe, T.; Yagata, H.; Saito, M.; Okada, H.; Yajima, T.; Tamai, N.; Yoshida, Y.; Takayama, T.; Imai, H.; Nozawa, K.; et al. A multicenter survey of temporal changes in chemotherapy-induced hair loss in breast cancer patients. PLoS ONE 2019, 14, e0208118. [Google Scholar] [CrossRef] [PubMed]
- Freites-Martinez, A.; Chan, D.; Sibaud, V.; Shapiro, J.; Fabbrocini, G.; Tosti, A.; Cho, J.; Goldfarb, S.; Modi, S.; Gajria, D.; et al. Assessment of quality of life and treatment outcomes of patients with persistent postchemotherapy alopecia. JAMA Dermatol. 2019, 155, 724–728. [Google Scholar] [CrossRef] [PubMed]
- Kluger, N.; Jacot, W.; Frouin, E.; Rigau, V.; Poujol, S.; Dereure, O.; Guillot, B.; Romieu, G.; Bessis, D. Permanent scalp alopecia related to breast cancer chemotherapy by sequential fluorouracil/epirubicin/cyclophosphamide (FEC) and docetaxel: A prospective study of 20 patients. Ann. Oncol. 2012, 23, 2879–2884. [Google Scholar] [CrossRef]
- Kang, D.; Kim, I.; Choi, E.; Im, Y.H.; Park, Y.H.; Ahn, J.S.; Lee, J.E.; Nam, S.J.; Lee, H.K.; Park, J.; et al. Permanent chemotherapy-induced alopecia in patients with breast cancer: A 3-year prospective cohort study. Oncologist 2019, 24, 414–420. [Google Scholar] [CrossRef] [Green Version]
- Kinahan, K.E.; Sharp, L.K.; Seidel, K.; Leisenring, W.; Didwania, A.; Lacouture, M.E.; Stovall, M.; Haryani, A.; Robison, L.L.; Krull, K.R. Scarring, disfigurement, and quality of life in long-term survivors of childhood cancer: A report from the Childhood Cancer Survivor study. J. Clin. Oncol. 2012, 30, 2466–2474. [Google Scholar] [CrossRef] [Green Version]
- Choi, E.K.; Kim, I.; Chang, O.; Kang, D.; Nam, S.; Lee, J.E.; Lee, S.K.; Im, Y.; Park, Y.H.; Yang, J.; et al. Impact of chemotherapy-induced alopecia distress on body image, psychosocial well-being, and depression in breast cancer patients. Psycho-Oncology 2014, 23, 1103–1110. [Google Scholar] [CrossRef]
- Zannini, L.; Verderame, F.; Cucchiara, G.; Zinna, B.; Alba, A.; Ferrara, M. My wig has been my journey’s companion: Perceived effects of an aesthetic care programme for Italian women suffering from chemotherapy-induced alopecia. Eur. J. Cancer Care 2012, 21, 650–660. [Google Scholar] [CrossRef]
- Freites-Martinez, A.; Shapiro, J.; Chan, D.; Fornier, M.; Modi, S.; Gajria, D.; Dusza, S.; Goldfarb, S.; Lacouture, M.E. Endocrine therapy-induced alopecia in patients with breast cancer. JAMA Dermatol. 2018, 154, 670–675. [Google Scholar] [CrossRef] [PubMed]
- Hoffer, L.; Shvarts, S.; Segal-Engelchin, D. Hair loss due to ringworm irradiation in childhood: Health and psychosocial risks for women. Isr. J. Health Policy Res. 2020, 9, 34. [Google Scholar] [CrossRef] [PubMed]
- Israel Ministry of Health. Law for Compensation of Scalp Ringworm Victims. 1994. Available online: https://www.health.gov.il/LegislationLibrary/Gazezet_01.pdf (accessed on 9 January 2020).
- Muthén, L.K.; Muthén, B.O. Mplus User’s Guide, 8th ed.; Muthén and Muthén: Los Angeles, CA, USA, 1998–2017.
- Israeli National Health Interview Survey (INHIS-1). 2003–2004: Selected Findings. Israel; Center for Disease Control, Ministry of Health: Ramat-Gan, Israel, 2006.
- Israel National Health Interview Survey INHIS-3. 2013–2015: Selected Findings. Israel; Center for Disease Control, Ministry of Health: Ramat-Gan, Israel, 2017.
- Rubin, D.B. Multiple Imputation for Nonresponse in Surveys; John Wiley and Sons: Hoboken, NJ, USA, 2009; p. 307. [Google Scholar]
- Amiel, P.; Dauchy, S.; Bodin, J.; Céline, C.; Franck, Z.; Elisabeth, P.; Anne-Marie, T.; Fabrice, A.; Mario, D. Evaluating beauty care provided by the hospital to women suffering from breast cancer: Qualitative aspects. Support. Care Cancer 2009, 17, 839–845. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lemieux, J.; Maunsell, E.; Provencher, L. Chemotherapy-induced alopecia and effects on quality of life among women with breast cancer: A literature review. Psycho-Oncology 2008, 17, 317–328. [Google Scholar] [CrossRef]
- Luoma, M.L.; Hakamies-Blomqvist, L. The meaning of quality of life in patients being treated for advanced breast cancer: A qualitative study. Psycho-Oncology 2004, 13, 729–739. [Google Scholar] [CrossRef] [PubMed]
- Trüeb, R.M. Minoxidil for endocrine therapy-induced alopecia in women with breast cancer—Saint Agatha’s blessing? JAMA Dermatol. 2018, 154, 656–658. [Google Scholar] [CrossRef]
- Nardi, A.E. Psychological impact of alopecia: Alopecia may lead to social anxiety. BMJ 2005, 331, 1084. [Google Scholar] [CrossRef] [Green Version]
- Hunt, N.; McHale, S. Reported experiences of persons with alopecia areata. J. Loss Trauma. 2005, 10, 33–50. [Google Scholar] [CrossRef]
- Li, S.J.; Huang, K.P.; Joyce, C.; Mostaghimi, A. The impact of alopecia areata on sexual quality of life. Int. J. Trichol. 2018, 10, 271–274. [Google Scholar] [CrossRef]
- Dua, P.; Heiland, M.F.; Kracen, A.C.; Deshields, T.L. Cancer-related hair loss: A selective review of the alopecia research literature. Psycho-Oncology 2017, 26, 438–443. [Google Scholar] [CrossRef]
- Kim, I.; Cho, J.; Choi, E.; Kwon, I.; Sung, Y.; Lee, J.; Nam, S.; Yang, J. Perception, attitudes, preparedness and experience of chemotherapy-induced alopecia among breast cancer patients: A qualitative study. Asian Pac. J. Cancer Prev. 2012, 13, 1383–1388. [Google Scholar] [CrossRef] [PubMed]
- Reid, E.E.; Haley, A.C.; Borovicka, J.H.; Rademaker, A.; West, D.P.; Colavincenzo, M.; Wickless, H. Clinical severity does not reliably predict quality of life in women with alopecia areata, telogen effluvium, or androgenic alopecia. J. Am. Acad. Dermatol. 2012, 66, e97–e102. [Google Scholar] [CrossRef] [PubMed]
- Chren, M.M.; Lasek, R.J.; Sahay, A.P.; Sands, L.P. Measurement properties of Skindex-16: A brief quality-of-life measure for patients with skin diseases. J. Cutan. Med. Surg. 2001, 5, 105–110. [Google Scholar] [CrossRef] [PubMed]
- Schmidt, J.; Martin, A. Appearance teasing and mental health: Gender differences and mediation effects of appearance-based rejection sensitivity and dysmorphic concerns. Front. Psychol. 2019, 10, 579. [Google Scholar] [CrossRef]
- Bottiroli, S.; Galli, F.; Viana, M.; Sances, G.; Tassorelli, C. Traumatic experiences, stressful events, and alexithymia in chronic migraine with medication overuse. Front. Psychol. 2018, 9, 704. [Google Scholar] [CrossRef] [Green Version]
- Tietjen, G.E.; Khubchandani, J.; Herial, N.A.; Shah, K. Adverse childhood experiences are associated with migraine and vascular biomarkers. Headache 2012, 52, 920–929. [Google Scholar] [CrossRef]
- Gregory, K.E.; Radovinsky, L. Research strategies that result in optimal data collection from the patient medical record. Appl. Nurs. Res. 2012, 25, 108–116. [Google Scholar] [CrossRef] [Green Version]
- Thomas, H.; Mitchell, G.; Rich, J.; Best, M. Definition of whole person care in general practice in the English language literature: A systematic review. BMJ Open 2018, 8, e023758. [Google Scholar] [CrossRef]
- Jeannie, L.H.; Marie-Dominique, B.; Raynald, P.; Frederick, B.; Jean-Frédéric, L.; Darcy, A.S.; Fatima, B.; Christine, B. Comprehensiveness of care from the patient perspective: Comparison of primary healthcare evaluation instruments. Healthc. Policy 2011, 7, 154–166. [Google Scholar]


{kind=link}
| Characteristics | %(n) or Mean (SD) | |
|---|---|---|
| Age | 56.79 (±7.43) | |
| Country of birth | Israel | 16.3 (300) |
| Europe | 1.9 (34) | |
| Asia/Africa | 81.4 (1489) | |
| America | 0.4 (7) | |
| Employed | 77.4 (1522) | |
| Family status | Married | 70.3 (1711) |
| Divorced | 12.9 (312) | |
| Widower | 12 (292) | |
| Single | 4.9 (119) | |
| Years of education | 9.05 (±3.39) | |
| Place of radiation | Israel | 55.9 (1386) |
| Radiation age | 0–5 years | 28.3 (711) |
| 6–10 years | 50.6 (1271) | |
| 11–15 years | 21 (527) | |
| High percentage (15%–20%) of disability | 46.4 (1164) | |
| under Article 77 | ||
| Use of wig | 45.2 (1105) | |
| Suicide attempts | 1.1 (27) | |
| Depression | 45.5 (1129) | |
| Emotional distress | 60.1 (1489) | |
| Anxiety | 35.7 (886) | |
| Low self-esteem | 56.6 (1409) | |
| Social anxiety | 22.6 (562) | |
| Suicidal ideation | 5.3 (132) | |
| Psychotherapy | 22.5 (553) | |
| Use of antidepressants | 25.7 (630) | |
| Marital problems | 22.6 (546) | |
| Intimate partner violence | 22.6 (546) | |
| Parent–child relationship difficulties | 6.2 (151) | |
| Child-to-parent violence | 1.3 (31) | |
| Social abuse during childhood | 31.8 (789) | |
| Social abuse during adulthood | 4.7 (117) | |
| Avoidance of social situations | 25.2 (621) | |
| Migraines | 60.4 (1501) | |
| Diabetes | 17.8 (436) | |
| Hypertension | 22.3 (541) | |
| Cancer | 40.8 (1006) |
| Variables | Hair loss | χ2 | RR (95% CI) | |||
|---|---|---|---|---|---|---|
| Low | High | |||||
| % | n | % | n | |||
| Suicide attempts | 1.2 | 16 | 1 | 11 | 0.34 | 0.80 (0.37, 1.71) |
| Depression | 39.9 | 534 | 51.7 | 595 | 34.48 *** | 1.29 (1.19, 1.41) |
| Emotional distress | 52.7 | 702 | 68.5 | 787 | 64.11 *** | 1.30 (1.21, 1.39) |
| Anxiety | 35.6 | 474 | 36 | 412 | 0.06 | 1.01 (0.91, 1.13) |
| Low self-esteem | 47.2 | 633 | 67.5 | 776 | 103.20 *** | 1.43 (1.33, 1.53) |
| Social anxiety | 13.6 | 180 | 33.2 | 382 | 135.59 *** | 2.44 (2.09, 2.87) |
| Suicidal ideation | 4.4 | 59 | 6.3 | 73 | 4.58 * | 1.43 (1.03, 2.01) |
| Psychotherapy | 22.3 | 296 | 22.6 | 257 | 0.04 | 1.01 (0.88, 1.18) |
| Antidepressants/anti-anxiety drugs | 29 | 379 | 22.1 | 251 | 15.32 *** | 0.76 (0.66, 0.87) |
| Variables | Hair loss | χ2 | RR (95% CI) | |||
|---|---|---|---|---|---|---|
| Low | High | |||||
| % | n | % | n | |||
| Marital problems | 20.1 | 264 | 25.3 | 282 | 9.23 * | 1.26 (1.08, 1.45) |
| Intimate partner violence | 20.1 | 264 | 25.3 | 282 | 9.23 * | 1.26 (1.08, 1.45) |
| Parent–child relationship difficulties | 6 | 78 | 6.5 | 73 | 0.29 | 1.08 (0.80, 1.48) |
| Child-to-parent violence | 1.4 | 18 | 1.2 | 13 | 0.26 | 0.89 (0.40, 1.69) |
| Social abuse during childhood | 27.5 | 366 | 36.8 | 423 | 24.70 *** | 1.34 (1.19, 1.50) |
| Social abuse during adulthood | 2.8 | 38 | 6.9 | 79 | 22.58 *** | 2.46 (1.66, 3.54) |
| Avoidance of social situations | 18.7 | 248 | 32.9 | 373 | 65.73 *** | 1.76 (1.53, 2.02) |
| Steps | Predictors | b (95% CI) | β |
|---|---|---|---|
| Step 1 | Age | 0.02 (0.01, 0.03) | 0.10 *** |
| Years of education | 0.003 (−0.02, 0.03) | 0.01 | |
| Family status (1 = married) | −0.33 (−0.51, −0.15) | −0.10 *** | |
| R2 | 2.00% | ||
| Step 2 | Age | 0.03 (0.02, 0.04) | 0.12 *** |
| Years of education | 0.01 (−0.01, 0.03) | 0.02 | |
| Family status (1 = married) | −0.24 (−0.42, −0.07) | −0.07 ** | |
| Intimate partner violence | 1.00 (0.81, 1.20) | 0.27 *** | |
| Parent-child relationship difficulties | 0.67 (0.31, 1.03) | 0.11 *** | |
| Child-to-parent violence | −0.15 (−0.88, 0.58) | −0.01 | |
| ΔR2 | 9.70% | ||
| Step 3 | Age | 0.03 (0.02, 0.04) | 0.12 *** |
| Years of education | 0.01 (−0.01, 0.04) | 0.03 | |
| Family status (1 = married) | −0.20 (−0.35, −0.04) | −0.06 * | |
| Intimate partner violence | 0.61 (0.42, 0.79) | 0.16 *** | |
| Parent-child relationship difficulties | 0.52 (0.19, 0.84) | 0.08 ** | |
| Child-to-parent violence | −0.33 (−0.99, 0.34) | −0.02 | |
| Abuse during childhood | 0.68 (0.52, 0.83) | 0.20 *** | |
| Abuse during adulthood | 0.18 (−0.18, 0.55) | 0.02 | |
| Avoidance of social situations | 1.19 (1.02, 1.35) | 0.33 *** | |
| ΔR2 | 15.90% | ||
| Step 4 | Age | 0.03 (0.02, 0.04) | 0.12 *** |
| Years of education | 0.01 (−0.01, 0.04) | 0.03 | |
| Family status (1 = married) | −0.20 (−0.36, −0.04) | −0.06 *** | |
| Intimate partner violence | 0.61 (0.43, 0.79) | 0.16 *** | |
| Parent-child relationship difficulties | 0.45 (0.13, 0.77) | 0.07 * | |
| Child-to-parent violence | −0.24 (−0.90, 0.42) | −0.02 | |
| Abuse during childhood | 0.64 (0.49, 0.80) | 0.19 *** | |
| Abuse during adulthood | 0.21 (−0.15, 0.57) | 0.03 | |
| Avoidance of social situations | 1.17 (1.00, 1.35) | 0.32 *** | |
| Migraines | 0.25 (0.10, 0.39) | 0.08 ** | |
| Diabetes | 0.03 (−0.17, 0.24) | 0.01 | |
| Hypertension | 0.20 (0.01, 0.39) | 0.05 * | |
| Cancer | 0.16 (0.02, 0.31) | 0.05 * | |
| ΔR2 | 1.20% | ||
| Step 5 | Age | 0.04 (0.03, 0.05) | 0.18 *** |
| Years of education | 0.01 (−0.01, 0.03) | 0.02 | |
| Family status (1 = married) | −0.15 (−0.30, 0.01) | −0.04 | |
| Partner violence | 0.59 (0.41, 0.77) | 0.16 *** | |
| Parent-child relationship difficulties | 0.47 (0.15, 0.79) | 0.07 * | |
| Child-to-parent violence | −0.17 (−0.82, 0.45) | −0.01 | |
| Abuse during childhood | 0.63 (0.48, 0.78) | 0.19 *** | |
| Abuse during adulthood | 0.14 (−0.22, 0.50) | 0.02 | |
| Avoidance of social situations | 1.13 (0.96, 1.29) | 0.31 *** | |
| Migraines | 0.27 (0.13, 0.42) | 0.08 | |
| Diabetes | 0.03 (−0.17, 0.23) | 0.01 | |
| Hypertension | 0.23 (0.04, 0.41) | 0.06 * | |
| Cancer | 0.18 (0.04, 0.32) | 0.06 * | |
| Age at radiation | −0.24 (−0.36, −0.12) | −0.10 *** | |
| Hair loss | 0.42 (0.27, 0.56) | 0.13 *** | |
| ΔR2 | 2.10% | ||
| Overall R2 | cc | ||
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Segal-Engelchin, D.; Shvarts, S. Does Severity of Hair Loss Matter? Factors Associated with Mental Health Outcomes in Women Irradiated for Tinea Capitis in Childhood. Int. J. Environ. Res. Public Health 2020, 17, 7388. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17207388
Segal-Engelchin D, Shvarts S. Does Severity of Hair Loss Matter? Factors Associated with Mental Health Outcomes in Women Irradiated for Tinea Capitis in Childhood. International Journal of Environmental Research and Public Health. 2020; 17(20):7388. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17207388
Chicago/Turabian StyleSegal-Engelchin, Dorit, and Shifra Shvarts. 2020. "Does Severity of Hair Loss Matter? Factors Associated with Mental Health Outcomes in Women Irradiated for Tinea Capitis in Childhood" International Journal of Environmental Research and Public Health 17, no. 20: 7388. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17207388