Adverse Effects of Proton Pump Inhibitors—Evidence and Plausibility



1
Department of Clinical and Molecular Medicine, Faculty of Medicine and Health Sciences, Norwegian University of Science and Technology (NTNU), Prinsesse Kristinas gate 3, 7006 Trondheim, Norway
2
Department of Gastroenterology and Hepatology, St Olav’s Hospital—Trondheim University Hospital, Prinsesse Kristinas gate 1, 7030 Trondheim, Norway
*
Author to whom correspondence should be addressed.
Int. J. Mol. Sci. 2019, 20(20), 5203; https://0-doi-org.brum.beds.ac.uk/10.3390/ijms20205203
Submission received: 28 August 2019
/
Revised: 17 October 2019
/
Accepted: 18 October 2019
/
Published: 21 October 2019
(This article belongs to the Special Issue Proton-Pump Inhibitors (PPIs))
{kind=link}
Abstract
:Proton pump inhibitors (PPIs) have been increasingly used over the last decades and there are concerns about overuse and the numerous reported side-effects. It is uncertain whether associations between PPI use and potential side effects are causal. However, important evidence from experimental and mechanistic studies that could support a causal relationship may have been underestimated by epidemiologists and meta-analysists. In the current manuscript we review the combined epidemiological and mechanistic evidence of the adverse effects of PPI use.
1. Introduction
Proton pump inhibitors (PPIs) are irreversible inhibitors of the gastric H+K+ATPase in parietal cells and they reduce acid secretion. PPIs have a short plasma half-life but bind irreversibly to proton pumps and new proton pumps must be synthesized before acid secretion is restored. The degree and duration of gastric hypoacidity caused by repeat PPI dosage exceed the effects of competitive histamine 2 receptor antagonists (H2RA) by far [1,2,3] and a phylogenetically well-preserved biological function [4] is nearly removed. PPIs have long been used in the management of acid-related gastrointestinal diseases, such as peptic ulcers and gastro-esophageal reflux disease (GERD). However, an increase in PPI use has been well described in many countries over the last decades [5,6]. This increase is perceived to be caused by the widespread use of PPIs in treatment of dyspepsia and prevention of gastrointestinal bleeding in patients prescribed antiplatelet therapy or non-steroid anti-inflammatory drugs (NSAIDs), coupled with the belief that PPIs have few adverse effects. Furthermore, even though the indications for PPI use have expanded, numerous studies have documented prevalent inappropriate PPI prescription [7,8,9], so that patients without indication may in many Western populations be the largest group of users. Side-effects of PPIs seem to be mainly caused by the desired drug effect, that is to induce gastric hypoacidity, which in turn may directly or indirectly cause harm. Short-term effects of PPIs are relatively well studied, but the consequences of long-term profound acid inhibition are not fully known, as the observation time in epidemiological studies is often too short for the detection of diseases that develop over many years. Another problem with epidemiologic studies is the inherent potential of unmeasured confounding factors. Therefore, we have emphasized essential translational research and mechanistic studies that may underpin observations in epidemiological studies. More importantly, mechanistic studies of long-term PPI use may be more significant than the relatively short, but large, epidemiological studies of patients using PPIs. This is particularly important when studying diseases with long latency, such as cancers.
2. Results and Discussion
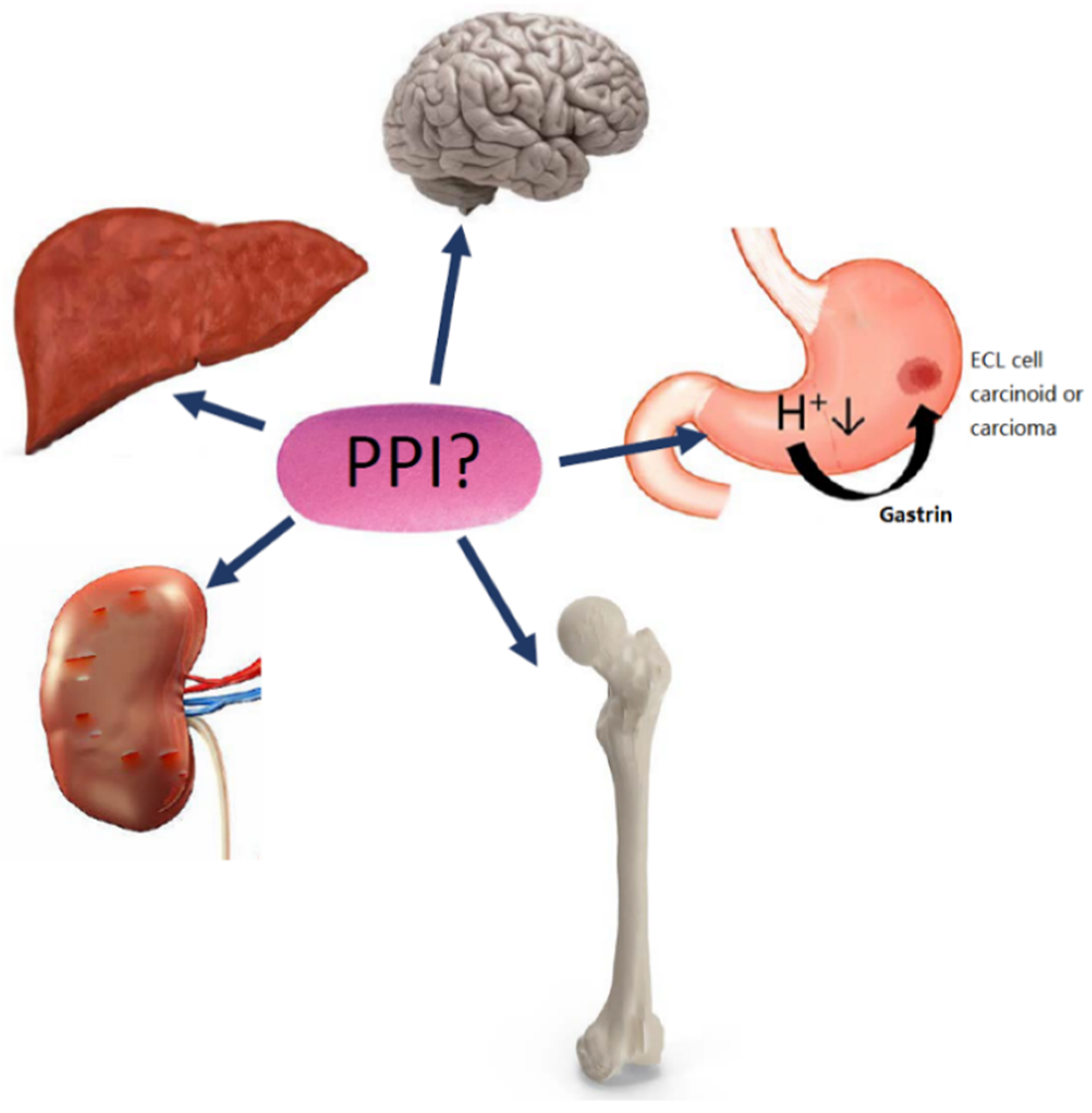
Numerous types of side effects of PPIs have been proposed and we have in this review focused on the increased risk of gastric neoplasia, kidney disease, bone fractures, impaired absorption of micronutrients, dementia, and liver disease (Figure 1). The increased risk of infections is reviewed in a separate publication in this Special issue of IJMS (Martinsen TC et al., pending submission). Many of the side-effects reviewed are relatively rare in contrast to the widespread worldwide use of PPIs. Some of this may be explained by inter-individual variation in acid inhibition in humans and that a proportion of PPI users have more profound and long-lasting acid inhibition following ingestion, which is reflected by variations in serum gastrin concentrations [10,11]. Genetic variation in CYP2C19 contributes to differences in the inhibitory activity of the PPIs. About 15–20% of Asians and 2–6% of Caucasians are known to be slow or poor metabolizers [12]. Patients with a CYP2C19 genotype resulting in a poor metabolizer phenotype have a considerable higher median 24 h intragastric pH than extensive metabolizers [13]. Although direct evidence is absent it seems likely that poor metabolizers, who have more pronounced hypoacidity and hypergastrinemia, are more likely to develop many of the adverse effects discussed in this manuscript. Animal studies of the effects of PPIs and H2RA have often used doses per kg body weight that are much higher than the doses used in patients. This was done in order to examine the intended and therapeutic effect of PPIs in patients, which is induction of gastric hypoacidity, and rodents require much higher doses to achieve such effects. Consequently, many appropriately-designed animal studies have used high doses of PPIs, which are particularly important if negative findings are to be reported. Whereas rats become hypoacidic at doses of 400 µmol/Kg/day omeprazole, it is nearly impossible to administer a PPI to mice in a sufficient dose (1750 µmol/Kg/day subcutaneously) to induce 24 h profound hypoacidity and hypergastrinemia [14].
2.1. Gastric Neoplasia
The risk of gastric neoplasia in patients with gastric hypoacidity and hypergastrinemia was noted in patients with chronic atrophic gastritis decades before PPIs were invented [15]. Before PPIs were marketed for widespread use, it was known that rats given omeprazole (400 µmol/Kg/day) or the irreversible H2RA loxtidine (250–600 mg/Kg/day) in doses sufficient to inhibit gastric acid secretion and cause hypergastrinemia, developed enterochromaffin-like (ECL)-cell tumours in the gastric corpus [16,17]. Shortly thereafter it was realized that the competitive H2RA ranitidine also caused ECL cell tumours, when given the dose needed to achieve prolonged acid inhibition [18]. Further studies have demonstrated that ECL cell tumours in the corpus remnant may also be induced by partial corpectomy causing hypergastrinemia [19,20] or by administration of ciprofibrate, a drug that induces hypergastrinemia without altering gastric acidity [21,22,23]. Transgenic INS-GAS mice have hypergastrinemia accompanied by gastric hyperacidity and develop tumours in the gastric corpus with an adenocarcinoma phenotype [24]. Inoculation by Helicobacter felis increases the hypergastrinemia and accelerates the carcinogenesis considerably [24]. The rodent Mastomys natalensis develops tumours in the gastric corpus that were originally classified as adenocarcinomas [25,26]. However, the lesions were later re-classified as ECL cell tumours and the observed propensity may be caused by a mutation leading to constitutively activation of the CCK2/gastrin receptor [27]. The tumorigenesis in M. natalensis is enhanced by the H2RA loxtidine [28] and inhibited by the gastrin receptor antagonist YF476 (later named netazepide) [29], further demonstrating the role of gastrin. Male Japanese cotton rats given loxtidine in order to induce gastric hypoacidity develop tumours with an adenocarcinoma phenotype, but neuroendocrine differentiation, after six months [30]. The spontaneous tumour formation in Japanese female cotton rats may be prevented by the gastrin receptor antagonist YF476 [31]. Through the above-mentioned series of animal studies, it has been documented that long-term hypergastrinemia, whether accompanied by gastric hypoacidity or hyperacidity, causes neoplasia in the gastric corpus with varying expression of neuroendocrine markers, in all species where sufficient hypergastrinemia has been be achieved [32]. The pivotal role of the ECL cell in hypergastrinemia-driven carcinogenesis has been described in a separate paper in IJMS [33]. The trophic effect of gastrin in rats [34] as well as in patients with chronic atrophic gastritis and ECL cell dysplasia [35,36] seems to level off at values below 500 pM and studies suggest that the dose-response relationship of gastrin on its target cell is very similar in rodents and humans. The increased risk of gastric ECL neuroendocrine tumours (NETs) and carcinomas in PPI users has therefore been predicted since the 1980s [37]. The ECL cell is the target cell of gastrin and ECL cell carcinoids in PPI users, although probably underreported by some [38,39,40], and the tumours may regress after cessation of PPI use [41]. Furthermore, patients homozygous of an inactivating mutation in the H+K+ATPase alpha subunit develop ECL cell carcinoids and adenocarcinoma in their third to fourth decade [42,43]. These patients represent the human genetic disease that best models the consequences of long-term PPI use and also indicate that the duration of profound acid inhibition needed to cause gastric neoplasia, either ECL cell carcinoids or adenocarcinomas, in most patients could be several decades. In this context, it should be noted that carcinogenesis driven by hypergastrinemia in rodent models takes months to years before neoplasia is found, a timespan that could translate into decades in humans and this observation could be relevant when starting long-term profound acid inhibition in young individuals. Another human disease that causes gastric hypoacidity and hypergastrinemia similar to a proportion of patients using long-term high-dose PPIs, is autoimmune chronic atrophic gastritis. These patients have an increased risk of adenocarcinomas in the gastric corpus and fundus, which was noted in the 1950s [15] and the risks of both adenocarcinoma and ECL cell tumours were studied during the subsequent decades [35,36,44]. The annual risk of gastric adenocarcinoma seems similar to the risk of ECL cell tumour formation in such patients and is in the range of 0.3–0.5% [44,45]. More recently, it was reported that PPI users have an increased risk of gastric adenocarcinoma in epidemiological studies, with an overall standardized incidence ratio of 3.38 in a Swedish population [46], and in an additional publication it was emphasized that the risk did not decline with time [47]. In a Japanese population of patients who received Helicobacter pylori eradication, PPI users had an adjusted hazard ratio (HR) of 3.61 for gastric cancer during follow-up [48]. Furthermore, Cheung et al. studied a population in Hong Kong and found an increased risk of gastric cancer in patients given H. pylori eradication treatment with an HR of 2.44, and the HR increased with longer duration of PPI use [49]. H2RA users did not have higher risks of gastric cancer in any of these studies. Numerous studies suggest that hypergastrinemia, the common factor found in many conditions with increased cancer risk, is a key element in gastric carcinogenesis of the corpus and fundus [50,51]. PPIs cause gastric atrophy in a larger proportion of patients with GERD compared to those operated by fundoplication, particularly in H. pylori-positive individuals, where nearly one third developed atrophy during the five-year follow-up [52]. Prolonged acid inhibition also seems to preclude the recovery of atrophy following H. pylori eradication [53], which may contribute to persistent hypoacidity and hypergastrinemia even after eradication. Recently, self-reported adverse effects of PPI use were examined by using data from a randomized controlled trial (COMPASS) with over 17,000 participants whereof half the patients received pantoprazole [54]. The overall number of GI cancers was low during the three years of follow-up; the incidence of gastric cancer was not specified and incidence of atrophic gastritis was only 0.2% in three years [54]. This is in marked contrast to the incidence of atrophy in studies with gastric PPI-effects as a primary endpoint, where 19% of patients overall and 30.5% of H. pylori-positive subjects developed atrophic gastritis after five years [52], whereas a less targeted study design may preclude the evaluation of the effects of PPIs on gastric premalignant changes. It should be noted that the prevalence of premalignant gastric lesions at baseline may differ between patients in the follow-up studies of H. pylori-positive patients who for clinical reasons were tested for H. pylori and then received eradication treatment, and the COMPASS population who were given prophylactic PPIs. In a stomach with premalignant changes such as atrophy, metaplasia, and dysplasia, cancer may develop more rapidly than without such changes.
Other macroscopic changes in the gastric mucosa of PPIs use include fundic gland polyps [55,56], black spots, and cobblestone-like lesions [57] which are of uncertain clinical significance. However, a small proportion of patients develop fundic gland polyposis and this sub-group may require further evaluation. In total, numerous mechanistic studies suggest that hypoacidity and hypergastrinemia increase the risk of gastric cancer in the corpus/fundus and this was also supported by some epidemiological studies.
2.2. Renal Disease
It was first reported in 1992 that PPI use could cause acute interstitial nephritis (AIN) [58] and more than a decade later PPI-induced AIN became recognized as a clinical entity [59]. Due to their widespread use, PPIs are now considered to be among the most common causes of drug-induced AIN worldwide [60]. While one has estimated the mean time from starting PPIs to the clinical presentation of AIN to be 10 weeks, AIN may develop as late as nine months after treatment start and the risk is not dose dependent. More recently, several studies have reported an increased risk of incident chronic kidney disease (CKD) in PPI users (HR 1.18) [61], also after adjusting for uneven distribution of factors that could affect the risk of CKD (HR 1.76 compared with propensity score-matched non-users) [62]. The studies have some methodological weaknesses, including adjustments for baseline estimated glomerular filtration rate (eGFR) [63] and the general uncertainty related to residual confounding factors. In the COMPASS trial, baseline renal function was known, but patient-reported incident of CKD during follow-up did not differ between the study groups [54]. Incident renal failure that required treatment seemed likely to be self-reported during the study, whereas the incidence of asymptomatic modest reduction of renal function was more likely to be underreported [54].
The mechanism behind the observed increased risk of CKD in PPI users is obscure. It was initially considered whether drugs designed to inhibit the gastric proton pump also inhibit other proton pumps, such as the renal tubular proton pump (H+-ATPase) which in an in vitro tubule suspension from rats seemed to be affected by high concentrations of omeprazole [64]. However, as PPIs are weak bases with a pKa of 4, they are mainly activated in the acidic parietal cell canaliculi and bind covalently to the H+K+ATPase [65]. Furthermore, omeprazole does not affect electrolyte handling or acidification in urine in patients using 60 mg/day in the short term [66], and there is no evidence of PPI effects mediated by inhibition of the tubular proton pump in vivo in a clinical setting. Interestingly, it was recently reported that over half of patients who suffered PPI-induced AIN did not fully recover [67] suggesting that PPI-induced CKD may be due to progression of AIN, with inflammatory interstitial infiltrate and oedema, to chronic interstitial scarring and tubular atrophy. Altogether, there is good evidence that PPIs cause AIN and some evidence that they also increase the risk of CKD.
2.3. Fracture Risk
The risk of osteoporosis-related fractures in long-term PPI users became a concern after several observational studies reported a time- and dose-dependent increase in fracture risk [68,69,70]. In two recent meta-analyses of observational studies, PPI use was found to be significantly associated with an increased risk of hip fracture (RR 1.30), any-site facture (HR 1.29), and spine fracture (HR 1.49), which was not observed in patients with H2RA exposure [71,72]. Despite these studies, one has not been able to find a reduction in bone mineral density (BMD) during PPI treatment [73,74] and it was proposed that the observed increase in fracture risk is caused by increased comorbidity and lower BMD at the start of treatment. It was also found that PPI use was associated with a higher risk of recurrent falls in older women [75]. In a recent randomized placebo-controlled study, PPI users had increased markers of bone turnover (P1NP and CTX), but no reduction in BMD after 26 weeks of use [76]. In the mentioned COMPASS trial, PPI users did not have an increased risk of fractures [54]. It seems likely that the incidence of self-reported fractures is reliable, and this study strongly suggests that PPI use for three years does not increase fracture risk.
However, findings from several animal models of gastric hypoacidity have supported a causal relationship between long-term PPI use and the previously observed increased fracture risk. Rats given long-term omeprazole 400 µmol/Kg/day for three months exhibited reduced bone mineralization [77]. CCKB (gastrin) receptor-deficient mice are hypoacidic with hypocalcaemia, secondary hyperparathyroidism, and reduced BMD and bone quality at one year of age [78]. Furthermore, the skeletal changes in CCKB receptor-deficient mice could be reversed by calcium supplementation [79], suggesting a mechanism somehow related to impaired calcium handling and uptake in the gastrointestinal tract. H+K+ATPase beta subunit-deficient mice are also hypoacidic, hypergastrinemic, display an elevated parathyroid hormone [80], and have reduced BMD and bone quality [80,81], which only slightly improved by administration of a gastrin receptor antagonist. Patients with chronic atrophic gastritis, a condition that may be analogous to long-term high-dose PPI use with respect to hypoacidity, hypergastrinemia, and absorption of micronutrients, have an increased risk of fractures [82,83], reduced BMD [84], and reduced calcium carbonate absorption in fasting state [85]. However, absorption of other calcium compounds and calcium carbonate ingested together with food seems unaffected by hypoacidity [85,86,87] and in a recent well-designed, randomized trial, PPI-use did not affect serum calcium, serum parathyroid hormone, or urinary calcium [76]. Although early in vitro studies of omeprazole suggested that it could decrease bone resorption [88], there has not been further convincing evidence that PPIs have direct in vivo effects on bone. A potential role of elevated circulating histamine has also been proposed based on knowledge about the gastrin—histamine sequence in regulation of acid secretion [89], the observation of osteoporosis in patients with hyperhistaminemia caused by systemic mastocytosis [90], the increased bone loss in histidine decarboxylase-deficient mice [91], and reduced fracture risk in PPI users also using a histamine 1 receptor antagonist (H1RA) [92]. However, a H1RA did not alter the osteoporotic phenotype in H+K+ATPase beta subunit-deficient mice [93].
In conclusion, although findings from several animal models and patients with chronic atrophic gastritis have suggested that gastric hypoacidity affects bone metabolism negatively, the recent data from a randomized trial [54] suggest that PPIs do not increase fracture risk. The lack of one plausible mechanism also weakens the hypothesis that PPI use cause increased fracture risk. The observed increased fracture risk in epidemiologic studies may be explained by residual confounding factors related to increased comorbidity and risk of falling.
2.4. Dementia
A few years ago, two epidemiological studies reported that PPI users had an increased risk of incident dementia during follow-up (HR 1.44) [94], whereas another study found an increased risk of all-cause dementia (HR 1.38) [95], and more specifically for Alzheimer’s disease (HR 1.44) [95]. Similar risks were also found in retrospective studies (OR 1.55) [96]. These positive epidemiological studies are supported by previous findings in animal studies where transgenic mice predisposed to accumulation of beta-amyloid administered lansoprazole 20–200 mg/Kg had dose-dependent accumulation of beta amyloid (Aβ40 and Aβ42) in the central nervous system [97]. Many researchers have also suggested prion-like mechanisms in Alzheimer’s disease [98,99], where beta amyloid and tau are the soluble components in formation of plaques and tangles, respectively. The role of gastric acid in the defence against transmissible degenerative encephalopathies has been examined in mice. Mice with gastric hypoacidity induced by administration of ranitidine in the drinking water were susceptible to infection by the scrapie agent 139A in a ranitidine concentration-dependent manner [100]. Furthermore, mice with short-term hypoacidity induced by omeprazole were also more likely to become infected after inoculation with a scrapie agent [101].
Altogether it seems plausible that the association between dementia and PPI use could be causal; the increased risk of dementia has not been reproduced in the following epidemiological studies [102,103]. The previously mentioned COMPASS trial did not find increased risk of dementia in PPI users [54], however, there are inherent limitations tied to recording patient-reported incident dementia and according to published calculations the study was not powered for detecting an OR of incident dementia in the same range as previous studies. In conclusion, while epidemiological studies are conflicting, preclinical studies support a possible causal relationship.
2.5. Liver Disease
PPI use has been claimed to increase the risk of the cirrhosis-related complications of hepatic encephalopathy (HE) and spontaneous bacterial peritonitis, as well as to influence the risk of cirrhosis and liver cancer. PPI use increases the risk of developing HE in patients with cirrhosis [104] as well as the severity of HE [105]. Two recent meta-analyses confirmed the association [106,107] and the proposed mechanism is that PPIs induce bacterial overgrowth in the intestine [108]. It is known that PPIs do not only change the bacterial composition in the stomach, but also in faeces with a significant shift towards oral flora in principal coordinate analyses (PCoA) [109,110], demonstrating that the entire gastrointestinal tract is affected downstream of gastric hypoacidity. PPI use has been identified as a risk factor for the development of spontaneous bacterial peritonitis (SBP), also in multivariate analyses adjusting for known risk factors including the severity of liver disease [111,112]. In H+K+ATPase alpha subunit-deficient mice as well as mice given omeprazole, alcohol-induced liver damage worsens, which was seen in relation to intestinal bacterial overgrowth and an altered intestinal microbial composition [113]. More specifically, hypoacidity caused expansion of Enterococci, which was hypothesized to worsen alcoholic liver disease in mice as well as in humans [113]. Furthermore, others have identified increased abundances of Veilonella parvula and Streptococcus salivarius in the faecal microbiome of cirrhotic PPI users to be associated with liver-related mortality during three years of follow-up [114].
The risk of liver cancer in PPI users was recently found to be increased in two different populations, whereas no such risk was seen in H2-blocker users [115]. The underlying mechanism may be similar to that of HE, SBP, and alcohol-induced liver damage, whereby bacterial overgrowth [116] results in increased portal venous concentrations of several proposed harmful substances, including secondary bile acids [117]. In general, there is considerable interest in the role of intestinal microbiome in the pathogenesis of chronic liver diseases [118] that cannot be reviewed in depth here.
Although the epidemiological evidence is limited for the influence of PPIs on the pathogenesis of liver diseases including cancer, bacterial overgrowth and altered bacterial composition are indeed well-documented phenomena that raise concerns about adverse liver effects in PPI users.
2.6. Micronutrient Deficiency
Numerous studies have documented that gastric acid influences the absorption of minerals ingested as salts and protein-bound vitamin B12.
2.6.1. Vitamin B12
Increased risk of vitamin B12 deficiency has been a concern since absorption of protein-bound, but not unbound, vitamin B12 was found to be reduced during PPI use [119]. Observational studies suggested an increased risk with an OR of 1.65 for PPI users and OR of 1.25 for H2-blocker users [120]. However, a considerable number of other studies has not reproduced these findings and there seems to be insufficient evidence for routine measurements of B12 concentration in blood [121,122].
2.6.2. Calcium
Profound acid inhibition may interfere with the absorption of calcium [123]. However, long-term PPI does not seem to reduce absorption of water-soluble calcium salts and calcium absorption from the diet [76,124] and this has also weakened the hypothesis of disturbed calcium metabolism as a mechanism causing increased fracture risk.
2.6.3. Iron
Absorption of iron may be reduced in patients with gastric hypoacidity, as seen in patients using oral ferrous sulphate supplementation and omeprazole [125]. Interestingly patients with hereditary hemochromatosis have reduced absorption of dietary non-heme iron and PPI use also seems to reduce the need for phlebotomy [126,127]. Reduced absorption of iron was also observed in patients with hypoacidity due to chronic atrophic gastritis [128]. A large case-control study found PPI use to be associated with an increased risk of iron deficiency [129], but the magnitude of reduced iron absorption is most likely small in most individuals and the clinical importance has been questioned.
2.6.4. Magnesium
Hypomagnesemia has been described in PPI users since 2006 [130]. Many studies have suggested an increased risk and that hypomagnesemia develops in a proportion of PPI users [131]. Meta-analyses have been problematic due to study heterogeneity, but a recent analysis found that PPI users had an increased risk of hypomagnesemia (RR 1.44) compared to non-users [132], whereas analysis of only high-quality studies found an RR of 1.63 [133]. Hypomagnesemia is rare and it seems that mainly patients who already use a diuretic are at risk [131]. The mechanism of hypomagnesemia in PPI users is uncertain, but in depth reviews of case series suggest that reduced intestinal absorption rather than renal tubular loss is important [134]. In conclusion, symptomatic hypomagnesemia in PPI users is well-documented, but rare.
3. Conclusions
Epidemiological studies on PPI use and side effects may suffer from residual confounding and in some instances reverse causation. Furthermore, studies designed to detect long-term effects or relatively rare side effects have not been performed. Results from mechanistic studies, including animal studies, suggest that there are known and most likely unknown side effects of long-term gastric acid inhibition that should be considered when prescribing PPIs. Many patients have appropriate indications for long-term PPI use that may outweigh the risks discussed above. However, a large proportion of PPI users without indication have no benefits to outweigh any risk of side effects at all and this is a major concern. As some of the potential side effects may have an incubation time of years or even decades [42,43], the risks and benefits of starting long-long PPI use should be carefully considered. This general consideration regarding long-term medical treatment seems especially relevant in younger individuals who may initiate PPI use that could last 70 to 80 years.
Author Contributions
R.F., T.C.M. and H.L.W. participated in the planning of the review, as well as in the writing of the manuscript.
Funding
This research received no external funding.
Conflicts of Interest
The authors declare no conflict of interest.
Abbreviations
| AIN | Acute interstitial nephritis |
| BMD | Bone mineral density |
| CCKB | Cholecystokinin B |
| CKD | Chronic kidney disease |
| CTX | carboxy-terminal collagen crosslinks |
| ECL | Enterochromaffin-like |
| eGFR | Estimated glomerular filtration rate |
| GERD | Gastroesophageal reflux disease |
| GI | Gastrointestinal |
| H1RA | Histamine 1 receptor antagonist |
| H2RA | Histamine 2 receptor antagonist |
| HE | Hepatic encephalopathy |
| H. pylori | Helicobacter pylori |
| HR | Hazard ratio |
| NET | Neuroendocrine tumour |
| NSAID | Non-steroid anti-inflammatory drug |
| OR | Odds ratio |
| P1NP | procollagen type 1 N-terminal propeptide |
| PCoA | Principal coordinate analysis |
| PPI | Proton pump inhibitor |
| RR | Relative risk |
| SBP | Spontaneous bacterial peritonitis |
References
- Cederberg, C.; Rohss, K.; Lundborg, P.; Olbe, L. Effect of once daily intravenous and oral omeprazole on 24-hour intragastric acidity in healthy subjects. Scand. J. Gastroenterol. 1993, 28, 179–184. [Google Scholar] [CrossRef] [PubMed]
- Wilder-Smith, C.; Halter, F.; Ernst, T.; Gennoni, M.; Zeyen, B.; Varga, L.; Roehmel, J.J.; Merki, H.S. Loss of acid suppression during dosing with H2-receptor antagonists. Aliment. Pharmacol. Ther. 1990, 4 (Suppl. 1), 15–27. [Google Scholar] [PubMed]
- Pounder, R.E.; Sharma, B.K.; Walt, R.P. Twenty-four hour intragastric acidity during treatment with oral omeprazole. Scand. J. Gastroenterol. 1986, 21 (Suppl. 118), 108–117. [Google Scholar] [CrossRef] [PubMed]
- Johnsen, A.H. Phylogeny of the cholecystokinin/gastrin family. Front. Neuroendocrinol. 1998, 19, 73–99. [Google Scholar] [CrossRef] [PubMed]
- De la Coba Ortiz, C.; Arguelles Arias, F.; Martin de Argila de Prados, C.; Judez Gutierrez, J.; Linares Rodriguez, A.; Ortega Alonso, A.; Rodriguez de Santiago, E.; Rodriguez-Tellez, M.; Vera Mendoza, M.I.; Aguilera Castro, L.; et al. Proton-pump inhibitors adverse effects: A review of the evidence and position statement by the Sociedad Espanola de Patologia Digestiva. Rev. Esp. Enferm. Dig. 2016, 108, 207–224. [Google Scholar] [CrossRef]
- Pottegard, A.; Broe, A.; Hallas, J.; de Muckadell, O.B.; Lassen, A.T.; Lodrup, A.B. Use of proton-pump inhibitors among adults: A Danish nationwide drug utilization study. Ther. Adv. Gastroenterol. 2016, 9, 671–678. [Google Scholar] [CrossRef]
- Zink, D.A.; Pohlman, M.; Barnes, M.; Cannon, M.E. Long-term use of acid suppression started inappropriately during hospitalization. Aliment. Pharmacol. Ther. 2005, 21, 1203–1209. [Google Scholar] [CrossRef]
- Eid, S.M.; Boueiz, A.; Paranji, S.; Mativo, C.; Landis, R.; Abougergi, M.S. Patterns and predictors of proton pump inhibitor overuse among academic and non-academic hospitalists. Intern. Med. 2010, 49, 2561–2568. [Google Scholar] [CrossRef]
- Ahrens, D.; Behrens, G.; Himmel, W.; Kochen, M.M.; Chenot, J.F. Appropriateness of proton pump inhibitor recommendations at hospital discharge and continuation in primary care. Int. J. Clin. Pract. 2012, 66, 767–773. [Google Scholar] [CrossRef]
- Prewett, E.J.; Hudson, M.; Nwokolo, C.U.; Sawyerr, A.M.; Pounder, R.E. Nocturnal intragastric acidity during and after a period of dosing with either ranitidine or omeprazole. Gastroenterology 1991, 100, 873–877. [Google Scholar] [CrossRef]
- Jansen, J.B.; Klinkenberg-Knol, E.C.; Meuwissen, S.G.; De Bruijne, J.W.; Festen, H.P.; Snel, P.; Luckers, A.E.; Biemond, I.; Lamers, C.B. Effect of long-term treatment with omeprazole on serum gastrin and serum group A and C pepsinogens in patients with reflux esophagitis. Gastroenterology 1990, 99, 621–628. [Google Scholar] [CrossRef]
- Tang, H.L.; Li, Y.; Hu, Y.F.; Xie, H.G.; Zhai, S.D. Effects of CYP2C19 loss-of-function variants on the eradication of H. pylori infection in patients treated with proton pump inhibitor-based triple therapy regimens: A meta-analysis of randomized clinical trials. PLoS ONE 2013, 8, e62162. [Google Scholar] [CrossRef] [PubMed]
- Klotz, U.; Schwab, M.; Treiber, G. CYP2C19 polymorphism and proton pump inhibitors. Basic Clin. Pharmacol. Toxicol. 2004, 95, 2–8. [Google Scholar] [CrossRef] [PubMed]
- Waldum, H.L.; Brenna, E.; Martinsen, T.C. Safety of proton pump inhibitors. Aliment. Pharmacol. Ther. 2000, 14, 1537–1538. [Google Scholar] [CrossRef] [PubMed]
- Zamcheck, N.; Grable, E.; Ley, A.; Normal, L. Occurrence of gastric cancer among patients with pernicious anemia at the Boston City Hospital. N. Engl. J. Med. 1955, 252, 1103–1110. [Google Scholar] [CrossRef]
- Havu, N. Enterochromaffin-like cell carcinoids of gastric mucosa in rats after life-long inhibition of gastric secretion. Digestion 1986, 35 (Suppl. 1), 42–55. [Google Scholar] [CrossRef]
- Poynter, D.; Selway, S.A.; Papworth, S.A.; Riches, S.R. Changes in the gastric mucosa of the mouse associated with long lasting unsurmountable histamine H2 blockade. Gut 1986, 27, 1338–1346. [Google Scholar] [CrossRef]
- Havu, N.; Mattsson, H.; Ekman, L.; Carlsson, E. Enterochromaffin-like cell carcinoids in the rat gastric mucosa following long-term administration of ranitidine. Digestion 1990, 45, 189–195. [Google Scholar] [CrossRef]
- Mattsson, H.; Havu, N.; Brautigam, J.; Carlsson, K.; Lundell, L.; Carlsson, E. Partial gastric corpectomy results in hypergastrinemia and development of gastric enterochromaffinlike-cell carcinoids in the rat. Gastroenterology 1991, 100, 311–319. [Google Scholar] [CrossRef]
- Fossmark, R.; Martinsen, T.C.; Bakkelund, K.E.; Kawase, S.; Torp, S.H.; Waldum, H.L. Hypergastrinaemia induced by partial corpectomy results in development of enterochromaffin-like cell carcinoma in male Japanese cotton rats. Scand. J. Gastroenterol. 2004, 39, 919–926. [Google Scholar] [CrossRef]
- Spencer, A.J.; Barbolt, T.A.; Henry, D.C.; Eason, C.T.; Sauerschell, R.J.; Bonner, F.W. Gastric morphological changes including carcinoid tumors in animals treated with a potent hypolipidemic agent, ciprofibrate. Toxicol. Pathol. 1989, 17, 7–15. [Google Scholar] [CrossRef]
- Martinsen, T.C.; Nesjan, N.; Ronning, K.; Sandvik, A.K.; Waldum, H.L. The peroxisome-proliferator ciprofibrate induces hypergastrinemia without raising gastric pH. Carcinogenesis 1996, 17, 2153–2155. [Google Scholar] [CrossRef] [Green Version]
- Martinsen, T.C.; Bakke, I.; Chen, D.; Sandvik, A.K.; Zahlsen, K.; Aamo, T.; Waldum, H.L. Ciprofibrate stimulates the gastrin-producing cell by acting luminally on antral PPAR-alpha. Am. J. Physiol. Gastrointest. Liver Physiol. 2005, 289, G1052–G1060. [Google Scholar] [CrossRef]
- Wang, T.C.; Dangler, C.A.; Chen, D.; Goldenring, J.R.; Koh, T.; Raychowdhury, R.; Coffey, R.J.; Ito, S.; Varro, A.; Dockray, G.J.; et al. Synergistic interaction between hypergastrinemia and Helicobacter infection in a mouse model of gastric cancer. Gastroenterology 2000, 118, 36–47. [Google Scholar] [CrossRef]
- Oettele, A.G. Spontaneous carcinoma of the glandular stomach in Rattus (mastomys) natalensis, an African rodent. Br. J. Cancer 1957, 11, 415–433. [Google Scholar] [CrossRef]
- Oettele, A.G. Spontaneous carcinoma of the glandular stomach in a laboratory stock of Rattus (Mastomys) natalensis. S. Afr. J. Med. Sci. 1955, 20, 36. [Google Scholar]
- Schaffer, K.; McBride, E.W.; Beinborn, M.; Kopin, A.S. Interspecies polymorphisms confer constitutive activity to the Mastomys cholecystokinin-B/gastrin receptor. J. Biol. Chem. 1998, 273, 28779–28784. [Google Scholar] [CrossRef]
- Nilsson, O.; Wangberg, B.; Johansson, L.; Theodorsson, E.; Dahlstrom, A.; Modlin, I.M.; Ahlman, H. Rapid induction of enterochromaffinlike cell tumors by histamine2-receptor blockade. Am. J. Pathol. 1993, 142, 1173–1185. [Google Scholar]
- Kidd, M.; Siddique, Z.L.; Drozdov, I.; Gustafsson, B.I.; Camp, R.L.; Black, J.W.; Boyce, M.; Modlin, I.M. The CCK(2) receptor antagonist, YF476, inhibits Mastomys ECL cell hyperplasia and gastric carcinoid tumor development. Regul. Pept. 2010, 162, 52–60. [Google Scholar] [CrossRef]
- Fossmark, R.; Martinsen, T.C.; Bakkelund, K.E.; Kawase, S.; Waldum, H.L. ECL-cell derived gastric cancer in male cotton rats dosed with the H2-blocker loxtidine. Cancer Res. 2004, 64, 3687–3693. [Google Scholar] [CrossRef]
- Martinsen, T.C.; Kawase, S.; Hakanson, R.; Torp, S.H.; Fossmark, R.; Qvigstad, G.; Sandvik, A.K.; Waldum, H.L. Spontaneous ECL cell carcinomas in cotton rats: Natural course and prevention by a gastrin receptor antagonist. Carcinogenesis 2003, 24, 1887–1896. [Google Scholar] [CrossRef]
- Fossmark, R.; Qvigstad, G.; Martinsen, T.C.; Hauso, O.; Waldum, H.L. Animal models to study the role of long-term hypergastrinemia in gastric carcinogenesis. J. Biomed. Biotechnol. 2011, 2011, 975479. [Google Scholar] [CrossRef]
- Waldum, H.L.; Sordal, O.F.; Mjones, P.G. The Enterochromaffin-like [ECL] Cell-Central in Gastric Physiology and Pathology. Int. J. Mol. Sci. 2019, 20, 2444. [Google Scholar] [CrossRef]
- Brenna, E.; Waldum, H.L. Trophic effect of gastrin on the enterochromaffin like cells of the rat stomach: Establishment of a dose response relationship. Gut 1992, 33, 1303–1306. [Google Scholar] [CrossRef]
- Sjoblom, S.M.; Sipponen, P.; Karonen, S.L.; Jarvinen, H.J. Mucosal argyrophil endocrine cells in pernicious anaemia and upper gastrointestinal carcinoid tumours. J. Clin. Pathol. 1989, 42, 371–377. [Google Scholar] [CrossRef]
- Sjöblom, S.M.; Sipponen, P.; Karonen, S.L.; Jarvinen, H.J. Argyrophilic cell hyperplasia and carcinoid tumours in oxyntic mucosa of the stomach. Dependence on duration of pernicious aniaemia. Eur. J. Gastroenterol. Hepatol. 1991, 31, 153–157. [Google Scholar]
- Waldum, H.L.; Fossmark, R. Proton pump inhibitors and gastric cancer: A long expected side effect finally reported also in man. Gut 2017. [Google Scholar] [CrossRef]
- Cavalcoli, F.; Zilli, A.; Conte, D.; Ciafardini, C.; Massironi, S. Gastric neuroendocrine neoplasms and proton pump inhibitors: Fact or coincidence? Scand. J. Gastroenterol. 2015, 50, 1397–1403. [Google Scholar] [CrossRef]
- Nandy, N.; Hanson, J.A.; Strickland, R.G.; McCarthy, D.M. Solitary Gastric Carcinoid Tumor Associated with Long-Term Use of Omeprazole: A Case Report and Review of the Literature. Dig. Dis. Sci. 2015, 61, 708–712. [Google Scholar] [CrossRef]
- Lahner, E.; Pilozzi, E.; Esposito, G.; Galli, G.; Annibale, B. Gastric carcinoid in the absence of atrophic body gastritis and with low Ki67 index: A clinical challenge. Scand. J. Gastroenterol. 2014, 49, 506–510. [Google Scholar] [CrossRef]
- Jianu, C.S.; Fossmark, R.; Viset, T.; Qvigstad, G.; Sordal, O.; Marvik, R.; Waldum, H.L. Gastric carcinoids after long-term use of a proton pump inhibitor. Aliment. Pharmacol. Ther. 2012, 36, 644–649. [Google Scholar] [CrossRef]
- Calvete, O.; Reyes, J.; Zuniga, S.; Paumard-Hernandez, B.; Fernandez, V.; Bujanda, L.; Rodriguez-Pinilla, M.S.; Palacios, J.; Heine-Suner, D.; Banka, S.; et al. Exome sequencing identifies ATP4A gene as responsible of an atypical familial type I gastric neuroendocrine tumour. Hum. Mol. Genet. 2015, 24, 2914–2922. [Google Scholar] [CrossRef]
- Fossmark, R.; Calvete, O.; Mjones, P.; Benitez, J.; Waldum, H.L. ECL-cell carcinoids and carcinoma in patients homozygous for an inactivating mutation in the gastric H K ATPase alpha subunit. APMIS 2016. [Google Scholar] [CrossRef]
- Elsborg, L.; Mosbech, J. Pernicious anaemia as a risk factor in gastric cancer. Acta Med. Scand. 1979, 206, 315–318. [Google Scholar] [CrossRef]
- Sjöblom, S.M.; Sipponen, P.; Miettinen, M.; Karonen, S.L.; Jrvinen, H.J. Gastroscopic screening for gastric carcinoids and carcinoma in pernicious anemia. Endoscopy 1988, 20, 52–56. [Google Scholar] [CrossRef]
- Brusselaers, N.; Wahlin, K.; Engstrand, L.; Lagergren, J. Maintenance therapy with proton pump inhibitors and risk of gastric cancer: A nationwide population-based cohort study in Sweden. BMJ Open 2017, 7, e017739. [Google Scholar] [CrossRef]
- Brusselaers, N.; Lagergren, J.; Engstrand, L. Duration of use of proton pump inhibitors and the risk of gastric and oesophageal cancer. Cancer Epidemiol. 2019, 62, 101585. [Google Scholar] [CrossRef]
- Niikura, R.; Hayakawa, Y.; Hirata, Y.; Yamada, A.; Fujishiro, M.; Koike, K. Long-term proton pump inhibitor use is a risk factor of gastric cancer after treatment for Helicobacter pylori: A retrospective cohort analysis. Gut 2017. [Google Scholar] [CrossRef]
- Cheung, K.S.; Chan, E.W.; Wong, A.Y.S.; Chen, L.; Wong, I.C.K.; Leung, W.K. Long-term proton pump inhibitors and risk of gastric cancer development after treatment for Helicobacter pylori: A population-based study. Gut 2018, 67, 28–35. [Google Scholar] [CrossRef]
- Murphy, G.; Abnet, C.C.; Choo-Wosoba, H.; Vogtmann, E.; Weinstein, S.J.; Taylor, P.R.; Mannisto, S.; Albanes, D.; Dawsey, S.M.; Rehfeld, J.F.; et al. Serum gastrin and cholecystokinin are associated with subsequent development of gastric cancer in a prospective cohort of Finnish smokers. Int. J. Epidemiol. 2017, 46, 914–923. [Google Scholar] [CrossRef] [Green Version]
- Fossmark, R.; Sagatun, L.; Nordrum, I.S.; Sandvik, A.K.; Waldum, H.L. Hypergastrinemia is associated with adenocarcinomas in the gastric corpus and shorter patient survival. APMIS 2015, 123, 509–514. [Google Scholar] [CrossRef]
- Kuipers, E.J.; Lundell, L.; Klinkenberg-Knol, E.C.; Havu, N.; Festen, H.P.; Liedman, B.; Lamers, C.B.; Jansen, J.B.; Dalenback, J.; Snel, P.; et al. Atrophic gastritis and Helicobacter pylori infection in patients with reflux esophagitis treated with omeprazole or fundoplication. N. Engl. J. Med. 1996, 334, 1018–1022. [Google Scholar] [CrossRef]
- Niikura, R.; Hayakawa, Y.; Hirata, Y.; Ogura, K.; Fujishiro, M.; Yamada, A.; Ushiku, T.; Konishi, M.; Fukayama, M.; Koike, K. The Reduction in Gastric Atrophy after Helicobacter pylori Eradication Is Reduced by Treatment with Inhibitors of Gastric Acid Secretion. Int. J. Mol. Sci. 2019, 20, 1913. [Google Scholar] [CrossRef]
- Moayyedi, P.; Eikelboom, J.W.; Bosch, J.; Connolly, S.J.; Dyal, L.; Shestakovska, O.; Leong, D.; Anand, S.S.; Stork, S.; Branch, K.R.H.; et al. Safety of Proton Pump Inhibitors Based on a Large, Multi-year, Randomized Trial of Patients Receiving Rivaroxaban or Aspirin. Gastroenterology 2019, 157, 682–691. [Google Scholar] [CrossRef]
- El-Zimaity, H.M.; Jackson, F.W.; Graham, D.Y. Fundic gland polyps developing during omeprazole therapy. Am. J. Gastroenterol. 1997, 92, 1858–1860. [Google Scholar]
- Jalving, M.; Koornstra, J.J.; Wesseling, J.; Boezen, H.M.; De Jong, S.; Kleibeuker, J.H. Increased risk of fundic gland polyps during long-term proton pump inhibitor therapy. Aliment. Pharmacol. Ther. 2006, 24, 1341–1348. [Google Scholar] [CrossRef]
- Takahari, K.; Haruma, K.; Ohtani, H.; Kiyoto, S.; Watanabe, A.; Kamada, T.; Manabe, N.; Hatano, Y. Proton Pump Inhibitor Induction of Gastric Cobblestone-like Lesions in the Stomach. Intern. Med. 2017, 56, 2699–2703. [Google Scholar] [CrossRef] [Green Version]
- Ruffenach, S.J.; Siskind, M.S.; Lien, Y.H. Acute interstitial nephritis due to omeprazole. Am. J. Med. 1992, 93, 472–473. [Google Scholar] [CrossRef]
- Geevasinga, N.; Coleman, P.L.; Webster, A.C.; Roger, S.D. Proton pump inhibitors and acute interstitial nephritis. Clin. Gastroenterol. Hepatol. 2006, 4, 597–604. [Google Scholar] [CrossRef]
- Moledina, D.G.; Perazella, M.A. PPIs and kidney disease: From AIN to CKD. J. Nephrol. 2016, 29, 611–616. [Google Scholar] [CrossRef]
- Xie, Y.; Bowe, B.; Li, T.; Xian, H.; Balasubramanian, S.; Al-Aly, Z. Proton Pump Inhibitors and Risk of Incident CKD and Progression to ESRD. J. Am. Soc. Nephrol. 2016, 27, 3153–3163. [Google Scholar] [CrossRef] [Green Version]
- Lazarus, B.; Chen, Y.; Wilson, F.P.; Sang, Y.; Chang, A.R.; Coresh, J.; Grams, M.E. Proton Pump Inhibitor Use and the Risk of Chronic Kidney Disease. JAMA Intern. Med. 2016, 176, 238–246. [Google Scholar] [CrossRef] [Green Version]
- Ness-Jensen, E.; Fossmark, R. Adverse Effects of Proton Pump Inhibitors in Chronic Kidney Disease. JAMA Intern. Med. 2016, 176, 868. [Google Scholar] [CrossRef]
- Froissart, M.; Borensztein, P.; Houillier, P.; Leviel, F.; Poggioli, J.; Marty, E.; Bichara, M.; Paillard, M. Plasma membrane Na(+)-H+ antiporter and H(+)-ATPase in the medullary thick ascending limb of rat kidney. Am. J. Physiol. 1992, 262, C963–C970. [Google Scholar] [CrossRef]
- Sachs, G.; Wallmark, B. Biological basis of omeprazole therapy. J. Gastroenterol. Hepatol. 1989, 4 (Suppl. 2), 7–18. [Google Scholar]
- Howden, C.W.; Reid, J.L. Omeprazole, a gastric ‘proton pump inhibitor’: Lack of effect on renal handling of electrolytes and urinary acidification. Eur. J. Clin. Pharmacol. 1984, 26, 639–640. [Google Scholar] [CrossRef]
- Muriithi, A.K.; Leung, N.; Valeri, A.M.; Cornell, L.D.; Sethi, S.; Fidler, M.E.; Nasr, S.H. Biopsy-proven acute interstitial nephritis, 1993-2011: A case series. Am. J. Kidney Dis. 2014, 64, 558–566. [Google Scholar] [CrossRef]
- Yang, Y.X.; Lewis, J.D.; Epstein, S.; Metz, D.C. Long-term proton pump inhibitor therapy and risk of hip fracture. JAMA 2006, 296, 2947–2953. [Google Scholar] [CrossRef]
- Targownik, L.E.; Lix, L.M.; Metge, C.J.; Prior, H.J.; Leung, S.; Leslie, W.D. Use of proton pump inhibitors and risk of osteoporosis-related fractures. CMAJ 2008, 179, 319–326. [Google Scholar] [CrossRef] [Green Version]
- Vestergaard, P.; Rejnmark, L.; Mosekilde, L. Proton pump inhibitors, histamine H2 receptor antagonists, and other antacid medications and the risk of fracture. Calcif. Tissue Int. 2006, 79, 76–83. [Google Scholar] [CrossRef]
- Poly, T.N.; Islam, M.M.; Yang, H.C.; Wu, C.C.; Li, Y.J. Proton pump inhibitors and risk of hip fracture: A meta-analysis of observational studies. Osteoporos. Int. 2019, 30, 103–114. [Google Scholar] [CrossRef]
- Liu, J.; Li, X.; Fan, L.; Yang, J.; Wang, J.; Sun, J.; Wang, Z. Proton pump inhibitors therapy and risk of bone diseases: An update meta-analysis. Life Sci. 2019, 218, 213–223. [Google Scholar] [CrossRef]
- Targownik, L.E.; Lix, L.M.; Leung, S.; Leslie, W.D. Proton-pump inhibitor use is not associated with osteoporosis or accelerated bone mineral density loss. Gastroenterology 2010, 138, 896–904. [Google Scholar] [CrossRef]
- Targownik, L.E.; Goertzen, A.L.; Luo, Y.; Leslie, W.D. Long-Term Proton Pump Inhibitor Use Is Not Associated With Changes in Bone Strength and Structure. Am. J. Gastroenterol. 2017, 112, 95–101. [Google Scholar] [CrossRef]
- Thaler, H.W.; Sterke, C.S.; van der Cammen, T.J. Association of Proton Pump Inhibitor Use with Recurrent Falls and Risk of Fractures in Older Women: A Study of Medication Use in Older Fallers. J. Nutr. Health Aging 2016, 20, 77–81. [Google Scholar] [CrossRef]
- Hansen, K.E.; Nieves, J.W.; Nudurupati, S.; Metz, D.C.; Perez, M.C. Dexlansoprazole and Esomeprazole Do Not Affect Bone Homeostasis in Healthy Postmenopausal Women. Gastroenterology 2019, 156, 926–934. [Google Scholar] [CrossRef]
- Cui, G.L.; Syversen, U.; Zhao, C.M.; Chen, D.; Waldum, H.L. Long-term omeprazole treatment suppresses body weight gain and bone mineralization in young male rats. Scand. J. Gastroenterol. 2001, 36, 1011–1015. [Google Scholar]
- Schinke, T.; Schilling, A.F.; Baranowsky, A.; Seitz, S.; Marshall, R.P.; Linn, T.; Blaeker, M.; Huebner, A.K.; Schulz, A.; Simon, R.; et al. Impaired gastric acidification negatively affects calcium homeostasis and bone mass. Nat. Med. 2009, 15, 674–681. [Google Scholar] [CrossRef]
- Krause, M.; Keller, J.; Beil, B.; van Driel, I.; Zustin, J.; Barvencik, F.; Schinke, T.; Amling, M. Calcium gluconate supplementation is effective to balance calcium homeostasis in patients with gastrectomy. Osteoporos. Int. 2014. [Google Scholar] [CrossRef]
- Fossmark, R.; Stunes, A.K.; Petzold, C.; Waldum, H.L.; Rubert, M.; Lian, A.M.; Reseland, J.E.; Syversen, U. Decreased bone mineral density and reduced bone quality in H(+) /K(+) ATPase beta-subunit deficient mice. J. Cell. Biochem. 2012, 113, 141–147. [Google Scholar] [CrossRef]
- Aasarod, K.M.; Ramezanzadehkoldeh, M.; Shabestari, M.; Mosti, M.P.; Stunes, A.K.; Reseland, J.E.; Beisvag, V.; Eriksen, E.F.; Sandvik, A.K.; Erben, R.G.; et al. Skeletal effects of a gastrin receptor antagonist in H+/K+ATPase beta subunit KO mice. J. Endocrinol. 2016, 230, 251–262. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Goerss, J.B.; Kim, C.H.; Atkinson, E.J.; Eastell, R.; O’Fallon, W.M.; Melton, L.J., 3rd. Risk of fractures in patients with pernicious anemia. J. Bone Miner. Res. 1992, 7, 573–579. [Google Scholar] [CrossRef] [PubMed]
- Merriman, N.A.; Putt, M.E.; Metz, D.C.; Yang, Y.X. Hip fracture risk in patients with a diagnosis of pernicious anemia. Gastroenterology 2010, 138, 1330–1337. [Google Scholar] [CrossRef] [PubMed]
- Aasarod, K.M.; Mosti, M.P.; Stunes, A.K.; Reseland, J.E.; Basso, T.; Syversen, U.; Fossmark, R. Impaired skeletal health in patients with chronic atrophic gastritis. Scand. J. Gastroenterol. 2016, 51, 774–781. [Google Scholar] [CrossRef]
- Recker, R.R. Calcium absorption and achlorhydria. N. Engl. J. Med. 1985, 313, 70–73. [Google Scholar] [CrossRef]
- Hansen, K.E.; Jones, A.N.; Lindstrom, M.J.; Davis, L.A.; Ziegler, T.E.; Penniston, K.L.; Alvig, A.L.; Shafer, M.M. Do proton pump inhibitors decrease calcium absorption? J. Bone Miner. Res. 2010, 25, 2786–2795. [Google Scholar] [CrossRef] [Green Version]
- Wright, M.J.; Sullivan, R.R.; Gaffney-Stomberg, E.; Caseria, D.M.; O’Brien, K.O.; Proctor, D.D.; Simpson, C.A.; Kerstetter, J.E.; Insogna, K.L. Inhibiting gastric acid production does not affect intestinal calcium absorption in young, healthy individuals: A randomized, crossover, controlled clinical trial. J. Bone Miner. Res. 2010, 25, 2205–2211. [Google Scholar] [CrossRef] [Green Version]
- Tuukkanen, J.; Vaananen, H.K. Omeprazole, a specific inhibitor of H+-K+-ATPase, inhibits bone resorption in vitro. Calcif. Tissue Int. 1986, 38, 123–125. [Google Scholar] [CrossRef]
- Waldum, H.L.; Sandvik, A.K.; Brenna, E.; Petersen, H. Gastrin-histamine sequence in the regulation of gastric acid secretion. Gut 1991, 32, 698–701. [Google Scholar] [CrossRef]
- Barete, S.; Assous, N.; de Gennes, C.; Grandpeix, C.; Feger, F.; Palmerini, F.; Dubreuil, P.; Arock, M.; Roux, C.; Launay, J.M.; et al. Systemic mastocytosis and bone involvement in a cohort of 75 patients. Ann. Rheum. Dis. 2010, 69, 1838–1841. [Google Scholar] [CrossRef]
- Fitzpatrick, L.A.; Buzas, E.; Gagne, T.J.; Nagy, A.; Horvath, C.; Ferencz, V.; Mester, A.; Kari, B.; Ruan, M.; Falus, A.; et al. Targeted deletion of histidine decarboxylase gene in mice increases bone formation and protects against ovariectomy-induced bone loss. Proc. Natl. Acad. Sci. USA 2003, 100, 6027–6032. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Abrahamsen, B.; Vestergaard, P. Proton pump inhibitor use and fracture risk—Effect modification by histamine H1 receptor blockade. Observational case-control study using National Prescription Data. Bone 2013, 57, 269–271. [Google Scholar] [CrossRef] [PubMed]
- Aasarod, K.M.; Stunes, A.K.; Mosti, M.P.; Ramezanzadehkoldeh, M.; Viggaklev, B.I.; Reseland, J.E.; Skallerud, B.H.; Fossmark, R.; Syversen, U. Effects of the Histamine 1 Receptor Antagonist Cetirizine on the Osteoporotic Phenotype in H/K ATPase Beta Subunit KO Mice. J. Cell. Biochem. 2016, 117, 2089–2096. [Google Scholar] [CrossRef] [PubMed]
- Gomm, W.; von Holt, K.; Thome, F.; Broich, K.; Maier, W.; Fink, A.; Doblhammer, G.; Haenisch, B. Association of Proton Pump Inhibitors With Risk of Dementia: A Pharmacoepidemiological Claims Data Analysis. JAMA Neurol. 2016, 73, 410–416. [Google Scholar] [CrossRef]
- Haenisch, B.; von Holt, K.; Wiese, B.; Prokein, J.; Lange, C.; Ernst, A.; Brettschneider, C.; Konig, H.H.; Werle, J.; Weyerer, S.; et al. Risk of dementia in elderly patients with the use of proton pump inhibitors. Eur. Arch. Psychiatry Clin. Neurosci. 2015, 265, 419–428. [Google Scholar] [CrossRef]
- Welu, J.; Metzger, J.; Bebensee, S.; Ahrendt, A.; Vasek, M. Proton Pump Inhibitor Use and Risk of Dementia in the Veteran Population. Fed. Pract. 2019, 36, S27–S31. [Google Scholar]
- Badiola, N.; Alcalde, V.; Pujol, A.; Munter, L.M.; Multhaup, G.; Lleo, A.; Coma, M.; Soler-Lopez, M.; Aloy, P. The proton-pump inhibitor lansoprazole enhances amyloid beta production. PLoS ONE 2013, 8, e58837. [Google Scholar] [CrossRef]
- Bloom, G.S. Amyloid-beta and tau: The trigger and bullet in Alzheimer disease pathogenesis. JAMA Neurol. 2014, 71, 505–508. [Google Scholar] [CrossRef]
- Yin, R.H.; Tan, L.; Jiang, T.; Yu, J.T. Prion-like Mechanisms in Alzheimer’s Disease. Curr. Alzheimer Res. 2014, 11, 755–764. [Google Scholar] [CrossRef]
- Martinsen, T.C.; Taylor, D.M.; Johnsen, R.; Waldum, H.L. Gastric acidity protects mice against prion infection? Scand. J. Gastroenterol. 2002, 37, 497–500. [Google Scholar] [CrossRef]
- Martinsen, T.C.; Benestad, S.L.; Moldal, T.; Waldum, H.L. Inhibitors of gastric acid secretion increase the risk of prion infection in mice. Scand. J. Gastroenterol. 2011, 46, 1418–1422. [Google Scholar] [CrossRef] [PubMed]
- Park, S.K.; Nam, J.H.; Lee, H.; Chung, H.; Lee, E.K.; Shin, J.Y. Beyond uncertainty: Negative findings for the association between the use of proton pump inhibitors and risk of dementia. J. Gastroenterol. Hepatol. 2019. [Google Scholar] [CrossRef] [PubMed]
- Taipale, H.; Tolppanen, A.M.; Tiihonen, M.; Tanskanen, A.; Tiihonen, J.; Hartikainen, S. No Association Between Proton Pump Inhibitor Use and Risk of Alzheimer’s Disease. Am. J. Gastroenterol. 2017, 112, 1802–1808. [Google Scholar] [CrossRef] [PubMed]
- Tsai, C.F.; Chen, M.H.; Wang, Y.P.; Chu, C.J.; Huang, Y.H.; Lin, H.C.; Hou, M.C.; Lee, F.Y.; Su, T.P.; Lu, C.L. Proton Pump Inhibitors Increase Risk for Hepatic Encephalopathy in Patients With Cirrhosis in A Population Study. Gastroenterology 2017, 152, 134–141. [Google Scholar] [CrossRef]
- Fasullo, M.; Rau, P.; Liu, D.Q.; Holzwanger, E.; Mathew, J.P.; Guilarte-Walker, Y.; Szabo, G. Proton pump inhibitors increase the severity of hepatic encephalopathy in cirrhotic patients. World J. Hepatol. 2019, 11, 522–530. [Google Scholar] [CrossRef]
- Ma, Y.J.; Cao, Z.X.; Li, Y.; Feng, S.Y. Proton pump inhibitor use increases hepatic encephalopathy risk: A systematic review and meta-analysis. World J. Gastroenterol. 2019, 25, 2675–2682. [Google Scholar] [CrossRef]
- Tantai, X.X.; Yang, L.B.; Wei, Z.C.; Xiao, C.L.; Chen, L.R.; Wang, J.H.; Liu, N. Association of proton pump inhibitors with risk of hepatic encephalopathy in advanced liver disease: A meta-analysis. World J. Gastroenterol. 2019, 25, 2683–2698. [Google Scholar] [CrossRef]
- Ghosh, G.; Jesudian, A.B. Small Intestinal Bacterial Overgrowth in Patients With Cirrhosis. J. Clin. Exp. Hepatol. 2019, 9, 257–267. [Google Scholar] [CrossRef]
- Jackson, M.A.; Goodrich, J.K.; Maxan, M.E.; Freedberg, D.E.; Abrams, J.A.; Poole, A.C.; Sutter, J.L.; Welter, D.; Ley, R.E.; Bell, J.T.; et al. Proton pump inhibitors alter the composition of the gut microbiota. Gut 2016, 65, 749–756. [Google Scholar] [CrossRef]
- Clooney, A.G.; Bernstein, C.N.; Leslie, W.D.; Vagianos, K.; Sargent, M.; Laserna-Mendieta, E.J.; Claesson, M.J.; Targownik, L.E. A comparison of the gut microbiome between long-term users and non-users of proton pump inhibitors. Aliment. Pharmacol. Ther. 2016, 43, 974–984. [Google Scholar] [CrossRef]
- Min, Y.W.; Lim, K.S.; Min, B.H.; Gwak, G.Y.; Paik, Y.H.; Choi, M.S.; Lee, J.H.; Kim, J.J.; Koh, K.C.; Paik, S.W.; et al. Proton pump inhibitor use significantly increases the risk of spontaneous bacterial peritonitis in 1965 patients with cirrhosis and ascites: A propensity score matched cohort study. Aliment. Pharmacol. Ther. 2014, 40, 695–704. [Google Scholar] [CrossRef] [PubMed]
- Bajaj, J.S.; Zadvornova, Y.; Heuman, D.M.; Hafeezullah, M.; Hoffmann, R.G.; Sanyal, A.J.; Saeian, K. Association of proton pump inhibitor therapy with spontaneous bacterial peritonitis in cirrhotic patients with ascites. Am. J. Gastroenterol. 2009, 104, 1130–1134. [Google Scholar] [CrossRef]
- Llorente, C.; Jepsen, P.; Inamine, T.; Wang, L.; Bluemel, S.; Wang, H.J.; Loomba, R.; Bajaj, J.S.; Schubert, M.L.; Sikaroodi, M.; et al. Gastric acid suppression promotes alcoholic liver disease by inducing overgrowth of intestinal Enterococcus. Nat. Commun. 2017, 8, 837. [Google Scholar] [CrossRef]
- Horvath, A.; Rainer, F.; Bashir, M.; Leber, B.; Schmerboeck, B.; Klymiuk, I.; Groselj-Strele, A.; Durdevic, M.; Freedberg, D.E.; Abrams, J.A.; et al. Biomarkers for oralization during long-term proton pump inhibitor therapy predict survival in cirrhosis. Sci. Rep. 2019, 9, 1–9. [Google Scholar] [CrossRef] [PubMed]
- Tran, K.T.; McMenamin, U.C.; Hicks, B.; Murchie, P.; Thrift, A.P.; Coleman, H.G.; Iversen, L.; Johnston, B.T.; Lee, A.J.; Cardwell, C.R. Proton pump inhibitor and histamine-2 receptor antagonist use and risk of liver cancer in two population-based studies. Aliment. Pharmacol. Ther. 2018, 48, 55–64. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Thorens, J.; Froehlich, F.; Schwizer, W.; Saraga, E.; Bille, J.; Gyr, K.; Duroux, P.; Nicolet, M.; Pignatelli, B.; Blum, A.L.; et al. Bacterial overgrowth during treatment with omeprazole compared with cimetidine: A prospective randomised double blind study. Gut 1996, 39, 54–59. [Google Scholar] [CrossRef]
- Llorente, C.; Schnabl, B. The gut microbiota and liver disease. Cell. Mol. Gastroenterol. Hepatol. 2015, 1, 275–284. [Google Scholar] [CrossRef]
- Kummen, M.; Hov, J.R. The gut microbial influence on cholestatic liver disease. Liver Int. 2019, 39, 1186–1196. [Google Scholar] [CrossRef] [Green Version]
- Schenk, B.E.; Festen, H.P.; Kuipers, E.J.; Klinkenberg-Knol, E.C.; Meuwissen, S.G. Effect of short- and long-term treatment with omeprazole on the absorption and serum levels of cobalamin. Aliment. Pharmacol. Ther. 1996, 10, 541–545. [Google Scholar] [CrossRef]
- Lam, J.R.; Schneider, J.L.; Zhao, W.; Corley, D.A. Proton pump inhibitor and histamine 2 receptor antagonist use and vitamin B12 deficiency. JAMA 2013, 310, 2435–2442. [Google Scholar] [CrossRef]
- Den Elzen, W.P.; Groeneveld, Y.; de Ruijter, W.; Souverijn, J.H.; le Cessie, S.; Assendelft, W.J.; Gussekloo, J. Long-term use of proton pump inhibitors and vitamin B12 status in elderly individuals. Aliment. Pharmacol. Ther. 2008, 27, 491–497. [Google Scholar] [CrossRef] [PubMed]
- Attwood, S.E.; Ell, C.; Galmiche, J.P.; Fiocca, R.; Hatlebakk, J.G.; Hasselgren, B.; Langstrom, G.; Jahreskog, M.; Eklund, S.; Lind, T.; et al. Long-term safety of proton pump inhibitor therapy assessed under controlled, randomised clinical trial conditions: Data from the SOPRAN and LOTUS studies. Aliment. Pharmacol. Ther. 2015, 41, 1162–1174. [Google Scholar] [CrossRef] [PubMed]
- O’Connell, M.B.; Madden, D.M.; Murray, A.M.; Heaney, R.P.; Kerzner, L.J. Effects of proton pump inhibitors on calcium carbonate absorption in women: A randomized crossover trial. Am. J. Med. 2005, 118, 778–781. [Google Scholar] [CrossRef]
- Serfaty-Lacrosniere, C.; Wood, R.J.; Voytko, D.; Saltzman, J.R.; Pedrosa, M.; Sepe, T.E.; Russell, R.R. Hypochlorhydria from short-term omeprazole treatment does not inhibit intestinal absorption of calcium, phosphorus, magnesium or zinc from food in humans. J. Am. Coll. Nutr. 1995, 14, 364–368. [Google Scholar] [CrossRef]
- Ajmera, A.V.; Shastri, G.S.; Gajera, M.J.; Judge, T.A. Suboptimal response to ferrous sulfate in iron-deficient patients taking omeprazole. Am. J. Ther. 2012, 19, 185–189. [Google Scholar] [CrossRef]
- Van Aerts, R.M.; van Deursen, C.T.; Koek, G.H. Proton Pump Inhibitors Reduce the Frequency of Phlebotomy in Patients With Hereditary Hemochromatosis. Clin. Gastroenterol. Hepatol. 2016, 14, 147–152. [Google Scholar] [CrossRef]
- Hutchinson, C.; Geissler, C.A.; Powell, J.J.; Bomford, A. Proton pump inhibitors suppress absorption of dietary non-haem iron in hereditary haemochromatosis. Gut 2007, 56, 1291–1295. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cavalcoli, F.; Zilli, A.; Conte, D.; Massironi, S. Micronutrient deficiencies in patients with chronic atrophic autoimmune gastritis: A review. World J. Gastroenterol. 2017, 23, 563–572. [Google Scholar] [CrossRef] [PubMed]
- Lam, J.R.; Schneider, J.L.; Quesenberry, C.P.; Corley, D.A. Proton Pump Inhibitor and Histamine-2 Receptor Antagonist Use and Iron Deficiency. Gastroenterology 2017, 152, 821–829. [Google Scholar] [CrossRef]
- Epstein, M.; McGrath, S.; Law, F. Proton-pump inhibitors and hypomagnesemic hypoparathyroidism. N. Engl. J. Med. 2006, 355, 1834–1836. [Google Scholar] [CrossRef]
- Danziger, J.; William, J.H.; Scott, D.J.; Lee, J.; Lehman, L.W.; Mark, R.G.; Howell, M.D.; Celi, L.A.; Mukamal, K.J. Proton-pump inhibitor use is associated with low serum magnesium concentrations. Kidney Int. 2013, 83, 692–699. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Liao, S.; Gan, L.; Mei, Z. Does the use of proton pump inhibitors increase the risk of hypomagnesemia: An updated systematic review and meta-analysis. Medicine 2019, 98, e15011. [Google Scholar] [CrossRef] [PubMed]
- Cheungpasitporn, W.; Thongprayoon, C.; Kittanamongkolchai, W.; Srivali, N.; Edmonds, P.J.; Ungprasert, P.; O’Corragain, O.A.; Korpaisarn, S.; Erickson, S.B. Proton pump inhibitors linked to hypomagnesemia: A systematic review and meta-analysis of observational studies. Ren. Fail. 2015, 37, 1237–1241. [Google Scholar] [CrossRef] [PubMed]
- Hess, M.W.; Hoenderop, J.G.; Bindels, R.J.; Drenth, J.P. Systematic review: Hypomagnesaemia induced by proton pump inhibition. Aliment. Pharmacol. Ther. 2012, 36, 405–413. [Google Scholar] [CrossRef] [PubMed]
Figure 1.
Numerous side effects of proton pump inhibitors (PPIs) have been proposed, including increased risk of gastric neoplasia, kidney disease, dementia, liver disease, and fractures.
Figure 1.
Numerous side effects of proton pump inhibitors (PPIs) have been proposed, including increased risk of gastric neoplasia, kidney disease, dementia, liver disease, and fractures.

© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
MDPI and ACS Style
Fossmark, R.; Martinsen, T.C.; Waldum, H.L. Adverse Effects of Proton Pump Inhibitors—Evidence and Plausibility. Int. J. Mol. Sci. 2019, 20, 5203. https://0-doi-org.brum.beds.ac.uk/10.3390/ijms20205203
AMA Style
Fossmark R, Martinsen TC, Waldum HL. Adverse Effects of Proton Pump Inhibitors—Evidence and Plausibility. International Journal of Molecular Sciences. 2019; 20(20):5203. https://0-doi-org.brum.beds.ac.uk/10.3390/ijms20205203
Chicago/Turabian StyleFossmark, Reidar, Tom C. Martinsen, and Helge L. Waldum. 2019. "Adverse Effects of Proton Pump Inhibitors—Evidence and Plausibility" International Journal of Molecular Sciences 20, no. 20: 5203. https://0-doi-org.brum.beds.ac.uk/10.3390/ijms20205203
Note that from the first issue of 2016, this journal uses article numbers instead of page numbers. See further details here.