
Physical Activity and Exertional Desaturation Are Associated with Mortality in Idiopathic Pulmonary Fibrosis

Abstract
:
1. Introduction
2. Methods
2.1. Subjects and Setting
2.2. Physical Activity Assessment
2.3. Six-Minute Walking Test (6MWT)
2.4. Pulmonary Function Tests
2.5. Statistical Analysis
3. Results
4. Discussion
Acknowledgments
Author Contributions
Conflicts of Interest
References
- Raghu, G.; Collard, H.R.; Egan, J.J.; Martinez, F.J.; Behr, J.; Brown, K.K.; Colby, T.V.; Cordier, J.F.; Flaherty, K.R.; Lasky, J.A.; et al. An official ATS/ERS/JRS/ALAT statement: Idiopathic pulmonary fibrosis: Evidence-based guidelines for diagnosis and management. Am. J. Respir. Crit. Care Med. 2011, 183, 788–824. [Google Scholar] [CrossRef] [PubMed]
- Olson, A.L.; Swigris, J.J.; Lezotte, D.C.; Norris, J.M.; Wilson, C.G.; Brown, K.K. Mortality from pulmonary fibrosis increased in the United States from 1992 to 2003. Am. J. Respir. Crit. Care Med. 2007, 176, 277–284. [Google Scholar] [CrossRef] [PubMed]
- Meltzer, E.B.; Noble, P.W. Idiopathic pulmonary fibrosis. Orphanet J. Rare Dis. 2008, 3, 8. [Google Scholar] [CrossRef] [PubMed]
- Lama, V.N.; Flaherty, K.R.; Toews, G.B.; Colby, T.V.; Travis, W.D.; Long, Q.; Murray, S.; Kazerooni, E.A.; Gross, B.H.; Lynch, J.P., 3rd; et al. Prognostic value of desaturation during a 6-min walk test in idiopathic interstitial pneumonia. Am. J. Respir. Crit. Care Med. 2003, 168, 1084–1090. [Google Scholar] [CrossRef] [PubMed]
- Swigris, J.J.; Brown, K.K.; Make, B.J.; Wamboldt, F.S. Pulmonary rehabilitation in idiopathic pulmonary fibrosis: A call for continued investigation. Respir. Med. 2008, 102, 1675–1680. [Google Scholar] [CrossRef] [PubMed]
- Wallaert, B.; Monge, E.; Le Rouzic, O.; Wemeau-Stervinou, L.; Salleron, J.; Grosbois, J.M. Physical activity in daily life of patients with fibrotic idiopathic interstitial pneumonia. Chest 2013, 144, 1652–1658. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. Global Recommendations on Physical Activity for Health; World Health Organization: Geneva, Switzerland, 2010. [Google Scholar]
- Hallal, P.C.; Andersen, L.B.; Bull, F.C.; Guthold, R.; Haskell, W.; Ekelund, U.; Lancet Physical Activity Series Working Group. Global physical activity levels: Surveillance progress, pitfalls, and prospects. Lancet 2012, 380, 247–257. [Google Scholar] [CrossRef]
- Lee, I.M.; Shiroma, E.J.; Lobelo, F.; Puska, P.; Blair, S.N.; Katzmarzyk, P.T.; Lancet Physical Activity Series Working Group. Effect of physical inactivity on major non-communicable diseases worldwide: An analysis of burden of disease and life expectancy. Lancet 2012, 380, 219–229. [Google Scholar] [CrossRef]
- Spruit, M.A.; Singh, S.J.; Garvey, C.; Zuwallack, R.; Nici, L.; Rochester, C.; Hill, K.; Holland, A.E.; Lareau, S.C.; Man, W.D.; et al. An official american thoracic society/european respiratory society statement: Key concepts and advances in pulmonary rehabilitation. Am. J. Respir. Crit. Care Med. 2013, 188, e13–e64. [Google Scholar] [CrossRef] [PubMed]
- Nakayama, M.; Bando, M.; Araki, K.; Sekine, T.; Kurosaki, F.; Sawata, T.; Nakazawa, S.; Mato, N.; Yamasawa, H.; Sugiyama, Y. Physical activity in patients with idiopathic pulmonary fibrosis. Respirology 2015, 20, 640–646. [Google Scholar] [CrossRef] [PubMed]
- Leuchte, H.H.; Mernitz, P.; Baezner, C.; Baumgartner, R.A.; von Wulffen, W.; Neurohr, C.; Behr, J. Self-Report Daily Life Activity as a Prognostic Marker of Idiopathic Pulmonary Fibrosis. Respiration 2015, 90, 460–467. [Google Scholar] [CrossRef] [PubMed]
- Bouchard, C.; Blair, S.N.; Katzmarzyk, P.T. Less Sitting, More Physical Activity, or Higher Fitness? Mayo Clin. Proc. 2015, 90, 1533–1540. [Google Scholar] [CrossRef] [PubMed]
- Watz, H.; Pitta, F.; Rochester, C.L.; Garcia-Aymerich, J.; ZuWallack, R.; Troosters, T.; Vaes, A.W.; Puhan, M.A.; Jehn, M.; Polkey, M.I.; et al. An official European Respiratory Society statement on physical activity in COPD. Eur. Respir. J. 2014, 44, 1521–1537. [Google Scholar] [CrossRef] [PubMed]
- Vainshelboim, B.; Oliveira, J.; Yehoshua, L.; Weiss, I.; Fox, B.D.; Fruchter, O.; Kramer, M.R. Exercise Training-Based Pulmonary Rehabilitation Program Is Clinically Beneficial for Idiopathic Pulmonary Fibrosis. Respiration 2014, 88, 378–388. [Google Scholar] [CrossRef] [PubMed]
- Florey, C.D. Sample size for beginners. BMJ 1993, 306, 1181–1184. [Google Scholar] [CrossRef] [PubMed]
- Holland, A.E.; Hill, C.J.; Conron, M.; Munro, P.; McDonald, C.F. Short term improvement in exercise capacity and symptoms following exercise training in interstitial lung disease. Thorax 2008, 63, 549–554. [Google Scholar] [CrossRef] [PubMed]
- Vainshelboim, B.; Oliveira, J.; Fox, B.D.; Soreck, Y.; Fruchter, O.; Kramer, M.R. Long-term effects of a 12-week exercise training program on clinical outcomes in idiopathic pulmonary fibrosis. Lung 2015, 193, 345–354. [Google Scholar] [CrossRef] [PubMed]
- Vainshelboim, B.; Oliveira, J.; Fox, B.D.; Kramer, M.R. The Prognostic Role of Ventilatory Inefficiency and Exercise Capacity in Idiopathic Pulmonary Fibrosis. Respir. Care 2016, 61, 1100–1109. [Google Scholar] [CrossRef] [PubMed]
- Mahler, D.A.; Wells, C.K. Evaluation of clinical methods for rating dyspnea. Chest 1988, 93, 580–586. [Google Scholar] [CrossRef] [PubMed]
- Papiris, S.A.; Daniil, Z.D.; Malagari, K.; Kapotsis, G.E.; Sotiropoulou, C.; Milic-Emili, J.; Roussos, C. The Medical Research Council dyspnea scale in the estimation of disease severity in idiopathic pulmonary fibrosis. Respir. Med. 2005, 99, 755–761. [Google Scholar] [CrossRef] [PubMed]
- Craig, C.L.; Marshall, A.L.; Sjostrom, M.; Bauman, A.E.; Booth, M.L.; Ainsworth, B.E.; Pratt, M.; Ekelund, U.; Yngve, A.; Sallis, J.F.; et al. International physical activity questionnaire: 12-Country reliability and validity. Med. Sci. Sports Exerc. 2003, 35, 1381–1395. [Google Scholar] [CrossRef] [PubMed]
- Booth, M. Assessment of physical activity: An international perspective. Res. Q. Exerc. Sport 2000, 71 (Suppl. S2), S114–S120. [Google Scholar] [CrossRef] [PubMed]
- Lee, P.H.; Macfarlane, D.J.; Lam, T.H.; Stewart, S.M. Validity of the International Physical Activity Questionnaire Short Form (IPAQ-SF): A systematic review. Int. J. Behav. Nutr. Phys. Act. 2011, 8. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Garber, C.E.; Blissmer, B.; Deschenes, M.R.; Franklin, B.A.; Lamonte, M.J.; Lee, I.M.; Nieman, D.C.; Swain, D.P.; American College of Sports Medicine. American College of Sports Medicine position stand. Quantity and quality of exercise for developing and maintaining cardiorespiratory, musculoskeletal, and neuromotor fitness in apparently healthy adults: Guidance for prescribing exercise. Med. Sci. Sports Exerc. 2011, 43, 1334–1359. [Google Scholar] [PubMed]
- Pescatello, L.S.; American College of Sports Medicine. ACSM’s Guidelines for Exercise Testing and Prescription, 9th ed.; Wolters Kluwer/Lippincott Williams & Wilkins Health: Philadelphia, PA, USA, 2014. [Google Scholar]
- Haskell, W.L.; Lee, I.M.; Pate, R.R.; Powell, K.E.; Blair, S.N.; Franklin, B.A.; Macera, C.A.; Heath, G.W.; Thompson, P.D.; Bauman, A.; et al. Physical activity and public health: Updated recommendation for adults from the American College of Sports Medicine and the American Heart Association. Circulation 2007, 116, 1081–1093. [Google Scholar] [CrossRef] [PubMed]
- Pate, R.R.; Pratt, M.; Blair, S.N.; Haskell, W.L.; Macera, C.A.; Bouchard, C.; Buchner, D.; Ettinger, W.; Heath, G.W.; King, A.C.; et al. Physical activity and public health. A recommendation from the Centers for Disease Control and Prevention and the American College of Sports Medicine. JAMA 1995, 273, 402–407. [Google Scholar] [CrossRef] [PubMed]
- ATS Committee on Proficiency Standards for Clinical Pulmonary Function Laboratories. ATS statement: Guidelines for the six-minute walk test. Am. J. Respir. Crit. Care Med. 2002, 166, 111–117. [Google Scholar]
- Macintyre, N.; Crapo, R.O.; Viegi, G.; Johnson, D.C.; van der Grinten, C.P.; Brusasco, V.; Burgos, F.; Casaburi, R.; Coates, A.; Enright, P.; et al. Standardisation of the single-breath determination of carbon monoxide uptake in the lung. Eur. Respir. J. 2005, 26, 720–735. [Google Scholar] [CrossRef] [PubMed]
- Miller, M.R.; Crapo, R.; Hankinson, J.; Brusasco, V.; Burgos, F.; Casaburi, R.; Coates, A.; Enright, P.; van der Grinten, C.P.; Gustafsson, P.; et al. General considerations for lung function testing. Eur. Respir. J. 2005, 26, 153–161. [Google Scholar] [CrossRef] [PubMed]
- Wanger, J.; Clausen, J.L.; Coates, A.; Pedersen, O.F.; Brusasco, V.; Burgos, F.; Casaburi, R.; Crapo, R.; Enright, P.; van der Grinten, C.P.; et al. Standardisation of the measurement of lung volumes. Eur. Respir. J. 2005, 26, 511–522. [Google Scholar] [CrossRef] [PubMed]
- Quanjer, P.H.; Tammeling, G.J.; Cotes, J.E.; Pedersen, O.F.; Peslin, R.; Yernault, J.C. Lung volumes and forced ventilatory flows. Report Working Party Standardization of Lung Function Tests, European Community for Steel and Coal. Official Statement of the European Respiratory Society. Eur. Respir. J. Suppl. 1993, 16, 5–40. [Google Scholar] [CrossRef] [PubMed]
- Mura, M.; Porretta, M.A.; Bargagli, E.; Sergiacomi, G.; Zompatori, M.; Sverzellati, N.; Taglieri, A.; Mezzasalma, F.; Rottoli, P.; Saltini, C.; et al. Predicting survival in newly diagnosed idiopathic pulmonary fibrosis: A 3-year prospective study. Eur. Respir. J. 2012, 40, 101–109. [Google Scholar] [CrossRef] [PubMed]
- Wallaert, B.; Guetta, A.; Wemeau-Stervinou, L.; Terce, G.; Valette, M.; Neviere, R.; Aguilaniu, B. [Prognostic value of clinical exercise testing in idiopathic pulmonary fibrosis]. Rev. Mal. Respir. 2011, 28, 290–296. [Google Scholar] [CrossRef] [PubMed]
- Mukaka, M.M. Statistics corner: A guide to appropriate use of correlation coefficient in medical research. Malawi Med. J. 2012, 24, 69–71. [Google Scholar] [PubMed]
- du Bois, R.M.; Albera, C.; Bradford, W.Z.; Costabel, U.; Leff, J.A.; Noble, P.W.; Sahn, S.A.; Valeyre, D.; Weycker, D.; King, T.E., Jr. 6-Min walk distance is an independent predictor of mortality in patients with idiopathic pulmonary fibrosis. Eur. Respir. J. 2014, 43, 1421–1429. [Google Scholar] [CrossRef] [PubMed]
- Caminati, A.; Bianchi, A.; Cassandro, R.; Mirenda, M.R.; Harari, S. Walking distance on 6-MWT is a prognostic factor in idiopathic pulmonary fibrosis. Respir. Med. 2009, 103, 117–123. [Google Scholar] [CrossRef] [PubMed]
- Lederer, D.J.; Arcasoy, S.M.; Wilt, J.S.; D’Ovidio, F.; Sonett, J.R.; Kawut, S.M. Six-minute-walk distance predicts waiting list survival in idiopathic pulmonary fibrosis. Am. J. Respir. Crit. Care Med. 2006, 174, 659–664. [Google Scholar] [CrossRef] [PubMed]
- Lee, D.C.; Pate, R.R.; Lavie, C.J.; Sui, X.; Church, T.S.; Blair, S.N. Leisure-time running reduces all-cause and cardiovascular mortality risk. J. Am. Coll. Cardiol. 2014, 64, 472–481. [Google Scholar] [CrossRef] [PubMed]
- Tudor-Locke, C.; Craig, C.L.; Aoyagi, Y.; Bell, R.C.; Croteau, K.A.; De Bourdeaudhuij, I.; Ewald, B.; Gardner, A.W.; Hatano, Y.; Lutes, L.D.; et al. How many steps/day are enough? For older adults and special populations. Int. J. Behav. Nutr. Phys. Act. 2011, 8, 80. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Flaherty, K.R.; Andrei, A.C.; Murray, S.; Fraley, C.; Colby, T.V.; Travis, W.D.; Lama, V.; Kazerooni, E.A.; Gross, B.H.; Toews, G.B.; et al. Idiopathic pulmonary fibrosis: Prognostic value of changes in physiology and six-minute-walk test. Am. J. Respir. Crit. Care Med. 2006, 174, 803–809. [Google Scholar] [CrossRef] [PubMed]
- Nelson, M.E.; Rejeski, W.J.; Blair, S.N.; Duncan, P.W.; Judge, J.O.; King, A.C.; Macera, C.A.; Castaneda-Sceppa, C. Physical activity and public health in older adults: Recommendation from the American College of Sports Medicine and the American Heart Association. Circulation 2007, 116, 1094–1105. [Google Scholar] [CrossRef] [PubMed]
- Chodzko-Zajko, W.J.; Proctor, D.N.; Fiatarone Singh, M.A.; Minson, C.T.; Nigg, C.R.; Salem, G.J.; Skinner, J.S. American College of Sports Medicine position stand. Exercise and physical activity for older adults. Med. Sci. Sports Exerc. 2009, 41, 1510–1530. [Google Scholar] [CrossRef] [PubMed]
- Garcia-Aymerich, J.; Lange, P.; Benet, M.; Schnohr, P.; Anto, J.M. Regular physical activity reduces hospital admission and mortality in chronic obstructive pulmonary disease: A population based cohort study. Thorax 2006, 61, 772–778. [Google Scholar] [CrossRef] [PubMed]
- Waschki, B.; Kirsten, A.; Holz, O.; Muller, K.C.; Meyer, T.; Watz, H.; Magnussen, H. Physical activity is the strongest predictor of all-cause mortality in patients with COPD: A prospective cohort study. Chest 2011, 140, 331–342. [Google Scholar] [CrossRef] [PubMed]
- Hupin, D.; Roche, F.; Gremeaux, V.; Chatard, J.C.; Oriol, M.; Gaspoz, J.M.; Barthelemy, J.C.; Edouard, P. Even a low-dose of moderate-to-vigorous physical activity reduces mortality by 22% in adults aged ≥60 years: A systematic review and meta-analysis. Br. J. Sports Med. 2015, 49, 1262–1267. [Google Scholar] [CrossRef] [PubMed]
- Warburton, D.E.; Nicol, C.W.; Bredin, S.S. Health benefits of physical activity: The evidence. Can. Med. Assoc. J. 2006, 174, 801–809. [Google Scholar] [CrossRef] [PubMed]
- Wen, C.P.; Wai, J.P.; Tsai, M.K.; Yang, Y.C.; Cheng, T.Y.; Lee, M.C.; Chan, H.T.; Tsao, C.K.; Tsai, S.P.; Wu, X. Minimum amount of physical activity for reduced mortality and extended life expectancy: A prospective cohort study. Lancet 2011, 378, 1244–1253. [Google Scholar] [CrossRef]
- Vainshelboim, B.; Oliveira, J.; Fox, B.D.; Adir, Y.; Ollech, J.E.; Kramer, M.R. Physiological Profile and Limitations in Exercise in Idiopathic Pulmonary Fibrosis. J. Cardiopulm. Rehabil. Prev. 2016, 36, 270–278. [Google Scholar] [CrossRef] [PubMed]
- Lee, S.H.; Shim, H.S.; Cho, S.H.; Kim, S.Y.; Lee, S.K.; Son, J.Y.; Jung, J.Y.; Kim, E.Y.; Lim, J.E.; Lee, K.J.; et al. Prognostic factors for idiopathic pulmonary fibrosis: Clinical, physiologic, pathologic, and molecular aspects. Sarcoidosis Vasc. Diffuse Lung Dis. 2011, 28, 102–112. [Google Scholar] [PubMed]
- Helmerhorst, H.J.; Brage, S.; Warren, J.; Besson, H.; Ekelund, U. A systematic review of reliability and objective criterion-related validity of physical activity questionnaires. Int. J. Behav. Nutr. Phys. Act. 2012, 9, 103. [Google Scholar] [CrossRef] [PubMed]
- Gaunaurd, I.A.; Gomez-Marin, O.W.; Ramos, C.F.; Sol, C.M.; Cohen, M.I.; Cahalin, L.P.; Cardenas, D.D.; Jackson, R.M. Physical activity and quality of life improvements of patients with idiopathic pulmonary fibrosis completing a pulmonary rehabilitation program. Respir. Care 2014, 59, 1872–1879. [Google Scholar] [CrossRef] [PubMed]
- Vainshelboim, B.; Fox, B.D.; Kramer, M.R.; Izhakian, S.; Gershman, E.; Oliveira, J. Short-Term Improvement in Physical Activity and Body Composition After Supervised Exercise Training Program in Idiopathic Pulmonary Fibrosis. Arch. Phys. Med. Rehabil. 2016, 97, 788–797. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
{kind=link}
| Variables | Values |
|---|---|
| Age (years) | 68 (50–81) |
| Male/Female (n/%) | 22/12 (65%/35%) |
| Body mass index | 29 (22–37) |
| Time from diagnosis (years) | 1 (0.1–15) |
| Patients with smoking history (n/%) | 20 (59%) |
| Packs/year | 27 (0–112) |
| Supplemental oxygen users | |
| Rest | 4 (12%) |
| Exertion | 9 (26%) |
| Co-morbidities | |
| Pulmonary hypertension according to echocardiography (n/%) | 13 (38%) |
| Coronary arterial disease (n/%) | 14 (41%) |
| Systemic hypertension (n/%) | 24 (71%) |
| Chronic obstructive pulmonary disease–Emphysema (n/%) | 8 (24%) |
| Type 2 Diabetes (n/%) | 13 (38%) |
| Osteoporosis (n/%) | 5 (15%) |
| Medications | |
| Corticosteroids (n/%) | 23 (68%) |
| Pirfenidone (n/%) | 3 (9%) |
| Beta blockers (n/%) | 13 (38%) |
| Modified Medical Research Council-dyspnea scale (0–4) | |
| 0 | 1 (3%) |
| 1 | 14 (41%) |
| 2 | 8 (24%) |
| 3 | 10 (29%) |
| 4 | 1 (3%) |
| Resting cardiopulmonary parameters | |
| FVC % predicted | 68 (37–109) |
| FEV1 % predicted | 70 (35–124) |
| TLC % predicted | 64 (35–99) |
| DLCO % predicted | 50 (23–91) |
| SpO2 at rest (%) | 97 (87–99) |
| Exercise capacity, physical activity, and desaturation | |
| 6MWD (m) | 505 (130–749) |
| % predicted | 99 (35–147) |
| IPAQ (METS-min/week) | 648 (0–12,200) |
| ∆SpO2 (%) | 9 (0–27) |
| Cut-off Point for Parameters | AUC CI (95%) | Sensitivity (%) | Specificity (%) | p-Value |
|---|---|---|---|---|
| IPAQ ≤ 417 (MET-min/week) | 0.808 (0.66–0.96) | 82 | 70 | 0.004 |
| ∆SpO2 ≥ 10 (%) | 0.785 (0.28–0.77) | 91 | 74 | 0.008 |
| Survivors | Non-Survivors | Total | p-Value | |
|---|---|---|---|---|
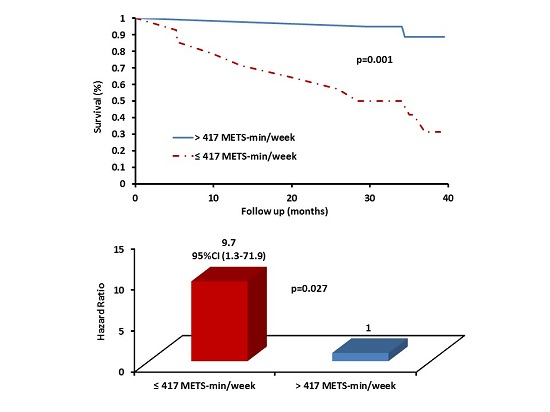
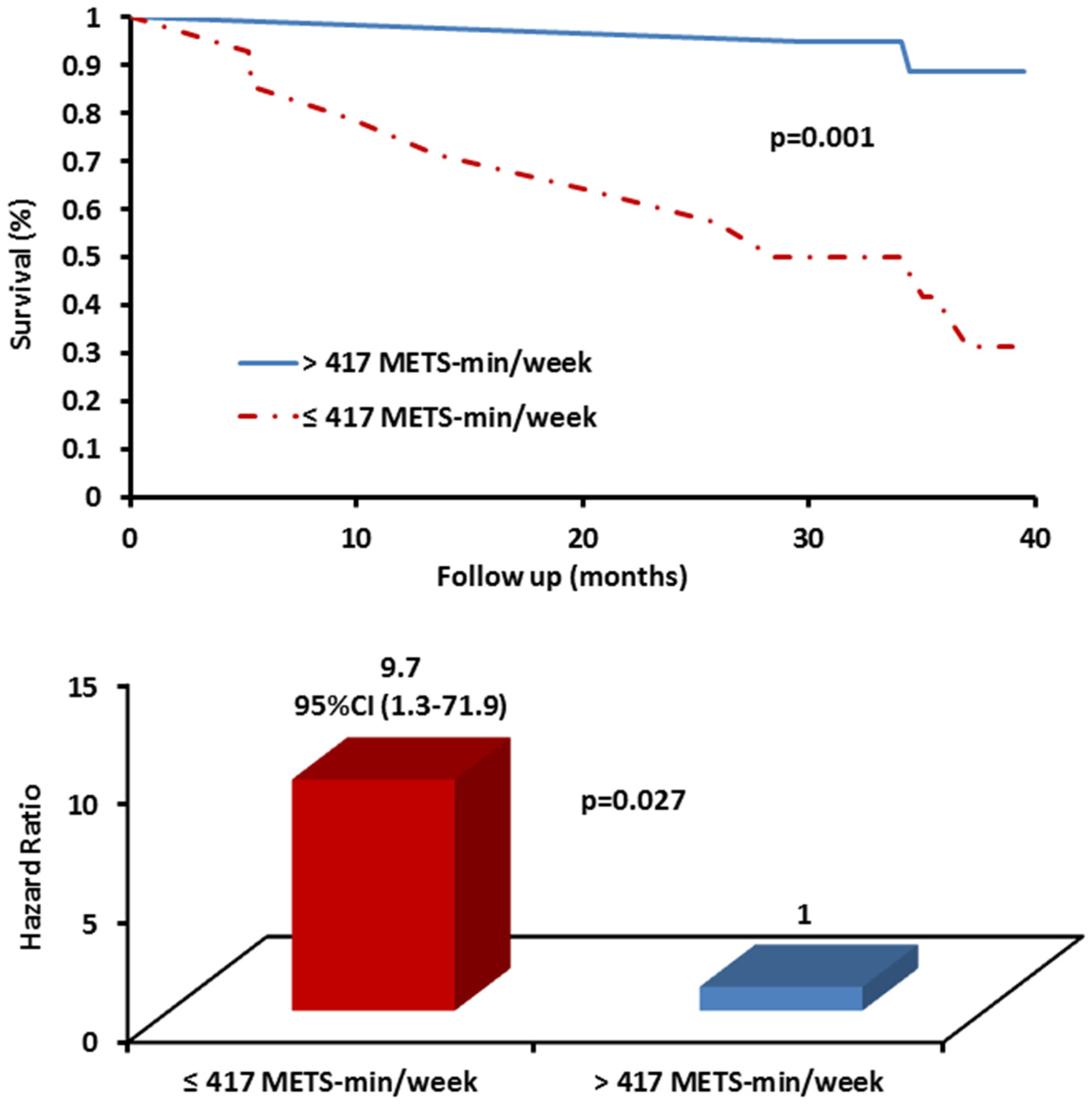
| IPAQ > 417 (MET-min/week) | 18 (90%) | 2 (10%) | 20 (100%) | 0.001 |
| IPAQ ≤ 417 (MET-min/week) | 5 (35.7%) | 9 (64.3%) | 14 (100%) | |
| ∆SpO2 < 10 (%) | 17 (94.4%) | 1 (5.6%) | 18 (100%) | <0.001 |
| ∆SpO2 ≥ 10 (%) | 6 (37.5%) | 10 (62.5%) | 16 (100%) |
© 2016 by the authors; licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC-BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Vainshelboim, B.; Kramer, M.R.; Izhakian, S.; Lima, R.M.; Oliveira, J. Physical Activity and Exertional Desaturation Are Associated with Mortality in Idiopathic Pulmonary Fibrosis. J. Clin. Med. 2016, 5, 73. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm5080073
Vainshelboim B, Kramer MR, Izhakian S, Lima RM, Oliveira J. Physical Activity and Exertional Desaturation Are Associated with Mortality in Idiopathic Pulmonary Fibrosis. Journal of Clinical Medicine. 2016; 5(8):73. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm5080073
Chicago/Turabian StyleVainshelboim, Baruch, Mordechai Reuven Kramer, Shimon Izhakian, Ricardo M. Lima, and Jose Oliveira. 2016. "Physical Activity and Exertional Desaturation Are Associated with Mortality in Idiopathic Pulmonary Fibrosis" Journal of Clinical Medicine 5, no. 8: 73. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm5080073