
Hepatic Hydrothorax—An Independent Decompensating Event Associated with Long-Term Mortality in Patients with Cirrhosis

 ,
,  , ,
, ,
Abstract
:1. Introduction
1.1. Background
1.2. Aims
2. Materials and Methods
2.1. Study Design
2.2. Variables and Data Collection
2.2.1. Imaging
2.2.2. Prognostic Scores
2.2.3. Follow-Up
2.3. Statistical Analysis
3. Results
3.1. Characteristics of Patients with and without Hepatic Hydrothorax
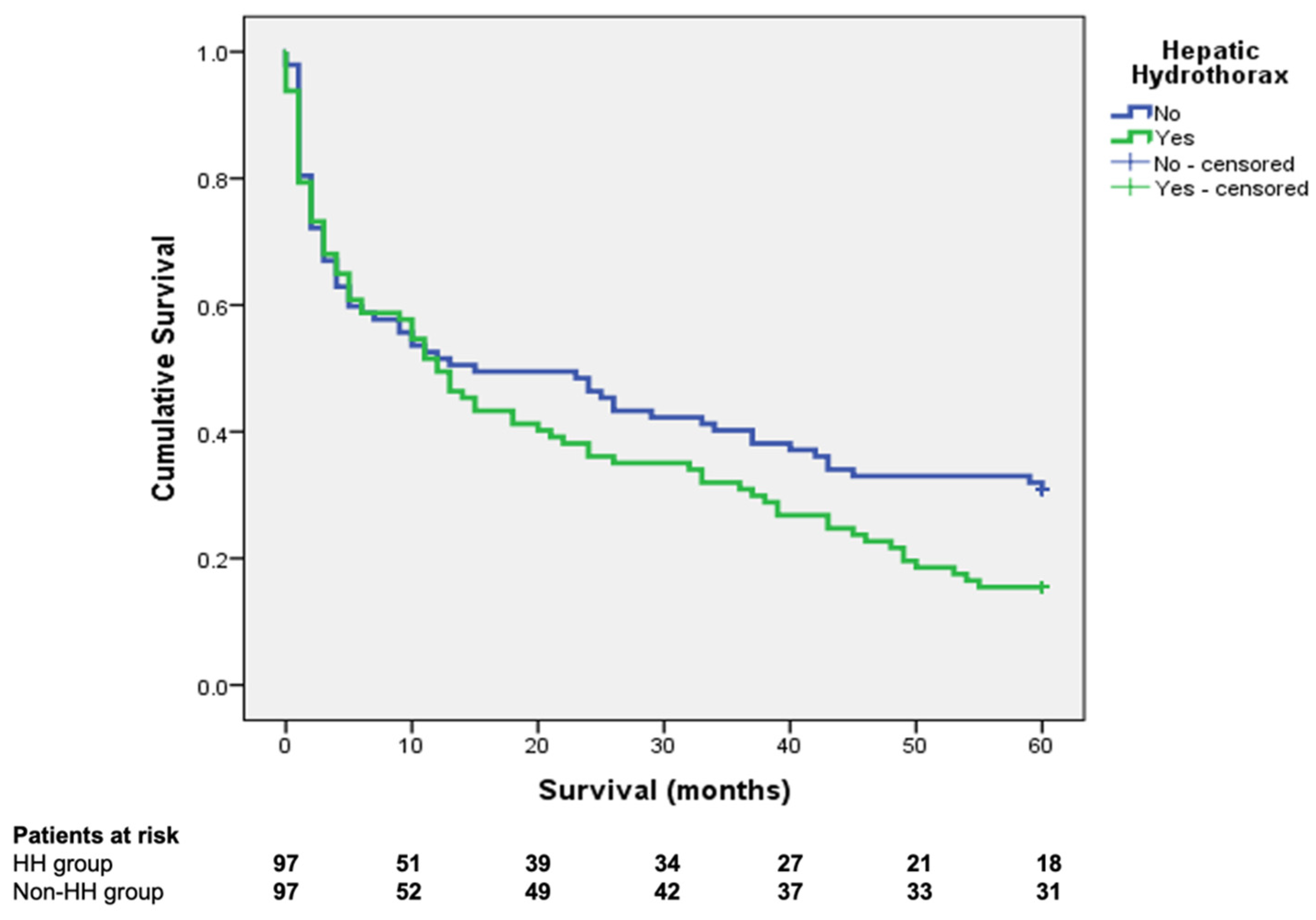
3.2. Long-Term Survival of Patients with Hepatic Hydrothorax
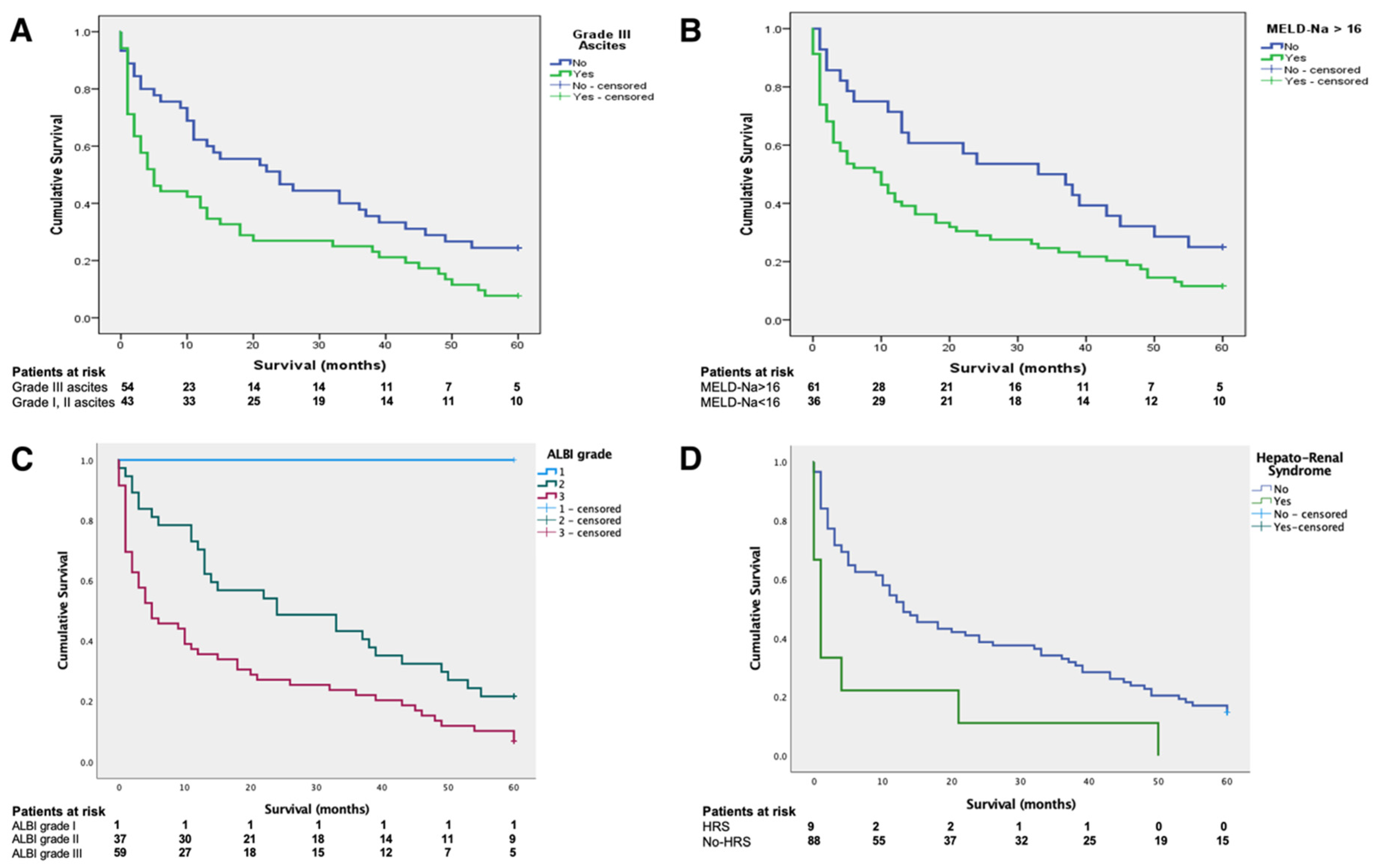
3.3. Natural History of HH and the Impact of Other Decompensating Events on Survival in Patients with HH
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Banini, B.A.; Alwatari, Y.; Stovall, M.; Ogden, N.; Gershman, E.; Shah, R.D.; Strife, B.J.; Shojaee, S.; Sterling, R.K. Multidisciplinary Management of Hepatic Hydrothorax in 2020: An Evidence-Based Review and Guidance. Hepatology 2020, 72, 1851–1863. [Google Scholar] [CrossRef]
- Chaaban, T.; Kanj, N.; Akl, I.B. Hepatic Hydrothorax: An Updated Review on a Challenging Disease. Lung 2019, 197, 399–405. [Google Scholar] [CrossRef]
- Lv, Y.; Han, G.; Fan, D. Hepatic hydrothorax. Ann. Hepatol. 2018, 17, 33–46. [Google Scholar] [CrossRef] [PubMed]
- Garbuzenko, D.V.; Arefyev, N. Hepatic hydrothorax: An update and review of the literature. World J. Hepatol. 2017, 9, 1197–1204. [Google Scholar] [CrossRef] [PubMed]
- Machicao, V.I.; Balakrishnan, M.; Fallon, M.B. Pulmonary complications in chronic liver disease. Hepatology 2014, 59, 1627–1637. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cardenas, A.; Kelleher, T.; Chopra, S. Review article: Hepatic hydrothorax. Aliment. Pharmacol. Ther. 2004, 20, 271–279. [Google Scholar] [CrossRef] [PubMed]
- Hou, F.; Qi, X.; Ning, Z.; Zhao, J.; Zhang, X.; Deng, H.; Peng, Y.; Li, J.; Yao, H.; Li, H.; et al. Prevalence, risk factors, and in-hospital outcome of pleural effusion in liver cirrhosis: A retrospective observational study. Int. J. Clin. Exp. Med. 2016, 9, 3265–3279. [Google Scholar]
- Angeli, P.; Bernardi, M.; Villanueva, C.; Francoz, C.; Mookerjee, R.; Trebicka, J.; Krag, A.; Laleman, W.; Gines, P. EASL Clinical Practice Guidelines for the management of patients with decompensated cirrhosis. J. Hepatol. 2018, 69, 406–460. [Google Scholar] [CrossRef] [Green Version]
- Atterbury, C.E.; Maddrey, W.C.; Conn, H.O. Neomycin-Sorbitol and Lactulose in the Treatment of Acute Portal-Systemic Encephalopathy—A controlled, Double-Blind clinical trial. Am. J. Dig. Dis. 1978, 23, 398–406. [Google Scholar] [CrossRef] [PubMed]
- Angeli, P.; Gines, P.; Wong, F.; Bernardi, M.; Boyer, T.D.; Gerbes, A.L.; Moreau, R.; Jalan, R.; Sarin, S.K.; Piano, S.; et al. Diagnosis and management of acute kidney injury in patients with cirrhosis: Revised consensus recommendations of the International Club of Ascites. Gut 2015, 64, 531–537. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pugh, R.N.H.; Murray-Lyon, I.M.; Dawson, J.L.; Pietroni, M.C.; Williams, R. Transection of the oesophagus for bleeding oesophageal varices. BJS 1973, 60, 646–649. [Google Scholar] [CrossRef] [PubMed]
- Biggins, S.W.; Kim, W.R.; Terrault, N.A.; Saab, S.; Balan, V.; Schiano, T.; Benson, J.; Therneau, T.; Kremers, W.; Wiesner, R.; et al. Evidence-Based Incorporation of Serum Sodium Concentration Into MELD. Gastroenterology 2006, 130, 1652–1660. [Google Scholar] [CrossRef]
- Johnson, P.J.; Berhane, S.; Kagebayashi, C.; Satomura, S.; Teng, M.; Reeves, H.L.; O’Beirne, J.; Fox, R.; Skowronska, A.; Palmer, D.; et al. Assessment of Liver Function in Patients with Hepatocellular Carcinoma: A New Evidence-Based Approach—The ALBI Grade. J. Clin. Oncol. 2015, 33, 550–558. [Google Scholar] [CrossRef] [PubMed]
- Kamath, P.S.; Kim, W.R. The model for end-stage liver disease (MELD). Hepatology 2007, 45, 797–805. [Google Scholar] [CrossRef] [PubMed]
- Arroyo, V.; Ginès, P.; Gerbes, A.L.; Dudley, F.J.; Gentilini, P.; Laffi, G.; Reynolds, T.B.; Ring-Larsen, H.; Schölmerich, J. Definition and diagnostic criteria of refractory ascites and hepatorenal syndrome in cirrhosis. Hepatology 1996, 23, 164–176. [Google Scholar] [CrossRef] [PubMed]
- Abbasi, A.; Bhutto, A.R.; Alam, M.T.; Aurangzaib, M.; Masroor, M. Frequency of Hepatic Hydrothorax and its Association with Child-Pugh Class in Liver Cirrhosis Patients. J. Coll. Phys. Surg. 2016, 26, 566–569. [Google Scholar]
- Badillo, R.; Rockey, D.C. Hepatic Hydrothorax: Clinical Features, Management, and Outcomes in 77 Patients and Review of the Literature. Medicine 2014, 93, 135–142. [Google Scholar] [CrossRef]
- Tseng, C.-W.; Hung, T.-H.; Tsai, C.-C.; Tsai, C.-C.; Tseng, K.-C.; Hsieh, Y.-H. The long-term outcomes of cirrhotic patients with pleural effusion. Saudi J. Gastroenterol. 2018, 24, 46–51. [Google Scholar] [CrossRef]
- Lee, W.J.; Kim, H.J.; Park, J.H.; Park, D.I.; Cho, Y.K.; Sohn, C.I.; Jeon, W.K.; Kim, B.I. Chemical pleurodesis for the management of refractory hepatic hydrothorax in patients with decompensated liver cirrhosis. Korean J. Hepatol. 2011, 17, 292–298. [Google Scholar] [CrossRef] [Green Version]
- Patil, M.; Dhillon, S.; Attwood, K.; Saoud, M.; Alraiyes, A.H.; Harris, K. Management of Benign Pleural Effusions Using Indwelling Pleural Catheters: A Systematic Review and Meta-analysis. Chest 2017, 151, 626–635. [Google Scholar] [CrossRef]
- Chen, A.; Massoni, J.; Jung, D.; Crippin, J. Indwelling Tunneled Pleural Catheters for the Management of Hepatic Hydrothorax. A Pilot Study. Ann. Am. Thorac. Soc. 2016, 13, 862–866. [Google Scholar] [CrossRef] [PubMed]
- Siegerstetter, V.; Deibert, P.; Ochs, A.; Olschewski, M.; Blum, H.E.; Rössle, M. Treatment of refractory hepatic hydrothorax with transjugular intrahepatic portosystemic shunt: Long-term results in 40 patients. Eur. J. Gastroenterol. Hepatol. 2001, 13, 529–534. [Google Scholar] [CrossRef] [PubMed]
- Ditah, I.C.; Al Bawardy, B.F.; Saberi, B.; Ditah, C.; Kamath, P.S. Transjugular intrahepatic portosystemic stent shunt for medically refractory hepatic hydrothorax: A systematic review and cumulative meta-analysis. World J. Hepatol. 2015, 7, 1797–1806. [Google Scholar] [CrossRef] [PubMed]
- Xiol, X.; Tremosa, G.; Castellote, J.; Gornals, J.; Lama, C.; López, C.; Figueras, J. Liver transplantation in patients with hepatic hydrothorax. Transpl. Int. 2005, 18, 672–675. [Google Scholar] [CrossRef]
- Sersté, T.; Moreno, C.; Francoz, C.; Razek, W.A.; Paugham, C.; Belghitti, J.; Valla, D.; Moreau, R.; Durand, F. The impact of preoperative hepatic hydrothorax on the outcome of adult liver transplantation. Eur. J. Gastroenterol. Hepatol. 2010, 22, 207–212. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Variable | No Hepatic Hydrothorax | Hepatic Hydrothorax | p-Value |
|---|---|---|---|
| N | 663 (86.89) | 100 (13.10) | |
| Gender—Female (N, %) | 238 (35.80) | 42 (42) | 0.24 |
| Age (years) | 60.57 ± 10.86 | 59.38 ± 9.20 | 0.29 |
| Liver disease etiology (N, %) | |||
| Alcohol Use | 279 (42.1) | 44 (44) | 0.60 |
| Viral | 256 (38.6) | 41 (41) | |
| Mixed (viral + alcoholic) | 66 (10) | 5 (5) | |
| Other | 62 (9.4) | 10 (10) | |
| Serum albumin (g/dL) | 3.14 ± 0.60 | 2.86 ± 0.54 | <0.01 |
| Total bilirubin (mg/dL) * | 2.30 (2.10–2.40) | 2.98 (2.58–3.41) | <0.01 |
| INR * | 1.54 (1.51–1.58) | 1.67 (1.59–1.77) | <0.01 |
| Child–Pugh A (N, %) | 147 (22.17) | 6 (6) | <0.01 |
| Child–Pugh B (N, %) | 290 (43.74) | 40 (40) | |
| Child–Pugh C (N, %) | 226 (34.08) | 54 (54) | |
| MELD | 16.08 ± 5.90 | 18.26 ± 6.18 | <0.01 |
| MELD-Na | 17.02 ± 6.95 | 20.16 ± 7.40 | <0.01 |
| ALBI Score | −1.59 ± 0.63 | −1.29 ± 0.61 | <0.01 |
| ALBI Grade 1 (N, %) | 35 (5.27) | 1(1) | <0.01 |
| ALBI Grade 2 (N, %) | 337 (50.8) | 39 (39) | |
| ALBI Grade 3 (N, %) | 251 (37.85) | 60 (60) | |
| Serum creatinine (mg/dL) * | 0.78 (0.75–0.80) | 0.86 (0.75–0.95) | <0.01 |
| 30 days mortality (N, %) | 99 (14.93) | 19 (19) | 0.15 |
| 6 months mortality (N, %) | 184 (27.75) | 32 (32) | 0.08 |
| Concomitant decompensating events | |||
| Grade 1 ascites (N, %) | 240 (36.19) | 18 (18) | <0.01 |
| Grade 2 ascites (N, %) | 192 (28.95) | 28 (28) | |
| Grade 3 ascites (N, %) | 231 (33.63) | 54 (54) | |
| Hepatic encephalopathy | 362 (54.60) | 74 (74) | <0.01 |
| Hepato-renal syndrome (N, %) | 30 (4.52) | 9 (9) | <0.01 |
| SPB OA (N, %) | 64 (9.65) | 21 (21) | <0.01 |
| ACLF | 14 (2.1) | 10 (10) | <0.01 |
| History of variceal bleeding (N, %) | 130 (19.6) | 23 (23) | 0.43 |
| Variables | Hazard Ratio | 95% Confidence Interval | p-Value |
|---|---|---|---|
| Age (years) | 1.01 | 0.99–1.03 | 0.16 |
| Gender (female) | 0.65 | 0.45–0.92 | 0.01 |
| Total bilirubin (mg/dL) | 1.05 | 1.03–1.08 | <0.01 |
| INR on admission | 1.1 | 0.90–1.60 | 0.21 |
| Creatinine on admission (mg/dL) | 1.05 | 0.89–1.23 | 0.55 |
| Kidney dysfunction during hospital stay | 3.27 | 1.80–5.95 | <0.01 |
| Hepato-renal syndrome during hospital stay | 4.72 | 2.18–10.21 | <0.01 |
| Sodium levels (mEq/L) | 0.93 | 0.91–0.96 | <0.01 |
| Serum albumin (g/dL) | 0.54 | 0.40–0.74 | <0.01 |
| Grade III ascites | 1.93 | 1.40–2.68 | <0.01 |
| Spontaneous bacterial peritonitis | 2.26 | 1.50–3.39 | <0.01 |
| Hepatic encephalopathy | 1.23 | 0.87–1.73 | 0.23 |
| Child–Pugh Class C | 1.24 | 0.79–1.66 | 0.41 |
| MELD score | 1.06 | 1.03–1.08 | <0.01 |
| MELD-Na score | 1.06 | 1.04–1.09 | <0.01 |
| ALBI score | 2.25 | 1.66–3.07 | <0.01 |
| ALBI grade | 2.27 | 1.67–3.10 | <0.01 |
| Hepatic hydrothorax | 1.37 | 1.00–1.89 | 0.05 |
| Variables | Hazard Ratio | 95% Confidence Interval | p-Value |
|---|---|---|---|
| MELD-Na score | 1.03 | 1.00–1.06 | 0.04 |
| ALBI grade | 1.66 | 1.15–2.38 | 0.01 |
| Hepato-renal syndrome during hospital stay | 2.60 | 1.05–6.41 | 0.03 |
| Grade III ascites | 1.58 | 1.13–2.21 | 0.01 |
| Hepatic hydrothorax | 1.18 | 1.00–1.68 | 0.04 |
| Variable | Hazard Ratio | 95% Confidence Interval | p-Value |
|---|---|---|---|
| Age (years) | 1.01 | 0.99–1.04 | 0.14 |
| Gender (female) | 0.68 | 0.43–1.07 | 0.09 |
| Total bilirubin (mg/dL) | 1.05 | 1.02–1.09 | <0.01 |
| INR on admission | 1.3 | 0.83–2.04 | 0.23 |
| Creatinine on admission (mg/dL) | 0.99 | 0.79–1.23 | 0.94 |
| Kidney dysfunction during hospital stay | 2.58 | 1.28–5.20 | <0.01 |
| Hepato-renal syndrome during hospital stay | 3.91 | 1.40–10.87 | <0.01 |
| Sodium levels (mEq/L) | 0.93 | 0.90–0.96 | <0.01 |
| Serum albumin (g/dL) | 0.55 | 0.35–0.87 | 0.01 |
| Grade III ascites | 1.75 | 1.12–2.73 | 0.01 |
| Spontaneous bacterial peritonitis | 2.1 | 1.24–3.53 | <0.01 |
| Hepatic encephalopathy | 1.29 | 0.77–2.16 | 0.32 |
| Child–Pugh Class C | 1.2 | 0.77–1.86 | 0.4 |
| MELD score | 1.05 | 1.01–1.09 | <0.01 |
| MELD-Na score | 1.06 | 1.03–1.09 | <0.01 |
| ALBI score | 2.01 | 1.31–3.09 | <0.01 |
| ALBI grade | 1.9 | 1.22–2.96 | 0.04 |
| Hazard Ratio | 95% Confidence Interval | p-Value | |
|---|---|---|---|
| MELD-Na score | 1.03 | 1.01–1.06 | 0.01 |
| ALBI grade | 1.69 | 1.19–2.40 | <0.01 |
| Hepato-renal syndrome during hospital stay | 2.43 | 1.31–4.51 | <0.01 |
| Grade III ascites | 1.53 | 1.09–2.13 | 0.01 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Matei, D.; Craciun, R.; Crisan, D.; Procopet, B.; Mocan, T.; Pasca, S.; Zaharie, R.; Popovici, B.; Sparchez, Z. Hepatic Hydrothorax—An Independent Decompensating Event Associated with Long-Term Mortality in Patients with Cirrhosis. J. Clin. Med. 2021, 10, 3688. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm10163688
Matei D, Craciun R, Crisan D, Procopet B, Mocan T, Pasca S, Zaharie R, Popovici B, Sparchez Z. Hepatic Hydrothorax—An Independent Decompensating Event Associated with Long-Term Mortality in Patients with Cirrhosis. Journal of Clinical Medicine. 2021; 10(16):3688. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm10163688
Chicago/Turabian StyleMatei, Daniela, Rares Craciun, Dana Crisan, Bogdan Procopet, Tudor Mocan, Sergiu Pasca, Roxana Zaharie, Bogdan Popovici, and Zeno Sparchez. 2021. "Hepatic Hydrothorax—An Independent Decompensating Event Associated with Long-Term Mortality in Patients with Cirrhosis" Journal of Clinical Medicine 10, no. 16: 3688. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm10163688