
The Role of Human Behavior in Plasmodium knowlesi Malaria Infection: A Systematic Review

 , , , , and
, , , , and
Abstract
:1. Introduction
Strengths and Limitations of This Study
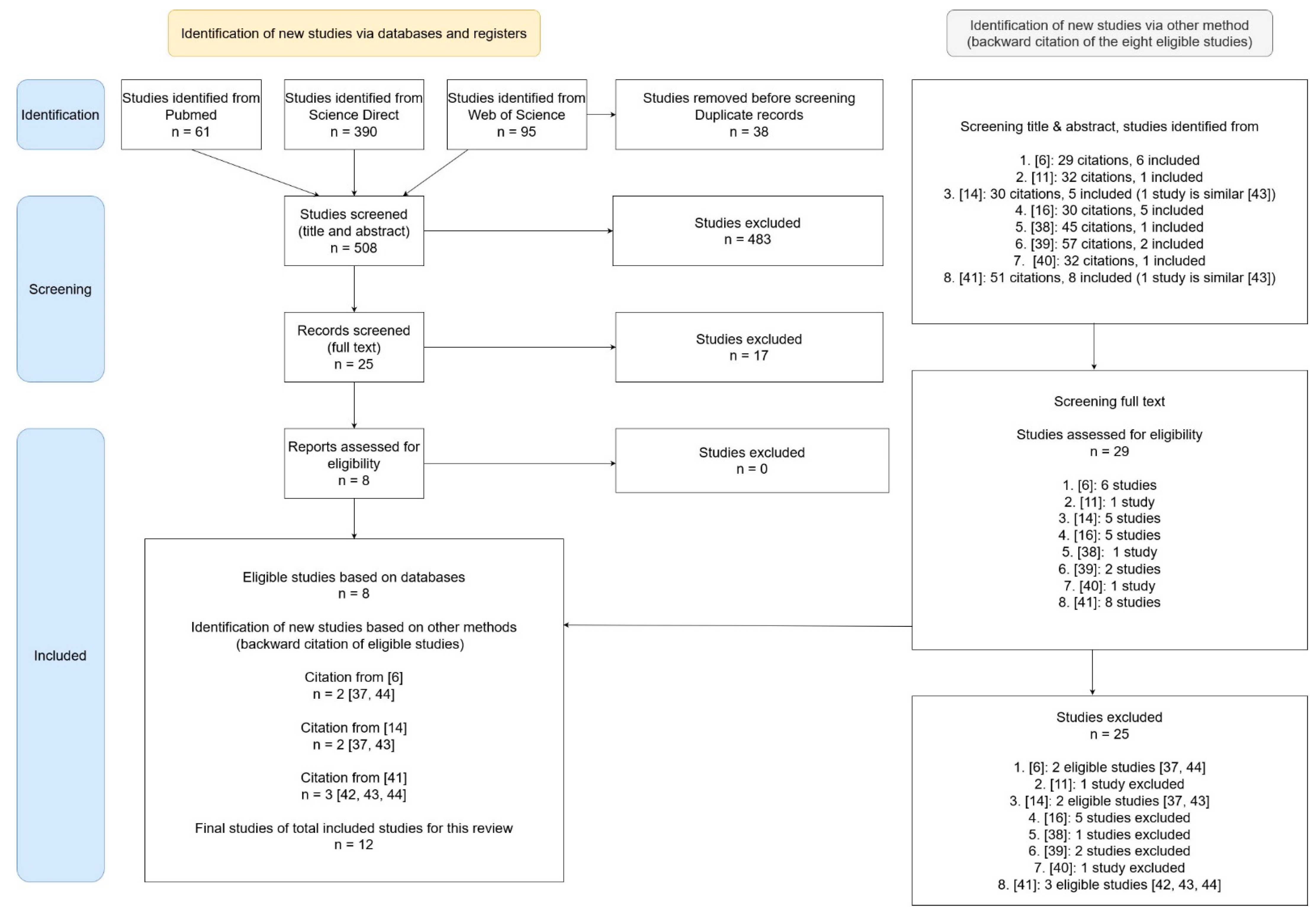
2. Methods
Data Extraction, Quality Assessment, Risk of Bias, Data Synthesis, and Data Checking
3. Results
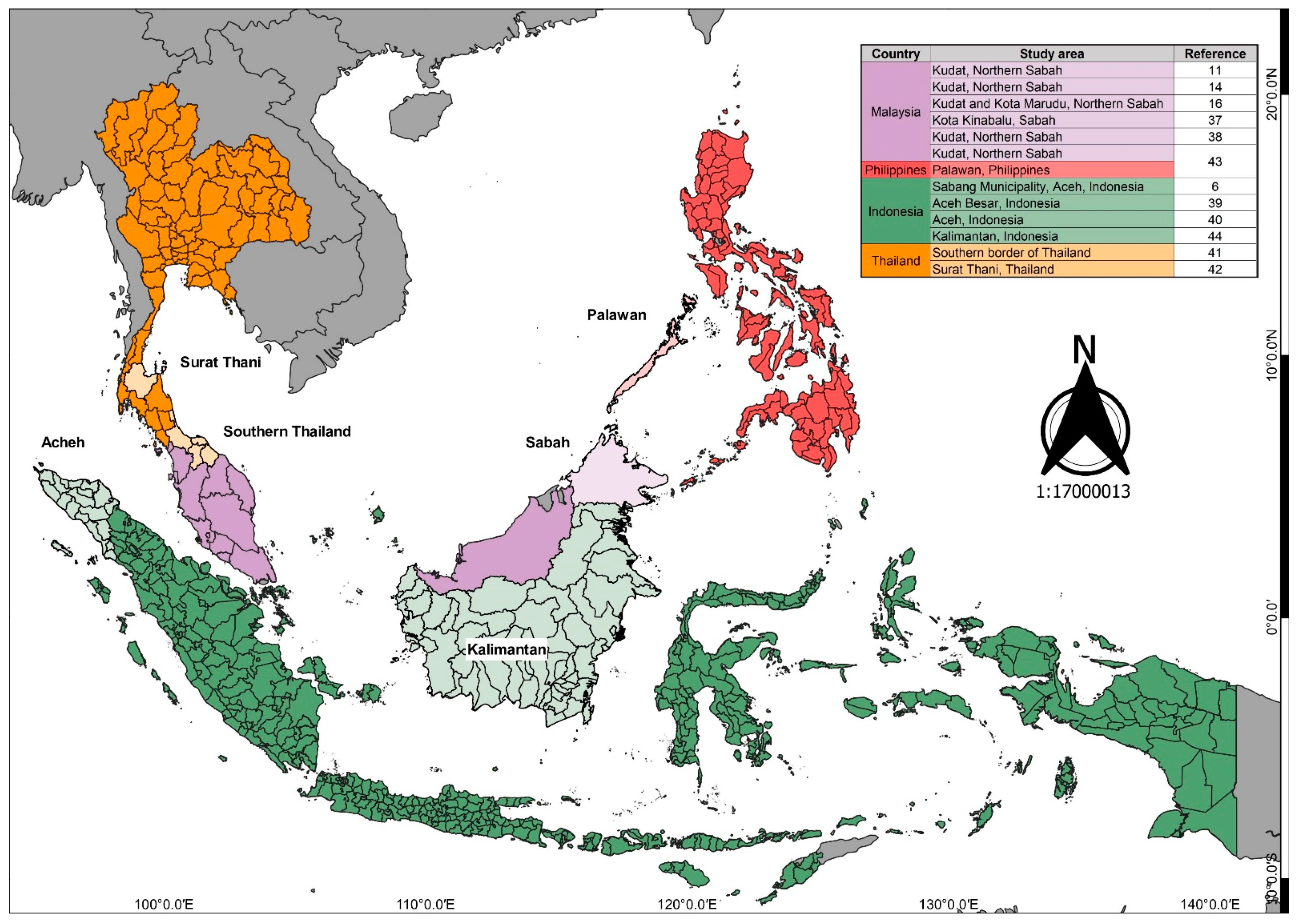
3.1. Description of Studies
3.2. Examination of Human Behavior in the Selected Studies
3.3. Perceived Threats, Beliefs, and Misconceptions about P. knowlesi Malaria
3.4. Significance of Behavior and Activities to P. knowlesi Malaria Exposure
3.5. Demographic Factors
3.5.1. Gender
3.5.2. Age
3.5.3. Place of Stay
3.6. Factors Related to Outdoor Activities
3.7. Other Related Themes
4. Discussion
Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Singh, B.; Daneshvar, C. Human Infections and Detection of Plasmodium knowlesi. Clin. Microbiol. Rev. 2013, 26, 165–184. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Abeyasinghe, R. Outcomes from the Evidence Review Group on Plasmodium knowlesi. 2017. Available online: https://www.who.int/malaria/mpac/mpac-mar2017-plasmodium-knowlesi-presentation.pdf (accessed on 30 November 2020).
- World Health Organization. WHO Malaria Policy Advisory Group (MPAG) Meeting. 2021. Available online: https://www.who.int/news-room/events/detail/2021/04/13/default-calendar/19th-meeting-of-the-malaria-policy-advisory-group (accessed on 30 April 2021).
- World Health organization. World Malaria Report: 20 Year of Global Progress and Challenges; World Health Organization: Geneva, Switzerland, 2020. [Google Scholar]
- Lubis, I.N.D.; Wijaya, H.; Lubis, M.; Lubis, C.P.; Divis, P.C.S.; Beshir, K.; Sutherland, C.J. Contribution of Plasmodium knowlesi to Multispecies Human Malaria Infections in North Sumatera, Indonesia. J. Infect. Dis. 2017, 215, 1148–1155. [Google Scholar] [CrossRef] [PubMed]
- Herdiana, H.; Irnawati, I.; Coutrier, F.N.; Munthe, A.; Mardiati, M.; Yuniarti, T.; Sariwati, E.; Sumiwi, M.E.; Noviyanti, R.; Pronyk, P.; et al. Two clusters of Plasmodium knowlesi cases in a malaria elimination area, Sabang Municipality, Aceh, Indonesia. Malar. J. 2018, 17, 186. [Google Scholar] [CrossRef] [PubMed]
- Eede, P.V.D.; Van, H.N.; Van Overmeir, C.; Vythilingam, I.; Duc, T.N.; Hung, L.X.; Manh, H.N.; Annette, E.; D’Alessandro, U.; Erhart, A. Human Plasmodium knowlesi infections in young children in central Vietnam. Malar. J. 2009, 8, 249. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Marchand, R.P.; Culleton, R.; Maeno, Y.; Quang, N.T.; Nakazawa, S. Co-infections of Plasmodium knowlesi, P. falciparum, and P. vivax among humans and Anopheles dirus mosquitoes, Southern Vietnam. Emerg. Infect. Dis. 2011, 17, 1232–1239. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Imwong, M.; Madmanee, W.; Suwannasin, K.; Kunasol, C.; Peto, T.; Tripura, R.; Von Seidlein, L.; Nguon, C.; Davoeung, C.; Day, N.P.J.; et al. Asymptomatic Natural Human Infections With the Simian Malaria Parasites Plasmodium cynomolgi and Plasmodium knowlesi. J. Infect. Dis. 2019, 219, 695–702. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Vythilingam, I.; Chua, T.H.; Liew, J.W.K.; Manin, B.O.; Ferguson, H.M. The vectors of Plasmodium knowlesi and other simian malarias Southeast Asia: Challenges in malaria elimination. Adv. Parasitol. 2021, 113, 131–189. [Google Scholar] [CrossRef] [PubMed]
- Manin, B.O.; Ferguson, H.; Vythilingam, I.; Fornace, K.; William, T.; Torr, S.; Drakeley, C.; Chua, T.H. Investigating the Contribution of Peri-domestic Transmission to Risk of Zoonotic Malaria Infection in Humans. PLoS Negl. Trop. Dis. 2016, 10, e0005064. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chua, T.H.; Manin, B.O.; Vythilingam, I.; Fornace, K.; Drakeley, C.J. Effect of different habitat types on abundance and biting times of Anopheles balabacensis Baisas (Diptera: Culicidae) in Kudat district of Sabah, Malaysia. Parasites Vectors 2019, 12, 364. [Google Scholar] [CrossRef]
- De Ang, J.X.; Yaman, K.; Kadir, K.A.; Matusop, A.; Singh, B. New vectors that are early feeders for Plasmodium knowlesi and other simian malaria parasites in Sarawak, Malaysian Borneo. Sci. Rep. 2021, 11, 7739. [Google Scholar] [CrossRef]
- Fornace, K.M.; Brock, P.M.; Abidin, T.R.; Grignard, L.; Herman, L.S.; Chua, T.H.; Daim, S.; William, T.; Patterson, C.L.; Hall, T.; et al. Environmental risk factors and exposure to the zoonotic malaria parasite Plasmodium knowlesi across northern Sabah, Malaysia: A population-based cross-sectional survey. Lancet Planet. Health 2019, 3, e179–e186. [Google Scholar] [CrossRef] [Green Version]
- Fornace, K.M.; Abidin, T.R.; Alexander, N.; Brock, P.; Grigg, M.J.; Murphy, A.; William, T.; Menon, J.; Drakeley, C.J.; Cox, J. Association between Landscape Factors and Spatial Patterns of Plasmodium knowlesi Infections in Sabah, Malaysia. Emerg. Infect. Dis. 2016, 22, 201–209. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Grigg, M.J.; Cox, J.; William, T.; Jelip, J.; Fornace, K.M.; Brock, P.M.; von Seidlein, L.; Barber, B.E.; Anstey, N.M.; Yeo, T.W.; et al. Individual-level factors associated with the risk of acquiring human Plasmodium knowlesi malaria in Malaysia: A case-control study. Lancet Planet. Health 2017, 1, e97–e104. [Google Scholar] [CrossRef]
- Müller, M.; Schlagenhauf, P. Plasmodium knowlesi in travellers, update 2014. Int. J. Infect. Dis. 2014, 22, 55–64. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Babalola, S.; Adedokun, S.T.; McCartney-Melstad, A.; Okoh, M.; Asa, S.; Tweedie, I.; Tompsett, A. Factors associated with caregivers’ consistency of use of bed nets in Nigeria: A multilevel multinomial analysis of survey data. Malar. J. 2018, 17, 280. [Google Scholar] [CrossRef] [Green Version]
- Nofal, S.D.; Peto, T.J.; Adhikari, B.; Tripura, R.; Callery, J.; Bui, T.M.; Von Seidlein, L.; Pell, C. How can interventions that target forest-goers be tailored to accelerate malaria elimination in the Greater Mekong Subregion? A systematic review of the qualitative literature. Malar. J. 2019, 18, 32. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ahorlu, C.S.; Adongo, P.; Koenker, H.; Zigirumugabe, S.; Sika-Bright, S.; Koka, E.; Tabong, P.T.-N.; Piccinini, D.; Segbaya, S.; Olapeju, B.; et al. Understanding the gap between access and use: A qualitative study on barriers and facilitators to insecticide-treated net use in Ghana. Malar. J. 2019, 18, 417. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sundararajan, R.; Kalkonde, Y.; Gokhale, C.; Greenough, P.G.; Bang, A. Barriers to Malaria Control among Marginalized Tribal Communities: A Qualitative Study. PLoS ONE 2013, 8, e81966. [Google Scholar] [CrossRef] [Green Version]
- Espino, F.; Manderson, L.; Acuin, C.; Domingo, F.; Ventura, E. Perceptions of malaria in a low endemic area in the Philippines: Transmission and prevention of disease. Acta Trop. 1997, 63, 221–239. [Google Scholar] [CrossRef]
- Kahissay, M.H.; Fenta, T.G.; Boon, H. Beliefs and perception of ill-health causation: A socio-cultural qualitative study in rural North-Eastern Ethiopia. BMC Public Health 2017, 17, 124. [Google Scholar] [CrossRef] [Green Version]
- Das, A.; Das Gupta, R.K.; Friedman, J.; Pradhan, M.M.; Mohapatra, C.C.; Sandhibigraha, D. Community perceptions on malaria and care-seeking practices in endemic Indian settings: Policy implications for the malaria control programme. Malar. J. 2013, 12, 39. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kamat, V.R. “I thought it was only ordinary fever!” cultural knowledge and the micropolitics of therapy seeking for childhood febrile illness in Tanzania. Soc. Sci. Med. 2006, 62, 2945–2959. [Google Scholar] [CrossRef] [PubMed]
- Taek, M.M.; Banilodu, L.; Neonbasu, G.; Watu, Y.V.; Prajogo, E.W.B.; Agil, M. Ethnomedicine of Tetun ethnic people in West Timor Indonesia: Philosophy and practice in the treatment of malaria. Integr. Med. Res. 2019, 8, 139–144. [Google Scholar] [CrossRef] [PubMed]
- Monroe, A.; Moore, S.; Olapeju, B.; Merritt, A.P.; Okumu, F. Unlocking the human factor to increase effectiveness and sustainability of malaria vector control. Malar. J. 2021, 20, 404. [Google Scholar] [CrossRef] [PubMed]
- Roll Back Malaria Partnership to End Malaria. The Strategic Framework for Malaria Social and Behaviour Change Communication 2018–2030. US Pres Malar Initiat. 2018. Available online: https://www.pmi.gov/docs/default-source/default-document-library/tools-curricula/framework-for-malaria-social-and-behavior-change-communication-2018-2030-english.pdf (accessed on 2 February 2022).
- Heggenhougen, H.K.; Hackethal, V.; Vivek, P. The behavioural and social aspects of malaria and its control: An introduction and annotated biliography. UNDP/World Bank/World Health Organization Special Programme for Research and Training in Tropical Diseases 2003. Available online: https://apps.who.int/iris/handle/10665/42504 (accessed on 2 February 2022).
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. BMJ 2021, 372, 71. [Google Scholar] [CrossRef] [PubMed]
- Shearer, F.M.; Huang, Z.; Weiss, D.J.; Wiebe, A.; Gibson, H.; Battle, K.; Pigott, D.M.; Brady, O.J.; Putaporntip, C.; Jongwutiwes, S.; et al. Estimating Geographical Variation in the Risk of Zoonotic Plasmodium knowlesi Infection in Countries Eliminating Malaria. PLoS Negl. Trop. Dis. 2016, 10, e0004915. [Google Scholar] [CrossRef] [PubMed]
- Monroe, A.; Moore, S.; Koenker, H.; Lynch, M.; Ricotta, E. Measuring and characterizing night time human behaviour as it relates to residual malaria transmission in sub-Saharan Africa: A review of the published literature. Malar. J. 2019, 18, 6. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Monroe, A.; Moore, S.; Okumu, F.; Kiware, S.; Lobo, N.F.; Koenker, H.; Sherrard-Smith, E.; Gimnig, J.; Killeen, G.F. Methods and indicators for measuring patterns of human exposure to malaria vectors. Malar. J. 2020, 19, 207. [Google Scholar] [CrossRef] [PubMed]
- Davis, R.; Campbell, R.; Hildon, Z.; Hobbs, L.; Michie, S. Theories of behaviour and behaviour change across the social and behavioural sciences: A scoping review. Health Psychol. Rev. 2014, 9, 323–344. [Google Scholar] [CrossRef] [PubMed]
- Tawfik, G.M.; Dila, K.A.S.; Mohamed, M.Y.F.; Tam, D.N.H.; Kien, N.D.; Ahmed, A.M.; Huy, N.T. A step by step guide for conducting a systematic review and meta-analysis with simulation data. Trop. Med. Health 2019, 47, 46. [Google Scholar] [CrossRef]
- Ma, L.-L.; Wang, X.; Yang, Z.-H.; Huang, D.; Weng, H.; Zeng, X.-T. Methodological quality (risk of bias) assessment tools for primary and secondary medical studies: What are they and which is better? Mil. Med. Res. 2020, 7, 7. [Google Scholar] [CrossRef] [Green Version]
- Barber, B.E.; William, T.; Grigg, M.J.; Menon, J.; Auburn, S.; Marfurt, J.; Anstey, N.M.; Yeo, T.W. A prospective comparative study of Plasmodium knowlesi, falciparum, and vivax malaria in Sabah, Malaysia: High proportion with severe disease from Plasmodium knowlesi and Plasmodium vivax but no mortality with early referral and artesunate therapy. Clin. Infect. Dis. 2013, 56, 383–397. [Google Scholar] [CrossRef] [PubMed]
- Fornace, K.M.; Alexander, N.; Abidin, T.R.; Brock, P.M.; Chua, T.H.; Vythilingam, I.; Ferguson, H.M.; Manin, B.O.; Wong, M.L.; Ng, S.H.; et al. Author response: Local human movement patterns and land use impact exposure to zoonotic malaria in Malaysian Borneo. eLife 2019, 8, e47602. [Google Scholar] [CrossRef] [PubMed]
- Herdiana, H.; Cotter, C.; Coutrier, F.N.; Zarlinda, I.; Zelman, B.W.; Tirta, Y.K.; Greenhouse, B.; Gosling, R.D.; Baker, P.; Whittaker, M.; et al. Malaria risk factor assessment using active and passive surveillance data from Aceh Besar, Indonesia, a low endemic, malaria elimination setting with Plasmodium knowlesi, Plasmodium vivax, and Plasmodium falciparum. Malar. J. 2016, 15, 468. [Google Scholar] [CrossRef] [Green Version]
- Ekawati, L.L.; Johnson, K.C.; Jacobson, J.O.; Cueto, C.A.; Zarlinda, I.; Elyazar, I.R.F.; Fatah, A.; Sumiwi, M.E.; Noviyanti, R.; Cotter, C.; et al. Defining malaria risks among forest workers in Aceh, Indonesia: A formative assessment. Malar. J. 2020, 19, 441. [Google Scholar] [CrossRef]
- Shimizu, S.; Chotirat, S.; Dokkulab, N.; Hongchad, I.; Khowsroy, K.; Kiattibutr, K.; Maneechai, N.; Manopwisedjaroen, K.; Petchvijit, P.; Phumchuea, K.; et al. Malaria cross-sectional surveys identified asymptomatic infections of Plasmodium falciparum, Plasmodium vivax and Plasmodium knowlesi in Surat Thani, a southern province of Thailand. Int. J. Infect. Dis. 2020, 96, 445–451. [Google Scholar] [CrossRef]
- Ngernna, S.; Rachaphaew, N.; Thammapalo, S.; Prikchoo, P.; Kaewnah, O.; Manopwisedjaroen, K.; Phumchuea, K.; Suansomjit, C.; Roobsoong, W.; Sattabongkot, J.; et al. Case Report: Case Series of Human Plasmodium knowlesi Infection on the Southern Border of Thailand. Am. J. Trop. Med. Hyg. 2019, 101, 1397–1401. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fornace, K.M.; Herman, L.; Abidin, T.R.; Chua, T.H.; Daim, S.; Lorenzo, P.J.; Grignard, L.; Nuin, N.A.; Ying, L.T.; Grigg, M.J.; et al. Exposure and infection to Plasmodium knowlesi in case study communities in Northern Sabah, Malaysia and Palawan, The Philippines. PLoS Negl. Trop. Dis. 2018, 12, e0006432. [Google Scholar] [CrossRef] [Green Version]
- Figtree, M.; Lee, R.; Bain, L.; Kennedy, T.; Mackertich, S.; Urban, M.; Cheng, Q.; Hudson, B.J. Plasmodium knowlesi in Human, Indonesian Borneo. Emerg. Infect. Dis. 2010, 16, 672–674. [Google Scholar] [CrossRef]
- Ioannidis, J.P.A.; Patsopoulos, N.; Rothstein, H. Reasons or excuses for avoiding meta-analysis in forest plots. BMJ 2008, 336, 1413–1415. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Manderson, L.; Cartwright, E.; Hardon, A. (Eds.) The Routledge Handbook of Medical Anthropology; Milton Park: Abingdon, UK; Routledge: New York, NY, USA, 2016. [Google Scholar]
- Storey, J.D.; Babalola, S.O.; Ricotta, E.E.; Fox, K.A.; Toso, M.; Lewicky, N.; Koenker, H. Associations between ideational variables and bed net use in Madagascar, Mali, and Nigeria. BMC Public Heath 2018, 18, 484. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ricotta, E.; Boulay, M.; Ainslie, R.; Babalola, S.; Fotheringham, M.; Koenker, H.; Lynch, M. The use of mediation analysis to assess the effects of a behaviour change communication strategy on bed net ideation and household universal coverage in Tanzania. Malar. J. 2015, 14, 15. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Olapeju, B.; Adams, C.; Wilson, S.; Simpson, J.; Hunter, G.C.; Davis, T.; Mitchum, L.; Cox, H.; James, K.; Orkis, J.; et al. Malaria care-seeking and treatment ideation among gold miners in Guyana. Malar. J. 2022, 21, 29. [Google Scholar] [CrossRef] [PubMed]
- Munajat, M.B.; Rahim, M.A.F.A.; Wahid, W.; Rakna, M.I.M.S.; Divis, P.C.S.; Chuangchaiya, S.; Lubis, I.N.D.; Osman, E.; Kasri, M.R.M.; Idris, Z.M. Perceptions and prevention practices on malaria among the indigenous Orang Asli community in Kelantan, Peninsular Malaysia. Malar. J. 2021, 20, 202. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. Multisectoral Approach to the Prevention and Control of Vector-Borne Disease; World Health Organization: Geneva, Switzerland, 2020. [Google Scholar]
- Scott, J. Proposed Integrated Control of Zoonotic Plasmodium knowlesi in Southeast Asia Using Themes of One Health. Trop. Med. Infect. Dis. 2020, 5, 175. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. Fact Sheet on Sustainable Development Goals (SDGs): Health Targets; World Health Organization: Geneva, Switzerland, 2018; Available online: www.euro.who.int/sdgs (accessed on 2 February 2022).
- Finda, M.F.; Moshi, I.R.; Monroe, A.; Limwagu, A.J.; Nyoni, A.P.; Swai, J.K.; Ngowo, H.; Minja, E.G.; Toe, L.P.; Kaindoa, E.W.; et al. Linking human behaviours and malaria vector biting risk in south-eastern Tanzania. PLoS ONE 2019, 14, e0217414. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Inclusion Criteria | Exclusion Criteria |
|---|---|
| 1. Present original (primary) data involving human behaviors, activities, or exposure to P. knowlesi malaria (e.g., bed nets usage, repellent usage, work exposure, and outdoor activities). | 1. Articles that include mosquito biting rates or any entomological study without measuring human behavior. |
| 2. Studies with sample populations from any malaria-endemic setting in Asia; studies involving travelers also accepted. | 2. Laboratory studies, in vivo and in vitro, small communication reports, posters, and Plasmodium malaria studies not relating to P. knowlesi. |
| 3. Quantitative or qualitative studies describing human behaviors during times when malaria transmission can occur (such as relationships, associations, or possible contributing factors); for example, presenting positive cases of P. knowlesi in the study site. | 3. Reviews, protocols, guidelines, abstracts, preprints, conference papers, and commentary papers. |
| 4. Published in English between January 2010 and December 2020. | |
| 5. Published as a full peer-reviewed paper. |
| Citation | Author | Location | The Night-Time Activities Identified in the Studies |
|---|---|---|---|
| [6] | Herdiana et al. | Indonesia | The subjects were exposed due to their livelihood activities, traveling history, and overnight sleeping. In case 2 (non-cluster cases), they had overnighted in Aceh but there was no description of the activities. In case 3 (non-cluster cases), they had overnighted at a campsite in Sabang due to work for 1 month. In case 8 (cluster cases), they spent the night at Sabang as the subject was an owner of a tourist shop |
| [11] | Manin et al. | Sabah, Malaysia | 50% of the villagers would be indoors by 8 p.m. and out the next morning by 5 a.m. for work at the plantation |
| [14] | Fornace et al. | Sabah, Malaysia | No description on night-time behavior or activities |
| [16] | Grigg et al. | Sabah, Malaysia | The study subjects traveled overnight outside the village and slept outside their home |
| [37] | Barber et al. | Sabah, Malaysia | The study subjects overnighted in a forest for 4 weeks, overnighted in a plantation for 4 weeks, and also performed livelihood activities |
| [38] | Fornace et al. | Sabah, Malaysia | No description of night-time behavior or activities |
| [39] | Herdiana et al. | Indonesia | The study subjects were exposed due to their livelihood activities; they slept outside the house the previous night and had their workplace near or in the forest that required them to sleep overnight |
| [40] | Ekawati et al. | Indonesia | The study subjects were exposed due to their livelihood activities and occupation (agricultural work) and they returned home at night. These forest workers stayed overnight at a plantation (slept in a basic hut). Subjects who guarded the cattle at ranches were also at risk, including the police who patrolled for 24 h or training academy cadets and forest ranger patrols 1 and 2: Not described in detail, but a few nights to 2 weeks at a forest fringe plantation and up to 1 month at a plantation located deeper in the forest 3. Spent the night in two night shifts at the ranches 4. 24-h shift or 2–4 months of training academy 5. 2–3 h at night and 2 days per week or 8–12 days per month from 9 a.m. to 5 p.m |
| [41] | Shimizu et al. | Thailand | No description of night-time behavior or activities |
| [42] | Ngernna et al. | Thailand | No description of night-time behavior or activities |
| [43] | Fornace et al. | Sabah, Malaysia | No description on night-time behavior or activities |
| [44] | Figtree et al. | Australian traveler who went to Kalimantan, Indonesia | Night-time activities were not mentioned |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Naserrudin, N.A.; Hod, R.; Jeffree, M.S.; Ahmed, K.; Culleton, R.; Hassan, M.R. The Role of Human Behavior in Plasmodium knowlesi Malaria Infection: A Systematic Review. Int. J. Environ. Res. Public Health 2022, 19, 3675. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph19063675
Naserrudin NA, Hod R, Jeffree MS, Ahmed K, Culleton R, Hassan MR. The Role of Human Behavior in Plasmodium knowlesi Malaria Infection: A Systematic Review. International Journal of Environmental Research and Public Health. 2022; 19(6):3675. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph19063675
Chicago/Turabian StyleNaserrudin, Nurul Athirah, Rozita Hod, Mohammad Saffree Jeffree, Kamruddin Ahmed, Richard Culleton, and Mohd Rohaizat Hassan. 2022. "The Role of Human Behavior in Plasmodium knowlesi Malaria Infection: A Systematic Review" International Journal of Environmental Research and Public Health 19, no. 6: 3675. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph19063675