
Targeting Angiogenesis in Biliary Tract Cancers: An Open Option

 ,
,  , , , and
, , , and
Abstract
:1. Introduction
2. BTC-Associated Angiogenesis and Lymphangiogenesis: From Pathological Features to Genic Regulation
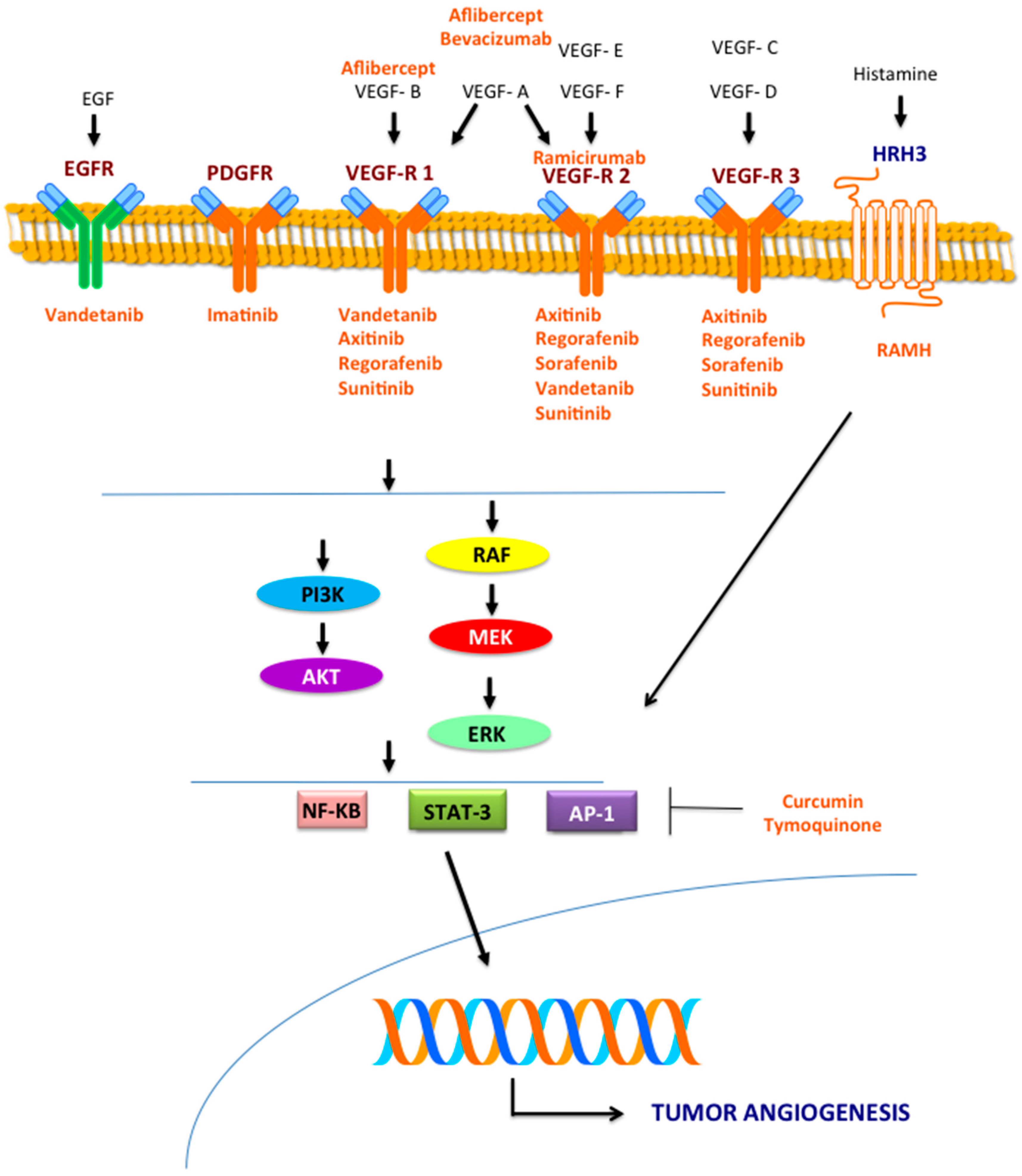
3. Molecular Pathways Involved in Angiogenesis
3.1. VEGF Pathway
3.2. MEK/ERK Pathway
3.3. Other Signaling Pathways
4. Preclinical Studies
4.1. Targeting the VEGF Pathway
4.2. Targeting the MEK/ERK Pathway
4.3. Other Drugs
5. Clinical Studies in BTC Patients: Is There a Chance for a Phase III Trial?
5.1. Bevacizumab
5.2. Ramucirumab
5.3. Aflibercept
5.4. Sorafenib
5.5. Vandetanib
5.6. Cediranib
5.7. Sunitinib
5.8. Regorafenib
5.9. Selumetinib
5.10. Phase III Trials
6. Conclusions
Conflicts of Interest
References
- Valle, J.W.; Borbath, I.; Khan, S.A.; Huguet, F.; Gruenberger, T.; Arnold, D.; ESMO Guidelines Committee. Biliary cancer: ESMO Clinical Practice Guidelines for diagnosis, treatment and follow-up. Ann. Oncol. 2016, 27, v28–v37. [Google Scholar] [CrossRef] [PubMed]
- Blechacz, B.; Komuta, M.; Roskams, T.; Gores, G.J. Clinical diagnosis and staging of cholangiocarcinoma. Nat. Rev. Gastroenterol. Hepatol. 2011, 8, 512–522. [Google Scholar] [CrossRef] [PubMed]
- Bridgewater, J.; Galle, P.R.; Khan, S.A.; Llovet, J.M.; Park, J.W.; Patel, T.; Pawlik, T.M.; Gores, G.J. Guidelines for the diagnosis and management of intrahepatic cholangiocarcinoma. J. Hepatol. 2014, 60, 1268–1289. [Google Scholar] [CrossRef] [PubMed]
- Blechacz, B. Cholangiocarcinoma: Current Knowledge and New Developments. Gut Liver 2017, 11, 13–26. [Google Scholar] [CrossRef] [PubMed]
- Khan, S.A.; Davidson, B.R.; Goldin, R.D.; Heaton, N.; Karani, J.; Pereira, S.P.; Rosenberg, W.M.; Tait, P.; Taylor-Robinson, S.D.; Thillainayagam, A.V.; et al. Guidelines for the diagnosis and treatment of cholangiocarcinoma: An update. Gut 2012, 61, 1657–1669. [Google Scholar] [CrossRef] [PubMed]
- Howlader, N.; Noone, A.M.; Krapcho, M.; Miller, D.; Bishop, K.; Altekruse, S.F.; Kosary, C.L.; Yu, M.; Ruhl, J.; Tatalovich, Z.; et al. (Eds.) SEER Cancer Statistics Review, 1975–2013, National Cancer Institute. Bethesda, MD, Based on November 2015 SEER Data Submission, Posted to the SEER Web Site; April 2016. Available online: http://seer.cancer.gov/csr/1975_2013/ (accessed on 10 December 2016).
- Valle, J.; Wasan, H.; Palmer, D.H.; Cunningham, D.; Anthoney, A.; Maraveyas, A.; Madhusudan, S.; Iveson, T.; Hughes, S.; Pereira, S.P.; et al. ABC-02 Trial Investigators. Cisplatin plus gemcitabine versus gemcitabine for biliary tract cancer. N. Engl. J. Med. 2010, 362, 1273–1281. [Google Scholar] [CrossRef] [PubMed]
- Fornaro, L.; Vivaldi, C.; Cereda, S.; Leone, F.; Aprile, G.; Lonardi, S.; Silvestris, N.; Santini, D.; Milella, M.; Caparello, C.; et al. GICO group (Gruppo Italiano COlangiocarcinoma). Second-line chemotherapy in advanced biliary cancer progressed to first-line platinum-gemcitabine combination: A multicenter survey and pooled analysis with published data. J. Exp. Clin. Cancer Res. 2015, 34, 156. [Google Scholar] [CrossRef] [PubMed]
- Yoon, J.H.; Canbay, A.E.; Werneburg, N.W.; Lee, S.P.; Gores, G.J. Oxysterols induce cyclooxygenase-2 expression in cholangiocytes: Implications for biliary tract carcinogenesis. Hepatology 2004, 39, 732–738. [Google Scholar] [CrossRef] [PubMed]
- Jaiswal, M.; LaRusso, N.F.; Gores, G.J. Nitric oxide in gastrointestinal epithelial cell carcinogenesis: Linking inflammation to oncogenesis. Am. J. Physiol. Gastrointest. Liver Physiol. 2001, 281, G626–G634. [Google Scholar] [PubMed]
- Leyva-Illades, D.; McMillin, M.; Quinn, M.; Demorrow, S. Cholangiocarcinoma pathogenesis: Role of the tumor microenvironment. Transl. Gastrointest. Cancer 2012, 1, 71–80. [Google Scholar] [PubMed]
- Hasita, H.; Komohara, Y.; Okabe, H.; Masuda, T.; Ohnishi, K.; Lei, X.F.; Beppu, T.; Baba, H.; Takeya, M. Significance of alternatively activated macrophages in patients with intrahepatic cholangiocarcinoma. Cancer Sci. 2010, 101, 1913–1919. [Google Scholar] [CrossRef] [PubMed]
- Bergers, G.; Benjamin, L.E. Tumorigenesis and the angiogenic switch. Nat. Rev. Cancer 2003, 3, 401–410. [Google Scholar] [CrossRef] [PubMed]
- Rmali, K.A.; Puntis, M.C.; Jiang, W.G. Tumour-associated angiogenesis in human colorectal cancer. Colorectal Dis. 2007, 9, 3–14. [Google Scholar] [CrossRef] [PubMed]
- Barzi, A.; Thara, E. Angiogenesis in esophageal and gastric cancer: A paradigm shift in treatment. Exp. Opin. Biol. Ther. 2014, 14, 1319–1332. [Google Scholar] [CrossRef] [PubMed]
- Zhu, A.X.; Duda, D.G.; Sahani, D.V.; Jain, R.K. HCC and angiogenesis: Possible targets and future directions. Nat. Rev. Clin. Oncol. 2011, 8, 292–301. [Google Scholar] [CrossRef] [PubMed]
- Fujimoto, K.; Hosotani, R.; Wada, M.; Lee, J.U.; Koshiba, T.; Miyamoto, Y.; Tsuji, S.; Nakajima, S.; Doi, R.; Imamura, M. Expression of two angiogenic factors, vascular endothelial growth factor and platelet-derived endothelial cell growth factor in human pancreatic cancer, and its relationship to angiogenesis. Eur. J. Cancer 1998, 34, 1439–1447. [Google Scholar] [CrossRef]
- Chen, Y.; Chen, Y.; Yu, G.; Ding, H. Lymphangiogenic and angiogentic microvessel density in gallbladder carcinoma. Hepatogastroenterology 2011, 58, 20–25. [Google Scholar] [PubMed]
- Thelen, A.; Scholz, A.; Weichert, W.; Wiedenmann, B.; Neuhaus, P.; Gessner, R.; Benckert, C.; Jonas, S. Tumor-associated angiogenesis and lymphangiogenesis correlate with progression of intrahepatic cholangiocarcinoma. Am. J. Gastroenterol. 2010, 105, 1123–1132. [Google Scholar] [CrossRef] [PubMed]
- Thelen, A.; Scholz, A.; Benckert, C.; Schröder, M.; Weichert, W.; Wiedenmann, B.; Neuhaus, P.; Jonas, S. Microvessel density correlates with lymph node metastases and prognosis in hilar cholangiocarcinoma. J. Gastroenterol. 2008, 43, 959–966. [Google Scholar] [CrossRef] [PubMed]
- Tang, D.; Nagano, H.; Yamamoto, H.; Wada, H.; Nakamura, M.; Kondo, M.; Ota, H.; Yoshioka, S.; Kato, H.; Damdinsuren, B.; et al. Angiogenesis in cholangiocellular carcinoma: Expression of vascular endothelial growth factor, angiopoietin-1/2, thrombospondin-1 and clinicopathological significance. Oncol. Rep. 2006, 15, 525–532. [Google Scholar] [CrossRef] [PubMed]
- Yoshikawa, D.; Ojima, H.; Iwasaki, M.; Hiraoka, N.; Kosuge, T.; Kasai, S.; Hirohashi, S.; Shibata, T. Clinicopathological and prognostic significance of EGFR, VEGF, and HER2 expression in cholangiocarcinoma. Br. J. Cancer 2008, 98, 418–425. [Google Scholar] [CrossRef] [PubMed]
- Guedj, N.; Zhan, Q.; Perigny, M.; Rautou, P.E.; Degos, F.; Belghiti, J.; Farges, O.; Bedossa, P.; Paradis, V. Comparative protein expression profiles of hilar and peripheral hepatic cholangiocarcinomas. J. Hepatol. 2009, 51, 93–101. [Google Scholar] [CrossRef] [PubMed]
- Hida, Y.; Morita, T.; Fujita, M.; Miyasaka, Y.; Horita, S.; Fujioka, Y.; Miyasaka, Y.; Horita, S.; Fujioka, Y.; Nagashima, K.; et al. Vascular endothelial growth factor expression is an independent negative predictor in extrahepatic biliary tract carcinomas. Anticancer Res. 1999, 19, 2257–2260. [Google Scholar] [PubMed]
- Giatromanolaki, A.; Koukourakis, M.I.; Simopoulos, C.; Polychronidis, A.; Sivridis, E. Vascular endothelial growth factor (VEGF) expression in operable gallbladder carcinomas. Eur. J. Surg. Oncol. 2003, 29, 879–883. [Google Scholar] [CrossRef] [PubMed]
- Harino, Y.; Imura, S.; Kanemura, H.; Morine, Y.; Fujii, M.; Ikegami, T.; Uehara, H.; Shimada, M. Role of tumor angiogenesis in gallbladder carcinoma: With special reference to thymidine phosphorylase. Int. J. Clin. Oncol. 2008, 13, 452–457. [Google Scholar] [CrossRef] [PubMed]
- Sun, X.N.; Cao, W.G.; Wang, X.; Wang, Q.; Gu, B.X.; Yang, Q.C.; Hu, J.B.; Liu, H.; Zheng, S. Prognostic impact of vascular endothelial growth factor-A expression in resected gallbladder carcinoma. Tumour. Biol. 2011, 32, 1183–1190. [Google Scholar] [CrossRef] [PubMed]
- Wiggers, J.K.; Ruys, A.T.; Groot Koerkamp, B.; Beuers, U.; Ten Kate, F.J.; van Gulik, T.M. Differences in immunohistochemical biomarkers between intra- and extrahepatic cholangiocarcinoma: A systematic review and meta-analysis. J. Gastroenterol. Hepatol. 2014, 29, 1582–1594. [Google Scholar] [CrossRef] [PubMed]
- Vidal-Vanaclocha, F. The prometastatic microenvironment of the liver. Cancer Microenviron. 2008, 1, 113–129. [Google Scholar] [CrossRef] [PubMed]
- Sica, A. Role of tumour-associated macrophages in cancer-related inflammation. Exp. Oncol. 2010, 32, 153–158. [Google Scholar] [PubMed]
- Mantovani, A.; Sozzani, S.; Locati, M.; Allavena, P.; Sica, A. Macrophage polarization: Tumor-associated macrophagesas a paradigm for polarized M2 mononuclear phagocytes. Trends Immunol. 2002, 23, 549–555. [Google Scholar] [CrossRef]
- Sun, T.; Yang, Y.; Luo, X.; Cheng, Y.; Zhang, M.; Wang, K.; Ge, C. Inhibition of tumor angiogenesis by interferon-γ by suppression of tumor-associated macrophage differentiation. Oncol. Res. 2014, 21, 227–235. [Google Scholar] [CrossRef] [PubMed]
- Lin, W.; Jiang, L.; Chen, Y.; She, F.; Han, S.; Zhu, J.; Zhou, L.; Tang, N.; Wang, X.; Li, X. Vascular endothelial growth factor-D promotes growth, lymphangiogenesis and lymphatic metastasis in gallbladder cancer. Cancer Lett. 2012, 314, 127–136. [Google Scholar] [CrossRef] [PubMed]
- Jiang, L.; Chen, Y.L.; She, F.F.; Tang, N.H.; Li, X.J.; Wang, X.X. Expressions of VEGF-C and VEGF-D and their correlation with lymphangiogenesis and angiogenesis in gallbladder carcinoma. Zhonghua Zhong Liu Za Zhi 2010, 32, 190–195. [Google Scholar] [PubMed]
- Du, Q.; Jiang, L.; Wang, X.; Wang, M.; She, F.; Chen, Y. Tumor necrosis factor-α promotes the lymphangiogenesis of gallbladder carcinoma through nuclear factor-κB-mediated upregulation of vascular endothelial growth factor-C. Cancer Sci. 2014, 105, 1261–1271. [Google Scholar] [CrossRef] [PubMed]
- Nakashima, T.; Kondoh, S.; Kitoh, H.; Ozawa, H.; Okita, S.; Harada, T.; Shiraishi, K.; Ryozawa, S.; Okita, K. Vascular endothelial growth factor-C expression in human gallbladder cancer and its relationship to lymph node metastasis. Int. J. Mol. Med. 2003, 11, 33–39. [Google Scholar] [CrossRef] [PubMed]
- Voigtländer, T.; David, S.; Thamm, K.; Schlué, J.; Metzger, J.; Manns, M.P.; Lankisch, T.O. Angiopoietin-2 and biliary diseases: Elevated serum, but not bile levels are associated with cholangiocarcinoma. PLoS ONE 2014, 9, e97046. [Google Scholar] [CrossRef] [PubMed]
- Boonjaraspinyo, S.; Boonmars, T.; Wu, Z.; Loilome, W.; Sithithaworn, P.; Nagano, I.; Pinlaor, S.; Yongvanit, P.; Nielsen, P.S.; Pairojkul, C.; et al. Platelet-derived growth factor may be a potential diagnostic and prognostic marker for cholangiocarcinoma. Tumour. Biol. 2012, 33, 1785–1802. [Google Scholar] [CrossRef] [PubMed]
- Cadamuro, M.; Nardo, G.; Indraccolo, S.; Dall’olmo, L.; Sambado, L.; Moserle, L.; Franceschet, I.; Colledan, M.; Massani, M.; Stecca, T.; et al. Platelet-derived growth factor-D and Rho GTPases regulate recruitment of cancer-associated fibroblasts in cholangiocarcinoma. Hepatology 2013, 58, 1042–1053. [Google Scholar] [CrossRef] [PubMed]
- Wang, Z.; Yan, X. CD146, a multi-functional molecule beyond adhesion. Cancer Lett. 2013, 330, 150–162. [Google Scholar] [CrossRef] [PubMed]
- Wang, W.; Yang, Z.L.; Liu, J.Q.; Jiang, S.; Miao, X.Y. Identification of CD146 expression, angiogenesis, and lymphangiogenesis as progression, metastasis, and poor-prognosis related markers for gallbladder adenocarcinoma. Tumour. Biol. 2012, 33, 173–182. [Google Scholar] [CrossRef] [PubMed]
- Nakamura, H.; Arai, Y.; Totoki, Y.; Shirota, T.; Elzawahry, A.; Kato, M.; Hama, N.; Hosoda, F.; Urushidate, T.; Ohashi, S.; et al. Genomic spectra of biliary tract cancer. Nat. Genet. 2015, 47, 1003–1010. [Google Scholar] [CrossRef] [PubMed]
- Presta, M.; Dell’Era, P.; Mitola, S.; Moroni, E.; Ronca, R.; Rusnati, M. Fibroblast growth factor/fibroblast growth factor receptor system in angiogenesis. Cytokine Growth Factor Rev. 2005, 16, 159–178. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chan-On, W.; Nairismägi, M.L.; Ong, C.K.; Lim, W.K.; Dima, S.; Pairojkul, C.; Lim, K.H.; McPherson, J.R.; Cutcutache, I.; Heng, H.L.; et al. Exome sequencing identifies distinct mutational patterns in liver fluke-related and non-infection-related bile duct cancers. Nat. Genet. 2013, 45, 1474–1478. [Google Scholar] [CrossRef] [PubMed]
- Andersen, J.B.; Spee, B.; Blechacz, B.R.; Avital, I.; Komuta, M.; Barbour, A.; Conner, E.A.; Gillen, M.C.; Roskams, T.; Roberts, L.R.; et al. Genomic and genetic characterization of cholangiocarcinoma identifies therapeutic targets for tyrosine kinase inhibitors. Gastroenterology 2012, 142, 1021.e15–1031.e15. [Google Scholar] [CrossRef] [PubMed]
- Ong, C.K.; Subimerb, C.; Pairojkul, C.; Wongkham, S.; Cutcutache, I.; Yu, W.; McPherson, J.R.; Allen, G.E.; Ng, C.C.; Wong, B.H.; et al. Exome sequencing of liver fluke-associated cholangiocarcinoma. Nat. Genet. 2012, 44, 690–693. [Google Scholar] [CrossRef] [PubMed]
- Sia, D.; Hoshida, Y.; Villanueva, A.; Roayaie, S.; Ferrer, J.; Tabak, B.; Peix, J.; Sole, M.; Tovar, V.; Alsinet, C.; et al. Integrative molecular analysis of intrahepatic cholangiocarcinoma reveals 2 classes that have different outcomes. Gastroenterology 2013, 144, 829–840. [Google Scholar] [CrossRef] [PubMed]
- Cheng, Q.; Feng, F.; Zhu, L.; Zheng, Y.; Luo, X.; Liu, C.; Yi, B.; Jiang, X. Circulating miR-106a is a Novel Prognostic and Lymph Node Metastasis Indicator for Cholangiocarcinoma. Sci. Rep. 2015, 5, 16103. [Google Scholar] [CrossRef] [PubMed]
- Li, J.; Gao, B.; Huang, Z.; Duan, T.; Li, D.; Zhang, S.; Zhao, Y.; Liu, L.; Wang, Q.; Chen, Z.; et al. Prognostic significance of microRNA-203 in cholangiocarcinoma. Int. J. Clin. Exp. Pathol. 2015, 8, 9512–9516. [Google Scholar] [PubMed]
- Zhang, J.; Han, C.; Zhu, H.; Song, K.; Wu, T. miR-101 inhibits cholangiocarcinoma angiogenesis through targeting vascular endothelial growth factor (VEGF). Am. J. Pathol. 2013, 182, 1629–1639. [Google Scholar] [CrossRef] [PubMed]
- Fukumura, D.; Xavier, R.; Sugiura, T.; Chen, Y.; Park, E.C.; Lu, N.; Selig, M.; Nielsen, G.; Taksir, T.; Jain, R.K.; et al. Tumor induction of VEGF promoter activity in stromal cells. Cell 1998, 94, 715–725. [Google Scholar] [CrossRef]
- Ferrara, N. Vascular endothelial growth factor: Basic science and clinical progress. Endocr. Rev. 2004, 25, 581–611. [Google Scholar] [CrossRef] [PubMed]
- Takahashi, T.; Ueno, H.; Shibuya, M. VEGF activates protein kinase C-dependent, but Ras-independent Raf-MEK-MAP kinase pathway for DNA synthesis in primary endothelial cells. Oncogene 1999, 18, 2221–2230. [Google Scholar] [CrossRef] [PubMed]
- Meadows, K.N.; Bryant, P.; Pumiglia, K. Vascular endothelial growth factor induction of the angiogenic phenotype requires Ras activation. J. Biol. Chem. 2001, 276, 49289–49298. [Google Scholar] [CrossRef] [PubMed]
- Gerber, H.P.; McMurtrey, A.; Kowalski, J.; Yan, M.; Keyt, B.A.; Dixit, V.; Ferrara, N. Vascular endothelial growth factor regulates endothelial cell survival through the phosphatidylinositol 3′-kinase/Akt signal transduction pathway. Requirement for Flk-1/KDR activation. J. Biol. Chem. 1998, 273, 30336–30343. [Google Scholar] [CrossRef] [PubMed]
- Masoud, G.N.; Li, W. HIF-1α pathway: Role, regulation and intervention for cancer therapy. Acta Pharm. Sin. B 2015, 5, 378–389. [Google Scholar] [CrossRef] [PubMed]
- Marti, P.; Stein, C.; Blumer, T.; Abraham, Y.; Dill, M.T.; Pikiolek, M.; Orsini, V.; Jurisic, G.; Megel, P.; Makowska, Z.; et al. YAP promotes proliferation, chemoresistance, and angiogenesis in human cholangiocarcinoma through TEAD transcription factors. Hepatology 2015, 62, 1497–1510. [Google Scholar] [CrossRef] [PubMed]
- Niu, G.; Wright, K.L.; Huang, M.; Song, L.; Haura, E.; Turkson, J.; Zhang, S.; Wang, T.; Sinibaldi, D.; Coppola, D.; et al. Constitutive Stat3 activity up-regulates VEGF expression and tumor angiogenesis. Oncogene 2002, 21, 2000–2008. [Google Scholar] [CrossRef] [PubMed]
- Aggarwal, B.B. Nuclear factor-κB: The enemy within. Cancer Cell 2004, 6, 203–208. [Google Scholar] [CrossRef] [PubMed]
- Kennedy, L.; Hodges, K.; Meng, F.; Alpini, G.; Francis, H. Histamine and histamine receptor regulation of gastrointestinal cancers. Transl. Gastrointest. Cancer 2012, 1, 215–227. [Google Scholar] [PubMed]
- Vaeteewoottacharn, K.; Kariya, R.; Dana, P.; Fujikawa, S.; Matsuda, K.; Ohkuma, K.; Kudo, E.; Kraiklang, R.; Wongkham, C.; Wongkham, S.; et al. Inhibition of carbonic anhydrase potentiates bevacizumab treatment in cholangiocarcinoma. Tumour. Biol. 2016, 37, 9023–9035. [Google Scholar] [CrossRef] [PubMed]
- Sugiyama, H.; Onuki, K.; Ishige, K.; Baba, N.; Ueda, T.; Matsuda, S.; Takeuchi, K.; Onodera, M.; Nakanuma, Y.; Yamato, M.; et al. Potent in vitro and in vivo antitumor activity of sorafenib against human intrahepatic cholangiocarcinoma cells. J. Gastroenterol. 2011, 46, 779–789. [Google Scholar] [CrossRef] [PubMed]
- Kim, D.H.; Jeong, Y.I.; Chung, C.W.; Kim, C.H.; Kwak, T.W.; Lee, H.M.; Kang, D.H. Preclinical evaluation of sorafenib-eluting stent for suppression of human cholangiocarcinoma cells. Int. J. Nanomed. 2013, 8, 1697–1711. [Google Scholar] [CrossRef] [PubMed]
- Yoshikawa, D.; Ojima, H.; Kokubu, A.; Ochiya, T.; Kasai, S.; Hirohashi, S.; Shibata, T. Vandetanib (ZD6474), an inhibitor of VEGFR and EGFR signalling, as a novel molecular-targeted therapy against cholangiocarcinoma. Br. J. Cancer 2009, 100, 1257–1266. [Google Scholar] [CrossRef] [PubMed]
- Takahashi, H.; Ojima, H.; Shimizu, H.; Furuse, J.; Furukawa, H.; Shibata, T. Axitinib (AG-013736), an oralspecific VEGFR TKI, shows potential therapeutic utility against cholangiocarcinoma. Jpn. J. Clin. Oncol. 2014, 44, 570–578. [Google Scholar] [CrossRef] [PubMed]
- Horiuchi, H.; Kawamata, H.; Fujimori, T.; Kuroda, Y. A MEK inhibitor (U0126) prolongs survival in nude mice bearing human gallbladder cancer cells with K-Ras mutation: Analysis in a novel orthotopic inoculation model. Int. J. Oncol. 2003, 23, 957–963. [Google Scholar] [CrossRef] [PubMed]
- Cavalloni, G.; Peraldo-Neia, C.; Varamo, C.; Chiorino, G.; Sassi, F.; Aglietta, M.; Leone, F. Preclinical activity of EGFR and MEK1/2 inhibitors in the treatment of biliary tract carcinoma. Oncotarget 2016. [Google Scholar] [CrossRef] [PubMed]
- Prakobwong, S.; Gupta, S.C.; Kim, J.H.; Sung, B.; Pinlaor, P.; Hiraku, Y.; Wongkham, S.; Sripa, B.; Pinlaor, S.; Aggarwal, B.B. Curcumin suppresses proliferation and induces apoptosis in human biliary cancer cells through modulation of multiple cell signaling pathways. Carcinogenesis 2011, 32, 1372–1380. [Google Scholar] [CrossRef] [PubMed]
- Prakobwong, S.; Khoontawad, J.; Yongvanit, P.; Pairojkul, C.; Hiraku, Y.; Sithithaworn, P.; Pinlaor, P.; Aggarwal, B.B.; Pinlaor, S. Curcumin decreases cholangiocarcinogenesis in hamsters by suppressing inflammation-mediated molecular events related to multistep carcinogenesis. Int. J. Cancer 2011, 129, 88–100. [Google Scholar] [CrossRef] [PubMed]
- Francis, H.; DeMorrow, S.; Venter, J.; Onori, P.; White, M.; Gaudio, E.; Francis, T.; Greene, J.F., Jr.; Tran, S.; Meininger, C.J.; et al. Inhibition of histidine decarboxylase ablates the autocrine tumorigenic effects of histamine in human cholangiocarcinoma. Gut 2012, 61, 753–764. [Google Scholar] [CrossRef] [PubMed]
- Francis, H.; Onori, P.; Gaudio, E.; Franchitto, A.; DeMorrow, S.; Venter, J.; Kopriva, S.; Carpino, G.; Mancinelli, R.; White, M.; et al. H3 histamine receptor-mediated activation of protein kinase Calpha inhibits the growth of cholangiocarcinoma in vitro and in vivo. Mol. Cancer Res. 2009, 7, 1704–1713. [Google Scholar] [CrossRef] [PubMed]
- Xu, D.; Ma, Y.; Zhao, B.; Li, S.; Zhang, Y.; Pan, S.; Wu, Y.; Wang, J.; Wang, D.; Pan, H.; et al. Thymoquinone induces G2/M arrest, inactivates PI3K/Akt and nuclear factor-κB pathways in human cholangiocarcinomas both in vitro and in vivo. Oncol. Rep. 2014, 31, 2063–2070. [Google Scholar] [CrossRef] [PubMed]
- Dey, N.; De, P.; Brian, L.J. Evading anti-angiogenic therapy: Resistance to anti-angiogenic therapy in solid tumors. Am. J. Transl. Res. 2015, 7, 1675–1698. [Google Scholar] [CrossRef] [PubMed]
- Eikesdal, H.P.; Kalluri, R. Drug resistance associated with antiangiogenesis therapy. Semin. Cancer Biol. 2009, 19, 310–317. [Google Scholar] [CrossRef] [PubMed]
- Zhu, A.X.; Meyerhardt, J.A.; Blaszkowsky, L.S.; Kambadakone, A.R.; Muzikansky, A.; Zheng, H.; Clark, J.W.; Abrams, T.A.; Chan, J.A.; Enzinger, P.C.; et al. Efficacy and safety of gemcitabine, oxaliplatin, and bevacizumab in advanced biliary-tract cancers and correlation of changes in 18-fluorodeoxyglucose PET with clinical outcome: A phase 2 study. Lancet Oncol. 2010, 11, 48–54. [Google Scholar] [CrossRef]
- Lubner, S.J.; Mahoney, M.R.; Kolesar, J.L.; Loconte, N.K.; Kim, G.P.; Pitot, H.C.; Philip, P.A.; Picus, J.; Yong, W.P.; Horvath, L.; et al. Report of a multicenter phase II trial testing a combination of biweekly bevacizumab and daily erlotinib in patients with unresectable biliary cancer: A phase II Consortium study. J. Clin. Oncol. 2010, 28, 3491–3497. [Google Scholar] [CrossRef] [PubMed]
- Guion-Dusserre, J.F.; Lorgis, V.; Vincent, J.; Bengrine, L.; Ghiringhelli, F. FOLFIRI plus bevacizumab as a second-line therapy for metastatic intrahepatic cholangiocarcinoma. World J. Gastroenterol. 2015, 21, 2096–2101. [Google Scholar] [CrossRef] [PubMed]
- NCT01206049: Combination Chemotherapy Plus Panitumumab or Bevacizumab for Inoperable Cholangiocarcinoma without KRAS Mutations (GOC-B-P). Available online: https://clinicaltrials.gov/ct2/show/NCT01206049 (accessed on 11 December 2016).
- A Study of FOLFOX6 with Bevacizumab for Biliary System Carcinoma. Available online: https://clinicaltrials.gov/ct2/show/study/NCT00881504 (accessed on 11 December 2016).
- NCT01007552: A Study of Gemcitabine, Capecitabine and Bevacizumab to Treat Cancer of the Gall Bladder or Bile Duct. Available online: https://clinicaltrials.gov/ct2/show/NCT01007552 (accessed on 11 December 2016).
- NCT02520141: A Phase II Study of Ramucirumab for Advanced, Pre-Treated Biliary Cancers. Available online: https://clinicaltrials.gov/ct2/show/NCT02520141 (accessed on 11 December 2016).
- An Open-Label, Multicenter, Phase I Study of Ramucirumab Plus Pembrolizumab in Patients with Locally Advanced and Unresectable or Metastatic Gastric or Gastroesophageal Junction Adenocarcinoma, Non-Small Cell Lung Cancer, Transitional Cell Carcinoma of the Urothelium, or Biliary Tract Cancer. Available online: https://clinicaltrials.gov/ct2/show/NCT02443324 (accessed on 11 December 2016).
- A Study of Ramucirumab (LY3009806) or Merestinib (LY2801653) in Advanced or Metastatic Biliary Tract Cancer. Available online: https://clinicaltrials.gov/ct2/show/NCT02711553 (accessed on 11 December 2016).
- Phase I Study Testing the Combination of Aflibercept and Capecitabine in Metastatic Digestive and Breast Cancers (MOMENTUM1). Available online: https://clinicaltrials.gov/ct2/show/NCT01843725 (accessed on 11 December 2016).
- Bengala, C.; Bertolini, F.; Malavasi, N.; Boni, C.; Aitini, E.; Dealis, C.; Zironi, S.; Depenni, R.; Fontana, A.; del Giovane, C.; et al. Sorafenib in patients with advanced biliary tract carcinoma: A phase II trial. Br. J. Cancer 2010, 102, 68–72. [Google Scholar] [CrossRef] [PubMed]
- El-Khoueiry, A.B.; Rankin, C.J.; Ben-Josef, E.; Lenz, H.J.; Gold, P.J.; Hamilton, R.D.; Govindarajan, R.; Eng, C.; Blanke, C.D. SWOG 0514: A phase II study of sorafenib in patients with unresectable or metastatic gallbladder carcinoma and cholangiocarcinoma. Investig. New Drugs 2012, 30, 1646–1651. [Google Scholar] [CrossRef] [PubMed]
- Moehler, M.; Maderer, A.; Schimanski, C.; Kanzler, S.; Denzer, U.; Kolligs, F.T.; Ebert, M.P.; Distelrath, A.; Geissler, M.; Trojan, J.; et al. Working Group of Internal Oncology. Gemcitabine plus sorafenib versus gemcitabine alone in advanced biliary tract cancer: A double-blind placebo-controlled multicentre phase II AIO study with biomarker and serum programme. Eur. J. Cancer 2014, 50, 3125–3135. [Google Scholar] [CrossRef] [PubMed]
- Lee, J.K.; Capanu, M.; O’Reilly, E.M.; Ma, J.; Chou, J.F.; Shia, J.; Katz, S.S.; Gansukh, B.; Reidy-Lagunes, D.; Segal, N.H.; et al. A phase II study of gemcitabine and cisplatin plus sorafenib in patients with advanced biliary adenocarcinomas. Br. J. Cancer 2013, 109, 915–919. [Google Scholar] [CrossRef] [PubMed]
- El-Khoueiry, A.B.; Rankin, C.; Siegel, A.B.; Iqbal, S.; Gong, I.Y.; Micetich, K.C.; Kayaleh, O.R.; Lenz, H.J.; Blanke, C.D. S0941: A phase 2 SWOG study of sorafenib and erlotinib in patients with advanced gallbladder carcinoma or cholangiocarcinoma. Br. J. Cancer 2014, 110, 882–887. [Google Scholar] [CrossRef] [PubMed]
- NCT00955721: A Study of Combination of Gemcitabine, Oxaliplatin (GEMOX)-Sorafenib in Patients with Advanced Biliary Tract Cancer. Available online: https://clinicaltrials.gov/ct2/show/study/NCT00955721?sect=X01256 (accessed on 11 December 2016).
- NCT00634751: CO07204-Phase I/II of Oxaliplatin, Capecitabine & Sorafenib for Advanced Pancreatic & Biliary Carcinoma. Available online: https://clinicaltrials.gov/ct2/show/results/NCT00634751 (accessed on 11 December 2016).
- NCT02836847: Molecularly Target Therapy with GEMOX in Advanced or Recurrent Extrahepatic Cholangiocarcinoma and Gallbladder Carcinoma. Available online: https://clinicaltrials.gov/ct2/show/NCT02836847 (accessed on 11 December 2016).
- Kessler, E.R.; Eckhardt, S.G.; Pitts, T.M.; Bradshaw-Pierce, E.L.; O’Byrant, C.L.; Messersmith, W.A.; Nallapreddy, S.; Weekes, C.; Spratlin, J.; Lieu, C.H.; et al. Phase I trial of vandetanib in combination with gemcitabine and capecitabine in patients with advanced solid tumors with an expanded cohort in pancreatic and biliary cancers. Invest. New Drugs 2016, 34, 176–183. [Google Scholar] [CrossRef] [PubMed]
- Santoro, A.; Gebbia, V.; Pressiani, T.; Testa, A.; Personeni, N.; Arrivas Bajardi, E.; Foa, P.; Buonadonna, A.; Bencardino, K.; Barone, C.; et al. A randomized, multicenter, phase II study of vandetanib monotherapy versus vandetanib in combination with gemcitabine versus gemcitabine plus placebo in subjects with advanced biliary tract cancer: The VanGogh study. Ann. Oncol. 2015, 26, 542–547. [Google Scholar] [CrossRef] [PubMed]
- Valle, J.W.; Wasan, H.; Lopes, A.; Backen, A.C.; Palmer, D.H.; Morris, K.; Duggan, M.; Cunningham, D.; Anthoney, D.A.; Corrie, P.; et al. Cediranib or placebo in combination with cisplatin and gemcitabine chemotherapy for patients with advanced biliary tract cancer (ABC-03): A randomised phase 2 trial. Lancet Oncol. 2015, 16, 967–978. [Google Scholar] [CrossRef]
- Yi, J.H.; Thongprasert, S.; Lee, J.; Doval, D.C.; Park, S.H.; Park, J.O.; Park, Y.S.; Kang, W.K.; Lim, H.Y. A phase II study of sunitinib as a second-line treatment in advanced biliary tract carcinoma: A multicentre, multinational study. Eur. J. Cancer 2012, 48, 196–201. [Google Scholar] [CrossRef] [PubMed]
- NCT01718327: A Phase II Open-Label Single Arm Study of Sunitinib in Patients with Advanced Cholangiocarcinoma. Available online: https://clinicaltrials.gov/ct2/show/NCT01718327 (accessed on 11 December 2016).
- NCT02115542: Single Agent Regorafenib in Refractory Advanced Biliary Cancers. Available online: https://clinicaltrials.gov/ct2/show/NCT02115542 (accessed on 11 December 2016).
- A Phase II Trial of Regorafenib as A Single Agent in Advanced and Metastatic Biliary Tract Carcinoma/Cholangiocarcinoma Patients Who Have Failed First-line Chemotherapy. Available online: https://clinicaltrials.gov/ct2/show/NCT02053376 (accessed on 11 December 2016).
- NCT02386397: Activity of Regorafenib in Combination with Chemotherapy in Patients with Advanced Biliary Tract Cancer (BREGO). Available online: https://clinicaltrials.gov/ct2/show/NCT02386397 (accessed on 11 December 2016).
- Bekaii-Saab, T.; Phelps, M.A.; Li, X.; Saji, M.; Goff, L.; Kauh, J.S.; O’Neil, B.H.; Balsom, S.; Balint, C.; Liersemann, R.; et al. Multi-institutional phase II study of selumetinib in patients with metastatic biliary cancers. J. Clin. Oncol. 2011, 29, 2357–2363. [Google Scholar] [CrossRef] [PubMed]
- Dreyer, C.; Sablin, M.P.; Bouattour, M.; Neuzillet, C.; Ronot, M.; Dokmak, S.; Belghiti, J.; Guedj, N.; Paradis, V.; et al. Disease control with sunitinib in advanced intrahepatic cholangiocarcinoma resistant to gemcitabine-oxaliplatin chemotherapy. World J. Hepatol. 2015, 7, 910–915. [Google Scholar] [CrossRef] [PubMed]
- A Study of Different Dosing Schedules of Selumetinib with Cisplatin/Gemcitabine (CIS/GEM) versus CIS/GEM Alone in Biliary Cancer. Available online: https://clinicaltrials.gov/ct2/show/NCT02151084?term=selumetinib+biliary&rank=2 (accessed on 27 January 2017).


{kind=link}
| Subtype of BTC | Genomic Aberrations |
|---|---|
| iCCA | FGFR2 fusion genes |
| IDH1/2 mutations | |
| pCCA | KRAS mutations |
| eCCA | PRKACA and PRKACB fusion genes |
| GBC | PTEN (inactivated) |
| TSC1 (inactivated) | |
| EGFR, ERBB2 and ERBB3 (activated) |
| Drug | Design | Regimen | Main Inclusion Criteria | Primary Outcomes | Status | Results | Reference |
|---|---|---|---|---|---|---|---|
| mAb | Phase II | Bevacizumab + GEMOX | Metastatic BTC | PFS | Terminated | mPFS: 7.0 months; PFS rate: 63% | [75] |
| mAb | Phase II | Bevacizumab + CT + erlotinib | Metastatic BTC | Response rate | Terminated | PR:12%; SD: 51%; mOS: 9.9 months; TTP: 4.4 months | [76] |
| mAb | Phase II | Bevacizumab + FOLFIRI | Second line therapy in GEMOX pretreated m-iCCA | Tolerance and efficacy | Terminated | PR: 5/13 pts; SD 6/13 pts; mPFS: 8 months; mOS: 20 months | [77] |
| mAb | Randomized phase II | Bevacizumab vs. panitumum + oxaliplatin/gemcitabine/capecitabine | Untreated advanced or metastatic K-RAS wild-type (WT) BTC | 6-month survival rate; 6-month progression rates | Ongoing | Not achieved | [78] |
| mAb | Phase II | Bevacizumab + FOLFOX | Advanced BTC | Safely | Closed for slow accrual | Not drawn | [79] |
| mAb | Phase II | Bevacizumab + gemcitabine + capecitabine | Advanced or metastatic adenoca. of gallbladder or biliary ducts | Safety/efficacy | Ongoing | Not achieved | [80] |
| mAb | Phase II | Ramucirumab | Advanced, pre-treated BTCs | Safety/efficacy | Ongoing | Not achieved | [81] |
| mAb | Phase I | Ramucirumab + pembrolizumab | Metastatic BTC | Safety/DLT | Ongoing | Not achieved | [82] |
| mAb | Phase II | Ramucirumab vs. merestinib + cisplatin/Gemcitabine | Advanced or metastatic BTC | PFS | Ongoing | Not achieved | [83] |
| VEGF trap | Phase I | Aflibercept + capecitabine | Chemorefractory metastatic BTC | DLT/MTD | On going | Not achieved | [84] |
| TKI | Phase II | Sorafenib | Advanced BTC | Disease control rate at 12 weeks | Terminated | Disease control rate at 12 weeks: 32.6%; mPFS: 2.3 months; mOS: 4.4 months | [85] |
| TKI | Phase II | Sorafenib | Advanced BTC | Objective response rate | Closed for not achieved primary objective | Response rate: 0%; SD: 39%; PFS: 3 months; OS: 9 months | [86] |
| TKI | Double-blind randomized phase II | Sorafenib + gemcitabine vs. placebo + gemcitabine | Unresectable or metastatic mBTC | PFS | Terminated | PFS: 4.9 vs. 3.0 months (p = 0.859); mOS: 11.2 vs. 8.4 months (p = 0.775) | [87] |
| TKI | Phase II | Sorafenib + gemcitabine/cisplatin | mBTC first-line therapy | 6-month PFS | Terminated | 6-month PFS: 51%, mPFS: 6.5 months; mOS: 14.4 months | [88] |
| TKI | Phase II | Sorafenib + erlotinib | mBTC first-line therapy | PFS | Stopped for failure to meet the main requirement | Unconfirmed PR: 2/13; mPFS: 2 months; mOS: 6 months | [89] |
| TKI | Phase I/II | Sorafenib + GEMOX | Advanced BTC | Safely | Closed for slow accrual | Not drawn | [90] |
| TKI | Phase I/II | Sorafenib + capecitabine/Oxaliplatine | Advanced BTC | Safety/efficacy | Ongoing | Not achieved | [91] |
| TKI | Umbrella phase I/II trial | Sorafenib vs. other TKI + GEMOX | Advanced or metastatic GBC or eCCA | Safety/efficacy | Ongoing | Not achieved | [92] |
| TKI | Phase I | Vandetanib + gemcitabine/capecitabine | mBTC | MTD/safety | Terminated | Vandetanib 300 mg daily; good safety profile | [93] |
| TKI | Randomized phase II | Vandetanib vs. vandetanib + gemcitabine vs. gemcitabine | Advanced BTC | mPFS | Terminated | mPFS: 105 vs. 114 vs. 148 days (p = 0.18) | [94] |
| TKI | Randomized phase II | Cediranib vs. placebo + cisplatin/gemcitabine | Advanced BTC | mPFS | Terminated | mPFS: 8 vs. 7.4 months (p = 0.72) | [95] |
| TKI | Phase II | Sunitinib | Second line unresectable, metastatic BTC | Safety/efficacy | Terminated | mTTP: 1.7 months; Objective RR: 8.9%; Grade 3–4 toxicities in 46.4% of patients | [96] |
| TKI | Phase II | Sunitinib | Advanced CCA | PFS/ORR | Ongoing | Not achieved | [97] |
| TKI | Phase II | Regorafenib | mBTC with no more than 2 prior lines CT | 6-month OS rate | Ongoing | Not achieved | [98] |
| TKI | Phase II | Regorafenib | advanced, metastatic BTC, after first-line CT | PFS | Ongoing | Not achieved | [99] |
| TKI | Phase Ib/II | Regorafenib + GEMOX | advanced BTC | MTD/safety | Ongoing | Not achieved | [100] |
| TKI | Phase II | Selumetinib | metastatic BTC | PFS | Terminated | mPFS: 3.7 months | [101] |
© 2017 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license ( http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Simone, V.; Brunetti, O.; Lupo, L.; Testini, M.; Maiorano, E.; Simone, M.; Longo, V.; Rolfo, C.; Peeters, M.; Scarpa, A.; et al. Targeting Angiogenesis in Biliary Tract Cancers: An Open Option. Int. J. Mol. Sci. 2017, 18, 418. https://0-doi-org.brum.beds.ac.uk/10.3390/ijms18020418
Simone V, Brunetti O, Lupo L, Testini M, Maiorano E, Simone M, Longo V, Rolfo C, Peeters M, Scarpa A, et al. Targeting Angiogenesis in Biliary Tract Cancers: An Open Option. International Journal of Molecular Sciences. 2017; 18(2):418. https://0-doi-org.brum.beds.ac.uk/10.3390/ijms18020418
Chicago/Turabian StyleSimone, Valeria, Oronzo Brunetti, Luigi Lupo, Mario Testini, Eugenio Maiorano, Michele Simone, Vito Longo, Christian Rolfo, Marc Peeters, Aldo Scarpa, and et al. 2017. "Targeting Angiogenesis in Biliary Tract Cancers: An Open Option" International Journal of Molecular Sciences 18, no. 2: 418. https://0-doi-org.brum.beds.ac.uk/10.3390/ijms18020418