
Early Diagnosis of Liver Metastases from Colorectal Cancer through CT Radiomics and Formal Methods: A Pilot Study

Abstract
:1. Introduction
- -
- To demonstrate the effectiveness and reliability of FMs also in a long follow-up time frame and in a small population cohort.
- -
- To assess the effectiveness and reliability of FMs imaging detection also after hepato-Biliary surgery.
2. Materials and Methods
2.1. Dataset
- -
- Evidence of CRC diagnosed at CT scan confirmed with histopathological exam;
- -
- Patients who performed the first CT scan and follow-up exams at our centre, in order to set the protocol on the same scan;
- -
- No evidence of liver lesion at the moment of primary diagnosis or at follow up after surgery;
- -
- Findings of previous liver surgery in metachronous patients already treated with surgical approach.
- -
- Evidence of synchronous liver lesions at first CT scan;
- -
- Underlying liver disease in both groups;
- -
- CT scan performed in other centres or with other type of scan setting.
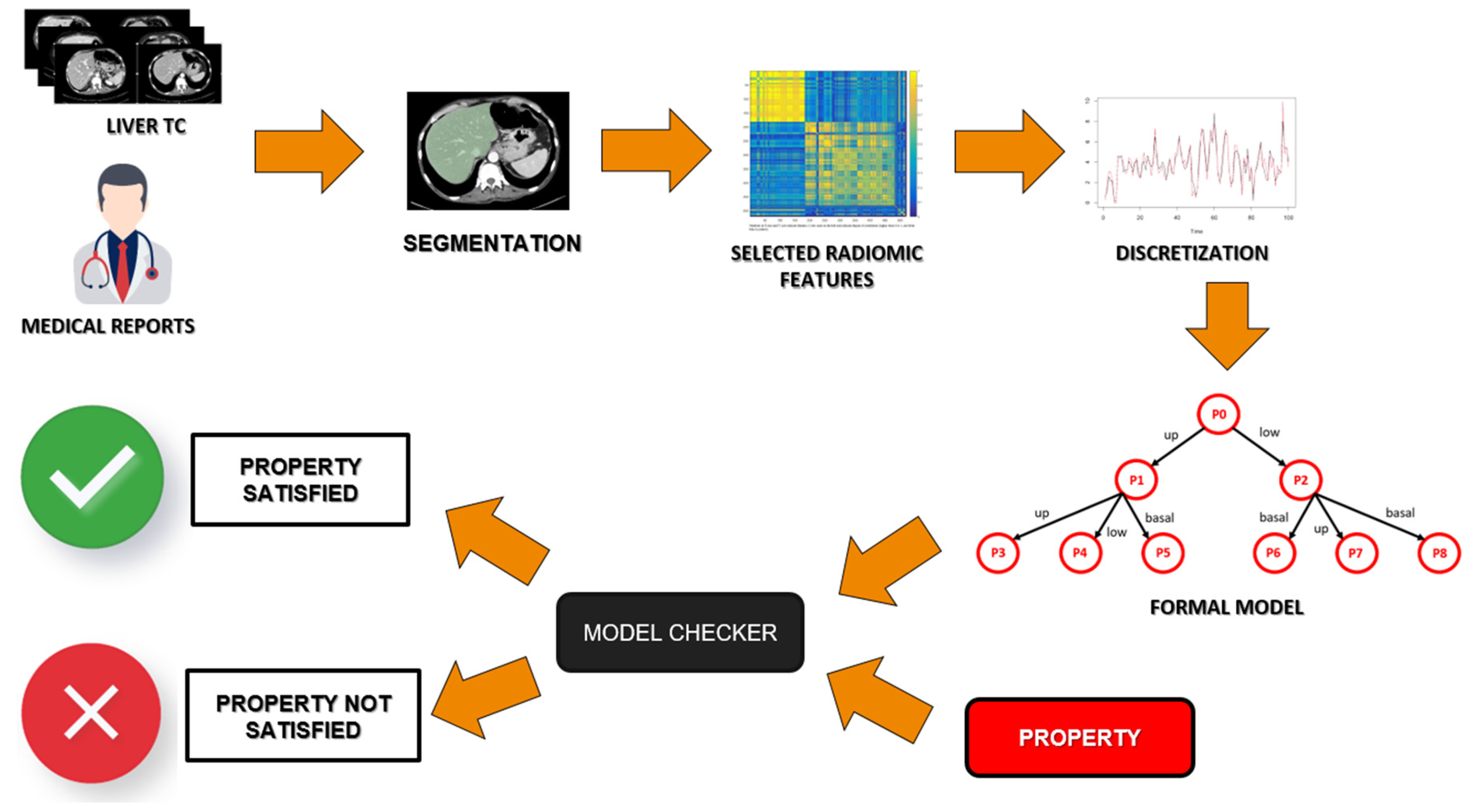
2.2. Image Acquisition and Segmentation
2.3. Radiomics Feature Extraction and Reduction
2.4. Formal Methodology
2.5. Outcome Extraction
- -
- True Positive Rate (TP): Number of metastatic patients correctly classified as “metastatic”;
- -
- False Positive Rate (FP): Number of healthy patients wrongly classified as “metastatic”;
- -
- False Negative Rate (FN): Number of metastatic patients wrongly classified as “healthy”;
- -
- True Negative Rate (TN): Number of healthy patients correctly classified as “healthy”.
- -
- Precision: correct assignment to the class of positives;
- -
- Recall: the completeness of the assignment to the class of the positives;
- -
- Accuracy: the fraction of correctly classified cases.
3. Results
4. Discussion
5. Limitations
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- World Health Organization International Agency for Research on Cancer (IARC). GLOBOCAN 2012: Estimated Cancer Incidence, Mortality and Prevalence Worldwide in 2012. Available online: https://gco.iarc.fr/ (accessed on 15 November 2021).
- Valderrama-Treviño, A.I.; Barrera-Mera, B.; Ceballos-Villalva, J.C.; Montalvo-Javé, E.E. Hepatic Metastasis from Colorectal Cancer. Euroasian J. Hepatogastroenterol. 2017, 7, 166–175. [Google Scholar] [CrossRef] [PubMed]
- Rocca, A.; Cipriani, F.; Belli, G.; Berti, S.; Boggi, U.; Bottino, V.; Cillo, U.; Cescon, M.; Cimino, M.; Corcione, F.; et al. The Italian Consensus on minimally invasive simultaneous resections for synchronous liver metastasis and primary colorectal cancer: A Delphi methodology. Updates Surg. 2021, 73, 1247–1265. [Google Scholar] [CrossRef]
- Loffredo, D.; Marvaso, A.; Ceraso, S.; Cinelli, N.; Rocca, A.; Vitale, M.; Rossi, M.; Genovese, E.; Amato, B.; Cinelli, M. Minimal invasive surgery in treatment of liver metastases from colorectal carcinomas: Case studies and survival rates. BMC Surg. 2013, 13 (Suppl. S2), S45. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ceccarelli, G.; Andolfi, E.; Fontani, A.; Calise, F.; Rocca, A.; Giuliani, A. Robot-assisted liver surgery in a general surgery unit with a “Referral Centre Hub&Spoke Learning Program”. Early outcomes after our first 70 consecutive patients. Minerva Chir. 2018, 73, 460–468. [Google Scholar] [CrossRef] [PubMed]
- Haggar, F.A.; Boushey, R.P. Colorectal cancer epidemiology: Incidence, mortality, survival, and risk factors. Clin. Colon Rectal Surg. 2009, 22, 191–197. [Google Scholar] [CrossRef] [Green Version]
- Adam, R.; De Gramont, A.; Figueras, J.; Guthrie, A.; Kokudo, N.; Kunstlinger, F.; Loyer, E.; Poston, G.; Rougier, P.; Rubbia-Brandt, L.; et al. The oncosurgery approach to managing liver metastases from colorectal cancer: A multidisciplinary international consensus. Oncologist 2012, 17, 1225–1239. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Adam, R.; de Gramont, A.; Figueras, J.; Kokudo, N.; Kunstlinger, F.; Loyer, E.; Poston, G.; Rougier, P.; Rubbia-Brandt, L.; Sobrero, A.; et al. Managing synchronous liver metastases from colorectal cancer: A multidisciplinary international consensus. Cancer Treat. Rev. 2015, 41, 729–741. [Google Scholar] [CrossRef] [Green Version]
- Keller, D.S.; Berho, M.; Perez, R.O.; Wexner, S.D.; Chand, M. The multidisciplinary management of rectal cancer. Nat. Rev. Gastroenterol. Hepatol. 2020, 17, 414–429. [Google Scholar] [CrossRef]
- Rocca, A.; Scacchi, A.; Cappuccio, M.; Avella, P.; Bugiantella, W.; De Rosa, M.; Costa, G.; Polistena, A.; Codacci-Pisanelli, M.; Amato, B.; et al. Robotic surgery for colorectal liver metastases resection: A systematic review. Int. J. Med. Robot. 2021, 17, e2330. [Google Scholar] [CrossRef]
- Ceccarelli, G.; Rocca, A.; De Rosa, M.; Fontani, A.; Ermili, F.; Andolfi, E.; Bugiantella, W.; Levi Sandri, G.B. Minimally invasive robotic-assisted combined colorectal and liver excision surgery: Feasibility, safety and surgical technique in a pilot series. Updates Surg. 2021, 73, 1015–1022. [Google Scholar] [CrossRef]
- Torzilli, G.; Montorsi, M.; Donadon, M.; Palmisano, A.; Del Fabbro, D.; Gambetti, A.; Olivari, N.; Makuuchi, M. “Radical but conservative” is the main goal for ultrasonography-guided liver resection: Prospective validation of this approach. J. Am. Coll. Surg. 2005, 201, 517–528. [Google Scholar] [CrossRef]
- Scharitzer, M.; Ba-Ssalamah, A.; Ringl, H.; Kölblinger, C.; Grünberger, T.; Weber, M.; Schima, W. Preoperative evaluation of colorectal liver metastases: Comparison between gadoxetic acid-enhanced 3.0-T MRI and contrast-enhanced MDCT with histopathological correlation. Eur. Radiol. 2013, 23, 2187–2196. [Google Scholar] [CrossRef]
- Rojas Llimpe, F.L.; Di Fabio, F.; Ercolani, G.; Giampalma, E.; Cappelli, A.; Serra, C.; Castellucci, P.; D’Errico, A.; Golfieri, R.; Pinna, A.D.; et al. Imaging in resectable colorectal liver metastasis patients with or without preoperative chemotherapy: Results of the PROMETEO-01 study. Br. J. Cancer 2014, 111, 667–673. [Google Scholar] [CrossRef] [Green Version]
- Rao, S.X.; Lambregts, D.M.; Schnerr, R.S.; van Ommen, W.; van Nijnatten, T.J.; Martens, M.H.; Heijnen, L.A.; Backes, W.H.; Verhoef, C.; Zeng, M.S.; et al. Whole-liver CT texture analysis in colorectal cancer: Does the presence of liver metastases affect the texture of the remaining liver? United Eur. Gastroenterol. J. 2014, 2, 530–538. [Google Scholar] [CrossRef] [Green Version]
- Beckers, R.C.J.; Beets-Tan, R.G.H.; Schnerr, R.S.; Maas, M.; da Costa Andrade, L.A.; Beets, G.L.; Dejong, C.H.; Houwers, J.B.; Lambregts, D.M.J. Whole-volume vs. segmental CT texture analysis of the liver to assess metachronous colorectal liver metastases. Abdom. Radiol. 2017, 42, 2639–2645. [Google Scholar] [CrossRef] [PubMed]
- Taghavi, M.; Trebeschi, S.; Simões, R.; Meek, D.B.; Beckers, R.C.J.; Lambregts, D.M.J.; Verhoef, C.; Houwers, J.B.; van der Heide, U.A.; Beets-Tan, R.G.H.; et al. Machine learning-based analysis of CT radiomics model for prediction of colorectal metachronous liver metastases. Abdom. Radiol. 2021, 46, 249–256. [Google Scholar] [CrossRef] [PubMed]
- Abdalla, E.K.; Vauthey, J.N.; Ellis, L.M.; Ellis, V.; Pollock, R.; Broglio, K.R.; Hess, K.; Curley, S.A. Recurrence and outcomes following hepatic resection, radiofrequency ablation, and combined resection/ablation for colorectal liver metastases. Ann. Surg. 2004, 239, 818–825; discussion 825–827. [Google Scholar] [CrossRef]
- Lee, S.J.; Zea, R.; Kim, D.H.; Lubner, M.G.; Deming, D.A.; Pickhardt, P.J. CT texture features of liver parenchyma for predicting development of metastatic disease and overall survival in patients with colorectal cancer. Eur. Radiol. 2018, 28, 1520–1528. [Google Scholar] [CrossRef] [PubMed]
- Fiz, F.; Viganò, L.; Gennaro, N.; Costa, G.; La Bella, L.; Boichuk, A.; Cavinato, L.; Sollini, M.; Politi, L.S.; Chiti, A.; et al. Radiomics of Liver Metastases: A Systematic Review. Cancers 2020, 12, 2881. [Google Scholar] [CrossRef]
- Beckers, R.C.J.; Lambregts, D.M.J.; Schnerr, R.S.; Maas, M.; Rao, S.X.; Kessels, A.G.H.; Thywissen, T.; Beets, G.L.; Trebeschi, S.; Houwers, J.B.; et al. Whole liver CT texture analysis to predict the development of colorectal liver metastases—A multicentre study. Eur. J. Radiol. 2017, 92, 64–71. [Google Scholar] [CrossRef]
- Hosny, A.; Parmar, C.; Quackenbush, J.; Schwartz, L.H.; Aerts, H. Artificial intelligence in radiology. Nat. Rev. Cancer 2018, 18, 500–510. [Google Scholar] [CrossRef]
- Reig, B.; Heacock, L.; Geras, K.J.; Moy, L. Machine learning in breast MRI. J. Magn. Reson. Imaging 2020, 52, 998–1018. [Google Scholar] [CrossRef]
- Santone, A.; Brunese, M.C.; Donnarumma, F.; Guerriero, P.; Mercaldo, F.; Reginelli, A.; Miele, V.; Giovagnoni, A.; Brunese, L. Radiomic features for prostate cancer grade detection through formal verification. Radiol. Med. 2021, 126, 688–697. [Google Scholar] [CrossRef] [PubMed]
- Granata, V.; Fusco, R.; Barretta, M.L.; Picone, C.; Avallone, A.; Belli, A.; Patrone, R.; Ferrante, M.; Cozzi, D.; Grassi, R.; et al. Radiomics in hepatic metastasis by colorectal cancer. Infect. Agent Cancer 2021, 16, 39. [Google Scholar] [CrossRef] [PubMed]
- Wesdorp, N.J.; van Goor, V.J.; Kemna, R.; Jansma, E.P.; van Waesberghe, J.; Swijnenburg, R.J.; Punt, C.J.A.; Huiskens, J.; Kazemier, G. Advanced image analytics predicting clinical outcomes in patients with colorectal liver metastases: A systematic review of the literature. Surg. Oncol. 2021, 38, 101578. [Google Scholar] [CrossRef]
- Santone, A.; Belfiore, M.P.; Mercaldo, F.; Varriano, G.; Brunese, L. On the Adoption of Radiomics and Formal Methods for COVID-19 Coronavirus Diagnosis. Diagnostics 2021, 11, 293. [Google Scholar] [CrossRef] [PubMed]
- Brunese, L.; Mercaldo, F.; Reginelli, A.; Santone, A. Formal methods for prostate cancer Gleason score and treatment prediction using radiomic biomarkers. Magn. Reson. Imaging 2020, 66, 165–175. [Google Scholar] [CrossRef]
- Brunese, L.; Mercaldo, F.; Reginelli, A.; Santone, A. Radiomics for Gleason Score Detection through Deep Learning. Sensors 2020, 20, 5411. [Google Scholar] [CrossRef] [PubMed]
- Francesco, N.D.; Lettieri, G.; Santone, A.; Vaglini, G. GreASE: A Tool for Efficient “Nonequivalence” Checking. ACM Trans. Softw. Eng. Methodol. (TOSEM) 2014, 23, 1–26. [Google Scholar] [CrossRef]
- Gradara, S.; Santone, A.; Villani, M.L. Using heuristic search for finding deadlocks in concurrent systems. Inf. Comput. 2005, 202, 191–226. [Google Scholar] [CrossRef] [Green Version]
- Fedorov, A.; Beichel, R.; Kalpathy-Cramer, J.; Finet, J.; Fillion-Robin, J.C.; Pujol, S.; Bauer, C.; Jennings, D.; Fennessy, F.; Sonka, M.; et al. 3D Slicer as an image computing platform for the Quantitative Imaging Network. Magn. Reson. Imaging 2012, 30, 1323–1341. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- van Griethuysen, J.J.M.; Fedorov, A.; Parmar, C.; Hosny, A.; Aucoin, N.; Narayan, V.; Beets-Tan, R.G.H.; Fillion-Robin, J.C.; Pieper, S.; Aerts, H. Computational Radiomics System to Decode the Radiographic Phenotype. Cancer Res. 2017, 77, e104–e107. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Eibe, F.; Hall, M.A.; Witten, I.H. The WEKA Workbench. Online Appendix for “Data Mining: Practical Machine Learning Tools and Techniques”; Morgan Kaufmann: Burlington, MA, USA, 2016. [Google Scholar]
- Hatt, M.; Vallieres, M.; Visvikis, D.; Zwanenburg, A. IBSI: An international community radiomics standardization initiative. J. Nucl. Med. 2018, 59 (Suppl. S1), 287. [Google Scholar]
- Hennessy, M.; Milner, R. Algebraic Laws for Nondeterminism and Concurrency; Association for Computing Machinery: New York, NY, USA, 1985; Volume 32, pp. 137–161. [Google Scholar]
- Milner, R. A Calculus of Communicating Systems; Springer: Berlin/Heidelberg, Germany, 1982. [Google Scholar]
- Pérez, B. Reasoning about clinical guidelines based on algebraic data types and constraint logic programming. J. Biomed. Inform. 2019, 92, 103134. [Google Scholar] [CrossRef] [PubMed]
- Horak, T.; Coenen, N.; Metzger, N.; Hahn, C.; Flemisch, T.; Mendez, J.; Dimov, D.; Finkbeiner, B.; Dachselt, R. Visual Analysis of Hyperproperties for Understanding Model Checking Results. IEEE Trans. Vis. Comput. Graph. 2021. [Google Scholar] [CrossRef] [PubMed]
- Mitchell, A.J. Sensitivity × PPV is a recognized test called the clinical utility index (CUI+). Eur. J. Epidemiol. 2011, 26, 251–252; author reply 252. [Google Scholar] [CrossRef] [Green Version]
- Liang, M.; Cai, Z.; Zhang, H.; Huang, C.; Meng, Y.; Zhao, L.; Li, D.; Ma, X.; Zhao, X. Machine Learning-based Analysis of Rectal Cancer MRI Radiomics for Prediction of Metachronous Liver Metastasis. Acad. Radiol. 2019, 26, 1495–1504. [Google Scholar] [CrossRef] [PubMed]
- Simpson, A.L.; Doussot, A.; Creasy, J.M.; Adams, L.B.; Allen, P.J.; DeMatteo, R.P.; Gönen, M.; Kemeny, N.E.; Kingham, T.P.; Shia, J.; et al. Computed Tomography Image Texture: A Noninvasive Prognostic Marker of Hepatic Recurrence After Hepatectomy for Metastatic Colorectal Cancer. Ann. Surg. Oncol. 2017, 24, 2482–2490. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| FIRST | GLDM | GLCM | GLRLM | GLSZM |
|---|---|---|---|---|
| Entropy | Dependence Entropy | Autocorrelation | High Grey-Level Run Emphasis | High Gray-Level Zone Emphasis |
| Interquartile Range Mean Absolute Deviation | High Grey-Level Emphasis | Joint Average | Long Run Low Grey-Level Emphasis | Low Grey-Level Zone Emphasis |
| Mean Absolute Deviation | Large Dependence Low Grey-Level Emphasis | Joint Entropy | Low Gray-Level Run Emphasis | Small Area Low Gray-Level Emphasis |
| Robust Mean Absolute Deviation | Low Grey-Level Emphasis | Sum Average | Short Run Low Grey-Level Emphasis | ________ |
| Uniformity | Small Dependance Low Grey-Level Emphasis | Sum Entropy | ________ | ________ |
| Confusion Matrix | Actual Values | ||
| Metastatic | Healthy | ||
| Predicted Values | Metastatic | TP = 7 | FP = 0 |
| Healthy | FN = 2 | TN = 21 | |
| Accuracy Statistics | Value | 95% Confidence Interval |
|---|---|---|
| Sensitivity | 77.8% | |
| Specificity | 100.0% | |
| Positive Predictive Value | 100.0% | |
| Negative Predictive Value | 91.3% | |
| Positive Likelihood Ratio (+Ve) | Inf | |
| Negative Likelihood Ratio (−Ve) | 0.222 | |
| Test Score (or fraction correct) % | 93.3% | |
| Prevalence | 30.0% | |
| Utility Statistics | Rating | 95% confidence interval |
| Clinical Utility (+Ve) | Good | 0.778 |
| Clinical Utility (−Ve) | Excellent | 0.913 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Rocca, A.; Brunese, M.C.; Santone, A.; Avella, P.; Bianco, P.; Scacchi, A.; Scaglione, M.; Bellifemine, F.; Danzi, R.; Varriano, G.; et al. Early Diagnosis of Liver Metastases from Colorectal Cancer through CT Radiomics and Formal Methods: A Pilot Study. J. Clin. Med. 2022, 11, 31. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm11010031
Rocca A, Brunese MC, Santone A, Avella P, Bianco P, Scacchi A, Scaglione M, Bellifemine F, Danzi R, Varriano G, et al. Early Diagnosis of Liver Metastases from Colorectal Cancer through CT Radiomics and Formal Methods: A Pilot Study. Journal of Clinical Medicine. 2022; 11(1):31. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm11010031
Chicago/Turabian StyleRocca, Aldo, Maria Chiara Brunese, Antonella Santone, Pasquale Avella, Paolo Bianco, Andrea Scacchi, Mariano Scaglione, Fabio Bellifemine, Roberta Danzi, Giulia Varriano, and et al. 2022. "Early Diagnosis of Liver Metastases from Colorectal Cancer through CT Radiomics and Formal Methods: A Pilot Study" Journal of Clinical Medicine 11, no. 1: 31. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm11010031