Analysis of Emergency Department Visits and Hospital Activity during Influenza Season, COVID-19 Epidemic, and Lockdown Periods in View of Managing a Future Disaster Risk: A Multicenter Observational Study

 , , and
, , and
Abstract
:1. Introduction
2. Methods
2.1. Study Design and Setting
2.2. Definitions and Outcomes
2.3. Ethics Statement
2.4. Analysis
3. Results
3.1. Trends in ED Visits and Through-ED Admissions to MSW and ICU
3.2. Impact of Influenza, COVID-19 Epidemic, and Lockdown on ED and through-ED Admissions to MSW and ICU
3.3. Multifaceted Analysis Model: Predictors of Daily ED Visits and through-ED Admissions to MSW and ICU
3.4. Trends on ED Main Characteristics and Diagnosis Groups
4. Discussion
Limitations
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
Appendix A

References
- Sohrabi, C.; Alsafi, Z.; O’Neill, N.; Khan, M.; Kerwan, A.; Al-Jabir, A.; Iosifidis, C.; Agha, R. World Health Organization declares global emergency: A review of the 2019 novel coronavirus (COVID-19). Int. J. Surg. 2020, 76, 71–76. [Google Scholar] [CrossRef]
- World Economic Forum. The Economic, Geopolitical and Health Consequences of COVID-19. 2012. Available online: https://www.weforum.org/agenda/2020/03/the-economic-geopolitical-and-health-consequences-of-covid-19/ (accessed on 24 September 2020).
- Elston, J.W.; Cartwright, C.; Ndumbi, P.; Wright, J. The health impact of the 2014-15 Ebola outbreak. Public Health 2017, 143, 60–70. [Google Scholar] [CrossRef]
- McQuilkin, P.A.; Udhayashankar, K.; Niescierenko, M.; Maranda, L. Health-Care Access during the Ebola Virus Epidemic in Liberia. Am. J. Trop. Med. Hygiene 2017, 97, 931–936. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wilhelm, J.A.; Helleringer, S. Utilization of non-Ebola health care services during Ebola outbreaks: A systematic review and meta-analysis. J. Glob. Health 2019, 9, 010406. [Google Scholar] [CrossRef] [PubMed]
- Vygen, S.; Tiffany, A.; Rull, M.; Ventura, A.; Wolz, A.; Jambai, A.; Porten, K. Changes in Health-Seeking Behavior Did Not Result in Increased All-Cause Mortality During the Ebola Outbreak in Western Area, Sierra Leone. Am. J. Trop. Med. Hyg. 2016, 95, 897–901. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Giamello, J.D.; Abram, S.; Bernardi, S.; Lauria, G. The emergency department in the COVID-19 era. Who are we missing? Eur. J. Emerg. Med. 2020. [Google Scholar] [CrossRef]
- Westgard, B.C.; Morgan, M.W.; Vazquez, G.-B.; Erickson, L.O.; Zwank, M.D. An analysis of changes in emergency department visits after a state declaration during the time of COVID-19. Ann. Emerg. Med. 2020, 76, 595–601. [Google Scholar] [CrossRef]
- Hartnett, K.P.; Kite-Powell, A.; DeVies, J.; Coletta, M.A.; Boehmer, T.K.; Adjemian, J.; Gundlapalli, A.V.; National Syndromic Surveillance Program Community of Practice. Impact of the COVID-19 Pandemic on Emergency Department Visits—United States, January 1, 2019–May 30, 2020. MMWR Morb. Mortal. Wkly. Rep. 2020, 69, 699–704. [Google Scholar] [CrossRef]
- Mantica, G.; Riccardi, N.; Terrone, C.; Gratarola, A. Non-COVID-19 visits to emergency departments during the pandemic: The impact of fear. Public Health 2020, 183, 40–41. [Google Scholar] [CrossRef]
- Lien, W.C.; Wu, J.L.; Tseng, W.P.; Ko, P.C.-I.; Chen, S.Y.; Tsai, M.S.; Chang, W.T.; Huang, C.H.; Chen, S.C. Fight COVID-19 Beyond the Borders: Emergency Department Patient Diversion in Taiwan. Ann. Emerg. Med. 2020, 75, 785–787. [Google Scholar] [CrossRef]
- Hautz, W.E.; Sauter, T.C.; Exadakytlos, A.K.; Krummrey, G.; Schauber, S.; Müller, M. Barriers to seeking emergency care during the COVID-19 pandemic may lead to higher morbidity and mortality—A retrospective study from a Swiss university hospital. Swiss Med. Wkly. 2020, 150, 20331. [Google Scholar] [CrossRef] [PubMed]
- Nuñez, J.H.; Sallent, A.; Lakhani, K.; Guerra-Farfana, E.; Vidala, N.; Ekhtiarid, S.; Minguell, J. Impact of the COVID-19 Pandemic on an Emergency Traumatology Service: Experience at a Tertiary Trauma Centre in Spain. Injury 2020, 51, 1414–1418. [Google Scholar] [CrossRef] [PubMed]
- Madanelo, M.; Ferreira, C.; Nunes, D.-C.; Pinto, A.; Rocha, M.A.; Correia, J.; Teixeira, B.; Mendes, G.; Tavares, C.; Mesquita, S.; et al. The impact of the coronavirus disease 2019 pandemic on the utilisation of emergency urological services. BJU Int. 2020, 126, 256–258. [Google Scholar] [CrossRef] [PubMed]
- Cano, O.-V.; Morales, X.; Ferrigni, C.J.; Martín, E.-A.; Turrado, V.; García, A.; Cuñarro, Y.-L.; Zarain, L.-O.; Duran, M.-P.; Balibrea, J.M.; et al. Reduction in emergency surgery activity during COVID-19 pandemic in three Spanish hospitals. Br. J. Surg. 2020, 107, e239. [Google Scholar] [CrossRef] [PubMed]
- Metzler, B.; Siostrzonek, P.; Binder, R.K.; Bauer, A.; Reinstadler, S.J. Decline of acute coronary syndrome admissions in Austria since the outbreak of COVID-19: The pandemic response causes cardiac collateral damage. Eur. Heart. J. 2020, 41, 1852–1853. [Google Scholar] [CrossRef] [Green Version]
- Santé Publique France. Bulletin épidémiologique grippe. Saison 2019–2020. Paris; Ministère de la Santé. 18 March 2020. Available online: https://www.santepubliquefrance.fr/maladies-et-traumatismes/maladies-a-prevention-vaccinale/grippe/donnees/#tabs (accessed on 24 September 2020).
- Nielsen, J.; Vestergaard, L.S.; Richter, L.; Schmid, D.; Bustos, N.; Asikainen, T.; Trebbien, R.; Denissov, G.; Innos, K.; Virtanen, M.J.; et al. European all-cause excess and influenza-attribuTable mortality in the 2017/18 season: Should the burden of influenza B be reconsidered? Clin. Microbiol. Infect. 2019, 25, 1266–1276. [Google Scholar] [CrossRef] [Green Version]
- Menec, V.H.; Black, C.; MacWilliam, L.; Aoki, F.; Peterson, S.; Friesen, D. The Impact of Influenza-Like Illness on the Winnipeg Health Care System: Is an Early Warning System Possible? Manitoba Centre for Health Policy and Evaluation. March 2001. Available online: http://mchp-appserv.cpe.umanitoba.ca/reference/flu-like.pdf (accessed on 24 September 2020).
- Menec, V.H.; Black, C.; MacWilliam, L.; Aoki, F. The impact of influenza-associated respiratory illnesses on hospitalizations, physician visits, emergency room visits, and mortality. Can. J. Public Health 2003, 94, 59–63. [Google Scholar] [CrossRef]
- Rosano, A.; Bella, A.; Gesualdo, F.; Acampora, A.; Pezzotti, P.; Marchetti, S.; Ricciardi, W.; Rizzo, C. Investigating the impact of influenza on excess mortality in all ages in Italy during recent seasons (2013/14-2016/17 seasons). Int. J. Infect. Dis. 2019, 88, 127–134. [Google Scholar] [CrossRef] [Green Version]
- Jeffery, M.M.; D’Onofrio, G.; Paek, H.; Platts-Mills, T.F.; Soares, W.E.; Hoppe, J.A.; Genes, N.; Nath, B.; Melnick, E.R. Trends in Emergency Department Visits and Hospital Admissions in Health Care Systems in 5 States in the First Months of the COVID-19 Pandemic in the US. JAMA Intern. Med. 2020, 180, 1328–1333. [Google Scholar] [CrossRef]
- Birkmeyer, J.D.; Barnato, A.; Birkmeyer, N.; Bessler, R.; Skinner, J. The Impact of The COVID-19 Pandemic On Hospital Admissions In The United States. Health Aff. 2020, 2020. [Google Scholar] [CrossRef]
- Song, X.; Delaney, M.; Shah, R.K.; Campos, J.M.; Wessel, D.L.; DeBiasi, R.L. Comparison of Clinical Features of COVID-19 vs Seasonal Influenza A and B in US Children. JAMA Netw. Open 2020, 3, e2020495. [Google Scholar] [CrossRef] [PubMed]
- Institut National de la Statistique et des Etudes Economiques (INSEE). The Consequences of the COVID-19 Health Crisis. Economic, Demographic and Societal Impacts (Les Conséquences de la Crise Sanitaire du Covid-19. Impacts Économiques, Démographiques et Sociétaux); Montrouge. 18 May 2020. Available online: https://www.insee.fr/fr/information/4479280 (accessed on 31 August 2020).
- Di Domenico, L.; Pullano, G.; Sabbatini, C.E.; Boëlle, P.Y.; Colizza, V. Impact of lockdown on COVID-19 epidemic in Île-de-France and possible exit strategies. BMC Med. 2020, 18, 240. [Google Scholar] [CrossRef] [PubMed]
- Santé Publique France. Bulletin épidémiologique du Covid-19. Paris; Ministère de la santé, 13 March 2020. Available online: https://www.santepubliquefrance.fr/presse/2020/surveillance-epidemiologique-du-covid-19 (accessed on 24 September 2020).
- Info Coronavirus Covid 19—Carte et Donnees Covid 19 en France; Données au. 27 October 2020. Available online: https://www.gouvernement.fr/info-coronavirus/carte-et-donnees (accessed on 28 October 2020).
- Bouzid, D.; Lucet, J.C.; Duval, X.; Houhou-Fidouh, N.; Casalino, E.; Visseaux, B. ED Influenza Management Study Group. Multiplex PCR implementation as point-of-care testing in a French emergency department. J. Hosp. Infect. 2020, 105. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Visseaux, B.; Le Hingrat, Q.; Collin, G.; Bouzid, D.; Lebourgeois, S.; Le Pluart, D.; Deconinck, L.; Lescure, F.X.; Lucet, J.C.; Bouadma, L.; et al. Evaluation of the QIAstat-Dx Respiratory SARS-CoV-2 Panel, the First Rapid Multiplex PCR Commercial Assay for SARS-CoV-2 Detection. J. Clin. Microbiol. 2020, 58, e00630-20. [Google Scholar] [CrossRef]
- Murray, M.J. The Canadian Triage and Acuity Scale: A Canadian perspective on emergency department triage. Emerg. Med. 2003, 15, 6–10. [Google Scholar] [CrossRef]
- Casalino, E.; Antoniol, S.; Fidouh, N.; Choquet, C.; Lucet, J.-C.; Duval, X.; Visseaux, B.; Pereira, L. Influenza virus infections among patients attending emergency department according to main reason to presenting to ED: A 3-year prospective observational study during seasonal epidemic periods. PLoS ONE 2017, 12, e0182191. [Google Scholar] [CrossRef] [Green Version]
- Wang, J.; Zhu, X.; Xu, Z.; Yang, G.; Mao, G.; Jia, Y.; Xie, Z.; Wang, J.; Ao, W.-Q. Clinical and CT findings of COVID-19: Differences among three age groups. BMC Infect. Dis. 2020, 20, 1–11. [Google Scholar] [CrossRef]
- Box, G.E.P.; Tiao, G.C. Intervention analysis with applications to economic and environmental problems. J. Am. Stat. Assoc. 1975, 70, 70–92. [Google Scholar] [CrossRef]
- Cochrane Effective Practice and Organisation of Care (EPOC). Interrupted Time Series (ITS) Analyses (plus SPSS Time Series Analysis). EPOC Resources for Review Authors, 2017; Norwegian Institute of Public Health: Oslo, Norway, 2017. Available online: https://epoc.cochrane.org/resources/epoc-resources-review-authors (accessed on 24 September 2020).
- Beard, E.; Marsden, J.; Brown, J.; Tombor, I.; Stapleton, J.; Michie, S.; West, R. Understanding and using time series analyzes in addiction research. Addiction 2019, 114, 1866–1884. [Google Scholar] [CrossRef]
- Ramsay, C.R.; Matowe, L.; Grilli, R.; Grimshaw, J.M.; Thomas, R.E. Interrupted time series designs in health technology assessment: Lessons from two systematic reviews of behavior change strategies. Int. J. Technol. Assess. Health Care 2003, 19, 613–623. [Google Scholar] [CrossRef] [Green Version]
- Hiller, K.M.; Stoneking, L.; Min, A.; Rhodes, S.M. Syndromic Surveillance for Influenza in the Emergency Department–A Systematic Review. PLoS ONE 2013, 8, e73832. [Google Scholar] [CrossRef] [PubMed]
- Jaarsma, T.; Cameron, J.; Riegel, B.; Stromberg, A. Factors Related to Self-Care in Heart Failure Patients According to the Middle-Range Theory of Self-Care of Chronic Illness: A Literature Update. Curr. Hear. Fail. Rep. 2017, 14, 71–77. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kilianski, A.; Evans, N.G. Effectively Communicating the Uncertainties Surrounding Ebola Virus Transmission. PLoS Pathog. 2015, 11, e1005097. [Google Scholar] [CrossRef] [Green Version]
- Rosenbaum, L. Communicating Uncertainty—Ebola, Public Health, and the Scientific Process. N. Engl. J. Med. 2015, 372, 7–9. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Carter, P.; Anderson, M.; Mossialos, E. Health system, public health, and economic implications of managing COVID-19 from a cardiovascular perspective. Eur. Hear. J. 2020, 41, 2516–2518. [Google Scholar] [CrossRef] [Green Version]
- Centers for Medicare & Medicaid Services (CMS). Recommendations Re-opening Facilities to Provide Non-emergent Non-COVID-19 Healthcare: Phase I. Baltimore; Department of Health and Human Services (HHS). 19 April 2020. Available online: https://www.cms.gov/files/document/covid-flexibility-reopen-essential-non-covid-services.pdf (accessed on 24 September 2020).
- Geraghty, J. Non-COVID Patients Need Care, Too; National Review. 20 April 2020. Available online: https://www.nationalreview.com/the-morning-jolt/non-covid-patients-need-care-too/ (accessed on 24 September 2020).
- Barnes, M.; Heywood, A.E.; Mahimbo, A.; Rahman, B.; Newall, A.T.; Macintyre, C.R. Acute myocardial infarction and influenza: A meta-analysis of case-control studies. Heart 2015, 101, 1738–1747. [Google Scholar] [CrossRef] [Green Version]
- Skajaa, N.; Horváth-Puhó, E.; Adelborg, K.; Prandoni, P.; Rothman, K.J.; Sørensen, H.T. Venous Thromboembolism in Denmark: Seasonality in Occurrence and Mortality. TH Open 2019, 3, e171–e179. [Google Scholar] [CrossRef] [Green Version]
- Helms, J.; Tacquard, C.; Severac, F.; Leonard-Lorant, I.; Ohana, M.; Delabranche, X.; Merdji, H.; Clere-Jehl, R.; Schenck, M.; Fagot Gandet, F.; et al. High risk of thrombosis in patients with severe SARS-CoV-2 infection: A multicenter prospective cohort study. Intensive Care Med. 2020, 46, 1089–1098. [Google Scholar] [CrossRef]
- Barnes, G.D.; Burnett, A.; Allen, A.; Blumenstein, M.; Clark, N.P.; Cuker, A.; Dager, W.E.; Deitelzweig, S.B.; Ellsworth, S.; Garcia, D.; et al. Thromboembolism and anticoagulant therapy during the COVID-19 pandemic: Interim clinical guidance from the anticoagulation forum. J. Thromb. Thrombolysis 2020, 50, 72–81. [Google Scholar] [CrossRef]
- Moe, J.; Kirkland, S.W.; Rawe, E.; Ospina, M.B.; VanderMeer, B.; Campbell, S.; Rowe, B.H. Effectiveness of Interventions to Decrease Emergency Department Visits by Adult Frequent Users: A Systematic Review. Acad. Emerg. Med. 2017, 24, 40–52. [Google Scholar] [CrossRef] [Green Version]
- Li, Y.; Campbell, H.; Kulkarni, D.; Harpur, A.; Nundy, M.; Wang, X.; Nair, H.; The Usher Network for COVID-19 Evidence Reviews (UNCOVER) group. The temporal association of introducing and lifting non-pharmaceutical interventions with the time-varying reproduction number (R) of SARS-CoV-2: A modelling study across 131 countries. Lancet Infect. Dis. 2020. [Google Scholar] [CrossRef]
- Davies, N.G.; Kucharski, A.J.; Eggo, R.M.; Gimma, A.; Edmunds, W.J.; Jombart, T.; O’Reilly, K.; Endo, A.; Hellewell, J.; Nightingale, E.S.; et al. Effects of non-pharmaceutical interventions on COVID-19 cases, deaths, and demand for hospital services in the UK: A modelling study. Lancet Public Health 2020, 5, e375–e385. [Google Scholar] [CrossRef]
- Maringe, C.; Spicer, J.; Morris, M.; Purushotham, A.; Nolte, E.; Sullivan, R.; Rachet, B.; Aggarwal, A. The impact of the COVID-19 pandemic on cancer deaths due to delays in diagnosis in England, UK: A national, population-based, modelling study. Lancet Oncol. 2020, 21, 1023–1034. [Google Scholar] [CrossRef]

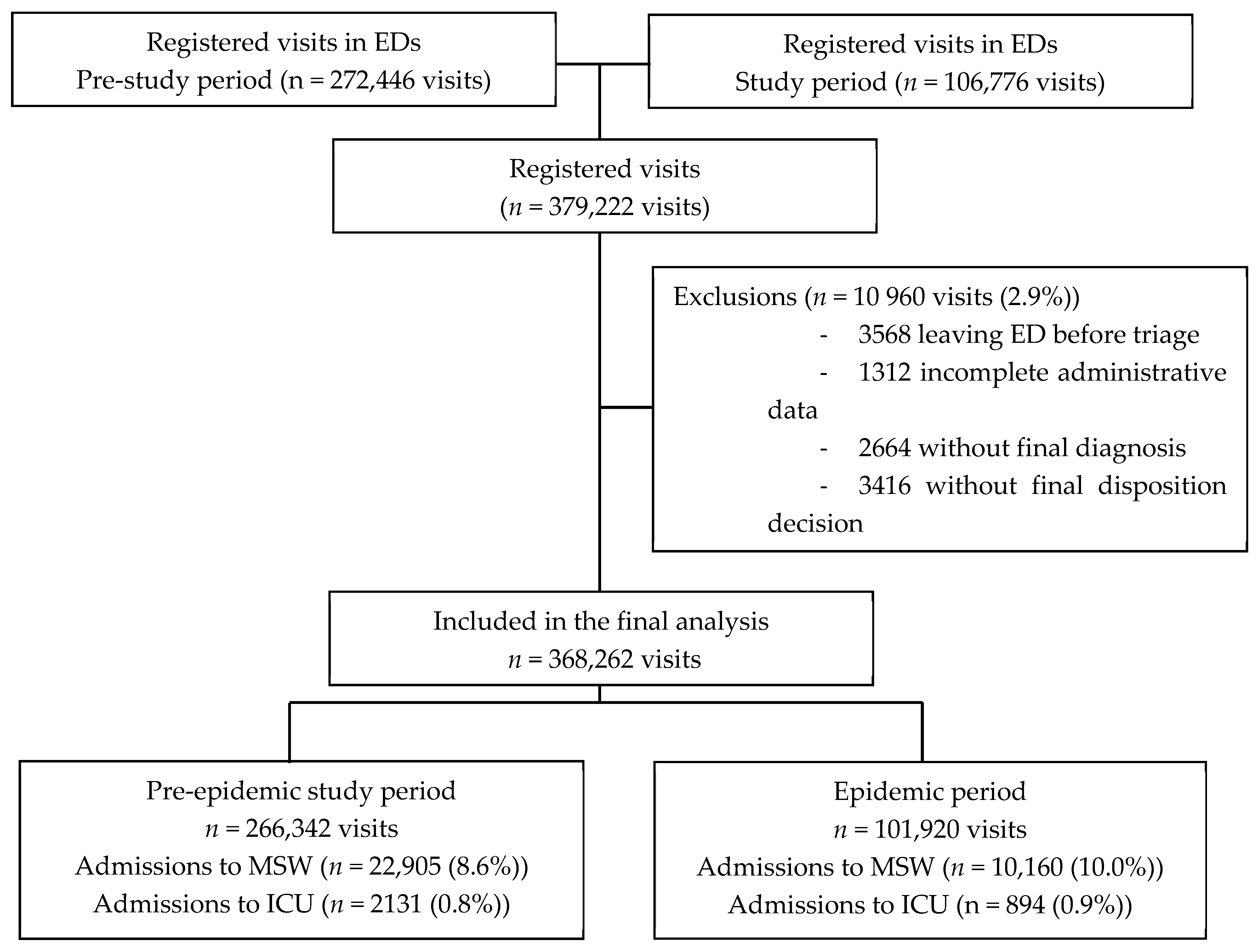
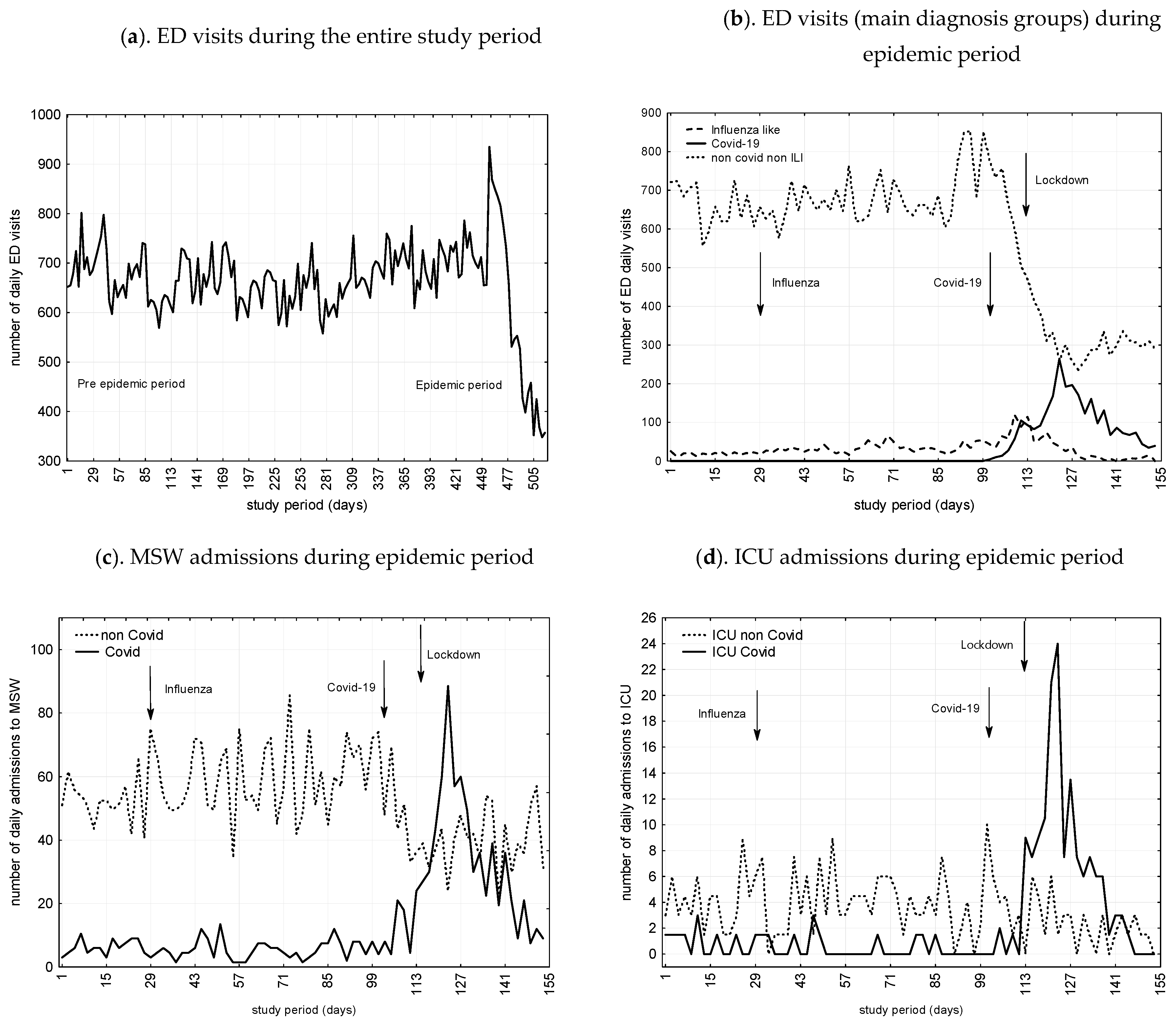
 Infuenza like related cases;
Infuenza like related cases;  non-COVID related cases;
non-COVID related cases;  COVID-19 related cases; ED, emergency department; ICU, intensive care unit; MSW, medical/surgical wards.
Infuenza like related cases; non-COVID related cases; COVID-19 related cases; ED, emergency department; ICU, intensive care unit; MSW, medical/surgical wards.
COVID-19 related cases; ED, emergency department; ICU, intensive care unit; MSW, medical/surgical wards.
Infuenza like related cases; non-COVID related cases; COVID-19 related cases; ED, emergency department; ICU, intensive care unit; MSW, medical/surgical wards.

{kind=link}
{kind=link}
| Variables- | Parameter | SE | t (150) | p | CI 95% | |
|---|---|---|---|---|---|---|
| Daily visits to ED | ||||||
| Influenza epidemic period | ||||||
| Omega | 160.8 | 51.7 | 3.1 | 0.002 | 58.5 | 263.0 |
| Delta | 0.98 | 0.006 | 176.4 | <0.001 | 0.97 | 0.99 |
| COVID-19 epidemic period | ||||||
| Omega | 124.7 | 110.8 | 1.1 | 0.3 | −94.3 | 343.7 |
| Delta | 0.6 | 0.3 | 1.9 | 0.06 | −0.03 | 1.3 |
| Lockdown period | ||||||
| Omega | −160.2 | 23.8 | −6.7 | <0.001 | <0.001 | −113.1 |
| Delta | 1.0 | 0.005 | 210.6 | <0.001 | 1.01 | 1.03 |
| Daily through ED admissions to MSW | ||||||
| Influenza epidemic period | ||||||
| Omega | 6.2 | 5.4 | 1.1 | 0.2 | −4.4 | 16.8 |
| Delta | 1.0 | 0.006 | 177.6 | <0.001 | 0.99 | 1.02 |
| COVID-19 epidemic period | ||||||
| Omega | −31.7 | 15.4 | −2.1 | 0.04 | 1.2 | 62.2 |
| Delta | 0.5 | 0.3 | 2.0 | 0.05 | −1.1 | −0.007 |
| Lockdown period | ||||||
| Omega | −14.6 | 7.6 | 1.9 | 0.05 | −0.4 | 29.6 |
| Delta | 1.0 | 0.02 | 48.2 | <0.001 | 0.9 | 1.0 |
| Daily through ED admissions to ICU | ||||||
| Influenza epidemic period | ||||||
| Omega | 0.7 | 0.8 | 0.9 | 0.4 | −0.8 | 2.1 |
| Delta | −1.0 | 0.02 | −39.7 | <0.001 | −1.0 | −0.9 |
| COVID-19 epidemic period | ||||||
| Omega | 13.9 | 2.1 | 1.8 | 0.05 | −0.3 | 8.1 |
| Delta | 0.8 | 0.1 | −7.5 | <0.001 | −1.0 | −0.6 |
| Lockdown period | ||||||
| Omega | −13.2 | 2.3 | 5.3 | <0.001 | 8.78 | 17.7 |
| Delta | 0.9 | 0.01 | 79.52 | <0.001 | 0.9 | 1.0 |
| Beta | SE of Beta | CI 95% | F | P | Adjusted R2 | |
|---|---|---|---|---|---|---|
| ED daily visits number | ||||||
| Number of patients aged <65 years | 0.2 | 0.02 | 0.09–0.2 | 28.9 | <0.001 | 0.6 |
| Lockdown period | 0.3 | 0.1 | 0.1–1.0 | 130.1 | <0.001 | 0.6 |
| Number of triage level 4/5 | 0.2 | 0.05 | 0.1–0.3 | 26.2 | <0.001 | 0.8 |
| Number of arrival mode by own resources | 0.6 | 0.05 | 0.5–0.7 | 179.5 | <0.001 | 0.9 |
| Trough ED daily admitted patients to MSW | ||||||
| Number of COVID proved cases | 0.9 | 0.1 | 0.7–1.1 | 76.9 | <0.001 | 0.3 |
| Number of triage level 1 to 3 | 0.5 | 0.07 | 0.4–0.7 | 51.5 | <0.001 | 0.4 |
| Number of ILI/COVID suspected cases | −0.7 | 0.1 | −0.9–−0.5 | 51.7 | <0.001 | 0.5 |
| Trough ED daily admitted patients to ICU | ||||||
| Number of triage level 1 to 3 | 0.3 | 0.07 | 0.1–0.4 | 14.3 | <0.001 | 0.3 |
| Number of admitted cases to MSW | 0.2 | 0.07 | 0.05–0.3 | 6.8 | 0.01 | 0.4 |
| Number of COVID proved cases | 0.4 | 0.07 | 0.2–0.5 | 26.2 | <0.001 | 0.4 |
| Variables- | Influenza Epidemic Period | COVID-19 Epidemic Period | Lockdown Period | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Trend (%) | CI 95% | p | Trend (%) | CI95% | p | Trend (%) | CI 95% | p | ||||
| ED and hospital activities | ||||||||||||
| ED visits | 10.6 | 7.3 | 13.9 | 0.01 | −36.9 | −43.0 | −30.7 | <0.001 | −49.6 | −55.7 | −43.4 | <0.001 |
| Admission to MSW | 12.8 | 9.2 | 16.4 | 0.003 | 33.9 | 28.1 | 39.7 | <0.001 | −16.8 | −21.2 | −11.4 | 0.001 |
| non-COVID ED admissions to MSW | - | - | - | - | −29.9 | −22.1 | −36.3 | <0.001 | −24.2 | −29.3 | 19.5 | <0.001 |
| COVID admissions to MSW | - | - | - | - | 366.0 | 248.0 | 435.0 | <0.001 | −68.0 | −79.6 | −52.1 | <0.001 |
| Admissions to ICU | 4.6 | 2.5 | 6.7 | 0.05 | 277.0 | 260.4 | 293.6 | <0.001 | −15.5 | −18.2 | 11.8 | −0.02 |
| non-COVID ED admissions to ICU | - | - | - | - | −71.1 | −76.3 | −64.9 | <0.001 | −13.8 | −18.2 | 8.4 | 0.03 |
| COVID admissions to ICU | - | - | - | - | 406.0 | 377.0 | 486.0 | <0.001 | −22.4 | −26.3 | −18.7 | 0.001 |
| ED visits number as a function of main case characteristics | ||||||||||||
| Age <65 years | 7.6 | 4.8 | 10.4 | 0.008 | −18.3 | −22.5 | −14.1 | 0.001 | −68.3 | −75.9 | −60.5 | <0.001 |
| Male | 8.8 | 5.8 | 11.8 | 0.001 | 9.2 | 6.2 | 12.2 | 0.03 | −62.6 | −70.3 | −54.3 | <0.001 |
| Frequent users | 128.5 | 117.2 | 139.8 | <0.001 | 221 | 206.1 | 235.9 | <0.001 | 188.9 | 174.3 | 201.7 | <0.001 |
| Arrival mode Own resources | 22.6 | 17.8 | 27.4 | <0.001 | −28.4 | 23.1 | 33.7 | <0.001 | −52.6 | −59.7 | −44.8 | <0.001 |
| Arrival mode Ambulance | 5.9 | 3.5 | 8.3 | 0.005 | 52.6 | 45.3 | 59.9 | <0.001 | 16.6 | 12.5 | 20.7 | 0.001 |
| Triages 1 to 3 | 16.7 | 12.6 | 20.8 | 0.05 | 74.4 | 65.8 | 83.0 | <0.001 | −21.6 | −26.4 | −16.8 | 0.001 |
| Triages 4 and 5 | 17.4 | 13.2 | 21.6 | <0.001 | 5.2 | 2.9 | 7.5 | 0.09 | −63.1 | −71.0 | −55.1 | <0.001 |
| Main Diagnosis- | Influenza Epidemic Period | COVID-19 Epidemic Period | Lockdown Period | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Trend (%) | CI 95% | p | Trend (%) | CI 95% | p | Trend (%) | CI 95% | p | ||||
| ILI | 161.0 | 148.3 | 173.7 | <0.001 | 225.0 | 210.0 | 240.0 | <0.001 | −42.1 | −48.1 | −36.0 | <0.001 |
| ILI plus COVID-19 suspected cases | 244.0 | 228.4 | 259.6 | <0.001 | 865.0 | 835.6 | 894.4 | <0.001 | 31.6 | 26.0 | 37.2 | <0.001 |
| COVID-19 proved cases | 125.0 | 97.0 | 199.0 | <0.001 | 388.0 | 296.0 | 477.0 | <0.001 | −69.0 | 33.0 | 109.0 | <0.001 |
| Acute coronary syndrome | 13.7 | 10.0 | 17.4 | 0.007 | −1.1 | −2.0 | 0.1 | 1 | −51.2 | −52.1 | −50.0 | <0.001 |
| Atrial fibrillation | −26.8 | −32.1 | −21.1 | 0.01 | −34.2 | −39.5 | −28.5 | 0.001 | −71.3 | −76.6 | −65.6 | <0.001 |
| Thoracic pain | 8.4 | 5.5 | 11.3 | 0.05 | −19.2 | −23.7 | −14.7 | 0.02 | −40.8 | −45.3 | −36.3 | <0.001 |
| Pulmonary embolism/deep vein thrombosis | 31.1 | 25.5 | 36.7 | 0.001 | 42.4 | 35.9 | 44.8 | <0.001 | 33.5 | 27.7 | 35.9 | <0.001 |
| Stroke | 1.9 | 0.5 | 3.3 | 0.6 | −5.8 | −8.2 | −3.4 | 0.09 | −57.1 | −64.6 | −49.4 | <0.001 |
| Seizures | 3.8 | 1.9 | 5.7 | 0.2 | 1.1 | 0.1 | 2.1 | 0.7 | −48.1 | −55.0 | −41.2 | <0.001 |
| Diabetes | 4.2 | 2.3 | 6.8 | 0.3 | 2.1 | 1.7 | 2.8 | 0.6 | −47.2 | −53.8 | −42.1 | 0.001 |
| Hip fracture | 5.1 | 2.8 | 7.4 | 0.1 | 1.9 | 0.5 | 3.3 | 0.6 | −44.6 | −51.2 | −38.0 | <0.001 |
| Hand wound | 6.9 | 4.3 | 9.5 | 0.1 | −1.9 | −3.4 | −0.5 | 0.3 | −51.3 | −52.8 | −49.9 | 0.001 |
| Head trauma | -0.8 | −1.7 | 0.5 | 0.9 | −6.6 | −7.5 | −5.3 | 0.06 | −59.7 | −67.4 | −52.1 | <0.001 |
| Headaches | 14.8 | 11.0 | 18.6 | 0.01 | 5.9 | 3.5 | 8.3 | 0.04 | −42.9 | −49.2 | −36.4 | <0.001 |
| Abdominal pain | 3.4 | 1.6 | 5.2 | 0.6 | 2.6 | 1.0 | 4.2 | 0.09 | −52.2 | −59.5 | −45.0 | <0.001 |
| Renal colic | 12.8 | 9.2 | 16.4 | 0.05 | −3.9 | −5.9 | −1.9 | 0.2 | −54.3 | −56.3 | −52.3 | <0.001 |
| Low back pain | −11.6 | −15.1 | −8.2 | 0.04 | −22.4 | −25.9 | −19.0 | 0.001 | −73.6 | −81.7 | −65.3 | <0.001 |
| Appendicitis | 14.6 | 10.8 | 18.4 | 0.05 | 1.9 | 0.5 | 3.3 | 0.6 | −57.4 | −64.5 | −49.6 | <0.001 |
| Urinary tract infection | −18.4 | −22.8 | −14.2 | 0.01 | −31.3 | −36.9 | −25.7 | <0.001 | −62.5 | −68.1 | −56.9 | <0.001 |
| Alcoholic intoxication | −7.9 | −10.7 | −5.1 | 0.07 | −24.8 | −27.6 | −19.8 | <0.001 | −73.4 | −81.6 | −65.0 | <0.001 |
| Psychiatric disorders | 7.8 | 5.0 | 10.6 | 0.07 | −8.4 | −11.3 | −5.5 | 0.005 | −23.8 | −28.5 | −18.9 | <0.001 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Casalino, E.; Choquet, C.; Bouzid, D.; Peyrony, O.; Curac, S.; Revue, E.; Fontaine, J.-P.; Plaisance, P.; Chauvin, A.; Ghazali, D.A. Analysis of Emergency Department Visits and Hospital Activity during Influenza Season, COVID-19 Epidemic, and Lockdown Periods in View of Managing a Future Disaster Risk: A Multicenter Observational Study. Int. J. Environ. Res. Public Health 2020, 17, 8302. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17228302
Casalino E, Choquet C, Bouzid D, Peyrony O, Curac S, Revue E, Fontaine J-P, Plaisance P, Chauvin A, Ghazali DA. Analysis of Emergency Department Visits and Hospital Activity during Influenza Season, COVID-19 Epidemic, and Lockdown Periods in View of Managing a Future Disaster Risk: A Multicenter Observational Study. International Journal of Environmental Research and Public Health. 2020; 17(22):8302. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17228302
Chicago/Turabian StyleCasalino, Enrique, Christophe Choquet, Donia Bouzid, Olivier Peyrony, Sonja Curac, Eric Revue, Jean-Paul Fontaine, Patrick Plaisance, Anthony Chauvin, and Daniel Aiham Ghazali. 2020. "Analysis of Emergency Department Visits and Hospital Activity during Influenza Season, COVID-19 Epidemic, and Lockdown Periods in View of Managing a Future Disaster Risk: A Multicenter Observational Study" International Journal of Environmental Research and Public Health 17, no. 22: 8302. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17228302