
A Realist Review of How Community-Based Drug Checking Services Could Be Designed and Implemented to Promote Engagement of People Who Use Drugs
 , , , , , ,
, , , , , ,  ,
, 
Abstract
:1. Introduction
Aims and Objectives
- How has increased engagement of PWUD with DCS been evidenced in the existing literature?
- What are the plausible mechanisms that increase engagement of PWUD?
- What is the role of context in enabling or constraining engagement with DCS?
2. Methods
2.1. Formation of Initial Programme Theories (IPTs)
2.2. Search Process
- (“Drug check *” OR “Drug test *” OR “Drug safety test *” OR “Pill test *” OR “Pill check *” OR “Multi-agency safety test *” OR “Street drug analysis” OR “Drug purity” OR “Drug market monitoring”)
- AND (“harm reduction” OR “overdose” OR “substance use” OR “drug use” OR “toxicology” OR “spectro *” OR “chemometrics”)
- (“Drug check *” OR “Drug test *” OR “Drug safety test *” OR “Pill test *” OR “Pill check *” OR “Drug purity”)
- AND (“harm reduction” OR “toxicology” OR “spectro *”)
2.3. Inclusion/Exclusion Criteria
- Experimental or intervention related studies including randomised controlled trials, prospective or other observational studies, case reports, feasibility/acceptability studies, implementation/evaluation/action or process research, quasi-experimental research, and qualitative methods;
- Existing reviews of all types;
- Grey literature of all types. The search for grey literature is justified by the goal of the realist review to seek out ‘the inner workings of interventions’ [25] (p. 29). Therefore, sources of all types that may contain important contextualisation of the intervention are deemed valuable.
2.4. Relevance and Rigour
2.5. Data Extraction and Synthesis
3. Results
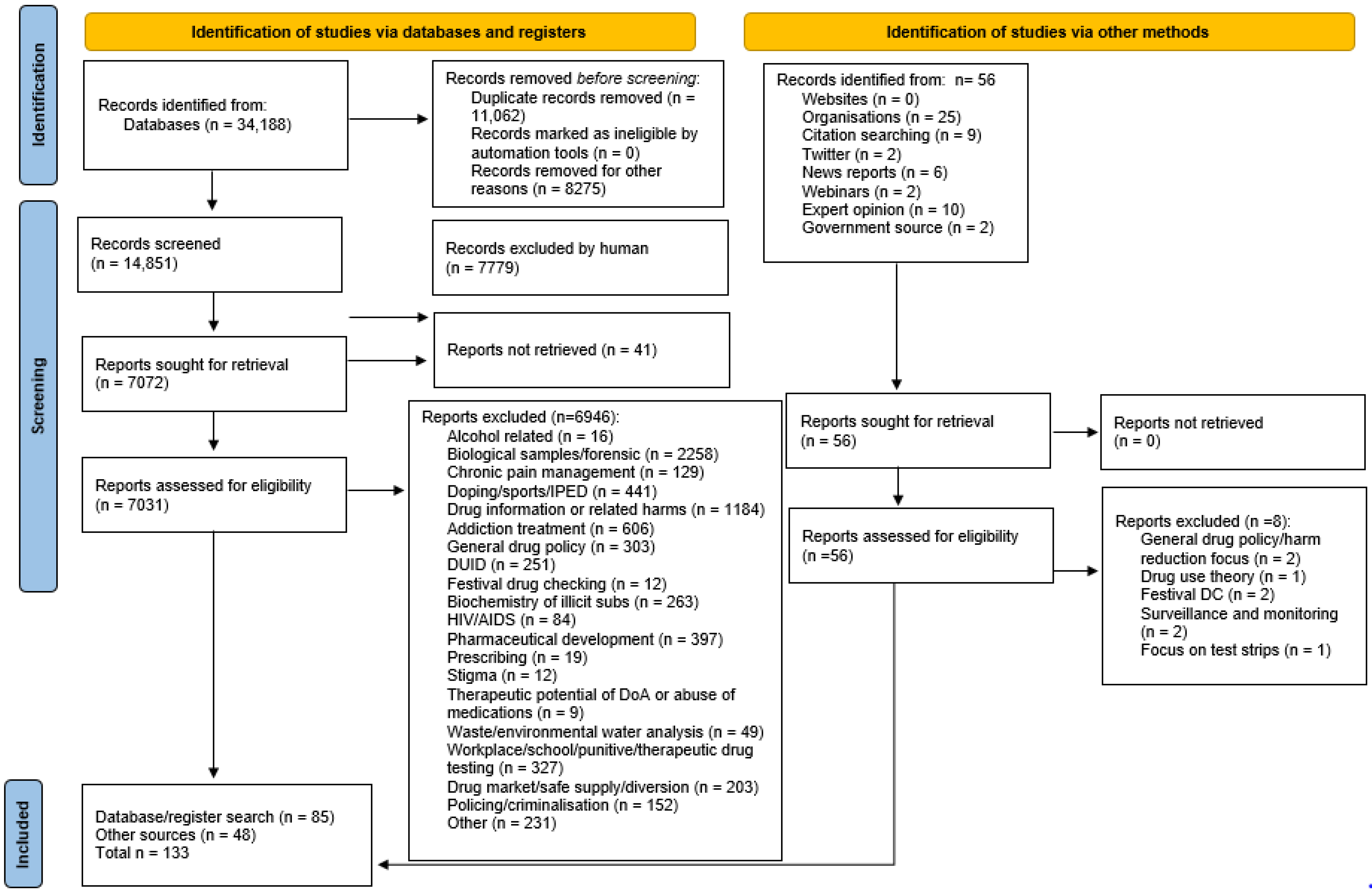
3.1. Search Results and Study Characteristics
3.2. Testing and Refinement of Programme Theories
3.2.1. Legislation and Regulation
“What’s to stop them from stopping us when we leave here? Right? To see if we finished all our dope and charging us with possession, right? You know, just leaving here, is that a probable cause for them to stop us?”.[39] (p. 5)
“For a person to be aiding and abetting the offence, they must be ‘linked in purpose’ with the drug user, and that it is also necessary for the person to engage in some action or encouragement which makes the offence more likely to occur”.[55] (p. 15)
3.2.2. Existing Drug Market and Level of Drug-Related Harm
3.2.3. Integration into an Existing Service
“Harm reduction counseling, health education and connection to services including treatment for substance use disorder should be part of any drug checking program”[83] (p. 11)
3.2.4. Lived/Living Experience at All Levels
3.2.5. Accessibility
“Physical distances between harm reduction services and the residences and drug purchase and use locations of PWUD have an impact on their willingness to access such services”.[77] (p. 4)
“There’s business people out there, there’s lawyers out there that use drugs. They’re not going to go to a place that let’s say people who are homeless would go to”.[19] (p. 4)
3.2.6. Testing Process
3.2.7. Service Users’ Previous Experience
“They’ve got better things to do with their time than line up on some machine. They just want to get fixed, you know? And most of them don’t really care. Most of them are in some kind of state where, quite frankly, if they died they wouldn’t really care anyway. Or the thought of it doesn’t really scare them anymore, you know what I mean?”.[20] (p. 8)
4. Discussion and Recommendations
Strengths and Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Wallace, B.; Van Roode, T.; Pagan, F.; Hore, D.; Pauly, B. The potential impacts of community drug checking within the overdose crisis: Qualitative study exploring the perspective of prospective service users. BMC Public Health 2021, 21, 1156. [Google Scholar] [CrossRef] [PubMed]
- Measham, F.C. Drug safety testing, disposals and dealing in an English field: Exploring the operational and behavioural outcomes of the UK’s first onsite ‘drug checking’ service. Int. J. Drug Policy 2019, 67, 102–107. [Google Scholar] [CrossRef] [PubMed]
- Maghsoudi, N.; Tanguay, J.; Scarfone, K.; Rammohan, I.; Ziegler, C.; Werb, D.; Scheim, A.I. Drug checking services for people who use drugs: A systematic review. Addiction 2021, 117, 532–544. [Google Scholar] [CrossRef] [PubMed]
- Trans-European Drug Information Project. TEDI Guidelines: Drug Checking Methodology; Editions for Social Change; Trans-European Drug Information Project 2022. IBSN 978-2-9199472-7-0. Available online: https://www.tedinetwork.org/wp-content/uploads/2022/03/TEDI_Guidelines_final.pdf (accessed on 3 August 2022).
- Barratt, M.J.; Kowalski, M.; Maier, L.J.; Ritter, A. Profiles of Drug Checking Services in 2017; Drug Policy Modelling Program Bulletin, No. 24; National Drug and Alcohol Research Centre, UNSW: Sydney, Australia, 2018; Available online: https://ndarc.med.unsw.edu.au/sites/default/files/Profiles%20of%20drug%20checking%20services%20in%202017.pdf (accessed on 3 August 2022).
- Barratt, M.J.; Kowalski, M.; Maier, L.J.; Ritter, A. Global Review of Drug Checking Services Operating in 2017; Drug Modelling Program Bulletin, No. 24; National Drug and Alcohol Research Centre, UNSW: Sydney, Australia, 2018; Available online: https://ndarc.med.unsw.edu.au/sites/default/files/ndarc/resources/Global%20review%20of%20drug%20checking%20services%20operating%20in%202017.pdf (accessed on 3 August 2022).
- Barratt, M.J.; Bruno, R.; Ezard, N.; Ritter, A. Pill testing or drug checking in Australia: Acceptability of service design features. Drug Alcohol Rev. 2018, 37, 226–236. [Google Scholar] [CrossRef]
- Giulini, F.; Keenan, E.; Killeen, N.; Ivers, J.H. A systematized review of drug-checking and related considerations for implementation as a harm reduction intervention. J. Psychoact. Drugs 2022, 1–9. [Google Scholar] [CrossRef]
- Digital, Culture, Media and Sport Committee. The Future of UK Music Festivals, First Report of Session 2021–2022. House of Commons, 29 May 2021. Available online: https://committees.parliament.uk/publications/6136/documents/68377/default/ (accessed on 3 August 2022).
- Sande, M.; Šabić, S. The importance of drug checking outside the context of nightlife in Slovenia. Harm Reduct. J. 2018, 15, 2. [Google Scholar] [CrossRef]
- Goncalves, R.; Titier, K.; Latour, V.; Peyre, A.; Castaing, N.; Daveluy, A.; Molimard, M. Suitability of infrared spectroscopy for drug checking in harm reduction centres. Int. J. Drug Policy 2021, 88, 103037. [Google Scholar] [CrossRef]
- Koning, R.P.J.; Benschop, A.; Wijffels, C.; Noijen, J. Visitors of the Dutch drug checking services: Profile and drug use experience. Int. J. Drug Policy 2021, 95, 103293. [Google Scholar] [CrossRef]
- Brunt, T.M. Drug Checking as a Harm Reduction tool for Recreational Drug Users: Opportunities and Challenges, Background Paper commissioned by the EMCDDA for Health and Social Response to Drug Problems: A European guide. European Monitoring Centre for Drugs and Drug Addiction, 30 October 2017. Available online: https://www.emcdda.europa.eu/system/files/attachments/6339/EuropeanResponsesGuide2017_BackgroundPaper-Drug-checking-harm-reduction_0.pdf (accessed on 3 August 2022).
- Laing, M.K.; Tupper, K.W.; Fairbairn, N. Drug checking as a potential strategic overdose response in the fentanyl era. Int. J. Drug Policy 2018, 62, 59–66. [Google Scholar] [CrossRef]
- Carroll, J.J.; Mackin, S.; Schmidt, C.; McKenzie, M.; Green, T.C. The Bronze Age of drug checking: Barriers and facilitators to implementing advanced drug checking amidst police violence and COVID-19. Harm Reduct. J. 2022, 19, 9. [Google Scholar] [CrossRef]
- Carroll, J.J. Auras of Detection: Power and knowledge in drug prohibition. Contemp. Drug Probl. 2021, 48, 327–345. [Google Scholar] [CrossRef]
- Sherman, S.G.; Morales, K.B.; Park, J.N.; McKenzie, M.; Marshall, B.D.L.; Green, T.C. Acceptability of implementing community-based drug checking services for people who use drugs in three United States cities: Baltimore, Boston and Providence. Int. J. Drug Policy 2019, 68, 46–53. [Google Scholar] [CrossRef] [PubMed]
- Karch, L.; Tobias, S.; Schmidt, C.; Doe-Simkins, M.; Carter, N.; Salisbury-Afshar, E.; Carberg-Racich, S. Results from a mobile drug checking pilot program using three technologies in Chicago, IL, USA. Drug Alcohol Depend. 2021, 228, 108976. [Google Scholar] [CrossRef]
- Wallace, B.; Van Roode, T.; Pagan, F.; Phillips, P.; Wagner, H.; Calder, S.; Aasen, J.; Pauly, B.; Hore, D. What is needed for implementing drug checking services in the context of the overdose crisis? A qualitative study to explore perspectives of potential service users. Harm Reduct. J. 2020, 17, 29. [Google Scholar] [CrossRef] [PubMed]
- Bardwell, G.; Boyd, J.; Tupper, K.W.; Kerr, T. “We don’t got that kind of time, man. We’re trying to get high!”: Exploring potential use of drug checking technologies among structurally vulnerable people who use drugs. Int. J. Drug Policy 2019, 71, 125–132. [Google Scholar] [CrossRef] [PubMed]
- Office for National Statistics. Deaths Related to Drug Poisoning in England and Wales: 2021 Registrations. 2021. Available online: https://www.ons.gov.uk/peoplepopulationandcommunity/birthsdeathsandmarriages/deaths/bulletins/deathsrelatedtodrugpoisoninginenglandandwales/2021registrations (accessed on 3 August 2022).
- National Records of Scotland. Drug Related Deaths in Scotland in 2021. 2022. Available online: https://www.nrscotland.gov.uk/files//statistics/drug-related-deaths/21/drug-related-deaths-21-report.pdf (accessed on 3 August 2022).
- European Monitoring Centre for Drugs and Drug Addiction. European Drug Report 2020: Trends and Developments; EMCDDA: Lisbon, Portugal, 2020; ISBN 978-92-9497-544-7. Available online: https://www.emcdda.europa.eu/publications/edr/trends-developments/2020_en (accessed on 3 August 2022).
- Measham, F.; Turnbull, G. Intentions, actions and outcomes: A follow up survey on harm reduction practices after using an English festival drug checking service. Int. J. Drug Policy 2021, 95, 103270. [Google Scholar] [CrossRef] [PubMed]
- Pawson, R.; Greenhalgh, T.; Harvey, G.; Walshe, K. Realist review-a new method of systematic review designed for complex policy interventions. J. Health Serv. Res. Policy 2005, 10 (Suppl. 1), 21–34. [Google Scholar] [CrossRef]
- Pawson, R.; Tilley, N. Realistic Evaluation; Sage Publications: Thousand Oaks, CA, USA, 1997. [Google Scholar]
- Rycroft-Malone, J.; McCormack, B.; Hutchinson, A.M.; DeCorby, K.; Bucknall, T.K.; Kent, B.; Schultz, A.; Snelgrove-Clarke, E.; Stetler, C.B.; Titler, M.; et al. Realist synthesis: Illustrating the method for implementation research. Implement. Sci. 2012, 7, 33. [Google Scholar] [CrossRef]
- Rhodes, T. Risk environments and drug harms: A social science for harm reduction approach. Int. J. Drug Policy 2009, 20, 193–201. [Google Scholar] [CrossRef]
- Collins, A.B.; Boyd, J.; Cooper, H.L.F.; McNeil, R. The intersectional risk environment of people who use drugs. Soc. Sci. Med. 2019, 234, 112384. [Google Scholar] [CrossRef]
- Duff, C. The drifting city: The role of affect and repair in the development of “Enabling Environments”. Int. J. Drug Policy 2009, 20, 202–208. [Google Scholar] [CrossRef] [PubMed]
- Duff, C. Exploring the role of ‘enabling places’ in promoting recovery from mental illness: A qualitative test of a relational model. Health Place 2012, 18, 1388–1395. [Google Scholar] [CrossRef] [PubMed]
- Damschroder, L.J.; Aron, D.C.; Keith, R.E.; Kirsh, S.R.; Alexander, J.A.; Lowery, J.C. Fostering implementation of health services research findings into practice: A consolidated framework for advancing implementation science. Implement. Sci. 2009, 4, 50. [Google Scholar] [CrossRef]
- Wong, G.; Greenhalgh, T.; Westhrop, G.; Pawson, R. Quality Standards for Realist Syntheses and Meta-Narrative Reviews; RAMESES: London, UK, 2014; Available online: https://www.betterevaluation.org/sites/default/files/Quality_standards_for_RS_and_MNR_v3final.pdf (accessed on 3 August 2022).
- Pawson, R.; Greenhalgh, T.; Harvey, G.; Walshe, K. Realist Synthesis: An Introduction; RMP Methods Paper 2/2004; University of Manchester, ESRC Res Methods Program: Manchester, UK, 2004; Available online: https://www.researchgate.net/publication/228855827_Realist_Synthesis_An_Introduction (accessed on 3 August 2022).
- Palamar, J.J.; Acosta, P.; Sutherland, R.; Shedlin, M.G.; Barratt, M.J. Adulterants and altruism: A qualitative investigation of “drug checkers” in North America. Int. J Drug Policy 2019, 74, 160–169. [Google Scholar] [CrossRef]
- Davis, C.S.; Lieberman, A.J.; O’Kelley-Bangsberg, M. Legality of drug checking equipment in the United States: A systematic legal analysis. Drug Alcohol Depend. 2022, 234, 109425. [Google Scholar] [CrossRef] [PubMed]
- Guirguis, A.; Gittins, R.; Schifano, F. Piloting the UK’s first Home-Office-licensed pharmacist-led drug checking service at a community substance misuse service. Behav. Sci. 2020, 10, 121. [Google Scholar] [CrossRef]
- Drug Checking Project Advisory Group Meeting Minutes; University of Stirling: Stirling, UK, 2022.
- Bardwell, G.; Strike, C.; Altenberg, J.; Barnaby, L.; Kerr, T. Implementation contexts and the impact of policing on access to supervised consumption services in Toronto, Canada: A qualitative comparative analysis. Harm Reduct. J. 2019, 16, 30. [Google Scholar] [CrossRef]
- Burris, S.; Blankenship, K.M.; Donoghoe, M.; Sherman, S.; Vernick, J.S.; Case, P.; Koester, S. Addressing the “risk environment” for injection drug users: The mysterious case of the missing cop. Milbank Q. 2004, 82, 125–156. [Google Scholar] [CrossRef] [PubMed]
- KnowYourStuffNZ. Drug and Substance Checking Legislation Bill Passes into Law. KnowYorStuffNZ, 23 November 2021. Available online: https://knowyourstuff.nz/2021/11/23/drug-and-substance-checking-legislation-bill-passes-into-law/ (accessed on 3 August 2022).
- Scottish Government. International approaches to drug law reform; Crime and Justice. Justice Directorate, 5 March 2021. ISBN 9781800047525. Available online: https://www.gov.scot/publications/international-approaches-drug-law-reform/ (accessed on 3 August 2022).
- Minutes from Conversations with two Staff Members at the Drug Information and Monitoring System, The Netherlands. Personal communication, 2021.
- Betzler, F.; Helbig, J.; Viohl, L.; Ernst, F.; Roediger, L.; Gutwinski, S.; Ströhle, A.; Köhler, S. Drug checking and its potential impact on substance use. Eur. Addict Res. 2021, 27, 25–32. [Google Scholar] [CrossRef]
- Goldman, J.E.; Waye, K.M.; Periera, K.A.; Krieger, M.S.; Yedinak, J.L.; Marshall, B.D.L. Perspectives on rapid fentanyl test strips as a harm reduction practice among young adults who use drugs: A qualitative study. Harm Reduct. J. 2019, 16, 3. [Google Scholar] [CrossRef] [Green Version]
- Rouhani, S.; Park, J.N.; Morales, K.B.; Green, T.C.; Sherman, S.G. Harm reduction measures employed by people using opioids with suspected fentanyl exposure in Boston, Baltimore, and Providence. BMC 2019, 16, 39. [Google Scholar] [CrossRef] [PubMed]
- Betsos, A.; Valleriani, J.; Boyd, J.; Bardwell, G.; Kerr, T.; McNeil, R. “I couldn’t live with killing one of my friends or anybody”: A rapid ethnographic study of drug sellers’ use of drug checking. Int. J. Drug Policy 2021, 87, 102845. [Google Scholar] [CrossRef] [PubMed]
- Reed, M.K.; Roth, A.M.; Tabb, L.P.; Groves, A.K.; Lankenau, S.E. “I probably got a minute”: Perceptions of fentanyl test strip use among people who use stimulants. Int. J. Drug Policy 2021, 92, 103147. [Google Scholar] [CrossRef] [PubMed]
- Weicker, N.P.; Owczarzak, J.; Urquhart, G.; Park, J.N.; Rouhani, S.; Ling, R.; Morris, M.; Sherman, S. Agency in the fentanyl era: Exploring the utility of fentanyl test strips in an opaque drug market. Int. J. Drug Policy 2020, 84, 102900. [Google Scholar] [CrossRef]
- Moore, D. Governing street-based injecting drug users: A critique of heroin overdose prevention in Australia. Soc. Sci. Med. 2004, 59, 1547–1557. [Google Scholar] [CrossRef]
- Shannon, K.; Rusch, M.; Shoveller, J.; Alexson, D.; Gibson, K.; Tyndall, M.W. Mapping violence and policing as an environmental–structural barrier to health service and syringe availability among substance-using women in street-level sex work. Int. J Drug Policy 2008, 19, 140–147. [Google Scholar] [CrossRef]
- Herbert, S.; Beckett, K.; Stuart, F. Policing social marginality: Contrasting approaches. Law Soc. Inq. 2018, 43, 1491–1513. [Google Scholar] [CrossRef]
- Sage, C.; Meeson, J.S.; Aasen, J. The Drug Checking Manual, Chapter 1: Creating Safer Spaces with Harm Reduction in Drug Checking Settings. The Drug Resource and Education Project. 2021. Available online: https://www.crismquebecatlantic.ca/wp-content/uploads/2022/02/thedrugcheckingmanual_chapter1.pdf (accessed on 3 August 2022).
- Measham, F. City checking: Piloting the UK’s first community-based drug safety testing (drug checking) service in 2 city centres. Br. J. Clin. Pharmacol. 2020, 86, 420–428. [Google Scholar] [CrossRef]
- Tregoning, W. Drug Checking Services brief, Unharm! Getting Drugs Right. 2016. Available online: https://www.unharm.org/drug-checking-brief/ (accessed on 3 August 2022).
- Green, T.C.; Park, J.N.; Sherman, S.G.; Gilbert, M.; McKenzie, M.; Struth, E.; Lucas, R.; Clarke, W. An assessment of the limits of detection, sensitivity and specificity of three devices for public health-based drug checking of fentanyl in street-acquired samples. Int. J. Drug Policy 2020, 77, 102661. [Google Scholar] [CrossRef]
- Larnder, A.; Burek, P.; Wallace, B.; Hore, D.K. Third party drug checking: Accessing harm reduction services on the behalf of others. Harm Reduct. J. 2021, 18, 99. [Google Scholar] [CrossRef]
- Minutes from the presentations of various speakers. In Proceedings of the Alliance for Collaborative Drug Checking Conference, online, 3–5 November 2021.
- Bacon, M. Desistance from criminalisation: Police culture and new directions in drugs policing. Polic. Soc. 2022, 32, 522–539. [Google Scholar] [CrossRef]
- Watson, T.M.; Bayoumi, A.M.; Hopkins, S.; Wright, A.; Naraine, R.; Khorasheh, T.; Challacombe, L.; Strike, C. Creating and sustaining cooperative relationships between supervised injection services and police: A qualitative interview study of international stakeholders. Int. J. Drug Policy 2018, 61, 1–6. [Google Scholar] [CrossRef] [PubMed]
- Greer, A.; Zakimi, N.; Butler, A.; Ferencz, S. Simple possession as a ‘tool’: Drug law enforcement practices among police officers in the context of depenalization in British Columbia, Canada. Int. J. Drug Policy 2022, 99, 103471. [Google Scholar] [CrossRef] [PubMed]
- Fregonese, M.; Albino, A.; Covino, C.; Gili, A.; Bacci, M.; Nicoletti, A.; Gambelunghe, C. Drug checking as strategy for harm reduction in recreational contests: Evaluation of two different drug analysis methodologies. Front. Psych. 2021, 12, 596895. [Google Scholar] [CrossRef] [PubMed]
- Karamouzian, M.; Dohoo, C.; Forsting, S.; McNeil, R.; Kerr, T.; Lysyshyn, M. Evaluation of a fentanyl drug checking service for clients of a supervised injection facility, Vancouver, Canada. Harm Reduct. J. 2018, 15, 46. [Google Scholar] [CrossRef]
- Maghsoudi, N.; MacDonald, K.; Thomas, R.; Toronto’s Drug Checking Service. Drug Policy Alliance Researchers’ Roundtable, Canada, 19 November 2020. Available online: https://www.youtube.com/watch?v=65WqErDu1-0 (accessed on 3 August 2022).
- Park, J.N.; Frankel, S.; Morris, M.; Dieni, O.; Fahey-Morrison, L.; Luta, M.; Sherman, S.G. Evaluation of fentanyl test strip distribution in two Mid-Atlantic syringe services programs. Int. J. Drug Policy 2021, 94, 103196. [Google Scholar] [CrossRef]
- Tupper, K.W.; McCrae, K.; Garber, I.; Lysyshyn, M.; Wood, E. Initial results of a drug checking pilot program to detect fentanyl adulteration in a Canadian setting. Drug Alcohol Depend. 2018, 190, 242–245. [Google Scholar] [CrossRef]
- Trayner, K.M.A.; Palmateer, N.E.; Hutchinson, S.J.; Goldberg, D.J.; Shepherd, S.J.; Gunson, R.N.; Tweed, E.J.; Priyadarshi, S.; Sumnall, H.; Atkinson, A.; et al. High willingness to use drug consumption rooms among people who inject drugs in Scotland: Findings from a national bio-behavioural survey among people who inject drugs. Int. J. Drug Policy 2021, 90, 102731. [Google Scholar] [CrossRef]
- Wood, J.D.; Taylor, C.J.; Groff, E.R.; Ratcliffe, J.H. Aligning policing and public health promotion: Insights from the world of foot patrol. Police Pract. Res. 2015, 16, 211–223. [Google Scholar] [CrossRef]
- Kerr, T.; Tupper, K. Drug Checking as a Harm Reduction Intervention. Evidence review report; British Columbiaa Centre on Substance Use. 2017. Available online: https://res.mdpi.com/data/mdpi_references_chicago_guide-update-v6.pdf (accessed on 3 August 2022).
- Ventura, M.; Noijen, J.; Buchel, A.; Isvy, A.; Van Huyck, C.; Martins, D.; Nagy, C.; Schipper, V.; Ugarte, M.; Valente, H. Drug Checking Service: Good Practice Standards; Nightlife Empowerment and Wellbeing Implementation Project. 2012. Available online: https://www.drugsandalcohol.ie/28907/1/NEWIP_Drug%20checking_standards.pdf (accessed on 3 August 2022).
- Ritter, A. Making drug policy in summer—Drug checking in Australia as providing more heat than light. Drug Alcohol Rev. 2020, 39, 12–20. [Google Scholar] [CrossRef] [Green Version]
- Groves, A. ‘Worth the test?’ Pragmatism, pill testing and drug policy in Australia. Harm Reduct. J. 2018, 15, 12. [Google Scholar] [CrossRef] [PubMed]
- Fisher, H.; Measham, F. Night Lives, Reducing Drug Related Harm in the Nighttime Economy. Volteface. 2018. Available online: https://volteface.me/app/uploads/2018/07/Night-Lives-PDF.pdf (accessed on 3 August 2022).
- Beckett, K. The uses and abuses of police discretion: Toward harm reduction policing. Harv. L. Pol’y Rev. 2016, 10, 77. Available online: https://harvardlpr.com/wp-content/uploads/sites/20/2016/02/10.1_6_Beckett.pdf (accessed on 3 August 2022).
- Eastwood, N.; Shiner, M.; Bear, D. The numbers in Black and White: Ethnic Disparities in the Policing and Prosecution of Drug Offences in England and Wales. Release. 2013. Available online: https://www.release.org.uk/sites/default/files/pdf/publications/Release%20-%20Race%20Disparity%20Report%20final%20version.pdf (accessed on 1 August 2022).
- McCann, M.; Vadivelu, S. Saving Lives. Changing Lives. Summary Report on the Findings from an Evaluation of London’s Temporary Overdose Prevention Site (TOPS); Middlesex-London Health Unit: London, ON, Canada, 2019; Available online: https://www.google.com/search?q=Saving+Lives.+Changing+Lives.+Summary+Report+on+the+findings+from+an+Evaluation+of+London%E2%80%99s+Temporary+Overdose+Prevention+Site+(TOPS)&rlz=1C1AWFC_enGB892GB893&oq=Saving+Lives.+Changing+Lives.+Summary+Report+on+the+findings+from+an+Evaluation+of+London%E2%80%99s+Temporary+Overdose+Prevention+Site+(TOPS)&aqs=chrome..69i57.2312j0j4&sourceid=chrome&ie=UTF-8 (accessed on 3 August 2022).
- McCrae, K.; Hayashi, K.; Bardwell, G.; Nosova, E.; Milloy, M.J.; Wood, E.; Ti, L. The effect of injecting alone on the use of drug checking services among people who inject drugs. Int. J. Drug Policy 2020, 79, 102756. [Google Scholar] [CrossRef] [PubMed]
- Beaulieu, T.; Hayashi, K.; Nosova, E.; Milloy, M.J.; De-Beck, K.; Wood, E.; Kerr, T.; Ti, L. Effect of witnessing an overdose on the use of drug checking services among people who use illicit drugs in Vancouver, Canada. Am. J. Drug Alcohol Abuse 2020, 46, 506–511. [Google Scholar] [CrossRef]
- Aasen, J. Drug checking: Shedding Light on Substance Use Issues; British Columbia Pharmacy Association. 2 November 2021. Available online: https://www.bcpharmacy.ca/tablet/fall-21/drug-checking-shedding-light-substance-use-issues (accessed on 3 August 2022).
- Kosmicare. Drug Checking Service Report—November 2019 to November 2020; Kosmic Publications: Lisbon, Portugal, 2020; Available online: https://kosmicare.org/files/kc_report_2020_en.pdf (accessed on 3 August 2022).
- Soukup-Baljak, Y.; Greer, A.M.; Amlani, A.; Sampson, O.; Buxton, J.A. Drug quality assessment practices and communication of drug alerts among people who use drugs. Int. J. Drug Policy 2015, 26, 1251–1257. [Google Scholar] [CrossRef]
- Oh, H.; Kim, K.; Miller, D.; Veloso, D.; Lin, J.; McFarland, W. Fentanyl self-testing in a community-based sample of people who inject drugs, San Francisco. Int. J. Drug Policy 2020, 82, 102787. [Google Scholar] [CrossRef]
- Sherman, S.G.; Morales, K.B.; Park, J.N.; Marshall, B.D.L.; Green, T.C. Fentanyl Overdose Reduction Checking Analysis Study (FORECAST). Johns Hopkins Bloomberg School of Public Health, 6 February 2018. Available online: https://www.btnx.com/files/Johns_Hopkins_Fentanyl_Executive_Summary.pdf (accessed on 3 August 2022).
- Grossman, N. Five years into the Overdose Crisis, Victoria’s Street Drugs are Stronger Than Ever. Capital Daily, 26 April 2021. Available online: https://www.capitaldaily.ca/news/five-years-into-the-overdose-crisis-victorias-street-drugs-are-stronger-than-ever (accessed on 3 August 2022).
- European Monitoring Centre for Drugs and Drug Addiction. European Drug Report 2022: Trends and Developments; Publications Office of the European Union: Luxembourg, 2022; Available online: https://www.emcdda.europa.eu/system/files/publications/14644/TDAT22001ENN.pdf (accessed on 3 August 2022).
- Zibbell, J.E.; Peiper, N.C.; Duhart-Clarke, S.E.; Salazar, Z.R.; Vincent, L.B.; Kral, A.H.; Feinberg, J.H. Consumer discernment of fentanyl in illicit opioids confirmed by fentanyl test strips: Lessons from a syringe services program in North Carolina. Int. J. Drug Policy 2021, 93, 103128. [Google Scholar] [CrossRef]
- Peiper, N.C.; Clarke, S.D.; Vincent, L.B.; Ciccarone, D.; Kral, A.H.; Zibbell, J.E. Fentanyl test strips as an opioid overdose prevention strategy: Findings from a syringe services program in the Southeastern United States. Int. J. Drug Policy 2019, 63, 122–128. [Google Scholar] [CrossRef]
- Olding, M.; Ivsins, A.; Mayer, S.; Betsos, A.; Boyd, J.; Sutherland, C.; Culbertson, C.; Kerr, T.; McNeil, R. A low-barrier and comprehensive community-based harm-reduction site in Vancouver, Canada. Am. J. Public Health 2020, 110, 833–835. [Google Scholar] [CrossRef]
- Kennedy, M.C.; Boyd, J.; Mayer, S.; Collins, A.; Kerr, T.; McNeil, R. Peer worker involvement in low-threshold supervised consumption facilities in the context of an overdose epidemic in Vancouver, Canada. Soc. Sci. Med. 2019, 225, 60–68. [Google Scholar] [CrossRef]
- Kennedy, M.C.; Scheim, A.; Rachlis, B.; Mitra, S.; Bardwell, G.; Rourke, S.; Kerr, T. Willingness to use drug checking within future supervised injection services among people who inject drugs in a mid-sized Canadian city. Drug Alcohol Depend. 2018, 185, 248–252. [Google Scholar] [CrossRef] [PubMed]
- Park, J.N.; Tomko, C.; Silberzahn, B.E.; Haney, K.; Marshall, B.D.L.; Sherman, S.G. A fentanyl test strip intervention to reduce overdose risk among female sex workers who use drugs in Baltimore: Results from a pilot study. Addict. Behav. 2020, 110, 106529. [Google Scholar] [CrossRef] [PubMed]
- Trans-European Drug Information Project. Factsheet on drug checking in Europe. Nightlife, empowerment and wellbeing implementation project. 2011. Available online: https://apdes.pt/wp-content/uploads/2015/12/Factsheet-on-Drug-Checking-in-Europe.pdf (accessed on 3 August 2022).
- Morgan, J.; Jones, A. Pill-testing as a harm reduction strategy: Time to have the conversation. Med. J. Aust. 2019, 211, 447. [Google Scholar] [CrossRef] [PubMed]
- Giné, C.V. Drug checking services: An essential tool for risk and harm reduction. Rev. Esp. Drog. 2019, 44, 67–77. [Google Scholar]
- Harper, L.; Powell, J.; Pijl, E.M. An overview of forensic drug testing methods and their suitability for harm reduction point-of-care services. Harm Reduct. J. 2017, 14, 52. [Google Scholar] [CrossRef]
- Laing, M.K.; Ti, L.; Marmel, A.; Tobias, S.; Shapiro, A.M.; Laing, R.; Lysyshyn, M.; Socias, M.E. An outbreak of novel psychoactive substance benzodiazepines in the unregulated drug supply: Preliminary results from a community drug checking program using point-of-care and confirmatory methods. Int. J. Drug Policy 2021, 93, 103169. [Google Scholar] [CrossRef]
- Tobias, S.; Shapiro, A.M.; Grant, C.J.; Patel, P.; Lysyshyn, M.; Ti, L. Drug checking identifies counterfeit alprazolam tablets. Drug Alcohol Depend. 2021, 218, 108300. [Google Scholar] [CrossRef]
- Brunt, T.M.; Niesink, R.J. The Drug Information and Monitoring System (DIMS) in the Netherlands: Implementation, results, and international comparison. Drug Test. Anal. 2011, 3, 621–634. [Google Scholar] [CrossRef]
- McCrae, K.; Tobias, S.; Grant, C.; Lysyshyn, M.; Laing, R.; Wood, E.; Ti, L. Assessing the limit of detection of Fourier-transform infrared spectroscopy and immunoassay strips for fentanyl in a real-world setting. Drug Alcohol Rev. 2020, 39, 98–102. [Google Scholar] [CrossRef]
- Maghsoudi, N.; McDonald, K.; Stefan, C.; Beriault, D.R.; Mason, K.; Barnaby, L.; Altenberg, J.; MacDonald, R.D.; Caldwell, J.; Nissenbaum, P.; et al. Drug checking services in Toronto working group. Evaluating networked drug checking services in Toronto, Ontario: Study protocol and rationale. Harm Reduct. J. 2020, 17, 9. [Google Scholar] [CrossRef]
- Glick, J.L.; Christensen, T.; Park, J.N.; McKenzie, M.; Green, T.C.; Sherman, S.G. Stakeholder perspectives on implementing fentanyl drug checking: Results from a multi-site study. Drug Alcohol Depend. 2019, 194, 527–532. [Google Scholar] [CrossRef]
- Benschop, A.; Rabes, M.; Korf, D.J. Pill Testing Ecstasy & Prevention: A Scientific Evaluation in Three European Cities; University of Amsterdam, Bonger Institute of Criminology: Amsterdam, The Netherlands, 2002; Available online: http://www.nls-suchtgefahren.de/eu-projekt/texte/EnglPart1[1].pdf (accessed on 4 August 2022).
- Hungerbuehler, I.; Schaub, M.; Buecheli, A. Drug Checking: A prevention measure for a heterogeneous group with high consumption frequency and polydrug use—Evaluation of Zurich’s drug checking services. Harm Reduct. J. 2011, 8, 16. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Krieger, M.S.; Goedel, W.C.; Marshall, B.D.L.; Buxton, J.A.; Lysyshyn, M.; Bernstein, E.; Sherman, S.G.; Rich, J.D.; Hadland, S.E.; Green, T.C. Use of rapid fentanyl test strips among young adults who use drugs. Int. J. Drug Policy 2018, 61, 52–58. [Google Scholar] [CrossRef] [PubMed]
- Valente, H.; Martins, D.; Carvalho, H.; Pires, C.V.; Carvalho, M.C.; Pinto, M.; Barratt, J.M. Evaluation of a drug checking service at a large scale electronic music festival in Portugal. Int. J. Drug Policy 2019, 73, 88–95. [Google Scholar] [CrossRef] [PubMed]
- Australasian Professional Society. Australasian Professional Society on Alcohol and other Drugs. In Proceedings of the APSAD 2019 Conference, Hobart, Australia, 10–13 November 2019. [Google Scholar] [CrossRef]
- Wallace, B.; Hills, R.; Rothwell, J.; Kumar, D.; Garber, I.; Van Roode, T.; Larnder, A.; Pagan, F.; Aasen, J.; Weatherston, J.; et al. Implementing an integrated multi-technology platform for drug checking: Social, scientific, and technological considerations. Drug Test. Anal. 2021, 13, 734–746. [Google Scholar] [CrossRef]
- Long, V.; Arredondo, J.; Ti, L.; Grant, C.; DeBeck, K.; Milloy, M.J.; Lysyshyn, M.; Wood, E.; Kerr, T.; Hayashi, K. Factors associated with drug checking service utilization among people who use drugs in a Canadian setting. Harm Reduct. J. 2020, 17, 100. [Google Scholar] [CrossRef] [PubMed]
- Bardwell, G.; Boyd, J.; Arredondo, J.; McNeil, R.; Kerr, T. Trusting the source: The potential role of drug dealers in reducing drug-related harms via drug checking. Drug Alcohol Depend. 2019, 198, 1–6. [Google Scholar] [CrossRef]
- Mistler, C.B.; Chandra, D.K.; Copenhaver, M.M.; Wickersham, J.A.; Shrestha, R. Engagement in harm reduction strategies after suspected fentanyl contamination among opioid-dependent individuals. J. Community Health 2021, 46, 349–357. [Google Scholar] [CrossRef]
- Wallace, B.; MacKinnon, K.; Strosher, H.; Macevicius, C.; Gordon, C.; Raworth, R.; Lacey, M.; Sana, S.; Lenora, M.; Karen, U.; et al. Equity-oriented frameworks to inform responses to opioid overdoses: A scoping review. JBI Evid. Synth. 2021, 19, 1760–1843. [Google Scholar] [CrossRef]
- Buxton, J.A.; Spearn, B.; Amlani, A.; Kuo, M.; Lysyshyn, M.; Young, S.; Purssell, R.; Papamihali, K.; Mill, C.; Shapiro, A. The British Columbia drug overdose and alert partnership: Interpreting and sharing timely illicit drug information to reduce harms. J. Community Saf. Well-Being 2019, 4, 4–9. [Google Scholar] [CrossRef]
- Deconinck, E.; Ait-Kaci, C.; Raes, A.; Canfyn, M.; Bothy, J.-L.; Duchateau, C.; Mees, C.; Braekeleer, K.; Gremaus, L.; Blanckaert, P. An infrared spectroscopic approach to characterise white powders, easily applicable in the context of drug checking, drug prevention and on-site analysis. Drug Test. Anal. 2021, 13, 679–693. [Google Scholar] [CrossRef] [PubMed]
- Ramsay, M.; Gozdzialski, L.; Larnder, A.; Wallace, B.; Hore, D. Fentanyl quantification using portable infrared absorption spectroscopy. A framework for community drug checking. Vib. Spectrosc. 2021, 114, 103243. [Google Scholar] [CrossRef]
- Ti, L.; Tobias, S.; Lysyshyn, M.; Laing, R.; Nosova, E.; Choi, J.; Arredondo, J.; McCrae, K.; Tupper, K.; Wood, E. Detecting fentanyl using point-of-care drug checking technologies: A validation study. Drug Alcohol Depend. 2020, 212, 108006. [Google Scholar] [CrossRef] [PubMed]
- Ti, L.; Tobias, S.; Maghsoudi, N.; Milloy, M.J.; McDonald, K.; Shapiro, A.; Beriault, D.; Stefan, C.; Lysyshyn, M.; Werb, D. Detection of synthetic cannabinoid adulteration in the unregulated drug supply in three Canadian settings. Drug Alcohol Rev. 2021, 40, 580–585. [Google Scholar] [CrossRef]
- Davies, N.; Guirguis, A. Introduction to the first Home Office-Licensed ‘Drug Checking’ Service: The SSA Talks to Dr. Amira Guirguis. Society for the study of Addiction, 9 July 2021. Available online: https://www.addiction-ssa.org/introduction-to-the-first-home-office-licensed-drug-checking-service-the-ssa-talks-to-dr-amira-guirguis/ (accessed on 4 August 2022).
- Gozdzialski, L.; Ramsay, M.; Larnder, A.; Wallace, B.; Hore, D.K. Fentanyl detection and quantification using portable Raman spectroscopy in community drug checking. J. Raman Spectrosc. 2021, 52, 1308–1316. [Google Scholar] [CrossRef]
- Schisler, C. New device That Tests Drugs in Minutes Boosted by Province Amid B.C.’s Overdose Crisis. Penisula News Review, 17 August 2021. Available online: https://www.peninsulanewsreview.com/news/new-device-that-tests-drugs-in-minutes-boosted-by-province-amid-b-c-s-overdose-crisis/ (accessed on 4 August 2022).
- McAuley, A.; Matheson, C.; Robertson, J.R. From the clinic to the street: The changing role of benzodiazepines in the Scottish overdose epidemic. Int. J. Drug Policy 2022, 100, 103512. [Google Scholar] [CrossRef]
- CBC Radio. How a New Drug-Checking Kit Could Turn Smartphones into Overdose Prevention Tools. CBC Radio, 1 August 2021. Available online: https://www.cbc.ca/radio/day6/anti-vax-propaganda-covering-climate-change-reducing-overdose-deaths-roger-bennett-s-ode-to-america-more-1.6123137/how-a-new-drug-checking-kit-could-turn-smartphones-into-overdose-prevention-tools-1.6123151 (accessed on 4 August 2022).
- Schneider, J.; Galettis, P.; Williams, M.; Lucas, C.; Martin, J.H. Pill testing at music festivals: Can we do more harm? Int. J. Med. 2016, 46, 1249–1251. [Google Scholar] [CrossRef]
- Scott, I.A.; Scott, R.J. Pill testing at music festivals: Is it evidence-based harm reduction? Int. J. Med. 2020, 50, 395–402. [Google Scholar] [CrossRef]
- Weatherston, J.; Perin, C.; Hore, D.; Wallace, B.; Storey, M.A. (Eds.) An unquantified uncertainty visualization design space during the opioid crisis. In Proceedings of the Extended Abstracts of the 2020 CHI Conference on Human Factors in Computing Systems, Honolulu, HI, USA, 25–30 April 2020. [Google Scholar] [CrossRef]
- Beaulieu, T.; Wood, E.; Tobias, S.; Lysyshyn, M.; Patel, P.; Matthews, J.; Ti, L. Is expected substance type associated with timing of drug checking service utilization?: A cross-sectional study. Harm Reduct. J. 2021, 18, 66. [Google Scholar] [CrossRef]
- Smit-Rigter, L.A.; Van der Gouwe, D. The neglected benefits of drug checking for harm reduction. Int. Med. J. 2020, 50, 1024. [Google Scholar] [CrossRef]
- Tissot, N. Promoting harm reduction personal strategies by means of drugs checking: Its use in CAARUD. In Psychotropic Drugs, Prevention and Harm Reduction; Elsevier: Amsterdam, The Netherlands, 2017; pp. 103–119. [Google Scholar] [CrossRef]
- Collins, A.B.; Boyd, J.; Mayer, S.; Fowler, A.; Kennedy, M.C.; Bluthenthal, R.N.; Kerr, T.; MCNeill, R. Policing space in the overdose crisis: A rapid ethnographic study of the impact of law enforcement practices on the effectiveness of overdose prevention sites. Int. J. Drug Policy 2019, 73, 199–207. [Google Scholar] [CrossRef] [PubMed]
- Butler, A.; Zakimi, N.; Greer, A. Total systems failure: Police officers’ perspectives on the impacts of the justice, health, and social service systems on people who use drugs. Harm Reduct. J. 2022, 19, 48. [Google Scholar] [CrossRef] [PubMed]
- Wallace, B.; Gozdzialski, L.; Qbaich, A.; Shafiul, A.; Burek, P.; Hutchison, A.; Taylor, T.; Louw, R.; Kielty, C.; Robinson, D.; et al. A distributed model to expand the reach of drug checking. Drugs Habits Soc. Pol. 2022; ahead of print. [Google Scholar] [CrossRef]


{kind=link}
| IPT Number | IPT Theme |
|---|---|
| 1 | Policing—service user point of view |
| 2 | Policing—police point of view |
| 3 | Affected family and service user involvement in implementation |
| 4 | Lived experience central to the service |
| 5 | Service users’ previous experience with substances |
| 6 | Existing drug market |
| 7 | Location of service |
| 8 | Integration into existing services |
| 9 | Community stigma |
| 10 | Existing relationships with service staff |
| 11 | Available equipment and expectations of tests |
| 12 | Reach of service |
| 13 | Existing level of drug-related harm |
| 14 | Focus of service (i.e., pill testing vs. other types of testing) |
| 15 | Individual differences of service users |
| Programme Theory Number and Name (Including Sub-Theories) |
|---|
| PT1: Legislation and regulation Sub-theory 1: Exemptions and service user risk Sub-theory 2: Exemptions and staff risk Sub-theory 3: Government and policing policy Sub-theory 4: On the ground policing practice |
| PT2: Existing drug market and level of drug-related harm |
| PT3: Integration into an existing service Sub-theory 1: Service staff point of view Sub-theory 2: Service user point of view |
| PT4: Lived/living experience at all levels |
| PT5: Accessibility |
| PT6: Testing process Sub-theory 1: Equipment and expertise availability Sub-theory 2: Service user expectations of DCS tests |
| PT7: Service users’ previous experience |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Masterton, W.; Falzon, D.; Burton, G.; Carver, H.; Wallace, B.; Aston, E.V.; Sumnall, H.; Measham, F.; Gittins, R.; Craik, V.; et al. A Realist Review of How Community-Based Drug Checking Services Could Be Designed and Implemented to Promote Engagement of People Who Use Drugs. Int. J. Environ. Res. Public Health 2022, 19, 11960. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph191911960
Masterton W, Falzon D, Burton G, Carver H, Wallace B, Aston EV, Sumnall H, Measham F, Gittins R, Craik V, et al. A Realist Review of How Community-Based Drug Checking Services Could Be Designed and Implemented to Promote Engagement of People Who Use Drugs. International Journal of Environmental Research and Public Health. 2022; 19(19):11960. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph191911960
Chicago/Turabian StyleMasterton, Wendy, Danilo Falzon, Gillian Burton, Hannah Carver, Bruce Wallace, Elizabeth V. Aston, Harry Sumnall, Fiona Measham, Rosalind Gittins, Vicki Craik, and et al. 2022. "A Realist Review of How Community-Based Drug Checking Services Could Be Designed and Implemented to Promote Engagement of People Who Use Drugs" International Journal of Environmental Research and Public Health 19, no. 19: 11960. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph191911960