Predictive Value of Decoy Receptor 3 in Postoperative Nosocomial Bacterial Meningitis

Abstract
:1. Introduction
2. Results and Discussion
2.1. Clinical and Biological Characteristics of Patients

{kind=link}
{kind=link}
| Characteristics | Non-Bacterial Meningitis (n = 43) | Bacterial Meningitis (n = 80) | p Value |
|---|---|---|---|
| Age (years) | 42.02 ± 13.90 | 43.75 ± 16.46 | 0.560 a |
| Gender, n (%) | 0.141 b | ||
| Male | 25 (58.12) | 57 (71.25) | |
| Female | 18 (41.88) | 23 (28.75) | |
| Receiving Steroid >24 h before CSF Sampling | 12 (27.91) | 27 (33.75) | 0.507 b |
| Receiving Antibiotic >24 h before CSF Sampling | 5 (11.63) | 39 (48.75) | <0.001 b |
| Hypertension n (%) | 7 (16.27) | 16 (20.00) | 0.614 b |
| Diabetes n (%) | 3 (6.98) | 6 (7.50) | 1.000 c |
| Leucocyte Count (×106/L) | 4.00 (2.00–36.00) | 765.00 (265.25–1976.00) | <0.001 d |
| Glucose (mmol/L) | 2.74 (1.59–3.20) | 1.59 (0.72–2.58) | <0.001 d |
| Protein (g/L) | 0.45 (0.17–0.79) | 0.82 (0.37–1.80) | 0.003 d |
| Lactate (mmol/L) | 1.73 (1.11–2.82) | 3.23 (1.87–6.42) | <0.001 d |
| DcR3 (ng/mL) | 0 (0–0.192) | 0.646 (0.229–1.514) | <0.001 d |
2.2. Levels of Decoy Receptor 3 (DcR3) in Patients according to Various Criteria

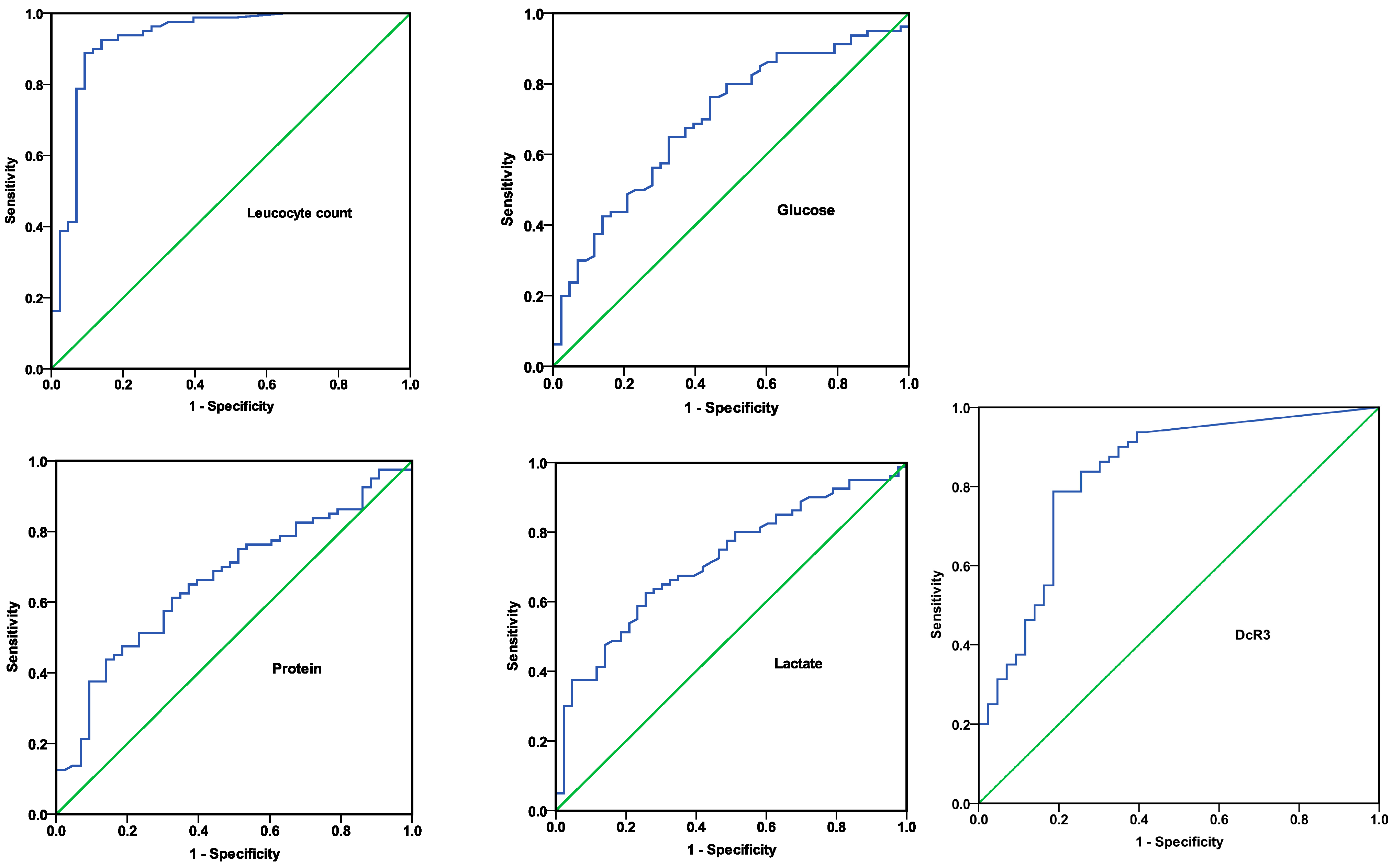
2.3. Accuracy of DcR3 and Different Cerebrospinal Fluid (CSF) Markers in Diagnosing Bacterial Meningitis

| Variable | Cut-off Value | Sensitivity (%) | Specificity (%) | PLR | NLR | PPV (%) | NPV (%) |
|---|---|---|---|---|---|---|---|
| Leucocyte count | 116 (×106/L) | 88.75 (79.24–94.41) | 90.70 (76.95–96.98) | 9.54 (3.74–24.34) | 0.12 (0.07–0.23) | 94.67 (86.19–98.28) | 81.25 (66.90–90.56) |
| Glucose | 2.14 (mmol/L) | 65.00 (53.44–75.10) | 67.44 (51.34–80.46) | 2.00 (1.26–3.16) | 0.52 (0.38–0.72) | 78.79 (66.66–87.52) | 50.88 (37.44–64.20) |
| Protein | 1.14 (g/L) | 43.75 (32.83–55.27) | 86.05 (71.37–94.20) | 3.14 (1.43–6.86) | 0.65 (0.53–0.80) | 85.37 (70.14–93.91) | 45.12 (34.24–56.46) |
| Lactate | 2.64 (mmol/L) | 62.50 (50.92–72.87) | 74.42 (58.53–85.96) | 2.44 (1.43–4.18) | 0.50 (0.37–0.68) | 81.97 (69.60–90.24) | 51.61 (38.68–64.34) |
| DcR3 | 0.201 (ng/mL) | 78.75 (67.89–86.79) | 81.40 (66.08–91.08) | 4.23 (2.24–7.99) | 0.26 (0.17–0.40) | 88.73 (78.47–94.66) | 67.31 (52.78–79.28) |
| Variable | Coefficient | SE | p Value | OR (95% CI) | Chi Square |
|---|---|---|---|---|---|
| Glucose | −0.35 | 0.18 | 0.047 | 0.70 (0.50–1.00) | 15.83 |
| Protein | 0.62 | 0.29 | 0.034 | 1.85 (1.05–3.28) | |
| DcR3 | 1.79 | 0.53 | 0.001 | 5.97 (2.13–16.73) |
2.4. Correlation between Age/CSF Parameters and DcR3 Levels
| Variable 1 | Variable 2 | Spearman’s Rho | p Value |
|---|---|---|---|
| DcR3 | Leucocyte count | 0.696 | <0.001 |
| Glucose | −0.384 | <0.001 | |
| Protein | 0.296 | 0.001 | |
| Lactate | 0.513 | <0.001 | |
| Age | 0.024 | 0.795 |
2.5. Discussion
3. Experimental Section
3.1. Patients and Data Collection
3.2. Detection of DcR3
3.3. Statistical Analysis
4. Conclusions
Acknowledgments
Author Contributions
Conflicts of Interest
References
- Van de Beek, D.; Drake, J.M.; Tunkel, A.R. Nosocomial bacterial meningitis. N. Engl. J. Med. 2010, 362, 146–154. [Google Scholar]
- Wang, K.W.; Chang, W.N.; Huang, C.R.; Tsai, N.W.; Tsui, H.W.; Wang, H.C.; Su, T.M.; Rau, C.S.; Cheng, B.C.; Chang, C.S.; et al. Post-neurosurgical nosocomial bacterial meningitis in adults: Microbiology, clinical features and outcomes. J. Clin. Neurosci. 2005, 12, 647–650. [Google Scholar]
- Erdem, I.; Hakan, T.; Ceran, N.; Metin, F.; Akcay, S.S.; Kucukercan, M.; Berkman, M.Z.; Goktas, P. Clinical features, laboratory data, management and the risk factors that affect the mortality in patients with postoperative meningitis. Neurol. India 2008, 56, 433–437. [Google Scholar] [CrossRef] [PubMed]
- Aronin, S.I.; Peduzzi, P.; Quagliarello, V.J. Community-acquired bacterial meningitis: Risk stratification for adverse clinical outcome and effect of antibiotic timing. Ann. Intern. Med. 1998, 129, 862–869. [Google Scholar] [CrossRef] [PubMed]
- Filka, J.; Huttova, M.; Kurak, J.; Tuharsky, J.; Kralinsky, K.; Sagat, T.; Krcmery, J.V.V. Inappropriately treated nosocomial meningitis is associated with higher mortality and more neurologic sequellae than appropriately treated meningitis. J. Infect. Chemother. 1999, 5, 108–109. [Google Scholar] [CrossRef] [PubMed]
- Mwangi, I.; Berkley, J.; Lowe, B.; Peshu, N.; Marsh, K.; Newton, C.R. Acute bacterial meningitis in children admitted to a rural Kenyan hospital: Increasing antibiotic resistance and outcome. Pediatr. Infect. Dis. J. 2002, 21, 1042–1048. [Google Scholar] [CrossRef] [PubMed]
- Pitti, R.M.; Marsters, S.A.; Lawrence, D.A.; Roy, M.; Kischkel, F.C.; Dowd, P.; Huang, A.; Donahue, C.J.; Sherwood, S.W.; Baldwin, D.T.; et al. Genomic amplification of a decoy receptor for Fas ligand in lung and colon cancer. Nature 1998, 396, 699–703. [Google Scholar]
- Hou, Y.Q.; Xu, P.; Zhang, M.; Han, D.; Peng, L.; Liang, D.Y.; Yang, S.; Zhang, Z.; Hong, J.; Lou, X.L.; et al. Serum decoy receptor 3, a potential new biomarker for sepsis. Clin. Chim. Acta 2012, 413, 744–748. [Google Scholar]
- Kim, S.; Mi, L.; Zhang, L. Specific elevation of DcR3 in sera of sepsis patients and its potential role as a clinically important biomarker of sepsis. Diagn. Microbiol. Infect. Dis. 2012, 73, 312–317. [Google Scholar] [CrossRef]
- Chen, C.Y.; Yang, K.Y.; Chen, M.Y.; Chen, H.Y.; Lin, M.T.; Lee, Y.C.; Perng, R.P.; Hsieh, S.L.; Yang, P.C.; Chou, T.Y. Decoy receptor 3 levels in peripheral blood predict outcomes of acute respiratory distress syndrome. Am. J. Respir. Crit. Care Med. 2009, 180, 751–760. [Google Scholar] [CrossRef] [PubMed]
- Hayashi, S.; Miura, Y.; Tateishi, K.; Takahashi, M.; Kurosaka, M. Decoy receptor 3 is highly expressed in patients with rheumatoid arthritis. Mod. Rheumatol. 2010, 20, 63–68. [Google Scholar] [CrossRef] [PubMed]
- Kim, S.; McAuliffe, W.J.; Zaritskaya, L.S.; Moore, P.A.; Zhang, L.; Nardelli, B. Selective induction of tumor necrosis receptor factor 6/decoy receptor 3 release by bacterial antigens in human monocytes and myeloid dendritic cells. Infect. Immun. 2004, 72, 89–93. [Google Scholar] [CrossRef] [PubMed]
- Lin, W.W.; Hsieh, S.L. Decoy receptor 3: A pleiotropic immunomodulator and biomarker for inflammatory diseases, autoimmune diseases and cancer. Biochem. Pharmacol. 2011, 81, 838–847. [Google Scholar] [CrossRef] [PubMed]
- Mueller, A.M.; Pedre, X.; Killian, S.; David, M.; Steinbrecher, A. The Decoy Receptor 3 (DcR3, TNFRSF6B) suppresses Th17 immune responses and is abundant in human cerebrospinal fluid. J. Neuroimmunol. 2009, 209, 57–64. [Google Scholar] [CrossRef] [PubMed]
- Yang, C.R.; Hsieh, S.L.; Ho, F.M.; Lin, W.W. Decoy receptor 3 increases monocyte adhesion to endothelial cells via NF-κB-dependent up-regulation of intercellular adhesion molecule-1, VCAM-1 and IL-8 expression. J. Immunol. 2005, 174, 1647–1656. [Google Scholar] [CrossRef] [PubMed]
- Hsu, M.J.; Lin, W.W.; Tsao, W.C.; Chang, Y.C.; Hsu, T.L.; Chiu, A.W.; Chio, C.C.; Hsieh, S.L. Enhanced adhesion of monocytes via reverse signaling triggered by decoy receptor 3. Exp. Cell Res. 2004, 292, 241–251. [Google Scholar] [CrossRef] [PubMed]
- Neal, J.W.; Gasque, P. How does the brain limit the severity of inflammation and tissue injury during bacterial meningitis. J. Neuropathol. Exp. Neurol. 2013, 72, 370–385. [Google Scholar] [CrossRef] [PubMed]
- Funke, B.; Autschbach, F.; Kim, S.; Lasitschka, F.; Strauch, U.; Rogler, G.; Gdynia, G.; Li, L.; Gretz, N.; Macher-Goeppinger, S.; et al. Functional characterisation of decoy receptor 3 in Crohn’s disease. Gut 2009, 58, 483–491. [Google Scholar]
- Hung, S.C.; Hsu, T.W.; Lin, Y.P.; Tarng, D.C. Decoy receptor 3, a novel inflammatory marker and mortality in hemodialysis patients. Clin. J. Am. Soc. Nephrol. 2012, 7, 1257–1265. [Google Scholar] [CrossRef] [PubMed]
- Otsuki, T.; Tomokuni, A.; Sakaguchi, H.; Aikoh, T.; Matsuki, T.; Isozaki, Y.; Hyodoh, F.; Ueki, H.; Kusaka, M.; Kita, S.; et al. Over-expression of the decoy receptor 3 (DcR3) gene in peripheral blood mononuclear cells (PBMC) derived from silicosis patients. Clin. Exp. Immunol. 2000, 119, 323–327. [Google Scholar]
- Fayad, R.; Brand, M.I.; Stone, D.; Keshavarzian, A.; Qiao, L. Apoptosis resistance in ulcerative colitis: High expression of decoy receptors by lamina propria T cells. Eur. J. Immunol. 2006, 36, 2215–2222. [Google Scholar] [CrossRef] [PubMed]
- Jereb, M.; Muzlovic, I.; Hojker, S.; Strle, F. Predictive value of serum and cerebrospinal fluid procalcitonin levels for the diagnosis of bacterial meningitis. Infection 2001, 29, 209–212. [Google Scholar] [CrossRef] [PubMed]
- Malla, K.K.; Malla, T.; Rao, K.S.; Basnet, S.; Shah, R. Is cerebrospinal fluid C-reactive protein a better tool than blood C-reactive protein in laboratory diagnosis of meningitis in children. Sultan Qaboos Univ. Med. J. 2013, 13, 93–99. [Google Scholar] [CrossRef] [PubMed]
- Van de Beek, D.; de Gans, J.; Spanjaard, L.; Weisfelt, M.; Reitsma, J.B.; Vermeulen, M. Clinical features and prognostic factors in adults with bacterial meningitis. N. Engl. J. Med. 2004, 351, 1849–1859. [Google Scholar] [CrossRef] [PubMed]
© 2014 by the authors; licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Liu, Y.-J.; Shao, L.-H.; Wang, Q.; Zhang, J.; Ma, R.-P.; Liu, H.-H.; Dong, X.-M.; Ma, L.-X. Predictive Value of Decoy Receptor 3 in Postoperative Nosocomial Bacterial Meningitis. Int. J. Mol. Sci. 2014, 15, 19962-19970. https://0-doi-org.brum.beds.ac.uk/10.3390/ijms151119962
Liu Y-J, Shao L-H, Wang Q, Zhang J, Ma R-P, Liu H-H, Dong X-M, Ma L-X. Predictive Value of Decoy Receptor 3 in Postoperative Nosocomial Bacterial Meningitis. International Journal of Molecular Sciences. 2014; 15(11):19962-19970. https://0-doi-org.brum.beds.ac.uk/10.3390/ijms151119962
Chicago/Turabian StyleLiu, Yong-Juan, Li-Hua Shao, Qian Wang, Jian Zhang, Rui-Ping Ma, Hai-Hong Liu, Xiao-Meng Dong, and Li-Xian Ma. 2014. "Predictive Value of Decoy Receptor 3 in Postoperative Nosocomial Bacterial Meningitis" International Journal of Molecular Sciences 15, no. 11: 19962-19970. https://0-doi-org.brum.beds.ac.uk/10.3390/ijms151119962