Are Early Warning Scores Useful Predictors for Mortality and Morbidity in Hospitalised Acutely Unwell Older Patients? A Systematic Review




Abstract
:1. Introduction
2. Materials and Methods
2.1. Search Strategy and Selection Criteria
2.2. Identification of Eligible Studies
2.3. Data Extraction
2.4. Quality Assessment
2.5. Data Analysis
3. Results
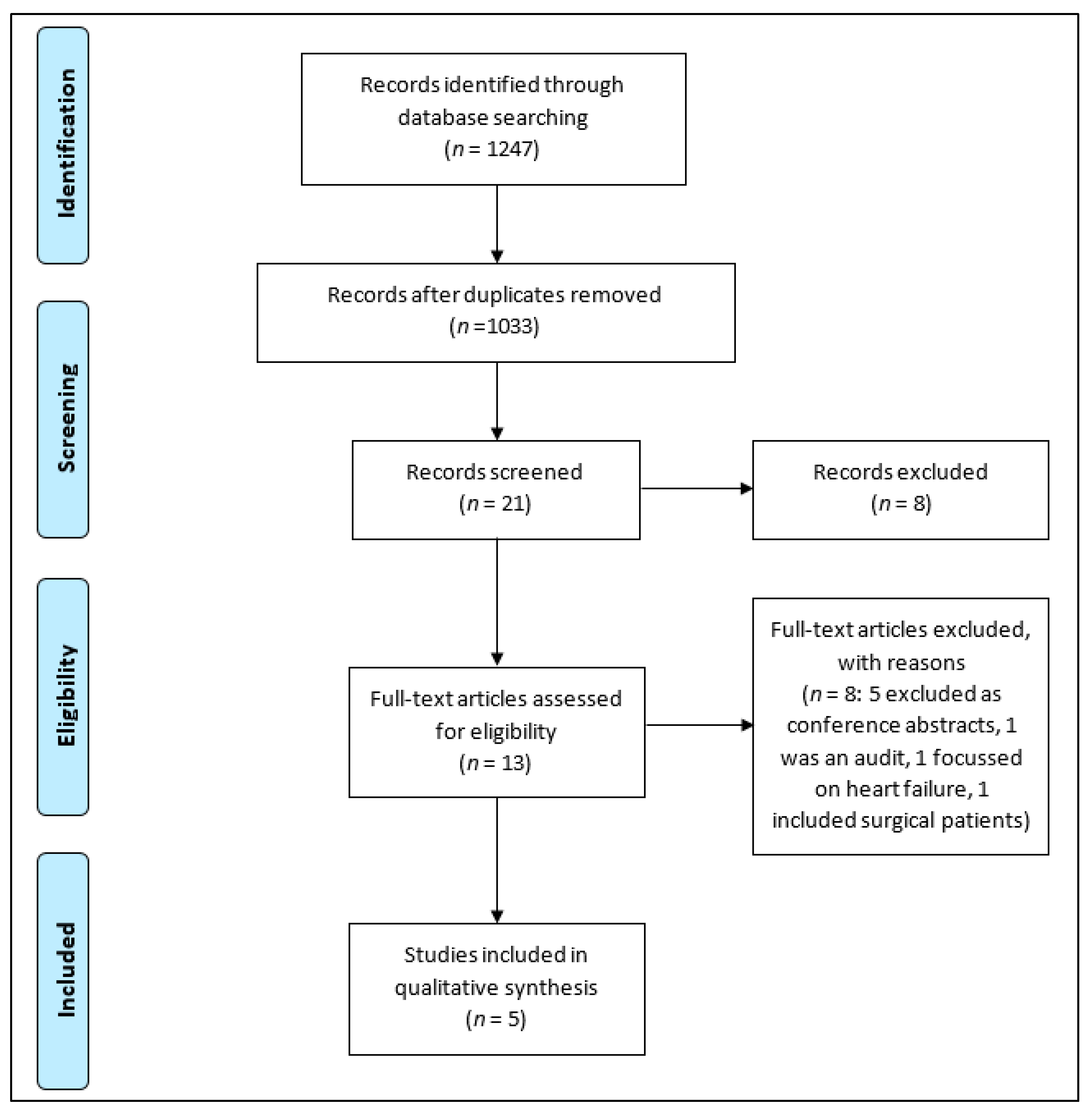
3.1. Search Strategy
3.2. Quality Assessment
3.3. Characteristics of Included Studies and EWS
3.4. Mortality
3.5. Morbidity
3.6. Composite Mortality/Morbidity Endpoint
4. Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgement
Conflicts of Interest
Ethical Approval
Appendix A
|
References
- Subbe, C.P.; Davies, R.G.; Williams, E.; Rutherford, P.; Gemmell, L. Effect of introducing the modified early warning score on clinical outcomes, cardio-pulmonary arrests and intensive care utilisation in acute medical admissions. Anaesthesia 2003, 58, 797–802. [Google Scholar] [CrossRef] [PubMed]
- Goldhill, D.R.; McNarry, A.F. Physiological abnormalities in early warning scores are related to mortality in adult inpatients. Br. J. Anaesth. 2004, 92, 882–884. [Google Scholar] [CrossRef] [PubMed]
- National Early Warning Score, National Clinical Guideline; NCEC: Dublin, Ireland, 2013. Available online: http://health.gov.ie/wp-content/uploads/2015/01/NEWSFull-ReportAugust2014.pdf (accessed on 1 February 2013).
- Subbe, C.P.; Kruger, M.; Rutherford, P.; Gemmel, L. Validation of a modified early warning score in medical admissions. QJM 2001, 94, 521–526. [Google Scholar] [CrossRef] [PubMed]
- Cei, M.; Bartolomei, C.; Mumoli, N. In-hospital mortality and morbidity of elderly medical patients can be predicted at admission by the modified early warning score: A prospective study. Int. J. Clin. Pract. 2009, 63, 591–595. [Google Scholar] [CrossRef] [PubMed]
- Liljehult, J.; Christensen, T. Early warning score predicts acute mortality in stroke patients. Acta. Neurol. Scand. 2016, 133, 261–267. [Google Scholar] [CrossRef] [PubMed]
- Huggan, P.J.; Akram, F.; Er, B.H.D.; Christen, L.S.J.; Weixian, L.; Lim, V.; Huang, Y.; Merchant, R.A. Measures of acute physiology, comorbidity and functional status to differentiate illness severity and length of stay among acute general medical admissions: A prospective cohort study. Intern. Med. J. 2015, 45, 732–740. [Google Scholar] [CrossRef] [PubMed]
- Health Quality and Safety Commission New Zealand. New Zealand Early Warning Score Vital Sign Chart User Guide; Health Quality and Safety Commission New Zealand: Wellington, New Zealand, 2017. Available online: https://www.hqsc.govt.nz/assets/Deteriorating-Patient/PR/Vital_sign_chart_user_guide_July_2017_.pdf (accessed on 21 July 2017).
- Royal College of Physicians. National Early Warning Score (NEWS)—Standardising the Assessment of Acute-Illness Severity in the NHS; Royal College of Physicians: London, UK, 2012; Available online: https://www.rcplondon.ac.uk/file/32/download?token=5NwjEyTq (accessed on 13 September 2018).
- Roney, J.K.; Whitley, B.E.; Maples, J.C.; Futrell, L.S.; Stunkard, K.A.; Long, J.A.D. Modified early warning scoring (MEWS): Evaluating the evidence for tool inclusion of sepsis screening criteria and impact on mortality and failure to rescue. J. Clin. Nurs. 2015, 24, 3343–3354. [Google Scholar] [CrossRef] [PubMed]
- Perera, Y.S.; Ranasinghe, P.; Adikari, A.M.M.C.; Welivita, W.D.T.S.; Perera, W.M.E.; Wijesundara, W.M.D.R.; Karunanayake, S.A.; Constantine, G.R. The value of the modified early warning score and biochemical parameters as predictors of patient outcome in acute medical admissions: A prospective study. Acute. Med. 2011, 10, 126–132. Available online: http://0-www-scopus-com.brum.beds.ac.uk/inward/record.url?eid=2-s2.0-80052882145&partnerID=tZOtx3y1 (accessed on 30 August 2011). [PubMed]
- Royal College of Physicians. Acute Medical Care for Frail Older People; Royal College of Physicians: London, UK, 2012; Available online: https://www.rcplondon.ac.uk/file/1197/download?token=-tA0spuS (accessed on 13 September 2018).
- Department of Health. Discharging Older Patients from Hospital. Available online: https://www.nao.org.uk/wp-content/uploads/2015/12/Discharging-older-patients-from-hospital-Summary.pdf (accessed on 26 May 2016).
- Nasa, P.; Juneja, D.; Singh, O. Severe sepsis and septic shock in the elderly: An overview. World J. Crit. Care Med. 2012, 1, 23–30. [Google Scholar] [PubMed]
- Yazdanyar, A.; Newman, A.B. The burden of cardiovascular disease in the elderly: Morbidity, mortality, and costs. Clin. Geriatr. Med. 2009, 25, 563–577. [Google Scholar] [CrossRef] [PubMed]
- Stupka, J.E.; Mortensen, E.M.; Anzueto, A.; Restrepo, M.I. Community-acquired pneumonia in elderly patients. Aging Health 2009, 5, 763–774. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- National Institute for Health and Care Excellence. Acutely Ill Adults in Hospital: Recognising and Responding to Deterioration. Guidance and Guidelines. Available online: https://www.nice.org.uk/guidance/cg50/chapter/1-Guidance#physiological-observations-in-acute-hospital-settings (accessed on 31 July 2007).
- SIGN. Care of Deteriorating Patients; SIGN: Edinburgh, UK, 2014; Available online: http://www.sign.ac.uk/assets/sign139.pdf (accessed on 31 May 2014).
- Sterne, J.A.; Hernán, M.A.; Reeves, B.C.; Savović, J.; Berkman, N.D.; Viswanathan, M.; Henry, D.; Altman, D.G.; Ansari, M.T.; Boutron, I. ROBINS-I: A tool for assessing risk of bias in non-randomised studies of interventions. BMJ 2016, 355, i4919. [Google Scholar] [CrossRef] [PubMed]
- Cochrane Methods: Bias. Robins-i Tool—Risk of Bias Tools. Available online: https://sites.google.com/site/riskofbiastool//welcome/home (accessed on 12 September 2018).
- Alrawi, Y.A.; Parker, R.A.; Harvey, R.C.; Sultanzadeh, S.J.; Patel, J.; Mallinson, R.; Potter, J.F.; Trepte, N.J.; Myint, P.K. Predictors of early mortality among hospitalized nursing home residents. QJM 2013, 106, 51–57. [Google Scholar] [CrossRef] [PubMed]
- Kellett, J.; Deane, B. The Simple Clinical Score predicts mortality for 30 days after admission to an acute medical unit. QJM 2006, 99, 771–781. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D. Preferred Reporting Items for Systematic Reviews and Meta-Analyses. PLoS Med. 2009, 6. Available online: http://prisma-statement.org/prismastatement/flowdiagram.aspx (accessed on 19 February 2018). [CrossRef] [PubMed]
- Johnstone, C.C.; Rattray, J.; Myers, L. Physiological risk factors, early warning scoring systems and organizational changes. Nurs. Crit. Care 2007, 12, 219–224. [Google Scholar] [CrossRef] [PubMed]
- Goldhill, D.R.; McNarry, A.F.; Hadjianastassiou, V.G.; Tekkis, P.P. The longer patients are in hospital before Intensive Care admission the higher their mortality. Intensive Care Med. 2004, 30, 1908–1913. [Google Scholar] [CrossRef] [PubMed]
- Tirkkonen, J.; Olkkola, K.T.; Huhtala, H.; Tenhunen, J.; Hoppu, S. Medical emergency team activation: Performance of conventional dichotomised criteria versus national early warning score. Acta Anaesthesiol. Scand. 2014, 58, 411–419. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Pre-Intervention | At Intervention | Post-Intervention | ||||||
|---|---|---|---|---|---|---|---|---|
| Study | Bias Due to Confounding | Bias in Selection of Participants | Bias in Classification of Interventions | Bias Due to Deviations from Intended Interventions | Bias Due to Missing Data | Bias in Measurement of Outcomes | Bias in Selection of Reported Result | Bias Across Domains |
| Liljehult and Christensen [6] | Critical | Low | Low | Low | Moderate | Moderate | Low | Moderate |
| Huggan et al. [7] | Low | Low | Low | Low | Low | Moderate | Low | Moderate |
| Alrawi et al. [21] | Low | Low | Low | Low | Low | Moderate | Low | Moderate |
| Cei et al. [5] | Moderate | Moderate | Low | Low | Low | Moderate | Low | Moderate |
| Kellett and Deane [22] | Serious | Low | Low | Low | Low | Moderate | Low | Moderate |
| Study | Population | Intervention | Outcomes | Total Number of Patients (n) | Age in Years | Country | Gender |
|---|---|---|---|---|---|---|---|
| Liljehult and Christensen [6] | Acute stroke admissions | EWS | Mortality within 30 days | 274 | 72.3 (12.7) | Denmark | 50% female |
| Huggan et al. [7] | Admissions to the acute medical ward | Modified EWS (MEWS) | (1) Death/higher level care admission (composite) (2) Excessive length of hospital stay (>7days) | 398 | 64.2 (10.2) | Singapore | 52% female |
| Alrawi et al. [21] | Admission to the acute medical unit from nursing homes | MEWS | Deaths within first week of admission. | 314 | 84.2 (8.3) | United Kingdom | 68% female |
| Cei et al. [5] | Admissions to medical ward from the emergency room or emergency medicine | MEWS | (1) In-hospital mortality (2) Mortality/ transfer to higher level care (composite) | 1107 | 89.9% >64 years | Italy | 56.1% female |
| Kellett and Deane [22] | Acute admissions to the medical unit | Simple clinical score | Mortality within 30 days | Derivation cohort = 6736 (Validation = 3228) | 61.9 (20.3) | Ireland | 47.4% female |
© 2018 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Jayasundera, R.; Neilly, M.; Smith, T.O.; Myint, P.K. Are Early Warning Scores Useful Predictors for Mortality and Morbidity in Hospitalised Acutely Unwell Older Patients? A Systematic Review. J. Clin. Med. 2018, 7, 309. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm7100309
Jayasundera R, Neilly M, Smith TO, Myint PK. Are Early Warning Scores Useful Predictors for Mortality and Morbidity in Hospitalised Acutely Unwell Older Patients? A Systematic Review. Journal of Clinical Medicine. 2018; 7(10):309. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm7100309
Chicago/Turabian StyleJayasundera, Romesh, Mark Neilly, Toby O. Smith, and Phyo Kyaw Myint. 2018. "Are Early Warning Scores Useful Predictors for Mortality and Morbidity in Hospitalised Acutely Unwell Older Patients? A Systematic Review" Journal of Clinical Medicine 7, no. 10: 309. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm7100309